Adenoma, Oxyphilic
Oxyphil Cells
Adenoma, Pleomorphic
Adenoma, Villous
Pituitary Neoplasms
Adrenocortical Adenoma
Adenoma, Chromophobe
Growth Hormone-Secreting Pituitary Adenoma
Colorectal Neoplasms
Colonic Polyps
ACTH-Secreting Pituitary Adenoma
Adenoma, Acidophil
Prolactinoma
Adenoma, Basophil
Expression of somatostatin receptors in oncocytic (Hurthle cell) neoplasia of the thyroid. (1/183)
Ten consecutive patients with Hurthle cell lesions of the thyroid (nodule/adenoma/carcinoma) were studied by (111)In-DTPA-D-Phe1-octreotide scintigraphy. Octreotide scintigraphy localized the primary Hurthle cell tumour in eight patients as distinct areas of increased uptake of radionuclide. Two patients with Hurthle cell carcinoma, previously thyroidectomized, had their metastases visualized by octreotide scintigraphy. Northern analyses showed expression of multiple somatostain receptor subtypes. Visualization of the Hurthle cell tumour may be due to a higher expression of somatostatin receptors in the lesions than in surrounding normal thyroid tissue. The tissue/blood (111)In concentration ratios for tumour samples from five patients showed clearly higher values than observed for normal connective tissue, muscle or lymph nodes. A relatively high uptake of (111)In was also observed in goiter tissue, which may lead to misinterpretations. The main indication for octreotide scintigraphy in patients with Hurthle cell carcinoma is suspicion of metastatic disease. (+info)Adrenocortical oncocytoma. (2/183)
The histopathology and ultrastructural features of an adrenocortical oncocytoma are reported. The tumour was discovered incidentally during investigation for hypertension in a 72 year old female. Oncocytic tumours of the adrenal cortex are rare, with only 20 examples described in English language reports. Most have been non-functioning and benign, like the present example. Molecular studies may help assess the significance of oncocytic change in the pathogenesis and behaviour of oncocytic neoplasms. (+info)Pathologic features, proliferative activity, and cyclin D1 expression in Hurthle cell neoplasms of the thyroid. (3/183)
Making a histologic distinction between Hurthle cell adenomas and carcinomas sometimes may be difficult. We analyzed a series of Hurthle cell lesions to determine whether specific histologic features and expression of Ki67 and cyclin D1 could be useful in distinguishing Hurthle cell adenomas from carcinomas. Formalin-fixed, paraffin-embedded tissues from 128 Hurthle cell neoplasms, including 59 adenomas; 55 carcinomas; and 14 tumors classified as neoplasms of uncertain malignant behavior (UMB), which had equivocal capsular invasion but no vascular invasion, were analyzed for expression of Ki67 and cyclin D1 by immunostaining. The distribution of immunoreactivity for Ki67 with antibody MIB-1 was analyzed by quantifying the percentage of positive nuclei that was expressed as the labeling index. None of the patients with adenomas or UMB tumors developed recurrent or metastatic disease after a mean follow-up of 7.8 and 7.9 years, respectively. Of the 55 patients with Hurthle cell carcinoma, 19 were associated with metastatic disease, 13 of whom died with disease. No patient with a Hurthle cell carcinoma without vascular invasion developed metastatic disease. The mean tumor size for Hurthle cell carcinomas (4.8 cm) was significantly larger than that of Hurthle cell adenomas (3.1 cm) or UMB tumors (3.7 cm). No patient with a Hurthle cell tumor smaller than 3.5 cm developed metastatic disease, even when vascular invasion was present. The Ki67 labeling index in Hurthle cell carcinomas (10.0 +/- 1.2) was 3-fold higher than in Hurthle cell adenomas (3.2 +/- 0.3). The Ki67 labeling index in the UMB group was 5.0 +/- 0.7. Cyclin D1 showed diffuse nuclear staining in 1 of the 59 (1.7%) Hurthle cell adenomas, in 10 of the 55 (18%) Hurthle cell carcinomas, and in none of the UMB tumors. In summary, analyses of the cell cycle proteins Ki67 and cyclin D1 in Hurthle cell thyroid neoplasms indicate that these markers may assist in distinguishing some Hurthle cell carcinomas from adenomas. Among the Hurthle cell carcinomas, large tumor size and vascular invasion are associated with clinically aggressive tumors. Our study also suggests that Hurthle cell neoplasms with only equivocal capsular invasion and no vascular invasion should behave in a benign manner. (+info)Bilateral renal oncocytoma in a Greyhound dog. (4/183)
A bilateral, locally invasive renal oncocytoma was diagnosed in a 10-year-old spayed female Greyhound dog. The diagnosis was based on positive staining of the tumor with the periodic acid-Schiff reaction prior to diastase treatment, on the immunohistochemical expression of cytoplasmic cytokeratin, and on the prominence of mitochondria in the tumor cells. (+info)VHL alterations in human clear cell renal cell carcinoma: association with advanced tumor stage and a novel hot spot mutation. (5/183)
To elucidate the role of somatic alterations for renal cancer etiology and prognosis, we analyzed 227 sporadic renal epithelial tumors for mutations and hypermethylations in the von Hippel-Lindau tumor suppressor gene VHL. Tumors were classified according to the recommendations of the Union Internationale Contre le Cancer (UICC) and the American Joint Committee on Cancer (AJCC). Somatic VHL mutations were identified by PCR, single-strand conformation polymorphism analysis, and sequencing, and hypermethylations were identified by restriction enzyme digestion and Southern blotting. Frequencies of VHL alterations were established, and an association with tumor type or tumor type and tumor stage was evaluated. VHL mutations and hypermethylations were identified in 45% of clear cell renal cell carcinomas (CCRCCs) and occasionally (3 of 28) in papillary (chromophilic) renal cell carcinomas (RCCs). Lack of VHL mutations and hypermethylations in chromophobe RCCs and oncocytomas was statistically significant (P = 0.0001 and P = 0.0004, respectively). RCCs carrying VHL alterations showed, in nine cases (12%), mutations at a hot spot involving a thymine repeat (ATT.TTT) in exon 2. Tumor staging was critical to the VHL mutation/hypermethylation detection rate in CCRCCs shown by separate evaluation of patients from medical centers in Munich, Heidelberg, and Mainz. The spectrum of pT1, pT2, and pT3 CCRCCs and the VHL mutation/hypermethylation detection rate varied among these three groups. Altogether, VHL alterations were significantly associated with pT3 CCRCCs (P = 0.009). This is the first evidence of frequent somatic VHL mutations at a particular site within exon 2 and an association of VHL mutations/hypermethylations with a standard prognostic factor. (+info)Hurthle cell adenoma diagnosed by core needle biopsy in a male patient. (6/183)
Hurthle cell adenomas (HCAs) are a rare and potentially lethal variant of follicular tumors of the thyroid. Considerable controversy exists regarding potential risk factors, diagnosis, and treatment of HCAs. The authors report the case of a 38-year-old male patient with an 8.3 cm x 3.5 cm HCA. Diagnosis was made preoperatively from a core needle biopsy and confirmed postoperatively on frozen section. Treatment consisted of a right lobectomy. (+info)Immunohistochemical and ultrastructural study of clinically nonfunctioning pituitary adenomas. (7/183)
Sixty-five clinically nonfunctioning pituitary adenomas were studied by immunohistochemistry, and 12 cases were also analyzed by electron microscopy. Thirty-nine cases (60%) were immunohistochemically identified as hormone-producing adenomas. Six adenomas produced multiple hormones. Electron microscopy found seven null cell adenomas and five oncocytomas. The oncocytomas had a significantly higher incidence of hormone expression that the null cell adenomas. These results indicate that clinically nonfunctioning pituitary adenomas produce hormones, even though blood hormone levels are normal or low. Furthermore, the evidence of multihormonal production implies that two or more cell lineages including a protein hormone-producing type and a glycoprotein hormone-producing type may exist in the same nonfunctioning pituitary adenoma. (+info)Bronchial oncocytoma. (8/183)
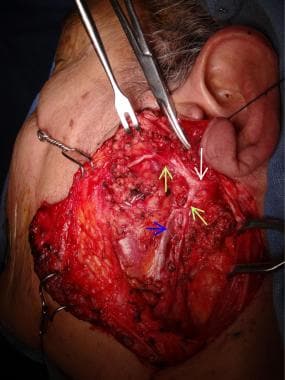
CONTEXT: Oncocytomas are generally small and present slow growth. Finding of the tumor usually occurs incidentally. Their incidence is higher among male patients. Oncocytomas in mucous bronchial glands are extremely rare. CASE REPORT: A 35-year-old male who presented bronchial oncocytoma. The tumor was found after bronchoscopy that investigated an atelectasis of the upper left lobe. Histological examination with optical microscopy revealed a mature neoplasm formed by ovoid cells with thin, granular, eosinophilic cytoplasm and small nuclei similar to oncocytes. Electron microscopy showed mitochondrial hyperplasia. A three-year follow-up after thoracotomy followed by lobectomy and removal of the bronchial tumor was uneventful. (+info)An oxyphilic adenoma is a type of benign tumor that develops in the endocrine glands, specifically in the parathyroid gland. This type of adenoma is characterized by the presence of cells called oxyphils, which have an abundance of mitochondria and appear pink on histological examination due to their high oxidative enzyme activity. Oxyphilic adenomas are a common cause of primary hyperparathyroidism, a condition in which the parathyroid glands produce too much parathyroid hormone (PTH), leading to an imbalance of calcium and phosphorus metabolism. Symptoms of primary hyperparathyroidism may include fatigue, weakness, bone pain, kidney stones, and psychological disturbances. Treatment typically involves surgical removal of the affected parathyroid gland.
An adenoma is a benign (noncancerous) tumor that develops from glandular epithelial cells. These types of cells are responsible for producing and releasing fluids, such as hormones or digestive enzymes, into the surrounding tissues. Adenomas can occur in various organs and glands throughout the body, including the thyroid, pituitary, adrenal, and digestive systems.
Depending on their location, adenomas may cause different symptoms or remain asymptomatic. Some common examples of adenomas include:
1. Colorectal adenoma (also known as a polyp): These growths occur in the lining of the colon or rectum and can develop into colorectal cancer if left untreated. Regular screenings, such as colonoscopies, are essential for early detection and removal of these polyps.
2. Thyroid adenoma: This type of adenoma affects the thyroid gland and may result in an overproduction or underproduction of hormones, leading to conditions like hyperthyroidism (overactive thyroid) or hypothyroidism (underactive thyroid).
3. Pituitary adenoma: These growths occur in the pituitary gland, which is located at the base of the brain and controls various hormonal functions. Depending on their size and location, pituitary adenomas can cause vision problems, headaches, or hormonal imbalances that affect growth, reproduction, and metabolism.
4. Liver adenoma: These rare benign tumors develop in the liver and may not cause any symptoms unless they become large enough to press on surrounding organs or structures. In some cases, liver adenomas can rupture and cause internal bleeding.
5. Adrenal adenoma: These growths occur in the adrenal glands, which are located above the kidneys and produce hormones that regulate stress responses, metabolism, and blood pressure. Most adrenal adenomas are nonfunctioning, meaning they do not secrete excess hormones. However, functioning adrenal adenomas can lead to conditions like Cushing's syndrome or Conn's syndrome, depending on the type of hormone being overproduced.
It is essential to monitor and manage benign tumors like adenomas to prevent potential complications, such as rupture, bleeding, or hormonal imbalances. Treatment options may include surveillance with imaging studies, medication to manage hormonal issues, or surgical removal of the tumor in certain cases.
Oxyphil cells, also known as oncocytes, are large granular cells with abundant mitochondria. They can be found in various organs, including the thyroid gland, parathyroid gland, salivary glands, and skin. In the thyroid gland, oxyphil cells are often observed in the context of follicular adenomas or follicular carcinomas, where they can make up a significant portion of the tumor. The exact function of oxyphil cells is not well understood, but it is thought that they may play a role in the production and metabolism of hormones or other substances. In general, the presence of oxyphil cells in a tumor is not considered to be indicative of a specific type or behavior of the tumor, but rather a histological feature that can be observed in a variety of contexts.
Thyroid neoplasms refer to abnormal growths or tumors in the thyroid gland, which can be benign (non-cancerous) or malignant (cancerous). These growths can vary in size and may cause a noticeable lump or nodule in the neck. Thyroid neoplasms can also affect the function of the thyroid gland, leading to hormonal imbalances and related symptoms. The exact causes of thyroid neoplasms are not fully understood, but risk factors include radiation exposure, family history, and certain genetic conditions. It is important to note that most thyroid nodules are benign, but a proper medical evaluation is necessary to determine the nature of the growth and develop an appropriate treatment plan.
A pleomorphic adenoma is a type of benign (non-cancerous) tumor that typically develops in the salivary glands, although they can also occur in other areas such as the nasopharynx and skin. "Pleomorphic" refers to the diverse appearance of the cells within the tumor, which can vary in size, shape, and arrangement.
Pleomorphic adenomas are composed of a mixture of epithelial and mesenchymal cells, which can form glandular structures, squamous (scale-like) cells, and areas that resemble cartilage or bone. These tumors tend to grow slowly and usually do not spread to other parts of the body.
While pleomorphic adenomas are generally not dangerous, they can cause problems if they become large enough to press on surrounding tissues or structures. In some cases, these tumors may also undergo malignant transformation, leading to a cancerous growth known as carcinoma ex pleomorphic adenoma. Surgical removal is the standard treatment for pleomorphic adenomas, and the prognosis is generally good with proper management.
A villous adenoma is a type of polyp (a growth that protrudes from the lining of an organ) found in the colon or rectum. It is named for its appearance under a microscope, which reveals finger-like projections called "villi" on the surface of the polyp.
Villous adenomas are typically larger than other types of polyps and can be several centimeters in size. They are also more likely to be cancerous or precancerous, meaning that they have the potential to develop into colon or rectal cancer over time.
Because of this increased risk, it is important for villous adenomas to be removed surgically if they are found during a colonoscopy or other diagnostic procedure. Regular follow-up colonoscopies may also be recommended to monitor for the development of new polyps or recurrence of previous ones.
Pituitary neoplasms refer to abnormal growths or tumors in the pituitary gland, a small endocrine gland located at the base of the brain. These neoplasms can be benign (non-cancerous) or malignant (cancerous), with most being benign. They can vary in size and may cause various symptoms depending on their location, size, and hormonal activity.
Pituitary neoplasms can produce and secrete excess hormones, leading to a variety of endocrine disorders such as Cushing's disease (caused by excessive ACTH production), acromegaly (caused by excessive GH production), or prolactinoma (caused by excessive PRL production). They can also cause local compression symptoms due to their size, leading to headaches, vision problems, and cranial nerve palsies.
The exact causes of pituitary neoplasms are not fully understood, but genetic factors, radiation exposure, and certain inherited conditions may increase the risk of developing these tumors. Treatment options for pituitary neoplasms include surgical removal, radiation therapy, and medical management with drugs that can help control hormonal imbalances.
An adrenocortical adenoma is a benign tumor that arises from the cells of the adrenal cortex, which is the outer layer of the adrenal gland. These tumors can produce and release various hormones, such as cortisol, aldosterone, or androgens, depending on the type of cells they originate from.
Most adrenocortical adenomas are nonfunctioning, meaning that they do not secrete excess hormones and may not cause any symptoms. However, some functioning adenomas can produce excessive amounts of hormones, leading to a variety of clinical manifestations. For example:
* Cortisol-secreting adenomas can result in Cushing's syndrome, characterized by weight gain, muscle wasting, thin skin, easy bruising, and mood changes.
* Aldosterone-producing adenomas can cause Conn's syndrome, marked by hypertension (high blood pressure), hypokalemia (low potassium levels), and metabolic alkalosis.
* Androgen-secreting adenomas may lead to hirsutism (excessive hair growth) or virilization (development of male secondary sexual characteristics) in women.
The diagnosis of an adrenocortical adenoma typically involves imaging tests, such as CT or MRI scans, and hormonal evaluations to determine if the tumor is functioning or not. Treatment usually consists of surgical removal of the tumor, especially if it is causing hormonal imbalances or growing in size.
A liver cell adenoma is a benign tumor that develops in the liver and is composed of cells similar to those normally found in the liver (hepatocytes). These tumors are usually solitary, but multiple adenomas can occur, especially in women who have taken oral contraceptives for many years. Liver cell adenomas are typically asymptomatic and are often discovered incidentally during imaging studies performed for other reasons. In rare cases, they may cause symptoms such as abdominal pain or discomfort, or complications such as bleeding or rupture. Treatment options include monitoring with periodic imaging studies or surgical removal of the tumor.
A chromophobe adenoma is a type of benign (non-cancerous) tumor that typically arises in the pituitary gland, which is a small endocrine gland located at the base of the brain. The term "chromophobe" refers to the appearance of the cells under a microscope - they lack pigment and have a characteristic appearance with abundant clear or lightly stained cytoplasm.
Chromophobe adenomas are slow-growing tumors that can vary in size, and they may cause symptoms due to pressure on surrounding structures or by producing excess hormones. The most common hormone produced by chromophobe adenomas is prolactin, leading to symptoms such as menstrual irregularities, milk production (galactorrhea), and decreased sexual function in women, and decreased libido, erectile dysfunction, and infertility in men.
Treatment for chromophobe adenomas typically involves surgical removal of the tumor, often through a transsphenoidal approach (through the nose and sphenoid sinus). In some cases, radiation therapy or medical management with hormone-blocking drugs may also be necessary. Regular follow-up with an endocrinologist is important to monitor for any recurrence or hormonal imbalances.
A Growth Hormone-Secreting Pituitary Adenoma (GH-secreting pituitary adenoma, or GHoma) is a type of benign tumor that develops in the pituitary gland and results in excessive production of growth hormone (GH). This leads to a condition known as acromegaly if it occurs in adults, or gigantism if it occurs in children before the closure of the growth plates.
Symptoms of GH-secreting pituitary adenoma may include:
1. Coarsening of facial features
2. Enlargement of hands and feet
3. Deepened voice due to thickening of vocal cords
4. Increased sweating and body odor
5. Joint pain and stiffness
6. Sleep apnea
7. Fatigue, weakness, or muscle wasting
8. Headaches
9. Vision problems
10. Irregular menstrual periods in women
11. Erectile dysfunction in men
Diagnosis typically involves measuring the levels of GH and insulin-like growth factor 1 (IGF-1) in the blood, along with imaging tests like MRI or CT scans to locate and characterize the tumor. Treatment options include surgical removal of the tumor, radiation therapy, and medication to control GH production. Regular follow-ups are necessary to monitor for potential recurrence.
Colorectal neoplasms refer to abnormal growths in the colon or rectum, which can be benign or malignant. These growths can arise from the inner lining (mucosa) of the colon or rectum and can take various forms such as polyps, adenomas, or carcinomas.
Benign neoplasms, such as hyperplastic polyps and inflammatory polyps, are not cancerous but may need to be removed to prevent the development of malignant tumors. Adenomas, on the other hand, are precancerous lesions that can develop into colorectal cancer if left untreated.
Colorectal cancer is a malignant neoplasm that arises from the uncontrolled growth and division of cells in the colon or rectum. It is one of the most common types of cancer worldwide and can spread to other parts of the body through the bloodstream or lymphatic system.
Regular screening for colorectal neoplasms is recommended for individuals over the age of 50, as early detection and removal of precancerous lesions can significantly reduce the risk of developing colorectal cancer.
Colonic polyps are abnormal growths that protrude from the inner wall of the colon (large intestine). They can vary in size, shape, and number. Most colonic polyps are benign, meaning they are not cancerous. However, some types of polyps, such as adenomas, have a higher risk of becoming cancerous over time if left untreated.
Colonic polyps often do not cause any symptoms, especially if they are small. Larger polyps may lead to symptoms like rectal bleeding, changes in bowel habits, abdominal pain, or iron deficiency anemia. The exact cause of colonic polyps is not known, but factors such as age, family history, and certain medical conditions (like inflammatory bowel disease) can increase the risk of developing them.
Regular screening exams, such as colonoscopies, are recommended for individuals over the age of 50 to detect and remove polyps before they become cancerous. If you have a family history of colonic polyps or colorectal cancer, your doctor may recommend earlier or more frequent screenings.
An ACTH-secreting pituitary adenoma is a type of tumor that develops in the pituitary gland, a small gland located at the base of the brain. This type of tumor is also known as Cushing's disease.
ACTH stands for adrenocorticotropic hormone, which is a hormone produced and released by the pituitary gland. ACTH stimulates the adrenal glands (small glands located on top of the kidneys) to produce cortisol, a steroid hormone that helps regulate metabolism, helps the body respond to stress, and suppresses inflammation.
In an ACTH-secreting pituitary adenoma, the tumor cells produce and release excessive amounts of ACTH, leading to overproduction of cortisol by the adrenal glands. This can result in a constellation of symptoms known as Cushing's syndrome, which may include weight gain (especially around the trunk), fatigue, muscle weakness, mood changes, thinning of the skin, easy bruising, and increased susceptibility to infections.
Treatment for an ACTH-secreting pituitary adenoma typically involves surgical removal of the tumor, followed by medications to manage cortisol levels if necessary. Radiation therapy may also be used in some cases.
An adenoma is a benign tumor that forms in glandular tissue. When referring to "acidophil," it describes the appearance of the cells under a microscope. Acidophils are cells that take up acidic dyes, giving them a distinct appearance. In the context of an adenoma, an acidophil adenoma would be a benign tumor composed of acidophil cells.
Acidophil adenomas are most commonly found in the pituitary gland and are also known as lactotroph or mammosomatotroph adenomas. These tumors can produce and release prolactin, growth hormone, or both, leading to various endocrine disorders such as hyperprolactinemia, acromegaly, or gigantism. Treatment options typically include surgical removal of the tumor or medical management with dopamine agonists or somatostatin analogs.
A colonoscopy is a medical procedure used to examine the large intestine, also known as the colon and rectum. It is performed using a flexible tube with a tiny camera on the end, called a colonoscope, which is inserted into the rectum and gently guided through the entire length of the colon.
The procedure allows doctors to visually inspect the lining of the colon for any abnormalities such as polyps, ulcers, inflammation, or cancer. If any polyps are found during the procedure, they can be removed immediately using special tools passed through the colonoscope. Colonoscopy is an important tool in the prevention and early detection of colorectal cancer, which is one of the leading causes of cancer-related deaths worldwide.
Patients are usually given a sedative to help them relax during the procedure, which is typically performed on an outpatient basis in a hospital or clinic setting. The entire procedure usually takes about 30-60 minutes to complete, although patients should plan to spend several hours at the medical facility for preparation and recovery.
Adenomatous polyps, also known as adenomas, are benign (noncancerous) growths that develop in the lining of the glandular tissue of certain organs, most commonly occurring in the colon and rectum. These polyps are composed of abnormal glandular cells that can grow excessively and form a mass.
Adenomatous polyps can vary in size, ranging from a few millimeters to several centimeters in diameter. They may be flat or have a stalk (pedunculated). While adenomas are generally benign, they can potentially undergo malignant transformation and develop into colorectal cancer over time if left untreated. The risk of malignancy increases with the size of the polyp and the presence of certain histological features, such as dysplasia (abnormal cell growth).
Regular screening for adenomatous polyps is essential to detect and remove them early, reducing the risk of colorectal cancer. Screening methods include colonoscopy, sigmoidoscopy, and stool-based tests.
A prolactinoma is a type of pituitary tumor that produces an excess amount of the hormone prolactin, leading to various symptoms. The pituitary gland, located at the base of the brain, is responsible for producing and releasing several hormones that regulate different bodily functions. Prolactin is one such hormone, primarily known for its role in stimulating milk production in women during lactation (breastfeeding).
Prolactinoma tumors can be classified into two types: microprolactinomas and macroprolactinomas. Microprolactinomas are smaller tumors, typically less than 10 millimeters in size, while macroprolactinomas are larger tumors, generally greater than 10 millimeters in size.
The overproduction of prolactin caused by these tumors can lead to several clinical manifestations, including:
1. Galactorrhea: Unusual and often spontaneous milk production or leakage from the nipples, which can occur in both men and women who do not have a recent history of pregnancy or breastfeeding.
2. Menstrual irregularities: In women, high prolactin levels can interfere with the normal functioning of other hormones, leading to menstrual irregularities such as infrequent periods (oligomenorrhea) or absent periods (amenorrhea), and sometimes infertility.
3. Sexual dysfunction: In both men and women, high prolactin levels can cause decreased libido and sexual desire. Men may also experience erectile dysfunction and reduced sperm production.
4. Bone loss: Over time, high prolactin levels can lead to decreased bone density and an increased risk of osteoporosis due to the disruption of other hormones that regulate bone health.
5. Headaches and visual disturbances: As the tumor grows, it may put pressure on surrounding structures in the brain, leading to headaches and potential vision problems such as blurred vision or decreased peripheral vision.
Diagnosis typically involves measuring prolactin levels in the blood and performing imaging tests like an MRI (magnetic resonance imaging) scan to assess the size of the tumor. Treatment usually consists of medication to lower prolactin levels, such as dopamine agonists (e.g., bromocriptine or cabergoline), which can also help shrink the tumor. In some cases, surgery may be necessary if medication is ineffective or if the tumor is large and causing severe symptoms.
A basophilic adenoma is a rare type of benign tumor that arises from the glandular cells of an endocrine gland, specifically the cells that produce and store hormones. The term "basophilic" refers to the appearance of the tumor cells under a microscope, which have a high affinity for basic dyes due to their rich content of ribonucleic acid (RNA).
Basophilic adenomas are most commonly found in the pituitary gland, a small endocrine gland located at the base of the brain. These tumors can produce and secrete excessive amounts of hormones, leading to various clinical symptoms depending on the type of hormone involved. The most common types of basophilic adenomas are prolactinomas, which secrete high levels of the hormone prolactin, and growth hormone-secreting adenomas, which produce excessive amounts of growth hormone.
Treatment for basophilic adenomas typically involves surgical removal of the tumor, followed by radiation therapy or medical management with drugs that suppress hormone production. The prognosis for patients with basophilic adenomas is generally good, with most individuals experiencing a significant improvement in symptoms and quality of life following treatment. However, regular follow-up care is necessary to monitor for recurrence and manage any residual hormonal imbalances.
Adrenal cortex neoplasms refer to abnormal growths (tumors) in the adrenal gland's outer layer, known as the adrenal cortex. These neoplasms can be benign or malignant (cancerous). Benign tumors are called adrenal adenomas, while cancerous tumors are called adrenocortical carcinomas.
Adrenal cortex neoplasms can produce various hormones, leading to different clinical presentations. For instance, they may cause Cushing's syndrome (characterized by excessive cortisol production), Conn's syndrome (caused by aldosterone excess), or virilization (due to androgen excess). Some tumors may not produce any hormones and are discovered incidentally during imaging studies for unrelated conditions.
The diagnosis of adrenal cortex neoplasms typically involves a combination of imaging techniques, such as CT or MRI scans, and hormonal assessments to determine if the tumor is functional or non-functional. In some cases, a biopsy may be necessary to confirm the diagnosis and differentiate between benign and malignant tumors. Treatment options depend on the type, size, location, and hormonal activity of the neoplasm and may include surgical excision, radiation therapy, chemotherapy, or a combination of these approaches.
Adenomatous Polyposis Coli (APC) is a genetic disorder characterized by the development of numerous adenomatous polyps in the colon and rectum. APC is caused by mutations in the APC gene, which is a tumor suppressor gene that helps regulate cell growth and division. When the APC gene is mutated, it can lead to uncontrolled cell growth and the development of polyps, which can eventually become cancerous.
Individuals with APC typically develop hundreds to thousands of polyps in their colon and rectum, usually beginning in adolescence or early adulthood. If left untreated, APC can lead to colorectal cancer in nearly all affected individuals by the age of 40.
APC is an autosomal dominant disorder, which means that a person has a 50% chance of inheriting the mutated gene from an affected parent. However, some cases of APC may also occur spontaneously due to new mutations in the APC gene. Treatment for APC typically involves surgical removal of the colon and rectum (colectomy) to prevent the development of colorectal cancer. Regular surveillance with colonoscopy is also recommended to monitor for the development of new polyps.
 Chief cell
Chief cell
Oncocytoma
Oncocyte
International Classification of Diseases for Oncology
Hürthle cell
List of MeSH codes (C04)
Papillary hidradenoma
Chief cell - Wikipedia
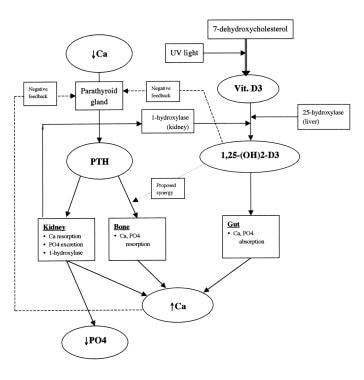
 Parathyroid Physiology: Calcium Homeostasis, Disorders of Parathyroid Hormone Metabolism, Pathophysiology
Parathyroid Physiology: Calcium Homeostasis, Disorders of Parathyroid Hormone Metabolism, Pathophysiology
 Eileen White - Research output
- Rutgers, The State University of New Jersey
Eileen White - Research output
- Rutgers, The State University of New Jersey
Code System Concept
HuGE Navigator|Genopedia|PHGKB
Bio2Vec
 Neoplasm staging. Medical search. Definitions
Neoplasm staging. Medical search. Definitions
 Division of Oncology - Research output
- Research Profiles at Washington University School of Medicine
Division of Oncology - Research output
- Research Profiles at Washington University School of Medicine
Medical Laboratory, Imaging and Radiologic Sciences<...
Schober, J. P.<...
College of Allied Health Sciences - Scholarly Output - Augusta University Research Profiles
Clayton K Trimmer - Research output - University of Texas Southwestern Medical Center
 Department of Pathology & Genomic Medicine - Research output
- Houston Methodist Scholars
Department of Pathology & Genomic Medicine - Research output
- Houston Methodist Scholars
Assessment of multiphasic contrast-enhanced mr textures in differentiating small renal mass subtypes<...
Imaging features of renal cell carcinoma differential diagnosis, staging, and posttreatment evaluation<...
Low-Grade Oncocytic Tumor of Kidney (CK7-Positive, CD117-Negative): Incidence in a single institutional experience with...
Differentiating papillary type I RCC from clear cell RCC and oncocytoma: application of whole-lesion volumetric ADC measurement...
 Adenoma
- Adenomas
Summary Report | CureHunter
Adenoma
- Adenomas
Summary Report | CureHunter
Making a knife from old and rusty wrench
 Pesquisa | Prevenção e Controle de Câncer
Pesquisa | Prevenção e Controle de Câncer
Hurthle Cell Carcinoma (Oncocytic Carcinoma): Practice Essentials, Pathophysiology, Etiology
ACTH-Secreting Pituitary Adenoma | Profiles RNS
Neoplasm metastasis - radiotherapy
 DeCS 2012 - February 22, 2012 version
DeCS 2012 - February 22, 2012 version
DeCS 2009 - February 20, 2009 version
DeCS 2013 - December 17, 2013 version
DeCS 2011 - December 22, 2011 version
Carcinoma5
- Approximately 85% of cases are found to be caused by an isolated parathyroid adenoma, 15% by diffuse parathyroid hyperplasia, and less than 1% by parathyroid carcinoma. (medscape.com)
- therefore, definitive differentiation of Hürthle cell carcinoma from Hürthle-cell adenoma is based on vascular invasion and/or capsular invasion, as well as on permanent histologic sections or extrathyroidal tumor spread and lymph node and systemic metastases. (medscape.com)
- Case report: ACTH-secreting pituitary carcinoma metastatic to the liver in a patient with a history of atypical pituitary adenoma and Cushing's disease. (uams.edu)
- We touched on the issue that follicular carcinoma cannot be distinguished from follicular adenoma by aspiration, and so if that quandary remains, in general I will recommend surgery to the patient. (cancerstreatment.com)
- According to the World Health Organization (WHO), these neoplasms are considered a variant of follicular carcinoma of the thyroid and are referred to as follicular carcinoma, oxyphilic type. (medscape.com)
Neoplasms1
- But occasionally one will see neoplasms which consist predominantly of oxyphilic cells with sort of a granular cytoplasm and this defines the Hurthle cell variant . (cancerstreatment.com)
Oncocytoma1
- Oxyphilic adenoma (oncocytoma) Oxyphilic adenoma (oncocytoma) was first described by Duplay in 1875. (stubensaenger.de)
Pleomorphic adenoma1
- Oct 19, 2022 Warthin tumors are the 2 nd most common benign parotid tumor (after pleomorphic adenoma) and represent up to 10 of all parotid tumors. (stubensaenger.de)
Tumor1
- [ 4 ] in a series of 23 patients, the mean tumor size was significantly greater for carcinomas than adenomas (3.1 cm vs 1.9 cm). (medscape.com)
Pituitary5
- ACTH-Secreting Pituitary Adenoma" is a descriptor in the National Library of Medicine's controlled vocabulary thesaurus, MeSH (Medical Subject Headings) . (uams.edu)
- A pituitary adenoma which secretes ADRENOCORTICOTROPIN, leading to CUSHING DISEASE. (uams.edu)
- This graph shows the total number of publications written about "ACTH-Secreting Pituitary Adenoma" by people in UAMS Profiles by year, and whether "ACTH-Secreting Pituitary Adenoma" was a major or minor topic of these publications. (uams.edu)
- Below are the most recent publications written about "ACTH-Secreting Pituitary Adenoma" by people in Profiles over the past ten years. (uams.edu)
- Orbital invasion by ACTH-secreting pituitary adenomas. (uams.edu)
Cancer1
- Thyroid nodules called adenomas are not cancer (benign). (cancercouncil.com.au)
Chief cell parathyroid1
- 1. Molecular profiles of oxyphilic and chief cell parathyroid adenoma. (nih.gov)
Follicular adenoma1
- A subtype of follicular adenoma in the THYROID GLAND. (bvsalud.org)
Descriptor1
- Adenoma, Islet Cell" is a descriptor in the National Library of Medicine's controlled vocabulary thesaurus, MeSH (Medical Subject Headings) . (uams.edu)
Mutations2
Histology1
- 16. Parathyroid function and histology in patients with parathyroid adenoma: correlation of clinical and morphologic findings. (nih.gov)
Profiles3
- 11. Gene expression profiles in parathyroid adenoma and normal parathyroid tissue. (nih.gov)
- This graph shows the total number of publications written about "Adenoma, Islet Cell" by people in UAMS Profiles by year, and whether "Adenoma, Islet Cell" was a major or minor topic of these publications. (uams.edu)
- Below are the most recent publications written about "Adenoma, Islet Cell" by people in Profiles over the past ten years. (uams.edu)
Cell2
- 8. Oxyphilic cell adenoma of parathyroid resulting in primary hyperparathyroidism and osteitis fibrosa cystica--a case report. (nih.gov)
- 13. Preoperative localization of parathyroid adenomas with technetium-99m methoxyisobutylisonitrile imaging: relationship with P-glycoprotein expression, oxyphilic cell content, and tumoral tissue volume. (nih.gov)
Specific1
- A specific type of acidophil adenoma may give rise to nonpuerperal galactorrhea. (nih.gov)
Type1
- 5. Increased protein kinase A type Iα regulatory subunit expression in parathyroid gland adenomas of patients with primary hyperparathyroidism. (nih.gov)