Adenomatoid Tumor
Neoplasms, Mesothelial
Cystic Adenomatoid Malformation of Lung, Congenital
Adenomatoid tumor of the pancreas: a case report with comparison of histology and aspiration cytology. (1/15)
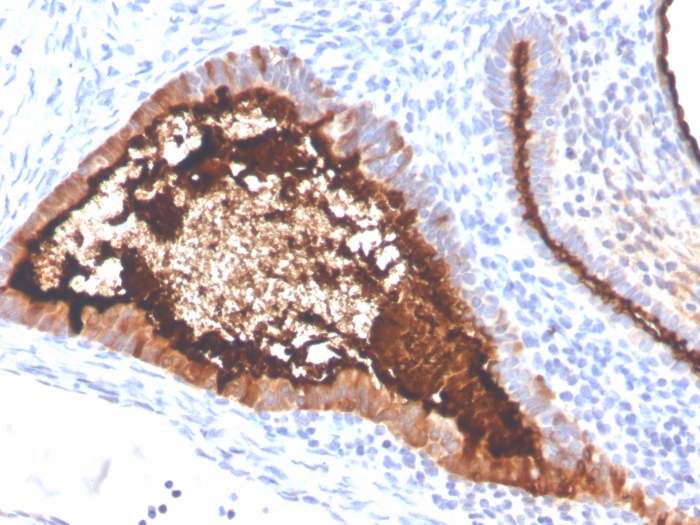
We present a 58-year-old woman who presented with a 1.5-cm, hypodense lesion in the head of the pancreas. Endoscopic ultrasound-guided fine-needle aspiration yielded bland, monotonous cells with wispy cytoplasm, slightly granular chromatin, and small nucleoli. A presumptive diagnosis of a neuroendocrine lesion was rendered. Whipple procedure yielded a well-circumscribed, encapsulated lesion with dense, hyalinized stroma and a peripheral rim of lymphocytes. Spindled and epithelioid cells formed short tubules, cords, and nests. The neoplasm stained for CK 5/6, calretinin, vimentin, CD 99, pancytokeratin, and EMA, consistent with mesothelial origin. This characteristic histology and immunohistochemistry is consistent with an adenomatoid tumor. We believe we are the first to report this benign neoplasm in such an unusual location. Herein we address the diagnosis of adenomatoid tumor by histology, immunohistochemistry, and aspiration cytology. Our case is particularly unique in that the histology and cytology are compared and correlated. (+info)Uncommon benign intrascrotal tumours. (2/15)
INTRODUCTION: Benign intrascrotal tumours are rare. CLINICAL PICTURE: Three patients with bilateral paratesticular leiomyomas, an adenomatoid tumour of the testis and a left paratesticular dermoid cyst coexisting with a synchronous left paratesticular epidermal cyst are presented. These tumours were discrete, hard and smooth lesions, in which the diagnosis of malignancy could not be safely excluded preoperatively even with ultrasonography. TREATMENT AND OUTCOME: The first patient had orchiectomy with contralateral testicular preserving surgery, the second patient underwent orchiectomy and the third had conservative testicular surgery. CONCLUSION: Awareness of these benign tumours may allow for testicular preservation. (+info)Selected other problematic testicular and paratesticular lesions: rete testis neoplasms and pseudotumors, mesothelial lesions and secondary tumors. (3/15)
The proximity and, in some instances, communication between several structures in the testis and paratestis (rete testis, epididymis, mesothelium, vestigial epithelium and paratesticular soft tissue) result in a plethora of interesting tumors and tumor-like lesions that together pose a formidable diagnostic challenge both because of their morphologic overlap and rarity. The occasional spread of tumors primarily at other sites to this region adds to the potential problem encountered. This review provides an overview of the pathology of nonmesenchymal paratesticular neoplasms and pseudotumors with a focus on the approach to tubulopapillary neoplasms for which diagnostic considerations may include carcinoma of the rete testis, malignant mesothelioma, ovarian-type epithelial tumors, epididymal carcinoma and metastatic carcinomas. The cornerstone of accurate characterization of these lesions is still a comprehensive, traditional clinicopathologic approach, clinical history (of another primary), gross examination (location) and routine light microscopy, but judicious incorporation of contemporary immunohistochemical markers may aid or in some instances be crucial in resolving the problems encountered. (+info)Adenomatoid tumor of supra-renal gland. (4/15)
Adenomatoid tumors of adrenal gland are rare, asymptomatic neoplasias, with benign behavior, and usually are diagnosed incidentally. We report a case of a voluminous adenomatoid tumor of left adrenal gland in a 42-year old man who sought evaluation because of renal colic due to left nephrolithiasis. During the investigation, a tumor localized in left adrenal gland was identified by ultrasonography (14.3 x 10.5 x 19.0). The patient underwent adrenalectomy and pyelolithotomy with histopathological and immunohistochemical diagnosis of adenomatoid tumor of adrenal gland, being the largest one described in the literature to the moment. The patient does not present any signs of recurring lesion after a 3-year follow-up. (+info)Adenomatoid odontogenic tumor of the mandible: review of the literature and report of a rare case. (5/15)
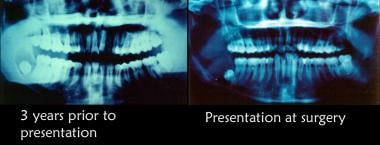
Adenomatoid odontogenic tumor (AOT) is a rare odontogenic tumor which is often misdiagnosed as odontogenic cyst. To acquire additional information about AOT, all reports regarding AOT and cited in "pubmed" since 1990 onward were reviewed. AOT accounts for about 1% until 9% of all odontogenic tumors. It is predominantly found in young and female patients, located more often in the maxilla in most cases associated with an uneruppted permanent tooth. For radiological diagnose the intraoral periapical radiograph seems to be more useful than panoramic. However, AOT frequently resemble other odontogenic lesions such as dentigerous cysts or ameloblastoma. Immunohistochemically AOT is characterized by positive reactions with certain cytokeratins. Treatment is conservative and the prognosis is excellent. For illustration a rare case of an AOT in the mandible is presented. (+info)Respiratory epithelial adenomatoid hamartoma of the maxillary sinus: case report. (6/15)
The case is described of a male patient with respiratory epithelial adenomatoid hamartoma of the left maxillary sinus that initially presented as a chronic sinus inflammation. This benign lesion is characterized by glandular proliferation originating from the surface of the respiratory epithelium. Maxillary sinus localisation is very rare but is very important to be able to distinguish hamartomas from schneiderian papillomas of the inverted type and adenocarcinomas, potentially requiring aggressive surgical treatment. Moreover, misinterpretation of the respiratory epithelial adenomatoid hamartoma as chronic sinus inflammation may result in inadequate treatment. The clinical and pathological features of this lesion are discussed. (+info)Adenomatoid tumour of the liver. (7/15)
(+info)Myocardial adenomatoid tumor in eight cattle: evidence for mesothelial origin of bovine myocardial epithelial inclusions. (8/15)
(+info)An adenomatoid tumor is a benign (non-cancerous) neoplasm that typically arises in the serosal surfaces of the reproductive organs, such as the epididymis in men and the fallopian tube or uterus in women. These tumors are composed of epithelioid cells arranged in tubules, glands, or cysts, and they can sometimes be mistaken for malignant tumors due to their gross appearance. However, adenomatoid tumors are generally slow-growing and do not spread to other parts of the body. They are usually treated with surgical excision and have an excellent prognosis.
Neoplasms, mesothelial are a type of tumor that develops from the mesothelial cells which form the lining of various body cavities such as the pleura (lungs), peritoneum (abdomen), and pericardium (heart). These tumors can be benign or malignant, with malignant mesotheliomas being associated with exposure to asbestos. Symptoms may include chest pain, cough, and difficulty breathing, depending on the location of the tumor. Treatment options include surgery, radiation therapy, and chemotherapy.
Genital neoplasms in males refer to abnormal growths or tumors that develop in the male reproductive organs. These can be benign (non-cancerous) or malignant (cancerous).
Malignant genital neoplasms are often referred to as genital cancers. The most common types of male genital cancers include:
1. Penile Cancer: This occurs when cancer cells form in the tissues of the penis.
2. Testicular Cancer: This forms in the testicles (testes), which are located inside the scrotum.
3. Prostate Cancer: This is a common cancer in men, forming in the prostate gland, which is part of the male reproductive system that helps make semen.
4. Scrotal Cancer: This is a rare form of cancer that forms in the skin or tissue of the scrotum.
5. Penile Intraepithelial Neoplasia (PeIN): This is not cancer, but it is considered a pre-cancerous condition of the penis.
Early detection and treatment of genital neoplasms can significantly improve the prognosis. Regular self-examinations and medical check-ups are recommended, especially for individuals with risk factors such as smoking, HIV infection, or a family history of these cancers.
Congenital Cystic Adenomatoid Malformation (CCAM) of the lung is a rare developmental anomaly of the lungs that affects the terminal ends of the bronchus. It is characterized by the presence of abnormal masses or nodules filled with mucus or air-filled cysts in the lung tissue. These malformations are typically present at birth but may not cause any symptoms until later in life, if at all.
CCAMs are classified into three types based on their size, location, and the number of cysts present. Type I CCAMs have one or more large cysts (greater than 2 cm in diameter), type II CCAMs have multiple small cysts (less than 1 cm in diameter), and type III CCAMs are solid masses without any visible cysts.
CCAMs can cause a range of symptoms, including respiratory distress, coughing, wheezing, recurrent lung infections, and difficulty gaining weight. In severe cases, they may lead to heart failure or fetal hydrops (a condition characterized by fluid accumulation in the fetus).
The diagnosis of CCAMs is typically made through prenatal ultrasound or imaging studies such as CT scans or MRIs after birth. Treatment usually involves surgical removal of the affected lung tissue, which can be done safely with minimal risk to the child's health and development.
Genital neoplasms in females refer to abnormal growths or tumors that occur in the female reproductive organs. These can be benign (non-cancerous) or malignant (cancerous). The most common types of female genital neoplasms are:
1. Cervical cancer: This is a malignancy that arises from the cells lining the cervix, usually caused by human papillomavirus (HPV) infection.
2. Uterine cancer: Also known as endometrial cancer, this type of female genital neoplasm originates in the lining of the uterus (endometrium).
3. Ovarian cancer: This is a malignancy that develops from the cells in the ovaries, which can be difficult to detect at an early stage due to its location and lack of symptoms.
4. Vulvar cancer: A rare type of female genital neoplasm that affects the external female genital area (vulva).
5. Vaginal cancer: This is a malignancy that occurs in the vagina, often caused by HPV infection.
6. Gestational trophoblastic neoplasia: A rare group of tumors that develop from placental tissue and can occur during or after pregnancy.
Regular screening and early detection are crucial for successful treatment and management of female genital neoplasms.
Odontogenic tumors are a group of neoplasms that originate from the dental tissues or their remnants, including the odontogenic epithelium, ectomesenchyme, and/or their derivatives. These tumors can be benign or malignant and may affect the jaw bones and surrounding structures. They can cause various symptoms, such as swelling, pain, loosening of teeth, and altered bite. The classification of odontogenic tumors includes a wide range of entities with different biological behaviors, clinical features, and treatment approaches. Accurate diagnosis is essential for proper management and prognosis.