Audiometry
Audiometry, Pure-Tone
Cochlear Diseases
Hearing Loss, Noise-Induced
Hearing
Evoked Potentials, Auditory, Brain Stem
Melopsittacus
Cochlea
Hearing Loss
Differential Threshold
Sensory perception: supernormal hearing in the blind? (1/1506)
A recent experimental study suggests that blind individuals may compensate for their lack of vision with better-than-normal hearing. This provides support for a view dating back to 18th century philosophers, but the data raise as many problems as they solve. (+info)Gene disruption of p27(Kip1) allows cell proliferation in the postnatal and adult organ of corti. (2/1506)
Hearing loss is most often the result of hair-cell degeneration due to genetic abnormalities or ototoxic and traumatic insults. In the postembryonic and adult mammalian auditory sensory epithelium, the organ of Corti, no hair-cell regeneration has ever been observed. However, nonmammalian hair-cell epithelia are capable of regenerating sensory hair cells as a consequence of nonsensory supporting-cell proliferation. The supporting cells of the organ of Corti are highly specialized, terminally differentiated cell types that apparently are incapable of proliferation. At the molecular level terminally differentiated cells have been shown to express high levels of cell-cycle inhibitors, in particular, cyclin-dependent kinase inhibitors [Parker, S. B., et al. (1995) Science 267, 1024-1027], which are thought to be responsible for preventing these cells from reentering the cell cycle. Here we report that the cyclin-dependent kinase inhibitor p27(Kip1) is selectively expressed in the supporting-cell population of the organ of Corti. Effects of p27(Kip1)-gene disruption include ongoing cell proliferation in postnatal and adult mouse organ of Corti at time points well after mitosis normally has ceased during embryonic development. This suggests that release from p27(Kip1)-induced cell-cycle arrest is sufficient to allow supporting-cell proliferation to occur. This finding may provide an important pathway for inducing hair-cell regeneration in the mammalian hearing organ. (+info)Assessment of hearing in 80 inbred strains of mice by ABR threshold analyses. (3/1506)
The common occurrence of hearing loss in both humans and mice, and the anatomical and functional similarities of their inner ears, attest to the potential of mice being used as models to study inherited hearing loss. A large-scale, auditory screening project is being undertaken at The Jackson Laboratory (TJL) to identify mice with inherited hearing disorders. To assess hearing sensitivity, at least five mice from each inbred strain had auditory brainstem response (ABR) thresholds determined. Thus far, we have screened 80 inbred strains of mice; 60 of them exhibited homogeneous ABR threshold values not significantly different from those of the control strain CBA/CaJ. This large database establishes a reliable reference for normal hearing mouse strains. The following 16 inbred strains exhibited significantly elevated ABR thresholds before the age of 3 months: 129/J, 129/ReJ, 129/SvJ, A/J, ALR/LtJ, ALS/LtJ, BUB/BnJ, C57BLKS/J, C57BR/cdJ, C57L/J, DBA/2J, I/LnJ, MA/MyJ, NOD/LtJ, NOR/LtJ, and SKH2/J. These hearing impaired strains may serve as models for some forms of human non-syndromic hearing loss and aid in the identification of the underlying genes. (+info)Inner ear damage in guinea pigs exposed to stable and impulse noise. (4/1506)
OBJECTIVE: To investigate the inner ear damage after exposure to stable noise, impulse noise and stable plus impulse noise in guinea pigs. METHODS: Ninety-six healthy guinea pigs were divided into 3 equal groups. (1) Stable noise group: exposed to 110 dBA stable noise for 3 days, 4 hours per day. (2) Impulse noise group: exposed to 165 dBA simulated cannon fire impulse noise 10 times successively at an interval of 10 seconds. (3) stable plus impulse noise group: exposed to the same stable noise as that in the first group, then after a 2-hour rest, the animals were followed with impulse noise exposures as that in the second group. After those exposure, each of the 3 groups was further divided into 4 subgroups according to the time after the noise exposure, namely, the right after, 7 d, 14 d and 30 d groups. The evoked cortical potential responses to click and tone burst stimulation sound were examined. The surface preparation and celloidine embedded serial section of the cochlea were observed under a light microscope. RESULTS: Both the stable and impulse noise could increase the hearing threshold and damage the inner ear hair cells. The damage in the first group was relatively slight, whereas in group 3 the damage was more severe than that in the other 2 groups. CONCLUSION: For seamen who are working in heavy noise environment, corresponding measures should be taken to protect their ears from noise which induces hearing loss. (+info)Single-unit responses in the inferior colliculus of decerebrate cats. I. Classification based on frequency response maps. (5/1506)
This study proposes a classification system for neurons in the central nucleus of the inferior colliculus (ICC) that is based on excitation and inhibition patterns of single-unit responses in decerebrate cats. The decerebrate preparation allowed extensive characterization of physiological response types without the confounding effects of anesthesia. The tone-driven discharge rates of individual units were measured across a range of frequencies and levels to map excitatory and inhibitory response areas for contralateral monaural stimulation. The resulting frequency response maps can be grouped into the following three populations: type V maps exhibit a wide V-shaped excitatory area and no inhibition; type I maps show a more restricted I-shaped region of excitation that is flanked by inhibition at lower and higher frequencies; and type O maps display an O-shaped island of excitation at low stimulus levels that is bounded by inhibition at higher levels. Units that produce a type V map typically have a low best frequency (BF: the most sensitive frequency), a low rate of spontaneous activity, and monotonic rate-level functions for both BF tones and broadband noise. Type I and type O units have BFs that span the cat's range of audible frequencies and high rates of spontaneous activity. Like type V units, type I units are excited by BF tones and noise at all levels, but their rate-level functions may become nonmonotonic at high levels. Type O units are inhibited by BF tones and noise at high levels. The existence of distinct response types is consistent with a conceptual model in which the unit types receive dominant inputs from different sources and shows that these functionally segregated pathways are specialized to play complementary roles in the processing of auditory information. (+info)Single-unit responses in the inferior colliculus of decerebrate cats. II. Sensitivity to interaural level differences. (6/1506)
Single units in the central nucleus of the inferior colliculus (ICC) of unanesthetized decerebrate cats can be grouped into three distinct types (V, I, and O) according to the patterns of excitation and inhibition revealed in contralateral frequency response maps. This study extends the description of these response types by assessing their ipsilateral and binaural response map properties. Here the nature of ipsilateral inputs is evaluated directly using frequency response maps and compared with results obtained from methods that rely on sensitivity to interaural level differences (ILDs). In general, there is a one-to-one correspondence between observed ipsilateral input characteristics and those inferred from ILD manipulations. Type V units receive ipsilateral excitation and show binaural facilitation (EE properties); type I and type O units receive ipsilateral inhibition and show binaural excitatory/inhibitory (EI) interactions. Analyses of binaural frequency response maps show that these ILD effects extend over the entire receptive field of ICC units. Thus the range of frequencies that elicits excitation from type V units is expanded with increasing levels of ipsilateral stimulation, whereas the excitatory bandwidth of type I and O units decreases under the same binaural conditions. For the majority of ICC units, application of bicuculline, an antagonist for GABAA-mediated inhibition, does not alter the basic effects of binaural stimulation; rather, it primarily increases spontaneous and maximum discharge rates. These results support our previous interpretations of the putative dominant inputs to ICC response types and have important implications for midbrain processing of competing free-field sounds that reach the listener with different directional signatures. (+info)A problem with auditory processing? (7/1506)
Recent studies have found associations between auditory processing deficits and language disorders such as dyslexia; but whether the former cause the latter, or simply co-occur with them, is still an open question. (+info)Frequency selective effects of alcohol on auditory detection and frequency discrimination thresholds. (8/1506)
In the first of two experiments, the effects of ethyl alcohol on monaural and binaural thresholds for pure tones were measured for a range of frequencies. The results showed a frequency-specific effect in which low frequencies were more severely affected than higher ones. Also, monaural thresholds tended to be more affected by alcohol than binaural ones. The second experiment extended this exploration by measuring frequency discrimination at several different frequencies. In this case, we also obtained a frequency-dependent effect: the increase in discrimination thresholds above 1000 Hz was three times greater than that for lower frequencies. The data suggest that the choice of stimuli may influence the ability to detect changes in auditory performance after alcohol and may account in part for the differences among earlier studies. The results are consistent with the hypothesis that alcohol is acting centrally, at the level of mechanisms involved in the temporal and binaural summation of auditory signals, rather than influencing peripheral structures. (+info)The auditory threshold is the minimum sound intensity or loudness level that a person can detect 50% of the time, for a given tone frequency. It is typically measured in decibels (dB) and represents the quietest sound that a person can hear. The auditory threshold can be affected by various factors such as age, exposure to noise, and certain medical conditions. Hearing tests, such as pure-tone audiometry, are used to measure an individual's auditory thresholds for different frequencies.
Audiometry is the testing of a person's ability to hear different sounds, pitches, or frequencies. It is typically conducted using an audiometer, a device that emits tones at varying volumes and frequencies. The person being tested wears headphones and indicates when they can hear the tone by pressing a button or raising their hand.
There are two main types of audiometry: pure-tone audiometry and speech audiometry. Pure-tone audiometry measures a person's ability to hear different frequencies at varying volumes, while speech audiometry measures a person's ability to understand spoken words at different volumes and in the presence of background noise.
The results of an audiometry test are typically plotted on an audiogram, which shows the quietest sounds that a person can hear at different frequencies. This information can be used to diagnose hearing loss, determine its cause, and develop a treatment plan.
Pure-tone audiometry is a hearing test that measures a person's ability to hear different sounds, pitches, or frequencies. During the test, pure tones are presented to the patient through headphones or ear inserts, and the patient is asked to indicate each time they hear the sound by raising their hand, pressing a button, or responding verbally.
The softest sound that the person can hear at each frequency is recorded as the hearing threshold, and a graph called an audiogram is created to show the results. The audiogram provides information about the type and degree of hearing loss in each ear. Pure-tone audiometry is a standard hearing test used to diagnose and monitor hearing disorders.
Cochlear diseases refer to conditions that affect the structure or function of the cochlea, which is a part of the inner ear responsible for hearing. These diseases can cause various types and degrees of hearing loss, ranging from mild to profound. Some common cochlear diseases include:
1. Cochlear otosclerosis: A condition where there is abnormal bone growth in the cochlea, which can lead to conductive or sensorineural hearing loss.
2. Cochlear Meniere's disease: A disorder that affects the inner ear and causes vertigo, tinnitus, and fluctuating hearing loss.
3. Cochlear damage due to exposure to loud noises: Prolonged or sudden exposure to loud noises can cause permanent cochlear damage and hearing loss.
4. Presbycusis: Age-related hearing loss that affects the cochlea and other structures of the auditory system.
5. Cochlear nerve tumors: Rare benign or malignant growths on the cochlear nerve can cause hearing loss, tinnitus, and balance problems.
6. Infections: Bacterial or viral infections such as meningitis, labyrinthitis, or otitis media can damage the cochlea and lead to hearing loss.
7. Ototoxicity: Certain medications can be toxic to the cochlea and cause hearing loss, tinnitus, or balance problems.
8. Genetic factors: Inherited genetic mutations can cause various types of cochlear diseases, such as connexin 26 deficiency, Waardenburg syndrome, or Usher syndrome.
It is important to note that early diagnosis and treatment of cochlear diseases can help prevent or minimize hearing loss and other complications.
Noise-induced hearing loss (NIHL) is a type of sensorineural hearing loss that occurs due to exposure to harmful levels of noise. The damage can be caused by a one-time exposure to an extremely loud sound or by continuous exposure to lower level sounds over time. NIHL can affect people of all ages and can cause permanent damage to the hair cells in the cochlea, leading to hearing loss, tinnitus (ringing in the ears), and difficulty understanding speech in noisy environments. Prevention measures include avoiding excessive noise exposure, wearing hearing protection, and taking regular breaks from noisy activities.
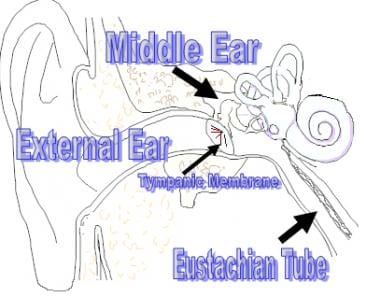
Hearing is the ability to perceive sounds by detecting vibrations in the air or other mediums and translating them into nerve impulses that are sent to the brain for interpretation. In medical terms, hearing is defined as the sense of sound perception, which is mediated by the ear and interpreted by the brain. It involves a complex series of processes, including the conduction of sound waves through the outer ear to the eardrum, the vibration of the middle ear bones, and the movement of fluid in the inner ear, which stimulates hair cells to send electrical signals to the auditory nerve and ultimately to the brain. Hearing allows us to communicate with others, appreciate music and sounds, and detect danger or important events in our environment.
Auditory brainstem evoked potentials (ABEPs or BAEPs) are medical tests that measure the electrical activity in the auditory pathway of the brain in response to sound stimulation. The test involves placing electrodes on the scalp and recording the tiny electrical signals generated by the nerve cells in the brainstem as they respond to clicks or tone bursts presented through earphones.
The resulting waveform is analyzed for latency (the time it takes for the signal to travel from the ear to the brain) and amplitude (the strength of the signal). Abnormalities in the waveform can indicate damage to the auditory nerve or brainstem, and are often used in the diagnosis of various neurological conditions such as multiple sclerosis, acoustic neuroma, and brainstem tumors.
The test is non-invasive, painless, and takes only a few minutes to perform. It provides valuable information about the functioning of the auditory pathway and can help guide treatment decisions for patients with hearing or balance disorders.
"Melopsittacus" is the genus name for the species of bird commonly known as the Budgerigar or Parakeet. It is the only species in its genus and belongs to the Psittacidae family, which includes parrots. The Melopsittacus undulatus is a small, long-tailed parrot native to Australia, known for its bright green, yellow, or blue feathers and sociable behavior. They are popular pets due to their ease of care, playful personalities, and ability to mimic human speech.
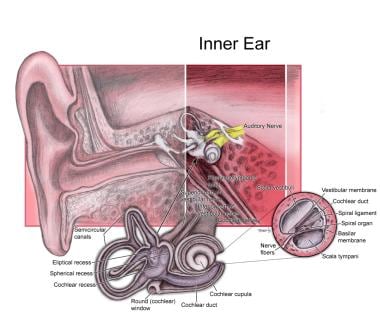
The cochlea is a part of the inner ear that is responsible for hearing. It is a spiral-shaped structure that looks like a snail shell and is filled with fluid. The cochlea contains hair cells, which are specialized sensory cells that convert sound vibrations into electrical signals that are sent to the brain.
The cochlea has three main parts: the vestibular canal, the tympanic canal, and the cochlear duct. Sound waves enter the inner ear and cause the fluid in the cochlea to move, which in turn causes the hair cells to bend. This bending motion stimulates the hair cells to generate electrical signals that are sent to the brain via the auditory nerve.
The brain then interprets these signals as sound, allowing us to hear and understand speech, music, and other sounds in our environment. Damage to the hair cells or other structures in the cochlea can lead to hearing loss or deafness.
In the context of medicine, particularly in audiology and otolaryngology (ear, nose, and throat specialty), "noise" is defined as unwanted or disturbing sound in the environment that can interfere with communication, rest, sleep, or cognitive tasks. It can also refer to sounds that are harmful to hearing, such as loud machinery noises or music, which can cause noise-induced hearing loss if exposure is prolonged or at high enough levels.
In some medical contexts, "noise" may also refer to non-specific signals or interfering factors in diagnostic tests and measurements that can make it difficult to interpret results accurately.
Hearing loss is a partial or total inability to hear sounds in one or both ears. It can occur due to damage to the structures of the ear, including the outer ear, middle ear, inner ear, or nerve pathways that transmit sound to the brain. The degree of hearing loss can vary from mild (difficulty hearing soft sounds) to severe (inability to hear even loud sounds). Hearing loss can be temporary or permanent and may be caused by factors such as exposure to loud noises, genetics, aging, infections, trauma, or certain medical conditions. It is important to note that hearing loss can have significant impacts on a person's communication abilities, social interactions, and overall quality of life.
Acoustic stimulation refers to the use of sound waves or vibrations to elicit a response in an individual, typically for the purpose of assessing or treating hearing, balance, or neurological disorders. In a medical context, acoustic stimulation may involve presenting pure tones, speech sounds, or other types of auditory signals through headphones, speakers, or specialized devices such as bone conduction transducers.
The response to acoustic stimulation can be measured using various techniques, including electrophysiological tests like auditory brainstem responses (ABRs) or otoacoustic emissions (OAEs), behavioral observations, or functional imaging methods like fMRI. Acoustic stimulation is also used in therapeutic settings, such as auditory training programs for hearing impairment or vestibular rehabilitation for balance disorders.
It's important to note that acoustic stimulation should be administered under the guidance of a qualified healthcare professional to ensure safety and effectiveness.
Sensory thresholds are the minimum levels of stimulation that are required to produce a sensation in an individual, as determined through psychophysical testing. These tests measure the point at which a person can just barely detect the presence of a stimulus, such as a sound, light, touch, or smell.
There are two types of sensory thresholds: absolute and difference. Absolute threshold is the minimum level of intensity required to detect a stimulus 50% of the time. Difference threshold, also known as just noticeable difference (JND), is the smallest change in intensity that can be detected between two stimuli.
Sensory thresholds can vary between individuals and are influenced by factors such as age, attention, motivation, and expectations. They are often used in clinical settings to assess sensory function and diagnose conditions such as hearing or vision loss.
The Differential Threshold, also known as the Just Noticeable Difference (JND), is the minimum change in a stimulus that can be detected or perceived as different from another stimulus by an average human observer. It is a fundamental concept in psychophysics, which deals with the relationship between physical stimuli and the sensations and perceptions they produce.
The differential threshold is typically measured using methods such as the method of limits or the method of constant stimuli, in which the intensity of a stimulus is gradually increased or decreased until the observer can reliably detect a difference. The difference between the original stimulus and the barely detectable difference is then taken as the differential threshold.
The differential threshold can vary depending on a number of factors, including the type of stimulus (e.g., visual, auditory, tactile), the intensity of the original stimulus, the observer's attention and expectations, and individual differences in sensory sensitivity. Understanding the differential threshold is important for many applications, such as designing sensory aids for people with hearing or vision impairments, optimizing the design of multimedia systems, and developing more effective methods for detecting subtle changes in physiological signals.
Pain threshold is a term used in medicine and research to describe the point at which a stimulus begins to be perceived as painful. It is an individual's subjective response and can vary from person to person based on factors such as their pain tolerance, mood, expectations, and cultural background.
The pain threshold is typically determined through a series of tests where gradually increasing levels of stimuli are applied until the individual reports feeling pain. This is often used in research settings to study pain perception and analgesic efficacy. However, it's important to note that the pain threshold should not be confused with pain tolerance, which refers to the maximum level of pain a person can endure.
 Evoked field
Evoked field Models of the auditory threshold - CLOK - Central Lancashire Online Knowledge
Models of the auditory threshold - CLOK - Central Lancashire Online Knowledge Retrospective auditory cues can improve detection of near-threshold visual targets | DEC Département d'études cognitives
Retrospective auditory cues can improve detection of near-threshold visual targets | DEC Département d'études cognitives ICD-10-CM/PCS MS-DRG v39.0 Definitions Manual
ICD-10-CM/PCS MS-DRG v39.0 Definitions Manual Hearing impairment in TRPV4 knockout mice
Hearing impairment in TRPV4 knockout mice Medical Science Monitor | Hearing threshold prediction with Auditory Steady State Responses and estimation of correction...
Medical Science Monitor | Hearing threshold prediction with Auditory Steady State Responses and estimation of correction... Speech processing for hearing-impaired listeners considering threshold elevation in the critical band with an expanded auditory...
Speech processing for hearing-impaired listeners considering threshold elevation in the critical band with an expanded auditory... PDF) Conditioned suppression/avoidance as a procedure for testing hearing in birds: The domestic pigeon (Columba livia)
PDF) Conditioned suppression/avoidance as a procedure for testing hearing in birds: The domestic pigeon (Columba livia) SciELO - Psicologia: Reflexão e Crítica, Volume: 24, Issue: 2, Published: 2011
SciELO - Psicologia: Reflexão e Crítica, Volume: 24, Issue: 2, Published: 2011 Middle Ear Function: Overview, What is Sound?, External Ear
Middle Ear Function: Overview, What is Sound?, External Ear MPD: Measure series: pip
MPD: Measure series: pip Frontiers | Altered Auditory and Multisensory Temporal Processing in Autism Spectrum Disorders
Frontiers | Altered Auditory and Multisensory Temporal Processing in Autism Spectrum Disorders Ida, be obnoxious | MetaFilter
Ida, be obnoxious | MetaFilter Amplitude Modulated Noise for Tinnitus Suppression in Tonal and Noise-Like Tinnitus | Audiology and Neurotology | Karger...
Amplitude Modulated Noise for Tinnitus Suppression in Tonal and Noise-Like Tinnitus | Audiology and Neurotology | Karger... Repetition suppression to objects is modulated by stimulus-specific expectations | Scientific Reports
Repetition suppression to objects is modulated by stimulus-specific expectations | Scientific Reports Carbon monoxide (EHC 13, 1979)
Carbon monoxide (EHC 13, 1979) Cheol-Ho Jeong - Publications
- Welcome to DTU Research Database
Cheol-Ho Jeong - Publications
- Welcome to DTU Research Database WikiGenes - AC1L2HRB - trimethyltin
WikiGenes - AC1L2HRB - trimethyltin The inner ear is slowly recovering from low frequency sound › Get a healthy home
The inner ear is slowly recovering from low frequency sound › Get a healthy home Hearing and age-related changes in the gray mouse lemur<...
Hearing and age-related changes in the gray mouse lemur<...