Barotrauma
Decompression Sickness
Diving
Ear, Middle
Lung Injury
Submarine Medicine
Paranasal Sinuses
Carbon Monoxide Poisoning
Aircraft
Hyperbaric Oxygenation
High-Frequency Jet Ventilation
Otitis Media with Effusion
High-Frequency Ventilation
Diving and the risk of barotrauma. (1/57)
STUDY OBJECTIVES: Pulmonary barotrauma (PBT) of ascent is a feared complication in compressed air diving. Although certain respiratory conditions are thought to increase the risk of suffering PBT and thus should preclude diving, in most cases of PBT, risk factors are described as not being present. The purpose of our study was to evaluate factors that possibly cause PBT. DESIGN: We analyzed 15 consecutive cases of PBT with respect to dive factors, clinical and radiologic features, and lung function. They were compared with 15 cases of decompression sickness without PBT, which appeared in the same period. RESULTS: Clinical features of PBT were arterial gas embolism (n = 13), mediastinal emphysema (n = 1), and pneumothorax (n = 1). CT of the chest (performed in 12 cases) revealed subpleural emphysematous blebs in 5 cases that were not detected in preinjury and postinjury chest radiographs. A comparison of predive lung function between groups showed significantly lower midexpiratory flow rates at 50% and 25% of vital capacity in PBT patients (p < 0.05 and p < 0.02, respectively). CONCLUSIONS: These results indicate that divers with preexisting small lung cysts and/or end-expiratory flow limitation may be at risk of PBT. (+info)Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. (2/57)
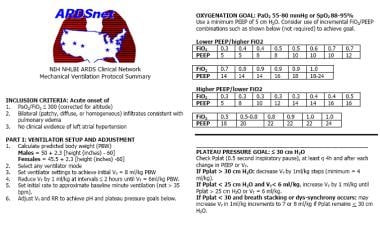
BACKGROUND: Traditional approaches to mechanical ventilation use tidal volumes of 10 to 15 ml per kilogram of body weight and may cause stretch-induced lung injury in patients with acute lung injury and the acute respiratory distress syndrome. We therefore conducted a trial to determine whether ventilation with lower tidal volumes would improve the clinical outcomes in these patients. METHODS: Patients with acute lung injury and the acute respiratory distress syndrome were enrolled in a multicenter, randomized trial. The trial compared traditional ventilation treatment, which involved an initial tidal volume of 12 ml per kilogram of predicted body weight and an airway pressure measured after a 0.5-second pause at the end of inspiration (plateau pressure) of 50 cm of water or less, with ventilation with a lower tidal volume, which involved an initial tidal volume of 6 ml per kilogram of predicted body weight and a plateau pressure of 30 cm of water or less. The primary outcomes were death before a patient was discharged home and was breathing without assistance and the number of days without ventilator use from day 1 to day 28. RESULTS: The trial was stopped after the enrollment of 861 patients because mortality was lower in the group treated with lower tidal volumes than in the group treated with traditional tidal volumes (31.0 percent vs. 39.8 percent, P=0.007), and the number of days without ventilator use during the first 28 days after randomization was greater in this group (mean [+/-SD], 12+/-11 vs. 10+/-11; P=0.007). The mean tidal volumes on days 1 to 3 were 6.2+/-0.8 and 11.8+/-0.8 ml per kilogram of predicted body weight (P<0.001), respectively, and the mean plateau pressures were 25+/-6 and 33+/-8 cm of water (P<0.001), respectively. CONCLUSIONS: In patients with acute lung injury and the acute respiratory distress syndrome, mechanical ventilation with a lower tidal volume than is traditionally used results in decreased mortality and increases the number of days without ventilator use. (+info)An approach to ventilation in acute respiratory distress syndrome. (3/57)
Appropriate management of patients with acute respiratory distress syndrome (ARDS) represents a challenge for physicians working in the critical care environment. Significant advances have been made in understanding the pathophysiology of ARDS. There is also an increasing appreciation of the role of ventilator-induced lung injury (VILI). VILI is most likely related to several different aspects of ventilator management: barotrauma due to high peak airway pressures, lung overdistension or volutrauma due to high transpulmonary pressures, alveolar membrane damage due to insufficient positive end expiratory pressure levels and oxygen-related cell toxicity. Various lung protective strategies have been suggested to minimize the damage caused by conventional modes of ventilation. These include the use of pressure- and volume-limited ventilation, the use of the prone position in the management of ARDS, and extracorporeal methods of oxygen delivery and carbon dioxide removal. Although the death rate resulting from ARDS has been declining over the past 10 years, there is no evidence that any specific treatment or change in approach to ventilation is the cause of this improved survival. (+info)Acute confusion secondary to pneumocephalus in an elderly patient. (4/57)
PRESENTATION: an 83-year-old man was admitted to hospital with acute confusion 3 days after a direct flight from Australia. OUTCOME: computed tomography (CT) brain scan and magnetic resonance imaging head scan revealed the cause to be pneumocephalus, apparently the result of barotrauma caused by Valsalva manoeuvres when he attempted to unblock his nose during the flight. After 5 days of nursing in the vertical position the patient's Abbreviated Mental Score returned to normal. A CT brain scan 6 weeks later showed complete resolution of the pneumocephalus. (+info)Neurologic complications of scuba diving. (5/57)
Recreational scuba diving has become a popular sport in the United States, with almost 9 million certified divers. When severe diving injury occurs, the nervous system is frequently involved. In dive-related barotrauma, compressed or expanding gas within the ears, sinuses and lungs causes various forms of neurologic injury. Otic barotrauma often induces pain, vertigo and hearing loss. In pulmonary barotrauma of ascent, lung damage can precipitate arterial gas embolism, causing blockage of cerebral blood vessels and alterations of consciousness, seizures and focal neurologic deficits. In patients with decompression sickness, the vestibular system, spinal cord and brain are affected by the formation of nitrogen bubbles. Common signs and symptoms include vertigo, thoracic myelopathy with leg weakness, confusion, headache and hemiparesis. Other diving-related neurologic complications include headache and oxygen toxicity. (+info)Cancer mortality after nasopharyngeal radium irradiation in the Netherlands: a cohort study. (6/57)
BACKGROUND: Nasopharyngeal radium irradiation (NRI) was used widely from 1940 through 1970 to treat otitis serosa in children and barotrauma in airmen and submariners. We assessed whether NRI-exposed individuals were at higher risk for cancer-related deaths than were nonexposed individuals. METHODS: We conducted a retrospective cohort study of all-cause and cancer-related mortality in 5358 NRI-exposed subjects and in 5265 frequency-matched nonexposed subjects, who as children were treated at nine ear, nose, and throat clinics in The Netherlands from 1945 through 1981. We recorded personal and medical data from original patient medical records and assessed vital status through follow-up at municipal population registries. Risk of mortality was evaluated by standardized mortality ratios (SMRs). All statistical tests were two-sided. RESULTS: The average radiation doses were 275, 10.9, 1.8, and 1.5 cGy for the nasopharynx, pituitary, brain, and thyroid, respectively. The median follow-up was 31.6 years. Three hundred two NRI-exposed subjects had died, with 269.2 deaths expected (SMR = 1.1; 95% confidence interval [CI] = 1.0 to 1.3); among nonexposed subjects, 315 died, with 283.5 deaths expected (SMR = 1.1; 95% CI = 0.99 to 1.2). Cancer-related deaths of 96 exposed subjects (SMR = 1.2; 95% CI = 0.95 to 1.4) and 87 nonexposed subjects (SMR = 1.0; 95% CI = 0.8 to 1.3) were documented. There were no excess deaths from cancers of the head and neck area among exposed subjects. However, there were excess deaths from cancers of lymphoproliferative and hematopoietic origin (SMR = 1.9; 95% CI = 1.1 to 3.0), mainly from non-Hodgkin's lymphoma (SMR = 2.6; 95% CI = 1.0 to 5.3). We found no evidence that breast cancer deaths were less than expected (SMR = 1.7; 95% CI = 0.9 to 2.8) in contrast to an earlier study. CONCLUSIONS: Our findings do not indicate an increased cancer mortality risk in a population exposed to NRI in childhood. More prolonged follow-up of this and other NRI cohorts is recommended. (+info)Proportional assist ventilation (PAV): a significant advance or a futile struggle between logic and practice? (7/57)
Proportional assist ventilation is a promising addition to other more conventional modes of mechanical ventilation with the theoretical advantage of improving patient-ventilator interaction. It may also be of use as a diagnostic tool in the control of breathing in mechanically ventilated patients. (+info)Continuous left hemidiaphragm sign revisited: a case of spontaneous pneumopericardium and literature review. (8/57)
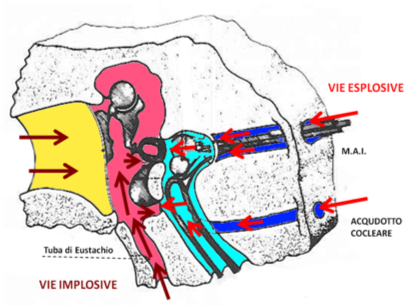
In pneumopericardium, a rare but potentially life threatening differential diagnosis of chest pain with a broad variety of causes, rapid diagnosis and adequate treatment are crucial. In upright posteroanterior chest radiography, the apical limit of a radiolucent rim, outlining both the left ventricle and the right atrium, lies at the level of the pulmonary artery and ascending aorta, reflecting the anatomical limits of the pericardium. The band of gas surrounding the heart may outline the normally invisible parts of the diaphragm, producing the continuous left hemidiaphragm sign in an upright lateral chest radiograph. If haemodynamic conditions are stable, the underlying condition should be treated and the patient should be monitored closely. Acute haemodynamic deterioration should prompt rapid further investigation and cardiac tamponade must be actively ruled out. Spontaneous pneumopericardium in a 20 year old man is presented, and its pathophysiology described. (+info)Barotrauma is a type of injury that occurs when there is a difference in pressure between the external environment and the internal body, leading to damage to body tissues. It commonly affects gas-filled spaces in the body, such as the lungs, middle ear, or sinuses.
In medical terms, barotrauma refers to the damage caused by changes in pressure that occur rapidly, such as during scuba diving, flying in an airplane, or receiving treatment in a hyperbaric chamber. These rapid changes in pressure can cause the gas-filled spaces in the body to expand or contract, leading to injury.
For example, during descent while scuba diving, the pressure outside the body increases, and if the diver does not equalize the pressure in their middle ear by swallowing or yawning, the increased pressure can cause the eardrum to rupture, resulting in barotrauma. Similarly, rapid ascent while flying can cause the air in the lungs to expand, leading to lung overexpansion injuries such as pneumothorax or arterial gas embolism.
Prevention of barotrauma involves equalizing pressure in the affected body spaces during changes in pressure and avoiding diving or flying with respiratory infections or other conditions that may increase the risk of injury. Treatment of barotrauma depends on the severity and location of the injury and may include pain management, antibiotics, surgery, or hyperbaric oxygen therapy.
Decompression sickness (DCS), also known as "the bends," is a medical condition that results from dissolved gases coming out of solution in the body's tissues and forming bubbles during decompression. This typically occurs when a person who has been exposed to increased pressure at depth, such as scuba divers or compressed air workers, ascends too quickly.
The elevated pressure at depth causes nitrogen to dissolve into the blood and tissues of the body. As the diver ascends and the pressure decreases, the dissolved gases form bubbles, which can cause symptoms ranging from joint pain and rashes to paralysis and death. The risk of DCS is influenced by several factors, including depth, duration of exposure, rate of ascent, and individual susceptibility.
Prevention of DCS involves following established dive tables or using a personal decompression computer to calculate safe ascent rates and decompression stops. Additionally, proper hydration, fitness, and avoiding alcohol and tobacco before diving can reduce the risk of DCS. Treatment typically involves administering oxygen and recompression therapy in a hyperbaric chamber.
The term "diving" is generally not used in the context of medical definitions. However, when referring to diving in relation to a medical or physiological context, it usually refers to the act of submerging the body underwater, typically for activities such as swimming, snorkeling, or scuba diving.
In a medical or physiological sense, diving can have specific effects on the human body due to changes in pressure, temperature, and exposure to water. Some of these effects include:
* Changes in lung volume and gas exchange due to increased ambient pressure at depth.
* Decompression sickness (DCS) or nitrogen narcosis, which can occur when dissolved gases form bubbles in the body during ascent from a dive.
* Hypothermia, which can occur if the water is cold and the diver is not adequately insulated.
* Barotrauma, which can occur due to pressure differences between the middle ear or sinuses and the surrounding environment.
* Other medical conditions such as seizures or heart problems can also be exacerbated by diving.
It's important for divers to undergo proper training and certification, follow safe diving practices, and monitor their health before and after dives to minimize the risks associated with diving.
The middle ear is the middle of the three parts of the ear, located between the outer ear and inner ear. It contains three small bones called ossicles (the malleus, incus, and stapes) that transmit and amplify sound vibrations from the eardrum to the inner ear. The middle ear also contains the Eustachian tube, which helps regulate air pressure in the middle ear and protects against infection by allowing fluid to drain from the middle ear into the back of the throat.
Lung injury, also known as pulmonary injury, refers to damage or harm caused to the lung tissue, blood vessels, or air sacs (alveoli) in the lungs. This can result from various causes such as infection, trauma, exposure to harmful substances, or systemic diseases. Common types of lung injuries include acute respiratory distress syndrome (ARDS), pneumonia, and chemical pneumonitis. Symptoms may include difficulty breathing, cough, chest pain, and decreased oxygen levels in the blood. Treatment depends on the underlying cause and may include medications, oxygen therapy, or mechanical ventilation.
Submarine Medicine is a specialized field of medicine that deals with the health and well-being of military personnel who serve on submarines. This includes preventing, diagnosing, and treating medical conditions that can occur in the unique environment of a submarine, such as changes in pressure, exposure to carbon monoxide and other gases, and isolation from medical resources on land. Submarine medicine also involves developing procedures and protocols for emergency medical situations that may arise while at sea, as well as ensuring the overall fitness of submariners to perform their duties. Additionally, submarine medicine specialists may provide guidance on issues related to nutrition, sleep, and mental health in order to maintain the optimal health and performance of submarine crews during prolonged submerged operations.
Paranasal sinuses are air-filled cavities in the skull that surround the nasal cavity. There are four pairs of paranasal sinuses, including the maxillary, frontal, ethmoid, and sphenoid sinuses. These sinuses help to warm, humidify, and filter the air we breathe. They also contribute to our voice resonance and provide a slight cushioning effect for the skull. The openings of the paranasal sinuses lead directly into the nasal cavity, allowing mucus produced in the sinuses to drain into the nose. Infections or inflammation of the paranasal sinuses can result in conditions such as sinusitis.
Carbon monoxide (CO) poisoning is a medical condition that occurs when carbon monoxide gas is inhaled, leading to the accumulation of this toxic gas in the bloodstream. Carbon monoxide is a colorless, odorless, and tasteless gas produced by the incomplete combustion of fossil fuels such as natural gas, propane, oil, wood, or coal.
When carbon monoxide is inhaled, it binds to hemoglobin, the protein in red blood cells responsible for carrying oxygen throughout the body. This binding forms carboxyhemoglobin (COHb), which reduces the oxygen-carrying capacity of the blood and leads to hypoxia, or insufficient oxygen supply to the body's tissues and organs.
The symptoms of carbon monoxide poisoning can vary depending on the level of exposure and the duration of exposure. Mild to moderate CO poisoning may cause symptoms such as headache, dizziness, weakness, nausea, vomiting, chest pain, and confusion. Severe CO poisoning can lead to loss of consciousness, seizures, heart failure, respiratory failure, and even death.
Carbon monoxide poisoning is a medical emergency that requires immediate treatment. Treatment typically involves administering high-flow oxygen therapy to help eliminate carbon monoxide from the body and prevent further damage to tissues and organs. In some cases, hyperbaric oxygen therapy may be used to accelerate the elimination of CO from the body.
Prevention is key in avoiding carbon monoxide poisoning. It is essential to ensure that all fuel-burning appliances are properly maintained and ventilated, and that carbon monoxide detectors are installed and functioning correctly in homes and other enclosed spaces.
An "aircraft" is not a medical term, but rather a general term used to describe any vehicle or machine designed to be powered and operated in the air. This includes fixed-wing aircraft such as airplanes and gliders, as well as rotary-wing aircraft such as helicopters and autogyros.
However, there are some medical conditions that can affect a person's ability to safely operate an aircraft, such as certain cardiovascular or neurological disorders. In these cases, the individual may be required to undergo medical evaluation and obtain clearance from aviation medical examiners before they are allowed to fly.
Additionally, there are some medical devices and equipment that are used in aircraft, such as oxygen systems and medical evacuation equipment. These may be used to provide medical care to passengers or crew members during flight.
Hyperbaric oxygenation is a medical treatment in which a patient breathes pure oxygen in a pressurized chamber, typically at greater than one atmosphere absolute (ATA). This process results in increased levels of oxygen being dissolved in the blood and delivered to body tissues, thereby promoting healing, reducing inflammation, and combating infection. Hyperbaric oxygen therapy is used to treat various medical conditions, including carbon monoxide poisoning, decompression sickness, gangrene, and wounds that are slow to heal due to diabetes or radiation injury.
In medical terms, "wind" is not a widely used or recognized term. It might be used informally to describe symptoms such as abdominal bloating, rumbling, or the sensation of gas moving within the intestines. However, these sensations are more accurately described as related to bowel function and gas in the digestive tract. If you're experiencing persistent or severe symptoms that you're describing as "wind," it would be best to consult with a healthcare professional for a proper evaluation.
High-frequency jet ventilation (HFJV) is a type of mechanical ventilation that delivers breaths at a frequency greater than 100 times per minute, typically in the range of 240-360 breaths per minute. It uses a high-pressure jet of gas to deliver small tidal volumes (usually less than 2 ml/kg of ideal body weight) into the airway.
The jet ventilation is often combined with a low-level positive end-expiratory pressure (PEEP) to maintain some lung volume and prevent atelectasis during exhalation. HFJV can be used in both invasive and noninvasive modes, depending on the patient's condition and requirements.
This mode of ventilation is particularly useful in patients with severe respiratory distress syndrome (ARDS), bronchopleural fistula, or air leaks from lung injury, as it minimizes gas flow and reduces the risk of air leakage while still maintaining adequate oxygenation and carbon dioxide elimination. However, HFJV requires careful monitoring and expertise to ensure proper settings and avoid complications such as barotrauma, hemodynamic instability, or inadequate ventilation.
I'm sorry for any confusion, but "power plants" is not a term used in medical definitions. It is a term commonly used to refer to industrial facilities that generate and distribute power, typically in the form of electricity. If you have any questions related to medicine or health, I would be happy to try to help answer those!
Otitis media with effusion (OME), also known as serous otitis media or glue ear, is a medical condition characterized by the presence of fluid in the middle ear without signs or symptoms of acute ear infection. The fluid accumulation occurs due to the dysfunction of the Eustachian tube, which results in negative pressure and subsequent accumulation of sterile fluid within the middle ear space.
OME can lead to hearing difficulties, especially in children, as the fluid buildup impairs sound conduction through the ossicles in the middle ear. Symptoms may include mild hearing loss, tinnitus (ringing in the ears), and a sensation of fullness or pressure in the affected ear. In some cases, OME can resolve on its own within a few weeks or months; however, persistent cases might require medical intervention, such as placement of tympanostomy tubes (ear tubes) to drain the fluid and restore hearing.
High-frequency ventilation (HFV) is a specialized mode of mechanical ventilation that delivers breaths at higher rates (usually 120-900 breaths per minute) and smaller tidal volumes (1-3 mL/kg) compared to conventional ventilation. This technique aims to reduce lung injury caused by overdistension and atelectasis, which can occur with traditional ventilator settings. It is often used in neonatal and pediatric intensive care units for the management of severe respiratory distress syndrome, meconium aspiration syndrome, and other conditions where conventional ventilation may be harmful.
There are two main types of high-frequency ventilation: high-frequency oscillatory ventilation (HFOV) and high-frequency jet ventilation (HFJV). Both techniques use different methods to generate the high-frequency breaths but share similar principles in delivering small tidal volumes at rapid rates.
In summary, high-frequency ventilation is a medical intervention that utilizes specialized ventilators to deliver faster and smaller breaths, minimizing lung injury and improving oxygenation for critically ill patients with severe respiratory distress.
Forensic medicine, also known as legal medicine or medical jurisprudence, is a branch of medicine that deals with the application of medical knowledge to legal issues and questions. It involves the examination, interpretation, and analysis of medical evidence for use in courts of law. This may include determining the cause and manner of death, identifying injuries or diseases, assessing the effects of substances or treatments, and evaluating the competency or capacity of individuals. Forensic medicine is often used in criminal investigations and court cases, but it can also be applied to civil matters such as personal injury claims or medical malpractice suits.