Chondrosarcoma
Chondrosarcoma, Mesenchymal
Chondroma
Chordoma
Myxosarcoma
Cartilage
Femoral Neoplasms
Skull Base Neoplasms
Exostoses, Multiple Hereditary
Neoplasms, Connective and Soft Tissue
Osteosarcoma
Ribs
Pelvic Bones
Chondroitinases and Chondroitin Lyases
Chondromatosis, Synovial
Osteochondroma
Inhibitory effects of transforming growth factor-beta1 pretreatment on experimental pulmonary metastasis of MCS-1 Chinese hamster mesenchymal chondrosarcoma cells. (1/35)
Recent studies have suggested that transforming growth factor(TGF)-beta1 acts as a multifunctional regulator of cell growth, and also modifies tumor progression and metastasis. In the present study, we investigated the effects of TGF-beta1 on the proliferation and experimental pulmonary metastasis of MCS-1. MCS-1 are undifferentiated type cloned tumor cells established from a mesenchymal chondrosarcoma which spontaneously occurred in the soft tissue of a female Chinese hamster. MCS-1 cells were pretreated with TGF-beta1 (0, 0.05, 0.5, 2, 10 ng/ml) for 72 hours in a medium containing 1% fetal bovine serum, then tested for in vitro growth by the MTT method, in vivo growth by subcutaneous inoculation into athymic nude mice (1 x 10(6) cells/mouse) and experimental pulmonary metastasis by injection into the lateral tail vein of athymic nude mice (5 x 10(4) cells/mouse). TGF-beta1 significantly inhibited in vitro growth of MCS-1, depending on its concentrations, and also experimental metastasis with maximal inhibition at 0.5 or 2 ng/ml treatment compared to untreated controls. TGF-beta1, however, was ineffective for in vivo subcutaneous growth of MCS-1. These results indicated that TGF-beta1 might be an inhibitor of metastasis of mesenchymal chondrosarcomas including other types of non-epitherial cartilage or bone formation tumors. (+info)Cell differentiation and matrix gene expression in mesenchymal chondrosarcomas. (2/35)
Mesenchymal chondrosarcomas are small-cell malignancies named as chondrosarcomas due to the focal appearance of cartilage islands. In this study, the use of in situ detection techniques on a large series of mesenchymal chondrosarcoma specimens allowed the identification of tumor-cell differentiation pathways in these neoplasms. We were able to trace all steps of chondrogenesis within mesenchymal chondrosarcoma by using characteristic marker genes of chondrocytic development. Starting from undifferentiated cells, which were negative for vimentin and any other mesenchymal marker, a substantial portion of the cellular (undifferentiated) tumor areas showed a chondroprogenitor phenotype with an onset of expression of vimentin and collagen type IIA. Cells in the chondroid areas showed the full expression panel of mature chondrocytes including type X collagen indicating focal hypertrophic differentiation of the neoplastic chondrocytes. Finally, evidence was found for transdifferentiation of the neoplastic chondrocytes to osteoblast-like cells in areas of neoplastic bone formation. These results establish mesenchymal chondrosarcoma as the very neoplasm of differentiating premesenchymal chondroprogenitor cells. The potential of neoplastic bone formation in mesenchymal chondrosarcoma introduces a new concept of neoplastic (chondrocytic) osteogenesis in musculoskeletal malignant neoplasms, which qualifies the old dogma that neoplastic bone/osteoid formation automatically implies the diagnosis of osteosarcoma. (+info)Prostaglandin D synthase (beta-trace) in meningeal hemangiopericytoma. (3/35)
The level of prostaglandin D synthase (PGDS), a major protein constituent of cerebrospinal fluid (CSF), is altered in various brain diseases, including meningitis. However, its role in the brain remains unclear. PGDS is mainly synthesized in the arachnoid cells, the choroid plexus and oligodendrocytes in the central nervous system. Among brain tumors, meningiomas showed intense immunoreactivity to PGDS in the perinuclear region. Thus, PGDS has been considered a specific cell marker of meningioma. In this study, we examined 25 meningeal hemangiopericytomas (HPCs) and found that 16 of the tumors (64%) showed immunoreactivity for PGDS in the perinuclear region. For comparison, 15 meningiomas, 14 soft-tissue HPCs, 1 mesenchymal chondrosarcoma, 3 choroid plexus papillomas, and 7 oligodendrogliomas were also examined. Meningiomas showed positive immunoreactivity for PGDS in 13 cases (80%). Except for one case located at the sacrum, none of the other soft-tissue HPCs showed immunostaining for PGDS. Mesenchymal chondrosarcoma arises in the bones of the skull, and its histological pattern resembles that of HPC; however, it showed no immunoreactivity for PGDS. Neither choroid plexus papillomas nor oligodendrogliomas were immunopositive for PGDS. These findings suggest that meningeal HPCs may have a unique molecular phenotype that is distinct from that of the soft-tissue HPCs. The origin of meningeal HPCs may be more closely related to the arachnoid cells. (+info)Chondrosarcoma of bone: an oncological and functional follow-up study. (4/35)
We retrospectively analysed the course of 42 out of 45 patients suffering from different chondrosarcomas which were treated surgically. We found a prospective 5- and 10-year survival of 64% for both time intervals. Follow-up examination was possible in 21 of 45 patients. Most of them were staged as NED, one as AWD, and 8 of 45 were lost to follow-up. From 16 dead patients 12 died of the disease and 4 of unknown but not to tumor related reasons. Survival was depending significantly on the histopathological grade, and the stage according to Enneking's surgical staging system. Eleven out of forty-five patients developed metastases within a mean period of twelve months after surgery. The survival of these patients was significantly reduced. Patients with centrally located tumors exhibited a distinct but non-significant worse survival than those suffering from peripheral tumors. In 18% (8 of 45) recurrence of the tumor was evident within a mean period of 24 months (5-85). Functional evaluation was performed in 21 out of 28 alive patients. After a mean follow-up time of 72 months the mean score was 64% (23-100). Females exhibited a distinct but non-significant better result, the same was observed for peripheral locations compared to centrally located tumors. Regarding age, grade, and line of resection no tendency of any dependence was detected, but worst results were seen in those with a stage III tumor and dedifferentiated CS. (+info)Translocation der(13;21)(q10;q10) in skeletal and extraskeletal mesenchymal chondrosarcoma. (5/35)
Cytogenetic studies of mesenchymal chondrosarcoma are few and to date, no specific or recurrent aberrations have been found. In this investigation, the cytogenetic and molecular cytogenetic (spectral karyotypic and fluorescence in situ hybridization) findings for two mesenchymal chondrosarcomas, one arising skeletally and the other extraskeletally, are reported. An identical Robertsonian translocation involving chromosomes 13 and 21 [der(13;21)(q10;q10)] was detected in both cases, possibly representing a characteristic rearrangement for this histopathologic entity. Both cases also exhibited loss of all or a portion of chromosomes 8 and 20 and gain of all or a portion of chromosome 12. The observation of similar chromosomal abnormalities in both skeletal and extraskeletal mesenchymal chondrosarcoma supports a genetic as well as histopathologic relationship between these anatomically distinct neoplasms. (+info)Retroperitoneal extraskeletal mesenchymal chondrosarcoma in a dog. (6/35)
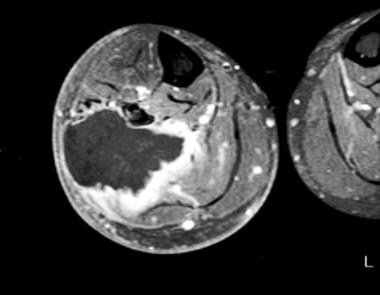
A young adult female Mastiff dog developed a large retroperitoneal mass, pleural effusion, and multiple pulmonary and pleural nodules. All masses were diagnosed as mesenchymal subtype chondrosarcomas, using histological and immunohistochemical criteria. Reports of canine extraskeletal mesenchymal chondrosarcomas (EMCs) are rare but involved animals less than 3 years of age in 60% of the cases. This is the first description of this type of tumor developing distant metastases. Evidence from this case and previous reports suggests that EMCs are associated with a poor prognosis. (+info)Mesenchymal chondrosarcoma originating from the femoral vein. (7/35)
Mesenchymal chondrosarcoma is a rare variant of chondrosarcomas characterized by a bimorphic pattern with areas of the undifferentiated malignant small cells and well differentiated cartilaginous islands.(1) It occurs most commonly in the bone but can also occur in the extraskeletal soft tissues, the brain, and the meninges. This type of tumor has also been described in the eyelids, parapharyngeal space, mediastinum, and the kidney.(1-5) An origin from the large vessels has not been reported in the medical literature. The authors report a case of mesenchymal chondrosarcoma originating from the femoral vein in a 28-year-old female patient, treated by the wide-margin resection. (+info)Cytopathology of mesenchymal chondrosarcomas: a report and comparison of four patients. (8/35)
BACKGROUND: Mesenchymal chondrosarcoma (MC) is an infrequent neoplasm, representing approximately 1% of all chondrosarcomas. Cytologic descriptions of MCs have been confined to rare case reports. In the current report, the authors describe their experience with the cytologic features of four MCs: two primary tumors and two metastatic lesions. METHODS: Four patients were diagnosed with MC at the authors' institution from 1994 to 2002. Three of four patients underwent fine-needle aspiration (FNA) biopsy as part of their diagnosis; in the fourth patient, imprint cytology was performed. Each tumor also received histologic confirmation. RESULTS: The patients studied included three females and one male. In three patients, the tumor presented initially as a soft tissue mass; whereas, in the remaining patient, the MC presented in the tibia. FNA results demonstrated small, oval-to-spindled cells with high nuclear-to-cytoplasmic ratios. Cells occurred singly and in clumps in a background of basophilic extracellular matrix. Histologic examination of each lesion demonstrated biphasic tumors, including focal areas of relatively mature cartilage formation as well as a small cell population. CONCLUSIONS: MC is a rare soft tissue tumor that occurs frequently in extraskeletal locations. FNA of these tumors can be diagnostic if the tumor is sampled appropriately and of critical features, such as the background extracellular matrix, are recognized. Given the propensity of these tumors to metastasize and the poor prognosis of patients with MC, early identification by FNA biopsy may allow earlier, more aggressive interventions. (+info)Chondrosarcoma is a type of cancer that develops in the cartilaginous tissue, which is the flexible and smooth connective tissue found in various parts of the body such as the bones, ribs, and nose. It is characterized by the production of malignant cartilage cells that can invade surrounding tissues and spread to other parts of the body (metastasis).
Chondrosarcomas are typically slow-growing tumors but can be aggressive in some cases. They usually occur in adults over the age of 40, and men are more commonly affected than women. The most common sites for chondrosarcoma development include the bones of the pelvis, legs, and arms.
Treatment for chondrosarcoma typically involves surgical removal of the tumor, along with radiation therapy or chemotherapy in some cases. The prognosis for chondrosarcoma depends on several factors, including the size and location of the tumor, the grade of malignancy, and whether it has spread to other parts of the body.
Chondrosarcoma, mesenchymal is a type of chondrosarcoma, which is a malignant (cancerous) tumor that arises from cartilaginous tissue. It is a rare and aggressive subtype of chondrosarcoma, accounting for less than 10% of all cases.
Mesenchymal chondrosarcomas are characterized by their undifferentiated small round blue cells intermixed with well-differentiated cartilaginous areas. They can occur in any age group but are more common in children and young adults. These tumors can arise in any bone, but they most commonly involve the long bones of the extremities, pelvis, and spine.
Mesenchymal chondrosarcomas tend to be aggressive with a high risk of local recurrence and metastasis (spread) to other parts of the body, such as the lungs, lymph nodes, or other bones. Treatment typically involves surgical resection of the tumor, often followed by radiation therapy and/or chemotherapy. The prognosis for mesenchymal chondrosarcoma is generally poorer than for other subtypes of chondrosarcoma due to its aggressive behavior and higher likelihood of metastasis.
A chondroma is a benign, slow-growing tumor that develops in the cartilage. Cartilage is a type of connective tissue found in various parts of the body, including the joints, ribcage, and nose. Chondromas are most commonly found in the hands and feet.
Chondromas are typically small, measuring less than 2 centimeters in diameter, and they usually do not cause any symptoms. However, if a chondroma grows large enough to press on nearby nerves or blood vessels, it may cause pain, numbness, or weakness in the affected area.
Chondromas are usually diagnosed through imaging tests such as X-rays, CT scans, or MRI scans. If a chondroma is suspected based on these tests, a biopsy may be performed to confirm the diagnosis and rule out other types of tumors.
Treatment for chondromas typically involves surgical removal of the tumor. In most cases, this can be done using minimally invasive techniques that allow for quicker recovery times. After surgery, patients will need to follow up with their healthcare provider to ensure that the tumor has been completely removed and to monitor for any signs of recurrence.
Bone neoplasms are abnormal growths or tumors that develop in the bone. They can be benign (non-cancerous) or malignant (cancerous). Benign bone neoplasms do not spread to other parts of the body and are rarely a threat to life, although they may cause problems if they grow large enough to press on surrounding tissues or cause fractures. Malignant bone neoplasms, on the other hand, can invade and destroy nearby tissue and may spread (metastasize) to other parts of the body.
There are many different types of bone neoplasms, including:
1. Osteochondroma - a benign tumor that develops from cartilage and bone
2. Enchondroma - a benign tumor that forms in the cartilage that lines the inside of the bones
3. Chondrosarcoma - a malignant tumor that develops from cartilage
4. Osteosarcoma - a malignant tumor that develops from bone cells
5. Ewing sarcoma - a malignant tumor that develops in the bones or soft tissues around the bones
6. Giant cell tumor of bone - a benign or occasionally malignant tumor that develops from bone tissue
7. Fibrosarcoma - a malignant tumor that develops from fibrous tissue in the bone
The symptoms of bone neoplasms vary depending on the type, size, and location of the tumor. They may include pain, swelling, stiffness, fractures, or limited mobility. Treatment options depend on the type and stage of the tumor but may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
Enchondromatosis is a rare skeletal disorder characterized by the development of multiple enchondromas, which are benign tumors made up of cartilage that form within the bone. These growths can occur in any bone but are most commonly found in the hands and feet. Enchondromatosis can be inherited or may develop sporadically.
There are two main types of enchondromatosis: Ollier disease and Maffucci syndrome. Ollier disease is characterized by multiple enchondromas, typically affecting one side of the body more than the other. Maffucci syndrome is a more severe form of enchondromatosis that includes both enchondromas and benign soft tissue tumors called hemangiomas.
The symptoms of enchondromatosis can vary widely, depending on the size and location of the enchondromas. Some individuals may experience bone pain, fractures, or deformities, while others may have no noticeable symptoms. In rare cases, enchondromas can become malignant, leading to the development of chondrosarcoma, a type of cancer that arises from cartilage.
Treatment for enchondromatosis typically involves monitoring for changes in the size or shape of the tumors and addressing any symptoms as they arise. Surgery may be necessary in some cases to remove large or symptomatic enchondromas, particularly if there is a risk of malignant transformation. Regular follow-up with an orthopedic specialist is recommended to monitor for potential complications.
A chordoma is a rare, slow-growing tumor that typically develops in the bones of the spine or skull. These tumors originate from remnants of the notochord, a structure that forms during embryonic development and eventually becomes part of the spinal cord. Chordomas are usually low-grade malignancies but can be aggressive and locally invasive, potentially causing pain, neurological symptoms, or structural damage to the spine or skull. Treatment typically involves surgical resection, often combined with radiation therapy.
Myxosarcoma is a very rare type of soft tissue sarcoma, a cancer that develops in the soft tissues of the body, such as fat, muscle, nerves, blood vessels, and fibrous tissues. Myxosarcomas are characterized by the presence of mucoid or gelatinous material in the tumor, which is composed of an abnormal accumulation of acid mucopolysaccharides. These tumors typically affect adults, with a peak incidence in the sixth to seventh decade of life. They usually occur in the extremities, particularly the lower limbs, and can also arise in the retroperitoneum or other deep soft tissues. Myxosarcomas are classified into several subtypes based on their histological features, with the most common being the myxofibrosarcoma. Treatment typically involves surgical resection with wide margins, often followed by radiation therapy and/or chemotherapy. The prognosis for patients with myxosarcoma depends on several factors, including the size and location of the tumor, the histological grade, and the patient's age and overall health.
Cartilage is a type of connective tissue that is found throughout the body in various forms. It is made up of specialized cells called chondrocytes, which are embedded in a firm, flexible matrix composed of collagen fibers and proteoglycans. This unique structure gives cartilage its characteristic properties of being both strong and flexible.
There are three main types of cartilage in the human body: hyaline cartilage, elastic cartilage, and fibrocartilage.
1. Hyaline cartilage is the most common type and is found in areas such as the articular surfaces of bones (where they meet to form joints), the nose, trachea, and larynx. It has a smooth, glassy appearance and provides a smooth, lubricated surface for joint movement.
2. Elastic cartilage contains more elastin fibers than hyaline cartilage, which gives it greater flexibility and resilience. It is found in structures such as the external ear and parts of the larynx and epiglottis.
3. Fibrocartilage has a higher proportion of collagen fibers and fewer chondrocytes than hyaline or elastic cartilage. It is found in areas that require high tensile strength, such as the intervertebral discs, menisci (found in joints like the knee), and the pubic symphysis.
Cartilage plays a crucial role in supporting and protecting various structures within the body, allowing for smooth movement and providing a cushion between bones to absorb shock and prevent wear and tear. However, cartilage has limited capacity for self-repair and regeneration, making damage or degeneration of cartilage tissue a significant concern in conditions such as osteoarthritis.
Femoral neoplasms refer to abnormal growths or tumors that develop in the femur, which is the long thigh bone in the human body. These neoplasms can be benign (non-cancerous) or malignant (cancerous). Benign femoral neoplasms are slow-growing and rarely spread to other parts of the body, while malignant neoplasms are aggressive and can invade nearby tissues and organs, as well as metastasize (spread) to distant sites.
There are various types of femoral neoplasms, including osteochondromas, enchondromas, chondrosarcomas, osteosarcomas, and Ewing sarcomas, among others. The specific type of neoplasm is determined by the cell type from which it arises and its behavior.
Symptoms of femoral neoplasms may include pain, swelling, stiffness, or weakness in the thigh, as well as a palpable mass or limited mobility. Diagnosis typically involves imaging studies such as X-rays, CT scans, or MRI, as well as biopsy to determine the type and grade of the tumor. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches, depending on the type, size, location, and stage of the neoplasm.
Skull base neoplasms refer to abnormal growths or tumors located in the skull base, which is the region where the skull meets the spine and where the brain connects with the blood vessels and nerves that supply the head and neck. These neoplasms can be benign (non-cancerous) or malignant (cancerous), and they can arise from various types of cells in this area, including bone, nerve, glandular, and vascular tissue.
Skull base neoplasms can cause a range of symptoms depending on their size, location, and growth rate. Some common symptoms include headaches, vision changes, hearing loss, facial numbness or weakness, difficulty swallowing, and balance problems. Treatment options for skull base neoplasms may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. The specific treatment plan will depend on the type, size, location, and stage of the tumor, as well as the patient's overall health and medical history.
Multiple hereditary exostoses (MHE) is a genetic condition characterized by the growth of multiple benign tumors known as osteochondromas. These tumors typically develop at the ends of long bones near the growth plates and can cause various skeletal deformities, limitations in mobility, and other health issues.
MHE is usually inherited in an autosomal dominant pattern, meaning that a child has a 50% chance of inheriting the condition if one parent has it. However, some cases may result from spontaneous mutations. The condition typically becomes apparent during childhood or adolescence and can affect both sexes equally.
The primary diagnostic feature of MHE is the presence of multiple osteochondromas, which are made up of bone and cartilage. These growths can cause a range of symptoms, including pain, swelling, decreased mobility, and an increased risk of fractures. In some cases, they may also lead to complications such as nerve compression or vascular damage.
Treatment for MHE typically involves surgical removal of the osteochondromas, particularly if they are causing significant symptoms or complications. Regular monitoring is also important to detect any new growths and assess their potential impact on health. In addition, physical therapy and other supportive measures may be recommended to help manage symptoms and maintain mobility.
Neoplasms of connective and soft tissue are abnormal growths or tumors that develop in the body's supportive tissues, such as cartilage, tendons, ligaments, fascia, and fat. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign connective and soft tissue neoplasms include:
- Lipomas: slow-growing, fatty tumors that develop under the skin.
- Fibromas: firm, benign tumors that develop in connective tissue such as tendons or ligaments.
- Nevi (plural of nevus): benign growths made up of cells called melanocytes, which produce pigment.
Malignant connective and soft tissue neoplasms include:
- Sarcomas: a type of cancer that develops in the body's supportive tissues such as muscle, bone, fat, cartilage, or blood vessels. There are many different types of sarcomas, including liposarcoma (fatty tissue), rhabdomyosarcoma (muscle), and osteosarcoma (bone).
- Desmoid tumors: a rare type of benign tumor that can become aggressive and invade surrounding tissues. While not considered cancerous, desmoid tumors can cause significant morbidity due to their tendency to grow and infiltrate nearby structures.
Connective and soft tissue neoplasms can present with various symptoms depending on their location and size. Treatment options include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular follow-up care is essential to monitor for recurrence or metastasis (spread) of the tumor.
Osteosarcoma is defined as a type of cancerous tumor that arises from the cells that form bones (osteoblasts). It's the most common primary bone cancer, and it typically develops in the long bones of the body, such as the arms or legs, near the growth plates. Osteosarcoma can metastasize (spread) to other parts of the body, including the lungs, making it a highly malignant form of cancer. Symptoms may include bone pain, swelling, and fractures. Treatment usually involves a combination of surgery, chemotherapy, and/or radiation therapy.
In medical terms, ribs are the long, curved bones that make up the ribcage in the human body. They articulate with the thoracic vertebrae posteriorly and connect to the sternum anteriorly via costal cartilages. There are 12 pairs of ribs in total, and they play a crucial role in protecting the lungs and heart, allowing room for expansion and contraction during breathing. Ribs also provide attachment points for various muscles involved in respiration and posture.
The pelvic bones, also known as the hip bones, are a set of three irregularly shaped bones that connect to form the pelvic girdle in the lower part of the human body. They play a crucial role in supporting the spine and protecting the abdominal and pelvic organs.
The pelvic bones consist of three bones:
1. The ilium: This is the largest and uppermost bone, forming the majority of the hip bone and the broad, flaring part of the pelvis known as the wing of the ilium or the iliac crest, which can be felt on the side of the body.
2. The ischium: This is the lower and back portion of the pelvic bone that forms part of the sitting surface or the "sit bones."
3. The pubis: This is the front part of the pelvic bone, which connects to the other side at the pubic symphysis in the midline of the body.
The pelvic bones are joined together at the acetabulum, a cup-shaped socket that forms the hip joint and articulates with the head of the femur (thigh bone). The pelvic bones also have several openings for the passage of blood vessels, nerves, and reproductive and excretory organs.
The shape and size of the pelvic bones differ between males and females due to their different roles in childbirth and locomotion. Females typically have a wider and shallower pelvis than males to accommodate childbirth, while males usually have a narrower and deeper pelvis that is better suited for weight-bearing and movement.
Chondroitinases and chondroitin lyases are enzymes that break down chondroitin sulfate, a type of glycosaminoglycan (GAG) found in connective tissues such as cartilage. Glycosaminoglycans are long, unbranched polysaccharides made up of repeating disaccharide units. In the case of chondroitin sulfate, the disaccharide unit consists of a glucuronic acid residue and a N-acetylgalactosamine residue that may be sulfated at various positions.
Chondroitinases are enzymes that cleave the linkage between the two sugars in the chondroitin sulfate chain, specifically between the carbon atom in the fourth position of the glucuronic acid and the nitrogen atom in the first position of the N-acetylgalactosamine. This results in the formation of unsaturated disaccharides. Chondroitinases are produced by certain bacteria and are used in research to study the structure and function of chondroitin sulfate and other GAGs.
Chondroitin lyases, on the other hand, are enzymes that cleave the same linkage but in the opposite direction, resulting in the formation of 4,5-unsaturated disaccharides. Chondroitin lyases are also produced by certain bacteria and are used in research to study the structure and function of chondroitin sulfate and other GAGs.
It is important to note that while both chondroitinases and chondroitin lyases break down chondroitin sulfate, they do so through different mechanisms and produce different products.
Synovial chondromatosis is a rare condition that affects the synovial membrane, which is the lining of joints, bursae (fluid-filled sacs that cushion bones), and tendon sheaths. In this condition, nodules made up of cartilage form in the synovial membrane. These nodules can detach from the synovial membrane and float freely in the synovial fluid, which lubricates the joint. If they become numerous, they can cause joint pain, stiffness, and decreased range of motion. In some cases, the loose bodies may also cause locking or catching sensations in the joint. Surgery is typically required to remove the cartilaginous nodules and relieve symptoms. If left untreated, synovial chondromatosis can lead to osteoarthritis and other joint problems.
Proteoglycans are complex, highly negatively charged macromolecules that are composed of a core protein covalently linked to one or more glycosaminoglycan (GAG) chains. They are a major component of the extracellular matrix (ECM) and play crucial roles in various biological processes, including cell signaling, regulation of growth factor activity, and maintenance of tissue structure and function.
The GAG chains, which can vary in length and composition, are long, unbranched polysaccharides that are composed of repeating disaccharide units containing a hexuronic acid (either glucuronic or iduronic acid) and a hexosamine (either N-acetylglucosamine or N-acetylgalactosamine). These GAG chains can be sulfated to varying degrees, which contributes to the negative charge of proteoglycans.
Proteoglycans are classified into four major groups based on their core protein structure and GAG composition: heparan sulfate/heparin proteoglycans, chondroitin/dermatan sulfate proteoglycans, keratan sulfate proteoglycans, and hyaluronan-binding proteoglycans. Each group has distinct functions and is found in specific tissues and cell types.
In summary, proteoglycans are complex macromolecules composed of a core protein and one or more GAG chains that play important roles in the ECM and various biological processes, including cell signaling, growth factor regulation, and tissue structure maintenance.
Osteochondroma is a benign (noncancerous) bone tumor that typically develops during childhood or adolescent growth years. It usually forms near the end of long bones, such as those in the arms and legs, but can also occur in other bones. An osteochondroma may have a cartilage cap covering its surface.
This type of tumor often grows slowly and typically stops growing once the person has stopped growing. In many cases, an osteochondroma doesn't cause any symptoms and doesn't require treatment. However, if it continues to grow or causes problems such as pain, restricted movement, or bone deformity, surgical removal may be necessary.
Most osteochondromas are solitary (occurring singly), but some people can develop multiple tumors, a condition known as multiple hereditary exostoses or diaphyseal aclasis. This genetic disorder is associated with a higher risk of developing sarcoma, a type of cancerous tumor that can arise from osteochondromas.
It's essential to have regular follow-ups with your healthcare provider if you have an osteochondroma to monitor its growth and any potential complications.
Maxillary neoplasms refer to abnormal growths or tumors in the maxilla, which is the upper jaw bone. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are slow-growing and do not spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and spread to distant sites.
Maxillary neoplasms can cause various symptoms such as swelling, pain, numbness, loose teeth, or difficulty in chewing or swallowing. They may also cause nasal congestion, nosebleeds, or visual changes if they affect the eye or orbit. The diagnosis of maxillary neoplasms usually involves a combination of clinical examination, imaging studies such as CT or MRI scans, and biopsy to determine the type and extent of the tumor.
Treatment options for maxillary neoplasms depend on several factors, including the type, size, location, and stage of the tumor, as well as the patient's overall health and preferences. Treatment may include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular follow-up care is essential to monitor for recurrence or metastasis and ensure optimal outcomes.
Osteosarcoma7
- There are three main types of bone sarcoma based on tissue type - an osteosarcoma, a Ewing's sarcoma, and a chondrosarcoma. (wikipedia.org)
- Subtypes of chondrosarcomas have different features and different outlooks, they include:[citation needed] Dedifferentiated Dedifferentiated chondrosarcomas can change in part to cells that are like those of an osteosarcoma for example which has a faster rate of growth. (wikipedia.org)
- A case of malignant mesenchymoma of the bladder containing leiomyosarcoma, rhabdomyosarcoma, chondrosarcoma, osteosarcoma, and myxomatous components is described. (biomedcentral.com)
- Solid primary lesions of the hyoid bone are exceedingly rare and the reported cases have included plasmacytoma, osteosarcoma, giant cell tumor, aneurysmal bone cysts, osteoma, chondroma, and chondrosarcoma. (ajnr.org)
- We investigated the effect of micronutrient synergy in vitro on human rhabdosarcoma, liposarcoma and chondrosarcoma cell lines and, in vitro and in vivo on human osteosarcoma, synovial sarcoma and fibrosarcoma cell lines. (drrathresearch.org)
- Bone sarcomas such as osteosarcoma and chondrosarcoma are frequently refractory to conventional chemotherapy and radiotherapy that exhibit poor prognosis. (oncotarget.com)
- With patients who present with locally advanced or metastatic chondrosarcoma, chordoma, or osteosarcoma, physicians should discuss the options surrounding deep-sequencing genomic tests, which may identify mutations that may be responsive to specific therapies and thus may guide referral to clinical trials. (medscape.com)
Tumors4
- Chondrosarcoma is a collective term for a group of tumors that consist predominantly of cartilage and that range from low-grade tumors with low metastatic potential to high-grade, aggressive tumors characterized by early metastasis. (medscape.com)
- Mesenchymal chondrosarcoma (MC) must be differentiated from other malignant small cell tumors of bone and soft tissue . (webpathology.com)
- Chondrosarcomas constitute approximately 11% of all primary bone tumors. (ajnr.org)
- The differential diagnosis of a malignant effusion is accordingly broad, especially for the small round blue cell tumors that includes not only mesenchymal tumors, but also non-mesenchymal tumors, such as neuroblastoma and Wilms tumor. (cytojournal.com)
Extraskeletal Myxoid Chondrosarcoma1
- It is also known as EMC (Extraskeletal Myxoid Chondrosarcoma). (healthadvicer.com)
Undifferentiated mesenchymal cells2
- The histological features of mesenchymal chondrosarcoma was first described by Lichtenstein and Bernstein (1959), consist of primitive undifferentiated mesenchymal cells in which islands of cartilage are noted. (e-crt.org)
- The tumor is composed of rich cellular and undifferentiated mesenchymal cells and well-differentiated cartilage. (e-crt.org)
Sarcoma3
- Ewing's sarcoma, and a chondrosarcoma. (wikipedia.org)
- Rhabdosarcoma , the most common soft tissue sarcoma is mesenchymal in origin, and affects infants and children up to five years (mostly males). (drrathresearch.org)
- The cancer is different from the other sarcoma due to the presence of the unique myxoid chondrosarcoma. (healthadvicer.com)
Diagnosis4
- The prognosis of chondrosarcoma correlates with the grade and stage of the lesion at the time of diagnosis . (wikidoc.org)
- The diagnosis of a chondrosarcoma of the hyoid bone may be missed because of its infrequent occurrence. (ajnr.org)
- Patient demographic data, histologic diagnosis, and chondrosarcoma grade were recorded. (rsna.org)
- A differential diagnosis of chondrosarcoma should be considered because of the life-threatening features of chondrosarcoma. (bvsalud.org)
Conventional chondrosarcoma3
- If the sample contains predominance of well-differentiated hyaline cartilage , it can be mistaken for conventional chondrosarcoma . (webpathology.com)
- Radiographic features of MC also resemble those of conventional chondrosarcoma. (webpathology.com)
- Conventional chondrosarcoma are further subdivided into grade I, grade II, and grade III. (abta.org)
Benign5
- Benign cartilage lesions can be difficult to differentiate from slow-growing, low-grade chondrosarcomas. (medscape.com)
- Secondary chondrosarcoma can occur in a previously benign cartilaginous lesion. (medscape.com)
- This study supports application of a standardized measuring technique for improved distinction of benign osteochondromas from chondrosarcomas, with a cartilage cap thickness of 2 cm or greater as the determinant of chondrosarcoma. (rsna.org)
- To validate a technique for reproducible measurement of the osteochondroma cartilage cap with computed tomography (CT) and magnetic resonance (MR) imaging and to reevaluate the correlation of the thickness of the cartilage cap with pathologic findings to improve noninvasive differentiation of benign osteochondromas from secondary chondrosarcomas. (rsna.org)
- With 2 cm used as a cutoff for distinguishing benign osteochondromas from chondrosarcomas, the sensitivities and specificities were 100% and 98% for MR imaging and 100% and 95% for CT, respectively. (rsna.org)
Type of bone2
- A chondrosarcoma is the type of bone cancer that starts in the cartilage cells. (wikipedia.org)
- Chondrosarcoma is the rare type of bone cancer. (healthadvicer.com)
Secondary2
- Cap thickness of 2 cm or greater strongly indicated secondary chondrosarcomas. (rsna.org)
- Therefore, this article reports a case of giant chondrosarcoma secondary to MS with a long medical history. (biomedcentral.com)
20201
- In the latest version of the guidelines released in November 2020, surgery is the main treatment for chondrosarcoma, chordoma, and giant cell tumor of bone, which can be combined with radiotherapy or targeted therapy. (bvsalud.org)
Histologic2
- Performing a truly representative biopsy of a chondrosarcoma is challenging because the lesion is composed of areas that carry different histologic grades. (medscape.com)
- Osteosarcomas and chondrosarcomas are recognized as the most common primary bone sarcomas [ 1 ], which involve mesenchymal tissues and exhibit highly heterogeneous histologic and molecular profiles [ 2 ]. (oncotarget.com)
Differentiation2
- Agreement between measurements with CT and MR imaging was also evaluated, as were the sensitivity and specificity of both modalities for differentiation of osteochondromas from chondrosarcomas. (rsna.org)
- The differentiation of mesenchymal stem cells (MSCs) into multiple cell lineages can be exploited as an attractive strategy for cell-based therapy and regenerative medicine [ 1 ]. (hindawi.com)
Subtype1
- Introduction Mesenchymal chondrosarcoma is a rare and aggressive variant subtype of chondrosarcoma, which represents ~1% of all chondrosarcomas. (docksci.com)
Rhabdomyosarcoma1
- Rhabdomyosarcoma (RMS) is a malignant tumor of mesenchymal origin and comprises the largest category of soft-tissue sarcomas both in children and adolescents. (biomedcentral.com)
Metastasis2
- Complications that can develop as a result of chondrosarcoma are metastasis and recurrence. (wikidoc.org)
- Follow up scans are extremely important for chondrosarcoma to make sure there has been no recurrence or metastasis . (wikidoc.org)
Primary bone1
- Here, we report two challenging cases involving 17- and 9-years-olds males where diffuse and multiplex bone lesions suggested either a hematological disease or a primary bone tumor (mesenchymal chondrosarcoma). (biomedcentral.com)
Cartilaginous1
- SC is a cartilaginous metaplasia of the mesenchymal remnants of the synovial tissue of the joints. (bvsalud.org)
Sarcomas1
- Dr. John Goldberg and Dr. Holcombe Grier give an informative introduction to one of the rarest sarcomas, mesenchymal chondrosarcoma. (sarcomahelp.org)
Soft-tissue1
- Malignant mesenchymoma, which was described by Stout in 1948, is defined as a malignant soft tissue tumor that consists of two or more distinctly different mesenchymal components in addition to fibrosarcomatous elements. (biomedcentral.com)
Epithelial1
- The tumor is composed of two cellular components: Epithelial and mesenchymal. (cytojournal.com)
20221
- The event is in memory of Matt Pfund who was 18 when he lost his 3-year battle, November 17, 2022, to a rare form of cancer, Mesenchymal chondrosarcoma. (washingtoncountyinsider.com)
Adult1
- Chondrosarcoma is more common in older adult males. (abta.org)
Orbit4
- Mesenchymal chondrosarcoma of the orbit is a exceedingly rare tumor. (e-crt.org)
- Seven mesenchyma1 chondrosarcoma of the orbit have been described in the literature. (e-crt.org)
- We report a case of 22-year old female patient with mesenchymal chondrosarcoma of the orbit. (e-crt.org)
- Extraskeletal mesenchymal chondrosarcoma (ESMC) may occur in any location that contains mesenchymal cells, however, the majority arise in the lower extremities (particularly the thigh), leptomeninges or the orbit (2). (docksci.com)
Osteosarcomas1
- Osteosarcomas are composed of mesenchymal cells that produce immature bone. (wikipedia.org)
Cancer3
- Bahareh was a 33-year old female member with mesenchymal chondrosarcoma, a form of cancer. (alcor.org)
- They selected a rare form of cancer, mesenchymal chondrosarcoma (MCS), which has not been well described and for which there is no effective treatment. (medindia.net)
- If your doctor suggests you have chondrosarcoma, then it means you have bone cancer. (healthadvicer.com)
Pelvis1
- Most chondrosarcomas develop in the pelvis, legs or arms. (wikipedia.org)
Lesions2
- In addition, the whole exon analysis results revealed isocitrate dehydrogenase 1 ( IDH1 ) R132C mutation in chondrosarcoma lesions but not in blood DNA. (biomedcentral.com)
- This case report showed MS complicated by giant chondrosarcoma in the left ankle with an IDH1 R132C mutation, which is appropriate to monitor the development of MS pathology and other concomitant lesions. (biomedcentral.com)
Findings2
- Mesenchymal chondrosarcoma: imaging features and clinical findings. (ocu-radiology.jp)
- 2008). This paper is about the macroscopic, surgical, radiological, and histopatholo-gical findings of chondrosarcoma in a cat. (ac.ir)
Clinical3
- 1999). "Clinical significance of genetic imbalances revealed by comparative genomic hybridization in chondrosarcomas" . (wikidoc.org)
- We present a case of a 45-year-old man with MS to supplement the clinical manifestations and explore the molecular mechanism of MS. The patient underwent amputation surgery to inhibit tumor development and was diagnosed with MS with 1-2 grade giant chondrosarcoma in the left ankle. (biomedcentral.com)
- Phase study of the tumor mutational burdenTtmb mutant IDH1 inhibitor ivosidenib: Safety and clinical activity in patients with advanced chondrosarcoma. (bvsalud.org)
Radiotherapy1
- Mesenchymal Mesenchymal chondrosarcomas can grow quickly but unlike other types may respond to radiotherapy, and chemotherapy. (wikipedia.org)
Radiation2
- Chondrosarcoma may recur and may need treatment with surgery , chemotherapy or radiation . (wikidoc.org)
- Standard treatment for chondrosarcoma is surgical removal, which may be followed by radiation therapy. (abta.org)
Clear2
- Clear cell Clear cell chondrosarcomas are rare, slow-growing, and seldom spread. (wikipedia.org)
- Clear cell chondrosarcoma: 70% survival rate at 5 years. (wikidoc.org)
Rare4
- Mesenchymal chondrosarcomas are extremely rare in comparison to conventional chondrosarcomas and even more so when arising in an extraskeletal location. (docksci.com)
- Chondrosarcoma of the hyoid bone is rare. (ajnr.org)
- Chondroma and chondrosarcoma are very rare. (abta.org)
- Reduction en masse of inguinal hernia is a rare condition following manual reduction of an unrecognized incarcerated inguinal hernia. (biomedcentral.com)
Cancerous1
- The malignant (cancerous) form of chondroma is chondrosarcoma. (abta.org)
Survival rate1
- Dedifferentiated chondrosarcoma: 10% survival rate after 1 year. (wikidoc.org)
Surgical1
- We present a case of chondrosarcoma of the hyoid bone with imaging, surgical, and pathologic correlation, and a review of the literature. (ajnr.org)
Involve1
- Chondrosarcoma may involve any part of the hyoid bone. (ajnr.org)
Commonly2
Grade3
- Chondrosarcomas are classified by grade as a measurement of their growth rate - I, II, and III. (wikipedia.org)
- Histopathologically, the neoplasm was composed of mature chondrocytes with minimal nuclear and cytoplasmic atypia compatible with grade I chondrosarcoma ( Fig 4 , Table ). (ajnr.org)
- Histopathology revealed grade 1 chondrosarcoma seen as mature chondrocytes with minimal nuclear and cytoplasmic atypia. (ajnr.org)
Cells3
- Mesenchymal stem cells (MSCs) possess great therapeutic potential. (hindawi.com)
- The chondrosarcoma has cells producing cartilage. (healthadvicer.com)
- Chondrosarcoma is an uncommon malignant neoplasm in which the neoplastic cells produce chondroid and fibrillar matrix (Durham, Popovitch, & Goldschmidt, 2008). (ac.ir)
Unlike1
- Unlike other cancers , chondrosarcoma can return many years later. (wikidoc.org)
Types1
- The chondrosarcoma is classified into different types. (healthadvicer.com)
Case report1
- Primary retroperitoneal extraskeletal mesenchymal chondrosarcoma involving the vena cava: A case report. (docksci.com)
Rarely1
- Chondrosarcoma can rarely metastatize to skin. (wikidoc.org)