Common Bile Duct Diseases
Bile Duct Diseases
Common Bile Duct
Bile Ducts
Gallstones
Common Bile Duct Neoplasms
Cholangiopancreatography, Endoscopic Retrograde
Cholangiography
Bile
Bile Ducts, Extrahepatic
Cholestasis
Cholestasis, Extrahepatic
Cholecystectomy, Laparoscopic
Sphincterotomy, Endoscopic
Bile Acids and Salts
Bile Ducts, Intrahepatic
Jaundice, Obstructive
Cholangiopancreatography, Magnetic Resonance
Sphincter of Oddi
Cholangitis
Cystic Duct
Cholelithiasis
Ampulla of Vater
Biliary Tract Diseases
Pancreatic Ducts
Hepatic Duct, Common
Gallbladder
Pancreatitis
Sphincterotomy, Transhepatic
Choledochal Cyst
Biliary Fistula
Choledochostomy
Endoscopes
Cholecystitis
Imino Acids
Gallbladder Diseases
Jaundice
Lithotripsy
Adenomyoma
Technetium Tc 99m Disofenin
Dilatation, Pathologic
Endoscopy
Cholestasis, Intrahepatic
Cholecystitis, Acute
Pancreaticoduodenectomy
Sphincter of Oddi Dysfunction
Jejunostomy
Duodenum
Liver
Postoperative Complications
Cholecystostomy
Bile Reflux
Endosonography
Liver Cirrhosis, Experimental
Constriction, Pathologic
Intraoperative Care
Catheterization
Liver Function Tests
Duodenal Diseases
Thoracic Duct
Calculi
Liver Cirrhosis, Biliary
Ascaridida
Surgical Instruments
Treatment Outcome
Lithiasis
Hepatopulmonary Syndrome
Colic
Intraoperative Complications
Pancreas
Retrospective Studies
Laparoscopy
Ursodeoxycholic Acid
Tomography, X-Ray Computed
Pancreatitis, Chronic
Anastomosis, Roux-en-Y
Diverticulum
Adenoma, Villous
Bile Canaliculi
Anastomosis, Surgical
Cholagogues and Choleretics
Postcholecystectomy Syndrome
Adenocarcinoma, Papillary
Fascioliasis
Preoperative Care
Obstructive jaundice and acute cholangitis due to papillary stenosis. (1/141)
Papillary stenosis is characterized by fixed fibrosis leading to structural outflow obstruction and it is usually secondary to inflammation and fibrosis from the chronic passage of gallstones, episodes of acute pancreatitis, chronic pancreatitis, sclerosing cholangitis, peptic ulcer disease, and cholesterolosis. However, obstructive jaundice with or without acute cholangitis which leads the physician to suspect the presence of malignancy as a cause is a rare manifestation of papillary stenosis. We report here a case of papillary stenosis presenting with obstructive jaundice and acute cholangitis. The lesion was so difficult to exclude the presence of malignancy preoperatively and intraoperatively that a pylorus-preserving pancreaticoduodenectomy was performed. Histologic examination of the resected specimen revealed fibrosis, adenomatoid ductal hyperplasia, and mild chronic inflammation of the papilla of Vater and distal common bile duct. (+info)Endoscopic retrograde cholangiopancreatography in elderly patients. (2/141)
BACKGROUND: the presentation of common bile duct disease, value of investigations and treatment outcome in elderly patients undergoing endoscopic retrograde cholangiopancreatography (ERCP) were assessed. METHODOLOGY: the clinical presentation, liver function tests, full blood counts, abdominal ultrasound and ERCP results were assessed retrospectively in 101 patients (59 women, 42 men; mean age 83 years, range 75-100) sequentially investigated for possible common bile duct disease. RESULTS: 59 patients had common bile duct gallstones, 35 had malignant biliary obstruction (13 with co-existing common bile duct stones) and seven had other outcomes. In the malignant-alone group 68% of those who had jaundice presented painlessly compared with 24% in the gallstones-alone group; 49% of the gallstones-alone group had pain compared with 28% of the malignant group. In the gallstones-alone group 43% had atypical presentations (non-specific symptoms or painless jaundice). Non-specific symptoms were found in 19% of the gallstones-alone group but in only 5% of the malignant group. Of the patients who had common bile duct stones, 18% had pancreatic or biliary malignancy. The co-existence of gallstones and malignancy was emphasized by eight patients in whom the clinical and ultrasound diagnosis was of common bile duct stones but malignancy was detected by ERCP. The sensitivity of ultrasound was 86% for detecting dilated common bile ducts was 86%, but only 69% for diagnosing gallstones within the common bile duct and 67% for diagnosing pancreatic masses. Ultrasound and ERCP were in agreement in 60 patients (60%). Endoscopic clearance of common bile duct gallstones was successful in 53 of 54 attempts (98%). Palliative ERCP treatment was performed in 30 patients who had malignant biliary obstruction and was successful in 22 (73%); in a further four patients (13%) an endoprothesis was successfully inserted percutaneously. The commonest complication of ERCP was cholangitis (four patients); pancreatitis and biliary perforation occurred in one patient each. Twenty-two patients (63%) who had malignancy died during follow-up, the mean survival being 11.3 weeks (range 3 days-2 years). Carcinoma of the ampulla was associated with a relatively good prognosis (three patients survived 18 months or more). CONCLUSION: in elderly patients, common bile duct stones often present atypically and co-existence with malignancy is not unusual; ampullary carcinoma has a relatively good prognosis and ERCP is a safe and effective procedure in the management of biliary obstruction. (+info)Functional disorders of the biliary tract and pancreas. (3/141)
The term "dysfunction" defines the motor disorders of the gall bladder and the sphincter of Oddi (SO) without note of the potential etiologic factors for the difficulty to differentiate purely functional alterations from subtle structural changes. Dysfunction of the gall bladder and/or SO produces similar patterns of biliopancreatic pain and SO dysfunction may occur in the presence of the gall bladder. The symptom-based diagnostic criteria of gall bladder and SO dysfunction are episodes of severe steady pain located in the epigastrium and right upper abdominal quadrant which last at least 30 minutes. Gall bladder and SO dysfunctions can cause significant clinical symptoms but do not explain many instances of biliopancreatic type of pain. The syndrome of functional abdominal pain should be differentiated from gall bladder and SO dysfunction. In the diagnostic workup, invasive investigations should be performed only in the presence of compelling clinical evidence and after non-invasive testing has yielded negative findings. Gall bladder dysfunction is suspected when laboratory, ultrasonographic, and microscopic bile examination have excluded the presence of gallstones and other structural abnormalities. The finding of decreased gall bladder emptying at cholecystokinin-cholescintigraphy is the only objective characteristic of gall bladder dysfunction. Symptomatic manifestation of SO dysfunction may be accompanied by features of biliary obstruction (biliary-type SO dysfunction) or significant elevation of pancreatic enzymes and pancreatitis (pancreatic-type SO dysfunction). Biliary-type SO dysfunction occurs more frequently in postcholecystectomy patients who are categorized into three types. Types I and II, but not type III, have biochemical and cholangiographic features of biliary obstruction. Pancreatic-type SO dysfunction is less well classified into types. When non-invasive investigations and endoscopic retrograde cholangiopanreatography show no structural abnormality, manometry of both biliary and pancreatic sphincter may be considered. (+info)Manometry based randomised trial of endoscopic sphincterotomy for sphincter of Oddi dysfunction. (4/141)
BACKGROUND: Endoscopic sphincterotomy for biliary-type pain after cholecystectomy remains controversial despite evidence of efficacy in some patients with a high sphincter of Oddi (SO) basal pressure (SO stenosis). AIM: To evaluate the effects of sphincterotomy in patients randomised on the basis of results from endoscopic biliary manometry. METHODS: Endoscopic biliary manometry was performed in 81 patients with biliary-type pain after cholecystectomy who had a dilated bile duct on retrograde cholangiography, transient increases in liver enzymes after episodes of pain, or positive responses to challenge with morphine/neostigmine. The manometric record was categorised as SO stenosis, SO dyskinesia, or normal, after which the patient was randomised in each category to sphincterotomy or to a sham procedure in a prospective double blind study. Symptoms were assessed at intervals of three months for 24 months by an independent observer, and the effects of sphincterotomy on sphincter function were monitored by repeat manometry after three and 24 months. RESULTS: In the SO stenosis group, symptoms improved in 11 of 13 patients treated by sphincterotomy and in five of 13 subjected to a sham procedure (p = 0.041). When manometric records were categorised as dyskinesia or normal, results from sphincterotomy and sham procedures did not differ. Complications were rare, but included mild pancreatitis in seven patients (14 episodes) and a collection in the right upper quadrant, presumably related to a minor perforation. At three months, the endoscopic incision was extended in 19 patients because of manometric evidence of incomplete division of the sphincter. CONCLUSION: In patients with presumed SO dysfunction, endoscopic sphincterotomy is helpful in those with manometric features of SO stenosis. (+info)Use of (99m)Tc-DISIDA biliary scanning with morphine provocation for the detection of elevated sphincter of Oddi basal pressure. (5/141)
BACKGROUND: Endoscopic biliary manometry is useful in the assessment of patients with types II and III sphincter of Oddi dysfunction, but it is time consuming and invasive. AIM: To investigate the role of (99m)Tc-DISIDA scanning, with and without morphine provocation, as a non-invasive investigation in these patients compared with endoscopic biliary manometry. SUBJECTS AND METHODS: A total of 34 patients with a clinical diagnosis of type II (n = 21) or III (n = 13) sphincter of Oddi dysfunction were studied. Biliary scintigraphy with 100 MBq of (99m)Tc-DISIDA was carried out with and without morphine provocation (0.04 mg/kg intravenously) and time/activity curves were compared with the results of subsequent endoscopic biliary manometry. RESULTS: Eighteen (nine type II, nine type III) of the 34 (53%) patients had sphincter of Oddi basal pressures above the upper limit of normal (40 mm Hg). In the standard DISIDA scan without morphine, no significant differences were observed in time to maximal activity (Tmax) or percentage excretion at 45 or 60 minutes between those with normal and those with abnormal biliary manometry. However, following morphine provocation, median percentage excretion at 60 minutes was 4.9% in those with abnormal manometry and 28.2% in the normal manometry group (p = 0.002). Using a cut off value of 15% excretion at 60 minutes, the sensitivity for detecting elevated sphincter of Oddi basal pressure by the morphine augmented DISIDA scan was 83% and specificity was 81%. Also, 14 of the 18 patients with abnormal manometry complained of biliary-type pain after morphine infusion compared with only two of 16 patients in the normal manometry group (p = 0.001). CONCLUSIONS: (99m)Tc-DISIDA with morphine provocation is a useful non-invasive investigation for types II and III sphincter of Oddi dysfunction to detect those with elevated sphincter basal pressures who may respond to endoscopic sphincterotomy. (+info)Biliary stenting versus bypass surgery for the palliation of malignant distal bile duct obstruction: a meta-analysis. (6/141)
The objective of this analysis is to compare endoscopic stenting with surgical bypass in patients with unresectable, malignant, distal common bile duct obstruction using the technique of meta-analysis. The inclusion criteria for the studies were randomized patient assignment, publication in the English language, 20 or more patients per group, all patients followed up until death, and follow-up and complications reported in an equivalent way for both treatment arms. Data extraction was performed independently by 2 of the authors. The number of treatment failures, serious complications, requirement for additional treatment sessions, and 30-day mortality were extracted. Three existing trials met the inclusion criteria, all of which compared surgery with the use of plastic stents. There were no studies identified that used metallic expandable stents. For the rate of treatment failure and serious complications, the odds ratios (ORs) of the 3 trials were heterogeneous, and no summary ORs were calculated. More treatment sessions were required after stent placement than after surgery, and a common OR was estimated to be 7.23 (95% confidence interval [CI], 3.73 to 13.98). Thirty-day mortality was not significantly different (OR = 0.522; 95% CI, 0.263 to 1.036). Although surgical bypass required fewer additional treatment sessions, existing data do not allow a definitive conclusion on which treatment is preferable. A larger randomized controlled trial using newer metallic stents and proper quality-of-life instruments is required. (+info)Repair of common bile duct injury with the round and falciform ligament after clip necrosis: case report. (7/141)
Occasionally, as abdominal surgeons, we are confronted with common bile duct injury noted during video laparoscopic or open cholecystectomy. Usually this is solved by endoscopic retrograde cholangiopancreatography (ERCP) sphincterotomy and stent, or enteric bypass, suture repair and tube drainage. However, after such procedures, there is a significant number of patients with postoperative stenosis. Another alternative to repair common bile duct injury and correct postoperative stenosis is using the round and falciform ligament as circumferencial patch. Due to their closeness to the common bile duct and their adequate blood supply, they make a perfect autologous biological graft. (+info)Vanishing bile duct syndrome in Hodgkin's disease: case report. (8/141)
CONTEXT: Liver damage is relatively common in patients affected by Hodgkin's disease. A smaller proportion of cases develops jaundice. Recently, the vanishing bile duct syndrome was described in Hodgkin's disease. The mechanisms of this severe complication have been poorly understood until now. OBJECTIVE: To describe a rare case of intra-hepatic cholestasis due to vanishing bile duct syndrome. DESIGN: Case report. CASE REPORT: A 38-year-old male patient affected by Hodgkin's disease. Liver biopsy showed no detectable Hodgkin's disease. Intra-hepatic cholestasis was found and none of the six portal tracts analyzed contained normal bile ducts. The treatment was based on conventional and high-dose escalation chemotherapy. The patient died from an irreversible liver failure while in complete remission from Hodgkin's disease. (+info)Common bile duct diseases refer to conditions that affect the common bile duct, a tube that carries bile from the liver and gallbladder into the small intestine. Some common examples of common bile duct diseases include:
1. Choledocholithiasis: This is the presence of stones (calculi) in the common bile duct, which can cause blockage, inflammation, and infection.
2. Cholangitis: This is an infection or inflammation of the common bile duct, often caused by obstruction due to stones, tumors, or strictures.
3. Common bile duct cancer (cholangiocarcinoma): This is a rare but aggressive cancer that arises from the cells lining the common bile duct.
4. Biliary strictures: These are narrowing or scarring of the common bile duct, which can be caused by injury, inflammation, or surgery.
5. Benign tumors: Non-cancerous growths in the common bile duct can also cause blockage and other symptoms.
Symptoms of common bile duct diseases may include abdominal pain, jaundice (yellowing of the skin and eyes), fever, chills, nausea, vomiting, and dark urine or light-colored stools. Treatment depends on the specific condition and severity but may include medications, endoscopic procedures, surgery, or a combination of these approaches.
Bile duct diseases refer to a group of medical conditions that affect the bile ducts, which are tiny tubes that carry bile from the liver to the gallbladder and small intestine. Bile is a digestive juice produced by the liver that helps break down fats in food.
There are several types of bile duct diseases, including:
1. Choledocholithiasis: This occurs when stones form in the common bile duct, causing blockage and leading to symptoms such as abdominal pain, jaundice, and fever.
2. Cholangitis: This is an infection of the bile ducts that can cause inflammation, pain, and fever. It can occur due to obstruction of the bile ducts or as a complication of other medical procedures.
3. Primary Biliary Cirrhosis (PBC): This is a chronic autoimmune disease that affects the bile ducts in the liver, causing inflammation and scarring that can lead to cirrhosis and liver failure.
4. Primary Sclerosing Cholangitis (PSC): This is another autoimmune disease that causes inflammation and scarring of the bile ducts, leading to liver damage and potential liver failure.
5. Bile Duct Cancer: Also known as cholangiocarcinoma, this is a rare form of cancer that affects the bile ducts and can cause jaundice, abdominal pain, and weight loss.
6. Benign Strictures: These are narrowing of the bile ducts that can occur due to injury, inflammation, or surgery, leading to blockage and potential infection.
Symptoms of bile duct diseases may include jaundice, abdominal pain, fever, itching, dark urine, and light-colored stools. Treatment depends on the specific condition and may involve medication, surgery, or other medical interventions.
The common bile duct is a duct that results from the union of the cystic duct (which drains bile from the gallbladder) and the common hepatic duct (which drains bile from the liver). The common bile duct transports bile, a digestive enzyme, from the liver and gallbladder to the duodenum, which is the first part of the small intestine.
The common bile duct runs through the head of the pancreas before emptying into the second part of the duodenum, either alone or in conjunction with the pancreatic duct, via a small opening called the ampulla of Vater. The common bile duct plays a crucial role in the digestion of fats by helping to break them down into smaller molecules that can be absorbed by the body.
Bile ducts are tubular structures that carry bile from the liver to the gallbladder for storage or directly to the small intestine to aid in digestion. There are two types of bile ducts: intrahepatic and extrahepatic. Intrahepatic bile ducts are located within the liver and drain bile from liver cells, while extrahepatic bile ducts are outside the liver and include the common hepatic duct, cystic duct, and common bile duct. These ducts can become obstructed or inflamed, leading to various medical conditions such as cholestasis, cholecystitis, and gallstones.
Gallstones are small, hard deposits that form in the gallbladder, a small organ located under the liver. They can range in size from as small as a grain of sand to as large as a golf ball. Gallstones can be made of cholesterol, bile pigments, or calcium salts, or a combination of these substances.
There are two main types of gallstones: cholesterol stones and pigment stones. Cholesterol stones are the most common type and are usually yellow-green in color. They form when there is too much cholesterol in the bile, which causes it to become saturated and form crystals that eventually grow into stones. Pigment stones are smaller and darker in color, ranging from brown to black. They form when there is an excess of bilirubin, a waste product produced by the breakdown of red blood cells, in the bile.
Gallstones can cause symptoms such as abdominal pain, nausea, vomiting, and bloating, especially after eating fatty foods. In some cases, gallstones can lead to serious complications, such as inflammation of the gallbladder (cholecystitis), infection, or blockage of the bile ducts, which can cause jaundice, a yellowing of the skin and eyes.
The exact cause of gallstones is not fully understood, but risk factors include being female, older age, obesity, a family history of gallstones, rapid weight loss, diabetes, and certain medical conditions such as cirrhosis or sickle cell anemia. Treatment for gallstones may involve medication to dissolve the stones, shock wave therapy to break them up, or surgery to remove the gallbladder.
Common bile duct neoplasms refer to abnormal growths that can occur in the common bile duct, which is a tube that carries bile from the liver and gallbladder into the small intestine. These growths can be benign or malignant (cancerous).
Benign neoplasms of the common bile duct include papillomas, adenomas, and leiomyomas. Malignant neoplasms are typically adenocarcinomas, which arise from the glandular cells lining the duct. Other types of malignancies that can affect the common bile duct include cholangiocarcinoma, gallbladder carcinoma, and metastatic cancer from other sites.
Symptoms of common bile duct neoplasms may include jaundice (yellowing of the skin and eyes), abdominal pain, dark urine, and light-colored stools. Diagnosis may involve imaging tests such as CT scans or MRCP (magnetic resonance cholangiopancreatography) and biopsy to confirm the type of neoplasm. Treatment options depend on the type and stage of the neoplasm and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Endoscopic retrograde cholangiopancreatography (ERCP) is a medical procedure that combines upper gastrointestinal (GI) endoscopy and fluoroscopy to diagnose and treat certain problems of the bile ducts and pancreas.
During ERCP, a flexible endoscope (a long, thin, lighted tube with a camera on the end) is passed through the patient's mouth and throat, then through the stomach and into the first part of the small intestine (duodenum). A narrow plastic tube (catheter) is then inserted through the endoscope and into the bile ducts and/or pancreatic duct. Contrast dye is injected through the catheter, and X-rays are taken to visualize the ducts.
ERCP can be used to diagnose a variety of conditions affecting the bile ducts and pancreas, including gallstones, tumors, strictures (narrowing of the ducts), and chronic pancreatitis. It can also be used to treat certain conditions, such as removing gallstones from the bile duct or placing stents to keep the ducts open in cases of stricture.
ERCP is an invasive procedure that carries a risk of complications, including pancreatitis, infection, bleeding, and perforation (a tear in the lining of the GI tract). It should only be performed by experienced medical professionals in a hospital setting.
Cholangiography is a medical procedure that involves taking X-ray images of the bile ducts (the tubes that carry bile from the liver to the small intestine). This is typically done by injecting a contrast dye into the bile ducts through an endoscope or a catheter that has been inserted into the body.
There are several types of cholangiography, including:
* Endoscopic retrograde cholangiopancreatography (ERCP): This procedure involves inserting an endoscope through the mouth and down the throat into the small intestine. A dye is then injected into the bile ducts through a small tube that is passed through the endoscope.
* Percutaneous transhepatic cholangiography (PTC): This procedure involves inserting a needle through the skin and into the liver to inject the contrast dye directly into the bile ducts.
* Operative cholangiography: This procedure is performed during surgery to examine the bile ducts for any abnormalities or blockages.
Cholangiography can help diagnose a variety of conditions that affect the bile ducts, such as gallstones, tumors, or inflammation. It can also be used to guide treatment decisions, such as whether surgery is necessary to remove a blockage.
Bile is a digestive fluid that is produced by the liver and stored in the gallbladder. It plays an essential role in the digestion and absorption of fats and fat-soluble vitamins in the small intestine. Bile consists of bile salts, bilirubin, cholesterol, phospholipids, electrolytes, and water.
Bile salts are amphipathic molecules that help to emulsify fats into smaller droplets, increasing their surface area and allowing for more efficient digestion by enzymes such as lipase. Bilirubin is a breakdown product of hemoglobin from red blood cells and gives bile its characteristic greenish-brown color.
Bile is released into the small intestine in response to food, particularly fats, entering the digestive tract. It helps to break down large fat molecules into smaller ones that can be absorbed through the walls of the intestines and transported to other parts of the body for energy or storage.
Choledocholithiasis is a medical condition characterized by the presence of one or more gallstones in the common bile duct, which is the tube that carries bile from the liver and gallbladder to the small intestine. Bile is a digestive fluid produced by the liver that helps break down fats in the small intestine. Gallstones are hardened deposits of digestive fluids that can form in the gallbladder or, less commonly, in the bile ducts.
Choledocholithiasis can cause a variety of symptoms, including abdominal pain, jaundice (yellowing of the skin and eyes), nausea, vomiting, and fever. If left untreated, it can lead to serious complications such as infection or inflammation of the bile ducts or pancreas, which can be life-threatening.
The condition is typically diagnosed through imaging tests such as ultrasound, CT scan, or MRI, and may require endoscopic or surgical intervention to remove the gallstones from the common bile duct.
Extrahepatic bile ducts refer to the portion of the biliary system that lies outside the liver. The biliary system is responsible for producing, storing, and transporting bile, a digestive fluid produced by the liver.
The extrahepatic bile ducts include:
1. The common hepatic duct: This duct is formed by the union of the right and left hepatic ducts, which drain bile from the corresponding lobes of the liver.
2. The cystic duct: This short duct connects the gallbladder to the common hepatic duct, allowing bile to flow into the gallbladder for storage and concentration.
3. The common bile duct: This is the result of the fusion of the common hepatic duct and the cystic duct. It transports bile from the liver and gallbladder to the duodenum, the first part of the small intestine, where it aids in fat digestion.
4. The ampulla of Vater (or hepatopancreatic ampulla): This is a dilated area where the common bile duct and the pancreatic duct join and empty their contents into the duodenum through a shared opening called the major duodenal papilla.
Extrahepatic bile ducts can be affected by various conditions, such as gallstones, inflammation (cholangitis), strictures, or tumors, which may require medical or surgical intervention.
Cholestasis is a medical condition characterized by the interruption or reduction of bile flow from the liver to the small intestine. Bile is a digestive fluid produced by the liver that helps in the breakdown and absorption of fats. When the flow of bile is blocked or reduced, it can lead to an accumulation of bile components, such as bilirubin, in the blood, which can cause jaundice, itching, and other symptoms.
Cholestasis can be caused by various factors, including liver diseases (such as hepatitis, cirrhosis, or cancer), gallstones, alcohol abuse, certain medications, pregnancy, and genetic disorders. Depending on the underlying cause, cholestasis may be acute or chronic, and it can range from mild to severe in its symptoms and consequences. Treatment for cholestasis typically involves addressing the underlying cause and managing the symptoms with supportive care.
Bile duct neoplasms, also known as cholangiocarcinomas, refer to a group of malignancies that arise from the bile ducts. These are the tubes that carry bile from the liver to the gallbladder and small intestine. Bile duct neoplasms can be further classified based on their location as intrahepatic (within the liver), perihilar (at the junction of the left and right hepatic ducts), or distal (in the common bile duct).
These tumors are relatively rare, but their incidence has been increasing in recent years. They can cause a variety of symptoms, including jaundice, abdominal pain, weight loss, and fever. The diagnosis of bile duct neoplasms typically involves imaging studies such as CT or MRI scans, as well as blood tests to assess liver function. In some cases, a biopsy may be necessary to confirm the diagnosis.
Treatment options for bile duct neoplasms depend on several factors, including the location and stage of the tumor, as well as the patient's overall health. Surgical resection is the preferred treatment for early-stage tumors, while chemotherapy and radiation therapy may be used in more advanced cases. For patients who are not candidates for surgery, palliative treatments such as stenting or bypass procedures may be recommended to relieve symptoms and improve quality of life.
Extrahepatic cholestasis is a medical condition characterized by the impaired flow of bile outside of the liver. Bile is a digestive fluid produced by the liver that helps in the absorption and digestion of fats. When the flow of bile is obstructed or blocked, it can lead to an accumulation of bile components, such as bilirubin, in the bloodstream, resulting in jaundice, dark urine, light-colored stools, and itching.
Extrahepatic cholestasis can be caused by various factors, including gallstones, tumors, strictures, or inflammation of the bile ducts. It is essential to diagnose and treat extrahepatic cholestasis promptly to prevent further complications, such as liver damage or infection. Treatment options may include medications, endoscopic procedures, or surgery, depending on the underlying cause of the condition.
Laparoscopic cholecystectomy is a surgical procedure to remove the gallbladder using a laparoscope, a thin tube with a camera, which allows the surgeon to view the internal structures on a video monitor. The surgery is performed through several small incisions in the abdomen, rather than a single large incision used in open cholecystectomy. This approach results in less postoperative pain, fewer complications, and shorter recovery time compared to open cholecystectomy.
The procedure is typically indicated for symptomatic gallstones or chronic inflammation of the gallbladder (cholecystitis), which can cause severe abdominal pain, nausea, vomiting, and fever. Laparoscopic cholecystectomy has become the standard of care for gallbladder removal due to its minimally invasive nature and excellent outcomes.
Cholecystectomy is a medical procedure to remove the gallbladder, a small pear-shaped organ located on the right side of the abdomen, just beneath the liver. The primary function of the gallbladder is to store and concentrate bile, a digestive fluid produced by the liver. During a cholecystectomy, the surgeon removes the gallbladder, usually due to the presence of gallstones or inflammation that can cause pain, infection, or other complications.
There are two primary methods for performing a cholecystectomy:
1. Open Cholecystectomy: In this traditional surgical approach, the surgeon makes an incision in the abdomen to access and remove the gallbladder. This method is typically used when there are complications or unique circumstances that make laparoscopic surgery difficult or risky.
2. Laparoscopic Cholecystectomy: This is a minimally invasive surgical procedure where the surgeon makes several small incisions in the abdomen, through which a thin tube with a camera (laparoscope) and specialized surgical instruments are inserted. The surgeon then guides these tools to remove the gallbladder while viewing the internal structures on a video monitor.
After the gallbladder is removed, bile flows directly from the liver into the small intestine through the common bile duct, and the body continues to function normally without any significant issues.
Endoscopic sphincterotomy is a medical procedure that involves the use of an endoscope (a flexible tube with a light and camera) to cut the papilla of Vater, which contains the sphincter of Oddi muscle. This procedure is typically performed to treat gallstones or to manage other conditions related to the bile ducts or pancreatic ducts.
The sphincterotomy helps to widen the opening of the papilla, allowing stones or other obstructions to pass through more easily. It may also be used to relieve pressure and pain caused by spasms of the sphincter of Oddi muscle. The procedure is usually done under sedation or anesthesia and carries a risk of complications such as bleeding, infection, perforation, and pancreatitis.
Bile acids and salts are naturally occurring steroidal compounds that play a crucial role in the digestion and absorption of lipids (fats) in the body. They are produced in the liver from cholesterol and then conjugated with glycine or taurine to form bile acids, which are subsequently converted into bile salts by the addition of a sodium or potassium ion.
Bile acids and salts are stored in the gallbladder and released into the small intestine during digestion, where they help emulsify fats, allowing them to be broken down into smaller molecules that can be absorbed by the body. They also aid in the elimination of waste products from the liver and help regulate cholesterol metabolism.
Abnormalities in bile acid synthesis or transport can lead to various medical conditions, such as cholestatic liver diseases, gallstones, and diarrhea. Therefore, understanding the role of bile acids and salts in the body is essential for diagnosing and treating these disorders.
Intrahepatic bile ducts are the small tubular structures inside the liver that collect bile from the liver cells (hepatocytes). Bile is a digestive fluid produced by the liver that helps in the absorption of fats and fat-soluble vitamins from food. The intrahepatic bile ducts merge to form larger ducts, which eventually exit the liver and join with the cystic duct from the gallbladder to form the common bile duct. The common bile duct then empties into the duodenum, the first part of the small intestine, where bile aids in digestion. Intrahepatic bile ducts can become obstructed or damaged due to various conditions such as gallstones, tumors, or inflammation, leading to complications like jaundice, liver damage, and infection.
Obstructive Jaundice is a medical condition characterized by the yellowing of the skin, sclera (whites of the eyes), and mucous membranes due to the accumulation of bilirubin in the bloodstream. This occurs when there is an obstruction or blockage in the bile ducts that transport bile from the liver to the small intestine.
Bile, which contains bilirubin, aids in digestion and is usually released from the liver into the small intestine. When the flow of bile is obstructed, bilirubin builds up in the blood, causing jaundice. The obstruction can be caused by various factors, such as gallstones, tumors, or strictures in the bile ducts.
Obstructive jaundice may present with additional symptoms like dark urine, light-colored stools, itching, abdominal pain, and weight loss, depending on the cause and severity of the obstruction. It is essential to seek medical attention if jaundice is observed, as timely diagnosis and management can prevent potential complications, such as liver damage or infection.
Magnetic resonance cholangiopancreatography (MRCP) is a non-invasive medical imaging technique that uses magnetic resonance imaging (MRI) to visualize the bile ducts and pancreatic duct. This diagnostic test does not use radiation like other imaging techniques such as computed tomography (CT) scans or endoscopic retrograde cholangiopancreatography (ERCP).
During an MRCP, the patient lies on a table that slides into the MRI machine. Contrast agents may be used to enhance the visibility of the ducts. The MRI machine uses a strong magnetic field and radio waves to produce detailed images of the internal structures, allowing radiologists to assess any abnormalities or blockages in the bile and pancreatic ducts.
MRCP is often used to diagnose conditions such as gallstones, tumors, inflammation, or strictures in the bile or pancreatic ducts. It can also be used to monitor the effectiveness of treatments for these conditions. However, it does not allow for therapeutic interventions like ERCP, which can remove stones or place stents.
The Sphincter of Oddi is a muscular valve that controls the flow of bile and pancreatic juice from the pancreatic and bile ducts into the duodenum, which is the first part of the small intestine. It is named after Ruggero Oddi, an Italian physiologist who discovered it in 1887. The Sphincter of Oddi has two parts: the sphincter papillae, which surrounds the common opening of the pancreatic and bile ducts into the duodenum, and the sphincter choledochus, which is located more proximally in the bile duct. The contraction and relaxation of these muscles help regulate the release of digestive enzymes from the pancreas and the flow of bile from the liver to aid in digestion.
Cholangitis is a medical condition characterized by inflammation of the bile ducts, which are the tubes that carry bile from the liver to the small intestine. Bile is a digestive juice produced by the liver that helps break down fats in food.
There are two types of cholangitis: acute and chronic. Acute cholangitis is a sudden and severe infection that can cause symptoms such as abdominal pain, fever, jaundice (yellowing of the skin and eyes), and dark urine. It is usually caused by a bacterial infection that enters the bile ducts through a blockage or obstruction.
Chronic cholangitis, on the other hand, is a long-term inflammation of the bile ducts that can lead to scarring and narrowing of the ducts. This can cause symptoms such as abdominal pain, itching, and jaundice. Chronic cholangitis can be caused by various factors, including primary sclerosing cholangitis (an autoimmune disease), bile duct stones, or tumors in the bile ducts.
Treatment for cholangitis depends on the underlying cause of the condition. Antibiotics may be used to treat bacterial infections, and surgery may be necessary to remove blockages or obstructions in the bile ducts. In some cases, medications may be prescribed to manage symptoms and prevent further complications.
The cystic duct is a short tube that connects the gallbladder to the common bile duct, which carries bile from the liver and gallbladder into the small intestine. The cystic duct allows bile to flow from the gallbladder into the common bile duct when it is needed for digestion. It is a part of the biliary system and plays an important role in the digestive process.
Cholelithiasis is a medical term that refers to the presence of gallstones in the gallbladder. The gallbladder is a small pear-shaped organ located beneath the liver that stores bile, a digestive fluid produced by the liver. Gallstones are hardened deposits that can form in the gallbladder when substances in the bile, such as cholesterol or bilirubin, crystallize.
Gallstones can vary in size and may be as small as a grain of sand or as large as a golf ball. Some people with gallstones may not experience any symptoms, while others may have severe abdominal pain, nausea, vomiting, fever, and jaundice (yellowing of the skin and eyes) if the gallstones block the bile ducts.
Cholelithiasis is a common condition that affects millions of people worldwide, particularly women over the age of 40 and those with certain medical conditions such as obesity, diabetes, and rapid weight loss. If left untreated, gallstones can lead to serious complications such as inflammation of the gallbladder (cholecystitis), infection, or pancreatitis (inflammation of the pancreas). Treatment options for cholelithiasis include medication, shock wave lithotripsy (breaking up the gallstones with sound waves), and surgery to remove the gallbladder (cholecystectomy).
The ampulla of Vater, also known as hepatopancreatic ampulla, is a dilated portion of the common bile duct where it joins the main pancreatic duct and empties into the second part of the duodenum. It serves as a conduit for both bile from the liver and digestive enzymes from the pancreas to reach the small intestine, facilitating the digestion and absorption of nutrients. The ampulla of Vater is surrounded by a muscular sphincter, the sphincter of Oddi, which controls the flow of these secretions into the duodenum.
Biliary tract diseases refer to a group of medical conditions that affect the biliary system, which includes the gallbladder, bile ducts, and liver. Bile is a digestive juice produced by the liver, stored in the gallbladder, and released into the small intestine through the bile ducts to help digest fats.
Biliary tract diseases can cause various symptoms such as abdominal pain, jaundice, fever, nausea, vomiting, and changes in stool color. Some of the common biliary tract diseases include:
1. Gallstones: Small, hard deposits that form in the gallbladder or bile ducts made up of cholesterol or bilirubin.
2. Cholecystitis: Inflammation of the gallbladder, often caused by gallstones.
3. Cholangitis: Infection or inflammation of the bile ducts.
4. Biliary dyskinesia: A motility disorder that affects the contraction and relaxation of the muscles in the biliary system.
5. Primary sclerosing cholangitis: A chronic autoimmune disease that causes scarring and narrowing of the bile ducts.
6. Biliary tract cancer: Rare cancers that affect the gallbladder, bile ducts, or liver.
Treatment for biliary tract diseases varies depending on the specific condition and severity but may include medications, surgery, or a combination of both.
The pancreatic ducts are a set of tubular structures within the pancreas that play a crucial role in the digestive system. The main pancreatic duct, also known as the duct of Wirsung, is responsible for transporting pancreatic enzymes and bicarbonate-rich fluid from the pancreas to the duodenum, which is the first part of the small intestine.
The exocrine portion of the pancreas contains numerous smaller ducts called interlobular ducts and intralobular ducts that merge and ultimately join the main pancreatic duct. This system ensures that the digestive enzymes and fluids produced by the pancreas are effectively delivered to the small intestine, where they aid in the breakdown and absorption of nutrients from food.
In addition to the main pancreatic duct, there is an accessory pancreatic duct, also known as Santorini's duct, which can sometimes join the common bile duct before emptying into the duodenum through a shared opening called the ampulla of Vater. However, in most individuals, the accessory pancreatic duct usually drains into the main pancreatic duct before entering the duodenum.
The common hepatic duct is a medical term that refers to the duct in the liver responsible for carrying bile from the liver. More specifically, it is the duct that results from the convergence of the right and left hepatic ducts, which themselves carry bile from the right and left lobes of the liver, respectively. The common hepatic duct then joins with the cystic duct from the gallbladder to form the common bile duct, which ultimately drains into the duodenum, a part of the small intestine.
The primary function of the common hepatic duct is to transport bile, a digestive juice produced by the liver, to the small intestine. Bile helps break down fats during the digestion process, making it possible for the body to absorb them properly. Any issues or abnormalities in the common hepatic duct can lead to problems with bile flow and potentially cause health complications such as jaundice, gallstones, or liver damage.
The biliary tract is a system of ducts that transport bile from the liver to the gallbladder and then to the small intestine. Bile is a digestive fluid produced by the liver that helps in the breakdown and absorption of fats in the small intestine. The main components of the biliary tract are:
1. Intrahepatic bile ducts: These are the smaller branches of bile ducts located within the liver that collect bile from the liver cells or hepatocytes.
2. Gallbladder: A small pear-shaped organ located beneath the liver, which stores and concentrates bile received from the intrahepatic bile ducts. The gallbladder releases bile into the small intestine when food is ingested, particularly fats, to aid digestion.
3. Common hepatic duct: This is a duct that forms by the union of the right and left hepatic ducts, which carry bile from the right and left lobes of the liver, respectively.
4. Cystic duct: A short duct that connects the gallbladder to the common hepatic duct, forming the beginning of the common bile duct.
5. Common bile duct: This is a larger duct formed by the union of the common hepatic duct and the cystic duct. It carries bile from the liver and gallbladder into the small intestine.
6. Pancreatic duct: A separate duct that originates from the pancreas, a gland located near the liver and stomach. The pancreatic duct joins the common bile duct just before they both enter the duodenum, the first part of the small intestine.
7. Ampulla of Vater: This is the dilated portion where the common bile duct and the pancreatic duct join together and empty their contents into the duodenum through a shared opening called the papilla of Vater.
Disorders related to the biliary tract include gallstones, cholecystitis (inflammation of the gallbladder), bile duct stones, bile duct strictures or obstructions, and primary sclerosing cholangitis, among others.
Ligation, in the context of medical terminology, refers to the process of tying off a part of the body, usually blood vessels or tissue, with a surgical suture or another device. The goal is to stop the flow of fluids such as blood or other substances within the body. It is commonly used during surgeries to control bleeding or to block the passage of fluids, gases, or solids in various parts of the body.
The gallbladder is a small, pear-shaped organ located just under the liver in the right upper quadrant of the abdomen. Its primary function is to store and concentrate bile, a digestive enzyme produced by the liver, which helps in the breakdown of fats during the digestion process. When food, particularly fatty foods, enter the stomach and small intestine, the gallbladder contracts and releases bile through the common bile duct into the duodenum, the first part of the small intestine, to aid in fat digestion.
The gallbladder is made up of three main parts: the fundus, body, and neck. It has a muscular wall that allows it to contract and release bile. Gallstones, an inflammation of the gallbladder (cholecystitis), or other gallbladder diseases can cause pain, discomfort, and potentially serious health complications if left untreated.
Pancreatitis is a medical condition characterized by inflammation of the pancreas, a gland located in the abdomen that plays a crucial role in digestion and regulating blood sugar levels. The inflammation can be acute (sudden and severe) or chronic (persistent and recurring), and it can lead to various complications if left untreated.
Acute pancreatitis often results from gallstones or excessive alcohol consumption, while chronic pancreatitis may be caused by long-term alcohol abuse, genetic factors, autoimmune conditions, or metabolic disorders like high triglyceride levels. Symptoms of acute pancreatitis include severe abdominal pain, nausea, vomiting, fever, and increased heart rate, while chronic pancreatitis may present with ongoing abdominal pain, weight loss, diarrhea, and malabsorption issues due to impaired digestive enzyme production. Treatment typically involves supportive care, such as intravenous fluids, pain management, and addressing the underlying cause. In severe cases, hospitalization and surgery may be necessary.
Transhepatic sphincterotomy is a medical procedure that involves the incision or cutting of the papilla of Vater, which is a small muscular structure located at the junction of the common bile duct and the main pancreatic duct, with the ampulla of Vater, within the second part of the duodenum. This procedure is performed using a special type of endoscope that is passed through the liver (transhepatically) to access the bile ducts.
The goal of transhepatic sphincterotomy is to relieve obstructions or blockages in the bile ducts, such as gallstones or tumors, that cannot be removed using other endoscopic techniques. This procedure is typically performed by an interventional radiologist or a gastroenterologist with specialized training in endoscopic retrograde cholangiopancreatography (ERCP).
Transhepatic sphincterotomy is considered a higher-risk procedure than traditional ERCP sphincterotomy due to the need for liver puncture and the potential complications associated with this approach, including bleeding, infection, and injury to surrounding organs. However, it may be necessary in certain situations where traditional ERCP is not feasible or has failed.
A Choledochal cyst is a congenital dilatation or abnormal enlargement of the bile ducts, which are the tubes that carry bile from the liver to the small intestine. Bile is a digestive juice produced by the liver that helps in the digestion of fats.
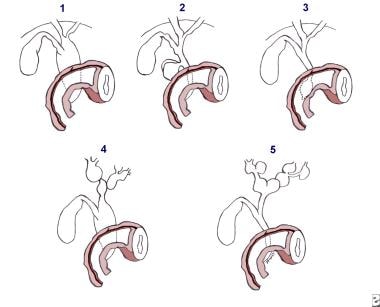
Choledochal cysts can be classified into several types based on their location and the anatomy of the biliary tree. The most common type, called Type I, involves dilatation of the common bile duct. Other types include dilatation of the intrahepatic bile ducts (Type II), dilatation of both the intrahepatic and extrahepatic bile ducts (Type III), and multiple cystic dilatations of the bile ducts (Type IV).
Choledochal cysts are more common in females than males, and they can present at any age. Symptoms may include abdominal pain, jaundice, vomiting, and fever. Complications of choledochal cysts can include bile duct stones, infection, and cancer. Treatment typically involves surgical removal of the cyst, followed by reconstruction of the biliary tree.
A biliary fistula is an abnormal connection or passage between the biliary system (which includes the gallbladder, bile ducts, and liver) and another organ or structure, usually in the abdominal cavity. This connection allows bile, which is a digestive fluid produced by the liver, to leak out of its normal pathway and into other areas of the body.
Biliary fistulas can occur as a result of trauma, surgery, infection, or inflammation in the biliary system. Symptoms may include abdominal pain, fever, jaundice (yellowing of the skin and eyes), nausea, vomiting, and clay-colored stools. Treatment typically involves addressing the underlying cause of the fistula, such as draining an infection or repairing damaged tissue, and diverting bile flow away from the site of the leak. In some cases, surgery may be necessary to repair the fistula.
Biliary tract surgical procedures refer to a range of operations that involve the biliary system, which includes the liver, gallbladder, and bile ducts. These procedures can be performed for various reasons, including the treatment of gallstones, bile duct injuries, tumors, or other conditions affecting the biliary tract. Here are some examples of biliary tract surgical procedures:
1. Cholecystectomy: This is the surgical removal of the gallbladder, which is often performed to treat symptomatic gallstones or chronic cholecystitis (inflammation of the gallbladder). It can be done as an open procedure or laparoscopically.
2. Bile duct exploration: This procedure involves opening the common bile duct to remove stones, strictures, or tumors. It is often performed during a cholecystectomy if there is suspicion of common bile duct involvement.
3. Hepaticojejunostomy: This operation connects the liver's bile ducts directly to a portion of the small intestine called the jejunum, bypassing a damaged or obstructed segment of the biliary tract. It is often performed for benign or malignant conditions affecting the bile ducts.
4. Roux-en-Y hepaticojejunostomy: This procedure involves creating a Y-shaped limb of jejunum and connecting it to the liver's bile ducts, bypassing the common bile duct and duodenum. It is often performed for complex biliary tract injuries or malignancies.
5. Whipple procedure (pancreaticoduodenectomy): This extensive operation involves removing the head of the pancreas, the duodenum, a portion of the jejunum, the gallbladder, and the common bile duct. It is performed for malignancies involving the pancreas, bile duct, or duodenum.
6. Liver resection: This procedure involves removing a portion of the liver to treat primary liver tumors (hepatocellular carcinoma or cholangiocarcinoma) or metastatic cancer from other organs.
7. Biliary stenting or bypass: These minimally invasive procedures involve placing a stent or creating a bypass to relieve bile duct obstructions caused by tumors, strictures, or stones. They can be performed endoscopically (ERCP) or percutaneously (PTC).
8. Cholecystectomy: This procedure involves removing the gallbladder, often for symptomatic cholelithiasis (gallstones) or cholecystitis (inflammation of the gallbladder). It can be performed laparoscopically or open.
9. Biliary drainage: This procedure involves placing a catheter to drain bile from the liver or bile ducts, often for acute or chronic obstructions caused by tumors, strictures, or stones. It can be performed endoscopically (ERCP) or percutaneously (PTC).
10. Bilioenteric anastomosis: This procedure involves connecting the biliary tract to a portion of the small intestine, often for benign or malignant conditions affecting the bile ducts or pancreas. It can be performed open or laparoscopically.
Choledochostomy is a surgical procedure that involves creating an opening (stoma) into the common bile duct, which carries bile from the liver and gallbladder to the small intestine. This procedure is typically performed to relieve obstructions or blockages in the bile duct, such as those caused by gallstones, tumors, or scar tissue.
During the choledochostomy procedure, a surgeon makes an incision in the abdomen and exposes the common bile duct. The duct is then cut open, and a small tube (catheter) is inserted into the duct to allow bile to drain out of the body. The catheter may be left in place temporarily or permanently, depending on the underlying condition causing the obstruction.
Choledochostomy is typically performed as an open surgical procedure, but it can also be done using minimally invasive techniques such as laparoscopy or robotic-assisted surgery. As with any surgical procedure, choledochostomy carries risks such as bleeding, infection, and damage to surrounding tissues. However, these risks are generally low in the hands of an experienced surgeon.
Adenoma of the bile duct is a benign (noncancerous) tumor that develops in the bile ducts, which are tiny tubes that carry bile from the liver to the gallbladder and small intestine. Bile is a digestive fluid produced by the liver.
Bile duct adenomas are rare and usually do not cause any symptoms. However, if they grow large enough, they may obstruct the flow of bile and cause jaundice (yellowing of the skin and whites of the eyes), abdominal pain, or itching. In some cases, bile duct adenomas may become cancerous and develop into bile duct carcinomas.
The exact cause of bile duct adenomas is not known, but they are more common in people with certain genetic disorders, such as Gardner's syndrome and von Hippel-Lindau disease. Treatment for bile duct adenomas typically involves surgical removal of the tumor.
Drainage, in medical terms, refers to the removal of excess fluid or accumulated collections of fluids from various body parts or spaces. This is typically accomplished through the use of medical devices such as catheters, tubes, or drains. The purpose of drainage can be to prevent the buildup of fluids that may cause discomfort, infection, or other complications, or to treat existing collections of fluid such as abscesses, hematomas, or pleural effusions. Drainage may also be used as a diagnostic tool to analyze the type and composition of the fluid being removed.
An endoscope is a medical device used for examining the interior of a body cavity or organ. It consists of a long, thin, flexible (or rigid) tube with a light and a camera at one end. The other end is connected to a video monitor that displays the images captured by the camera. Endoscopes can be inserted through natural openings in the body, such as the mouth or anus, or through small incisions. They are used for diagnostic purposes, as well as for performing various medical procedures, including biopsies and surgeries. Different types of endoscopes include gastroscopes, colonoscopes, bronchoscopes, and arthroscopes, among others.
Duodenoscopy is a medical procedure that involves the insertion of a duodenoscope, which is a flexible, lighted tube with a camera and tiny tools on the end, through the mouth and down the throat to examine the upper part of the small intestine (duodenum) and the opening of the bile and pancreatic ducts.
During the procedure, the doctor can take tissue samples for biopsy, remove polyps or other abnormal growths, or perform other interventions as needed. Duodenoscopy is commonly used to diagnose and treat conditions such as gastrointestinal bleeding, inflammation, infection, and cancer.
It's important to note that duodenoscopes have been associated with the spread of antibiotic-resistant bacteria in some cases, so healthcare providers must follow strict cleaning and disinfection protocols to minimize this risk.
Cholecystitis is a medical condition characterized by inflammation of the gallbladder, a small pear-shaped organ located under the liver that stores and concentrates bile produced by the liver. Bile is a digestive fluid that helps break down fats in the small intestine during digestion.
Acute cholecystitis is a sudden inflammation of the gallbladder, often caused by the presence of gallstones that block the cystic duct, the tube that carries bile from the gallbladder to the common bile duct. This blockage can cause bile to build up in the gallbladder, leading to inflammation, swelling, and pain.
Chronic cholecystitis is a long-term inflammation of the gallbladder, often caused by repeated attacks of acute cholecystitis or the presence of gallstones that cause ongoing irritation and damage to the gallbladder wall. Over time, chronic cholecystitis can lead to thickening and scarring of the gallbladder wall, which can reduce its ability to function properly.
Symptoms of cholecystitis may include sudden and severe abdominal pain, often in the upper right or center of the abdomen, that may worsen after eating fatty foods; fever; nausea and vomiting; bloating and gas; and clay-colored stools. Treatment for cholecystitis typically involves antibiotics to treat any infection present, pain relief, and surgery to remove the gallbladder (cholecystectomy). In some cases, a nonsurgical procedure called endoscopic retrograde cholangiopancreatography (ERCP) may be used to remove gallstones from the bile duct.
Imino acids are organic compounds that contain a nitrogen atom as part of an amide-like structure. They are structurally similar to amino acids, which contain a carboxyl group and an amino group, but instead of the amino group, imino acids have a structural unit known as an imine or Schiff base, which is a carbon-nitrogen double bond with a hydrogen atom attached to the nitrogen atom.
One example of an imino acid is proline, which is a cyclic imino acid that plays important roles in protein structure and function. Proline is unique among the 20 standard amino acids because its side chain is linked to the nitrogen atom of the backbone, forming a ring-like structure. This structural feature gives proline unique properties, such as restricted rotation around the bond between the nitrogen and alpha carbon atoms, which can affect protein folding and stability.
Other imino acids may be formed through chemical reactions or enzymatic processes, and they can play important roles in various biological pathways, including the biosynthesis of amino acids, nucleotides, and other biomolecules. However, imino acids are not typically considered to be part of the standard set of 20 amino acids that make up proteins.
Gallbladder diseases refer to a range of conditions that affect the function and structure of the gallbladder, a small pear-shaped organ located beneath the liver. The primary role of the gallbladder is to store, concentrate, and release bile into the small intestine to aid in digesting fats. Gallbladder diseases can be chronic or acute and may cause various symptoms, discomfort, or complications if left untreated. Here are some common gallbladder diseases with brief definitions:
1. Cholelithiasis: The presence of gallstones within the gallbladder. Gallstones are small, hard deposits made of cholesterol, bilirubin, or a combination of both, which can vary in size from tiny grains to several centimeters.
2. Cholecystitis: Inflammation of the gallbladder, often caused by obstruction of the cystic duct (the tube connecting the gallbladder and the common bile duct) due to a gallstone. This condition can be acute or chronic and may cause abdominal pain, fever, and tenderness in the right upper quadrant of the abdomen.
3. Choledocholithiasis: The presence of gallstones within the common bile duct, which can lead to obstruction, jaundice, and potential infection of the biliary system (cholangitis).
4. Acalculous gallbladder disease: Gallbladder dysfunction or inflammation without the presence of gallstones. This condition is often seen in critically ill patients and can lead to similar symptoms as cholecystitis.
5. Gallbladder polyps: Small growths attached to the inner wall of the gallbladder. While most polyps are benign, some may have malignant potential, especially if they are larger than 1 cm in size or associated with certain risk factors.
6. Gallbladder cancer: A rare form of cancer that originates in the gallbladder tissue. It is often asymptomatic in its early stages and can be challenging to diagnose. Symptoms may include abdominal pain, jaundice, or a palpable mass in the right upper quadrant of the abdomen.
It is essential to consult with a healthcare professional if experiencing symptoms related to gallbladder disease for proper diagnosis and treatment.
Jaundice is a medical condition characterized by the yellowing of the skin, sclera (whites of the eyes), and mucous membranes due to an excess of bilirubin in the bloodstream. Bilirubin is a yellow-orange pigment produced when hemoglobin from red blood cells is broken down. Normally, bilirubin is processed by the liver and excreted through bile into the digestive system. However, if there's an issue with bilirubin metabolism or elimination, it can accumulate in the body, leading to jaundice.
Jaundice can be a symptom of various underlying conditions, such as liver diseases (hepatitis, cirrhosis), gallbladder issues (gallstones, tumors), or blood disorders (hemolysis). It is essential to consult a healthcare professional if jaundice is observed, as it may indicate a severe health problem requiring prompt medical attention.
Lithotripsy is a medical procedure that uses shock waves or other high-energy sound waves to break down and remove calculi (stones) in the body, particularly in the kidneys, ureters, or gallbladder. The procedure is typically performed on an outpatient basis and does not require any incisions.
During lithotripsy, the patient lies on a cushioned table while a lithotripter, a device that generates shock waves, is positioned around the area of the stone. As the shock waves pass through the body, they break the stone into tiny fragments that can then be easily passed out of the body in urine.
Lithotripsy is generally a safe and effective procedure, but it may not be suitable for everyone. Patients with certain medical conditions, such as bleeding disorders or pregnancy, may not be able to undergo lithotripsy. Additionally, some stones may be too large or too dense to be effectively treated with lithotripsy. In these cases, other treatment options, such as surgery, may be necessary.
Adenomyoma is a benign (non-cancerous) growth that occurs when the glands and muscle tissue from the lining of the uterus (endometrium) become embedded in the muscular wall of the uterus (myometrium). This condition most commonly affects women in their 40s and 50s, and it can cause symptoms such as heavy menstrual bleeding, painful periods, and pelvic pain or discomfort.
The term "adenomyoma" is derived from two words: "adeno," which means gland, and "myoma," which refers to a benign muscle tumor. Therefore, an adenomyoma can be thought of as a benign growth that contains both glandular tissue and muscle tissue.
Adenomyomas are typically found in the lower part of the uterus, near the cervix, and they can vary in size from small nodules to larger masses. In some cases, adenomyomas may cause no symptoms at all, while in other cases, they can lead to significant discomfort and pain.
The exact cause of adenomyoma is not fully understood, but it is thought to be related to hormonal factors, as well as trauma or injury to the uterus. Treatment options for adenomyoma may include medication to manage symptoms, such as pain relievers or hormone therapy, or surgical intervention, such as a hysterectomy (removal of the uterus).
Technetium Tc 99m Disofenin is not a medical condition, but rather a radiopharmaceutical used in diagnostic imaging. It is a radioactive tracer used in nuclear medicine scans, specifically for liver and biliary system imaging. The compound consists of the radioisotope Technetium-99m (Tc-99m) bonded to the pharmaceutical Disofenin.
The Tc-99m is a gamma emitter with a half-life of 6 hours, making it ideal for diagnostic imaging. When administered to the patient, the compound is taken up by the liver and excreted into the bile ducts and gallbladder, allowing medical professionals to visualize these structures using a gamma camera. This can help detect various conditions such as tumors, gallstones, or obstructions in the biliary system.
It's important to note that Technetium Tc 99m Disofenin is used diagnostically and not for therapeutic purposes. The radiation exposure from this compound is generally low and considered safe for diagnostic use. However, as with any medical procedure involving radiation, the benefits and risks should be carefully weighed and discussed with a healthcare professional.
Pathologic dilatation refers to an abnormal and excessive widening or enlargement of a body cavity or organ, which can result from various medical conditions. This abnormal dilation can occur in different parts of the body, including the blood vessels, digestive tract, airways, or heart chambers.
In the context of the cardiovascular system, pathologic dilatation may indicate a weakening or thinning of the heart muscle, leading to an enlarged chamber that can no longer pump blood efficiently. This condition is often associated with various heart diseases, such as cardiomyopathy, valvular heart disease, or long-standing high blood pressure.
In the gastrointestinal tract, pathologic dilatation may occur due to mechanical obstruction, neuromuscular disorders, or inflammatory conditions that affect the normal motility of the intestines. Examples include megacolon in Hirschsprung's disease, toxic megacolon in ulcerative colitis, or volvulus (twisting) of the bowel.
Pathologic dilatation can lead to various complications, such as reduced organ function, impaired circulation, and increased risk of infection or perforation. Treatment depends on the underlying cause and may involve medications, surgery, or other interventions to address the root problem and prevent further enlargement.
Endoscopy of the digestive system, also known as gastrointestinal (GI) endoscopy, is a medical procedure that allows healthcare professionals to visually examine the inside lining of the digestive tract using a flexible tube with a light and camera attached to it, called an endoscope. This procedure can help diagnose and treat various conditions affecting the digestive system, including gastroesophageal reflux disease (GERD), ulcers, inflammatory bowel disease (IBD), and cancer.
There are several types of endoscopy procedures that focus on different parts of the digestive tract:
1. Esophagogastroduodenoscopy (EGD): This procedure examines the esophagus, stomach, and duodenum (the first part of the small intestine). It is often used to investigate symptoms such as difficulty swallowing, abdominal pain, or bleeding in the upper GI tract.
2. Colonoscopy: This procedure explores the large intestine (colon) and rectum. It is commonly performed to screen for colon cancer, as well as to diagnose and treat conditions like inflammatory bowel disease, diverticulosis, or polyps.
3. Sigmoidoscopy: Similar to a colonoscopy, this procedure examines the lower part of the colon (sigmoid colon) and rectum. It is often used as a screening tool for colon cancer and to investigate symptoms like rectal bleeding or changes in bowel habits.
4. Upper GI endoscopy: This procedure focuses on the esophagus, stomach, and duodenum, using a thin, flexible tube with a light and camera attached to it. It is used to diagnose and treat conditions such as GERD, ulcers, and difficulty swallowing.
5. Capsule endoscopy: This procedure involves swallowing a small capsule containing a camera that captures images of the digestive tract as it passes through. It can help diagnose conditions in the small intestine that may be difficult to reach with traditional endoscopes.
Endoscopy is typically performed under sedation or anesthesia to ensure patient comfort during the procedure. The images captured by the endoscope are displayed on a monitor, allowing the healthcare provider to assess the condition of the digestive tract and make informed treatment decisions.
Endoscopy is a medical procedure that involves the use of an endoscope, which is a flexible tube with a light and camera at the end, to examine the interior of a body cavity or organ. The endoscope is inserted through a natural opening in the body, such as the mouth or anus, or through a small incision. The images captured by the camera are transmitted to a monitor, allowing the physician to visualize the internal structures and detect any abnormalities, such as inflammation, ulcers, or tumors. Endoscopy can also be used for diagnostic purposes, such as taking tissue samples for biopsy, or for therapeutic purposes, such as removing polyps or performing minimally invasive surgeries.
Gallbladder neoplasms refer to abnormal growths in the tissue of the gallbladder, which can be benign or malignant. Benign neoplasms are non-cancerous and typically do not spread to other parts of the body. Malignant neoplasms, also known as gallbladder cancer, can invade nearby tissues and organs and may metastasize (spread) to distant parts of the body. Gallbladder neoplasms can cause symptoms such as abdominal pain, jaundice, and nausea, but they are often asymptomatic until they have advanced to an advanced stage. The exact causes of gallbladder neoplasms are not fully understood, but risk factors include gallstones, chronic inflammation of the gallbladder, and certain inherited genetic conditions.
Intrahepatic cholestasis is a medical condition characterized by the interruption or reduction of bile flow within the liver. Bile is a digestive fluid produced by the liver that helps in the absorption of fats and fat-soluble vitamins. Intrahepatic cholestasis occurs when there is a problem with the transport of bile components inside the liver cells (hepatocytes). This can lead to an accumulation of bile acids, bilirubin, and other substances in the liver, which can cause damage to liver cells and result in symptoms such as jaundice, itching, and dark urine.
Intrahepatic cholestasis can be caused by various factors, including medications, alcohol abuse, hepatitis viruses, autoimmune disorders, genetic defects, and cancer. Depending on the underlying cause, intrahepatic cholestasis can be acute or chronic, and it can range from mild to severe. Treatment typically involves addressing the underlying cause of the condition, as well as providing supportive care to manage symptoms and prevent complications.
Acute cholecystitis is a medical condition characterized by inflammation of the gallbladder (cholecystitis) that develops suddenly (acute). The gallbladder is a small pear-shaped organ located in the upper right part of the abdomen, beneath the liver. It stores bile, a digestive juice produced by the liver, which helps break down fats in the food we eat.
Acute cholecystitis occurs when the gallbladder becomes inflamed and irritated, often due to the presence of gallstones that block the cystic duct, the tube that carries bile from the gallbladder into the small intestine. When the cystic duct is obstructed, bile builds up in the gallbladder, causing it to become swollen, inflamed, and infected.
Symptoms of acute cholecystitis may include sudden and severe abdominal pain, often located in the upper right or middle part of the abdomen, that may radiate to the back or shoulder blade area. Other symptoms may include fever, nausea, vomiting, loss of appetite, and abdominal tenderness or swelling.
Acute cholecystitis is typically diagnosed through a combination of medical history, physical examination, laboratory tests, and imaging studies such as ultrasound or CT scan. Treatment may involve hospitalization, antibiotics to treat infection, pain relief medications, and surgery to remove the gallbladder (cholecystectomy). In some cases, nonsurgical treatments such as endoscopic sphincterotomy or percutaneous cholecystostomy may be used to relieve obstruction and inflammation.
Pancreaticoduodenectomy, also known as the Whipple procedure, is a complex surgical operation that involves the removal of the head of the pancreas, the duodenum (the first part of the small intestine), the gallbladder, and the distal common bile duct. In some cases, a portion of the stomach may also be removed. The remaining parts of the pancreas, bile duct, and intestines are then reconnected to allow for the digestion of food and drainage of bile.
This procedure is typically performed as a treatment for various conditions affecting the pancreas, such as tumors (including pancreatic cancer), chronic pancreatitis, or traumatic injuries. It is a major surgical operation that requires significant expertise and experience to perform safely and effectively.
Sphincter of Oddi dysfunction (SOD) is a condition characterized by abnormalities in the functioning of the Sphincter of Oddi, which is a muscular valve that controls the flow of bile and pancreatic juice from the pancreas and gallbladder into the duodenum (the first part of the small intestine).
In SOD, the sphincter may either fail to relax properly or become overactive, leading to a variety of symptoms such as abdominal pain, nausea, vomiting, bloating, and elevated liver enzymes. The condition can be classified into two types: Type I, which is associated with elevated liver enzymes and/or pancreatic enzymes, and Type II, which is characterized by abdominal pain without biochemical abnormalities.
The diagnosis of SOD typically involves a series of tests such as manometry (measuring the pressure inside the sphincter), endoscopic ultrasound, or magnetic resonance cholangiopancreatography (MRCP) to visualize the anatomy and function of the sphincter. Treatment options may include medications to relax the sphincter, endoscopic therapy to cut or stretch the muscle, or surgery in severe cases.
A jejunostomy is a surgical procedure where an opening (stoma) is created in the lower part of the small intestine, called the jejunum. This stoma allows for the passage of nutrients and digestive enzymes from the small intestine into a tube or external pouch, bypassing the mouth, esophagus, stomach, and upper small intestine (duodenum).
Jejunostomy is typically performed to provide enteral nutrition support in patients who are unable to consume food or liquids by mouth due to various medical conditions such as dysphagia, gastroparesis, bowel obstruction, or after certain surgical procedures. The jejunostomy tube can be used for short-term or long-term nutritional support, depending on the patient's needs and underlying medical condition.
Cholecystolithiasis is the medical term for the presence of gallstones in the gallbladder. The gallbladder is a small pear-shaped organ located under the liver that stores and concentrates bile, a digestive fluid produced by the liver. Gallstones are hardened deposits that can form in the gallbladder when substances in the bile, such as cholesterol or bilirubin, become concentrated and crystallize.
Gallstones can vary in size, from tiny grains of sand to large stones several centimeters in diameter. Some people may have a single gallstone, while others may have many. Gallstones may cause no symptoms at all, but if they block the flow of bile out of the gallbladder, they can cause pain, inflammation, and infection.
Symptoms of cholecystolithiasis may include abdominal pain, often in the upper right or center of the abdomen, that may be sharp or crampy and may occur after eating fatty foods. Other symptoms may include nausea, vomiting, fever, and chills. If gallstones are left untreated, they can lead to serious complications such as cholecystitis (inflammation of the gallbladder), pancreatitis (inflammation of the pancreas), or cholangitis (infection of the bile ducts). Treatment for cholecystolithiasis may include medication to dissolve the gallstones, shock wave lithotripsy to break up the stones, or surgery to remove the gallbladder.
Bilirubin is a yellowish pigment that is produced by the liver when it breaks down old red blood cells. It is a normal byproduct of hemoglobin metabolism and is usually conjugated (made water-soluble) in the liver before being excreted through the bile into the digestive system. Elevated levels of bilirubin can cause jaundice, a yellowing of the skin and eyes. Increased bilirubin levels may indicate liver disease or other medical conditions such as gallstones or hemolysis. It is also measured to assess liver function and to help diagnose various liver disorders.
The duodenum is the first part of the small intestine, immediately following the stomach. It is a C-shaped structure that is about 10-12 inches long and is responsible for continuing the digestion process that begins in the stomach. The duodenum receives partially digested food from the stomach through the pyloric valve and mixes it with digestive enzymes and bile produced by the pancreas and liver, respectively. These enzymes help break down proteins, fats, and carbohydrates into smaller molecules, allowing for efficient absorption in the remaining sections of the small intestine.
Pancreatic diseases refer to a group of medical conditions that affect the structure and function of the pancreas, a vital organ located in the abdomen. The pancreas has two main functions: an exocrine function, which involves the production of digestive enzymes that help break down food in the small intestine, and an endocrine function, which involves the production of hormones such as insulin and glucagon that regulate blood sugar levels.
Pancreatic diseases can be broadly classified into two categories: inflammatory and non-inflammatory. Inflammatory pancreatic diseases include conditions such as acute pancreatitis, which is characterized by sudden inflammation of the pancreas, and chronic pancreatitis, which is a long-term inflammation that can lead to scarring and loss of function.
Non-inflammatory pancreatic diseases include conditions such as pancreatic cancer, which is a malignant tumor that can arise from the cells of the pancreas, and benign tumors such as cysts or adenomas. Other non-inflammatory conditions include pancreatic insufficiency, which can occur when the pancreas does not produce enough digestive enzymes, and diabetes mellitus, which can result from impaired insulin production or action.
Overall, pancreatic diseases can have serious consequences on a person's health and quality of life, and early diagnosis and treatment are essential for optimal outcomes.
The intraoperative period is the phase of surgical treatment that refers to the time during which the surgery is being performed. It begins when the anesthesia is administered and the patient is prepared for the operation, and it ends when the surgery is completed, the anesthesia is discontinued, and the patient is transferred to the recovery room or intensive care unit (ICU).
During the intraoperative period, the surgical team, including surgeons, anesthesiologists, nurses, and other healthcare professionals, work together to carry out the surgical procedure safely and effectively. The anesthesiologist monitors the patient's vital signs, such as heart rate, blood pressure, oxygen saturation, and body temperature, throughout the surgery to ensure that the patient remains stable and does not experience any complications.
The surgeon performs the operation, using various surgical techniques and instruments to achieve the desired outcome. The surgical team also takes measures to prevent infection, control bleeding, and manage pain during and after the surgery.
Overall, the intraoperative period is a critical phase of surgical treatment that requires close collaboration and communication among members of the healthcare team to ensure the best possible outcomes for the patient.
The liver is a large, solid organ located in the upper right portion of the abdomen, beneath the diaphragm and above the stomach. It plays a vital role in several bodily functions, including:
1. Metabolism: The liver helps to metabolize carbohydrates, fats, and proteins from the food we eat into energy and nutrients that our bodies can use.
2. Detoxification: The liver detoxifies harmful substances in the body by breaking them down into less toxic forms or excreting them through bile.
3. Synthesis: The liver synthesizes important proteins, such as albumin and clotting factors, that are necessary for proper bodily function.
4. Storage: The liver stores glucose, vitamins, and minerals that can be released when the body needs them.
5. Bile production: The liver produces bile, a digestive juice that helps to break down fats in the small intestine.
6. Immune function: The liver plays a role in the immune system by filtering out bacteria and other harmful substances from the blood.
Overall, the liver is an essential organ that plays a critical role in maintaining overall health and well-being.
Postoperative complications refer to any unfavorable condition or event that occurs during the recovery period after a surgical procedure. These complications can vary in severity and may include, but are not limited to:
1. Infection: This can occur at the site of the incision or inside the body, such as pneumonia or urinary tract infection.
2. Bleeding: Excessive bleeding (hemorrhage) can lead to a drop in blood pressure and may require further surgical intervention.
3. Blood clots: These can form in the deep veins of the legs (deep vein thrombosis) and can potentially travel to the lungs (pulmonary embolism).
4. Wound dehiscence: This is when the surgical wound opens up, which can lead to infection and further complications.
5. Pulmonary issues: These include atelectasis (collapsed lung), pneumonia, or respiratory failure.
6. Cardiovascular problems: These include abnormal heart rhythms (arrhythmias), heart attack, or stroke.
7. Renal failure: This can occur due to various reasons such as dehydration, blood loss, or the use of certain medications.
8. Pain management issues: Inadequate pain control can lead to increased stress, anxiety, and decreased mobility.
9. Nausea and vomiting: These can be caused by anesthesia, opioid pain medication, or other factors.
10. Delirium: This is a state of confusion and disorientation that can occur in the elderly or those with certain medical conditions.
Prompt identification and management of these complications are crucial to ensure the best possible outcome for the patient.
Cholecystostomy is a medical procedure that involves the creation of an opening or fistula between the gallbladder and the stomach or the skin surface to drain bile from the gallbladder. This procedure is typically performed when there is an obstruction in the cystic duct or common bile duct, leading to inflammation or infection of the gallbladder (cholecystitis).
There are two types of cholecystostomy: percutaneous and open. Percutaneous cholecystostomy is a minimally invasive procedure that involves inserting a small tube through the skin and into the gallbladder under the guidance of imaging techniques such as ultrasound or CT scan. Open cholecystostomy, on the other hand, requires an open surgical incision to access the gallbladder and create the fistula.
Cholecystostomy is usually a temporary measure to manage acute cholecystitis in high-risk patients who are not suitable candidates for surgery or until they become stable enough to undergo a more definitive treatment, such as cholecystectomy (surgical removal of the gallbladder).
Bile reflux is a condition in which bile flows backward from the small intestine into the stomach and sometimes into the esophagus, causing symptoms such as heartburn, nausea, vomiting a greenish-yellow fluid (bile), and abdominal pain. Bile is a digestive fluid produced by the liver that helps to break down fats in the small intestine. Normally, a muscle called the sphincter of Oddi prevents bile from flowing backward into the stomach. However, if this muscle becomes weak or damaged, bile reflux can occur.
Bile reflux is different from gastroesophageal reflux disease (GERD), which occurs when stomach acid flows backward into the esophagus. Although both conditions can cause similar symptoms, such as heartburn and regurgitation, they require different treatments. Bile reflux can increase the risk of complications such as inflammation of the stomach lining (gastritis), ulcers, and cancer of the esophagus. If left untreated, bile reflux can lead to serious health problems, so it is important to seek medical attention if you experience symptoms.
Endosonography, also known as endoscopic ultrasound (EUS), is a medical procedure that combines endoscopy and ultrasound to obtain detailed images and information about the digestive tract and surrounding organs. An endoscope, which is a flexible tube with a light and camera at its tip, is inserted through the mouth or rectum to reach the area of interest. A high-frequency ultrasound transducer at the tip of the endoscope generates sound waves that bounce off body tissues and create echoes, which are then translated into detailed images by a computer.
Endosonography allows doctors to visualize structures such as the esophageal, stomach, and intestinal walls, lymph nodes, blood vessels, and organs like the pancreas, liver, and gallbladder. It can help diagnose conditions such as tumors, inflammation, and infections, and it can also be used to guide biopsies or fine-needle aspirations of suspicious lesions.
Overall, endosonography is a valuable tool for the diagnosis and management of various gastrointestinal and related disorders.
Experimental liver cirrhosis refers to a controlled research setting where various factors and substances are intentionally introduced to induce liver cirrhosis in animals or cell cultures. The purpose is to study the mechanisms, progression, potential treatments, and prevention strategies for liver cirrhosis. This could involve administering chemicals, drugs, alcohol, viruses, or manipulating genes associated with liver damage and fibrosis. It's important to note that results from experimental models may not directly translate to human conditions, but they can provide valuable insights into disease pathophysiology and therapeutic development.
Lithotripsy, laser refers to a medical procedure that uses laser energy to break down and fragment stones located in the urinary tract, such as kidney or ureteral stones. The laser energy is delivered through a flexible fiberoptic endoscope, which is inserted into the urinary tract. Once the stone is targeted, the laser energy is focused on it, causing the stone to fragment into tiny pieces that can then be passed naturally through the urine. This procedure is typically performed under anesthesia and may require hospitalization depending on the size and location of the stone. It is a minimally invasive alternative to traditional surgical methods for treating urinary tract stones.
Pathological constriction refers to an abnormal narrowing or tightening of a body passage or organ, which can interfere with the normal flow of blood, air, or other substances through the area. This constriction can occur due to various reasons such as inflammation, scarring, or abnormal growths, and can affect different parts of the body, including blood vessels, airways, intestines, and ureters. Pathological constriction can lead to a range of symptoms and complications depending on its location and severity, and may require medical intervention to correct.
Intraoperative care refers to the medical care and interventions provided to a patient during a surgical procedure. This care is typically administered by a team of healthcare professionals, including anesthesiologists, surgeons, nurses, and other specialists as needed. The goal of intraoperative care is to maintain the patient's physiological stability throughout the surgery, minimize complications, and ensure the best possible outcome.
Intraoperative care may include:
1. Anesthesia management: Administering and monitoring anesthetic drugs to keep the patient unconscious and free from pain during the surgery.
2. Monitoring vital signs: Continuously tracking the patient's heart rate, blood pressure, oxygen saturation, body temperature, and other key physiological parameters to ensure they remain within normal ranges.
3. Fluid and blood product administration: Maintaining adequate intravascular volume and oxygen-carrying capacity through the infusion of fluids and blood products as needed.
4. Intraoperative imaging: Utilizing real-time imaging techniques, such as X-ray, ultrasound, or CT scans, to guide the surgical procedure and ensure accurate placement of implants or other devices.
5. Neuromonitoring: Using electrophysiological methods to monitor the functional integrity of nerves and neural structures during surgery, particularly in procedures involving the brain, spine, or peripheral nerves.
6. Intraoperative medication management: Administering various medications as needed for pain control, infection prophylaxis, or the treatment of medical conditions that may arise during the surgery.
7. Temperature management: Regulating the patient's body temperature to prevent hypothermia or hyperthermia, which can have adverse effects on surgical outcomes and overall patient health.
8. Communication and coordination: Ensuring effective communication among the members of the surgical team to optimize patient care and safety.
Catheterization is a medical procedure in which a catheter (a flexible tube) is inserted into the body to treat various medical conditions or for diagnostic purposes. The specific definition can vary depending on the area of medicine and the particular procedure being discussed. Here are some common types of catheterization:
1. Urinary catheterization: This involves inserting a catheter through the urethra into the bladder to drain urine. It is often performed to manage urinary retention, monitor urine output in critically ill patients, or assist with surgical procedures.
2. Cardiac catheterization: A procedure where a catheter is inserted into a blood vessel, usually in the groin or arm, and guided to the heart. This allows for various diagnostic tests and treatments, such as measuring pressures within the heart chambers, assessing blood flow, or performing angioplasty and stenting of narrowed coronary arteries.
3. Central venous catheterization: A catheter is inserted into a large vein, typically in the neck, chest, or groin, to administer medications, fluids, or nutrition, or to monitor central venous pressure.
4. Peritoneal dialysis catheterization: A catheter is placed into the abdominal cavity for individuals undergoing peritoneal dialysis, a type of kidney replacement therapy.
5. Neurological catheterization: In some cases, a catheter may be inserted into the cerebrospinal fluid space (lumbar puncture) or the brain's ventricular system (ventriculostomy) to diagnose or treat various neurological conditions.
These are just a few examples of catheterization procedures in medicine. The specific definition and purpose will depend on the medical context and the particular organ or body system involved.
Liver function tests (LFTs) are a group of blood tests that are used to assess the functioning and health of the liver. These tests measure the levels of various enzymes, proteins, and waste products that are produced or metabolized by the liver. Some common LFTs include:
1. Alanine aminotransferase (ALT): An enzyme found primarily in the liver, ALT is released into the bloodstream in response to liver cell damage. Elevated levels of ALT may indicate liver injury or disease.
2. Aspartate aminotransferase (AST): Another enzyme found in various tissues, including the liver, heart, and muscles. Like ALT, AST is released into the bloodstream following tissue damage. High AST levels can be a sign of liver damage or other medical conditions.
3. Alkaline phosphatase (ALP): An enzyme found in several organs, including the liver, bile ducts, and bones. Elevated ALP levels may indicate a blockage in the bile ducts, liver disease, or bone disorders.
4. Gamma-glutamyl transferase (GGT): An enzyme found mainly in the liver, pancreas, and biliary system. Increased GGT levels can suggest liver disease, alcohol consumption, or the use of certain medications.
5. Bilirubin: A yellowish pigment produced when hemoglobin from red blood cells is broken down. Bilirubin is processed by the liver and excreted through bile. High bilirubin levels can indicate liver dysfunction, bile duct obstruction, or certain types of anemia.
6. Albumin: A protein produced by the liver that helps maintain fluid balance in the body and transports various substances in the blood. Low albumin levels may suggest liver damage, malnutrition, or kidney disease.
7. Total protein: A measure of all proteins present in the blood, including albumin and other types of proteins produced by the liver. Decreased total protein levels can indicate liver dysfunction or other medical conditions.
These tests are often ordered together as part of a routine health checkup or when evaluating symptoms related to liver function or disease. The results should be interpreted in conjunction with clinical findings, medical history, and other diagnostic tests.
Duodenal diseases refer to a range of medical conditions that affect the duodenum, which is the first part of the small intestine. Here are some examples of duodenal diseases:
1. Duodenitis: This is inflammation of the duodenum, which can cause symptoms such as abdominal pain, nausea, vomiting, and bloating. Duodenitis can be caused by bacterial or viral infections, excessive use of nonsteroidal anti-inflammatory drugs (NSAIDs), or chronic inflammation due to conditions like Crohn's disease.
2. Peptic ulcers: These are sores that develop in the lining of the duodenum, usually as a result of infection with Helicobacter pylori bacteria or long-term use of NSAIDs. Symptoms can include abdominal pain, bloating, and heartburn.
3. Duodenal cancer: This is a rare type of cancer that affects the duodenum. Symptoms can include abdominal pain, weight loss, and blood in the stool.
4. Celiac disease: This is an autoimmune disorder that causes the immune system to attack the lining of the small intestine in response to gluten, a protein found in wheat, barley, and rye. This can lead to inflammation and damage to the duodenum.
5. Duodenal diverticulosis: This is a condition in which small pouches form in the lining of the duodenum. While many people with duodenal diverticulosis do not experience symptoms, some may develop complications such as inflammation or infection.
6. Duodenal atresia: This is a congenital condition in which the duodenum does not form properly, leading to blockage of the intestine. This can cause symptoms such as vomiting and difficulty feeding in newborns.
Cholangiocarcinoma is a type of cancer that arises from the cells that line the bile ducts, which are small tubes that carry digestive enzymes from the liver to the small intestine. It can occur in different parts of the bile duct system, including the bile ducts inside the liver (intrahepatic), the bile ducts outside the liver (extrahepatic), and the area where the bile ducts join the pancreas and small intestine (ampulla of Vater).
Cholangiocarcinoma is a relatively rare cancer, but its incidence has been increasing in recent years. It can be difficult to diagnose because its symptoms are often nonspecific and similar to those of other conditions, such as gallstones or pancreatitis. Treatment options depend on the location and stage of the cancer, and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Duodenal neoplasms refer to abnormal growths in the duodenum, which is the first part of the small intestine that receives digestive secretions from the pancreas and bile duct. These growths can be benign or malignant (cancerous).
Benign neoplasms include adenomas, leiomyomas, lipomas, and hamartomas. They are usually slow-growing and do not spread to other parts of the body. However, they may cause symptoms such as abdominal pain, bleeding, or obstruction of the intestine.
Malignant neoplasms include adenocarcinomas, neuroendocrine tumors (carcinoids), lymphomas, and sarcomas. They are more aggressive and can invade surrounding tissues and spread to other parts of the body. Symptoms may include abdominal pain, weight loss, jaundice, anemia, or bowel obstruction.
The diagnosis of duodenal neoplasms is usually made through imaging tests such as CT scans, MRI, or endoscopy with biopsy. Treatment depends on the type and stage of the tumor and may include surgery, chemotherapy, radiation therapy, or a combination of these modalities.
The thoracic duct is the largest lymphatic vessel in the human body. It is a part of the lymphatic system, which helps to regulate fluid balance and immune function. The thoracic duct originates from the cisterna chyli, a dilated sac located in the abdomen near the aorta.
The thoracic duct collects lymph from the lower extremities, abdomen, pelvis, and left side of the thorax (chest). It ascends through the diaphragm and enters the chest, where it passes through the mediastinum (the central part of the chest between the lungs) and eventually drains into the left subclavian vein.
The thoracic duct plays a crucial role in transporting lymphatic fluid, which contains white blood cells, fats, proteins, and other substances, back into the circulatory system. Any obstruction or damage to the thoracic duct can lead to lymph accumulation in the surrounding tissues, causing swelling and other symptoms.
"Calculi" is a medical term that refers to abnormal concretions or hard masses formed within the body, usually in hollow organs or cavities. These masses are typically composed of minerals such as calcium oxalate, calcium phosphate, or magnesium ammonium phosphate, and can vary in size from tiny granules to large stones. The plural form of the Latin word "calculus" (meaning "pebble"), calculi are commonly known as "stones." They can occur in various locations within the body, including the kidneys, gallbladder, urinary bladder, and prostate gland. The presence of calculi can cause a range of symptoms, such as pain, obstruction, infection, or inflammation, depending on their size, location, and composition.
Biliary cirrhosis is a specific type of liver cirrhosis that results from chronic inflammation and scarring of the bile ducts, leading to impaired bile flow, liver damage, and fibrosis. It can be further classified into primary biliary cholangitis (PBC) and secondary biliary cirrhosis. PBC is an autoimmune disease, while secondary biliary cirrhosis is often associated with chronic gallstones, biliary tract obstruction, or recurrent pyogenic cholangitis. Symptoms may include fatigue, itching, jaundice, and abdominal discomfort. Diagnosis typically involves blood tests, imaging studies, and sometimes liver biopsy. Treatment focuses on managing symptoms, slowing disease progression, and preventing complications.
Ascaridida is an order of large, parasitic roundworms that belong to the phylum Nematoda. These worms are known to infect a wide range of hosts, including humans, and can cause significant damage to their host's health. The most well-known species in this order is Ascaris lumbricoides, which is the causative agent of ascariasis in humans.
Ascariasis is a common parasitic infection that affects millions of people worldwide, particularly in areas with poor sanitation and hygiene. The life cycle of Ascaris lumbricoides involves the ingestion of eggs present in contaminated food or water. Once inside the human body, the larvae hatch from the eggs and migrate through the lungs, where they mature into adult worms that can grow up to 15 inches long. The adult worms then lay thousands of eggs that are passed through the feces, perpetuating the life cycle.
Symptoms of ascariasis can range from mild to severe and may include abdominal pain, nausea, vomiting, diarrhea, and coughing. In severe cases, the worms can cause intestinal obstruction or perforation, which can be life-threatening if left untreated.
Prevention of ascariasis involves practicing good hygiene and sanitation, including washing hands thoroughly with soap and water before eating or preparing food, avoiding contact with contaminated soil or water, and cooking food thoroughly. Treatment typically involves the use of anti-parasitic drugs that kill the worms and their eggs.
Surgical instruments are specialized tools or devices that are used by medical professionals during surgical procedures to assist in various tasks such as cutting, dissecting, grasping, holding, retracting, clamping, and suturing body tissues. These instruments are designed to be safe, precise, and effective, with a variety of shapes, sizes, and materials used depending on the specific surgical application. Some common examples of surgical instruments include scalpels, forceps, scissors, hemostats, retractors, and needle holders. Proper sterilization and maintenance of these instruments are crucial to ensure patient safety and prevent infection.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
Lithiasis is a medical term that refers to the formation of stones or calculi in various organs of the body. These stones can develop in the kidneys (nephrolithiasis), gallbladder (cholelithiasis), urinary bladder (cystolithiasis), or salivary glands (sialolithiasis). The stones are usually composed of minerals and organic substances, and their formation can be influenced by various factors such as diet, dehydration, genetic predisposition, and chronic inflammation. Lithiasis can cause a range of symptoms depending on the location and size of the stone, including pain, obstruction, infection, and damage to surrounding tissues. Treatment may involve medication, shock wave lithotripsy, or surgical removal of the stones.
Hepatopulmonary syndrome (HPS) is a pulmonary vascular disorder characterized by the abnormal dilatation of the blood vessels in the lungs and intrapulmonary shunting, leading to hypoxemia (low levels of oxygen in the blood). This condition primarily affects individuals with liver diseases, particularly those with cirrhosis.
HPS is defined by the following triad of symptoms:
1. Liver dysfunction or portal hypertension
2. Intrapulmonary vascular dilatations
3. Hypoxemia (PaO2 ≤ 80 mmHg or alveolar-arterial oxygen gradient ≥ 15 mmHg in room air)
The pathophysiology of HPS involves the production and release of vasoactive substances from the liver, which cause dilation of the pulmonary vessels. This results in ventilation-perfusion mismatch and right-to-left shunting, leading to hypoxemia. Clinical manifestations include shortness of breath, platypnea (worsening dyspnea while in the upright position), orthodeoxia (decrease in oxygen saturation when changing from supine to upright position), digital clubbing, and cyanosis.
Diagnosis is confirmed through contrast-enhanced echocardiography or macroaggregated albumin lung scan, which demonstrates intrapulmonary shunting. Treatment of HPS primarily focuses on managing the underlying liver disease and improving hypoxemia with supplemental oxygen or other supportive measures. In some cases, liver transplantation may be considered as a definitive treatment option for both the liver disease and HPS.
Colic is a term used to describe excessive, frequent crying or fussiness in a healthy infant, often lasting several hours a day and occurring several days a week. Although the exact cause of colic is unknown, it may be related to digestive issues, such as gas or indigestion. The medical community defines colic by the "Rule of Three": crying for more than three hours per day, for more than three days per week, and for longer than three weeks in an infant who is well-fed and otherwise healthy. It typically begins within the first few weeks of life and improves on its own, usually by age 3-4 months. While colic can be distressing for parents and caregivers, it does not cause any long-term harm to the child.
Intraoperative complications refer to any unforeseen problems or events that occur during the course of a surgical procedure, once it has begun and before it is completed. These complications can range from minor issues, such as bleeding or an adverse reaction to anesthesia, to major complications that can significantly impact the patient's health and prognosis.
Examples of intraoperative complications include:
1. Bleeding (hemorrhage) - This can occur due to various reasons such as injury to blood vessels or organs during surgery.
2. Infection - Surgical site infections can develop if the surgical area becomes contaminated during the procedure.
3. Anesthesia-related complications - These include adverse reactions to anesthesia, difficulty maintaining the patient's airway, or cardiovascular instability.
4. Organ injury - Accidental damage to surrounding organs can occur during surgery, leading to potential long-term consequences.
5. Equipment failure - Malfunctioning surgical equipment can lead to complications and compromise the safety of the procedure.
6. Allergic reactions - Patients may have allergies to certain medications or materials used during surgery, causing an adverse reaction.
7. Prolonged operative time - Complications may arise if a surgical procedure takes longer than expected, leading to increased risk of infection and other issues.
Intraoperative complications require prompt identification and management by the surgical team to minimize their impact on the patient's health and recovery.
The pancreas is a glandular organ located in the abdomen, posterior to the stomach. It has both exocrine and endocrine functions. The exocrine portion of the pancreas consists of acinar cells that produce and secrete digestive enzymes into the duodenum via the pancreatic duct. These enzymes help in the breakdown of proteins, carbohydrates, and fats in food.
The endocrine portion of the pancreas consists of clusters of cells called islets of Langerhans, which include alpha, beta, delta, and F cells. These cells produce and secrete hormones directly into the bloodstream, including insulin, glucagon, somatostatin, and pancreatic polypeptide. Insulin and glucagon are critical regulators of blood sugar levels, with insulin promoting glucose uptake and storage in tissues and glucagon stimulating glycogenolysis and gluconeogenesis to raise blood glucose when it is low.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
Laparoscopy is a surgical procedure that involves the insertion of a laparoscope, which is a thin tube with a light and camera attached to it, through small incisions in the abdomen. This allows the surgeon to view the internal organs without making large incisions. It's commonly used to diagnose and treat various conditions such as endometriosis, ovarian cysts, infertility, and appendicitis. The advantages of laparoscopy over traditional open surgery include smaller incisions, less pain, shorter hospital stays, and quicker recovery times.
Ursodeoxycholic acid (UDCA) is a naturally occurring bile acid that is used medically as a therapeutic agent. It is commonly used to treat gallstones, particularly cholesterol gallstones, and other conditions associated with abnormal liver function, such as primary biliary cholangitis (PBC). UDCA works by decreasing the amount of cholesterol in bile and protecting liver cells from damage. It is also known as ursodiol or Ursotan.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
Chronic pancreatitis is a long-standing inflammation of the pancreas that leads to irreversible structural changes and impaired function of the pancreas. It is characterized by recurrent or persistent abdominal pain, often radiating to the back, and maldigestion with steatorrhea (fatty stools) due to exocrine insufficiency. The pancreatic damage results from repeated episodes of acute pancreatitis, alcohol abuse, genetic predisposition, or autoimmune processes. Over time, the pancreas may lose its ability to produce enough digestive enzymes and hormones like insulin, which can result in diabetes mellitus. Chronic pancreatitis also increases the risk of developing pancreatic cancer.
Roux-en-Y anastomosis is a type of surgical connection between two parts of the gastrointestinal tract, typically performed during gastric bypass surgery for weight loss. In this procedure, a small pouch is created from the upper stomach, and the remaining portion of the stomach is bypassed. The Roux limb, a segment of the small intestine, is then connected to both the pouch and the bypassed stomach, creating two separate channels for food and digestive juices to mix. This surgical technique helps to reduce the amount of food that can be consumed and absorbed, leading to weight loss.
A diverticulum is a small sac or pouch that forms as a result of a weakness in the wall of a hollow organ, such as the intestine. These sacs can become inflamed or infected, leading to conditions like diverticulitis. Diverticula are common in the large intestine, particularly in the colon, and are more likely to develop with age. They are usually asymptomatic but can cause symptoms such as abdominal pain, bloating, constipation, or diarrhea if they become inflamed or infected.
A villous adenoma is a type of polyp (a growth that protrudes from the lining of an organ) found in the colon or rectum. It is named for its appearance under a microscope, which reveals finger-like projections called "villi" on the surface of the polyp.
Villous adenomas are typically larger than other types of polyps and can be several centimeters in size. They are also more likely to be cancerous or precancerous, meaning that they have the potential to develop into colon or rectal cancer over time.
Because of this increased risk, it is important for villous adenomas to be removed surgically if they are found during a colonoscopy or other diagnostic procedure. Regular follow-up colonoscopies may also be recommended to monitor for the development of new polyps or recurrence of previous ones.
Cholecystography is a medical procedure that involves the use of X-rays to examine the gallbladder and bile ducts. It is also known as an oral cholecystogram (OCG).
The procedure involves administering a contrast agent, typically a iodine-based dye, which is absorbed by the liver and excreted into the bile ducts and gallbladder. The dye makes the bile ducts and gallbladder visible on X-ray images, allowing doctors to diagnose conditions such as gallstones, tumors, or inflammation of the gallbladder.
Cholecystography is not commonly used today due to the development of more advanced imaging techniques, such as ultrasound and computed tomography (CT) scans, which are non-invasive and do not require the use of contrast agents. However, it may still be used in certain cases where other imaging tests are inconclusive or unavailable.
Bile canaliculi are the smallest bile-transporting structures in the liver. They are formed by the close apposition of hepatocyte (liver cell) plasma membranes, and they are responsible for the majority of bile production. The bile canaliculi merge to form bile ductules, which then merge to form larger bile ducts that transport bile to the gallbladder and small intestine. Bile is a fluid that contains water, electrolytes, bile salts, cholesterol, phospholipids, and bilirubin, which are produced by the liver and play important roles in digestion and elimination of waste products.
Surgical anastomosis is a medical procedure that involves the connection of two tubular structures, such as blood vessels or intestines, to create a continuous passage. This technique is commonly used in various types of surgeries, including vascular, gastrointestinal, and orthopedic procedures.
During a surgical anastomosis, the ends of the two tubular structures are carefully prepared by removing any damaged or diseased tissue. The ends are then aligned and joined together using sutures, staples, or other devices. The connection must be secure and leak-free to ensure proper function and healing.
The success of a surgical anastomosis depends on several factors, including the patient's overall health, the location and condition of the structures being joined, and the skill and experience of the surgeon. Complications such as infection, bleeding, or leakage can occur, which may require additional medical intervention or surgery.
Proper postoperative care is also essential to ensure the success of a surgical anastomosis. This may include monitoring for signs of complications, administering medications to prevent infection and promote healing, and providing adequate nutrition and hydration.
Cholagogues and choleretics are terms used to describe medications or substances that affect bile secretion and flow in the body. Here is a medical definition for each:
1. Cholagogue: A substance that promotes the discharge of bile from the gallbladder into the duodenum, often by stimulating the contraction of the gallbladder muscle. This helps in the digestion and absorption of fats. Examples include chenodeoxycholic acid, ursodeoxycholic acid, and some herbal remedies like dandelion root and milk thistle.
2. Choleretic: A substance that increases the production of bile by the liver or its flow through the biliary system. This can help with the digestion of fats and the elimination of waste products from the body. Examples include certain medications like ursodeoxycholic acid, as well as natural substances such as lemon juice, artichoke extract, and turmeric.
It is important to note that while cholagogues and choleretics can aid in digestion, they should be used under the guidance of a healthcare professional, as improper use or overuse may lead to complications like diarrhea or gallstone formation.
Postcholecystectomy Syndrome is a condition that occurs in some patients following the surgical removal of the gallbladder (cholecystectomy). The syndrome encompasses a variety of symptoms such as abdominal pain, bloating, gas, indigestion, and diarrhea, which can be caused by several factors including:
1. Abnormal functioning or motility of the sphincter of Oddi (a muscle that controls the flow of bile and pancreatic juice into the small intestine)
2. Formation of gallstones in the bile ducts (choledocholithiasis)
3. Biliary dyskinesia (impaired functioning of the biliary tract muscles)
4. Persistent or recurrent infection or inflammation of the bile ducts (biliopathy)
5. Formation of abnormal bile-filled pouches (biliolethiasis or bile duct cysts)
6. Changes in bowel habits due to altered enterohepatic circulation of bile acids
The symptoms of Postcholecystectomy Syndrome can vary in severity and frequency, and they may appear soon after the surgery or develop months or even years later. The diagnosis of this condition typically involves a comprehensive medical evaluation, including a detailed history, physical examination, laboratory tests, and imaging studies such as ultrasound, CT scan, MRI, or endoscopic retrograde cholangiopancreatography (ERCP).
Treatment options for Postcholecystectomy Syndrome depend on the underlying cause of the symptoms and may include medications, dietary modifications, endoscopic procedures, or surgery. In some cases, the syndrome may resolve on its own without any specific treatment.
Adenocarcinoma, papillary is a type of cancer that begins in the glandular cells and grows in a finger-like projection (called a papilla). This type of cancer can occur in various organs, including the lungs, pancreas, thyroid, and female reproductive system. The prognosis and treatment options for papillary adenocarcinoma depend on several factors, such as the location and stage of the tumor, as well as the patient's overall health. It is important to consult with a healthcare professional for an accurate diagnosis and personalized treatment plan.
Fascioliasis is a parasitic infection caused by two species of flatworms (trematodes) called Fasciola hepatica and Fasciola gigantica. These worms are commonly known as liver flukes. The infection occurs when people consume raw or undercooked watercress, watercress salad, or other contaminated vegetables.
The life cycle of these parasites involves a complex series of stages involving snails and aquatic vegetation. When humans ingest the larval stage of the parasite, it migrates through the intestinal wall, enters the abdominal cavity, and eventually reaches the liver. Here, it causes damage to the bile ducts and liver parenchyma, leading to symptoms such as fever, abdominal pain, diarrhea, and jaundice.
Fascioliasis is more common in areas where livestock farming is prevalent, particularly in parts of South America, Africa, and Asia. However, it can also occur in travelers who have consumed contaminated food or water while visiting endemic areas. Treatment typically involves the use of anti-parasitic medications such as triclabendazole or praziquantel.
Liver diseases refer to a wide range of conditions that affect the normal functioning of the liver. The liver is a vital organ responsible for various critical functions such as detoxification, protein synthesis, and production of biochemicals necessary for digestion.
Liver diseases can be categorized into acute and chronic forms. Acute liver disease comes on rapidly and can be caused by factors like viral infections (hepatitis A, B, C, D, E), drug-induced liver injury, or exposure to toxic substances. Chronic liver disease develops slowly over time, often due to long-term exposure to harmful agents or inherent disorders of the liver.
Common examples of liver diseases include hepatitis, cirrhosis (scarring of the liver tissue), fatty liver disease, alcoholic liver disease, autoimmune liver diseases, genetic/hereditary liver disorders (like Wilson's disease and hemochromatosis), and liver cancers. Symptoms may vary widely depending on the type and stage of the disease but could include jaundice, abdominal pain, fatigue, loss of appetite, nausea, and weight loss.
Early diagnosis and treatment are essential to prevent progression and potential complications associated with liver diseases.
Preoperative care refers to the series of procedures, interventions, and preparations that are conducted before a surgical operation. The primary goal of preoperative care is to ensure the patient's well-being, optimize their physical condition, reduce potential risks, and prepare them mentally and emotionally for the upcoming surgery.
Preoperative care typically includes:
1. Preoperative assessment: A thorough evaluation of the patient's overall health status, including medical history, physical examination, laboratory tests, and diagnostic imaging, to identify any potential risk factors or comorbidities that may impact the surgical procedure and postoperative recovery.
2. Informed consent: The process of ensuring the patient understands the nature of the surgery, its purpose, associated risks, benefits, and alternative treatment options. The patient signs a consent form indicating they have been informed and voluntarily agree to undergo the surgery.
3. Preoperative instructions: Guidelines provided to the patient regarding their diet, medication use, and other activities in the days leading up to the surgery. These instructions may include fasting guidelines, discontinuing certain medications, or arranging for transportation after the procedure.
4. Anesthesia consultation: A meeting with the anesthesiologist to discuss the type of anesthesia that will be used during the surgery and address any concerns related to anesthesia risks, side effects, or postoperative pain management.
5. Preparation of the surgical site: Cleaning and shaving the area where the incision will be made, as well as administering appropriate antimicrobial agents to minimize the risk of infection.
6. Medical optimization: Addressing any underlying medical conditions or correcting abnormalities that may negatively impact the surgical outcome. This may involve adjusting medications, treating infections, or managing chronic diseases such as diabetes.
7. Emotional and psychological support: Providing counseling, reassurance, and education to help alleviate anxiety, fear, or emotional distress related to the surgery.
8. Preoperative holding area: The patient is transferred to a designated area near the operating room where they are prepared for surgery by changing into a gown, having intravenous (IV) lines inserted, and receiving monitoring equipment.
By following these preoperative care guidelines, healthcare professionals aim to ensure that patients undergo safe and successful surgical procedures with optimal outcomes.
Salivary ducts are the excretory tubules that transport saliva from the major and minor salivary glands to the oral cavity. The main function of these ducts is to convey the salivary secretions, which contain enzymes and lubricants, into the mouth to aid in digestion, speech, and swallowing.
There are two pairs of major salivary glands: the parotid glands and the submandibular glands. Each pair has its own set of ducts. The parotid gland's saliva is drained through the parotid duct, also known as Stensen's duct, which opens into the oral cavity opposite the upper second molar tooth. The submandibular gland's saliva is transported through the submandibular duct, or Wharton's duct, which empties into the floor of the mouth near the base of the tongue.
Minor salivary glands are scattered throughout the oral cavity and pharynx, and their secretions are drained via small ducts directly into the oral mucosa.
 Common bile duct
Common bile duct
List of MeSH codes (C06)
Common bile duct stone
Biliary colic
CBD
Cholangitis (disambiguation)
Cholangiocarcinoma
Gallstone
Ernie Fletcher
Obeticholic acid
Pancreatic duct
Foregut
Cirrhosis
Liver function tests
Acute pancreatitis
Gallbladder disease
Bile duct
Nucleoporin
Kayser-Fleischer ring
Crohn's disease
Primary biliary cholangitis
Choledochoduodenostomy
Primary sclerosing cholangitis
Jaundice
Jean-François Calot
Cholecystectomy
Cholestasis
Bernhard Moritz Carl Ludwig Riedel
Choledochal cysts
Ulcerative colitis
 Pediatric Choledochal Cyst Surgery: Practice Essentials, Anatomy, Pathophysiology
Pediatric Choledochal Cyst Surgery: Practice Essentials, Anatomy, Pathophysiology
 IndexCat
IndexCat Liver Transplantation | Liver Transplant | MedlinePlus
Liver Transplantation | Liver Transplant | MedlinePlus
 Cirrhosis of the Liver: Symptoms, Causes & Treatments
Cirrhosis of the Liver: Symptoms, Causes & Treatments
 Sanne Van Campenhout
Sanne Van Campenhout
 Gallbladder Cancer Treatment in Oklahoma | INTEGRIS Health
Gallbladder Cancer Treatment in Oklahoma | INTEGRIS Health
Common bile duct - Wikipedia
Definition of age-dependent reference values for the diameter of the common bile duct and pancreatic duct on MRCP: a population...
Apparent Triclabendazole-Resistant Human Fasciola hepatica Infection, the Netherlands - Volume 18, Number 6-June 2012 -...
 Transpancreatic precut sphincterotomy for cannulation of inaccessible common bile duct: a safe and successful technique
Transpancreatic precut sphincterotomy for cannulation of inaccessible common bile duct: a safe and successful technique
Biliary colic - Wikipedia
 Cholecystectomy following percutaneous cholecystostomy tube placement from the SAGES Video Library
Cholecystectomy following percutaneous cholecystostomy tube placement from the SAGES Video Library
Sri Venkateswara Institute of Medical Sciences (SVIMS)
 Kratom - Erowid Exp - 'Almost Destroyed My Liver'
Kratom - Erowid Exp - 'Almost Destroyed My Liver'
 General Requirements | IJES
General Requirements | IJES
Bio2Vec
 Bile Duct Cancer
Bile Duct Cancer
(Cholangiocarcinoma) (15234) ... Define Common Diseases. Brain and Nerve Center helps you find information, definitaions and treatement options for most common ... This is used to detect diseases that affect the bile ducts including bile duct cancer, gallstones stuck in the bile duct, and ...
 Malignant Carcinoid Tumor of the Common Bile Duct: Report of a Case | SpringerLink
Malignant Carcinoid Tumor of the Common Bile Duct: Report of a Case | SpringerLink OUH - OUS-research.no
OUH - OUS-research.no Cholangiocarcinoma | Bile Duct Cancer, Asbestos Link
Cholangiocarcinoma | Bile Duct Cancer, Asbestos Link Búsqueda | BVS Bolivia
Búsqueda | BVS Bolivia Primary Sclerosing Cholangitis (PSC) - Health 2023
Primary Sclerosing Cholangitis (PSC) - Health 2023 Atrophy, atrophic (of) - ICD-10-CM Index to Diseases and Injuries
Atrophy, atrophic (of) - ICD-10-CM Index to Diseases and Injuries Apollo Hospitals Navi Mumbai is the first hospital in Western India to successfully perform 25 Paediatric Liver Transplants
Apollo Hospitals Navi Mumbai is the first hospital in Western India to successfully perform 25 Paediatric Liver Transplants
 MRCP (MR Cholangiopancreatography)
MRCP (MR Cholangiopancreatography) Human Organ Transplantation | Find Me A Cure
Human Organ Transplantation | Find Me A Cure









![Cirrhosis Handbook - [PDF Document]](https://cdn.vdocuments.net/doc/1200x630/55cf8c815503462b138d1a77/cirrhosis-handbook.jpg?t=1695331343)

![10 Best Clinics for Esophageal Cancer Treatment in Thailand [2023 Prices]](https://www.mymeditravel.com/cdn-cgi/image/f=auto,fit=contain,quality=75/uploads/property/gallery/5af2758efa6b7e04401f8c27/5af51dadfa6b7e4212052361/preview.jpg)