Cranial Nerve Neoplasms
Optic Nerve Neoplasms
Cranial Nerves
Cranial Nerve Diseases
Cranial Nerve Injuries
Abducens Nerve Diseases
Facial Nerve
Oculomotor Nerve Diseases
Sciatic Nerve
Glossopharyngeal Nerve
Oculomotor Nerve
Peripheral Nerves
Trigeminal Nerve
Abducens Nerve
Vestibulocochlear Nerve
Optic Nerve
Nerve Fibers
Mobius Syndrome
Nerve Compression Syndromes
Accessory Nerve
Ophthalmoplegia
Facial Paralysis
Trigeminal Nerve Diseases
Vestibulocochlear Nerve Diseases
Skull Base Neoplasms
Trochlear Nerve
Trigeminal Neuralgia
Paralysis
Facial Nerve Diseases
Facial Nerve Injuries
Hypoglossal Nerve
Glomus Jugulare Tumor
Nerve Block
Nerve Endings
Petrous Bone
Sural Nerve
Cavernous Sinus
Median Nerve
Pancreatic Neoplasms
Tibial Nerve
Skull Base
Magnetic Resonance Imaging
Ulnar Nerve
Diplopia
Neurilemmoma
Glossopharyngeal Nerve Diseases
Cranial Fossa, Posterior
Neoplasms
Femoral Nerve
Spinal Nerves
Cochlear Nerve
Intra-operative localisation of skull base tumours. A case report using the ISG viewing wand in the management of trigeminal neuroma. (1/171)
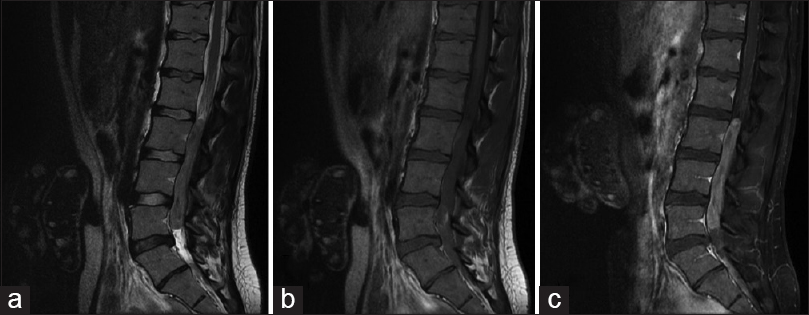
Deep-seated skull base tumours provide as much a challenge to the surgeons' skills of localisation as to his technical abilities during the resection. These lesions are frequently inaccessible and lie adjacent to vital structures requiring extensive cerebral retraction for adequate exposure and direct visualisation. The ISG viewing wand is a newly developed image guidance system to aid direction of the operative approach and localisation of intracerebral pathology. We discuss its use in the management of a trigeminal neuroma. (+info)Association of lower cranial nerve schwannoma with spinal ependymoma in ? NF2. (2/171)
A 15 year old male, who had earlier been operated for intraspinal intramedullary ependymoma, subsequently developed a right cerebello pontine (CP) angle mass. A diagnosis of right CP angle ependymoma was considered, in view of established histology of previously operated spinal lesion. Histopathological examination of the well defined extra-axial mass, which was attached with ninth cranial nerve, however revealed a schwannoma. A diagnosis of Neurofibromatosis-2 (NF2) is strongly suspected, because of well established fact, that the spinal ependymomas may have association with lower cranial nerve schwannomas in NF2. Cranial and spinal MRI screening for early diagnosis of associated, asymptomatic lesions, in suspected cases of NF2, particularly in children, is recommended. (+info)Cavernous angioma of the optic chiasm--case report. (3/171)
A 31-year-old female presented with cavernous angioma originating from the optic chiasm manifesting as sudden onset of right retroorbital pain and right visual disturbance. She had a psychomotor seizure 10 years ago. Cavernous angioma at the right basal ganglia had been partially removed at that time. After the operation, the patient had left hemiparesis, but gradually improved. Neurological examination revealed decreased right visual acuity, left homonymous hemianopsia, and left hemiparesis. Magnetic resonance imaging revealed a mixed signal intensity mass at the right optic nerve to the optic chiasm with a low signal intensity rim on T2-weighted imaging, situated at the right basal ganglia where the cavernous angioma had been partially resected. Right frontotemporal craniotomy was performed by the pterional approach. A subpial hematoma was situated at the right optic nerve to the optic chiasm. The hematoma with an angiomatous component was completely resected from the surrounding structure. Histological examination of the specimens confirmed cavernous angioma. Postoperatively, her right visual acuity was slightly improved, but the visual field defect was unchanged. We emphasize the importance of correct diagnosis by magnetic resonance imaging and subsequent resection for preserving and improving the visual function of patients with cavernous angiomas of the optic chiasm. (+info)Isolated metastases of adenocarcinoma in the bilateral internal auditory meatuses mimicking neurofibromatosis type 2--case report. (4/171)
A 56-year-old male with a history of lung cancer presented with isolated metastases of adenocarcinoma in the bilateral internal auditory meatuses (IAMs), mimicking the bilateral acoustic schwannomas of neurofibromatosis type 2, and manifesting as rapidly worsening tinnitus and bilateral hearing loss. Magnetic resonance imaging showed small tumors in both IAMs with no sign of leptomeningeal metastasis. The preoperative diagnosis was neurofibromatosis type 2. Both tumors were removed and the histological diagnoses were adenocarcinoma. Neuroimaging differentiation of a solitary metastatic IAM tumor from a benign tumor is difficult, although rapidly progressive eighth cranial nerve dysfunction suggests a malignant process. Metastases should be considered as a rare diagnostic possibility in a patient with small tumors in both IAMs. (+info)Pure extradural approach for skull base lesions. (5/171)
Lesions in the parasellar and paracavernous regions can be removed by various skull base approaches involving basal osteotomies. A major complication of intradural skull base approaches is CSF leak and associated meningitis. We have managed 5 patients with skull base lesions with a pure extradural approach using wide basal osteotomies. The operative techniques are described. (+info)Infratemporal fossa approaches to the lateral skull base. (6/171)
The infra-temporal fossa approach is one of the lateral approaches to the skull base. It is indicated for the treatment of tumors such as glomus tumor, petrous apex cholesteatoma, chondroma, lower cranial nerve neuroma and nasopharyngeal cancer. In the present paper, we described the surgical anatomy of the lateral skull base and the indications for the infra-temporal fossa approach with its variants. We showed the hints and pitfalls in the procedures. Five illustrative cases are also presented. (+info)Multiple intracranial lipomas, hypogenetic corpus callosum and vestibular schwannoma: an unusual spectrum of MR findings in a patient. (7/171)
We describe imaging findings of a patient with multiple intracranial lipomas, hypogenetic corpus callosum and a vestibular schwannoma. We did not find association of intracranial lipomas and vestibular schwannoma in English literature. (+info)Imaging findings in schwannomas of the jugular foramen. (8/171)
BACKGROUND AND PURPOSE: Tumors of the cranial nerve sheath constitute 5% to 10% of all intracranial neoplasms, yet few articles have described their CT and MR characteristics. We report the imaging findings in a relatively large series of schwannomas of the jugular foramen, contrasting them with other disease entities, especially vestibular schwannomas and tumors of the glomus jugulare. METHODS: CT and/or MR studies of eight patients who underwent surgery for histologically proved schwannomas were reviewed retrospectively. One additional patient with an assumed schwannoma of the jugular foramen, who did not have surgery, was also included. RESULTS: Surgical findings showed schwannomas of the glossopharyngeal nerve in seven patients and tumor involvement of both the glossopharyngeal and vagal nerves in one patient. All tumors were partially located within the jugular foramen. Growth extending within the temporal bone was typical. Tumor extended into the posterior cranial fossa in all nine patients and produced mass effect on the brain stem and/or cerebellum in seven patients; in five patients, tumor extended below the skull base. On unenhanced CT scans, tumors were isodense with brain in six patients and hypodense in two. In seven patients, CT scans with bone algorithm showed an enlarged jugular foramen with sharply rounded bone borders and a sclerotic rim. On MR images, T1 signal from tumor was low and T2 signal was high relative to white matter in all patients. Contrast enhancement on CT and/or MR studies was strong in eight patients and moderate in one. CONCLUSION: Schwannoma of the jugular foramen is characteristically a sharply demarcated, contrast-enhancing tumor, typically centered on or based in an enlarged jugular foramen with sharply rounded bone borders and a sclerotic rim. Intraosseous extension may be marked. (+info)Cranial nerve neoplasms refer to abnormal growths or tumors that develop within or near the cranial nerves. These nerves are responsible for transmitting sensory and motor information between the brain and various parts of the head, neck, and trunk. There are 12 pairs of cranial nerves, each with a specific function and location in the skull.
Cranial nerve neoplasms can be benign or malignant and may arise from the nerve itself (schwannoma, neurofibroma) or from surrounding tissues that invade the nerve (meningioma, epidermoid cyst). The growth of these tumors can cause various symptoms depending on their size, location, and rate of growth. Common symptoms include:
* Facial weakness or numbness
* Double vision or other visual disturbances
* Hearing loss or tinnitus (ringing in the ears)
* Difficulty swallowing or speaking
* Loss of smell or taste
* Uncontrollable eye movements or drooping eyelids
Treatment for cranial nerve neoplasms depends on several factors, including the type, size, location, and extent of the tumor, as well as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or complications.
Optic nerve neoplasms refer to abnormal growths or tumors that develop within or near the optic nerve. These tumors can be benign (non-cancerous) or malignant (cancerous).
Benign optic nerve neoplasms include optic nerve meningiomas and schwannomas, which originate from the sheaths surrounding the optic nerve. They usually grow slowly and may not cause significant vision loss, but they can lead to compression of the optic nerve, resulting in visual field defects or optic disc swelling (papilledema).
Malignant optic nerve neoplasms are rare but more aggressive. The most common type is optic nerve glioma, which arises from the glial cells within the optic nerve. These tumors can quickly damage the optic nerve and cause severe vision loss.
It's important to note that any optic nerve neoplasm requires prompt medical evaluation and treatment, as they can potentially lead to significant visual impairment or even blindness if left untreated.
Cranial nerves are a set of twelve pairs of nerves that originate from the brainstem and skull, rather than the spinal cord. These nerves are responsible for transmitting sensory information (such as sight, smell, hearing, and taste) to the brain, as well as controlling various muscles in the head and neck (including those involved in chewing, swallowing, and eye movement). Each cranial nerve has a specific function and is named accordingly. For example, the optic nerve (cranial nerve II) transmits visual information from the eyes to the brain, while the vagus nerve (cranial nerve X) controls parasympathetic functions in the body such as heart rate and digestion.
Cranial nerve diseases refer to conditions that affect the cranial nerves, which are a set of 12 pairs of nerves that originate from the brainstem and control various functions in the head and neck. These functions include vision, hearing, taste, smell, movement of the eyes and face, and sensation in the face.
Diseases of the cranial nerves can result from a variety of causes, including injury, infection, inflammation, tumors, or degenerative conditions. The specific symptoms that a person experiences will depend on which cranial nerve is affected and how severely it is damaged.
For example, damage to the optic nerve (cranial nerve II) can cause vision loss or visual disturbances, while damage to the facial nerve (cranial nerve VII) can result in weakness or paralysis of the face. Other common symptoms of cranial nerve diseases include pain, numbness, tingling, and hearing loss.
Treatment for cranial nerve diseases varies depending on the underlying cause and severity of the condition. In some cases, medication or surgery may be necessary to treat the underlying cause and relieve symptoms. Physical therapy or rehabilitation may also be recommended to help individuals regain function and improve their quality of life.
Cranial nerve injuries refer to damages or trauma to one or more of the twelve cranial nerves (CN I through CN XII). These nerves originate from the brainstem and are responsible for transmitting sensory information (such as vision, hearing, smell, taste, and balance) and controlling various motor functions (like eye movement, facial expressions, swallowing, and speaking).
Cranial nerve injuries can result from various causes, including head trauma, tumors, infections, or neurological conditions. The severity of the injury may range from mild dysfunction to complete loss of function, depending on the extent of damage to the nerve. Treatment options vary based on the type and location of the injury but often involve a combination of medical management, physical therapy, surgical intervention, or rehabilitation.
The abducens nerve, also known as the sixth cranial nerve, is responsible for controlling the lateral rectus muscle of the eye, which enables the eye to move outward. Abducens nerve diseases refer to conditions that affect this nerve and can result in various symptoms, primarily affecting eye movement.
Here are some medical definitions related to abducens nerve diseases:
1. Abducens Nerve Palsy: A condition characterized by weakness or paralysis of the abducens nerve, causing difficulty in moving the affected eye outward. This results in double vision (diplopia), especially when gazing towards the side of the weakened nerve. Abducens nerve palsy can be congenital, acquired, or caused by various factors such as trauma, tumors, aneurysms, infections, or diseases like diabetes and multiple sclerosis.
2. Sixth Nerve Palsy: Another term for abducens nerve palsy, referring to the weakness or paralysis of the sixth cranial nerve.
3. Internuclear Ophthalmoplegia (INO): A neurological condition affecting eye movement, often caused by a lesion in the medial longitudinal fasciculus (MLF), a bundle of nerve fibers that connects the abducens nucleus with the oculomotor nucleus. INO results in impaired adduction (inward movement) of the eye on the side of the lesion and nystagmus (involuntary eye movements) of the abducting eye on the opposite side when attempting to look towards the side of the lesion.
4. One-and-a-Half Syndrome: A rare neurological condition characterized by a combination of INO and internuclear ophthalmoplegia with horizontal gaze palsy on the same side, caused by damage to both the abducens nerve and the paramedian pontine reticular formation (PPRF). This results in limited or no ability to move the eyes towards the side of the lesion and impaired adduction of the eye on the opposite side.
5. Brainstem Encephalitis: Inflammation of the brainstem, which can affect the abducens nerve and other cranial nerves, leading to various neurological symptoms such as diplopia (double vision), ataxia (loss of balance and coordination), and facial weakness. Brainstem encephalitis can be caused by infectious agents, autoimmune disorders, or paraneoplastic syndromes.
6. Multiple Sclerosis (MS): An autoimmune disorder characterized by inflammation and demyelination of the central nervous system, including the brainstem and optic nerves. MS can cause various neurological symptoms, such as diplopia, nystagmus, and INO, due to damage to the abducens nerve and other cranial nerves.
7. Wernicke's Encephalopathy: A neurological disorder caused by thiamine (vitamin B1) deficiency, often seen in alcoholics or individuals with malnutrition. Wernicke's encephalopathy can affect the brainstem and cause various symptoms such as diplopia, ataxia, confusion, and oculomotor abnormalities.
8. Pontine Glioma: A rare type of brain tumor that arises from the glial cells in the pons (a part of the brainstem). Pontine gliomas can cause various neurological symptoms such as diplopia, facial weakness, and difficulty swallowing due to their location in the brainstem.
9. Brainstem Cavernous Malformation: A benign vascular lesion that arises from the small blood vessels in the brainstem. Brainstem cavernous malformations can cause various neurological symptoms such as diplopia, ataxia, and facial weakness due to their location in the brainstem.
10. Pituitary Adenoma: A benign tumor that arises from the pituitary gland, located at the base of the brain. Large pituitary adenomas can compress the optic nerves and cause various visual symptoms such as diplopia, visual field defects, and decreased vision.
11. Craniopharyngioma: A benign tumor that arises from the remnants of the Rathke's pouch, a structure that gives rise to the anterior pituitary gland. Craniopharyngiomas can cause various neurological and endocrine symptoms such as diplopia, visual field defects, headaches, and hormonal imbalances due to their location near the optic nerves and pituitary gland.
12. Meningioma: A benign tumor that arises from the meninges, the protective covering of the brain and spinal cord. Meningiomas can cause various neurological symptoms such as diplopia, headaches, and seizures depending on their location in the brain or spinal cord.
13. Chordoma: A rare type of malignant tumor that arises from the remnants of the notochord, a structure that gives rise to the spine during embryonic development. Chordomas can cause various neurological and endocrine symptoms such as diplopia, visual field defects, headaches, and hormonal imbalances due to their location near the brainstem and spinal cord.
14. Metastatic Brain Tumors: Malignant tumors that spread from other parts of the body to the brain. Metastatic brain tumors can cause various neurological symptoms such as diplopia, headaches, seizures, and cognitive impairment depending on their location in the brain.
15. Other Rare Brain Tumors: There are many other rare types of brain tumors that can cause diplopia or other neurological symptoms, including gliomas, ependymomas, pineal region tumors, and others. These tumors require specialized diagnosis and treatment by neuro-oncologists and neurosurgeons with expertise in these rare conditions.
In summary, diplopia can be caused by various brain tumors, including pituitary adenomas, meningiomas, chordomas, metastatic brain tumors, and other rare types of tumors. It is important to seek medical attention promptly if you experience diplopia or other neurological symptoms, as early diagnosis and treatment can improve outcomes and quality of life.
The facial nerve, also known as the seventh cranial nerve (CN VII), is a mixed nerve that carries both sensory and motor fibers. Its functions include controlling the muscles involved in facial expressions, taste sensation from the anterior two-thirds of the tongue, and secretomotor function to the lacrimal and salivary glands.
The facial nerve originates from the brainstem and exits the skull through the internal acoustic meatus. It then passes through the facial canal in the temporal bone before branching out to innervate various structures of the face. The main branches of the facial nerve include:
1. Temporal branch: Innervates the frontalis, corrugator supercilii, and orbicularis oculi muscles responsible for eyebrow movements and eyelid closure.
2. Zygomatic branch: Supplies the muscles that elevate the upper lip and wrinkle the nose.
3. Buccal branch: Innervates the muscles of the cheek and lips, allowing for facial expressions such as smiling and puckering.
4. Mandibular branch: Controls the muscles responsible for lower lip movement and depressing the angle of the mouth.
5. Cervical branch: Innervates the platysma muscle in the neck, which helps to depress the lower jaw and wrinkle the skin of the neck.
Damage to the facial nerve can result in various symptoms, such as facial weakness or paralysis, loss of taste sensation, and dry eyes or mouth due to impaired secretion.
The oculomotor nerve, also known as the third cranial nerve (CN III), is responsible for controlling several important eye movements and functions. Oculomotor nerve diseases refer to conditions that affect this nerve and can lead to various symptoms related to eye movement and function. Here's a medical definition of oculomotor nerve diseases:
Oculomotor nerve diseases are a group of medical disorders characterized by the dysfunction or damage to the oculomotor nerve (CN III), resulting in impaired eye movements, abnormalities in pupillary response, and potential effects on eyelid position. These conditions can be congenital, acquired, or traumatic in nature and may lead to partial or complete paralysis of the nerve. Common oculomotor nerve diseases include oculomotor nerve palsy, third nerve ganglionopathies, and compressive oculomotor neuropathies caused by various pathologies such as aneurysms, tumors, or infections.
The sciatic nerve is the largest and longest nerve in the human body, running from the lower back through the buttocks and down the legs to the feet. It is formed by the union of the ventral rami (branches) of the L4 to S3 spinal nerves. The sciatic nerve provides motor and sensory innervation to various muscles and skin areas in the lower limbs, including the hamstrings, calf muscles, and the sole of the foot. Sciatic nerve disorders or injuries can result in symptoms such as pain, numbness, tingling, or weakness in the lower back, hips, legs, and feet, known as sciatica.
The glossopharyngeal nerve, also known as the ninth cranial nerve (IX), is a mixed nerve that carries both sensory and motor fibers. It originates from the medulla oblongata in the brainstem and has several functions:
1. Sensory function: The glossopharyngeal nerve provides general sensation to the posterior third of the tongue, the tonsils, the back of the throat (pharynx), and the middle ear. It also carries taste sensations from the back one-third of the tongue.
2. Special visceral afferent function: The nerve transmits information about the stretch of the carotid artery and blood pressure to the brainstem.
3. Motor function: The glossopharyngeal nerve innervates the stylopharyngeus muscle, which helps elevate the pharynx during swallowing. It also provides parasympathetic fibers to the parotid gland, stimulating saliva production.
4. Visceral afferent function: The glossopharyngeal nerve carries information about the condition of the internal organs in the thorax and abdomen to the brainstem.
Overall, the glossopharyngeal nerve plays a crucial role in swallowing, taste, saliva production, and monitoring blood pressure and heart rate.
The oculomotor nerve, also known as the third cranial nerve (CN III), is a motor nerve that originates from the midbrain. It controls the majority of the eye muscles, including the levator palpebrae superioris muscle that raises the upper eyelid, and the extraocular muscles that enable various movements of the eye such as looking upward, downward, inward, and outward. Additionally, it carries parasympathetic fibers responsible for pupillary constriction and accommodation (focusing on near objects). Damage to this nerve can result in various ocular motor disorders, including strabismus, ptosis, and pupillary abnormalities.
Peripheral nerves are nerve fibers that transmit signals between the central nervous system (CNS, consisting of the brain and spinal cord) and the rest of the body. These nerves convey motor, sensory, and autonomic information, enabling us to move, feel, and respond to changes in our environment. They form a complex network that extends from the CNS to muscles, glands, skin, and internal organs, allowing for coordinated responses and functions throughout the body. Damage or injury to peripheral nerves can result in various neurological symptoms, such as numbness, weakness, or pain, depending on the type and severity of the damage.
Hypoglossal nerve injuries refer to damages or impairments to the twelfth cranial nerve, also known as the hypoglossal nerve. This nerve is primarily responsible for controlling the movements of the tongue.
An injury to this nerve can result in various symptoms, depending on the severity and location of the damage. These may include:
1. Deviation of the tongue to one side when protruded (usually away from the side of the lesion)
2. Weakness or paralysis of the tongue muscles
3. Difficulty with speaking, swallowing, and articulation
4. Changes in taste and sensation on the back of the tongue (in some cases)
Hypoglossal nerve injuries can occur due to various reasons, such as trauma, surgical complications, tumors, or neurological disorders like stroke or multiple sclerosis. Treatment for hypoglossal nerve injuries typically focuses on managing symptoms and may involve speech and language therapy, exercises to strengthen the tongue muscles, and, in some cases, surgical intervention.
The trigeminal nerve, also known as the fifth cranial nerve or CNV, is a paired nerve that carries both sensory and motor information. It has three major branches: ophthalmic (V1), maxillary (V2), and mandibular (V3). The ophthalmic branch provides sensation to the forehead, eyes, and upper portion of the nose; the maxillary branch supplies sensation to the lower eyelid, cheek, nasal cavity, and upper lip; and the mandibular branch is responsible for sensation in the lower lip, chin, and parts of the oral cavity, as well as motor function to the muscles involved in chewing. The trigeminal nerve plays a crucial role in sensations of touch, pain, temperature, and pressure in the face and mouth, and it also contributes to biting, chewing, and swallowing functions.
The abducens nerve, also known as the sixth cranial nerve (CN VI), is a motor nerve that controls the lateral rectus muscle of the eye. This muscle is responsible for moving the eye away from the midline (towards the temple) and enables the eyes to look towards the side while keeping them aligned. Any damage or dysfunction of the abducens nerve can result in strabismus, where the eyes are misaligned and point in different directions, specifically an adduction deficit, also known as abducens palsy or sixth nerve palsy.
The vestibulocochlear nerve, also known as the auditory-vestibular nerve or cranial nerve VIII, is a paired peripheral nerve that transmits sensory information from the inner ear to the brain. It has two distinct parts: the cochlear part and the vestibular part.
The cochlear part is responsible for hearing and transmits sound signals from the cochlea to the brain. The vestibular part, on the other hand, is responsible for maintaining balance and spatial orientation by transmitting information about head movement and position from the vestibular apparatus (utricle, saccule, and semicircular canals) in the inner ear to the brain.
Together, these two parts of the vestibulocochlear nerve play a crucial role in our ability to hear and maintain balance. Damage to this nerve can result in hearing loss, tinnitus (ringing in the ears), vertigo (dizziness), or balance problems.
The optic nerve, also known as the second cranial nerve, is the nerve that transmits visual information from the retina to the brain. It is composed of approximately one million nerve fibers that carry signals related to vision, such as light intensity and color, from the eye's photoreceptor cells (rods and cones) to the visual cortex in the brain. The optic nerve is responsible for carrying this visual information so that it can be processed and interpreted by the brain, allowing us to see and perceive our surroundings. Damage to the optic nerve can result in vision loss or impairment.
Nerve fibers are specialized structures that constitute the long, slender processes (axons) of neurons (nerve cells). They are responsible for conducting electrical impulses, known as action potentials, away from the cell body and transmitting them to other neurons or effector organs such as muscles and glands. Nerve fibers are often surrounded by supportive cells called glial cells and are grouped together to form nerve bundles or nerves. These fibers can be myelinated (covered with a fatty insulating sheath called myelin) or unmyelinated, which influences the speed of impulse transmission.
Möbius syndrome is a rare neurological disorder characterized by congenital facial palsy and abducens palsy, which are paralyses of the muscles that control lateral movement of the eye and facial expression. The condition is present at birth and is thought to be caused by underdevelopment of the cranial nerves (VI and VII) during embryonic development.
Individuals with Möbius syndrome may have a variety of symptoms, including:
* Inability to move the eyes from side to side
* Absent or weak facial expressions
* Difficulty with sucking, swallowing, and speaking
* Dental abnormalities
* Hearing loss
* Limb abnormalities
Möbius syndrome is typically diagnosed based on physical examination and medical history. There is no cure for the condition, but treatment may include physical therapy, speech therapy, and surgical interventions to improve function and appearance. The exact cause of Möbius syndrome is not known, but it is believed to be related to genetic or environmental factors during fetal development.
Nerve compression syndromes refer to a group of conditions characterized by the pressure or irritation of a peripheral nerve, causing various symptoms such as pain, numbness, tingling, and weakness in the affected area. This compression can occur due to several reasons, including injury, repetitive motion, bone spurs, tumors, or swelling. Common examples of nerve compression syndromes include carpal tunnel syndrome, cubital tunnel syndrome, radial nerve compression, and ulnar nerve entrapment at the wrist or elbow. Treatment options may include physical therapy, splinting, medications, injections, or surgery, depending on the severity and underlying cause of the condition.
The accessory nerve, also known as the eleventh cranial nerve (XI), has both a cranial and spinal component. It primarily controls the function of certain muscles in the back of the neck and shoulder.
The cranial part arises from nuclei in the brainstem and innervates some of the muscles that help with head rotation, including the sternocleidomastoid muscle. The spinal root originates from nerve roots in the upper spinal cord (C1-C5), exits the spine, and joins the cranial part to form a single trunk. This trunk then innervates the trapezius muscle, which helps with shoulder movement and stability.
Damage to the accessory nerve can result in weakness or paralysis of the affected muscles, causing symptoms such as difficulty turning the head, weak shoulder shrugging, or winged scapula (a condition where the shoulder blade protrudes from the back).
Laryngeal nerve injuries refer to damages or injuries to the recurrent laryngeal nerve (RLN) and/or the superior laryngeal nerve (SLN), which are the primary nerves that supply the larynx, or voice box. These nerves play crucial roles in controlling the vocal cord movements and protecting the airway during swallowing.
The recurrent laryngeal nerve provides motor function to all intrinsic muscles of the larynx, except for the cricothyroid muscle, which is innervated by the superior laryngeal nerve. The RLN also carries sensory fibers from a small area of the mucous membrane below the vocal folds.
Injuries to these nerves can result in voice changes, breathing difficulties, and swallowing problems. Depending on the severity and location of the injury, patients may experience hoarseness, weak voice, breathy voice, coughing while swallowing, or even complete airway obstruction in severe cases. Laryngeal nerve injuries can occur due to various reasons, such as surgical complications (e.g., thyroid, esophageal, and cardiovascular surgeries), neck trauma, tumors, infections, or iatrogenic causes.
Ophthalmoplegia is a medical term that refers to the paralysis or weakness of the eye muscles, which can result in double vision (diplopia) or difficulty moving the eyes. It can be caused by various conditions, including nerve damage, muscle disorders, or neurological diseases such as myasthenia gravis or multiple sclerosis. Ophthalmoplegia can affect one or more eye muscles and can be partial or complete. Depending on the underlying cause, ophthalmoplegia may be treatable with medications, surgery, or other interventions.
Facial paralysis is a loss of facial movement due to damage or dysfunction of the facial nerve (cranial nerve VII). This nerve controls the muscles involved in facial expressions, such as smiling, frowning, and closing the eyes. Damage to one side of the facial nerve can cause weakness or paralysis on that side of the face.
Facial paralysis can result from various conditions, including:
1. Bell's palsy - an idiopathic (unknown cause) inflammation of the facial nerve
2. Trauma - skull fractures, facial injuries, or surgical trauma to the facial nerve
3. Infections - Lyme disease, herpes zoster (shingles), HIV/AIDS, or bacterial infections like meningitis
4. Tumors - benign or malignant growths that compress or invade the facial nerve
5. Stroke - damage to the brainstem where the facial nerve originates
6. Congenital conditions - some people are born with facial paralysis due to genetic factors or birth trauma
Symptoms of facial paralysis may include:
* Inability to move one or more parts of the face, such as the eyebrows, eyelids, mouth, or cheeks
* Drooping of the affected side of the face
* Difficulty closing the eye on the affected side
* Changes in saliva and tear production
* Altered sense of taste
* Pain around the ear or jaw
* Speech difficulties due to weakened facial muscles
Treatment for facial paralysis depends on the underlying cause. In some cases, such as Bell's palsy, spontaneous recovery may occur within a few weeks to months. However, physical therapy, medications, and surgical interventions might be necessary in other situations to improve function and minimize complications.
Trigeminal nerve diseases refer to conditions that affect the trigeminal nerve, which is one of the cranial nerves responsible for sensations in the face and motor functions such as biting and chewing. The trigeminal nerve has three branches: ophthalmic, maxillary, and mandibular, which innervate different parts of the face and head.
Trigeminal nerve diseases can cause various symptoms, including facial pain, numbness, tingling, or weakness. Some common trigeminal nerve diseases include:
1. Trigeminal neuralgia: A chronic pain condition that affects the trigeminal nerve, causing intense, stabbing, or electric shock-like pain in the face.
2. Hemifacial spasm: A neuromuscular disorder that causes involuntary muscle spasms on one side of the face, often affecting the muscles around the eye and mouth.
3. Trigeminal neuropathy: Damage or injury to the trigeminal nerve, which can result in numbness, tingling, or weakness in the face.
4. Herpes zoster oticus (Ramsay Hunt syndrome): A viral infection that affects the facial nerve and geniculate ganglion of the trigeminal nerve, causing facial paralysis, ear pain, and a rash around the ear.
5. Microvascular compression: Compression of the trigeminal nerve by a blood vessel, which can cause symptoms similar to trigeminal neuralgia.
Treatment for trigeminal nerve diseases depends on the specific condition and its severity. Treatment options may include medication, surgery, or radiation therapy.
The vestibulocochlear nerve, also known as the 8th cranial nerve, is responsible for transmitting sound and balance information from the inner ear to the brain. Vestibulocochlear nerve diseases refer to conditions that affect this nerve and can result in hearing loss, vertigo, and balance problems.
These diseases can be caused by various factors, including genetics, infection, trauma, tumors, or degeneration. Some examples of vestibulocochlear nerve diseases include:
1. Vestibular neuritis: an inner ear infection that causes severe vertigo, nausea, and balance problems.
2. Labyrinthitis: an inner ear infection that affects both the vestibular and cochlear nerves, causing vertigo, hearing loss, and tinnitus.
3. Acoustic neuroma: a benign tumor that grows on the vestibulocochlear nerve, causing hearing loss, tinnitus, and balance problems.
4. Meniere's disease: a inner ear disorder that causes vertigo, hearing loss, tinnitus, and a feeling of fullness in the ear.
5. Ototoxicity: damage to the inner ear caused by certain medications or chemicals that can result in hearing loss and balance problems.
6. Vestibular migraine: a type of migraine that is associated with vertigo, dizziness, and balance problems.
Treatment for vestibulocochlear nerve diseases varies depending on the specific condition and its severity. It may include medication, physical therapy, surgery, or a combination of these approaches.
Skull base neoplasms refer to abnormal growths or tumors located in the skull base, which is the region where the skull meets the spine and where the brain connects with the blood vessels and nerves that supply the head and neck. These neoplasms can be benign (non-cancerous) or malignant (cancerous), and they can arise from various types of cells in this area, including bone, nerve, glandular, and vascular tissue.
Skull base neoplasms can cause a range of symptoms depending on their size, location, and growth rate. Some common symptoms include headaches, vision changes, hearing loss, facial numbness or weakness, difficulty swallowing, and balance problems. Treatment options for skull base neoplasms may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. The specific treatment plan will depend on the type, size, location, and stage of the tumor, as well as the patient's overall health and medical history.
Nerve regeneration is the process of regrowth and restoration of functional nerve connections following damage or injury to the nervous system. This complex process involves various cellular and molecular events, such as the activation of support cells called glia, the sprouting of surviving nerve fibers (axons), and the reformation of neural circuits. The goal of nerve regeneration is to enable the restoration of normal sensory, motor, and autonomic functions impaired due to nerve damage or injury.
The trochlear nerve, also known as the fourth cranial nerve (CN IV), is a nerve that originates in the midbrain and innervates the superior oblique muscle of the eye. This muscle helps with the downward and outward movement of the eye, playing a crucial role in controlling eye movements and maintaining binocular vision. The trochlear nerve's main function is to provide motor (efferent) innervation to the superior oblique muscle, enabling fine-tuning of eye movements during activities such as reading, writing, or driving. Damage to this nerve can result in vertical diplopia (double vision), strabismus (eye misalignment), and other visual impairments.
Trigeminal neuralgia is a chronic pain condition that affects the trigeminal nerve, which is one of the largest nerves in the head. It carries sensations from the face to the brain.
Medically, trigeminal neuralgia is defined as a neuropathic disorder characterized by episodes of intense, stabbing, electric shock-like pain in the areas of the face supplied by the trigeminal nerve (the ophthalmic, maxillary, and mandibular divisions). The pain can be triggered by simple activities such as talking, eating, brushing teeth, or even touching the face lightly.
The condition is more common in women over 50, but it can occur at any age and in either gender. While the exact cause of trigeminal neuralgia is not always known, it can sometimes be related to pressure on the trigeminal nerve from a nearby blood vessel or other causes such as multiple sclerosis. Treatment typically involves medications, surgery, or a combination of both.
Paralysis is a loss of muscle function in part or all of your body. It can be localized, affecting only one specific area, or generalized, impacting multiple areas or even the entire body. Paralysis often occurs when something goes wrong with the way messages pass between your brain and muscles. In most cases, paralysis is caused by damage to the nervous system, especially the spinal cord. Other causes include stroke, trauma, infections, and various neurological disorders.
It's important to note that paralysis doesn't always mean a total loss of movement or feeling. Sometimes, it may just cause weakness or numbness in the affected area. The severity and extent of paralysis depend on the underlying cause and the location of the damage in the nervous system.
The cerebellopontine angle (CPA) is a narrow space located at the junction of the brainstem and the cerebellum, where the pons and cerebellum meet. This region is filled with several important nerves, blood vessels, and membranous coverings called meninges. The CPA is a common site for various neurological disorders because it contains critical structures such as:
1. Cerebellum: A part of the brain responsible for coordinating muscle movements, maintaining balance, and fine-tuning motor skills.
2. Pons: A portion of the brainstem that plays a role in several vital functions, including facial movements, taste sensation, sleep regulation, and respiration.
3. Cranial nerves: The CPA is home to the following cranial nerves:
* Vestibulocochlear nerve (CN VIII): This nerve has two components - cochlear and vestibular. The cochlear part is responsible for hearing, while the vestibular part contributes to balance and eye movement.
* Facial nerve (CN VII): This nerve controls facial expressions, taste sensation in the anterior two-thirds of the tongue, salivary gland function, and lacrimation (tear production).
4. Blood vessels: The CPA contains critical blood vessels like the anterior inferior cerebellar artery (AICA), which supplies blood to various parts of the brainstem, cerebellum, and cranial nerves.
5. Meninges: These are protective membranes surrounding the brain and spinal cord. In the CPA, the meninges include the dura mater, arachnoid mater, and pia mater.
Disorders that can affect the structures in the cerebellopontine angle include acoustic neuromas (vestibular schwannomas), meningiomas, epidermoids, and arteriovenous malformations. These conditions may cause symptoms such as hearing loss, tinnitus (ringing in the ears), vertigo (dizziness), facial weakness or numbness, difficulty swallowing, and imbalance.
Facial nerve diseases refer to a group of medical conditions that affect the function of the facial nerve, also known as the seventh cranial nerve. This nerve is responsible for controlling the muscles of facial expression, and it also carries sensory information from the taste buds in the front two-thirds of the tongue, and regulates saliva flow and tear production.
Facial nerve diseases can cause a variety of symptoms, depending on the specific location and extent of the nerve damage. Common symptoms include:
* Facial weakness or paralysis on one or both sides of the face
* Drooping of the eyelid and corner of the mouth
* Difficulty closing the eye or keeping it closed
* Changes in taste sensation or dryness of the mouth and eyes
* Abnormal sensitivity to sound (hyperacusis)
* Twitching or spasms of the facial muscles
Facial nerve diseases can be caused by a variety of factors, including:
* Infections such as Bell's palsy, Ramsay Hunt syndrome, and Lyme disease
* Trauma or injury to the face or skull
* Tumors that compress or invade the facial nerve
* Neurological conditions such as multiple sclerosis or Guillain-Barre syndrome
* Genetic disorders such as Moebius syndrome or hemifacial microsomia
Treatment for facial nerve diseases depends on the underlying cause and severity of the symptoms. In some cases, medication, physical therapy, or surgery may be necessary to restore function and relieve symptoms.
Facial nerve injuries refer to damages or trauma inflicted on the facial nerve, also known as the seventh cranial nerve (CN VII). This nerve is responsible for controlling the muscles involved in facial expressions, eyelid movement, and taste sensation in the front two-thirds of the tongue.
There are two main types of facial nerve injuries:
1. Peripheral facial nerve injury: This type of injury occurs when damage affects the facial nerve outside the skull base, usually due to trauma from cuts, blunt force, or surgical procedures in the parotid gland or neck region. The injury may result in weakness or paralysis on one side of the face, known as Bell's palsy, and may also impact taste sensation and salivary function.
2. Central facial nerve injury: This type of injury occurs when damage affects the facial nerve within the skull base, often due to stroke, brain tumors, or traumatic brain injuries. Central facial nerve injuries typically result in weakness or paralysis only on the lower half of the face, as the upper motor neurons responsible for controlling the upper face receive innervation from both sides of the brain.
Treatment for facial nerve injuries depends on the severity and location of the damage. For mild to moderate injuries, physical therapy, protective eyewear, and medications like corticosteroids and antivirals may be prescribed. Severe cases might require surgical intervention, such as nerve grafts or muscle transfers, to restore function. In some instances, facial nerve injuries may heal on their own over time, particularly when the injury is mild and there is no ongoing compression or tension on the nerve.
A Trochlear nerve injury, also known as Fourth cranial nerve palsy, refers to damage or dysfunction of the fourth cranial nerve (trochlear nerve). This nerve is responsible for controlling the movement of the eye's superior oblique muscle, which helps in downward and outward movement of the eye.
Trochlear nerve injuries can result in vertical diplopia (double vision), where images appear double when looking downwards or to the side. The diplopia may be worse when looking down and out, such as when walking down stairs or reading.
The injury can be caused by various factors including head trauma, increased intracranial pressure, tumors, aneurysms, or other neurological conditions. Treatment options depend on the severity and cause of the injury and may include eye patches, prism lenses, or surgical intervention in some cases.
The hypoglossal nerve, also known as the 12th cranial nerve (CN XII), is primarily responsible for innervating the muscles of the tongue, allowing for its movement and function. These muscles include the intrinsic muscles that alter the shape of the tongue and the extrinsic muscles that position it in the oral cavity. The hypoglossal nerve also has some minor contributions to the innervation of two muscles in the neck: the sternocleidomastoid and the trapezius. These functions are related to head turning and maintaining head position. Any damage to this nerve can lead to weakness or paralysis of the tongue, causing difficulty with speech, swallowing, and tongue movements.
A Glomus Jugulare Tumor is a rare, usually benign, slow-growing tumor that develops from the glomus body, a small collection of modified blood vessels involved in temperature regulation, located near the jugular bulb in the skull. This type of tumor can cause symptoms such as hearing loss, pulsatile tinnitus (a rhythmic sound in the ear), and cranial nerve palsies due to its proximity to critical structures in the head and neck. Treatment typically involves surgical removal or radiation therapy.
A nerve block is a medical procedure in which an anesthetic or neurolytic agent is injected near a specific nerve or bundle of nerves to block the transmission of pain signals from that area to the brain. This technique can be used for both diagnostic and therapeutic purposes, such as identifying the source of pain, providing temporary or prolonged relief, or facilitating surgical procedures in the affected region.
The injection typically contains a local anesthetic like lidocaine or bupivacaine, which numbs the nerve, preventing it from transmitting pain signals. In some cases, steroids may also be added to reduce inflammation and provide longer-lasting relief. Depending on the type of nerve block and its intended use, the injection might be administered close to the spine (neuraxial blocks), at peripheral nerves (peripheral nerve blocks), or around the sympathetic nervous system (sympathetic nerve blocks).
While nerve blocks are generally safe, they can have side effects such as infection, bleeding, nerve damage, or in rare cases, systemic toxicity from the anesthetic agent. It is essential to consult with a qualified medical professional before undergoing this procedure to ensure proper evaluation, technique, and post-procedure care.
Nerve endings, also known as terminal branches or sensory receptors, are the specialized structures present at the termination point of nerve fibers (axons) that transmit electrical signals to and from the central nervous system (CNS). They primarily function in detecting changes in the external environment or internal body conditions and converting them into electrical impulses.
There are several types of nerve endings, including:
1. Free Nerve Endings: These are unencapsulated nerve endings that respond to various stimuli like temperature, pain, and touch. They are widely distributed throughout the body, especially in the skin, mucous membranes, and visceral organs.
2. Encapsulated Nerve Endings: These are wrapped by specialized connective tissue sheaths, which can modify their sensitivity to specific stimuli. Examples include Pacinian corpuscles (responsible for detecting deep pressure and vibration), Meissner's corpuscles (for light touch), Ruffini endings (for stretch and pressure), and Merkel cells (for sustained touch).
3. Specialised Nerve Endings: These are nerve endings that respond to specific stimuli, such as auditory, visual, olfactory, gustatory, and vestibular information. They include hair cells in the inner ear, photoreceptors in the retina, taste buds in the tongue, and olfactory receptors in the nasal cavity.
Nerve endings play a crucial role in relaying sensory information to the CNS for processing and initiating appropriate responses, such as reflex actions or conscious perception of the environment.
The petrous bone is a part of the temporal bone, one of the 22 bones in the human skull. It is a thick and irregularly shaped bone located at the base of the skull and forms part of the ear and the cranial cavity. The petrous bone contains the cochlea, vestibule, and semicircular canals of the inner ear, which are responsible for hearing and balance. It also helps protect the brain from injury by forming part of the bony structure surrounding the brain.
The term "petrous" comes from the Latin word "petrosus," meaning "stony" or "rock-like," which describes the hard and dense nature of this bone. The petrous bone is one of the densest bones in the human body, making it highly resistant to fractures and other forms of damage.
In medical terminology, the term "petrous" may also be used to describe any structure that resembles a rock or is hard and dense, such as the petrous apex, which refers to the portion of the petrous bone that points towards the sphenoid bone.
The sural nerve is a purely sensory peripheral nerve in the lower leg and foot. It provides sensation to the outer ( lateral) aspect of the little toe and the adjacent side of the fourth toe, as well as a small portion of the skin on the back of the leg between the ankle and knee joints.
The sural nerve is formed by the union of branches from the tibial and common fibular nerves (branches of the sciatic nerve) in the lower leg. It runs down the calf, behind the lateral malleolus (the bony prominence on the outside of the ankle), and into the foot.
The sural nerve is often used as a donor nerve during nerve grafting procedures due to its consistent anatomy and relatively low risk for morbidity at the donor site.
The cavernous sinus is a venous structure located in the middle cranial fossa, which is a depression in the skull that houses several important nerves and blood vessels. The cavernous sinus is situated on either side of the sphenoid bone, near the base of the skull, and it contains several important structures:
* The internal carotid artery, which supplies oxygenated blood to the brain
* The abducens nerve (cranial nerve VI), which controls lateral movement of the eye
* The oculomotor nerve (cranial nerve III), which controls most of the muscles that move the eye
* The trochlear nerve (cranial nerve IV), which controls one of the muscles that moves the eye
* The ophthalmic and maxillary divisions of the trigeminal nerve (cranial nerve V), which transmit sensory information from the face and head
The cavernous sinus is an important structure because it serves as a conduit for several critical nerves and blood vessels. However, it is also vulnerable to various pathological conditions such as thrombosis (blood clots), infection, tumors, or aneurysms, which can lead to serious neurological deficits or even death.
The median nerve is one of the major nerves in the human body, providing sensation and motor function to parts of the arm and hand. It originates from the brachial plexus, a network of nerves that arise from the spinal cord in the neck. The median nerve travels down the arm, passing through the cubital tunnel at the elbow, and continues into the forearm and hand.
In the hand, the median nerve supplies sensation to the palm side of the thumb, index finger, middle finger, and half of the ring finger. It also provides motor function to some of the muscles that control finger movements, allowing for flexion of the fingers and opposition of the thumb.
Damage to the median nerve can result in a condition called carpal tunnel syndrome, which is characterized by numbness, tingling, and weakness in the hand and fingers.
Pancreatic neoplasms refer to abnormal growths in the pancreas that can be benign or malignant. The pancreas is a gland located behind the stomach that produces hormones and digestive enzymes. Pancreatic neoplasms can interfere with the normal functioning of the pancreas, leading to various health complications.
Benign pancreatic neoplasms are non-cancerous growths that do not spread to other parts of the body. They are usually removed through surgery to prevent any potential complications, such as blocking the bile duct or causing pain.
Malignant pancreatic neoplasms, also known as pancreatic cancer, are cancerous growths that can invade and destroy surrounding tissues and organs. They can also spread (metastasize) to other parts of the body, such as the liver, lungs, or bones. Pancreatic cancer is often aggressive and difficult to treat, with a poor prognosis.
There are several types of pancreatic neoplasms, including adenocarcinomas, neuroendocrine tumors, solid pseudopapillary neoplasms, and cystic neoplasms. The specific type of neoplasm is determined through various diagnostic tests, such as imaging studies, biopsies, and blood tests. Treatment options depend on the type, stage, and location of the neoplasm, as well as the patient's overall health and preferences.
A nerve crush injury is a type of peripheral nerve injury that occurs when there is excessive pressure or compression applied to a nerve, causing it to become damaged or dysfunctional. This can happen due to various reasons such as trauma from accidents, surgical errors, or prolonged pressure on the nerve from tight casts, clothing, or positions.
The compression disrupts the normal functioning of the nerve, leading to symptoms such as numbness, tingling, weakness, or pain in the affected area. In severe cases, a nerve crush injury can cause permanent damage to the nerve, leading to long-term disability or loss of function. Treatment for nerve crush injuries typically involves relieving the pressure on the nerve, providing supportive care, and in some cases, surgical intervention may be necessary to repair the damaged nerve.
Peripheral nerve injuries refer to damage or trauma to the peripheral nerves, which are the nerves outside the brain and spinal cord. These nerves transmit information between the central nervous system (CNS) and the rest of the body, including sensory, motor, and autonomic functions. Peripheral nerve injuries can result in various symptoms, depending on the type and severity of the injury, such as numbness, tingling, weakness, or paralysis in the affected area.
Peripheral nerve injuries are classified into three main categories based on the degree of damage:
1. Neuropraxia: This is the mildest form of nerve injury, where the nerve remains intact but its function is disrupted due to a local conduction block. The nerve fiber is damaged, but the supporting structures remain intact. Recovery usually occurs within 6-12 weeks without any residual deficits.
2. Axonotmesis: In this type of injury, there is damage to both the axons and the supporting structures (endoneurium, perineurium). The nerve fibers are disrupted, but the connective tissue sheaths remain intact. Recovery can take several months or even up to a year, and it may be incomplete, with some residual deficits possible.
3. Neurotmesis: This is the most severe form of nerve injury, where there is complete disruption of the nerve fibers and supporting structures (endoneurium, perineurium, epineurium). Recovery is unlikely without surgical intervention, which may involve nerve grafting or repair.
Peripheral nerve injuries can be caused by various factors, including trauma, compression, stretching, lacerations, or chemical exposure. Treatment options depend on the type and severity of the injury and may include conservative management, such as physical therapy and pain management, or surgical intervention for more severe cases.
The Tibial nerve is a major branch of the sciatic nerve that originates in the lower back and runs through the buttock and leg. It provides motor (nerve impulses that control muscle movement) and sensory (nerve impulses that convey information about touch, temperature, and pain) innervation to several muscles and skin regions in the lower limb.
More specifically, the Tibial nerve supplies the following structures:
1. Motor Innervation: The Tibial nerve provides motor innervation to the muscles in the back of the leg (posterior compartment), including the calf muscles (gastrocnemius and soleus) and the small muscles in the foot (intrinsic muscles). These muscles are responsible for plantarflexion (pointing the foot downward) and inversion (turning the foot inward) of the foot.
2. Sensory Innervation: The Tibial nerve provides sensory innervation to the skin on the sole of the foot, as well as the heel and some parts of the lower leg.
The Tibial nerve travels down the leg, passing behind the knee and through the calf, where it eventually joins with the common fibular (peroneal) nerve to form the tibial-fibular trunk. This trunk then divides into several smaller nerves that innervate the foot's intrinsic muscles and skin.
Damage or injury to the Tibial nerve can result in various symptoms, such as weakness or paralysis of the calf and foot muscles, numbness or tingling sensations in the sole of the foot, and difficulty walking or standing on tiptoes.
The skull base is the lower part of the skull that forms the floor of the cranial cavity and the roof of the facial skeleton. It is a complex anatomical region composed of several bones, including the frontal, sphenoid, temporal, occipital, and ethmoid bones. The skull base supports the brain and contains openings for blood vessels and nerves that travel between the brain and the face or neck. The skull base can be divided into three regions: the anterior cranial fossa, middle cranial fossa, and posterior cranial fossa, which house different parts of the brain.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
The Ulnar nerve is one of the major nerves in the forearm and hand, which provides motor function to the majority of the intrinsic muscles of the hand (except for those innervated by the median nerve) and sensory innervation to the little finger and half of the ring finger. It originates from the brachial plexus, passes through the cubital tunnel at the elbow, and continues down the forearm, where it runs close to the ulna bone. The ulnar nerve then passes through the Guyon's canal in the wrist before branching out to innervate the hand muscles and provide sensation to the skin on the little finger and half of the ring finger.
Diplopia is a medical term that refers to the condition where a person sees two images of a single object. It is commonly known as double vision. This can occur due to various reasons, such as nerve damage or misalignment of the eyes. Diplopia can be temporary or chronic and can affect one or both eyes. If you're experiencing diplopia, it's essential to consult an eye care professional for proper evaluation and treatment.
A neurilemmoma, also known as schwannoma or peripheral nerve sheath tumor, is a benign, slow-growing tumor that arises from the Schwann cells, which produce the myelin sheath that surrounds and insulates peripheral nerves. These tumors can occur anywhere along the course of a peripheral nerve, but they most commonly affect the acoustic nerve (vestibulocochlear nerve), leading to a type of tumor called vestibular schwannoma or acoustic neuroma. Neurilemmomas are typically encapsulated and do not invade the surrounding tissue, although larger ones may cause pressure-related symptoms due to compression of nearby structures. Rarely, these tumors can undergo malignant transformation, leading to a condition called malignant peripheral nerve sheath tumor or neurofibrosarcoma.
The glossopharyngeal nerve, also known as the ninth cranial nerve (CN IX), is primarily responsible for providing motor innervation to the stylopharyngeus muscle and sensory innervation to parts of the pharynx, middle ear, and posterior tongue. It also plays a role in the reflexive control of heart rate via the baroreceptors located in the carotid sinus.
Glossopharyngeal nerve diseases refer to conditions that affect the function of this nerve, leading to various symptoms. These diseases can be classified into two main categories: peripheral and central. Peripheral disorders are caused by damage or injury to the nerve itself, while central disorders result from problems in the brainstem where the glossopharyngeal nerve originates.
Some examples of glossopharyngeal nerve diseases include:
1. Glossopharyngeal neuralgia: A rare condition characterized by severe, stabbing pain in the throat, ear, or tongue, often triggered by swallowing or talking. This disorder may be caused by compression of the nerve by blood vessels or other structures.
2. Infections: Bacterial and viral infections can cause inflammation and damage to the glossopharyngeal nerve, leading to dysfunction. Examples include Lyme disease, herpes zoster (shingles), and meningitis.
3. Tumors: Benign or malignant growths in the head and neck region can compress and injure the glossopharyngeal nerve, resulting in symptoms related to its dysfunction.
4. Trauma: Direct trauma to the neck or skull base can damage the glossopharyngeal nerve, causing various deficits depending on the severity of the injury.
5. Neurological disorders: Conditions such as multiple sclerosis and stroke can affect the central connections of the glossopharyngeal nerve in the brainstem, leading to dysfunction.
6. Genetic conditions: Rare genetic disorders like Moersch-Woltman syndrome (also known as stiff person syndrome) can involve the glossopharyngeal nerve and cause symptoms related to its dysfunction.
Symptoms of glossopharyngeal nerve dysfunction may include difficulty swallowing, hoarseness, loss of taste on the back of the tongue, decreased sensation in the throat or ear, and pain in the neck, throat, or ear. Treatment for these conditions depends on the underlying cause and may involve medications, surgery, or other interventions to address the specific problem.
The posterior cranial fossa is a term used in anatomy to refer to the portion of the skull that forms the lower, back part of the cranial cavity. It is located between the occipital bone and the temporal bones, and it contains several important structures including the cerebellum, pons, medulla oblongata, and the lower cranial nerves (IX-XII). The posterior fossa also contains the foramen magnum, which is a large opening through which the spinal cord connects to the brainstem. This region of the skull is protected by the occipital bone, which forms the base of the skull and provides attachment for several neck muscles.
Neoplasms are abnormal growths of cells or tissues in the body that serve no physiological function. They can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow growing and do not spread to other parts of the body, while malignant neoplasms are aggressive, invasive, and can metastasize to distant sites.
Neoplasms occur when there is a dysregulation in the normal process of cell division and differentiation, leading to uncontrolled growth and accumulation of cells. This can result from genetic mutations or other factors such as viral infections, environmental exposures, or hormonal imbalances.
Neoplasms can develop in any organ or tissue of the body and can cause various symptoms depending on their size, location, and type. Treatment options for neoplasms include surgery, radiation therapy, chemotherapy, immunotherapy, and targeted therapy, among others.
The femoral nerve is a major nerve in the thigh region of the human body. It originates from the lumbar plexus, specifically from the ventral rami (anterior divisions) of the second, third, and fourth lumbar nerves (L2-L4). The femoral nerve provides motor and sensory innervation to various muscles and areas in the lower limb.
Motor Innervation:
The femoral nerve is responsible for providing motor innervation to several muscles in the anterior compartment of the thigh, including:
1. Iliacus muscle
2. Psoas major muscle
3. Quadriceps femoris muscle (consisting of four heads: rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius)
These muscles are involved in hip flexion, knee extension, and stabilization of the hip joint.
Sensory Innervation:
The sensory distribution of the femoral nerve includes:
1. Anterior and medial aspects of the thigh
2. Skin over the anterior aspect of the knee and lower leg (via the saphenous nerve, a branch of the femoral nerve)
The saphenous nerve provides sensation to the skin on the inner side of the leg and foot, as well as the medial malleolus (the bony bump on the inside of the ankle).
In summary, the femoral nerve is a crucial component of the lumbar plexus that controls motor functions in the anterior thigh muscles and provides sensory innervation to the anterior and medial aspects of the thigh and lower leg.
Spinal nerves are the bundles of nerve fibers that transmit signals between the spinal cord and the rest of the body. There are 31 pairs of spinal nerves in the human body, which can be divided into five regions: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each spinal nerve carries both sensory information (such as touch, temperature, and pain) from the periphery to the spinal cord, and motor information (such as muscle control) from the spinal cord to the muscles and other structures in the body. Spinal nerves also contain autonomic fibers that regulate involuntary functions such as heart rate, digestion, and blood pressure.
The cochlear nerve, also known as the auditory nerve, is the sensory nerve that transmits sound signals from the inner ear to the brain. It consists of two parts: the outer spiral ganglion and the inner vestibular portion. The spiral ganglion contains the cell bodies of the bipolar neurons that receive input from hair cells in the cochlea, which is the snail-shaped organ in the inner ear responsible for hearing. These neurons then send their axons to form the cochlear nerve, which travels through the internal auditory meatus and synapses with neurons in the cochlear nuclei located in the brainstem.
Damage to the cochlear nerve can result in hearing loss or deafness, depending on the severity of the injury. Common causes of cochlear nerve damage include acoustic trauma, such as exposure to loud noises, viral infections, meningitis, and tumors affecting the nerve or surrounding structures. In some cases, cochlear nerve damage may be treated with hearing aids, cochlear implants, or other assistive devices to help restore or improve hearing function.
 C72
C72
Fundus photography
List of ICD-9 codes 140-239: neoplasms
Extramedullary hematopoiesis
Infratemporal fossa
Parinaud's syndrome
Tolosa-Hunt syndrome
List of MeSH codes (C04)
Genetics of migraine headaches
Idiopathic orbital inflammatory disease
Orbit (anatomy)
Transillumination
Nodular fasciitis
Facial nerve paralysis
Radiation therapy
Schwannoma
Facial muscles
Pleomorphic adenoma
List of MeSH codes (C21)
Proton therapy
Cerebritis
Krapina Neanderthal site
Sialadenitis
Neuro-oncology
Dextroscope
Facial nerve decompression
Paraganglioma
Parotid gland
Index of oncology articles
List of diseases (S)
International Classification of Headache Disorders
 Optic Nerve Decompression Surgery - Medical Clinical Policy Bulletins | Aetna
Optic Nerve Decompression Surgery - Medical Clinical Policy Bulletins | Aetna
 MeSH Browser
MeSH Browser
 Brain Tumors in Dogs and Cats: Diagnosis and Therapy - WSAVA 2003 Congress - VIN
Brain Tumors in Dogs and Cats: Diagnosis and Therapy - WSAVA 2003 Congress - VIN
Plus it
 Related Articles - Annals Singapore
Related Articles - Annals Singapore
C72 - Wikipedia
 Stereotactic radiotherapy for trigeminal schwannomas.
Stereotactic radiotherapy for trigeminal schwannomas.
Simultaneous presentation of facial nerve neuroma and otosclerosis. · NEOMED Bibliography Database
 Median Neuropathy; Median Nerve Diseases
Median Neuropathy; Median Nerve Diseases
 Primary Sphenoidal Sinus Lymphoma with Initial Presentation as Unilateral Abducens Nerve Palsy Symptom
Primary Sphenoidal Sinus Lymphoma with Initial Presentation as Unilateral Abducens Nerve Palsy Symptom
Bio2Vec
 Oropharyngeal Dysphagia Detected on VFSS in a Patient with Pancoast Tumor: A Case Report
Oropharyngeal Dysphagia Detected on VFSS in a Patient with Pancoast Tumor: A Case Report
 Correlation of MRI Pattern and Histological Features in a Schwannoma of the Soft Palate in a 13-Year-Old Girl | OMICS...
Correlation of MRI Pattern and Histological Features in a Schwannoma of the Soft Palate in a 13-Year-Old Girl | OMICS...
 Pesquisa | Portal Regional da BVS
Pesquisa | Portal Regional da BVS
 Effect of antiretroviral treatment on blood-brain barrier integrity in HIV-1 infection | BMC Neurology | Full Text
Effect of antiretroviral treatment on blood-brain barrier integrity in HIV-1 infection | BMC Neurology | Full Text
 Clinical Policy Bulletin: Chronic Vertigo - KIPDF.COM
Clinical Policy Bulletin: Chronic Vertigo - KIPDF.COM
MH DELETED MN ADDED MN
 MH DELETED MN ADDED MN
MH DELETED MN ADDED MN
MH DELETED MN ADDED MN
MH DELETED MN ADDED MN
MH DELETED MN ADDED MN
 Neurilemmoma | University of Edinburgh Archive and Manuscript Collections
Neurilemmoma | University of Edinburgh Archive and Manuscript Collections
Neurilemmoma | University of Edinburgh Archive and Manuscript Collections
 Download Operative Otolaryngology head and Neck Surgery 2 Volume Set 3rd Edition PDF Free: - Pick Pdfs
Download Operative Otolaryngology head and Neck Surgery 2 Volume Set 3rd Edition PDF Free: - Pick Pdfs
 Article - Billing and Coding: MolDX: Next-Generation Sequencing for Solid Tumors (A57831)
Article - Billing and Coding: MolDX: Next-Generation Sequencing for Solid Tumors (A57831)
 The April 2004 issue of Otolaryngology focuses on head and neck surgery
The April 2004 issue of Otolaryngology focuses on head and neck surgery
Carotid and Cranial Nerve Reconstruction after Removal of Cavernous Sinus Lesions<...
Brain Stem Neoplasms | Palmetto Profiles
Tumors10
- Pituitary gland neoplasms and tumors arising from cranial nerves are considered secondary brain tumors. (vin.com)
- Tumors of the cranial nerve sheath constitute 5% to 10% of all intracranial neoplasms, yet few articles have described their CT and MR characteristics. (ajnr.org)
- Cranial nerve sheath tumors constitute 5% to 10% of all intracranial neoplasms. (ajnr.org)
- When the origin could be identified, almost all these tumors were histologically proved to be schwannomas of the glossopharyngeal nerve. (ajnr.org)
- Clinically, these tumors may present as a cranial neuropathy, abdominal or soft tissue mass, intracranial lesion, or with spinal cord compression. (ed.ac.uk)
- Cerebellopontine tumors may affect the seventh, eighth, and fifth cranial nerves simultaneously. (medscape.com)
- Tumors in the temporal bone, such as facial nerve neuromas, meningiomas, hemangiomas, and malignant primary and metastatic lesions, should be considered as well. (medscape.com)
- Pituitary tumors may compress adjacent structures, including the HYPOTHALAMUS, several CRANIAL NERVES, and the OPTIC CHIASM. (embl.de)
- Symptoms from posterior fossa tumors also occur when the tumor damages local structures, such as the cranial nerves. (medlineplus.gov)
- Secondary tumours may invade peripheral nerve from its vicinity, they are muscle tumours (leiomyomas and leiomyosarcomas), rhabdomyomas and rhabdomyosarcoma) or bone tumors such as osteosarcomas and chondrosarcomas, and others. (ivis.org)
Spinal3
- The common abnormalities include disease of the muscle itself (myopathy), and motor nerve damage in peripheral/spinal cord/brain from cancer or trauma. (usc.edu)
- A nerve which originates in the lumbar and sacral spinal cord (L4 to S3) and supplies motor and sensory innervation to the lower extremity. (lookformedical.com)
- The nerves outside of the brain and spinal cord, including the autonomic, cranial, and spinal nerves. (lookformedical.com)
Palsy14
- A very large vestibular schwannoma may cause ninth cranial nerve palsy. (ajnr.org)
- A physical examination revealed isolated left abducens nerve palsy. (hindawi.com)
- This report is unique in two aspects: the unilateral abducens nerve palsy as the initial and isolated symptom of ENKL, and the primary sphenoidal sinus ENKL. (hindawi.com)
- Abducens nerve palsy is a common clinical finding in neurology practice and the etiology of the palsy is complicated. (hindawi.com)
- The common causes of unilateral abducens nerve palsy are neoplasm and vascular disease in middle-aged people [ 1 ]. (hindawi.com)
- Multiple cranial nerve deficits or bilateral abducens nerve palsy associated with ENKL have been reported [ 3 ], but isolated unilateral abducens palsy is rarely reported. (hindawi.com)
- Herein we report a case with unilateral abducens nerve palsy as initial symptom in the primary sphenoidal sinus ENKL and investigated the clinical feature of the diagnosis and therapy. (hindawi.com)
- He was found to have isolated left abducens nerve palsy. (hindawi.com)
- Bell palsy is an acute, unilateral, peripheral, lower-motor-neuron facial nerve paralysis that gradually resolves over time in 80-90% of cases. (medscape.com)
- Bell palsy is one of the most common neurologic disorders affecting the cranial nerves, and it is the most common cause of facial paralysis worldwide. (medscape.com)
- Symptoms associated with seventh nerve neoplasm include slowly progressive paralysis, facial hyperkinesis, severe pain, recurrent palsy, and other cranial nerve involvement. (medscape.com)
- Approximately 5-10% of untreated Lyme patients may have a peripheral facial nerve palsy. (medscape.com)
- Neoplasm is the most common cause of cranial nerve 6 and cranial nerve 3 palsies, while the decompensated congenital form is the the most common cause of acquired cranial nerve 4 palsy in children and adolescents. (eye.com.ph)
- The objectives of this study were to examine the differential palsy rates between the left and right RLNs, and the role of intraoperative nerve swelling as a risk factor of postoperative palsy. (symptoma.com)
Autonomic2
- Schawnnoma or neurilemmoma is a benign slow-growing neoplasm of Schwann cells that can arise from any cranial, peripheral or autonomic nerve. (omicsonline.org)
- Notes = A neoplasm that arises from SCHWANN CELLS of the cranial, peripheral, and autonomic nerves. (ed.ac.uk)
Posterior crani1
- Schwannomas of the jugular foramen, usually with origin from the ninth nerve, are rare, but the presenting symptoms may be similar to those of a vestibular schwannoma owing to mass effect by tumor growth in the posterior cranial fossa (2-4) . (ajnr.org)
Cerebral meninges3
- Patients with benign neoplasms of the cerebral meninges, cranial nerves, pituitary gland, craniopharyngeal duct, and brain were included in the study. (bvsalud.org)
- What is the ICD 9 code for neoplasm of cerebral meninges? (wanderluce.com)
- ICD-9-CM Diagnosis Code 225.2 : Benign neoplasm of cerebral meninges Free, official info about 2015 ICD-9-CM diagnosis code 225.2. (wanderluce.com)
Neurologic3
- It is one of the most common neurologic disorders of the cranial nerves (see the image below). (medscape.com)
- When the patient cannot track motion this means neurologic damage involving cranial nerves III, IV, or VI. (usc.edu)
- The spectrum of neurologic manifestations and neoplasms associated with voltage-gated potassium channel (VGKC) autoimmunity is broader than previously recognized. (qxmd.com)
Brainstem1
- Ventral surface of the brain of a 4.5-year-old golden retriever with a germ cell neoplasm compressing the rostral brainstem and the cranial nerves coursing through the middle cranial fossa. (veteriankey.com)
Disorders3
- Disorders of one or more of the twelve cranial nerves. (sdsu.edu)
- With the exception of the optic and olfactory nerves, this includes disorders of the brain stem nuclei from which the cranial nerves originate or terminate. (sdsu.edu)
- Nerve Root Injury and Plexus Disorders (incl. (healthgrades.com)
Sensory5
- The olfactory is a sensory nerve, and damage in the nasal epithelium or the basal gangliamight impair the ability to discriminate different smells. (usc.edu)
- The trigeminal nerve provides sensory supply to the face and mouth. (usc.edu)
- The corneal reflex should also be examined as the sensory supply to the cornea is from this nerve. (usc.edu)
- The corneal reflex has two parts: the sensory, or afferent, part of the reflex is mediated by the ophthalmic branch of the trigeminal nerve, and the motor, or efferent, part of the reflex is mediated by the facial nerve. (usc.edu)
- That portion of the nasal mucosa containing the sensory nerve endings for SMELL, located at the dome of each NASAL CAVITY. (lookformedical.com)
Diseases4
- Diseases of the ninth cranial (glossopharyngeal) nerve or its nuclei in the medulla. (nih.gov)
- The nerve may be injured by diseases affecting the lower brain stem, floor of the posterior fossa, jugular foramen, or the nerve's extracranial course. (nih.gov)
- Experience in the SEER registries has shown that using the Supplemental List increases casefinding for benign brain and CNS, hematopoietic neoplasms, and other reportable diseases. (cancer.gov)
- Diseases of the first cranial (olfactory) nerve, which usually feature anosmia or other alterations in the sense of smell and taste. (lookformedical.com)
Parotid gland1
- Recurrent ipsilateral facial paralysis must raise the suspicion of a tumor of the facial nerve or parotid gland. (medscape.com)
Optic nerve11
- Visual loss secondary to optic nerve drusen. (aetna.com)
- Optic nerve decompression surgery (also known as optic nerve sheath decompression surgery) involves cutting slits or a window in the optic nerve sheath to allow cerebrospinal fluid to escape, thereby reducing the pressure around the optic nerve. (aetna.com)
- Diamox, Lasix, corticosteroids), and disc swelling with visual field loss progresses, direct fenestration of the optic nerve sheaths via medial or lateral orbitotomy has been shown to be an effective and relatively simple procedure for relief of papilledema. (aetna.com)
- It is caused by infarction of the short posterior ciliary arteries supplying the anterior optic nerve. (aetna.com)
- There is no direct treatment for NAION, although corticosteroids are sometimes used to reduce optic nerve edema. (aetna.com)
- Initial results of uncontrolled studies suggested that optic nerve sheath decompression was a promising treatment of progressive visual loss in patients with NAION. (aetna.com)
- To resolve the controversy over the effectiveness of optic nerve decompression for NAION, the National Eye Institute sponsored the Ischemic Optic Neuropathy Decompression Trial, a multicenter, randomized controlled clinical trial of optic nerve decompression surgery for patients with NAION. (aetna.com)
- The investigators concluded that optic nerve decompression surgery is not an effective treatment for NAION, and in fact, may increase the risk of progressive visual loss in NAION patients. (aetna.com)
- A structured evidence review (Dickersin and Manheimer, 2002) concluded that "[r]esults from the Ischemic Optic Neuropathy Decompression Trial indicate that optic nerve decompression surgery for nonarteritic ischemic optic neuropathy is not effective. (aetna.com)
- A Cochrane review (Dickersin et al, 2012) concluded that results from the single trial indicate no evidence of a beneficial effect of optic nerve decompression surgery for NAION. (aetna.com)
- Visual deficits may accompany masses that involve the visual pathways from the occipital lobe of the cerebrum to the optic nerve. (vin.com)
Malignant Neoplasms2
- In their study, "Facial Nerve Paralysis Secondary to Occult Malignant Neoplasms," the researchers conclude that facial nerve exploration should be considered for patients with a history of pain or regional skin cancer, involvement of other cranial nerves, and prolonged facial paralysis. (news-medical.net)
- Malignant neoplasms show a greater degree of anaplasia and have the properties of invasion and metastasis, compared to benign neoplasms . (lookformedical.com)
Tumor6
- Cerebral meningioma is the most frequently reported primary brain tumor of cats and accounts for almost 10% of all nonhematopoietic neoplasms. (vin.com)
- Surgical findings showed schwannomas of the glossopharyngeal nerve in seven patients and tumor involvement of both the glossopharyngeal and vagal nerves in one patient. (ajnr.org)
- At surgery, the tumor was found to originate at the union of the nervus intermedius and the facial nerve. (omeka.net)
- A video fluoroscopic swallow study confirmed the presence of oropharyngeal dysphagia, which was attributed to left glossopharyngeal and vagus nerve damage associated with the Pancoast tumor. (jkds.org)
- Although not technically a brain tumor, it is included in this category because it may compress or squeeze the adjacent brain, nerves and vessels. (wanderluce.com)
- Overall, the common etiologies in children and adolescents include the following, in decreasing order: neoplasm (tumor), idiopathic, inflammation, and non-aneurysmal vascular problem. (eye.com.ph)
Histologically2
- The neoplasms may be histologically the same or different, and may be found in the same or different sites. (lookformedical.com)
- Neoplasms encountered (confirmed histologically in 33%) included 18 carcinomas, 5 adenomas, 1 thymoma, and 3 hematologic malignancies. (qxmd.com)
Peripheral Nerves1
- Peripheral nerves contain non-neuronal cells and connective tissue as well as axons. (lookformedical.com)
Primary3
- Primary and metastatic neoplasms may occur in this location. (musc.edu)
- Primary brain stem neoplasms are more frequent in children. (musc.edu)
- Transfer of a neoplasm from its primary site to lymph nodes or to distant parts of the body by way of the lymphatic system. (lookformedical.com)
Intraoperative1
- Contains state-of-the-art guidance on the ear/temporal bone/skull base, including fully- and semi-implantable auditory implants, vestibular implants, imaging advances, radiosurgical treatment of posterior fossa and skull base neoplasms, intraoperative monitoring of cranial nerve and CNS function, minimally-invasive surgical approaches to the entire skull base, vertigo and postural disequilibrium, and much more. (pickpdfs.com)
Vascular lesions2
- During the last 7 years, approximately 170 neoplasms, and 35 vascular lesions involving the cavernous sinus were treated by the first two authors. (elsevierpure.com)
- Failure to recognize structural, infectious, or vascular lesions leading to seventh cranial (facial) nerve damage may result in further deterioration of the patient's condition. (medscape.com)
Cancer1
- Offers expanded coverage of endoscopic techniques for cranial base surgery, plus information on the latest endoscopic cancer techniques including robotic surgery, minimally invasive thyroid surgery, and new techniques for the treatment of obstructive sleep apnea including implantable nerve stimulators. (pickpdfs.com)
Clinical2
- Now, otolaryngologist - head and neck surgeons at the Mayo Clinic have determined that malignancy of the facial nerve can be another cause of unilateral facial paralysis in patients with otherwise normal clinical and imaging findings. (news-medical.net)
- They are slow growing neoplasms and their clinical signs appear insidiously. (ivis.org)
Middle ear1
- The CT then exits the middle ear to join the facial nerve in the facial canal. (medscape.com)
Bone3
- The inner ear is completely encased in bone and consists of the cochlear-vestibular apparatus and its associated nerves. (medscape.com)
- Ovoid body resting on the CRIBRIFORM PLATE of the ethmoid bone where the OLFACTORY NERVE terminates. (lookformedical.com)
- After entering the infratemporal fossa between the medial pterygoid muscle and mandible, the chorda tympani leaves the lingual nerve and crosses the spine of the sphenoid bone, to proceed to the petrous temporal bone through the petrotympanic fissure (canal of Huguier). (medscape.com)
Dysfunction1
- Dysfunction of one or more cranial nerves causally related to a traumatic injury. (lookformedical.com)
Trauma1
- and trauma to the facial region are conditions associated with cranial nerve injuries. (lookformedical.com)
Brain stem4
- Neoplasms involving the brain stem may result in cranial nerve deficits. (vin.com)
- Brain Stem Neoplasms" is a descriptor in the National Library of Medicine's controlled vocabulary thesaurus, MeSH (Medical Subject Headings) . (musc.edu)
- This graph shows the total number of publications written about "Brain Stem Neoplasms" by people in this website by year, and whether "Brain Stem Neoplasms" was a major or minor topic of these publications. (musc.edu)
- Below are the most recent publications written about "Brain Stem Neoplasms" by people in Profiles. (musc.edu)
Vestibular3
- The vestibular apparatus gives off 2 nerves: the superior and the inferior vestibular nerves. (medscape.com)
- Together with the cochlear and facial nerves, the vestibular nerves travel through the internal auditory canal to the cerebellopontine angle. (medscape.com)
- They most commonly arise from the vestibular portion of the eighth cranial nerve (1) . (ajnr.org)
Abnormalities1
- Acute myeloid leukemia has a number of subtypes and precursor neoplasms that are distinguished from each other by morphology, immunophenotype, cytochemistry, and genetic abnormalities (see also The 2016 World Health Organization [WHO] Classification of myeloid neoplasms ) all of which have important implications for prognosis and treatment. (msdmanuals.com)
Structures1
- Tumour size, cavernous sinus invasion, traction or displacement of intracranial pain-sensitive structures such as blood vessels, cranial nerves and dura mater, and hormonal hypersecretion are implicated causes. (medscape.com)
Arise2
- Neoplasms which arise from or metastasize to the PITUITARY GLAND. (embl.de)
- The components of CN VII that reach the tongue include the chorda tympani and the greater petrosal nerve, which arise from the nervus intermedius (smallest afferent branch of the facial nerve). (medscape.com)
Recurrent1
- Abstract We report a case of sarcoidosis in which the presenting features were hoarseness of voice, hilar lymphadenopathy and paralysis of the left recurrent laryngeal nerve. (symptoma.com)
Absent1
- The cranial nerve exam confirmed hoarseness and an absent gag reflex. (jkds.org)