Cystadenoma
Cystadenoma, Mucinous
Cystadenoma, Serous
Cystadenocarcinoma
Mucocele
Biliary Tract Neoplasms
Cysts
Sertoli-Leydig Cell Tumor
Bile Ducts, Intrahepatic
Pancreatic Neoplasms
Adenolymphoma
Cystadenocarcinoma, Mucinous
Hepatic Duct, Common
Spermatocele
Ovarian Neoplasms
Aspermia
Pseudomyxoma Peritonei
Pancreatic Cyst
Neoplasms, Multiple Primary
Retroperitoneal Neoplasms
Salivary Glands, Minor
Tomography, X-Ray Computed
Pancreatic Pseudocyst
Cholangiopancreatography, Magnetic Resonance
Bile Ducts, Extrahepatic
Cystadenocarcinoma, Serous
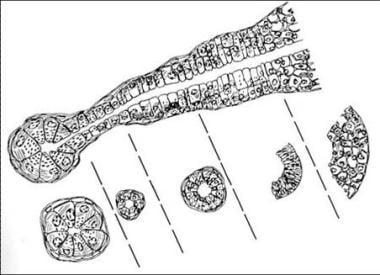
Epithelial thyroid tumors in cows. (1/197)
From 1964 to 1973, 370 tumors were collected from cows of unknown age. Ten (2.7%) of these were primary thyroid tumors. Three were malignant. The benign tumors were solitary encapsulated adenomas in the parenchyma with more or less defined trabeculae, tubular, and microfollicular pattern. One of the malignant tumors was a cystic papillary adenocarcinoma, and two were small cell carcinomas consisting of small, sometimes binuclear, pleomorphic cells. (+info)Vascular endothelial growth factor levels in ovarian cyst fluid correlate with malignancy. (2/197)
Ovarian cancer is a richly vascularized neoplasm with solid and cystic components. The purpose of this study was to determine whether cyst fluid could be used to quantitatively evaluate production of angiogenic factors in ovarian lesions. ELISA was used to measure vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF) in the cyst fluid of patients with ovarian cancer (n = 13), benign cysts and cystadenomas (n = 23), borderline tumors (n = 5), and functional cysts (n = 8). VEGF levels were markedly elevated in the fluid of malignant cysts (38.5+/-8.2 ng/ml) as compared with benign (1.6+/-0.4 ng/ml; P < 0.001), borderline (5.7+/-1.5 ng/ml; P < 0.001), or functional cysts (3.8+/-2.0 ng/ml; P < 0.001). The presence of VEGF in cancer cells was confirmed by immunohistochemistry. Follow-up of patients with malignant and borderline lesions demonstrated a correlation between VEGF levels in cyst fluid and tumor recurrence (P = 0.03). bFGF in malignant cysts was either undetectable or very low (0.3+/-0.2 ng/ml), and no significant differences were found in bFGF levels among malignant, benign, borderline, and functional cysts. This study demonstrates that ovarian malignancy is associated with dramatic elevation of VEGF levels in ovarian cyst fluid. Conversely, there is no correlation between cyst fluid bFGF levels and malignant transformation. The high levels of VEGF in malignant cysts are consistent with the hypothesis that this growth factor plays an important role in ovarian cancer related-angiogenesis and tumor progression and represents a potentially important target of antiangiogenic therapy. (+info)Mucin Hypersecreting Intraductal Papillary Neoplasm of the pancreas. (3/197)
Mucin Hypersecreting Intraductal Papillary Neoplasm is a rare neoplasm that arises from ductal epithelial cells. This entity is distinct from the more commonly known Mucinous Cystadenoma or Mucinous Cystadenocarcinoma. Despite this distinction, it has been erroneously categorized with these more common cystic neoplasms. Characteristic clinical presentation, radiographic, and endoscopic findings help distinguish this neoplasm from the cystadenomas and cystadenocarcinomas. Histopathologic identification is not crucial to the preoperative diagnosis. This neoplasm is considered to represent a premalignant condition and, therefore, surgical resection is warranted. Prognosis, following resection, is felt to be curative for the majority of patients. We present two cases of Mucin Hypersecreting Intraductal Papillary Neoplasm and discuss their diagnosis and surgical therapy. (+info)Tsc2(+/-) mice develop tumors in multiple sites that express gelsolin and are influenced by genetic background. (4/197)
Tuberous sclerosis (TSC) is an autosomal dominant genetic disorder in which benign hamartomas develop in multiple organs, caused by mutations in either TSC1 or TSC2. We developed a murine model of Tsc2 disease using a gene targeting approach. Tsc2-null embryos die at embryonic days 9.5-12.5 from hepatic hypoplasia. Tsc2 heterozygotes display 100% incidence of multiple bilateral renal cystadenomas, 50% incidence of liver hemangiomas, and 32% incidence of lung adenomas by 15 months of age. Progression to renal carcinoma, fatal bleeding from the liver hemangiomas, and extremity angiosarcomas all occur at a rate of less than 10%. The renal cystadenomas develop from intercalated cells of the cortical collecting duct and uniformly express gelsolin at high levels, enabling detection of early neoplastic lesions. The tumor expression pattern of the mice is influenced by genetic background, with fewer large renal cystadenomas in the outbred Black Swiss background and more angiosarcomas in 129/SvJae chimeric mice. The slow growth of the tumors in the heterozygote mice matches the limited growth potential of the great majority of TSC hamartomas, and the influence of genetic background on phenotype correlates with the marked variability in expression of TSC seen in patients. (+info)Alterations in the expression of the DNA repair/redox enzyme APE/ref-1 in epithelial ovarian cancers. (5/197)
The DNA base excision repair pathway is responsible for the repair of alkylation and oxidative DNA damage. A crucial step in the base excision repair pathway involves the cleavage of an apurinic/apyrimidinic (AP) site in DNA by an AP endonuclease (APE). The major AP endonuclease in mammalian cells is APE/ref-1, a multifunctional enzyme that acts not only as an AP endonuclease but as a redox-modifying factor for a variety of transcription factors. The purpose of this study was to determine the expression of APE/redox factor-1 (ref-1) in ovarian tissues, particularly ovarian cancers. Formalin-fixed, paraffin-embedded specimens of ovarian tissues (normal, various benign conditions, and epithelial cancers) were studied using both polyclonal and monoclonal antibodies to APE/ref-1. The relationship between APE/ref-1 protein levels and DNA repair activity was studied in ovarian Hey and Hey-C2 cell lines using Western blot and a specific AP-site oligonucleotide cleavage assay. Hey and Hey-C2 cells were fractionated, and the nuclear and cytoplasmic extracts were quantitated for protein levels and assessed for APE/ref-1 with Western blot. Normal ovarian tissues consistently demonstrated strong nuclear staining of the surface epithelium, epithelial inclusions, corpora lutea and albicantia, and stroma. Cytoplasmic staining was absent. A similar pattern was seen for benign conditions including endometriosis. Low malignant potential ovarian cancers stained in a pattern similar to normal ovarian and nonneoplastic tissues; however, two specimens also had areas of cytoplasmic staining. Epithelial ovarian cancers were remarkably different from all other ovarian tissues studied. Both nuclear and cytoplasmic staining of the malignant epithelium were seen and ranged from strong to weak, often with considerable staining heterogeneity within the same tumor. The AP-site oligonucleotide cleavage assay indicated that APE/ref-1 protein levels correlate well with DNA repair activity. The increased levels of APE/ref-1 in the Hey-C2 cells was mainly attributable to increased cytoplasmic enzyme. APE/ref-1 immunoreactivity is altered in malignant ovarian tumors. Further studies will determine whether the altered expression and subcellular location reflect changes in redox regulatory functions. (+info)Accumulation of collagen in ovarian benign tumours. (6/197)
Extracellular matrix components of benign ovarian tumours (cystadenoma, adenofibroma, cystadenofibroma) were analysed. The investigated tumours contained twice as much collagen than control ovarian tissues. Significant alterations in mutual quantitative relationships between collagens of various types were observed. The proportion of type I collagen decreased and that of type III collagen increased. The accumulation of collagen was accompanied by a reduction in sulphated glycosaminoglycan content whereas the amount of hyaluronic acid was not changed. Dermatan sulphate was the most abundant glycosaminoglycan component. It is suggested that the accumulation of collagen (natural barrier to the migration of tumour cells) and underexpression of glycosaminoglycans/proteoglycans (binding some growth factors and interleukins) may exert an inhibitory effect on tumour growth. (+info)Contrast-enhanced sonography in the examination of benign and malignant adnexal masses. (7/197)
Our objective was to characterize the properties of an intravascular ultrasonographic contrast agent in examination of adnexal masses and to compare contrast agent properties between benign and malignant adnexal tumors. Fifty-eight consecutively examined women with suspected ovarian tumors were examined preoperatively by power Doppler ultrasonography, first without and then with contrast agent enhancement (Levovist). Fourteen women had ovarian cancer, 3 had borderline ovarian tumors, 18 had benign ovarian neoplasms, and 23 had functional adnexal cystic masses or endometriomas. The effect of the contrast agent was evaluated visually and by using computerized power Doppler signal intensity measurements. In visual evaluation, the brightness of the power Doppler signal and the amount of recognizable vascular areas increased in each tumor after contrast agent administration. The number of vessels in power Doppler ultrasonograms, both before and after contrast agent enhancement, was significantly higher in malignant than in benign adnexal masses, as also was the increase in the number of recognizable vessels after contrast agent administration. Contrast agent uptake time was significantly shorter in malignant than in benign tumors. No significant differences were found in the power Doppler signal intensities or their changes between benign and malignant tumors. In conclusion, use of sonographic contrast agent facilitates imaging of tumor vessels. For differentiation of benign and malignant tumors, the kinetic properties of the contrast agent, such as uptake and washout times, may have more potential than the use of the contrast agent in anatomic imaging of the tumor vessels. (+info)Molecular characterization of pancreatic serous microcystic adenomas: evidence for a tumor suppressor gene on chromosome 10q. (8/197)
Pancreatic serous microcystic adenomas (SCAs) are rare, benign tumors with a striking female preference. Virtually no information is available about chromosomal or genetic anomalies in this disease. We performed extensive molecular characterization of 21 cases of formalin-fixed, paraffin-embedded sporadic SCAs consisting in genome-wide allelic loss analysis with 79 microsatellite markers covering all 22 autosomes, assessment of microsatellite instability, and mutational analysis of the VHL, K-ras, and p53 genes in nine cases for which frozen tissue was available. Although no case showed microsatellite instability of the type seen in mismatch repair-deficient tumors, a relatively low fractional allelic loss of 0.08 was found. Losses on chromosome 10q were the most frequent event in SCAs (50% of cases), followed by allelic losses on chromosome 3p (40% of cases). Moderately frequent losses (>25% of cases) were found on chromosomes 1q, 2q, and 7q. The VHL gene, located on chromosome 3p, had somatic inactivating mutations in two of nine cases (22%), whereas no mutations were found in either K-ras or p53, in agreement with the finding that all 21 cases stained negative for p53 by immunohistochemistry. Our study indicates that the involvement of chromosomal arms 10q and 3p is characteristic of SCAs and that the VHL gene is involved in a subset of sporadic cases. (+info)Cystadenoma is a type of benign tumor (not cancerous), which arises from glandular epithelial cells and is covered by a thin layer of connective tissue. These tumors can develop in various locations within the body, including the ovaries, pancreas, and other organs that contain glands.
There are two main types of cystadenomas: serous and mucinous. Serous cystadenomas are filled with a clear or watery fluid, while mucinous cystadenomas contain a thick, gelatinous material. Although they are generally not harmful, these tumors can grow quite large and cause discomfort or other symptoms due to their size or location. In some cases, cystadenomas may undergo malignant transformation and develop into cancerous tumors, known as cystadenocarcinomas. Regular medical follow-up and monitoring are essential for individuals diagnosed with cystadenomas to ensure early detection and treatment of any potential complications.
Mucinous cystadenoma is a type of benign tumor that arises from the epithelial cells lining the mucous membranes of the body. It is most commonly found in the ovary, but can also occur in other locations such as the pancreas or appendix.
Mucinous cystadenomas are characterized by the production of large amounts of mucin, a slippery, gel-like substance that accumulates inside the tumor and causes it to grow into a cystic mass. These tumors can vary in size, ranging from a few centimeters to over 20 centimeters in diameter.
While mucinous cystadenomas are generally benign, they have the potential to become cancerous (mucinous cystadenocarcinoma) if left untreated. Symptoms of mucinous cystadenoma may include abdominal pain or swelling, bloating, and changes in bowel movements or urinary habits. Treatment typically involves surgical removal of the tumor.
A serous cystadenoma is a type of benign tumor that arises from the epithelial cells lining the serous glands, which are glands that produce a watery, lubricating fluid. This type of tumor typically develops in the ovary or the pancreas.
Serous cystadenomas of the ovary are usually filled with a clear, watery fluid and have multiple loculations (compartments). They can vary in size from a few millimeters to several centimeters in diameter. Although these tumors are benign, they can cause symptoms if they become large enough to press on surrounding organs or if they rupture and release their contents into the abdominal cavity.
Serous cystadenomas of the pancreas are less common than ovarian serous cystadenomas. They typically occur in the tail of the pancreas and can range in size from a few millimeters to several centimeters in diameter. These tumors are usually asymptomatic, but they can cause symptoms such as abdominal pain or discomfort if they become large enough to press on surrounding organs.
It is important to note that while serous cystadenomas are generally benign, there is a small risk that they may undergo malignant transformation and develop into a type of cancer known as a serous cystadenocarcinoma. For this reason, it is important for patients with these tumors to be followed closely by a healthcare provider and to have regular imaging studies and/or surgical excision to monitor for any changes in the tumor.
Papillary cystadenoma is a type of benign (non-cancerous) tumor that arises from the glandular cells in various organs. It is characterized by the growth of finger-like projections (papillae) inside the cysts. These tumors can occur in different parts of the body, including the ovaries, pancreas, and the lining of the abdominal cavity (peritoneum).
In general, papillary cystadenomas are slow-growing and do not typically spread to other organs. However, they can cause symptoms such as pain or discomfort if they become large enough to press on surrounding tissues. Treatment usually involves surgical removal of the tumor. It is important to note that while papillary cystadenomas are generally benign, there is a small risk that they may undergo malignant transformation and develop into cancerous tumors over time. Regular follow-up with a healthcare provider is recommended to monitor for any changes in the tumor or the development of new symptoms.
Cystadenocarcinoma is a type of tumor that arises from the epithelial lining of a cyst, and it has the potential to invade surrounding tissues and spread (metastasize) to other parts of the body. It typically affects glandular organs such as the ovaries, pancreas, and salivary glands.
Cystadenocarcinomas can be classified into two types: serous and mucinous. Serous cystadenocarcinomas produce a watery fluid, while mucinous cystadenocarcinomas produce a thick, mucus-like fluid. Both types of tumors can be benign or malignant, but malignant cystadenocarcinomas are more aggressive and have a higher risk of metastasis.
Symptoms of cystadenocarcinoma depend on the location and size of the tumor. In some cases, there may be no symptoms until the tumor has grown large enough to cause pain or other problems. Treatment typically involves surgical removal of the tumor, along with any affected surrounding tissue. Chemotherapy and radiation therapy may also be used in some cases to help prevent recurrence or spread of the cancer.
Appendiceal neoplasms refer to various types of tumors that can develop in the appendix, a small tube-like structure attached to the large intestine. These neoplasms can be benign or malignant and can include:
1. Adenomas: These are benign tumors that arise from the glandular cells lining the appendix. They are usually slow-growing and may not cause any symptoms.
2. Carcinoids: These are neuroendocrine tumors that arise from the hormone-producing cells in the appendix. They are typically small and slow-growing, but some can be aggressive and spread to other parts of the body.
3. Mucinous neoplasms: These are tumors that produce mucin, a slippery substance that can cause the appendix to become distended and filled with mucus. They can be low-grade (less aggressive) or high-grade (more aggressive) and may spread to other parts of the abdomen.
4. Adenocarcinomas: These are malignant tumors that arise from the glandular cells lining the appendix. They are relatively rare but can be aggressive and spread to other parts of the body.
5. Pseudomyxoma peritonei: This is a condition in which mucin produced by an appendiceal neoplasm leaks into the abdominal cavity, causing a jelly-like accumulation of fluid and tissue. It can be caused by both benign and malignant tumors.
Treatment for appendiceal neoplasms depends on the type and stage of the tumor, as well as the patient's overall health. Treatment options may include surgery, chemotherapy, or radiation therapy.
A mucocele is a mucus-containing cystic lesion that results from the accumulation of mucin within a damaged minor salivary gland duct or mucous gland. It is typically caused by trauma, injury, or blockage of the duct. Mucocele appears as a round, dome-shaped, fluid-filled swelling, which may be bluish or clear in color. They are most commonly found on the lower lip but can also occur on other areas of the oral cavity. Mucocele is generally painless unless it becomes secondarily infected; however, it can cause discomfort during speaking, chewing, or swallowing, and may affect aesthetics. Treatment usually involves surgical excision of the mucocele to prevent recurrence.
Biliary tract neoplasms refer to abnormal growths or tumors that develop in the biliary system, which includes the gallbladder, bile ducts inside and outside the liver, and the ducts that connect the liver to the small intestine. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Malignant biliary tract neoplasms are often referred to as cholangiocarcinoma if they originate in the bile ducts, or gallbladder cancer if they arise in the gallbladder. These cancers are relatively rare but can be aggressive and difficult to treat. They can cause symptoms such as jaundice (yellowing of the skin and eyes), abdominal pain, weight loss, and dark urine.
Risk factors for biliary tract neoplasms include chronic inflammation of the biliary system, primary sclerosing cholangitis, liver cirrhosis, hepatitis B or C infection, parasitic infections, and certain genetic conditions. Early detection and treatment can improve outcomes for patients with these neoplasms.
Bile duct neoplasms, also known as cholangiocarcinomas, refer to a group of malignancies that arise from the bile ducts. These are the tubes that carry bile from the liver to the gallbladder and small intestine. Bile duct neoplasms can be further classified based on their location as intrahepatic (within the liver), perihilar (at the junction of the left and right hepatic ducts), or distal (in the common bile duct).
These tumors are relatively rare, but their incidence has been increasing in recent years. They can cause a variety of symptoms, including jaundice, abdominal pain, weight loss, and fever. The diagnosis of bile duct neoplasms typically involves imaging studies such as CT or MRI scans, as well as blood tests to assess liver function. In some cases, a biopsy may be necessary to confirm the diagnosis.
Treatment options for bile duct neoplasms depend on several factors, including the location and stage of the tumor, as well as the patient's overall health. Surgical resection is the preferred treatment for early-stage tumors, while chemotherapy and radiation therapy may be used in more advanced cases. For patients who are not candidates for surgery, palliative treatments such as stenting or bypass procedures may be recommended to relieve symptoms and improve quality of life.
The appendix is a small, tube-like structure that projects from the large intestine, located in the lower right quadrant of the abdomen. Its function in humans is not well understood and is often considered vestigial, meaning it no longer serves a necessary purpose. However, in some animals, the appendix plays a role in the immune system. Inflammation of the appendix, known as appendicitis, can cause severe abdominal pain and requires medical attention, often leading to surgical removal of the appendix (appendectomy).
Adenoma of the bile duct is a benign (noncancerous) tumor that develops in the bile ducts, which are tiny tubes that carry bile from the liver to the gallbladder and small intestine. Bile is a digestive fluid produced by the liver.
Bile duct adenomas are rare and usually do not cause any symptoms. However, if they grow large enough, they may obstruct the flow of bile and cause jaundice (yellowing of the skin and whites of the eyes), abdominal pain, or itching. In some cases, bile duct adenomas may become cancerous and develop into bile duct carcinomas.
The exact cause of bile duct adenomas is not known, but they are more common in people with certain genetic disorders, such as Gardner's syndrome and von Hippel-Lindau disease. Treatment for bile duct adenomas typically involves surgical removal of the tumor.
A cyst is a closed sac, having a distinct membrane and division between the sac and its surrounding tissue, that contains fluid, air, or semisolid material. Cysts can occur in various parts of the body, including the skin, internal organs, and bones. They can be caused by various factors, such as infection, genetic predisposition, or blockage of a duct or gland. Some cysts may cause symptoms, such as pain or discomfort, while others may not cause any symptoms at all. Treatment for cysts depends on the type and location of the cyst, as well as whether it is causing any problems. Some cysts may go away on their own, while others may need to be drained or removed through a surgical procedure.
A Sertoli-Leydig cell tumor is a rare type of sex cord-stromal tumor that develops in the ovaries. These tumors arise from the cells that produce hormones and help to form and maintain the ovarian tissue. Sertoli-Leydig cell tumors can occur in people of any age but are most commonly found in women between the ages of 20 and 40.
These tumors can be functional, meaning they produce hormones, or nonfunctional. Functional Sertoli-Leydig cell tumors may cause symptoms related to the production of male hormones (androgens), such as excess facial hair, a deepened voice, and irregular menstrual periods. Nonfunctional tumors typically do not cause any specific symptoms and are often found during routine pelvic examinations or imaging studies performed for other reasons.
Sertoli-Leydig cell tumors are usually slow-growing and can vary in size. Most of these tumors are benign (not cancerous), but some can be malignant (cancerous) and may spread to other parts of the body. Treatment typically involves surgical removal of the tumor, and additional therapies such as chemotherapy or radiation therapy may be recommended depending on the stage and grade of the tumor. Regular follow-up care is essential to monitor for any recurrence of the tumor.
Intrahepatic bile ducts are the small tubular structures inside the liver that collect bile from the liver cells (hepatocytes). Bile is a digestive fluid produced by the liver that helps in the absorption of fats and fat-soluble vitamins from food. The intrahepatic bile ducts merge to form larger ducts, which eventually exit the liver and join with the cystic duct from the gallbladder to form the common bile duct. The common bile duct then empties into the duodenum, the first part of the small intestine, where bile aids in digestion. Intrahepatic bile ducts can become obstructed or damaged due to various conditions such as gallstones, tumors, or inflammation, leading to complications like jaundice, liver damage, and infection.
Pancreatic neoplasms refer to abnormal growths in the pancreas that can be benign or malignant. The pancreas is a gland located behind the stomach that produces hormones and digestive enzymes. Pancreatic neoplasms can interfere with the normal functioning of the pancreas, leading to various health complications.
Benign pancreatic neoplasms are non-cancerous growths that do not spread to other parts of the body. They are usually removed through surgery to prevent any potential complications, such as blocking the bile duct or causing pain.
Malignant pancreatic neoplasms, also known as pancreatic cancer, are cancerous growths that can invade and destroy surrounding tissues and organs. They can also spread (metastasize) to other parts of the body, such as the liver, lungs, or bones. Pancreatic cancer is often aggressive and difficult to treat, with a poor prognosis.
There are several types of pancreatic neoplasms, including adenocarcinomas, neuroendocrine tumors, solid pseudopapillary neoplasms, and cystic neoplasms. The specific type of neoplasm is determined through various diagnostic tests, such as imaging studies, biopsies, and blood tests. Treatment options depend on the type, stage, and location of the neoplasm, as well as the patient's overall health and preferences.
Adenolymphoma is a rare, benign tumor that arises from the lymphoid tissue found in glandular structures, such as the salivary glands. It is also known as Warthin's tumor or cystic papillary adenolymphoma.
The tumor is composed of multiple cyst-like spaces lined by columnar epithelial cells and surrounded by lymphoid tissue, which may contain lymphocytes, plasma cells, and occasionally, germinal centers. The etiology of adenolymphoma is unclear, but it has been associated with smoking and genetic factors.
Adenolymphomas are typically slow-growing and painless, although they can cause discomfort or facial asymmetry if they become large enough. They are usually diagnosed through imaging studies such as ultrasound, CT scan, or MRI, followed by a biopsy to confirm the diagnosis.
Treatment of adenolymphoma typically involves surgical excision, which is usually curative. Recurrence after surgery is rare, but long-term follow-up is recommended due to the potential for malignant transformation into squamous cell carcinoma or other malignancies.
Mucinous cystadenocarcinoma is a type of cancer that arises from the mucin-producing cells in the lining of a cyst. It is a subtype of cystadenocarcinoma, which is a malignant tumor that develops within a cyst. Mucinous cystadenocarcinomas are typically found in the ovary or pancreas but can also occur in other organs such as the appendix and the respiratory tract.
These tumors are characterized by the production of large amounts of mucin, a gel-like substance that can accumulate within the cyst and cause it to grow. Mucinous cystadenocarcinomas tend to grow slowly but can become quite large and may eventually spread (metastasize) to other parts of the body if left untreated.
Symptoms of mucinous cystadenocarcinoma depend on the location and size of the tumor, but they may include abdominal pain or discomfort, bloating, changes in bowel movements, or vaginal bleeding. Treatment typically involves surgical removal of the tumor, followed by chemotherapy or radiation therapy to kill any remaining cancer cells. The prognosis for mucinous cystadenocarcinoma depends on several factors, including the stage of the disease at diagnosis and the patient's overall health.
Cecal diseases refer to medical conditions that affect the cecum, which is a pouch-like structure located at the junction of the small and large intestines. The cecum plays an important role in digestion, particularly in the fermentation of certain types of food.
There are several different types of cecal diseases, including:
1. Cecal volvulus: This is a rare condition in which the cecum twists on itself, cutting off blood flow and causing severe pain and other symptoms.
2. Diverticulitis: This occurs when small pouches called diverticula form in the wall of the cecum and become inflamed or infected.
3. Appendicitis: Although not strictly a cecal disease, the appendix is a small tube-like structure that branches off from the cecum. Inflammation of the appendix (appendicitis) can cause severe pain in the lower right abdomen and may require surgical removal of the appendix.
4. Crohn's disease: This is a chronic inflammatory bowel disease that can affect any part of the digestive tract, including the cecum.
5. Tuberculosis: The cecum can also be affected by tuberculosis, which is a bacterial infection that primarily affects the lungs but can spread to other parts of the body.
6. Cancer: Although rare, cancer can also affect the cecum, leading to symptoms such as abdominal pain, bloating, and changes in bowel habits.
Treatment for cecal diseases depends on the specific condition and its severity. Treatment options may include antibiotics, surgery, or other medical interventions. If you are experiencing symptoms that may be related to a cecal disease, it is important to seek medical attention promptly.
The common hepatic duct is a medical term that refers to the duct in the liver responsible for carrying bile from the liver. More specifically, it is the duct that results from the convergence of the right and left hepatic ducts, which themselves carry bile from the right and left lobes of the liver, respectively. The common hepatic duct then joins with the cystic duct from the gallbladder to form the common bile duct, which ultimately drains into the duodenum, a part of the small intestine.
The primary function of the common hepatic duct is to transport bile, a digestive juice produced by the liver, to the small intestine. Bile helps break down fats during the digestion process, making it possible for the body to absorb them properly. Any issues or abnormalities in the common hepatic duct can lead to problems with bile flow and potentially cause health complications such as jaundice, gallstones, or liver damage.
A spermatocele is a type of cyst that develops in the epididymis, which is a small, coiled tube located on the back surface of the testicle. This cyst typically contains sperm and fluid from the epididymis, and it is usually benign and harmless.
Spermatoceles are often asymptomatic and may be discovered during a routine physical examination or self-examination. In some cases, however, they may cause discomfort or pain, particularly if they become large enough to press on the testicle or surrounding structures.
While spermatoceles do not typically require treatment unless they are causing symptoms, it is important to have them evaluated by a healthcare provider to rule out other potential causes of any symptoms and to ensure that appropriate treatment is provided if necessary.
Endocrine gland neoplasms refer to abnormal growths (tumors) that develop in the endocrine glands. These glands are responsible for producing hormones, which are chemical messengers that regulate various functions and processes in the body. Neoplasms can be benign or malignant (cancerous). Benign neoplasms tend to grow slowly and do not spread to other parts of the body. Malignant neoplasms, on the other hand, can invade nearby tissues and organs and may also metastasize (spread) to distant sites.
Endocrine gland neoplasms can occur in any of the endocrine glands, including:
1. Pituitary gland: located at the base of the brain, it produces several hormones that regulate growth and development, as well as other bodily functions.
2. Thyroid gland: located in the neck, it produces thyroid hormones that regulate metabolism and calcium balance.
3. Parathyroid glands: located near the thyroid gland, they produce parathyroid hormone that regulates calcium levels in the blood.
4. Adrenal glands: located on top of each kidney, they produce hormones such as adrenaline, cortisol, and aldosterone that regulate stress response, metabolism, and blood pressure.
5. Pancreas: located behind the stomach, it produces insulin and glucagon, which regulate blood sugar levels, and digestive enzymes that help break down food.
6. Pineal gland: located in the brain, it produces melatonin, a hormone that regulates sleep-wake cycles.
7. Gonads (ovaries and testicles): located in the pelvis (ovaries) and scrotum (testicles), they produce sex hormones such as estrogen, progesterone, and testosterone that regulate reproductive function and secondary sexual characteristics.
Endocrine gland neoplasms can cause various symptoms depending on the type and location of the tumor. For example, a pituitary gland neoplasm may cause headaches, vision problems, or hormonal imbalances, while an adrenal gland neoplasm may cause high blood pressure, weight gain, or mood changes.
Diagnosis of endocrine gland neoplasms typically involves a combination of medical history, physical examination, imaging studies such as CT or MRI scans, and laboratory tests to measure hormone levels. Treatment options may include surgery, radiation therapy, chemotherapy, or hormonal therapy, depending on the type and stage of the tumor.
Ovarian neoplasms refer to abnormal growths or tumors in the ovary, which can be benign (non-cancerous) or malignant (cancerous). These growths can originate from various cell types within the ovary, including epithelial cells, germ cells, and stromal cells. Ovarian neoplasms are often classified based on their cell type of origin, histological features, and potential for invasive or metastatic behavior.
Epithelial ovarian neoplasms are the most common type and can be further categorized into several subtypes, such as serous, mucinous, endometrioid, clear cell, and Brenner tumors. Some of these epithelial tumors have a higher risk of becoming malignant and spreading to other parts of the body.
Germ cell ovarian neoplasms arise from the cells that give rise to eggs (oocytes) and can include teratomas, dysgerminomas, yolk sac tumors, and embryonal carcinomas. Stromal ovarian neoplasms develop from the connective tissue cells supporting the ovary and can include granulosa cell tumors, thecomas, and fibromas.
It is essential to diagnose and treat ovarian neoplasms promptly, as some malignant forms can be aggressive and potentially life-threatening if not managed appropriately. Regular gynecological exams, imaging studies, and tumor marker tests are often used for early detection and monitoring of ovarian neoplasms. Treatment options may include surgery, chemotherapy, or radiation therapy, depending on the type, stage, and patient's overall health condition.
Aspermia is a medical term that refers to the absence of semen, which is typically released during ejaculation in males. This condition can occur due to various reasons such as obstruction in the reproductive tract, retrograde ejaculation (where semen flows backward into the bladder instead of out through the urethra), or a failure of the testicles to produce sperm. Aspermia is often associated with infertility and requires medical evaluation and treatment.
Pseudomyxoma Peritonei (PMP) is a rare, slow-growing, and invasive cancer that typically starts in the appendix as a low-grade mucinous neoplasm, although it can also arise from other organs of the abdominal cavity. The primary characteristic of PMP is the accumulation of copious amounts of gelatinous ascites (peritoneal fluid containing mucin) within the peritoneal cavity, causing progressive abdominal distension and discomfort.
The condition is classified into three main histological subtypes: disseminated peritoneal adenomucinosis (DPAM), peritoneal mucinous carcinomatosis (PMCA), and hybrid tumors. DPAM is the least aggressive form, while PMCA is more invasive and has a worse prognosis.
The primary treatment for Pseudomyxoma Peritonei involves cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC). This approach aims to remove all visible tumors and destroy any remaining cancer cells within the abdominal cavity. Early diagnosis and aggressive treatment can significantly improve the prognosis for patients with PMP, although long-term survival rates remain variable due to the disease's rarity and heterogeneity.
Salivary gland neoplasms refer to abnormal growths or tumors that develop in the salivary glands. These glands are responsible for producing saliva, which helps in digestion, lubrication of food and maintaining oral health. Salivary gland neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign neoplasms are slow-growing and typically do not spread to other parts of the body. They may cause symptoms such as swelling, painless lumps, or difficulty swallowing if they grow large enough to put pressure on surrounding tissues.
Malignant neoplasms, on the other hand, can be aggressive and have the potential to invade nearby structures and metastasize (spread) to distant organs. Symptoms of malignant salivary gland neoplasms may include rapid growth, pain, numbness, or paralysis of facial nerves.
Salivary gland neoplasms can occur in any of the major salivary glands (parotid, submandibular, and sublingual glands) or in the minor salivary glands located throughout the mouth and throat. The exact cause of these neoplasms is not fully understood, but risk factors may include exposure to radiation, certain viral infections, and genetic predisposition.
A pancreatic cyst is a fluid-filled sac that forms in the pancreas, a gland located behind the stomach that produces enzymes to help with digestion and hormones to regulate blood sugar levels. Pancreatic cysts can be classified into several types, including congenital (present at birth), retention (formed due to blockage of pancreatic ducts), and pseudocysts (formed as a result of injury or inflammation).
While some pancreatic cysts may not cause any symptoms, others can lead to abdominal pain, bloating, nausea, vomiting, or jaundice. Some cysts may also have the potential to become cancerous over time. Therefore, it is essential to monitor and evaluate pancreatic cysts through imaging tests such as ultrasound, CT scan, or MRI, and in some cases, endoscopic ultrasound (EUS) with fine-needle aspiration (FNA) may be necessary for further evaluation.
Treatment options for pancreatic cysts depend on the type, size, location, and symptoms of the cyst, as well as the patient's overall health condition. Some cysts may require surgical removal, while others can be managed with regular monitoring and follow-up care. It is essential to consult a healthcare provider for proper evaluation and management of pancreatic cysts.
Urologic surgical procedures in males refer to various surgical operations performed on the male urinary system and reproductive organs. These may include:
1. Transurethral Resection of the Prostate (TURP): A procedure used to treat an enlarged prostate, where excess tissue is removed through the urethra using a specialized instrument.
2. Radical Prostatectomy: The surgical removal of the entire prostate gland and some surrounding tissues, usually performed as a treatment for prostate cancer.
3. Cystectomy: Surgical removal of the bladder, often due to bladder cancer. In males, this procedure may also involve removing the prostate and seminal vesicles.
4. Nephrectomy: The surgical removal of a kidney, usually performed due to kidney disease or cancer.
5. Pyeloplasty: A procedure to correct a blockage in the renal pelvis, the part of the kidney where urine collects before flowing into the ureter.
6. Ureterostomy: A surgical procedure that creates an opening from the ureter to the outside of the body, often performed when a portion of the urinary system needs to be bypassed or drained.
7. Orchiectomy: The surgical removal of one or both testicles, often performed as a treatment for testicular cancer.
8. Vasectomy: A minor surgical procedure for male sterilization, where the vas deferens are cut and sealed to prevent sperm from reaching the semen.
9. Testicular Sperm Extraction (TESE): A surgical procedure used to extract sperm directly from the testicles, often performed as part of assisted reproductive techniques for infertile couples.
These procedures may be performed using open surgery, laparoscopy, or robotic-assisted surgery, depending on the specific circumstances and patient factors.
Multiple primary neoplasms refer to the occurrence of more than one primary malignant tumor in an individual, where each tumor is unrelated to the other and originates from separate cells or organs. This differs from metastatic cancer, where a single malignancy spreads to multiple sites in the body. Multiple primary neoplasms can be synchronous (occurring at the same time) or metachronous (occurring at different times). The risk of developing multiple primary neoplasms increases with age and is associated with certain genetic predispositions, environmental factors, and lifestyle choices such as smoking and alcohol consumption.
Retroperitoneal neoplasms refer to abnormal growths or tumors that develop in the retroperitoneal space. This is the area located behind the peritoneum, which is the membrane that lines the abdominal cavity and covers the abdominal organs. The retroperitoneal space contains several vital structures such as the kidneys, adrenal glands, pancreas, aorta, and lymphatic vessels.
Retroperitoneal neoplasms can be benign or malignant (cancerous). Malignant retroperitoneal neoplasms are often aggressive and can invade surrounding tissues and organs, leading to various complications. Common types of retroperitoneal neoplasms include lymphomas, sarcomas, and metastatic tumors from other primary sites. Symptoms may vary depending on the size and location of the tumor but can include abdominal or back pain, weight loss, and swelling in the legs. Diagnosis typically involves imaging studies such as CT scans or MRI, followed by a biopsy to determine the type and grade of the tumor. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Minor salivary glands are numerous small exocrine glands that produce saliva and are distributed throughout the oral cavity, nasal cavity, pharynx, larynx, and paranasal sinuses. They are classified as "minor" due to their smaller size compared to the three pairs of major salivary glands (parotid, submandibular, and sublingual). The minor salivary glands are primarily mucous glands, although some contain serous cells. They are responsible for producing approximately 5-10% of the total saliva in the mouth. These glands help moisten the oral cavity, protect the mucosal lining, and facilitate speaking, chewing, and swallowing.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
A pancreatic pseudocyst is a fluid-filled sac that forms in the abdomen, usually as a result of pancreatitis or trauma to the pancreas. It is composed of cells and tissues from the pancreas, along with enzymes, debris, and fluids. Unlike true cysts, pseudocysts do not have an epithelial lining. They can vary in size and may cause symptoms such as abdominal pain, nausea, vomiting, or fever. In some cases, they may resolve on their own, but larger or symptomatic pseudocysts may require medical intervention, such as drainage or surgery.
An ovarian cyst is a sac or pouch filled with fluid that forms on the ovary. Ovarian cysts are quite common in women during their childbearing years, and they often cause no symptoms. In most cases, ovarian cysts disappear without treatment over a few months. However, larger or persistent cysts may require medical intervention, including surgical removal.
There are various types of ovarian cysts, such as functional cysts (follicular and corpus luteum cysts), which develop during the menstrual cycle due to hormonal changes, and non-functional cysts (dermoid cysts, endometriomas, and cystadenomas), which can form due to different causes.
While many ovarian cysts are benign, some may have malignant potential or indicate an underlying medical condition like polycystic ovary syndrome (PCOS). Regular gynecological check-ups, including pelvic examinations and ultrasounds, can help detect and monitor ovarian cysts.
Magnetic resonance cholangiopancreatography (MRCP) is a non-invasive medical imaging technique that uses magnetic resonance imaging (MRI) to visualize the bile ducts and pancreatic duct. This diagnostic test does not use radiation like other imaging techniques such as computed tomography (CT) scans or endoscopic retrograde cholangiopancreatography (ERCP).
During an MRCP, the patient lies on a table that slides into the MRI machine. Contrast agents may be used to enhance the visibility of the ducts. The MRI machine uses a strong magnetic field and radio waves to produce detailed images of the internal structures, allowing radiologists to assess any abnormalities or blockages in the bile and pancreatic ducts.
MRCP is often used to diagnose conditions such as gallstones, tumors, inflammation, or strictures in the bile or pancreatic ducts. It can also be used to monitor the effectiveness of treatments for these conditions. However, it does not allow for therapeutic interventions like ERCP, which can remove stones or place stents.
Pancreatic diseases refer to a group of medical conditions that affect the structure and function of the pancreas, a vital organ located in the abdomen. The pancreas has two main functions: an exocrine function, which involves the production of digestive enzymes that help break down food in the small intestine, and an endocrine function, which involves the production of hormones such as insulin and glucagon that regulate blood sugar levels.
Pancreatic diseases can be broadly classified into two categories: inflammatory and non-inflammatory. Inflammatory pancreatic diseases include conditions such as acute pancreatitis, which is characterized by sudden inflammation of the pancreas, and chronic pancreatitis, which is a long-term inflammation that can lead to scarring and loss of function.
Non-inflammatory pancreatic diseases include conditions such as pancreatic cancer, which is a malignant tumor that can arise from the cells of the pancreas, and benign tumors such as cysts or adenomas. Other non-inflammatory conditions include pancreatic insufficiency, which can occur when the pancreas does not produce enough digestive enzymes, and diabetes mellitus, which can result from impaired insulin production or action.
Overall, pancreatic diseases can have serious consequences on a person's health and quality of life, and early diagnosis and treatment are essential for optimal outcomes.
Extrahepatic bile ducts refer to the portion of the biliary system that lies outside the liver. The biliary system is responsible for producing, storing, and transporting bile, a digestive fluid produced by the liver.
The extrahepatic bile ducts include:
1. The common hepatic duct: This duct is formed by the union of the right and left hepatic ducts, which drain bile from the corresponding lobes of the liver.
2. The cystic duct: This short duct connects the gallbladder to the common hepatic duct, allowing bile to flow into the gallbladder for storage and concentration.
3. The common bile duct: This is the result of the fusion of the common hepatic duct and the cystic duct. It transports bile from the liver and gallbladder to the duodenum, the first part of the small intestine, where it aids in fat digestion.
4. The ampulla of Vater (or hepatopancreatic ampulla): This is a dilated area where the common bile duct and the pancreatic duct join and empty their contents into the duodenum through a shared opening called the major duodenal papilla.
Extrahepatic bile ducts can be affected by various conditions, such as gallstones, inflammation (cholangitis), strictures, or tumors, which may require medical or surgical intervention.
An appendectomy is a surgical procedure in which the vermiform appendix is removed. This procedure is performed when a patient has appendicitis, which is an inflammation of the appendix that can lead to serious complications such as peritonitis or sepsis if not treated promptly. The surgery can be done as an open procedure, in which a single incision is made in the lower right abdomen, or as a laparoscopic procedure, in which several small incisions are made and specialized instruments are used to remove the appendix. In some cases, if the appendix has burst, a more extensive surgery may be required to clean out the abdominal cavity.
A pancreatectomy is a surgical procedure in which all or part of the pancreas is removed. There are several types of pancreatectomies, including:
* **Total pancreatectomy:** Removal of the entire pancreas, as well as the spleen and nearby lymph nodes. This type of pancreatectomy is usually done for patients with cancer that has spread throughout the pancreas or for those who have had multiple surgeries to remove pancreatic tumors.
* **Distal pancreatectomy:** Removal of the body and tail of the pancreas, as well as nearby lymph nodes. This type of pancreatectomy is often done for patients with tumors in the body or tail of the pancreas.
* **Partial (or segmental) pancreatectomy:** Removal of a portion of the head or body of the pancreas, as well as nearby lymph nodes. This type of pancreatectomy is often done for patients with tumors in the head or body of the pancreas that can be removed without removing the entire organ.
* **Pylorus-preserving pancreaticoduodenectomy (PPPD):** A type of surgery used to treat tumors in the head of the pancreas, as well as other conditions such as chronic pancreatitis. In this procedure, the head of the pancreas, duodenum, gallbladder, and bile duct are removed, but the stomach and lower portion of the esophagus (pylorus) are left in place.
After a pancreatectomy, patients may experience problems with digestion and blood sugar regulation, as the pancreas plays an important role in these functions. Patients may need to take enzyme supplements to help with digestion and may require insulin therapy to manage their blood sugar levels.
Cystadenocarcinoma, serous is a type of cystic tumor that arises from the lining of the abdominal or pelvic cavity (the peritoneum). It is called "serous" because the tumor cells produce a thin, watery fluid similar to serum.
Cystadenocarcinoma is a malignant (cancerous) tumor that can invade surrounding tissues and spread (metastasize) to other parts of the body. It typically affects women over the age of 50 and can cause symptoms such as abdominal pain, bloating, and changes in bowel or bladder habits.
Serous cystadenocarcinoma is a subtype of ovarian cancer that arises from the surface of the ovary. It can also occur in other organs, including the fallopian tubes, peritoneum, and endometrium. This type of tumor tends to grow slowly but can spread widely throughout the abdominal cavity, making it difficult to treat.
Treatment for serous cystadenocarcinoma typically involves surgery to remove the tumor and any affected tissues, followed by chemotherapy to kill any remaining cancer cells. The prognosis for this type of cancer depends on several factors, including the stage of the disease at diagnosis, the patient's age and overall health, and the response to treatment.
Adenocarcinoma, mucinous is a type of cancer that begins in the glandular cells that line certain organs and produce mucin, a substance that lubricates and protects tissues. This type of cancer is characterized by the presence of abundant pools of mucin within the tumor. It typically develops in organs such as the colon, rectum, lungs, pancreas, and ovaries.
Mucinous adenocarcinomas tend to have a distinct appearance under the microscope, with large pools of mucin pushing aside the cancer cells. They may also have a different clinical behavior compared to other types of adenocarcinomas, such as being more aggressive or having a worse prognosis in some cases.
It is important to note that while a diagnosis of adenocarcinoma, mucinous can be serious, the prognosis and treatment options may vary depending on several factors, including the location of the cancer, the stage at which it was diagnosed, and the individual's overall health.
 Cystadenoma
Cystadenoma
Ovarian cystadenoma
Serous cystadenoma
Mucinous cystadenoma
Pancreatic mucinous cystadenoma
Pancreatic serous cystadenoma
Ovarian serous cystadenoma
Ovary
Mucinous cystadenocarcinoma of the lung
Papillary serous cystadenocarcinoma
Surgical Outcomes Analysis and Research
Adenoma
Cystadenocarcinoma
Pancreatic mucinous cystic neoplasm
Appendix cancer
Hereditary leiomyomatosis and renal cell cancer syndrome
Aldred Scott Warthin
Intraductal papillary mucinous neoplasm
Bicornuate uterus
Ovarian cyst
Hidrocystoma
International Classification of Diseases for Oncology
Warthin's tumor
Endolymphatic sac tumor
Solid pseudopapillary tumour
List of skin conditions
Forme fruste
Serous cystadenocarcinoma
List of MeSH codes (C04)
Salivary gland tumour
Cystadenoma - Wikipedia
Ovarian cystadenoma - Wikipedia
 Pancreatic Serous Cystadenoma Imaging: Practice Essentials, Computed Tomography, Magnetic Resonance Imaging
Pancreatic Serous Cystadenoma Imaging: Practice Essentials, Computed Tomography, Magnetic Resonance Imaging
![Ovarian cystadenoma AND humans[mesh] AND review[publication type] - Search Results - PubMed](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAARVBMVEVHcEwoU45gYmYAUpQAUpRPYGVgYmZLXnJgYmYAUZUAUpRJXnIAUpQAUpRgYmYAUpRgYmZgYmZhYmYAUpQAUpQAUpRgYmaDiPJuAAAAFXRSTlMADOJ+6QewGO8/uTRqtH7GdFJ11p1bCL3TAAAAZUlEQVQYlV2PVw7AIAxDTeney7n/UcsoldX3E+VJOAboEi7MBpHWMs1ADlG8u7UYWauwyZFeRQVPOhG2o+aiwhByJxUx91Jxhje3iJSqGfHuLKI0+0TpXvY1twCOPlFh5pa/++MB0vIOBm+1zaoAAAAASUVORK5CYII=) Ovarian cystadenoma AND humans[mesh] AND review[publication type] - Search Results - PubMed
Ovarian cystadenoma AND humans[mesh] AND review[publication type] - Search Results - PubMed
 Cystadenoma | Ask or chat with U.S. doctors on HealthTap
Cystadenoma | Ask or chat with U.S. doctors on HealthTap
 Pancreatic Serous Cystadenoma | SeekHealthZ
Pancreatic Serous Cystadenoma | SeekHealthZ
Cystadenoma, Mucinous | Profiles RNS
Bronchial Cystadenoma - MD Nexus
 cystadenoma Archives - Small Animal Ultrasonography
cystadenoma Archives - Small Animal Ultrasonography
 Ovarian mucinous cystadenoma 2 - Radiology Cases
Ovarian mucinous cystadenoma 2 - Radiology Cases
 Serous Oligocystic Cystadenoma (SOA) - GI Cancer India...
Serous Oligocystic Cystadenoma (SOA) - GI Cancer India...
 Pages that link to "Serous cystadenoma" - Libre Pathology
Pages that link to "Serous cystadenoma" - Libre Pathology
 Humongous Ovarian Serous Cystadenoma in a Postmenopausal Woman | Scitechnol
Humongous Ovarian Serous Cystadenoma in a Postmenopausal Woman | Scitechnol
 A Postmenopausal Woman with Giant Ovarian Serous Cyst Adenoma - MediHelp
A Postmenopausal Woman with Giant Ovarian Serous Cyst Adenoma - MediHelp
 Case report Solid variant of serous cystadenoma of the pancreas
Case report Solid variant of serous cystadenoma of the pancreas
 An unusual presentation of pancreatic serous cystadenoma
| International Surgery Journal
An unusual presentation of pancreatic serous cystadenoma
| International Surgery Journal
 A giant serous ovarian cystadenoma in a young teenager patient - BosnianPathology
A giant serous ovarian cystadenoma in a young teenager patient - BosnianPathology
 Campagnacci R
Campagnacci R
Postmenopausal virilization second to a big ovarian cystadenoma using stromal hyperthecosis. | Jak signal
Adrenal Ectopia Within the Wall of an Ovarian Serous Cystadenoma - Balkan Medical Journal
 A massive ovarian mucinous cystadenoma: a case report | Reproductive Biology and Endocrinology | Full Text
A massive ovarian mucinous cystadenoma: a case report | Reproductive Biology and Endocrinology | Full Text
 Ovarian Cysts: Causes, Symptoms, and Treatment
Ovarian Cysts: Causes, Symptoms, and Treatment
Perspectives: Did you say biliary cystadenoma? Um, actually it's mucinous cystic neoplasm of the liver.
 Mucinous cystadenoma of the ovary with stromal luteinization and hyperestrinism in a post-menopausal female
Mucinous cystadenoma of the ovary with stromal luteinization and hyperestrinism in a post-menopausal female
The first case of primary retroperitoneal mucinous cystadenoma in Korea: A case report - Korea University
 Mucinous cystadenoma of a horseshoe kidney: A case report and literature review
| Canadian Urological Association...
Mucinous cystadenoma of a horseshoe kidney: A case report and literature review
| Canadian Urological Association...
 Ovarian Cyst Size: Types, What's Normal, When is Surgery Needed?
Ovarian Cyst Size: Types, What's Normal, When is Surgery Needed?
 High concentrations of inhibin A and inhibin B in ovarian serous cystadenoma: Relationship with oestradiol and nitric oxide...
High concentrations of inhibin A and inhibin B in ovarian serous cystadenoma: Relationship with oestradiol and nitric oxide...
EP729 A rare form of ovarian serous cystadenoma with monodermal teratoma in a 53 year old patient | International Journal of...
Mucinous cystadenoma10
- However, the following classifications also exist: serous cystadenoma (8441-8442) papillary cystadenoma (8450-8451, 8561) mucinous cystadenoma (8470-8473) Bile duct cystadenoma (8161) or biliary cystadenoma is a slow-growing tumour arising from bile ducts of the liver. (wikipedia.org)
- Endometrioid cystadenoma (8380) Appendix: The term mucinous cystadenoma is an obsolete term for appendiceal mucinous neoplasm The term "cystadenoma" may also refer to a hidrocystoma. (wikipedia.org)
- Macrocystic neoplasms of the pancreas: CT differentiation of serous oligocystic adenoma from mucinous cystadenoma and intraductal papillary mucinous tumor. (gicancerindia.com)
- To report the occurrence of a rare case of a huge benign ovarian tumour (mucinous cystadenoma) in Jazan city, Saudi Arabia. (biomedcentral.com)
- The case was reported as a rare massive ovarian mucinous cystadenoma. (biomedcentral.com)
- Ovarian mucinous cystadenoma is a benign tumour that arises from the surface epithelium of the ovary. (biomedcentral.com)
- This report presents a case of a giant ovarian mucinous cystadenoma in a Saudi woman, one of the biggest reported ovarian tumours in the medical literature. (biomedcentral.com)
- Cystectomy revealed a benign mucinous cystadenoma with stromal luteinization associated with elevated estradiol levels and features of hyperestrinism. (imrpress.com)
- The diagnosis was mucinous cystadenoma of the kidney. (cuaj.ca)
- Laparoscopic technique for removal of a retroperitoneal pubic bone mucinous cystadenoma. (advancedfertility.com)
Biliary cystadenoma6
- About 30% of biliary cystadenoma can progressively become malignant over time. (wikipedia.org)
- Perspectives: Did you say biliary cystadenoma? (nellymd.com)
- Watch Aarti Sekhar eloquently explain the new classification for biliary cystadenoma in 4 minutes at June Cases For Aces ! (nellymd.com)
- Computed tomography (CT) appearance of biliary cystadenoma. (medscape.com)
- Giant biliary cystadenoma complicated with polycystic liver: A case report. (wjgnet.com)
- Abdominal ultrasonography and subsequent computed tomography revealed a lesion with solid and liquid components in liver segment 4, considered consistent with a biliary cystadenoma or an echinococcal cyst. (cdc.gov)
Ovary4
- Ovarian cystadenoma is a cystic benign tumor of the ovary. (wikipedia.org)
- On histopathological examination, the cyst was confirmed as benign serous cystadenoma of the ovary. (medihelp.life)
- The histopathology was suggestive of benign serous cystadenoma of the ovary. (medihelp.life)
- Results The histology of the ovary showed a large serous cystadenoma (size 8.5 × 5.5 cm). (bmj.com)
Pancreas5
- The 2 most common cystic neoplasms of the pancreas are serous cystadenoma and mucinous cystic neoplasm. (medscape.com)
- A pancreatic serous cystadenoma is a benign glycogen-rich serous epithelial pancreatic neoplasm that can occur anywhere in the pancreas and is typically encountered in elderly women. (seekhealthz.com)
- Serous Cystadenoma of the pancreas: tumor growth rates and recommendations for treatment. (gicancerindia.com)
- We describe a case of a solid variant of serous cystadenoma of the pancreas. (archivesofmedicalscience.com)
- Solid variant of serous cystadenoma of the pancreas is difficult to diagnose preoperatively. (archivesofmedicalscience.com)
Tumour1
- The tumour was diagnosed as a solid variant of serous cystadenoma by histopathological examination. (archivesofmedicalscience.com)
Neoplasm3
- The important point to remember is that serous cystadenoma is benign, whereas the biologic behavior of the mucinous cystic neoplasm and the IPMT ranges from benign to malignant. (medscape.com)
- Serous cystadenoma (SCA) is a relatively rare pancreatic neoplasm which accounts for only 2% of pancreatic tumors (1-3). (spg.pt)
- Microcystic serous cystadenoma mimicking pancreatic neuroendocrine neoplasm: report of a resected case with preoperative diagnostic difficulty and review of the literature. (spg.pt)
Cystadenocarcinoma3
- Cyst fluid can be sent for CA 19-9 testing at the time of surgery as a marker for cystadenoma and cystadenocarcinoma. (medscape.com)
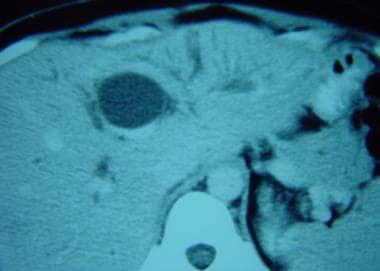
- Cystadenoma (see the image below) and cystadenocarcinoma usually appear multiloculated with internal septations, heterogeneous density, and irregularities in the cyst wall. (medscape.com)
- Unlike many tumors, cystadenoma and cystadenocarcinoma are rarely associated with calcifications. (medscape.com)
Solid serous cystadenoma1
- Hamid M, Tbouda M, Majbar AM, Raiss M, Ahallat M. Pancreatic solid serous cystadenoma treated by laparoscopy: Presentation of a new case report and review of the literature. (spg.pt)
Diagnosis1
- MRI revealed a cystic lesion with multiple millimetric cysts separated by filiform septations with mild wall enhancement and no restricted diffusion, establishing a diagnosis of serous cystadenoma. (spg.pt)
Epithelial1
- Inhibin production has been demonstrated in malignant epithelial ovarian tumours, but secretion of inhibins by benign cystadenoma has not yet been reported. (uniud.it)
Suggested a benign1
- Histopathological evaluation of mass suggested a benign serous cystadenoma. (scitechnol.com)
Ovarian serous2
- It is concluded that high amounts of dimeric inhibins are present in ovarian serous cystadenoma. (uniud.it)
- We present an interesting case of ovarian serous cystadenoma with monodermal teratoma, without clinical or biochemical features of hyperthyroidism, as well as the therapeutic approach. (bmj.com)
Adenoma1
- Cystadenoma (or "cystoma") is a type of cystic adenoma. (wikipedia.org)
Cysts1
- However, while functional cysts typically go away after several menstrual cycles, a cystadenoma will grow. (healthline.com)
Stromal1
- Postmenopausal virilization second to a big ovarian cystadenoma using stromal hyperthecosis. (jak-signal.com)
Retroperitoneal1
- We present here a case report of a 38-year-old Korean woman with primary retroperitoneal cystadenoma. (korea.ac.kr)
Findings3
- Findings from plain radiography and upper GI series are nondiagnostic, except the finding of a classic sunburst central calcification, which is suggestive of a serous cystadenoma. (medscape.com)
- A serous cystadenoma should be diagnosed with caution unless the lesion has all of the typical findings. (medscape.com)
- Serous oligocystic cystadenoma is a subgroup of pancreatic serous cystadenoma (SA) characterized by image findings described above. (gicancerindia.com)
Surgery1
- To avoid serious complications of pancreatic surgery, serous cystadenoma should be diagnosed accurately at the preoperative level. (medscape.com)
Patients1
- In a study of 2622 patients with serous cystadenoma, 74% were women, with a mean age of 58 years. (medscape.com)
Mesh1
- Cystadenoma, Mucinous" is a descriptor in the National Library of Medicine's controlled vocabulary thesaurus, MeSH (Medical Subject Headings) . (jefferson.edu)
Scan1
- Serous cystadenoma on a contrast-enhanced CT scan. (medscape.com)
Year1
- This graph shows the total number of publications written about "Cystadenoma, Mucinous" by people in this website by year, and whether "Cystadenoma, Mucinous" was a major or minor topic of these publications. (jefferson.edu)
Serous16
- However, the following classifications also exist: serous cystadenoma (8441-8442) papillary cystadenoma (8450-8451, 8561) mucinous cystadenoma (8470-8473) Bile duct cystadenoma (8161) or biliary cystadenoma is a slow-growing tumour arising from bile ducts of the liver. (wikipedia.org)
- The 2 most common cystic neoplasms of the pancreas are serous cystadenoma and mucinous cystic neoplasm. (medscape.com)
- The important point to remember is that serous cystadenoma is benign, whereas the biologic behavior of the mucinous cystic neoplasm and the IPMT ranges from benign to malignant. (medscape.com)
- In a study of 2622 patients with serous cystadenoma, 74% were women, with a mean age of 58 years. (medscape.com)
- To avoid serious complications of pancreatic surgery, serous cystadenoma should be diagnosed accurately at the preoperative level. (medscape.com)
- Findings from plain radiography and upper GI series are nondiagnostic, except the finding of a classic sunburst central calcification, which is suggestive of a serous cystadenoma. (medscape.com)
- Serous cystadenoma on a contrast-enhanced CT scan. (medscape.com)
- MRIs of serous cystadenoma. (medscape.com)
- Sonogram of serous cystadenoma. (medscape.com)
- A serous cystadenoma should be diagnosed with caution unless the lesion has all of the typical findings. (medscape.com)
- They account for nearly half of cystic neoplasms of the pancreas, with the others being serous cystadenoma (SCN) and intraductal papillary mucinous neoplasm (IPMN). (statpearls.com)
- To define the natural history and optimal treatment of pancreatic serous cystadenoma. (americansurgical.org)
- Records of 106 patients with pancreatic serous cystadenoma (1976-2004) were evaluated for patient and tumor characteristics, diagnostic workup, treatment, and outcomes. (americansurgical.org)
- Microscopic examination showed ischemic necrosis in most places and features of serous cystadenoma in viable areas of the lesion. (webpathology.com)
- She underwent a liver resection, and histopathology confirmed a serous biliary cystadenoma. (uwi.edu)
- Serous cystadenoma of the pancreas (or microcystic adenoma) benign cystic pancreatic neoplasm. (indianradiology.com)
Biliary4
- About 30% of biliary cystadenoma can progressively become malignant over time. (wikipedia.org)
- 4. Intrahepatic biliary cystadenoma mimicking hydatid cyst of liver: a clinicopathologic study of six cases. (nih.gov)
- 20. Biliary cystadenoma. (nih.gov)
- Abdominal ultrasonography and subsequent computed tomography revealed a lesion with solid and liquid components in liver segment 4, considered consistent with a biliary cystadenoma or an echinococcal cyst. (cdc.gov)
Benign2
- Ovarian cystadenoma is a cystic benign tumor of the ovary. (wikipedia.org)
- It was a benign cystadenoma. (cancer.org)
Borderline2
- Here, we present a case of a borderline ovarian mucinous cystadenoma with anaplastic mural nodule that has sarcomatoid differentiation, in a 39-year-old woman who presented with a 1-year history of progressive abdominal swelling and pain. (ecancer.org)
- In an independent cohort, the observed methylation was 40% (146/365) in OC, 12.5% (2/16) in borderline tumors, 11% (2/18) in cystadenoma and 0% (0/13) in normal ovarian epithelium samples. (ugent.be)
Malignant1
- Because of the malignant potential of cystadenoma, a role also does not exist for medical therapy for this lesion. (medscape.com)