Orbital Fractures
Proplast
Skull Fractures
Diplopia
Eyelid Diseases
Compartment Syndromes
The silent sinus syndrome. (1/20)
Patients with silent sinus syndrome typically present for investigation of facial asymmetry. Unilateral, spontaneous enophthalmos and hypoglobus are the prominent findings at examination. Imaging of the orbit and sinuses characteristically show unilateral maxillary sinus opacification and collapse with inferior bowing of the orbital floor. It has been suggested that SSS is due to hypoventilation of the maxillary sinus secondary to ostial obstruction and sinus atelectasis with chronic negative pressure within the sinus. Treatment involves functional endoscopic sinus surgery for reestablishing a functional drainage passage, and a reconstructive procedure of the floor of the orbit for repairing the hypoglobus and cosmetic deformity. Ophthalmologists, otorhinolaryngologists, and radiologists must be familiarized with this relatively newly reported disease. (+info)Lagophthalmos in enophthalmic eyes. (2/20)
AIMS: To report a case series of enophthalmic patients with lagophthalmos. METHODS: A retrospective review of the electronic medical records at a tertiary health care centre of all patients with the diagnoses of "enophthalmos" and "lagophthalmos". Patients who had a history of diseases (such as Graves' orbitopathy), trauma or surgery of the orbit and eyelid were excluded. Enophthalmos was defined as exophthalmometric reading of 14 mm or less in both eyes. RESULTS: Seven patients (14 eyes) with bilateral enophthalmos were found to have concomitant lagophthalmos. All patients had deep superior sulci bilaterally. The upper eyelids were seen to be severely retro-placed behind the superior orbital rim. The extraocular motilities were full with no focal neurological deficit. The orbicularis oculi function was normal with no facial paralysis. The orbits were soft on retropulsion and no facial asymmetry was noted. The mean exophthalmolmetry reading measured 12.6 (SD 1.1) mm. The lagophthalmos varied from 1-5 mm. One patient (one eye) with 3 mm lagophthalmos developed a corneal ulcer and was treated with topical antibiotics and gold weight placement in the upper eyelid. CONCLUSION: Enophthalmic patients with deep superior sulci and retro-placed upper eyelids may present with lagophthalmos and exposure keratopathy. (+info)Correction of superior sulcus deformity and enophthalmos with porous high-density polyethylene sheet in anophthalmic patients. (3/20)
PURPOSE: Superior sulcus deformity is the main cosmetic problem in anophthalmic patients. Many methods of correcting enophthalmos have been reported, especially in patients with orbital wall fracture. The purpose of this study is to review the long term results of effectiveness in superior sulcus deformity correction by subperiosteal Medpor sheet implantation in anophthalmic patients. METHODS: Subperiosteal Medpor sheets were used in 11 eyes of 11 anophthalmic patients. To estimate the effectiveness, photographs were taken and exophthalmometric value with their own prosthesis using Hertel exophthalmometer was measured in all patients before and after surgery. RESULTS: The overall cosmetic results in superior sulcus deformity were 'excellent' in 3 (27.3%), 'good' in 6 (54.5%), 'fair' in 2 (18.2%). The overall results in enophthalmos were 'excellent' in 3 (27.2%), 'markedly improved' in 4 (36.4%), 'slightly improved' in 4 (36.4%). Most patients had a marked increase in orbital volume, except two patients. They received irradiation treatment in early childhood so showed unsatisfactory results in both superior sulcus deformity and enophthalmos. CONCLUSIONS: Subperiosteal Medpor sheet implantation is considered to be a reliable and safe procedure without serious complication and with an excellent cosmetic result. (+info)Wide clinical variability among 13 new Cockayne syndrome cases confirmed by biochemical assays. (4/20)
Cockayne syndrome is a multi-systemic, autosomal recessive disease characterised by postnatal growth failure and progressive multi-organ dysfunction. The main clinical features are severe dwarfism (<-2 SD), microcephaly (<-3 SD), psychomotor delay, sensorial loss (cataracts, pigmentary retinopathy, and deafness), and cutaneous photosensitivity. Here, 13 new cases of Cockayne syndrome are reported, which have been clinically diagnosed and confirmed using a biochemical transcription assay. The wide clinical variability, ranging from prenatal features to normal psychomotor development, is emphasised. When cardinal features are lacking, the diagnosis of Cockayne syndrome should be considered when presented with growth retardation, microcephaly, and one of the suggesting features such as enophthalmia, limb ataxia, abnormal auditory evoked responses, or increased ventricular size on cerebral imaging. (+info)Evaluation of computer-based volume measurement and porous polyethylene channel implants in reconstruction of large orbital wall fractures. (5/20)
PURPOSE: To describe the use of computer-based orbital volume measurement as a predictor of late enophthalmos, and to assess the effectiveness of the MedPor (Porex Surgical Products Group, Newnan, GA) porous polyethylene channel implant to restore orbital volume in repairing large orbital wall fractures. METHODS: Sixteen patients with unilateral large orbital fractures were included. Computed tomographic (CT) scans were used to obtain computer-based orbital volume measurement to predict the likelihood of late enophthalmos and to assess the change in orbital volume before and after surgery. The effectiveness of a channel implant was evaluated by the orbital volume and postoperative exophthalmetric measurement. RESULTS: The average time interval between injury and surgery was 17.4 +/- 10 days, and the mean follow-up was 9 months. The orbital volume of the injured orbit was significantly increased (mean, 4.22 +/- 2.61 cm2) compared with the unaffected orbit before surgery (t = 3.046, P = 0.005). There was not a significant difference in orbital volume between the two orbits after orbital reconstruction (t = 0.069, P = 0.945). The orbital volume change after reconstructive surgery was significantly positively correlated with the decrease of enophthalmos (r = 0.715, P = 0.001; enophthalmos [E] = 0.72; volume increment [V] = 0.06). To resolve 2 mm enophthalmos, more than 2.9 cm3 orbital volume augmentation is recommended for early reconstructive surgery. Postoperative CT scan showed most of the channel implants to be well positioned. CONCLUSIONS: Computer-based orbital volume measurement from a CT scan is useful in the posttraumatic evaluation of orbital fractures, and it can help predict the degree of late enophthalmos that can be expected. Orbital reconstruction with the MedPor channel implant (Porex Surgical Products Group), when indicated, is recommended, especially for large orbital wall fractures. (+info)Management of posttraumatic enophthalmos. (6/20)
Posttraumatic enophthalmos is one of the common sequelae that appears after facial injury and remains a challenge to treat for craniomaxillofacial surgeons. Several theories have been advocated regarding enophthalmos; however, the most well accepted concept is the enlargement of the orbital cavity after displacement due to orbital fractures. Generally, a 1 cm3 increase in orbital volume causes 0.8 mm of enophthalmos. Thorough knowledge of the orbital anatomy is fundamental and critical for the successful surgical correction of enophthalmos because most treatment failures are due to inadequate orbital dissection from fear of injuring the optic nerve and globe. A complete preoperative plan should be built on a comprehensive clinical examination of the periorbital soft tissue and bony components, detailed ophthalmic examination, and high resolution computed tomography scans in the axial, coronal and reformatted sagittal planes. Based on the anatomic deformities, there are two major fracture types including orbital blow out fractures and zygomatico-orbital fractures, resulting in posttraumatic enophthalmos. Treatment modalities and methods of approach are adapted according to the severity of the orbital deformities. Minor complications include ectropion, entropion, dystopia, diplopia, and residual enophthalmos. Rare but severe complications such as intraconal misplacement of the bone graft or retrobulbar hemorrhage with subsequent blindness may be encountered. The success of the procedures depend on adequate dissection and mobilization of the displaced soft tissue, correct repositioning of the dislocated or malunited bony orbit, and proper intra-orbital grafting. (+info)The ophthalmic implications of the correction of late enophthalmos following severe midfacial trauma. (7/20)
Severe midfacial trauma presents several challenges to the reconstructive surgeon. Acute rigid fixation of the facial skeleton accompanied by bone grafting to restore the confines and volume of the orbit provide the best opportunity for acceptable aesthetic results. The severity of the trauma causes the late postoperative complication of enophthalmos. Injury to orbital structures with subsequent cicatricial change results in significant alteration in extraocular motility with resultant diplopia. There are no reports in the literature which critically evaluate the effect of late enophthalmos correction on extraocular motility, diplopia, and vision in patients who have suffered Le Fort or NOE fractures. A retrospective study is presented which reviews the results of late surgery for the correction of enophthalmos in 40 patients, all of whom had severe "impure" orbital fractures. This study addresses the following questions: (1) Can the globe effectively be repositioned?, (2) Is there a change in subjective diplopia?, (3) Does a change in extraocular motility occur, and if it does, is it predictable?, (4) Is there a risk to visual acuity? and finally, (5) Do the answers to questions 1 through 4 suggest that late surgical intervention for the correction of enophthalmos should be recommended for this patient population? During a 9-year period, 44 patients with severe diplopia trauma received surgery for enophthalmos correction. A review of 40 patients on whom 56 operations were performed is presented. Thirty-eight patients had enophthalmos and 35 had inferior displacement of the globe. Medial displacement of the globe occurred in 11 patients. Twenty-nine patients had diplopia. Six patients had vision too poor on the injured side to have diplopia. Enophthalmos was improved in 32 patients. Dystopia of the globe was improved in 31 cases. However, neither enophthalmos nor dystopia of the globe could be improved with every operation. Only 35 of the 48 operations for enophthalmos for which measurements were available produced an improvement; in 1 case the enophthalmos was thought to be worse postoperatively. Dystopia operations resulted in improvement in 40 of 48 operations; in 2 instances dystopia was worse postoperatively. Diplopia was unchanged by 33 operations, improved by 11 procedures, and worsened by 6. If patients are considered before and after their total reconstruction course, diplopia was improved in 9 of the 29 patients. In seven of these nine, diplopia was eliminated. There was no change in or production of diplopia in 19 patients, and 5 patients had worsening of their double vision.(ABSTRACT TRUNCATED AT 400 WORDS) (+info)Pulsating enophthalmos in association with an orbital varix. (8/20)
(+info)Enophthalmos is a medical term that refers to the abnormal positioning of the eyeball within its socket, resulting in a posterior or backward displacement of the eye. This condition can occur due to various reasons such as trauma, surgical procedures, or diseases that affect the orbital tissues, including cancer, inflammation, or infection. Enophthalmos may lead to cosmetic concerns and visual disturbances, depending on its severity. A thorough examination by an ophthalmologist or an oculoplastic surgeon is necessary for accurate diagnosis and management of this condition.
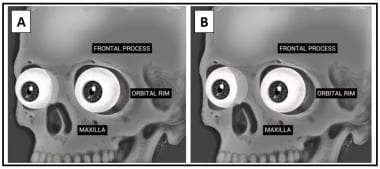
Orbital fractures refer to breaks in the bones that make up the eye socket, also known as the orbit. These bones include the maxilla, zygoma, frontal bone, and palatine bone. Orbital fractures can occur due to trauma, such as a blunt force injury or a penetrating wound.
There are several types of orbital fractures, including:
1. Blowout fracture: This occurs when the thin bone of the orbital floor is broken, often due to a direct blow to the eye. The force of the impact can cause the eyeball to move backward, breaking the bone and sometimes trapping the muscle that moves the eye (the inferior rectus).
2. Blow-in fracture: This type of fracture involves the breakage of the orbital roof, which is the bone that forms the upper boundary of the orbit. It typically occurs due to high-impact trauma, such as a car accident or a fall from a significant height.
3. Direct fracture: A direct fracture happens when there is a break in one or more of the bones that form the walls of the orbit. This type of fracture can result from a variety of traumas, including motor vehicle accidents, sports injuries, and assaults.
4. Indirect fracture: An indirect fracture occurs when the force of an injury is transmitted to the orbit through tissues surrounding it, causing the bone to break. The most common type of indirect orbital fracture is a blowout fracture.
Orbital fractures can cause various symptoms, including pain, swelling, bruising, and double vision. In some cases, the fracture may also lead to enophthalmos (sinking of the eye into the orbit) or telecanthus (increased distance between the inner corners of the eyes). Imaging tests, such as CT scans, are often used to diagnose orbital fractures and determine the best course of treatment. Treatment may include observation, pain management, and in some cases, surgery to repair the fracture and restore normal function.
Facial injuries refer to any damage or trauma caused to the face, which may include the bones of the skull that form the face, teeth, salivary glands, muscles, nerves, and skin. Facial injuries can range from minor cuts and bruises to severe fractures and disfigurement. They can be caused by a variety of factors such as accidents, falls, sports-related injuries, physical assaults, or animal attacks.
Facial injuries can affect one or more areas of the face, including the forehead, eyes, nose, cheeks, ears, mouth, and jaw. Common types of facial injuries include lacerations (cuts), contusions (bruises), abrasions (scrapes), fractures (broken bones), and burns.
Facial injuries can have significant psychological and emotional impacts on individuals, in addition to physical effects. Treatment for facial injuries may involve simple first aid, suturing of wounds, splinting or wiring of broken bones, reconstructive surgery, or other medical interventions. It is essential to seek prompt medical attention for any facial injury to ensure proper healing and minimize the risk of complications.
In medical terms, the orbit refers to the bony cavity or socket in the skull that contains and protects the eye (eyeball) and its associated structures, including muscles, nerves, blood vessels, fat, and the lacrimal gland. The orbit is made up of several bones: the frontal bone, sphenoid bone, zygomatic bone, maxilla bone, and palatine bone. These bones form a pyramid-like shape that provides protection for the eye while also allowing for a range of movements.
I'm sorry for any confusion, but "Proplast" is not a term commonly used in medical terminology. Proplast was a brand name for a type of biocompatible material that was often used in medical and dental applications as an implant material or for the coating of orthopedic and dental implants. It was composed of a combination of carbon, polyethylene, and other materials. However, it is no longer in use due to concerns about its long-term durability and biocompatibility.
If you have any questions related to medical terminology or health-related topics, I would be happy to help!
A skull fracture is a break in one or more of the bones that form the skull. It can occur from a direct blow to the head, penetrating injuries like gunshot wounds, or from strong rotational forces during an accident. There are several types of skull fractures, including:
1. Linear Skull Fracture: This is the most common type, where there's a simple break in the bone without any splintering, depression, or displacement. It often doesn't require treatment unless it's near a sensitive area like an eye or ear.
2. Depressed Skull Fracture: In this type, a piece of the skull is pushed inward toward the brain. Surgery may be needed to relieve pressure on the brain and repair the fracture.
3. Diastatic Skull Fracture: This occurs along the suture lines (the fibrous joints between the skull bones) that haven't fused yet, often seen in infants and young children.
4. Basilar Skull Fracture: This involves fractures at the base of the skull. It can be serious due to potential injury to the cranial nerves and blood vessels located in this area.
5. Comminuted Skull Fracture: In this severe type, the bone is shattered into many pieces. These fractures usually require extensive surgical repair.
Symptoms of a skull fracture can include pain, swelling, bruising, bleeding (if there's an open wound), and in some cases, clear fluid draining from the ears or nose (cerebrospinal fluid leak). Severe fractures may cause brain injury, leading to symptoms like confusion, loss of consciousness, seizures, or neurological deficits. Immediate medical attention is necessary for any suspected skull fracture.
Diplopia is a medical term that refers to the condition where a person sees two images of a single object. It is commonly known as double vision. This can occur due to various reasons, such as nerve damage or misalignment of the eyes. Diplopia can be temporary or chronic and can affect one or both eyes. If you're experiencing diplopia, it's essential to consult an eye care professional for proper evaluation and treatment.
Eyelid diseases refer to a variety of medical conditions that affect the function and/or appearance of the eyelids. These can include structural abnormalities, such as entropion (inward turning of the eyelid) or ectropion (outward turning of the eyelid), as well as functional issues like ptosis (drooping of the upper eyelid). Other common eyelid diseases include blepharitis (inflammation of the eyelid margin), chalazion (a blocked oil gland in the eyelid), and cancerous or benign growths on the eyelid. Symptoms of eyelid diseases can vary widely, but often include redness, swelling, pain, itching, tearing, and sensitivity to light. Treatment for these conditions depends on the specific diagnosis and may range from self-care measures and medications to surgical intervention.
Orbital diseases refer to a group of medical conditions that affect the orbit, which is the bony cavity in the skull that contains the eye, muscles, nerves, fat, and blood vessels. These diseases can cause various symptoms such as eyelid swelling, protrusion or displacement of the eyeball, double vision, pain, and limited extraocular muscle movement.
Orbital diseases can be broadly classified into inflammatory, infectious, neoplastic (benign or malignant), vascular, traumatic, and congenital categories. Some examples of orbital diseases include:
* Orbital cellulitis: a bacterial or fungal infection that causes swelling and inflammation in the orbit
* Graves' disease: an autoimmune disorder that affects the thyroid gland and can cause protrusion of the eyeballs (exophthalmos)
* Orbital tumors: benign or malignant growths that develop in the orbit, such as optic nerve gliomas, lacrimal gland tumors, and lymphomas
* Carotid-cavernous fistulas: abnormal connections between the carotid artery and cavernous sinus, leading to pulsatile proptosis and other symptoms
* Orbital fractures: breaks in the bones surrounding the orbit, often caused by trauma
* Congenital anomalies: structural abnormalities present at birth, such as craniofacial syndromes or dermoid cysts.
Proper diagnosis and management of orbital diseases require a multidisciplinary approach involving ophthalmologists, neurologists, radiologists, and other specialists.
Compartment syndromes refer to a group of conditions characterized by increased pressure within a confined anatomical space (compartment), leading to impaired circulation and nerve function. These compartments are composed of bones, muscles, tendons, blood vessels, and nerves, surrounded by a tough fibrous fascial covering that does not expand easily.
There are two main types of compartment syndromes: acute and chronic.
1. Acute Compartment Syndrome (ACS): This is a medical emergency that typically occurs after trauma, fractures, or prolonged compression of the affected limb. The increased pressure within the compartment reduces blood flow to the muscles and nerves, causing ischemia, pain, and potential muscle and nerve damage if not promptly treated with fasciotomy (surgical release of the fascial covering). Symptoms include severe pain disproportionate to the injury, pallor, paresthesia (abnormal sensation), pulselessness, and paralysis.
2. Chronic Compartment Syndrome (CCS) or Exertional Compartment Syndrome: This condition is caused by repetitive physical activities that lead to increased compartment pressure over time. The symptoms are usually reversible with rest and may include aching, cramping, tightness, or swelling in the affected limb during exercise. CCS rarely leads to permanent muscle or nerve damage if managed appropriately with activity modification, physical therapy, and occasionally surgical intervention (fasciotomy or fasciectomy).
Early recognition and appropriate management of compartment syndromes are crucial for preventing long-term complications such as muscle necrosis, contractures, and nerve damage.
A retrobulbar hemorrhage is a rare but serious condition that involves the accumulation of blood in the retrobulbar space, which is the area between the back surface of the eyeball (the globe) and the front part of the bony socket (orbit) that contains it. This space is normally filled with fatty tissue and various supportive structures like muscles, nerves, and blood vessels.
Retrobulbar hemorrhage typically occurs as a result of trauma or surgery to the eye or orbit, causing damage to the blood vessels in this area. The bleeding can lead to increased pressure within the orbit, which may compress the optic nerve and restrict the flow of blood and oxygen to the eye. This can result in rapid vision loss, proptosis (forward displacement of the eyeball), pain, and other ocular dysfunctions.
Immediate medical attention is required for retrobulbar hemorrhage, as it can lead to permanent visual impairment or blindness if not treated promptly. Treatment options may include observation, medication, or surgical intervention to relieve the pressure and restore blood flow to the eye.
An eye hemorrhage, also known as subconjunctival hemorrhage, is a condition where there is bleeding in the eye, specifically under the conjunctiva which is the clear membrane that covers the white part of the eye (sclera). This membrane has tiny blood vessels that can rupture and cause blood to accumulate, leading to a visible red patch on the surface of the eye.
Eye hemorrhages are usually painless and harmless, and they often resolve on their own within 1-2 weeks without any treatment. However, if they occur frequently or are accompanied by other symptoms such as vision changes, pain, or sensitivity to light, it is important to seek medical attention as they could indicate a more serious underlying condition. Common causes of eye hemorrhages include trauma, high blood pressure, blood thinners, and aging.
Surgical decompression is a medical procedure that involves relieving pressure on a nerve or tissue by creating additional space. This is typically accomplished through the removal of a portion of bone or other tissue that is causing the compression. The goal of surgical decompression is to alleviate symptoms such as pain, numbness, tingling, or weakness caused by the compression.
In the context of spinal disorders, surgical decompression is often used to treat conditions such as herniated discs, spinal stenosis, or bone spurs that are compressing nerves in the spine. The specific procedure used may vary depending on the location and severity of the compression, but common techniques include laminectomy, discectomy, and foraminotomy.
It's important to note that surgical decompression is a significant medical intervention that carries risks such as infection, bleeding, and injury to surrounding tissues. As with any surgery, it should be considered as a last resort after other conservative treatments have been tried and found to be ineffective. A thorough evaluation by a qualified medical professional is necessary to determine whether surgical decompression is appropriate in a given case.
 Enophthalmos - Wikipedia
Enophthalmos - Wikipedia
 Enophthalmos: Background, Pathophysiology, Epidemiology
Enophthalmos: Background, Pathophysiology, Epidemiology
301920009 - Enophthalmos present - SNOMED CT
 Correlation between increased orbital volume and enophthalmos and diplopia in patients with fractures of the orbital floor or...
Correlation between increased orbital volume and enophthalmos and diplopia in patients with fractures of the orbital floor or...
Enophthalmos definition, causes, symptoms, diagnosis & treatment
 Enophthalmos Wedges - Matrix Surgical | Omnipore surgical implants
Enophthalmos Wedges - Matrix Surgical | Omnipore surgical implants
 December 1974 - Volume 54 - Issue 6 : Plastic and Reconstructive Surgery
December 1974 - Volume 54 - Issue 6 : Plastic and Reconstructive Surgery
 Prediction of post-traumatic enophthalmos based on orbital volume measurements: a systematic review
Prediction of post-traumatic enophthalmos based on orbital volume measurements: a systematic review
 Lally SE - Search Results - PubMed
Lally SE - Search Results - PubMed
 Comparison of Postoperative Enophthalmos Between Fresh and Delayed Unilateral Orbital Fractures After Orbital Reconstruction...
Comparison of Postoperative Enophthalmos Between Fresh and Delayed Unilateral Orbital Fractures After Orbital Reconstruction...
 Leber Congenital Amaurosis - American Academy of Ophthalmology
Leber Congenital Amaurosis - American Academy of Ophthalmology
 César A. Briceño, MD profile | PennMedicine.org
César A. Briceño, MD profile | PennMedicine.org
 Molecular Vision: Yzer, Mol Vis 2012; 18:412-425. Table 2
Molecular Vision: Yzer, Mol Vis 2012; 18:412-425. Table 2
 Orbital Socket Fractures: How to Identify and Treat Them
Orbital Socket Fractures: How to Identify and Treat Them
 Duane syndrome
Duane syndrome
 IndexCat
IndexCat
Neck Trauma Management Clinical Presentation: History, Physical Examination
Lateral Canthotomy and Cantholysis: Overview, Indications, Contraindications
 Effects of Aging on the Eyes - Eye Disorders - Merck Manuals Consumer Version
Effects of Aging on the Eyes - Eye Disorders - Merck Manuals Consumer Version
 Clinical Services Offered
Clinical Services Offered
GMS | GMS Current Topics in Otorhinolaryngology - Head and Neck Surgery | Risks and complications in rhinoplasty
 The Israel Medical Association Journal (IMAJ) | Search results
The Israel Medical Association Journal (IMAJ) | Search results
 Changes in fluid volume
Changes in fluid volume
The Neurologic Examination of Animals - Nervous System - Merck Veterinary Manual
Orbital medial wall fractures: diagnosis and treatment - Italian Journal of Maxillofacial Surgery 2010 December;21(3):133-8 -...
Eyelids in Animals - Eye Diseases and Disorders - Merck Veterinary Manual
Sphenoid Wing Meningioma: Practice Essentials, Background, Pathophysiology
 Ptosis Correction - StatPearls - NCBI Bookshelf
Ptosis Correction - StatPearls - NCBI Bookshelf
 Course Content - #92073: Care of the Pediatric Trauma Patient - NetCE
Course Content - #92073: Care of the Pediatric Trauma Patient - NetCEPost-traumatic enophthalmos2
- [ 2 ] An example of a blow-out fracture with post-traumatic enophthalmos is shown in the image below. (medscape.com)
- None of the currently used techniques is able to accurately predict for post-traumatic enophthalmos (PE). (univ-lille.fr)
Diplopia2
- Diplopia and enophthalmos measurements 3 months after surgery were compared with preoperative measurement. (minervamedica.it)
- Using this approach, they achieved several advantages, including avoidance of external scars, anatomically correct reconstruction of the orbital floor, resolution of enophthalmos and diplopia, minimal discomfort for the patient, and substantial reduction of costs. (materialise.com)
Orbit6
- Enophthalmos is a posterior displacement of the eyeball within the orbit. (wikipedia.org)
- It may be a congenital anomaly, or be acquired as a result of trauma (such as in a blowout fracture of the orbit), Horner's syndrome (apparent enophthalmos due to ptosis), Marfan syndrome, Duane's syndrome, silent sinus syndrome or phthisis bulbi. (wikipedia.org)
- Secondary enophthalmos is due to an acquired change in volumetric relationship between the rigid bone cavity, the orbit, and its contents (predominantly the orbital fat, the extraocular muscles, and the eye). (medscape.com)
- Enophthalmos Wedges help elevate and anteriorize the globe and provide volume to restore the orbit to its normal size and shape. (matrixsurgicalusa.com)
- It may occur when the eye itself moves backwards into the orbit (enophthalmos), or when the eye becomes shrunken following a severe injury or infection. (petplace.com)
- Orbital floor fractures can increase volume of the orbit with resultant hypoglobus and enophthalmos. (medscape.com)
Entropion1
- In foals and lambs, entropion is secondary to enophthalmos from mild dehydration and/or corneal ulceration. (merckvetmanual.com)
Ptosis3
- New data finds that preoperative ptosis occurs commonly and more often in patients with reactive blepharospasm or enophthalmos. (ophthalmologytimes.com)
- Analysis of data from a cohort of patients who underwent enucleation indicated that preoperative ptosis occurs commonly and more often in patients with reactive blepharospasm or enophthalmos. (ophthalmologytimes.com)
- The ptosis is due to denervation of the tarsal muscle (Müller muscle) in both the upper and the lower eyelids, producing a noticeably narrower palpebral fissure and the false impression of enophthalmos. (aao.org)
Fractures5
- Acute posttraumatic enophthalmos, in absence of direct injuries of the globe is generally due to blowout fractures with herniation of the orbital soft tissues in the adjacent paranasal sinuses. (healthjade.com)
- Comparison of Postoperative Enophthalmos Between Fresh and Delayed Unilateral Orbital Fractures After Orbital Reconstruction With Titanium Mesh Using Computer-Assisted Navigation. (bvsalud.org)
- enophthalmos between T1 and T2) was similar in patients with fresh and delayed fractures. (bvsalud.org)
- Furthermore, the recurrence of enophthalmos is similar between the 2 groups, but it is higher in patients with orbital fractures involving 2 walls. (bvsalud.org)
- To provide surgeons with an adequate implant that addresses the requirements of two wall acute orbital fractures or for secondary reconstruction of enophthalmos and dystopia, a new series of preformed orbital plates was developed for the new orbital matrix system. (aofoundation.org)
Spontaneous enophthalmos2
- A cause of spontaneous enophthalmos. (medscape.com)
- Silent sinus syndrome is a rare disease characterized by spontaneous enophthalmos and hypoglobus (an abnormal lowering of the globe usually due to a deficient anterior orbital floor) secondary to collapse of the orbital floor in patients with asymptomatic maxillary sinusitis. (healthjade.com)
Fracture6
- Expansion of the orbital cavity without change in the volume of orbital contents (ie, a blow-out fracture) leads to enophthalmos. (medscape.com)
- One of the most common causes of enophthalmos is orbital fracture. (medscape.com)
- Correlation of types of orbital fracture and occurrence of enophthalmos. (medscape.com)
- Surgical correction of severe strabismus and enophthalmos secondary to zygomatic arch fracture in a dog. (ncsu.edu)
- The sample was composed of 45 patients with post-traumatic unilateral enophthalmos who were divided into the fresh fracture group and the delayed fracture group. (bvsalud.org)
- The following parameters were measured with computed tomography images the degree of enophthalmos , orbital volume, and fracture defect area. (bvsalud.org)
Posterior displacement1
- Enophthalmos is the posterior displacement of the globe into the orbital cavity. (medscape.com)
Preoperative1
- The findings indicate that postoperative enophthalmos is common in both the groups and is closely related to the degree of preoperative enophthalmos . (bvsalud.org)
Displacement2
- The difficulty has always been the best method to use to accurately determine when the orbital wall displacement will lead to clinically relevant enophthalmos. (univ-lille.fr)
- It has been notoriously difficult to determine when orbital wall displacement will lead to clinically relevant enophthalmos. (univ-lille.fr)
Volumetric1
- METHODS: The terms searched in each database were "(orbital volumetry) and enophthalmos," "volumetry and enophthalmos," "volume and enophthalmos," and "volumetric and enophthalmos. (univ-lille.fr)
Unilateral1
- Unilateral enophthalmos. (nih.gov)
Eyeball1
- Enophthalmos is the sinking of the eyeball towards the back part of the eye socket. (healthjade.com)
Clinically2
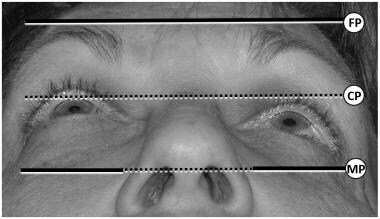
- Enophthalmos becomes clinically obvious if the anterior globe projection is less than 12 mm or differs from the opposite side by 3 mm or more as measured by a Hertel exophthalmometer. (healthjade.com)
- OBJECTIVE: Enophthalmos greater than 2 mm should be considered clinically relevant and can be responsible for esthetic and functional morbidity. (univ-lille.fr)
Facial1
- Some degree of facial asymmetry is common, but congenital relative enophthalmos or ocular retrusion may occur with in utero maldevelopment (eg, plagiocephaly, microphthalmos). (medscape.com)
Palpebral fissure1
- The supratarsal crease may deepen, along with narrowing of the palpebral fissure stemming from enophthalmos or fibrous tissue contraction. (medscape.com)
Atrophy1
- [ 4 , 5 ] Other potential causes for enophthalmos include age-related fat atrophy or HIV-related lipodystrophy, although these usually present with bilaterally symmetric enophthalmos. (medscape.com)
Surgical1
- Most causes of enophthalmos are treatable, and surgical correction is most frequently excellent following outpatient surgery. (medscape.com)
Etiology1
- Primary enophthalmos indicates a congenital or developmental etiology. (medscape.com)
Assessment1
- Enophthalmos assessment using radiologic evaluation provides increased accuracy and reproducibility compared with clinical measurement using an exophthalmometer. (univ-lille.fr)
Volume1
- Alternatively, scarring contracture of the orbital fat and extraocular muscles may decrease soft tissue volume, making the orbital cavity less full and causing enophthalmos. (medscape.com)
Patient3
- Perhaps the single most important advice to give a patient until the workup of suspected new-onset enophthalmos has been completed is not to blow their nose and to sneeze with their mouth open. (medscape.com)
- Patient has significant enophthalmos in the left eye. (healthjade.com)
- Patient has improvement in enophthalmos. (healthjade.com)
Greater than 2 mm1
- Enophthalmos greater than 2 mm relative to the contralateral eye creates an observable cosmetic deformity. (medscape.com)
Obvious1
- this may result in obvious enophthalmos and sunken eye particularly when brokers are used unilaterally. (atpobtvs.com)
Present1
- Every study reported a different numerical relationship between the OV and PE, with a mean enophthalmos of 0.80 mm after a 1-cm3 CONCLUSIONS: The present review found that most studies concluded that a direct relationship exists between the OV and PE and defined the degree of PE in relation to the OV expansion. (univ-lille.fr)
Degree1
- The prognosis of enophthalmos is directly related to both the underlying cause and the degree of deformity. (medscape.com)
Common1
- Enophthalmos is common. (medscape.com)
Condition1
- This condition is called enophthalmos. (merckmanuals.com)