Femur Head Necrosis
Femur Head
Head
Necrosis
Tumor Necrosis Factor-alpha
The prevalence and clinicopathological appearance of extension of osteonecrosis in the femoral head. (1/547)
In about 50% of cases, osteonecrosis of the femoral head is known to occupy more than one site. There is controversy as to whether a single focus may increase in size. We have reviewed 606 consecutive femoral heads which had been surgically removed for osteonecrosis. Extension of osteonecrosis was observed in only two (0.3%) and was confirmed histopathologically by the enlargement of the necrotic segment beyond the repair zone formed for the primary necrosis into the adjacent, previously uninvolved bone. In both cases, the necrotic regions were wedge-shaped and occupied over 80% of the femoral head. It appears that an increase in size is extremely rare and that osteonecrosis is due to a single event. Our findings may be of value in assessing the use of joint-salvage procedures for osteonecrosis of the femoral head. (+info)Decrease in the mesenchymal stem-cell pool in the proximal femur in corticosteroid-induced osteonecrosis. (2/547)
We have evaluated bone-marrow activity in the proximal femur of patients with corticosteroid-induced osteonecrosis and compared it with that of patients with osteonecrosis related to sickle-cell disease and with a control group without osteonecrosis. Bone marrow was obtained by puncture of the femoral head outside the area of necrosis and in the intertrochanteric region. The activity of stromal cells was assessed by culturing fibroblast colony-forming units (FCFUs). We found a decrease in the number of FCFUs outside the area of osteonecrosis in the upper end of the femur of patients with corticosteroid-induced osteonecrosis compared with the other groups. We suggest that glucocorticosteroids may also have an adverse effect on bone by decreasing the number of progenitors. The possible relevance of this finding to osteonecrosis is discussed. (+info)Slipped capital femoral epiphysis after septic arthritis of the hip in an adolescent: report of a case. (3/547)
Septic arthritis of the hip must be managed promptly to avoid the serious complications associated with the condition. In the case reported here, the diagnosis was delayed and was complicated by a slipped capital femoral epiphysis. The patient, an adolescent boy previously in good health, presented with a 2-week history of hip pain and systemic illness. Septic arthritis was diagnosed and was managed by incision and drainage and antibiotic therapy. Two weeks later he presented with a subcutaneous abscess and a slipped capital femoral epiphysis, which was pinned in situ. There was a 2.5-cm leg-length discrepancy. Avascular necrosis of the femoral head subsequently developed leaving the boy with a permanent disability. (+info)Cyclosporin A mono-therapy in nephrotic syndrome with contra-indication of steroid therapy. (4/547)
We describe three cases of nephrotic syndrome with a contra-indication for steroid therapy successfully treated with cyclosporin A (CsA). A 21-year-old man with focal segmental glomerulosclerosis (FSGS) complicated by necrosis of the femoral head, and a 34-year-old woman and a 48-year-old man with minimal change disease (MCD) complicated by psychogenic reaction and diabetes mellitus, respectively, were given CsA at initial dosages of 3.8-5.0 mg/kg/day and immediately remitted completely. However, two of these patients suffered relapses when CsA was tapered. They are currently maintained in complete or partial remission on CsA at dosages of 3.2-4.7 mg/kg/day. These findings suggest that CsA mono-therapy may be useful in nephrotic syndrome patients contra-indicated for steroid therapy. (+info)Increased level of apolipoprotein B/apolipoprotein A1 ratio as a potential risk for osteonecrosis. (5/547)
OBJECTIVE: This study was performed to investigate whether a high ratio of apolipoprotein B to apolipoprotein A1 (apo B/apo A1 ratio) is significantly associated with the risk of developing non-traumatic osteonecrosis of the femoral head (ON). METHODS: Fifty consecutive non-traumatic ON cases were compared with 50 age and sex matched controls, using both univariate and stepwise discriminant analyses, regarding the factors of corticosteroid, alcohol, cigarettes, cholesterol, triglyceride, and apo B/apo A1 ratio. To eliminate the possibility that ON or osteoarthritic change itself can increase the apo B/apo A1 ratio, a further 32 consecutive cases comprising nine traumatic ON and 23 osteoarthritis (OA) patients were analysed using Scheffe's test. RESULTS: There was a significant association between a high apo B/apo A1 ratio and the development of non-traumatic ON with both univariate (p=0.0001) and stepwise discriminant analyses (partial r(2)=0.1239, p=0.0004). The apo B/apo A1 ratio in the non-traumatic ON group was significantly higher than that in the traumatic ON (p<0.01), control (p<0.001), or the OA groups (p<0.001). CONCLUSION: A high apo B/apo A1 ratio is significantly associated with the risk of developing ON. This ratio may be useful for assessing the potential risk of developing osteonecrosis. (+info)Treatment of osteonecrosis of the femoral head by free vascularized fibular grafting: an analysis of surgical outcome and patient health status. (6/547)
OBJECTIVE: To evaluate the limb-specific outcome and general health status of patients with osteonecrosis of the femoral head treated with vascularized fibular grafting. DESIGN: A retrospective review. SETTING: A single tertiary care centre. PATIENTS: Fifty-five consecutive patients with osteonecrosis of the femoral head who underwent fibular grafting (8 bilaterally). INTERVENTION: Vascularized fibular grafting. OUTCOME MEASURES: Limb-specific scores (Harris Hip Score, St. Michael's Hospital Hip Score), general health status (Nottingham Health Profile, SF-36 health status survey) and radiographic outcome measures (Steinberg stage). RESULTS: Patients were young (mean age 34 years, range from 18 to 52 years) and 80% had advanced osteonecrosis (Steinberg stages IV and V). Fifty-nine hips were followed up for an average of 50 months (range from 24 to 117 months) after vascularized fibular grafting. Sixteen hips (27%) were converted to total hip arthroplasty (THA). To date, 73% of hips treated with vascularized fibular grafting have required no further surgery. Preoperative and postoperative Harris Hip Scores were 57.3 and 83.6 respectively (p < 0.001). As measured by patient-oriented health status questionnaires (SF-36, Nottingham Health Profile) and compared with population controls, patients had normal mental health scores and only slight decreases in physical component scores. CONCLUSIONS: Free vascularized fibular grafting for osteonecrosis of the femoral head provides satisfactory pain relief, functional improvement and general health status and halts the progression of symptomatic disease. (+info)Diagnostic criteria for non-traumatic osteonecrosis of the femoral head. A multicentre study. (7/547)
Six major and seven minor diagnostic criteria have been developed by the Japanese Investigation Committee for osteonecrosis of the femoral head (ONFH). We have carried out a multicentre study to clarify these. We studied prospectively 277 hips in 222 patients, from six hospitals, who had ONFH and other hip pathology and from whom histological material was available. We identified five criteria with high specificity: 1) collapse of the femoral head without narrowing of the joint space or acetabular abnormality on radiographs, including the crescent sign; 2) demarcating sclerosis in the femoral head without narrowing or acetabular abnormality; 3) a 'cold-in-hot' appearance on the bone scan; 4) a low-intensity band on T1-weighted images (band pattern); and 5) evidence of trabecular and marrow necrosis on histological examination. With any combination of two of these criteria, the sensitivity and specificity of the diagnosis were 91% and 99%, respectively. (+info)Femoral head necrosis treated with vascularized iliac crest graft. (8/547)
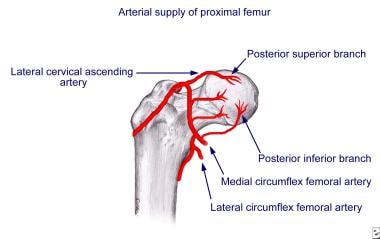
We reviewed 24 hips with avascular necrosis of the femoral head in 24 patients treated with vascularized iliac bone grafts 12 years after operation. In 7 patients the necrosis was classified as Ficat Stage II and in 17 patients as Stage III. Eight patients showed poor results. In 6 hips with fair results, moderate progression of the necrosis was noted at 3 to 8 years postoperatively. In 5 hips showing good results, slow progression with incipient signs of arthrosis were noted 8 years after surgery. In the remaining 5 patients with excellent results, no evidence of progression was noted 9 to 14 years postoperatively. The method described is recommended for treatment in the Ficat Stage II and early Stage III, when necrosis does not yet involve the complete femoral head. (+info)Femoral head necrosis, also known as avascular necrosis of the femoral head, is a medical condition that results from the interruption of blood flow to the femoral head, which is the rounded end of the thigh bone that fits into the hip joint. This lack of blood supply can cause the bone tissue to die, leading to the collapse of the femoral head and eventually resulting in hip joint damage or arthritis.
The condition can be caused by a variety of factors, including trauma, alcohol abuse, corticosteroid use, radiation therapy, and certain medical conditions such as sickle cell disease and lupus. Symptoms may include pain in the hip or groin, limited range of motion, and difficulty walking. Treatment options depend on the severity and progression of the necrosis and may include medication, physical therapy, or surgical intervention.
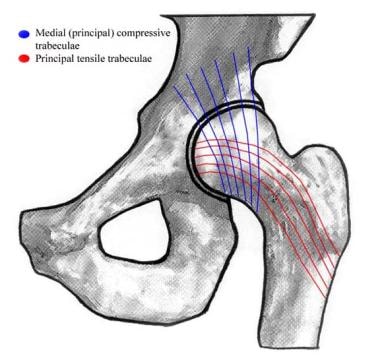
The femoral head is the rounded, ball-like top portion of the femur (thigh bone) that fits into the hip socket (acetabulum) to form the hip joint. It has a smooth, articular cartilage surface that allows for smooth and stable articulation with the pelvis. The femoral head is connected to the femoral neck, which is a narrower section of bone that angles downward and leads into the shaft of the femur. Together, the femoral head and neck provide stability and range of motion to the hip joint.
The femur is the medical term for the thigh bone, which is the longest and strongest bone in the human body. It connects the hip bone to the knee joint and plays a crucial role in supporting the weight of the body and allowing movement during activities such as walking, running, and jumping. The femur is composed of a rounded head, a long shaft, and two condyles at the lower end that articulate with the tibia and patella to form the knee joint.
In medical terms, the "head" is the uppermost part of the human body that contains the brain, skull, face, eyes, nose, mouth, and ears. It is connected to the rest of the body by the neck and is responsible for many vital functions such as sight, hearing, smell, taste, touch, and thought processing. The head also plays a crucial role in maintaining balance, speech, and eating.
Necrosis is the premature death of cells or tissues due to damage or injury, such as from infection, trauma, infarction (lack of blood supply), or toxic substances. It's a pathological process that results in the uncontrolled and passive degradation of cellular components, ultimately leading to the release of intracellular contents into the extracellular space. This can cause local inflammation and may lead to further tissue damage if not treated promptly.
There are different types of necrosis, including coagulative, liquefactive, caseous, fat, fibrinoid, and gangrenous necrosis, each with distinct histological features depending on the underlying cause and the affected tissues or organs.
Tumor Necrosis Factor-alpha (TNF-α) is a cytokine, a type of small signaling protein involved in immune response and inflammation. It is primarily produced by activated macrophages, although other cell types such as T-cells, natural killer cells, and mast cells can also produce it.
TNF-α plays a crucial role in the body's defense against infection and tissue injury by mediating inflammatory responses, activating immune cells, and inducing apoptosis (programmed cell death) in certain types of cells. It does this by binding to its receptors, TNFR1 and TNFR2, which are found on the surface of many cell types.
In addition to its role in the immune response, TNF-α has been implicated in the pathogenesis of several diseases, including autoimmune disorders such as rheumatoid arthritis, inflammatory bowel disease, and psoriasis, as well as cancer, where it can promote tumor growth and metastasis.
Therapeutic agents that target TNF-α, such as infliximab, adalimumab, and etanercept, have been developed to treat these conditions. However, these drugs can also increase the risk of infections and other side effects, so their use must be carefully monitored.
 Quadratus femoris muscle
Quadratus femoris muscle Intralesional autologous mesenchymal stem cells in management of osteonecrosis of femur: a preliminary study
Intralesional autologous mesenchymal stem cells in management of osteonecrosis of femur: a preliminary study Knee Osteonecrosis: Practice Essentials, History of the Procedure, Problem
Knee Osteonecrosis: Practice Essentials, History of the Procedure, Problem Hip Fractures - OrthoInfo - AAOS
Hip Fractures - OrthoInfo - AAOS Bone Regeneration Therapy of Atraumatic Necrosis of Femoral Head
Bone Regeneration Therapy of Atraumatic Necrosis of Femoral Head Diagnosis of Acute or Subacute Avascular Necrosis | CADTH
Diagnosis of Acute or Subacute Avascular Necrosis | CADTH Orthopedic Doctors in Las Vegas | MountainView Hospital
Orthopedic Doctors in Las Vegas | MountainView Hospital The Effect of Repeated Electromagnetic Fields Stimulation in Biological Systems | IntechOpen
The Effect of Repeated Electromagnetic Fields Stimulation in Biological Systems | IntechOpen Long-term outcome in polymyositis and dermatomyositis | Annals of the Rheumatic Diseases
Long-term outcome in polymyositis and dermatomyositis | Annals of the Rheumatic Diseases Avascular Necrosis Case Report of Direct Bone Marrow Injections and Prolotherapy Treatment - Caring Medical Florida
Avascular Necrosis Case Report of Direct Bone Marrow Injections and Prolotherapy Treatment - Caring Medical Florida The role of imaging in diagnosis and management of femoral head avascular necrosis
The role of imaging in diagnosis and management of femoral head avascular necrosis COL2A1 gene: MedlinePlus Genetics
COL2A1 gene: MedlinePlus Genetics Barton Branam, MD | UC Health Provider Profile
Barton Branam, MD | UC Health Provider Profile Orthoseek | Orthopedic Topics | (Legg-Calve) Perthes' Disease
Orthoseek | Orthopedic Topics | (Legg-Calve) Perthes' Disease A V N f e m o r a l h e a d - JOURNAL OF ORTHOPAEDICS AND REHABILITATION
A V N f e m o r a l h e a d - JOURNAL OF ORTHOPAEDICS AND REHABILITATION Current diagnostic and therapeutic approach to patients with slipped capital femoral epiphysis - TOTBİD Dergisi
Current diagnostic and therapeutic approach to patients with slipped capital femoral epiphysis - TOTBİD Dergisi Division of Pediatrics - Research output
- Research Profiles at Washington University School of Medicine
Division of Pediatrics - Research output
- Research Profiles at Washington University School of Medicine Adolescent Lateral Entry Femoral Nail
Adolescent Lateral Entry Femoral Nail Charles Sturt University - Research Outputs
- Charles Sturt University Research Output
Charles Sturt University - Research Outputs
- Charles Sturt University Research Output Ayurvedic treatment for back pain and neck pain |UAE
Ayurvedic treatment for back pain and neck pain |UAE