Fibrocystic Breast Disease
Breast
Adenofibroma
Fibroadenoma
Natural history of fibroadenomas based on the correlation between size and patient age. (1/234)
BACKGROUND: Several recent studies have reported that most fibroadenomas remain static or regress when they are managed conservatively; however, no such studies have evaluated the breast disorder in Japanese women. To understand the natural history of fibroadenomas in Japanese women, we examined the correlation between the sizes of the fibroadenomas and the women's age. METHODS: Fifty-eight consecutive patients (age range, 17-51 years; mean, 33.9 years) with histologically confirmed fibroadenoma were enrolled in this study. The sizes of the excised fibroadenomas were analyzed in relation to the women's ages. RESULTS: The fibroadenomas decreased significantly in size (Y, mm) with patient age (X, years) (P = 0.0012) according the equation Y = -0.340X + 27.0 (95% confidence limits for the slope, -0.139 to -0.540). From this equation, the mean sizes of the fibroadenoma in women aged 20, 30 and 40 years were expected to be 20.2 mm (95% confidence interval, 16.2-24.2 mm), 16.8 mm (95% confidence interval, 10.8-22.8 mm) and 13.4 mm (95% confidence interval, 5.4-21.4 mm), respectively. The mean annual decrease in the size of the fibroadenomas was 0.340 mm. CONCLUSIONS: Our results indicate that in Japanese women fibroadenomas increase in size more frequently in younger than in older women. Moreover, it is speculated that most fibroadenomas might stop growing when they reach an approximate maximum diameter of 20 mm, after which time they might remain static or regress. (+info)Measurement of prostate-specific antigen in detection of benign or malignant breast disease in women. (2/234)
Using a highly sensitive chemiluminescent enzyme immunoassay, we have evaluated the measurement of serum prostate-specific antigen (PSA) as a potential diagnostic test for differentiation between women with breast cancer and those with benign breast disease. In a controlled study consisting of 284 women with well-documented patient files and matched for age and long-term place of residence, serum samples collected from 90 women with histologically confirmed breast cancer, 94 women with benign breast disease and 100 controls were analysed. Serum total PSA levels in benign breast disease and cancer patients are not statistically different from those of healthy controls. Total PSA levels decrease with age in normal controls and breast cancer patients but not in those with benign breast disease. The total PSA concentration decreases after menopause in healthy women, though not in patients with breast cancer or benign breast disease. Total PSA bore no relation to the histological type or grade of the tumour or the disease stage of the breast cancer patients. In benign breast disease, all mastopathy patients had normal total PSA, whereas elevation of the values was observed in 7% of fibroadenoma patients. Our results show that serum total PSA cannot be used to distinguish between healthy women and/or women with breast cancer or benign breast disease. (+info)Vascular stroma formation in carcinoma in situ, invasive carcinoma, and metastatic carcinoma of the breast. (3/234)
The generation of vascular stroma is essential for solid tumor growth and involves stimulatory and inhibiting factors as well as stromal components that regulate functions such as cellular adhesion, migration, and gene expression. In an effort to obtain a more integrated understanding of vascular stroma formation in breast carcinoma, we examined expression of the angiogenic factor vascular permeability factor (VPF)/vascular endothelial growth factor (VEGF); the VPF/VEGF receptors flt-1 and KDR; thrombospondin-1, which has been reported to inhibit angiogenesis; and the stromal components collagen type I, total fibronectin, ED-A+ fibronectin, versican, and decorin by mRNA in situ hybridization on frozen sections of 113 blocks of breast tissue from 68 patients including 28 sections of breast tissue without malignancy, 18 with in situ carcinomas, 56 with invasive carcinomas, and 8 with metastatic carcinomas. A characteristic expression profile emerged that was remarkably similar in invasive carcinoma, carcinoma in situ, and metastatic carcinoma, with the following characteristics: strong tumor cell expression of VPF/VEGF; strong endothelial cell expression of VPF/VEGF receptors; strong expression of thrombospondin-1 by stromal cells and occasionally by tumor cells; and strong stromal cell expression of collagen type I, total fibronectin, ED-A+ fibronectin, versican, and decorin. The formation of vascular stroma preceded invasion, raising the possibility that tumor cells invade not into normal breast stroma but rather into a richly vascular stroma that they have induced. Similarly, tumor cells at sites of metastasis appear to induce the vascular stroma in which they grow. We conclude that a distinct pattern of mRNA expression characterizes the generation of vascular stroma in breast cancer and that the formation of vascular stroma may play a role not only in growth of the primary tumor but also in invasion and metastasis. (+info)Enhanced apoptotic response to photodynamic therapy after bcl-2 transfection. (4/234)
Apoptosis is a cellular death process involving the sequential activation of a series of caspases, endonucleases, and other enzymes. The initiation of apoptosis can be inhibited by overexpression of bcl-2 and certain other members of a related family of proteins. We examined the effects of bcl-2 overexpression on the apoptotic response to photodynamic therapy (PDT), using aluminum phthalocyanine as the photosensitizing agent. In this study, we compared the immortalized human breast epithelial cell line MCF10A with a subline (MCF10A/bcl-2) transfected with the human bcl-2 gene. The latter was approximately 2-fold more sensitive to the phototoxic effects of PDT. At a 50 mJ/cm2 light dose, photodamage to MCF-10A/bcl-2 resulted in a greater loss of the mitochondrial membrane potential (delta(psi)m), enhanced release of mitochondrial cytochrome c, a more rapid and greater activation of caspase-3, and a greater apoptotic response. Western blot analysis revealed that the transfected cell line showed overexpression of both bcl-2 and bax, and that PDT caused selective destruction of bcl-2, leaving bax unaffected. The greater apoptotic response by the transfected line is, therefore, attributed to the higher bax:bcl-2 ratio after photodamage. (+info)Human mammary gland and breast carcinoma contain immunoreactive inhibin/activin subunits: evidence for a secretion into cystic fluid. (5/234)
OBJECTIVE: Inhibins and activins are members of the transforming growth factor beta superfamily and are known to modulate the growth and differentiation of several cell types. The present study investigated the localization of inhibin and activin subunits in human normal and pathological breast tissues. DESIGN: A cross-sectional study comparing the expression of inhibin/activin subunits alpha, betaA and betaB in surgical specimens from women undergoing reductive mammoplasty (classified, according to the phase of the menstrual cycle, as follicular, luteal, or postmenopausal), and patients submitted to lumpectomy for fibrocystic disease, benign (intraductal papilloma, adenomyoepithelioma, and hamartoma) or malignant breast neoplams (intraductal, intralobular, and invasive carcinoma). METHODS: Immunohistochemistry was used to localize inhibin alpha and activin betaA and betaB subunits in the cytoplasm of epithelial cells of mammary glands. Dimeric activin A, inhibin A and inhibin B were measured by specific two-site enzyme immunoassay in the cystic fluid collected from patients with fibrocystic disease. RESULTS: An intense staining for the alpha inhibin subunit and a mild staining for betaA and betaB subunits were present in samples obtained from normal breast tissue regardless of menstrual cycle phase, and in fibrocystic disease and benign neoplasms. Carcinoma cells stained weakly to moderately for alpha subunit and were negative for betaA and betaB subunits. Fibrocystic disease was associated with absence of betaA subunit expression in normal epithelial cells and intense staining for all subunits in the apocrine cells. Immunoreactive inhibin A, inhibin B, and activin A were also present in cystic fluid, suggesting a local secretion of these proteins. CONCLUSION: These data suggest a local expression and secretion of inhibin and activin in human normal, fibrocystic disease and neoplastic breast tissues. The low expression of these proteins may facilitate abnormal cell proliferation in breast carcinoma. (+info)Teaching family practice residents breast cyst aspiration. (6/234)
OBJECTIVE: To conduct the first study of teaching family practice residents the technique of breast cyst aspiration (BCA) using the Toronto Breast Cyst Aspiration Model (TBCAM) in a workshop. To determine whether this training increases their likelihood of performing the procedure in the future. To discover how residents evaluate the workshop as a teaching method. DESIGN: Prospective parallel-group trial from August to November 1997. Baseline questionnaires were given to both experimental and control groups in August. The experimental group was given a 1.5-hour workshop and a postworkshop questionnaire. Both groups were then given 3-month follow-up questionnaires. SETTING: Family practice residency program at the University of Toronto. PARTICIPANTS: The experimental group consisted of 15 family practice residents from one university-affiliated hospital site. The control group consisted of 54 family practice residents selected from the remaining sites. MAIN OUTCOME MEASURES: Confidence score, likelihood of performing BCA, and effectiveness of the workshop rated on a Likert scale ranging from 1-low to 5-high; and knowledge of BCA rated from 0 to 7. RESULTS: Three months after the workshop, 62% of study subjects and 31% of controls were above the median confidence score of 3.2 (chi 2 3.4, P > .05); 76% of subjects but only 11% of controls were above the median knowledge score of 4 (chi 2 16.67, P < .001); and 75% of subjects and 34% of controls were above the median likelihood to perform score of 3 (chi 2 5.37, P < .05). Most (95%) workshop effectiveness scores were 4s or 5s. CONCLUSIONS: Workshop training resulted in higher confidence, greater knowledge, and more likelihood of performing BCA. The workshop using the TBCAM was evaluated as a highly effective way to teach BCA. (+info)Management of palpable breast lumps. Consensus guideline for family physicians. (7/234)
OBJECTIVE: To describe an approach to managing women who present with palpable breast lumps. QUALITY OF EVIDENCE: Databases were searched from 1990 to 1998 using the search terms breast lumps, breast diseases, and breast cysts. Bibliographies of the articles obtained were searched for further relevant titles. Most evidence on management of breast cysts was obtained from cohort studies. Evidence on family physicians' approach to managing breast lumps is based on a review of the 1998 Canadian consensus guidelines and a review of a 1998 consensus guideline by 12 University of Toronto surgical oncologists (U of T guidelines). MAIN MESSAGE: Family physicians can manage women presenting with breast lumps if they have skill in breast cyst aspiration. Most breast cysts can be cured in minutes, thus avoiding unwarranted anxiety and eliminating unnecessary additional investigations and referrals. Women presenting with solid lesions should be referred to a surgeon. CONCLUSIONS: Breast cyst aspiration is a simple technique family physicians can use to either cure breast lumps or define appropriate cases for referral. (+info)Human glandular kallikrein in breast milk, amniotic fluid, and breast cyst fluid. (8/234)
BACKGROUND: Human glandular kallikrein (hK2) belongs to the serine protease family of enzymes and has high sequence homology with prostate-specific antigen (PSA). The physiological role of hK2 has not as yet been determined, but there is evidence that it can regulate the proteolytic activity of PSA through processing and activating pro-PSA, an inactive precursor. Thus, it is conceivable that these two secreted proteins may coexist in biological fluids. Currently, hK2 is considered an androgen-regulated and prostate-specific protein. Recently, it has been demonstrated that hK2 is expressed in the breast cancer cell line T-47D after stimulation by steroid hormones, and we reported that hK2 can be detected in a subset of breast tumor extracts. These data suggest that hK2 may be expressed in tissues other than the prostate, such as those in which PSA has already been detected. Because hK2 is a secreted protein, it may be present in various biological fluids. METHODS: We analyzed milk samples from lactating women, amniotic fluid from pregnant women, and breast cyst fluid from patients with gross breast cystic disease, using a highly sensitive and specific immunoassay for hK2. RESULTS: hK2 was present in all three biological fluids. We suggest that the female breast may produce hK2 and provide evidence that hK2 may have value as an additional marker for the discrimination between type I and type II breast cysts. CONCLUSIONS: The female breast produces hK2 in addition to PSA. More studies are necessary to establish the role of this kallikrein in nondiseased breast, gross breast cystic disease, and breast cancer. (+info)Fibrocystic breast disease, also known as fibrocystic change or chronic cystic mastitis, is not actually a disease but a condition that affects many women at some point in their lives. It is characterized by the formation of benign (non-cancerous) lumps or cysts in the breasts, often accompanied by breast pain, tenderness, and swelling.
The condition is caused by hormonal fluctuations that affect the breast tissue, making it more prone to developing fibrous tissue and fluid-filled sacs called cysts. Fibrocystic breast changes are usually harmless and do not increase the risk of breast cancer. However, in some cases, they can make it harder to detect early signs of breast cancer through mammography or self-examination.
The symptoms of fibrocystic breast change may vary from woman to woman and can range from mild to severe. They tend to be more noticeable just before a woman's menstrual period and may improve after menopause. Treatment options for fibrocystic breast changes include pain relievers, hormonal medications, and lifestyle modifications such as reducing caffeine intake and wearing a well-supportive bra. In some cases, draining or removing the cysts may be necessary to alleviate symptoms.
Breast diseases refer to a wide range of conditions that affect the breast tissue. These can be broadly categorized into non-cancerous and cancerous conditions.
Non-cancerous breast diseases include:
1. Fibrocystic breast changes: This is a common condition where the breast tissue becomes lumpy, tender, and sometimes painful. It is caused by hormonal changes and is most common in women aged 20 to 50.
2. Mastitis: This is an infection of the breast tissue, usually occurring in breastfeeding women. Symptoms include redness, swelling, warmth, and pain in the affected area.
3. Breast abscess: This is a collection of pus in the breast tissue, often caused by bacterial infection. It can be painful and may require surgical drainage.
4. Fibroadenomas: These are benign tumors made up of glandular and fibrous tissue. They are usually round, firm, and mobile, and can be removed if they cause discomfort.
5. Intraductal papillomas: These are small, wart-like growths that occur in the milk ducts. They may cause nipple discharge, which can be bloody or clear.
Cancerous breast diseases include:
1. Breast cancer: This is a malignant tumor that starts in the breast tissue. It can spread to other parts of the body if left untreated. There are several types of breast cancer, including ductal carcinoma, lobular carcinoma, and inflammatory breast cancer.
2. Paget's disease of the nipple: This is a rare form of breast cancer that affects the skin of the nipple and areola. It can cause symptoms such as redness, itching, burning, and flaking of the nipple skin.
3. Phyllodes tumors: These are rare breast tumors that can be benign or malignant. They usually grow quickly and may require surgical removal.
It is important to note that not all breast lumps are cancerous, and many non-cancerous conditions can cause breast changes. However, any new or unusual breast symptoms should be evaluated by a healthcare professional to rule out serious conditions such as breast cancer.
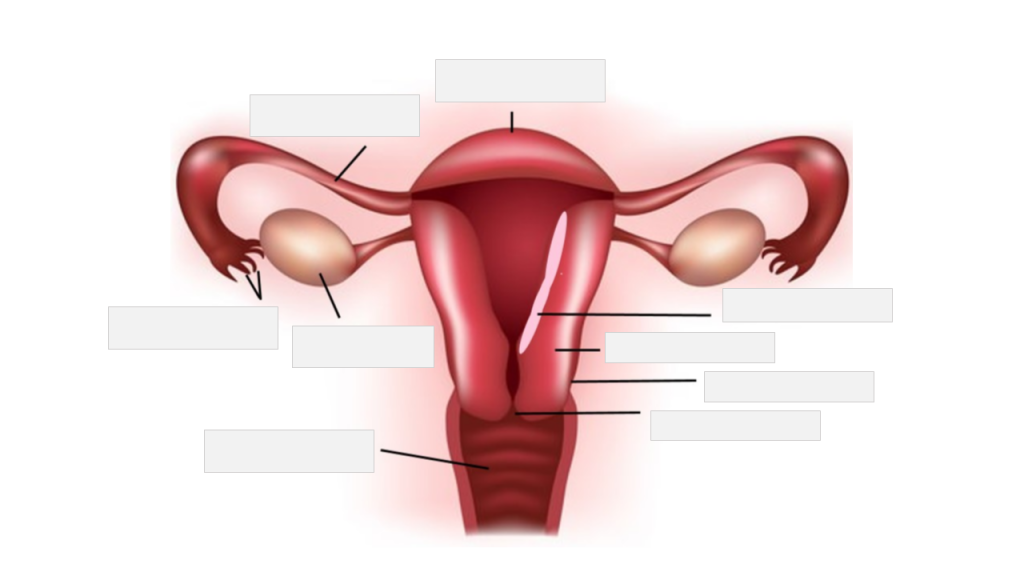
The breast is the upper ventral region of the human body in females, which contains the mammary gland. The main function of the breast is to provide nutrition to infants through the production and secretion of milk, a process known as lactation. The breast is composed of fibrous connective tissue, adipose (fatty) tissue, and the mammary gland, which is made up of 15-20 lobes that are arranged in a radial pattern. Each lobe contains many smaller lobules, where milk is produced during lactation. The milk is then transported through a network of ducts to the nipple, where it can be expressed by the infant.
In addition to its role in lactation, the breast also has important endocrine and psychological functions. It contains receptors for hormones such as estrogen and progesterone, which play a key role in sexual development and reproduction. The breast is also a source of sexual pleasure and can be an important symbol of femininity and motherhood.
It's worth noting that males also have breast tissue, although it is usually less developed than in females. Male breast tissue consists mainly of adipose tissue and does not typically contain functional mammary glands. However, some men may develop enlarged breast tissue due to conditions such as gynecomastia, which can be caused by hormonal imbalances or certain medications.
Adenofibroma is a rare, benign tumor that occurs most commonly in the salivary glands. It is composed of both glandular tissue (adeno-) and fibrous tissue (-fibroma). These tumors are slow-growing and typically do not spread to other parts of the body.
Adenofibromas can also occur in other areas of the body, such as the skin, where they may be referred to as "fibroepithelial polyps" or "skin tags." In general, adenofibromas are not cancerous and can often be removed surgically. However, it is important to have any new growths or lumps evaluated by a healthcare professional to determine the appropriate course of treatment.
A fibroadenoma is a benign (noncancerous) breast tumor that is most commonly found in women between the ages of 15 and 35, although it can occur at any age. It is composed of glandular and connective tissue. The tumor typically feels firm, smooth, and rubbery, and its size may vary from quite small to over 2 inches in diameter.
Fibroadenomas are usually mobile within the breast tissue, which means they can be moved around easily when touched. They can occur as a single lump or multiple lumps (known as fibroadenomatosis). The exact cause of fibroadenomas is not known, but hormonal factors may play a role in their development.
Fibroadenomas are generally not painful, although some women may experience discomfort or tenderness, especially before their menstrual period. In most cases, fibroadenomas do not require treatment and can be monitored with regular breast exams and imaging studies such as mammography or ultrasound. However, if a fibroadenoma grows larger or becomes uncomfortable, it may be removed through a surgical procedure.
Breast neoplasms refer to abnormal growths in the breast tissue that can be benign or malignant. Benign breast neoplasms are non-cancerous tumors or growths, while malignant breast neoplasms are cancerous tumors that can invade surrounding tissues and spread to other parts of the body.
Breast neoplasms can arise from different types of cells in the breast, including milk ducts, milk sacs (lobules), or connective tissue. The most common type of breast cancer is ductal carcinoma, which starts in the milk ducts and can spread to other parts of the breast and nearby structures.
Breast neoplasms are usually detected through screening methods such as mammography, ultrasound, or MRI, or through self-examination or clinical examination. Treatment options for breast neoplasms depend on several factors, including the type and stage of the tumor, the patient's age and overall health, and personal preferences. Treatment may include surgery, radiation therapy, chemotherapy, hormone therapy, or targeted therapy.
A breast cyst is a fluid-filled sac that forms within the breast tissue. It is a common, benign (non-cancerous) condition and can affect people of any age, but it is more commonly found in women between the ages of 35 and 50. Breast cysts can vary in size and may be asymptomatic or cause discomfort or pain, especially just before menstruation.
Breast cysts are usually diagnosed through a physical examination, breast ultrasound, or mammography. In some cases, a fine-needle aspiration (FNA) may be performed to drain the fluid from the cyst and confirm the diagnosis. If the cyst is small, causes no symptoms, and appears benign on imaging studies, then further treatment may not be necessary. However, if the cyst is large, painful, or has concerning features on imaging studies, then additional diagnostic tests or drainage procedures may be recommended.
It's important to note that while breast cysts are generally harmless, they can sometimes mimic the symptoms of breast cancer. Therefore, any new or unusual changes in the breast should be evaluated by a healthcare professional.
 Fibrocystic breast changes
Fibrocystic breast changes 5 Natural Ways to Fight Fibrocystic Breast Disease | HubPages
5 Natural Ways to Fight Fibrocystic Breast Disease | HubPages Fibrocystic Breast Disease | Novant Health
Fibrocystic Breast Disease | Novant Health fibrocystic breast disease Archives - Stop The Thyroid Madness
fibrocystic breast disease Archives - Stop The Thyroid Madness Iodine replacement in fibrocystic disease of the breast - PubMed
Iodine replacement in fibrocystic disease of the breast - PubMed Fibrocystic breasts: MedlinePlus Medical Encyclopedia
Fibrocystic breasts: MedlinePlus Medical Encyclopedia Fibrocystic breast changes - Mayo Clinic
Fibrocystic breast changes - Mayo Clinic Fibrocystic Breast Condition | Diseases and Disorders
Fibrocystic Breast Condition | Diseases and Disorders fibrocystic breast disease Archives - Fertility Friday
fibrocystic breast disease Archives - Fertility Friday Fibrocystic Breast Disease in Indore - Dr Hema Jajoo
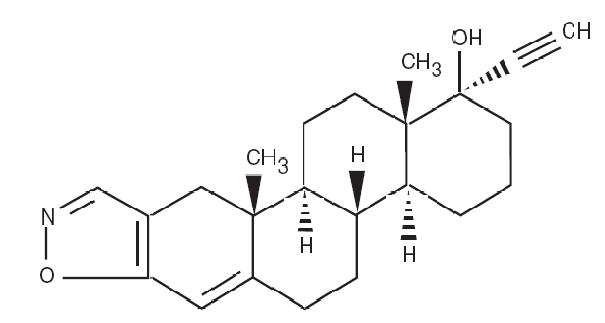
Fibrocystic Breast Disease in Indore - Dr Hema Jajoo DANOCRINE®
Brand of DANAZOL CAPSULES, USP
DANOCRINE®
Brand of DANAZOL CAPSULES, USP Fibrocystic Breast Disease | Surgical treatment . Hospital Prices, Ranking, Reviews - Bookinghealth
Fibrocystic Breast Disease | Surgical treatment . Hospital Prices, Ranking, Reviews - Bookinghealth Iodine - Health Professional Fact Sheet
Iodine - Health Professional Fact Sheet danazol) dosing, indications, interactions, adverse effects, and more
danazol) dosing, indications, interactions, adverse effects, and more ATSDR - Camp Lejeune, North Carolina - Transcript Camp Lejeune Expert Panel, Day Two
ATSDR - Camp Lejeune, North Carolina - Transcript Camp Lejeune Expert Panel, Day Two Low/Decreased Fat Diet - Information; Why it is Recommended
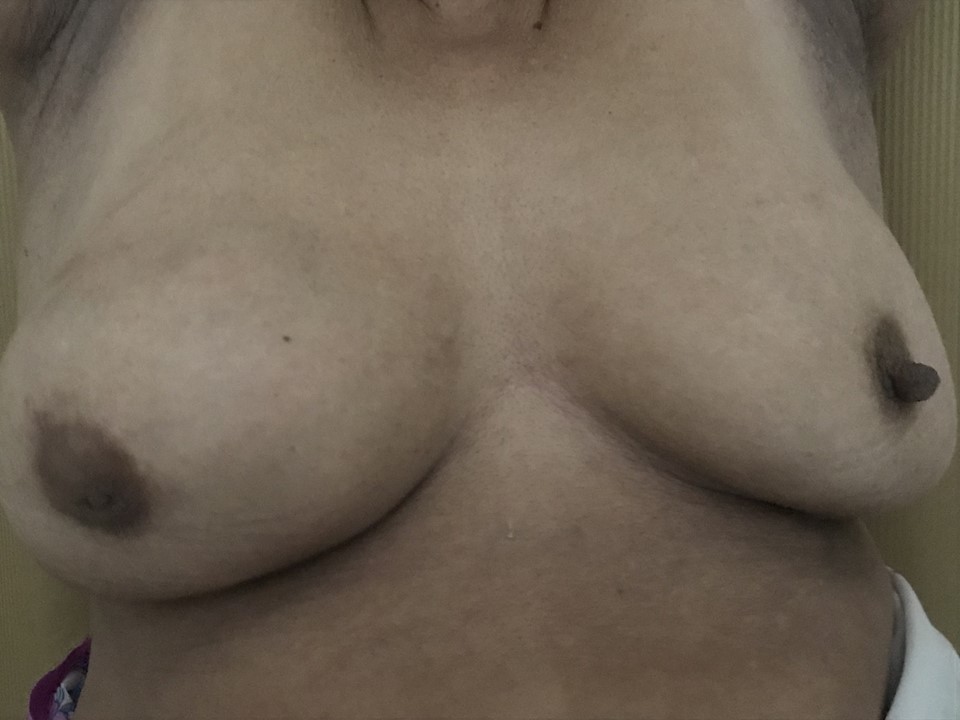
Low/Decreased Fat Diet - Information; Why it is Recommended Breast Disfigurement
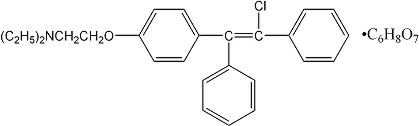
Breast Disfigurement Ethinyl estradiol and desogestrel Uses, Side Effects & Warnings
Ethinyl estradiol and desogestrel Uses, Side Effects & Warnings Guarana: Health Benefits, Side Effects, Uses, Dose & Precautions
Guarana: Health Benefits, Side Effects, Uses, Dose & Precautions Selection of 1,647 RR Messages from the forum Iodine Supplementation Support by VWT Team , Sorted by Stars
Selection of 1,647 RR Messages from the forum Iodine Supplementation Support by VWT Team , Sorted by Stars