Gastric Outlet Obstruction
Urinary Bladder Neck Obstruction
Duodenal Obstruction
Gastroenterostomy
Pyloric Stenosis, Hypertrophic
Pyloric Stenosis
Pylorus
Duodenal Diseases
Jejunostomy
Biliary Fistula
Pyloric Antrum
Endoscopy, Gastrointestinal
Gastric Bypass
Intestinal Obstruction
Gastrectomy
Urinary Bladder
Stents
Laparoscopy
Primary hypertrophic tuberculosis of the pyloroduodenal area: report of 2 cases. (1/103)
Tuberculosis of the stomach and duodenum is rare in patients with pulmonary tuberculosis. Primary involvement is even rarer. Two cases of primary tuberculosis of the localised to the pyloro-duodenal area are presented. The most common symptoms are non-specific leading to a difficulty in establishing a pre-operative diagnosis. A high degree of suspicion is therefore required for its diagnosis and to differentiate it from more frequent causes of gastric outlet obstruction such as chronic peptic ulcer disease and gastric carcinoma. The treatment of gastric tuberculosis is primarily medical with anti-tuberculous drug therapy. The role of surgery lies in the cases with obstruction following hypertrophic tuberculosis. The surgery done is usually a gastroenterostomy. With the relative rate of extra-pulmonary tuberculosis increasing, tuberculosis of the pyloro-duodenal area should be considered in the differential diagnosis of gastric outlet obstruction. (+info)Duplication cyst of the pylorus--a rare cause of gastric outlet obstruction in the newborn. (2/103)
Duplication cysts of the pylorus are the rarest of alimentary tract duplications with very few reported cases. We present such a cyst in a neonate presenting with gastric outlet obstruction. We have also reviewed the literature and outlined the theories of origin, modes of presentation, diagnosis and the surgical procedures. Even though several modes of surgery have been described, it is best to individualize the surgical option in each case. The results depend on the nature and site of duplication, complications and the associated anomalies. (+info)Potential uses of intravenous proton pump inhibitors to control gastric acid secretion. (3/103)
Proton pump inhibitors are the most effective agents for suppressing gastric acidity and are the preferred therapy for many acid-related conditions. While proton pump inhibitors have been accessible in intravenous formulations in several European countries, they have been available only as oral drugs in the United States. In the near future, the proton pump inhibitor pantoprazole is likely to become available in an intravenous formulation for American patients. Potential uses for intravenous proton pump inhibitors include treatment of Zollinger-Ellison syndrome and peptic ulcers complicated by bleeding or gastric outlet obstruction, as well as prevention of stress ulcers and acid-induced lung injury. These intravenous proton pump inhibitors are also likely to be beneficial to patients undergoing long-term maintenance with oral proton pump inhibitors who cannot take oral therapy for a period of time. Intravenous pantoprazole is especially distinguished in its lack of clinically relevant drug interactions, and it requires no dosage adjustment for patients with renal insufficiency or with mild to moderate hepatic dysfunction. Both omeprazole and pantoprazole are well tolerated in both oral and intravenous forms. Although further studies are needed to define their roles clearly, the availability of intravenous formulations of proton pump inhibitors will certainly assist with the treatment of gastric acid-related disorders. (+info)Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR Study Group. (4/103)
BACKGROUND: Each year, clinical upper gastrointestinal events occur in 2 to 4 percent of patients who are taking nonselective nonsteroidal antiinflammatory drugs (NSAIDs). We assessed whether rofecoxib, a selective inhibitor of cyclooxygenase-2, would be associated with a lower incidence of clinically important upper gastrointestinal events than is the nonselective NSAID naproxen among patients with rheumatoid arthritis. METHODS: We randomly assigned 8076 patients who were at least 50 years of age (or at least 40 years of age and receiving long-term glucocorticoid therapy) and who had rheumatoid arthritis to receive either 50 mg of rofecoxib daily or 500 mg of naproxen twice daily. The primary end point was confirmed clinical upper gastrointestinal events (gastroduodenal perforation or obstruction, upper gastrointestinal bleeding, and symptomatic gastroduodenal ulcers). RESULTS: Rofecoxib and naproxen had similar efficacy against rheumatoid arthritis. During a median follow-up of 9.0 months, 2.1 confirmed gastrointestinal events per 100 patient-years occurred with rofecoxib, as compared with 4.5 per 100 patient-years with naproxen (relative risk, 0.5; 95 percent confidence interval, 0.3 to 0.6; P<0.001). The respective rates of complicated confirmed events (perforation, obstruction, and severe upper gastrointestinal bleeding) were 0.6 per 100 patient-years and 1.4 per 100 patient-years (relative risk, 0.4; 95 percent confidence interval, 0.2 to 0.8; P=0.005). The incidence of myocardial infarction was lower among patients in the naproxen group than among those in the rofecoxib group (0.1 percent vs. 0.4 percent; relative risk, 0.2; 95 percent confidence interval, 0.1 to 0.7); the overall mortality rate and the rate of death from cardiovascular causes were similar in the two groups. CONCLUSIONS: In patients with rheumatoid arthritis, treatment with rofecoxib, a selective inhibitor of cyclooxygenase-2, is associated with significantly fewer clinically important upper gastrointestinal events than treatment with naproxen, a nonselective inhibitor. (+info)Bouveret's syndrome complicated by distal gallstone ileus after laser lithotropsy using Holmium: YAG laser. (5/103)
BACKGROUND: Bouveret's syndrome is an unusual presentation of duodenal obstruction caused by the passage of a large gallstone through a cholecystoduodenal fistula. Endoscopic therapy has been used as first-line treatment, especially in patients with high surgical risk. CASE PRESENTATION: We report a 67-year-old woman who underwent an endoscopic attempt to fragment and retrieve a duodenal stone using a Holmium: Yttrium-Aluminum-Garnet Laser (Ho:YAG) which resulted in small bowel obstruction. The patient successfully underwent enterolithotomy without cholecystectomy or closure of the fistula. CONCLUSION: We conclude that, distal gallstone obstruction, due to migration of partially fragmented stones, can occur as a possible complication of laser lithotripsy treatment of Bouveret's syndrome and might require urgent enterolithotomy. (+info)Duodenal stents for malignant duodenal strictures. (6/103)
Duodenal obstruction may be caused by inoperable malignant disease. Symptoms of nausea and vomiting have been traditionally palliated by surgery. The aim of the study was to determine the efficacy of the endoscopic placement of metal self expanding duodenal stents for the palliation of malignant duodenal obstruction. Four patients with malignant gastric outlet obstruction are described. One patient had a history of oesophagectomy for oesophageal adenocarcinoma and presented with further dysphagia. At endoscopy the recurrent oesophageal tumour and an adenocarcinoma involving the pylorus were both stented. In the other three patients there was a previous history of colonic carcinoma, cholangiocarcinoma and oesophageal adenocarcinoma respectively. All four patients were successfully stented with good palliation of their symptoms. Duodenal Wallstents are a useful alternative to surgery in patients with inoperable malignant duodenal obstruction or those who are unfit for surgery. (+info)Review article: Helicobacter pylori infection and gastric outlet obstruction - prevalence of the infection and role of antimicrobial treatment. (7/103)
The prevalence of Helicobacter pylori infection in peptic ulcer disease complicated by gastric outlet obstruction seems to be, overall, lower than that reported in non-complicated ulcer disease, with a mean value of 69%. However, H. pylori infection rates in various studies range from 33% to 91%, suggesting that differences in variables, such as the number and type of diagnostic methods used or the frequency of non-steroidal anti-inflammatory drug intake, may be responsible for the low prevalence reported in some studies. The resolution of gastric outlet obstruction after the eradication of H. pylori has been demonstrated by several studies. It seems that the beneficial effect of H. pylori eradication on gastric outlet obstruction is observed early, just a few weeks after the administration of antimicrobial treatment. Furthermore, this favourable effect seems to remain during long-term follow-up. Nevertheless, gastric outlet obstruction does not always resolve after H. pylori eradication treatment and an explanation for the failures is not completely clear, non-steroidal anti-inflammatory drug intake perhaps playing a major role in these cases. Treatment should start pharmacologically with the eradication of H. pylori even when stenosis is considered to be fibrotic, or when there is some gastric stasis. In summary, H. pylori eradication therapy should be considered as the first step in the treatment of duodenal or pyloric H. pylori-positive stenosis, whereas dilation or surgery should be reserved for patients who do not respond to such medical therapy. (+info)Ectopic pancreas with gastric outlet obstruction: report of two cases and literature review. (8/103)
Ectopic pancreas is a rare entity and is usually an incidental finding in clinical practice. Most patients with an ectopic pancreas are asymptomatic, and if present, symptoms are non-specific according to the site of the lesion and different complications encountered. The most-common site is the stomach, accounting for 25%-38.2% of all patients. An asymptomatic ectopic pancreas is usually of no clinical importance, and there is no surgical indication in such a situation. However if there are complications caused by an ectopic pancreas, a variety of actions becomes necessary. We report 2 cases of ectopic pancreas with gastric outlet obstruction. The first case was a 41-year-old man who suffered from epigastric fullness and dyspepsia for 3 years. Endoscopic examination revealed a submucosal tumor measuring 2.5 cm in diameter in the prepyloric area. The second case was a 53-year-old man, who initially underwent a craniotomy to remove a pituitary adenoma, and laparotomy and duodenorrhaphy due to a perforated peptic ulcer. The postoperative course was not uneventful, and an upper gastrointestinal series showed a 2-cm intramural mass with a mucosal ulcer at the distal antrum. Both cases had symptoms and signs of gastric outlet obstruction, and both cases accepted subtotal gastrectomy with Billroth II anastomosis. A review of the literature revealed few cases of ectopic pancreas with gastric outlet obstruction. An ectopic pancreas must be considered in the differential diagnosis of gastric outlet obstruction. (+info)Gastric outlet obstruction (GOO) is a medical condition that refers to the blockage of the passage from the stomach to the small intestine, also known as the pylorus. This blockage can be caused by various factors, including tumors, scar tissue, or gallstones. As a result, food and digestive enzymes cannot pass through the pylorus into the small intestine, leading to symptoms such as vomiting, abdominal pain, bloating, and weight loss. In severe cases, GOO can lead to malnutrition, dehydration, and other complications if left untreated. Treatment options for GOO depend on the underlying cause of the obstruction and may include medication, endoscopic procedures, or surgery.
Urinary bladder neck obstruction is a medical condition that refers to a partial or complete blockage at the bladder neck, which is the area where the bladder connects to the urethra. This obstruction can be caused by various factors such as prostate enlargement, bladder tumors, scar tissue, or nerve damage.
The bladder neck obstruction can lead to difficulty in urinating, a weak urine stream, and the need to strain while urinating. In severe cases, it can cause urinary retention, kidney failure, and other complications. Treatment for this condition depends on the underlying cause and may include medications, surgery, or minimally invasive procedures.
Duodenal obstruction is a medical condition characterized by the blockage or impediment of the normal flow of contents through the duodenum, which is the first part of the small intestine. This blockage can be partial or complete and can be caused by various factors such as:
1. Congenital abnormalities: Duodenal atresia or stenosis, where there is a congenital absence or narrowing of a portion of the duodenum.
2. Inflammatory conditions: Duodenitis, Crohn's disease, or tumors that cause swelling and inflammation in the duodenum.
3. Mechanical obstructions: Gallstones, tumors, strictures, or adhesions (scar tissue) from previous surgeries can physically block the duodenum.
4. Neuromuscular disorders: Conditions like progressive systemic sclerosis or amyloidosis that affect the neuromuscular function of the intestines can lead to duodenal obstruction.
Symptoms of duodenal obstruction may include nausea, vomiting (often with bilious or fecal matter), abdominal pain, distention, and decreased bowel movements. Diagnosis typically involves imaging studies such as X-rays, CT scans, or upper gastrointestinal series to visualize the blockage. Treatment depends on the underlying cause but may involve surgery, endoscopic procedures, or medications to manage symptoms and address the obstruction.
Gastroenterostomy is a surgical procedure that creates an anastomosis (a connection or junction) between the stomach and the small intestine, usually between the stomach's lesser curvature and the jejunum (the second part of the small intestine). This procedure is often performed to bypass a diseased or obstructed portion of the gastrointestinal tract, such as in the case of gastric ulcers, tumors, or other conditions that prevent normal digestion and absorption.
There are different types of gastroenterostomy procedures, including:
1. Billroth I (or "gastroduodenostomy"): The stomach is connected directly to the duodenum (the first part of the small intestine).
2. Billroth II (or "gastrojejunostomy"): The stomach is connected to the jejunum, bypassing the duodenum.
3. Roux-en-Y gastrojejunostomy: A more complex procedure in which a portion of the jejunum is separated and reconnected further down the small intestine, creating a Y-shaped configuration. This type of gastroenterostomy is often used in bariatric surgery for weight loss.
The choice of gastroenterostomy technique depends on the specific medical condition being treated and the patient's overall health status.
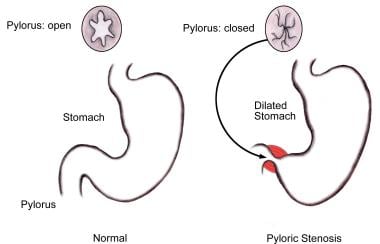
Hypertrophic pyloric stenosis is a condition that affects the muscular valve between the stomach and the small intestine (pylorus). It is characterized by an abnormal thickening (hypertrophy) of the pylorus muscle, which can cause narrowing (stenosis) of the pyloric canal. This makes it difficult for food to pass from the stomach into the small intestine, leading to symptoms such as vomiting, dehydration, and poor weight gain in infants. The condition is typically diagnosed through physical examination, medical history, and imaging tests like ultrasound or X-rays. Treatment usually involves surgery to correct the narrowed pylorus and alleviate symptoms.
Pyloric stenosis is a condition that results in the narrowing or complete obstruction of the pylorus, which is the opening from the stomach into the small intestine. This narrowing is usually caused by hypertrophy (thickening) of the muscles in the pylorus, making it difficult for food to pass from the stomach into the duodenum.
The most common form of this condition is infantile hypertrophic pyloric stenosis, which typically affects infants between 3-6 weeks of age. In this case, the pyloric muscle becomes abnormally thick and narrows the opening, making it difficult for stomach contents to empty into the small intestine. This can lead to symptoms such as vomiting (often projectile), dehydration, and poor weight gain.
The diagnosis of pyloric stenosis is often made through physical examination, ultrasound, or other imaging studies. Treatment typically involves surgery to correct the narrowed opening, known as a pyloromyotomy. This procedure involves making an incision in the pylorus to relieve the obstruction and allow normal stomach emptying.
In some cases, pyloric stenosis can also occur in adults, although this is much less common than in infants. Adult pyloric stenosis can be caused by various factors, including chronic gastritis, peptic ulcers, or previous surgeries. The symptoms and treatment approach for adult pyloric stenosis may differ from those seen in infants.
The pylorus is the lower, narrow part of the stomach that connects to the first part of the small intestine (duodenum). It consists of the pyloric canal, which is a short muscular tube, and the pyloric sphincter, a circular muscle that controls the passage of food from the stomach into the duodenum. The pylorus regulates the entry of chyme (partially digested food) into the small intestine by adjusting the size and frequency of the muscular contractions that push the chyme through the pyloric sphincter. This process helps in further digestion and absorption of nutrients in the small intestine.
Stomach diseases refer to a range of conditions that affect the stomach, a muscular sac located in the upper part of the abdomen and is responsible for storing and digesting food. These diseases can cause various symptoms such as abdominal pain, nausea, vomiting, heartburn, indigestion, loss of appetite, and bloating. Some common stomach diseases include:
1. Gastritis: Inflammation of the stomach lining that can cause pain, irritation, and ulcers.
2. Gastroesophageal reflux disease (GERD): A condition where stomach acid flows back into the esophagus, causing heartburn and damage to the esophageal lining.
3. Peptic ulcers: Open sores that develop on the lining of the stomach or duodenum, often caused by bacterial infections or long-term use of nonsteroidal anti-inflammatory drugs (NSAIDs).
4. Stomach cancer: Abnormal growth of cancerous cells in the stomach, which can spread to other parts of the body if left untreated.
5. Gastroparesis: A condition where the stomach muscles are weakened or paralyzed, leading to difficulty digesting food and emptying the stomach.
6. Functional dyspepsia: A chronic disorder characterized by symptoms such as pain, bloating, and fullness in the upper abdomen, without any identifiable cause.
7. Eosinophilic esophagitis: A condition where eosinophils, a type of white blood cell, accumulate in the esophagus, causing inflammation and difficulty swallowing.
8. Stomal stenosis: Narrowing of the opening between the stomach and small intestine, often caused by scar tissue or surgical complications.
9. Hiatal hernia: A condition where a portion of the stomach protrudes through the diaphragm into the chest cavity, causing symptoms such as heartburn and difficulty swallowing.
These are just a few examples of stomach diseases, and there are many other conditions that can affect the stomach. Proper diagnosis and treatment are essential for managing these conditions and preventing complications.
Duodenal neoplasms refer to abnormal growths in the duodenum, which is the first part of the small intestine that receives digestive secretions from the pancreas and bile duct. These growths can be benign or malignant (cancerous).
Benign neoplasms include adenomas, leiomyomas, lipomas, and hamartomas. They are usually slow-growing and do not spread to other parts of the body. However, they may cause symptoms such as abdominal pain, bleeding, or obstruction of the intestine.
Malignant neoplasms include adenocarcinomas, neuroendocrine tumors (carcinoids), lymphomas, and sarcomas. They are more aggressive and can invade surrounding tissues and spread to other parts of the body. Symptoms may include abdominal pain, weight loss, jaundice, anemia, or bowel obstruction.
The diagnosis of duodenal neoplasms is usually made through imaging tests such as CT scans, MRI, or endoscopy with biopsy. Treatment depends on the type and stage of the tumor and may include surgery, chemotherapy, radiation therapy, or a combination of these modalities.
Duodenal diseases refer to a range of medical conditions that affect the duodenum, which is the first part of the small intestine. Here are some examples of duodenal diseases:
1. Duodenitis: This is inflammation of the duodenum, which can cause symptoms such as abdominal pain, nausea, vomiting, and bloating. Duodenitis can be caused by bacterial or viral infections, excessive use of nonsteroidal anti-inflammatory drugs (NSAIDs), or chronic inflammation due to conditions like Crohn's disease.
2. Peptic ulcers: These are sores that develop in the lining of the duodenum, usually as a result of infection with Helicobacter pylori bacteria or long-term use of NSAIDs. Symptoms can include abdominal pain, bloating, and heartburn.
3. Duodenal cancer: This is a rare type of cancer that affects the duodenum. Symptoms can include abdominal pain, weight loss, and blood in the stool.
4. Celiac disease: This is an autoimmune disorder that causes the immune system to attack the lining of the small intestine in response to gluten, a protein found in wheat, barley, and rye. This can lead to inflammation and damage to the duodenum.
5. Duodenal diverticulosis: This is a condition in which small pouches form in the lining of the duodenum. While many people with duodenal diverticulosis do not experience symptoms, some may develop complications such as inflammation or infection.
6. Duodenal atresia: This is a congenital condition in which the duodenum does not form properly, leading to blockage of the intestine. This can cause symptoms such as vomiting and difficulty feeding in newborns.
A jejunostomy is a surgical procedure where an opening (stoma) is created in the lower part of the small intestine, called the jejunum. This stoma allows for the passage of nutrients and digestive enzymes from the small intestine into a tube or external pouch, bypassing the mouth, esophagus, stomach, and upper small intestine (duodenum).
Jejunostomy is typically performed to provide enteral nutrition support in patients who are unable to consume food or liquids by mouth due to various medical conditions such as dysphagia, gastroparesis, bowel obstruction, or after certain surgical procedures. The jejunostomy tube can be used for short-term or long-term nutritional support, depending on the patient's needs and underlying medical condition.
A biliary fistula is an abnormal connection or passage between the biliary system (which includes the gallbladder, bile ducts, and liver) and another organ or structure, usually in the abdominal cavity. This connection allows bile, which is a digestive fluid produced by the liver, to leak out of its normal pathway and into other areas of the body.
Biliary fistulas can occur as a result of trauma, surgery, infection, or inflammation in the biliary system. Symptoms may include abdominal pain, fever, jaundice (yellowing of the skin and eyes), nausea, vomiting, and clay-colored stools. Treatment typically involves addressing the underlying cause of the fistula, such as draining an infection or repairing damaged tissue, and diverting bile flow away from the site of the leak. In some cases, surgery may be necessary to repair the fistula.
A choristoma is a type of growth that occurs when normally functioning tissue is found in an abnormal location within the body. It is not cancerous or harmful, but it can cause problems if it presses on surrounding structures or causes symptoms. Choristomas are typically congenital, meaning they are present at birth, and are thought to occur due to developmental errors during embryonic growth. They can be found in various organs and tissues throughout the body, including the brain, eye, skin, and gastrointestinal tract.
The pyloric antrum is the distal part of the stomach, which is the last portion that precedes the pylorus and the beginning of the duodenum. It is a thickened, muscular area responsible for grinding and mixing food with gastric juices during digestion. The pyloric antrum also helps regulate the passage of chyme (partially digested food) into the small intestine through the pyloric sphincter, which controls the opening and closing of the pylorus. This region is crucial in the gastrointestinal tract's motor functions and overall digestive process.
Gastrointestinal endoscopy is a medical procedure that allows direct visualization of the inner lining of the digestive tract, which includes the esophagus, stomach, small intestine, large intestine (colon), and sometimes the upper part of the small intestine (duodenum). This procedure is performed using an endoscope, a long, thin, flexible tube with a light and camera at its tip. The endoscope is inserted through the mouth for upper endoscopy or through the rectum for lower endoscopy (colonoscopy), and the images captured by the camera are transmitted to a monitor for the physician to view.
Gastrointestinal endoscopy can help diagnose various conditions, such as inflammation, ulcers, tumors, polyps, or bleeding in the digestive tract. It can also be used for therapeutic purposes, such as removing polyps, taking tissue samples (biopsies), treating bleeding, and performing other interventions to manage certain digestive diseases.
There are different types of gastrointestinal endoscopy procedures, including:
1. Upper Endoscopy (Esophagogastroduodenoscopy or EGD): This procedure examines the esophagus, stomach, and duodenum.
2. Colonoscopy: This procedure examines the colon and rectum.
3. Sigmoidoscopy: A limited examination of the lower part of the colon (sigmoid colon) using a shorter endoscope.
4. Enteroscopy: An examination of the small intestine, which can be performed using various techniques, such as push enteroscopy, single-balloon enteroscopy, or double-balloon enteroscopy.
5. Capsule Endoscopy: A procedure that involves swallowing a small capsule containing a camera, which captures images of the digestive tract as it passes through.
Gastrointestinal endoscopy is generally considered safe when performed by experienced medical professionals. However, like any medical procedure, there are potential risks and complications, such as bleeding, infection, perforation, or adverse reactions to sedatives used during the procedure. Patients should discuss these risks with their healthcare provider before undergoing gastrointestinal endoscopy.
Palliative care is a type of medical care that focuses on relieving the pain, symptoms, and stress of serious illnesses. The goal is to improve quality of life for both the patient and their family. It is provided by a team of doctors, nurses, and other specialists who work together to address the physical, emotional, social, and spiritual needs of the patient. Palliative care can be provided at any stage of an illness, alongside curative treatments, and is not dependent on prognosis.
The World Health Organization (WHO) defines palliative care as: "an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychological and spiritual."
Gastric bypass is a surgical procedure that involves creating a small pouch in the stomach and rerouting the small intestine to connect to this pouch, thereby bypassing the majority of the stomach and the first part of the small intestine (duodenum). This procedure is typically performed as a treatment for morbid obesity and related health conditions such as type 2 diabetes, sleep apnea, and high blood pressure.
The smaller stomach pouch restricts food intake, while the rerouting of the small intestine reduces the amount of calories and nutrients that are absorbed, leading to weight loss. Gastric bypass can also result in hormonal changes that help regulate appetite and metabolism, further contributing to weight loss and improved health outcomes.
There are different types of gastric bypass procedures, including Roux-en-Y gastric bypass and laparoscopic gastric bypass. The choice of procedure depends on various factors such as the patient's overall health, medical history, and personal preferences. Gastric bypass is generally considered a safe and effective treatment for morbid obesity, but like any surgical procedure, it carries risks and requires careful consideration and preparation.
Intestinal obstruction, also known as bowel obstruction, is a medical condition characterized by a blockage that prevents the normal flow of contents through the small intestine or large intestine (colon). This blockage can be caused by various factors such as tumors, adhesions (scar tissue), hernias, inflammation, or impacted feces.
The obstruction can be mechanical, where something physically blocks the intestinal lumen, or functional, where the normal muscular contractions of the bowel are impaired. Mechanical obstructions are more common than functional ones.
Symptoms of intestinal obstruction may include abdominal pain and cramping, nausea and vomiting, bloating, inability to pass gas or have a bowel movement, and abdominal distention. If left untreated, intestinal obstruction can lead to serious complications such as tissue death (necrosis), perforation of the intestine, and sepsis. Treatment typically involves hospitalization, intravenous fluids, nasogastric decompression, and possibly surgery to remove the obstruction.
A Gastrectomy is a surgical procedure involving the removal of all or part of the stomach. This procedure can be total (complete resection of the stomach), partial (removal of a portion of the stomach), or sleeve (removal of a portion of the stomach to create a narrow sleeve-shaped pouch).
Gastrectomies are typically performed to treat conditions such as gastric cancer, benign tumors, severe peptic ulcers, and in some cases, for weight loss in individuals with morbid obesity. The type of gastrectomy performed depends on the patient's medical condition and the extent of the disease.
Following a gastrectomy, patients may require adjustments to their diet and lifestyle, as well as potential supplementation of vitamins and minerals that would normally be absorbed in the stomach. In some cases, further reconstructive surgery might be necessary to reestablish gastrointestinal continuity.
The urinary bladder is a muscular, hollow organ in the pelvis that stores urine before it is released from the body. It expands as it fills with urine and contracts when emptying. The typical adult bladder can hold between 400 to 600 milliliters of urine for about 2-5 hours before the urge to urinate occurs. The wall of the bladder contains several layers, including a mucous membrane, a layer of smooth muscle (detrusor muscle), and an outer fibrous adventitia. The muscles of the bladder neck and urethra remain contracted to prevent leakage of urine during filling, and they relax during voiding to allow the urine to flow out through the urethra.
Stomach neoplasms refer to abnormal growths in the stomach that can be benign or malignant. They include a wide range of conditions such as:
1. Gastric adenomas: These are benign tumors that develop from glandular cells in the stomach lining.
2. Gastrointestinal stromal tumors (GISTs): These are rare tumors that can be found in the stomach and other parts of the digestive tract. They originate from the stem cells in the wall of the digestive tract.
3. Leiomyomas: These are benign tumors that develop from smooth muscle cells in the stomach wall.
4. Lipomas: These are benign tumors that develop from fat cells in the stomach wall.
5. Neuroendocrine tumors (NETs): These are tumors that develop from the neuroendocrine cells in the stomach lining. They can be benign or malignant.
6. Gastric carcinomas: These are malignant tumors that develop from the glandular cells in the stomach lining. They are the most common type of stomach neoplasm and include adenocarcinomas, signet ring cell carcinomas, and others.
7. Lymphomas: These are malignant tumors that develop from the immune cells in the stomach wall.
Stomach neoplasms can cause various symptoms such as abdominal pain, nausea, vomiting, weight loss, and difficulty swallowing. The diagnosis of stomach neoplasms usually involves a combination of imaging tests, endoscopy, and biopsy. Treatment options depend on the type and stage of the neoplasm and may include surgery, chemotherapy, radiation therapy, or targeted therapy.
Airway obstruction is a medical condition that occurs when the normal flow of air into and out of the lungs is partially or completely blocked. This blockage can be caused by a variety of factors, including swelling of the tissues in the airway, the presence of foreign objects or substances, or abnormal growths such as tumors.
When the airway becomes obstructed, it can make it difficult for a person to breathe normally. They may experience symptoms such as shortness of breath, wheezing, coughing, and chest tightness. In severe cases, airway obstruction can lead to respiratory failure and other life-threatening complications.
There are several types of airway obstruction, including:
1. Upper airway obstruction: This occurs when the blockage is located in the upper part of the airway, such as the nose, throat, or voice box.
2. Lower airway obstruction: This occurs when the blockage is located in the lower part of the airway, such as the trachea or bronchi.
3. Partial airway obstruction: This occurs when the airway is partially blocked, allowing some air to flow in and out of the lungs.
4. Complete airway obstruction: This occurs when the airway is completely blocked, preventing any air from flowing into or out of the lungs.
Treatment for airway obstruction depends on the underlying cause of the condition. In some cases, removing the obstruction may be as simple as clearing the airway of foreign objects or mucus. In other cases, more invasive treatments such as surgery may be necessary.
Urodynamics is a medical test that measures the function and performance of the lower urinary tract, which includes the bladder, urethra, and sphincters. It involves the use of specialized equipment to record measurements such as bladder pressure, urine flow rate, and residual urine volume. The test can help diagnose various urinary problems, including incontinence, urinary retention, and overactive bladder.
During the test, a small catheter is inserted into the bladder through the urethra to measure bladder pressure while filling it with sterile water or saline solution. Another catheter may be placed in the rectum to record abdominal pressure. The patient is then asked to urinate, and the flow rate and any leaks are recorded.
Urodynamics can help identify the underlying cause of urinary symptoms and guide treatment decisions. It is often recommended for patients with complex or persistent urinary problems that have not responded to initial treatments.
A stent is a small mesh tube that's used to treat narrow or weak arteries. Arteries are blood vessels that carry blood away from your heart to other parts of your body. A stent is placed in an artery as part of a procedure called angioplasty. Angioplasty restores blood flow through narrowed or blocked arteries by inflating a tiny balloon inside the blocked artery to widen it.
The stent is then inserted into the widened artery to keep it open. The stent is usually made of metal, but some are coated with medication that is slowly and continuously released to help prevent the formation of scar tissue in the artery. This can reduce the chance of the artery narrowing again.
Stents are also used in other parts of the body, such as the neck (carotid artery) and kidneys (renal artery), to help maintain blood flow and prevent blockages. They can also be used in the urinary system to treat conditions like ureteropelvic junction obstruction or narrowing of the urethra.
Laparoscopy is a surgical procedure that involves the insertion of a laparoscope, which is a thin tube with a light and camera attached to it, through small incisions in the abdomen. This allows the surgeon to view the internal organs without making large incisions. It's commonly used to diagnose and treat various conditions such as endometriosis, ovarian cysts, infertility, and appendicitis. The advantages of laparoscopy over traditional open surgery include smaller incisions, less pain, shorter hospital stays, and quicker recovery times.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
 Gastric outlet obstruction
Gastric outlet obstruction
Vagotomy
Sternocostal triangle
Eosinophilic gastroenteritis
Gastric antral vascular ectasia
Succussion splash
Obstructed defecation
Pyloric stenosis
Domperidone
Gastric lymphoma
Antrectomy
Gallstone ileus
Self-expandable metallic stent
Junctional epidermolysis bullosa (medicine)
Bowel obstruction
Pizotifen
Michel Kahaleh
Nausea
List of syndromes
Phytobezoar
Plexiform angiomyxoid myofibroblastic tumor
Bouveret syndrome
Léon Bouveret
Helicobacter pylori
Goo
Peptic ulcer disease
Outlet obstruction
List of MeSH codes (C06)
Obstruction
Gastric atresia
Gastric outlet obstruction - Wikipedia
 Gastric Outlet Obstruction: Background, Anatomy, Pathophysiology
Gastric Outlet Obstruction: Background, Anatomy, Pathophysiology
 Through-the-scope stent for malignant gastric outlet obstruction | HKMJ
Through-the-scope stent for malignant gastric outlet obstruction | HKMJ
Management of Malignant Alimentary Tract Obstruction
GASTRIC OUTLET OBSTRUCTION | Abdominal Key
 Gastric outlet obstruction, another case by Dr. Siddique Akbar Satti
Gastric outlet obstruction, another case by Dr. Siddique Akbar Satti
Endoscopic pyloromyotomy for postesophagectomy gastric outlet obstruction - Fingerprint - Yonsei University
 A CLINICAL STUDY ON GASTRIC OUTLET OBSTRUCTION IN A SOUTH IN | 82588
A CLINICAL STUDY ON GASTRIC OUTLET OBSTRUCTION IN A SOUTH IN | 82588
 Gastric outlet obstruction: a rare complication in patients with intragastric balloon treatment for obesity - 368
Gastric outlet obstruction: a rare complication in patients with intragastric balloon treatment for obesity - 368
 Bouveret's syndrome as an unusual cause of gastric outlet obstruction: A case report - UEA Digital Repository
Bouveret's syndrome as an unusual cause of gastric outlet obstruction: A case report - UEA Digital Repository
 Pyloric stenosis in infants: MedlinePlus Medical Encyclopedia
Pyloric stenosis in infants: MedlinePlus Medical Encyclopedia
 bariatric
bariatric
 Bleeding ulcer: What causes it and is it serious?
Bleeding ulcer: What causes it and is it serious?
 Gastric outlet obstruction secondary to
paraesophageal herniation of gastric antrum after laparoscopic
fundoplication - Coskun...
Gastric outlet obstruction secondary to
paraesophageal herniation of gastric antrum after laparoscopic
fundoplication - Coskun...
 Endoscopic ultrasound-guided gastrojejunostomy versus robotic gastrojejunostomy for unresectable malignant gastric outlet...
Endoscopic ultrasound-guided gastrojejunostomy versus robotic gastrojejunostomy for unresectable malignant gastric outlet...
 Surgery for peptic ulcer disease in children in the post-histamine2-blocker era
Surgery for peptic ulcer disease in children in the post-histamine2-blocker era
A short term outcome of laparoscopic hand sewn roux-en-y gastrojejunostomy in gastric outlet obstruction from a developing...
 Early Satiety: Causes, Symptoms & Diagnosis
Early Satiety: Causes, Symptoms & Diagnosis
 GOO Archives - American College of Gastroenterology
GOO Archives - American College of Gastroenterology
 Hiram D. Ortega-cruz, MD
Hiram D. Ortega-cruz, MD
Benign Gastric Tumors: Practice Essentials, Pathophysiology, Epidemiology
 Gastric Bypass | Omaha | Nebraska Medicine
Gastric Bypass | Omaha | Nebraska Medicine
 Motion Sickness - Traveler Summary - TripPrep.com
Motion Sickness - Traveler Summary - TripPrep.com
 Portal hypertensive polyps, a new entity?
Portal hypertensive polyps, a new entity?
Esophageal Perforation after Gastric Balloon Extraction - SAGES Abstract Archives
Pernicious anemia
 Thieme E-Books & E-Journals - Endoscopy / Issue
Thieme E-Books & E-Journals - Endoscopy / Issue
 Hypergastrinemia: Causes, Definition, Symptoms & Treatment
Hypergastrinemia: Causes, Definition, Symptoms & Treatment
 Magiran | فهرست مطالب «Hamidreza Kianifar»
Magiran | فهرست مطالب «Hamidreza Kianifar»Esophageal4
- For patients with esophageal obstruction who are candidates for resection or chemoradiation, Ahmed and colleagues advised against routine use of self-expanding metal stents (SEMS) due to "high rates of stent migration, higher morbidity and mortality, and potentially lower R0 (microscopically negative margins) resection rates. (medscape.com)
- Among patients with esophageal obstruction who are not candidates for resection, SEMS insertion or brachytherapy may be used separately or in combination, according to the investigators. (medscape.com)
- Upper GI series findings may reveal esophageal stricture, duodenal ulcers, duodenal strictures, and hypertrophic gastric and duodenal folds. (medscape.com)
- EGD may be necessary to detect erosive esophagitis, peptic strictures, esophageal cancer, gastric outlet obstruction, and other potentially significant upper GI tract findings. (onteenstoday.com)
Duodenal6
- In benign causes, the obstruction is typically the result of inflammation, edema, or scarring in the region of the pyloric channel or duodenal bulb. (abdominalkey.com)
- With PUD, the obstruction typically results from acute inflammation and edema or chronic fibrosis and scarring of the pyloric channel or duodenal bulb. (abdominalkey.com)
- In the case of gastric and duodenal malignancies, GOO typically results from intrinsic obstruction by the primary tumor. (abdominalkey.com)
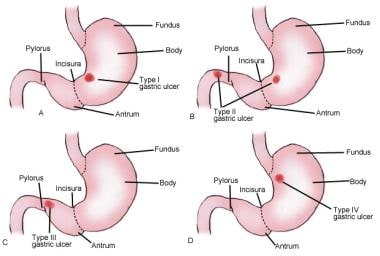
- The most common causes of acute gastric outlet obstruction (GOO) are duodenal and type 3 gastric ulcers. (scipedia.com)
- In the gastric antrum a multiple polypoid and polylobed lesions were observed, occupying prepyloric region and extending into the pylorus and duodenal bulb ( Fig. 1 ). (isciii.es)
- This article summarizes surgical, endoscopic, and other palliative techniques for relief of obstructive jaundice, relief of duodenal or gastric outlet obstruction, and relief of pain due to invasion of the celiac plexus. (ahrq.gov)
Duodenum6
- Malignant Tumours of the stomach, including adenocarcinoma (and its linitis plastica variant), lymphoma, and gastrointestinal stromal tumours In a peptic ulcer it is believed to be a result of edema and scarring of the ulcer, followed by healing and fibrosis, which leads to obstruction of the gastroduodenal junction (usually an ulcer in the first part of the duodenum). (wikipedia.org)
- Ulcers within the pyloric channel and first portion of the duodenum usually are responsible for outlet obstruction. (medscape.com)
- GOO results from either an intrinsic or an extrinsic obstruction of the pyloric channel or duodenum. (abdominalkey.com)
- Dr. S A Satti writes in his report, "There is a Polypoidal growth in the duodenum bulb causing obstruction in the passage of D2. (medicotips.com)
- Endoscopy of upper gastrointestinal tract has been a sensitive and specific investigation to study the status of gastric outlet -the pylorus and has enabled early detection of lesions of both stomach and duodenum. (jebmh.com)
- The ulcer extends into the muscularis propria layer of the gastric epithelium and usually occurs in the stomach or duodenum. (obgproject.com)
Cause of gastric5
- This is another cause of gastric outlet obstruction or pyloric stenosis . (medicotips.com)
- The management of this rare cause of gastric outlet obstruction is discussed. (uea.ac.uk)
- Antral hyperplastic polyp: A rare cause of gastric outlet obstruction. (isciii.es)
- Hypertrophic pyloric stenosis is a common cause of intestinal obstruction in infancy, and is not initially considered as a cause of gastric outlet obstruction in childhood. (cshd.org.tr)
- In conclusion, we suggest that hypertrophic pyloric stenosis should be considered as a rare cause of gastric outlet obstruction in childhood as well as infancy. (cshd.org.tr)
Cases of gastric outlet obst2
- citation needed] Surgery is indicated in cases of gastric outlet obstruction in which there is significant obstruction and in cases where medical therapy has failed. (wikipedia.org)
- We undertook a prospective clinical study regarding incidence, etiology, investigation and management of cases of Gastric outlet obstruction in adults in a period of three years. (jebmh.com)
Ulcers1
- It is the main cause of ulcers occurring in the lining of the upper part of the small intestine and in the lining of the stomach, which are called gastric ulcers. (express.co.uk)
Malignant gastric outlet obst3
- This report is of the technique and results for through-the-scope stent in palliating malignant gastric outlet obstruction for 17 patients. (hkmj.org)
- Endoscopic ultrasound-guided gastrojejunostomy versus robotic gastrojejunostomy for unresectable malignant gastric outlet obstruction. (bvsalud.org)
- Malignant gastric outlet obstruction (GOO) has traditionally been managed with enteral stenting and surgical gastrojejunostomy . (bvsalud.org)
Endoscopic4
- it can involve antibiotic treatment when Helicobacter pylori is related to an ulcer, endoscopic therapies (such as dilation of the obstruction with balloons or the placement of self-expandable metallic stents), other medical therapies, or surgery to resolve the obstruction. (wikipedia.org)
- Endoscopic balloon dilation for benign gastric outlet obstruction with or without Helicobacter pylori infection. (wikipedia.org)
- Endoscopic image may suggest malignant lesions such as gastric adenocarcinoma, even submucosal tumor lesions. (isciii.es)
- This American Society for Gastrointestinal Endoscopy guideline provides evidence-based recommendations for the endoscopic management of gastric outlet obstruction (GOO). (bvsalud.org)
Stomach6
- Gastric outlet obstruction (GOO) is a medical condition where there is an obstruction at the level of the pylorus, which is the outlet of the stomach. (wikipedia.org)
- Individuals with gastric outlet obstruction will often have recurrent vomiting of food that has accumulated in the stomach, but which cannot pass into the small intestine due to the obstruction. (wikipedia.org)
- CT scan of the abdomen and pelvis revealed a dilated stomach proximal to the baloon with a retained device and a small passage of contrast to the small bowel, consistent with mechanical gastric outlet obstruction due to the BIB. (sages.org)
- Gastrin stimulates your stomach to release acid (gastric acid). (clevelandclinic.org)
- Gastric outlet obstruction, which blocks the passageway between your stomach and your small intestine. (clevelandclinic.org)
- The condition could indicate a person is suffering from a stomach ulcer - an ailment which can lead to serious complications such as internal bleeding, perforation and gastric outlet obstruction. (express.co.uk)
Endoscopy3
- All these symptoms in view of his age and previous history of APD suggest that there could be some stricture or growth around gastric outlet, so in order to confirm that Dr. Siddique Akbar Satti went for upper GI endoscopy which was done on 6/4/15. (medicotips.com)
- With the advent of modern techniques and the widespread use of gastric endoscopy, benign gastric-wall lesions are now diagnosed more frequently and can be studied using the tissue obtained by biopsy or polypectomy. (medscape.com)
- In the past, the diagnosis of gastric tumors was based on radiographic examination, but in 1922, Schendler was the first to make an endoscopy-based diagnosis. (medscape.com)
Tumors8
- One of the presentations of gastric tumors is Gastric outlet obstruction which presents with biochemical and anatomicosurgical syndrome in these patients. (journalcra.com)
- The majority of benign gastric tumors are asymptomatic, but in very rare cases, they present with epigastric pain, gastric outlet obstruction , and bleeding. (medscape.com)
- Many benign gastric tumors are found incidentally on gastroscopy. (medscape.com)
- Of the large variety of gastric tumors, GISTs are the only type that has a real systemic medical therapy. (medscape.com)
- Gastric polyps, polyposis syndromes , and nonmucosal intramural tumors are treated surgically or endoscopically. (medscape.com)
- Polyps account for 3.1% of all gastric tumors, and their frequency increases to almost 90% of benign gastric tumors. (medscape.com)
- In 1955, Zollinger and Ellison first described the classic triad of fulminating peptic ulcer disease, gastric acid hypersecretion, and non-beta islet cell tumors. (medscape.com)
- A syndrome that is characterized by the triad of severe PEPTIC ULCER, hypersecretion of GASTRIC ACID, and GASTRIN-producing tumors of the PANCREAS or other tissue (GASTRINOMA). (bvsalud.org)
Gastrointestinal9
- Usually asymptomatic, but in rare cases, they can cause anemia, gastrointestinal bleeding and gastric outlet obstruction, due to their antral location (4). (isciii.es)
- The diagnosis of gastric outlet obstruction was confirmed by an upper gastrointestinal series. (sages.org)
- If gastrointestinal symptoms develop, patients should be evaluated for gastric cancers given their increased risk. (logicalimages.com)
- When the symptoms are present immediately after birth, the most common cause is a gastrointestinal obstruction. (radiologyassistant.nl)
- In this article we will discuss the congenital gastrointestinal obstructions and also some acquired diseases that present as an acute abdomen in the neonate. (radiologyassistant.nl)
- Gastric bezoars can occur in all age groups and often occur in patients with behavior disorders, abnormal gastric emptying, or altered gastrointestinal anatomy. (msdmanuals.com)
- Pathophysiology is due to discontinuation of the inner lining of the gastrointestinal (GI) tract due to gastric acid secretion or pepsin causing an ulcer. (obgproject.com)
- Gastrointestinal bezoars are a relatively common clinical reality ever since the introduction of truncal vagotomy associated with drainage of gastric resection in the treatment of gastroduodenal peptic ulcer [4]. (who.int)
- Misurata city, and swallowing it is recomc mulation of entericccoated aspirin tablets mended for the treatment of gastrointestinal due to gastric outlet scarring and impaired diseases in this area. (who.int)
Acute4
- In the acute or chronic phase of obstruction, continuous vomiting may lead to dehydration and electrolyte abnormalities. (medscape.com)
- Obstruction can occur in an acute setting secondary to acute inflammation and edema or, more commonly, in a chronic setting secondary to scarring and fibrosis. (medscape.com)
- In both acute and chronic phases of obstruction, persistent emesis can result in severe dehydration and, oftentimes, profound electrolyte abnormalities. (abdominalkey.com)
- Acute GOO is characterized by delayed gastric emptying, anorexia, or nausea accompanied by vomiting. (scipedia.com)
Etiology2
- the mechanism of obstruction depends upon the underlying etiology. (medscape.com)
- The onset of symptoms varies depending on the etiology of the obstruction. (abdominalkey.com)
Hypertrophic1
- The presence of hypertrophic gastric folds on plain radiographs has a sensitivity of 94% for Zollinger-Ellison syndrome. (medscape.com)
Tumor2
- The surgical approach in gastric cancer depends on the location, size, and locally invasive characteristics of the tumor. (medscape.com)
- Síndrome caracterizado por la triada de ÚLCERA PÉPTICA grava, hipersecreción de ÁCIDO GÁSTRICO y tumor secretor de GASTRINA, en el PÁNCREAS o en otros tejidos (GASTRINOMA). (bvsalud.org)
Pancreatic1
- A pancreatic pseudocyst can cause gastric compression. (wikipedia.org)
Malignancy1
- however, one review showed that only 37% of patients with GOO have benign disease and the remaining patients have obstruction secondary to malignancy. (medscape.com)
Benign causes1
- Causes of gastric outlet obstruction include both benign causes (such as peptic ulcer disease affecting the area around the pylorus), as well as malignant causes, such as gastric cancer. (wikipedia.org)
Antrum3
- Herein we report a 56-year-old man diagnosed with GOO secondary to paraesophageal hiatal herniation of gastric antrum after laparoscopic fundoplication. (scipedia.com)
- Inflammation, scarring, or infiltration of the antrum and pylorus are associated with the development of gastric outlet obstruction (GOO). (scipedia.com)
- Here, we presented a patient diagnosed with benign GOO secondary to paraesophageal herniation (PEH) of gastric antrum after laparoscopic fundoplication. (scipedia.com)
Differential diagnosis1
- The differential diagnosis of gastric outlet obstruction may include: early gastric carcinoma, hiatal hernia, gastroesophageal reflux, adrenal insufficiency, and inborn errors of metabolism. (wikipedia.org)
Symptoms of gastric2
- Large distal lesions have been associated with symptoms of gastric outlet obstruction. (medscape.com)
- Most symptoms of gastric cancer reflect advanced disease. (medscape.com)
Gastrojejunostomy3
- According to the update, patients with gastric outlet obstruction who have good functional status and a life expectancy greater than 2 months should undergo surgical gastrojejunostomy, ideally via a laparoscopic approach instead of an open approach because of shorter hospital stays and less blood loss. (medscape.com)
- We became interested to study the surgical outcome of laparoscopic hand sewn Roux En Y Gastrojejunostomy anastomosis in gastric outlet obstruction. (journalcra.com)
- The conclusion of the study was Laparoscopic Roux En Y Gastrojejunostomy is effective in achieving quality of life and the chances of afferent loop syndrome are least with it. (journalcra.com)
Acid3
- Gastric acid helps your body digest food and absorb nutrients, such as amino acids and proteins. (clevelandclinic.org)
- To diagnose hypergastrinemia, healthcare providers need to find out how much gastric acid you're producing. (clevelandclinic.org)
- [ 11 ] The diagnosis of Zollinger-Ellison syndrome is made on the basis of a combination of criteria, including the clinical presentation, gastrin radioimmunoassay findings, gastric acid secretory testing, and diagnostic imaging evaluation. (medscape.com)
Polyps9
- Gastric polyps are defined as luminal lesions projecting above the plane of the mucosal surface and are relatively frequent in routine pathology practice. (medscape.com)
- Various subtypes of gastric polyps are recognized and divided into nonneoplastic and neoplastic and are also further classified by their association with polyposis syndromes. (medscape.com)
- Gastric polyps: a retrospective analysis of 26,000 digestive endoscopies. (medscape.com)
- Gastric polyps: classification and management. (medscape.com)
- Current Management of Benign Epithelial Gastric Polyps. (medscape.com)
- Pathological study described gastric hyperplastic polyps with edema, vascular congestion and smooth muscle hyperplasia without dysplasia or adenomatous changes ( Fig. 2 ). (isciii.es)
- Portal hypertensive polyps (PHP) are a recent entity, described in cirrhotic patients with portal hypertension, portal venous obstruction or antral vascular ectasia. (isciii.es)
- Gastric polyps in patients with portal hypertension. (isciii.es)
- Diagnostic accuracy of forceps biopsy versus polypectomy for gastric polyps: A prospective multicentre study. (isciii.es)
Early gastric1
- however, some patients with incidental complaints are diagnosed with early gastric cancer. (medscape.com)
Peptic ulcer d1
- The incidence of gastric outlet obstruction (GOO) is not precisely known, though it is likely lower in recent years due to the decrease in peptic ulcer disease (PUD). (abdominalkey.com)
Complication2
- A common complication is gastric outlet obstruction at the band site. (sages.org)
- Phytobezoars can occur in adult patients as a postoperative complication after gastric bypass or partial gastrectomy, especially when partial gastrectomy is accompanied by vagotomy. (msdmanuals.com)
Mechanical5
- it is the clinical and pathophysiological consequence of any disease process that produces a mechanical impediment to gastric emptying. (medscape.com)
- Once a mechanical obstruction is confirmed, differentiate between benign and malignant processes because definitive treatment is based on recognition of the specific underlying cause. (medscape.com)
- In contrast, obstruction secondary to a large gastric polyp, gastric bezoar, gastric volvulus, or migration of a gastrostomy tube represents a discrete mechanical problem. (abdominalkey.com)
- Gastric outlet obstruction is defined as a clinical and patho-physiological consequence of any disease process that produces a mechanical impediment to gastric emptying which may be extrinsic or intrinsic. (jebmh.com)
- Intestinal Obstruction Intestinal obstruction is significant mechanical impairment or complete arrest of the passage of contents through the intestine due to pathology that causes blockage of the bowel. (msdmanuals.com)
Gastroparesis3
- As part of the initial workup, exclude the possibility of functional nonmechanical causes of obstruction, such as diabetic gastroparesis. (medscape.com)
- We present the results of a double blind, placebo controlled, crossover study of ghrelin in gastric emptying in patients with diabetic gastroparesis. (bmj.com)
- Ghrelin increases gastric emptying in patients with diabetic gastroparesis. (bmj.com)
Intestinal Obstruction1
- Intestinal obstruction of gastroenterology, 2nd ed. (who.int)
Bezoar3
- other systemic illness, or drugs increases the risk of gastric bezoar formation. (msdmanuals.com)
- We report a 17-year-old Libyan female with coeliac disease who developed a gastric bezoar as a result of excessive olibanum intake. (who.int)
- We report a 17cyearcold Libyan female with coeliac disease who developed a gastric bezoar as a result of excessive olibanum intake. (who.int)
Refractory1
- Indications for operation were bleeding (n = 11), pneumoperitoneum (n = 13), peritonitis (n = 3), and gastric outlet obstruction refractory to medical therapy (n = 2). (nih.gov)
Diagnosis1
- Abdominal X-ray may show a gastric fluid level which would support the diagnosis. (wikipedia.org)
Complications2
- The most commonly reported complications include balloon intolerance requiring early removal, gastric erosions, gastric ulcerations, esophagitis, and early deflation of the device. (sages.org)
- Due to the risk of anticholinergic complications, caution should be used in patients susceptible to intestinal or urinary outlet obstructions. (janusinfo.se)
Abdominal radiograph2
- The patient presented with high-volume non-bile- stained output from a nasogastric tube and a dilated gastric bubble on abdominal radiograph. (hkmj.org)
- In suspected neonatal obstruction the first step is an abdominal radiograph. (radiologyassistant.nl)
Surgery4
- For patients with malignant colonic obstruction, SEMS may be considered as a "bridge to surgery," wrote Ahmed and colleagues, and in the case of proximal or right-sided malignant obstruction, as a bridge to surgery or a palliative measure, keeping in mind "the technical challenges of SEMS insertion in those areas. (medscape.com)
- While gastric bypass surgery can be effective, there are other non-surgical options available to you. (nebraskamed.com)
- What is Roux-en-Y Gastric Bypass Surgery and How Does it Promote Weight-loss? (nebraskamed.com)
- The Roux-en-Y gastric bypass is considered the gold standard for weight-loss surgery. (nebraskamed.com)
Occurs1
- Delayed gastric emptying occurs in up to 50% of patients with chronic diabetes and is associated with significant impairments in both quality of life and diabetic control. (bmj.com)
Clinical3
- The American Gastroenterological Association published a clinical practice update expert review for managing malignant alimentary tract obstructions (MATOs) that includes 14 best practice advice statements, ranging from general principles to specific clinical choices. (medscape.com)
- Management of gastric schwannoma: A retrospective analysis of clinical characteristics, treatments, and outcomes. (medscape.com)
- Although in high obstruction vomiting will be the most striking symptom, whereas in low obstruction this will be constipation, both symptoms are often present concurrently, and the clinical differentiation between a high and a low obstruction is difficult. (radiologyassistant.nl)
Asymptomatic1
- Gastric bezoars are usually asymptomatic. (msdmanuals.com)
Luminal1
- however, they should not be used in patients with severely impaired gastric motility or multiple luminal obstructions "because of limited benefit in these scenarios. (medscape.com)
Volvulus1
- Symptoms generally occur abruptly when the obstruction is secondary to conditions such as gastric volvulus, prolapse of a large gastric polyp, or migration of a gastrostomy tube. (abdominalkey.com)
Stent1
- To conclude, through-the-scope stent was safe and feasible, offering an alternative minimal invasive method to palliate obstructive symptoms for patients with inoperable tumours causing gastric outlet obstruction. (hkmj.org)
Depends1
- citation needed] Treatment of gastric outlet obstruction depends on the cause, but is usually either surgical or medical. (wikipedia.org)
Dilatation2
- When obstruction persists, patients may develop significant and progressive gastric dilatation. (medscape.com)
- Massive dilatation is seen in complete obstruction and is accompanied by fluid levels on the dorsal decubitus radiograph. (radiologyassistant.nl)
Ultrasound1
- Gastric emptying rate (GER) was calculated by real time ultrasound following a test meal. (bmj.com)
Patients4
- Patients present with intermittent symptoms that progress until obstruction is complete. (medscape.com)
- 7 Initially, patients have intermittent symptoms that then progress until the obstruction is complete. (abdominalkey.com)
- The patients complaints were relieved when a nasogastric tube was inserted and 3 L of gastric fluid was decompressed. (scipedia.com)
- 1 Impaired gastric emptying in diabetic patients can be associated with a number of possible metabolic consequences: poor glycaemic control, increased risk of postprandial hypoglycaemia, and variable drug absorption. (bmj.com)