Pancreatic Neoplasms
Neoplasms
Neoplasms, Cystic, Mucinous, and Serous
Genitalia, Female
Neoplasms, Multiple Primary
Neoplasms, Second Primary
Sex Characteristics
Adenocarcinoma, Mucinous
Sex Factors
Myeloproliferative Disorders
Cystadenoma
Immunohistochemistry
Neoplasms, Connective and Soft Tissue
Neoplasms, Plasma Cell
Ovarian Neoplasms
Neoplasms, Experimental
Cystadenoma, Mucinous
Gastrointestinal Neoplasms
Carcinoma, Pancreatic Ductal
Neoplasms, Radiation-Induced
Neoplasms, Vascular Tissue
Carcinoma, Papillary
Adenocarcinoma, Papillary
Neoplasms, Muscle Tissue
Testicular Neoplasms
Neoplasms, Glandular and Epithelial
Neoplasm Staging
Soft Tissue Neoplasms
Cystadenocarcinoma, Mucinous
Hematologic Neoplasms
Neoplasm Proteins
Vascular Neoplasms
Dog Diseases
Neoplasms, Adnexal and Skin Appendage
Sweat Gland Neoplasms
Palatal Neoplasms
Retrospective Studies
Antigens, Neoplasm
Cystadenocarcinoma
Condoms, Female
Heart Neoplasms
Tumor Markers, Biological
Cystadenoma, Serous
Bcl10 is not a target for frequent mutation in human carcinomas. (1/552)
The recently described Bcl10 gene has been suggested to be a major target gene for inactivation in a variety of human cancers. In order to further evaluate the role of this gene in human adult malignancies, we have analysed a series of carcinomas for mutations in the Bcl10 gene. We have screened a panel of 174 carcinoma samples in total, comprised of 47 breast, 36 epithelial ovarian, 36 endometrial, 12 cervical, 23 colorectal and 20 head/neck carcinomas, all unselected for grade or stage. This panel reflects, in part, tumours reported to have involvement of the 1p22 region of chromosome 1, the region harbouring the Bcl10 gene. No deleterious mutations were detected in any of the samples analysed, strongly suggesting that Bcl10 is not a common target for inactivation in adult malignancies and that BCL10 is not the gene targeted for frequent inactivation at 1p22. (+info)Three dimensional ultrasound and power doppler in assessment of uterine and ovarian angiogenesis: a prospective study. (2/552)
AIM: To determine whether three-dimensional power Doppler can improve the recognition of pelvic tumor morphology and angiogenesis. METHODS: Using this technique we analyzed 180 adnexal masses and 110 uterine lesions. Tumor volume, morphology, and vascularity were evaluated in each patient. Irregular and randomly dispersed vessels with complex branching depicted by comprehensive three dimensional display were suggestive of pelvic malignancy, while linear-like vascular morphology, single vessel arrangement and regular branching were typical for benign structures. RESULTS: Addition of qualitative analysis of vascular architecture of adnexal tumor to morphological parameters reached 96.15% sensitivity and 98.73% specificity. When endometrial lesions were prospectively analyzed, sensitivity and specificity were 91.67% and 98.49%, respectively. Because the lowest positive predictive value of 16.67% was obtained for myometrial lesions, this method should not be advised for their eva luation. CONCLUSION: Good results achieved by three dimensional ultrasound can be explained by improved recognition of the pelvic lesion anatomy, characterization of the surface features, detection of the tumor infiltration, and precise depiction of the size and volume. Three dimensional power Doppler imaging can detect structural abnormalities of the malignant tumor vessels, such as arteriovenous shunts, microaneurysms, tumoral lakes, disproportional calibration, coiling, and dichotomous branching. Therefore it enhances and facilitates the morphologic and functional evaluation of both benign and malignant pelvic tumors. (+info)New approaches for estimating risk from exposure to diethylstilbestrol. (3/552)
A subgroup from a National Institute of Environmental Health Sciences, workshop concerned with characterizing the effects of endocrine disruptors on human health at environmental exposure levels considered the question, If diethylstilbestrol (DES) were introduced into the market for human use today and likely to result in low-dose exposure of the human fetus, what would be required to assess risk? On the basis of an analysis of the quality of data on human DES exposure, the critical times and doses for inducing genital tract malformations and cancer must be determined. This would be facilitated through analysis of the ontogeny of estrogen receptor expression in the developing human genital tract. Models of low-dose estrogenic effects will have to be developed for human and rodent genital tract development. Mouse models offer many advantages over other potential animal models because of the wealth of the earlier literature, the availability of sensitive end points, the availability of mutant lines, and the possibility of generating genetically engineered model systems. Through multidisciplinary approaches, it should be possible to elucidate the cellular and molecular mechanisms of endocrine disruption elicited by estrogens during development and facilitate an assessment of risk to humans. (+info)Gynaecological cancer. (4/552)
Gynaecological cancer encompasses a number of tumours with different epidemiology, pathology and treatment strategies. This article reviews the principal clinical advances and areas of development in cancer of the ovary, cervix, endometrium and vulva. (+info)Expression of folate receptor type alpha in relation to cell type, malignancy, and differentiation in ovary, uterus, and cervix. (5/552)
The folate receptor (FR) type alpha is known to be frequently overexpressed in ovarian cancer and is the target for a number of novel experimental cancer therapies. The relative levels of FR expression among specific cell types and its relationship to malignant transformation have not been adequately established because of several inherent limitations of the immunocytochemical approaches used previously. We used a quantitative in situ hybridization method to examine the expression of the mRNAs for the known isoforms of FR in paraffin-embedded tissue sections of multiple samples of the various subtypes of ovarian, uterine, and cervical cancers. Benign lesions, as well as the various normal cell types in the ovary, the uterus, and the cervix, were examined similarly. FR mRNA levels were quantitated relative to the transcript levels for beta-actin using NIH Image 1.57 computer software. The results show that the ovary, the uterus, and the cervix present different patterns of FR regulation in differentiation and in malignancy. In the ovary, benign differentiation of the germinal epithelium into mucinous or serous tumors or malignant transformation into mucinous tumors is associated with down-regulation of FR-alpha, whereas FR-alpha expression is retained in malignant lesions of serous and endometrioid differentiation. In contrast, malignant transformation of the glandular epithelial cells of the uterine endometrium is associated with de novo expression of FR-alpha. Heterogeneity in FR expression within malignant ovarian and uterine tumors is related to differentiation. In contrast to the uterus, malignant transformation of glandular epithelial cells in the cervix may frequently result in down-regulation of FR-alpha. These results shed new light for the identification of malignancies suitable for FR-mediated therapies and for prognostic/diagnostic applications of FR. They also provide a phenomenological basis for molecular studies of FR regulation in malignant cells. (+info)Immunohistochemical analysis of uroplakins, urothelial specific proteins, in ovarian Brenner tumors, normal tissues, and benign and neoplastic lesions of the female genital tract. (6/552)
Uroplakins are the characteristic integral membrane proteins in terminally differentiated, superficial urothelial asymmetric unit membrane. Brenner tumors of the ovary and Walthard cell nests of Fallopian tubes have been considered to represent urothelial differentiation in the female genital tract, but no definitive differentiation marker has been demonstrated supporting such a conclusion. An immunohistochemical analysis was performed to assess the expression of uroplakins in these lesions as well as in various benign and neoplastic lesions and normal tissues of the female genital tract. Focal expression of uroplakins was observed on the luminal surface of ovarian Brenner tumor cells forming microcysts in all 5 cases examined. In contrast, uroplakins were slightly expressed in only 1 of 12 cases of Walthard cell nests, even in the presence of microcyst formation. Uroplakins were not expressed in other benign or malignant lesions or normal tissues of the female genital tract. These results support the hypothesis that the Brenner tumor and possibly Walthard cell nests represent urothelial (transitional cell) differentiation. (+info)Application of a marker of ciliated epithelial cells to gynaecological pathology. (7/552)
BACKGROUND: The assessment of neoplastic disease in gynaecological histopathology can be complicated by the high incidence of metaplasia seen in tissues of the female genital tract. There is a need to identify specific tissue markers which can be applied in routine histopathological practice. AIM: To examine the clinical potential of a monoclonal antibody, LhS28, which reacts with basal bodies of ciliated epithelial cells. METHODS: A panel of normal and pathological gynaecological tissues was processed and labelled with LhS28. RESULTS: LhS28 immunoreactivity was found in the normal Fallopian tube where it was confined to ciliated rather than secretory epithelial cells. In the remaining specimens, LhS28 was associated exclusively with ciliated cells in tubal metaplasias of the cervix and endometrium and in benign serous lined inclusion cysts. CONCLUSIONS: LhS28 may be a valuable marker for identifying metaplasia of tubal type and may find application in distinguishing tubal metaplasia from low grade cervical glandular intraepithelial neoplasia. (+info)Clinical features of hypersensitivity reactions to carboplatin. (8/552)
PURPOSE: To characterize the clinical features of carboplatin-associated hypersensitivity reactions. PATIENTS: Patients with gynecologic malignancies treated at the Cleveland Clinic Foundation from June 1995 through July 1998 who experienced a carboplatin-associated hypersensitivity reaction were the subjects of this evaluation. RESULTS: Of the 205 patients treated with carboplatin during this time period, 24 (12%) developed a carboplatin hypersensitivity reaction. The median number of platinum (carboplatin plus cisplatin) courses for the first episode was eight (range, six to 21). Only three patients (13%) developed this toxicity during their initial chemotherapy regimen, with the remainder experiencing a reaction during their second (n = 15) or third (n = 6) carboplatin treatment program for recurrent disease. Thirteen patients (54%) developed at least moderately severe symptoms (diffuse erythroderma, tachycardia, chest tightness, wheezing, facial swelling, dyspnea, hypertension, or hypotension). In approximately one half of patients, the reaction developed after more than 50% of the carboplatin had been infused. Only one of three patients was successfully treated with the agent upon rechallenge. CONCLUSION: Carboplatin hypersensitivity reactions develop in patients who have been extensively pretreated with the agent. The clinical features are highly variable, but they are sufficiently different from those noted after the administration of paclitaxel that it should not be difficult to distinguish between reactions to the two agents. As carboplatin is increasingly used as initial and second-line chemotherapy of ovarian cancer and other malignancies, it can be anticipated that hypersensitivity reactions to the drug will become a more common and difficult clinical management issue. (+info)Genital neoplasms in males refer to abnormal growths or tumors that develop in the male reproductive organs. These can be benign (non-cancerous) or malignant (cancerous).
Malignant genital neoplasms are often referred to as genital cancers. The most common types of male genital cancers include:
1. Penile Cancer: This occurs when cancer cells form in the tissues of the penis.
2. Testicular Cancer: This forms in the testicles (testes), which are located inside the scrotum.
3. Prostate Cancer: This is a common cancer in men, forming in the prostate gland, which is part of the male reproductive system that helps make semen.
4. Scrotal Cancer: This is a rare form of cancer that forms in the skin or tissue of the scrotum.
5. Penile Intraepithelial Neoplasia (PeIN): This is not cancer, but it is considered a pre-cancerous condition of the penis.
Early detection and treatment of genital neoplasms can significantly improve the prognosis. Regular self-examinations and medical check-ups are recommended, especially for individuals with risk factors such as smoking, HIV infection, or a family history of these cancers.
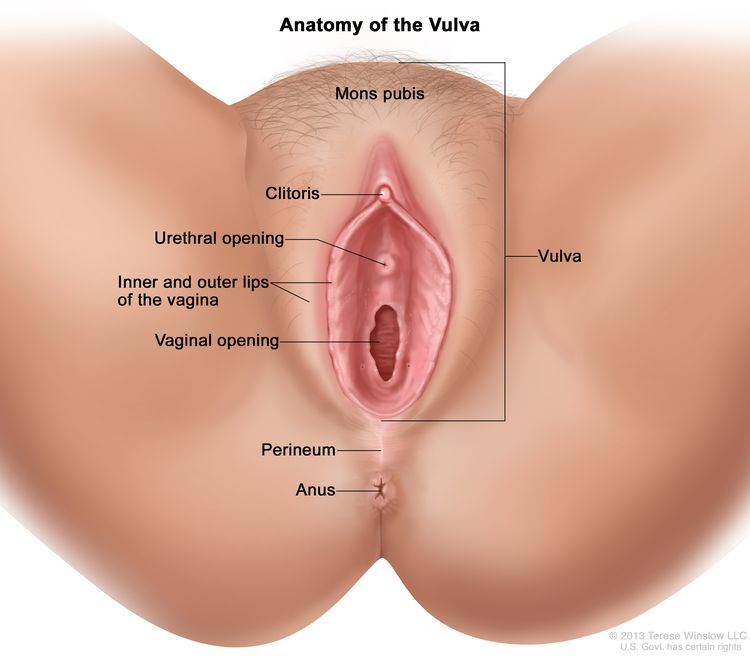
Genital neoplasms in females refer to abnormal growths or tumors that occur in the female reproductive organs. These can be benign (non-cancerous) or malignant (cancerous). The most common types of female genital neoplasms are:
1. Cervical cancer: This is a malignancy that arises from the cells lining the cervix, usually caused by human papillomavirus (HPV) infection.
2. Uterine cancer: Also known as endometrial cancer, this type of female genital neoplasm originates in the lining of the uterus (endometrium).
3. Ovarian cancer: This is a malignancy that develops from the cells in the ovaries, which can be difficult to detect at an early stage due to its location and lack of symptoms.
4. Vulvar cancer: A rare type of female genital neoplasm that affects the external female genital area (vulva).
5. Vaginal cancer: This is a malignancy that occurs in the vagina, often caused by HPV infection.
6. Gestational trophoblastic neoplasia: A rare group of tumors that develop from placental tissue and can occur during or after pregnancy.
Regular screening and early detection are crucial for successful treatment and management of female genital neoplasms.
Pancreatic neoplasms refer to abnormal growths in the pancreas that can be benign or malignant. The pancreas is a gland located behind the stomach that produces hormones and digestive enzymes. Pancreatic neoplasms can interfere with the normal functioning of the pancreas, leading to various health complications.
Benign pancreatic neoplasms are non-cancerous growths that do not spread to other parts of the body. They are usually removed through surgery to prevent any potential complications, such as blocking the bile duct or causing pain.
Malignant pancreatic neoplasms, also known as pancreatic cancer, are cancerous growths that can invade and destroy surrounding tissues and organs. They can also spread (metastasize) to other parts of the body, such as the liver, lungs, or bones. Pancreatic cancer is often aggressive and difficult to treat, with a poor prognosis.
There are several types of pancreatic neoplasms, including adenocarcinomas, neuroendocrine tumors, solid pseudopapillary neoplasms, and cystic neoplasms. The specific type of neoplasm is determined through various diagnostic tests, such as imaging studies, biopsies, and blood tests. Treatment options depend on the type, stage, and location of the neoplasm, as well as the patient's overall health and preferences.
Neoplasms are abnormal growths of cells or tissues in the body that serve no physiological function. They can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow growing and do not spread to other parts of the body, while malignant neoplasms are aggressive, invasive, and can metastasize to distant sites.
Neoplasms occur when there is a dysregulation in the normal process of cell division and differentiation, leading to uncontrolled growth and accumulation of cells. This can result from genetic mutations or other factors such as viral infections, environmental exposures, or hormonal imbalances.
Neoplasms can develop in any organ or tissue of the body and can cause various symptoms depending on their size, location, and type. Treatment options for neoplasms include surgery, radiation therapy, chemotherapy, immunotherapy, and targeted therapy, among others.
Neoplasms: Neoplasms refer to abnormal growths of tissue that can be benign (non-cancerous) or malignant (cancerous). They occur when the normal control mechanisms that regulate cell growth and division are disrupted, leading to uncontrolled cell proliferation.
Cystic Neoplasms: Cystic neoplasms are tumors that contain fluid-filled sacs or cysts. These tumors can be benign or malignant and can occur in various organs of the body, including the pancreas, ovary, and liver.
Mucinous Neoplasms: Mucinous neoplasms are a type of cystic neoplasm that is characterized by the production of mucin, a gel-like substance produced by certain types of cells. These tumors can occur in various organs, including the ovary, pancreas, and colon. Mucinous neoplasms can be benign or malignant, and malignant forms are often aggressive and have a poor prognosis.
Serous Neoplasms: Serous neoplasms are another type of cystic neoplasm that is characterized by the production of serous fluid, which is a thin, watery fluid. These tumors commonly occur in the ovary and can be benign or malignant. Malignant serous neoplasms are often aggressive and have a poor prognosis.
In summary, neoplasms refer to abnormal tissue growths that can be benign or malignant. Cystic neoplasms contain fluid-filled sacs and can occur in various organs of the body. Mucinous neoplasms produce a gel-like substance called mucin and can also occur in various organs, while serous neoplasms produce thin, watery fluid and commonly occur in the ovary. Both mucinous and serous neoplasms can be benign or malignant, with malignant forms often being aggressive and having a poor prognosis.
Skin neoplasms refer to abnormal growths or tumors in the skin that can be benign (non-cancerous) or malignant (cancerous). They result from uncontrolled multiplication of skin cells, which can form various types of lesions. These growths may appear as lumps, bumps, sores, patches, or discolored areas on the skin.
Benign skin neoplasms include conditions such as moles, warts, and seborrheic keratoses, while malignant skin neoplasms are primarily classified into melanoma, squamous cell carcinoma, and basal cell carcinoma. These three types of cancerous skin growths are collectively known as non-melanoma skin cancers (NMSCs). Melanoma is the most aggressive and dangerous form of skin cancer, while NMSCs tend to be less invasive but more common.
It's essential to monitor any changes in existing skin lesions or the appearance of new growths and consult a healthcare professional for proper evaluation and treatment if needed.
Female genitalia refer to the reproductive and sexual organs located in the female pelvic region. They are primarily involved in reproduction, menstruation, and sexual activity. The external female genitalia, also known as the vulva, include the mons pubis, labia majora, labia minora, clitoris, and the external openings of the urethra and vagina. The internal female genitalia consist of the vagina, cervix, uterus, fallopian tubes, and ovaries. These structures work together to facilitate menstruation, fertilization, pregnancy, and childbirth.
Multiple primary neoplasms refer to the occurrence of more than one primary malignant tumor in an individual, where each tumor is unrelated to the other and originates from separate cells or organs. This differs from metastatic cancer, where a single malignancy spreads to multiple sites in the body. Multiple primary neoplasms can be synchronous (occurring at the same time) or metachronous (occurring at different times). The risk of developing multiple primary neoplasms increases with age and is associated with certain genetic predispositions, environmental factors, and lifestyle choices such as smoking and alcohol consumption.
Kidney neoplasms refer to abnormal growths or tumors in the kidney tissues that can be benign (non-cancerous) or malignant (cancerous). These growths can originate from various types of kidney cells, including the renal tubules, glomeruli, and the renal pelvis.
Malignant kidney neoplasms are also known as kidney cancers, with renal cell carcinoma being the most common type. Benign kidney neoplasms include renal adenomas, oncocytomas, and angiomyolipomas. While benign neoplasms are generally not life-threatening, they can still cause problems if they grow large enough to compromise kidney function or if they undergo malignant transformation.
Early detection and appropriate management of kidney neoplasms are crucial for improving patient outcomes and overall prognosis. Regular medical check-ups, imaging studies, and urinalysis can help in the early identification of these growths, allowing for timely intervention and treatment.
A "second primary neoplasm" is a distinct, new cancer or malignancy that develops in a person who has already had a previous cancer. It is not a recurrence or metastasis of the original tumor, but rather an independent cancer that arises in a different location or organ system. The development of second primary neoplasms can be influenced by various factors such as genetic predisposition, environmental exposures, and previous treatments like chemotherapy or radiation therapy.
It is important to note that the definition of "second primary neoplasm" may vary slightly depending on the specific source or context. In general medical usage, it refers to a new, separate cancer; however, in some research or clinical settings, there might be more precise criteria for defining and diagnosing second primary neoplasms.
"Sex characteristics" refer to the anatomical, chromosomal, and genetic features that define males and females. These include both primary sex characteristics (such as reproductive organs like ovaries or testes) and secondary sex characteristics (such as breasts or facial hair) that typically develop during puberty. Sex characteristics are primarily determined by the presence of either X or Y chromosomes, with XX individuals usually developing as females and XY individuals usually developing as males, although variations and exceptions to this rule do occur.
Thyroid neoplasms refer to abnormal growths or tumors in the thyroid gland, which can be benign (non-cancerous) or malignant (cancerous). These growths can vary in size and may cause a noticeable lump or nodule in the neck. Thyroid neoplasms can also affect the function of the thyroid gland, leading to hormonal imbalances and related symptoms. The exact causes of thyroid neoplasms are not fully understood, but risk factors include radiation exposure, family history, and certain genetic conditions. It is important to note that most thyroid nodules are benign, but a proper medical evaluation is necessary to determine the nature of the growth and develop an appropriate treatment plan.
Adenocarcinoma, mucinous is a type of cancer that begins in the glandular cells that line certain organs and produce mucin, a substance that lubricates and protects tissues. This type of cancer is characterized by the presence of abundant pools of mucin within the tumor. It typically develops in organs such as the colon, rectum, lungs, pancreas, and ovaries.
Mucinous adenocarcinomas tend to have a distinct appearance under the microscope, with large pools of mucin pushing aside the cancer cells. They may also have a different clinical behavior compared to other types of adenocarcinomas, such as being more aggressive or having a worse prognosis in some cases.
It is important to note that while a diagnosis of adenocarcinoma, mucinous can be serious, the prognosis and treatment options may vary depending on several factors, including the location of the cancer, the stage at which it was diagnosed, and the individual's overall health.
"Sex factors" is a term used in medicine and epidemiology to refer to the differences in disease incidence, prevalence, or response to treatment that are observed between males and females. These differences can be attributed to biological differences such as genetics, hormones, and anatomy, as well as social and cultural factors related to gender.
For example, some conditions such as autoimmune diseases, depression, and osteoporosis are more common in women, while others such as cardiovascular disease and certain types of cancer are more prevalent in men. Additionally, sex differences have been observed in the effectiveness and side effects of various medications and treatments.
It is important to consider sex factors in medical research and clinical practice to ensure that patients receive appropriate and effective care.
Myeloproliferative disorders (MPDs) are a group of rare, chronic blood cancers that originate from the abnormal proliferation or growth of one or more types of blood-forming cells in the bone marrow. These disorders result in an overproduction of mature but dysfunctional blood cells, which can lead to serious complications such as blood clots, bleeding, and organ damage.
There are several subtypes of MPDs, including:
1. Chronic Myeloid Leukemia (CML): A disorder characterized by the overproduction of mature granulocytes (a type of white blood cell) in the bone marrow, leading to an increased number of these cells in the blood. CML is caused by a genetic mutation that results in the formation of the BCR-ABL fusion protein, which drives uncontrolled cell growth and division.
2. Polycythemia Vera (PV): A disorder characterized by the overproduction of all three types of blood cells - red blood cells, white blood cells, and platelets - in the bone marrow. This can lead to an increased risk of blood clots, bleeding, and enlargement of the spleen.
3. Essential Thrombocythemia (ET): A disorder characterized by the overproduction of platelets in the bone marrow, leading to an increased risk of blood clots and bleeding.
4. Primary Myelofibrosis (PMF): A disorder characterized by the replacement of normal bone marrow tissue with scar tissue, leading to impaired blood cell production and anemia, enlargement of the spleen, and increased risk of infections and bleeding.
5. Chronic Neutrophilic Leukemia (CNL): A rare disorder characterized by the overproduction of neutrophils (a type of white blood cell) in the bone marrow, leading to an increased number of these cells in the blood. CNL can lead to an increased risk of infections and organ damage.
MPDs are typically treated with a combination of therapies, including chemotherapy, targeted therapy, immunotherapy, and stem cell transplantation. The choice of treatment depends on several factors, including the subtype of MPD, the patient's age and overall health, and the presence of any comorbidities.
Sexual behavior in animals refers to a variety of behaviors related to reproduction and mating that occur between members of the same species. These behaviors can include courtship displays, mating rituals, and various physical acts. The specific forms of sexual behavior displayed by a given species are influenced by a combination of genetic, hormonal, and environmental factors.
In some animals, sexual behavior is closely tied to reproductive cycles and may only occur during certain times of the year or under specific conditions. In other species, sexual behavior may be more frequent and less closely tied to reproduction, serving instead as a means of social bonding or communication.
It's important to note that while humans are animals, the term "sexual behavior" is often used in a more specific sense to refer to sexual activities between human beings. The study of sexual behavior in animals is an important area of research within the field of animal behavior and can provide insights into the evolutionary origins of human sexual behavior as well as the underlying mechanisms that drive it.
Lung neoplasms refer to abnormal growths or tumors in the lung tissue. These tumors can be benign (non-cancerous) or malignant (cancerous). Malignant lung neoplasms are further classified into two main types: small cell lung carcinoma and non-small cell lung carcinoma. Lung neoplasms can cause symptoms such as cough, chest pain, shortness of breath, and weight loss. They are often caused by smoking or exposure to secondhand smoke, but can also occur due to genetic factors, radiation exposure, and other environmental carcinogens. Early detection and treatment of lung neoplasms is crucial for improving outcomes and survival rates.
The term "DNA, neoplasm" is not a standard medical term or concept. DNA refers to deoxyribonucleic acid, which is the genetic material present in the cells of living organisms. A neoplasm, on the other hand, is a tumor or growth of abnormal tissue that can be benign (non-cancerous) or malignant (cancerous).
In some contexts, "DNA, neoplasm" may refer to genetic alterations found in cancer cells. These genetic changes can include mutations, amplifications, deletions, or rearrangements of DNA sequences that contribute to the development and progression of cancer. Identifying these genetic abnormalities can help doctors diagnose and treat certain types of cancer more effectively.
However, it's important to note that "DNA, neoplasm" is not a term that would typically be used in medical reports or research papers without further clarification. If you have any specific questions about DNA changes in cancer cells or neoplasms, I would recommend consulting with a healthcare professional or conducting further research on the topic.
Liver neoplasms refer to abnormal growths in the liver that can be benign or malignant. Benign liver neoplasms are non-cancerous tumors that do not spread to other parts of the body, while malignant liver neoplasms are cancerous tumors that can invade and destroy surrounding tissue and spread to other organs.
Liver neoplasms can be primary, meaning they originate in the liver, or secondary, meaning they have metastasized (spread) to the liver from another part of the body. Primary liver neoplasms can be further classified into different types based on their cell of origin and behavior, including hepatocellular carcinoma, cholangiocarcinoma, and hepatic hemangioma.
The diagnosis of liver neoplasms typically involves a combination of imaging studies, such as ultrasound, CT scan, or MRI, and biopsy to confirm the type and stage of the tumor. Treatment options depend on the type and extent of the neoplasm and may include surgery, radiation therapy, chemotherapy, or liver transplantation.
Parotid neoplasms refer to abnormal growths or tumors in the parotid gland, which is the largest of the salivary glands and is located in front of the ear and extends down the neck. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign parotid neoplasms are typically slow-growing, painless masses that may cause facial asymmetry or difficulty in chewing or swallowing if they become large enough to compress surrounding structures. The most common type of benign parotid tumor is a pleomorphic adenoma.
Malignant parotid neoplasms, on the other hand, are more aggressive and can invade nearby tissues and spread to other parts of the body. They may present as rapidly growing masses that are firm or fixed to surrounding structures. Common types of malignant parotid tumors include mucoepidermoid carcinoma, adenoid cystic carcinoma, and squamous cell carcinoma.
The diagnosis of parotid neoplasms typically involves a thorough clinical evaluation, imaging studies such as CT or MRI scans, and fine-needle aspiration biopsy (FNAB) to determine the nature of the tumor. Treatment options depend on the type, size, and location of the neoplasm but may include surgical excision, radiation therapy, and chemotherapy.
Cystadenoma is a type of benign tumor (not cancerous), which arises from glandular epithelial cells and is covered by a thin layer of connective tissue. These tumors can develop in various locations within the body, including the ovaries, pancreas, and other organs that contain glands.
There are two main types of cystadenomas: serous and mucinous. Serous cystadenomas are filled with a clear or watery fluid, while mucinous cystadenomas contain a thick, gelatinous material. Although they are generally not harmful, these tumors can grow quite large and cause discomfort or other symptoms due to their size or location. In some cases, cystadenomas may undergo malignant transformation and develop into cancerous tumors, known as cystadenocarcinomas. Regular medical follow-up and monitoring are essential for individuals diagnosed with cystadenomas to ensure early detection and treatment of any potential complications.
Immunohistochemistry (IHC) is a technique used in pathology and laboratory medicine to identify specific proteins or antigens in tissue sections. It combines the principles of immunology and histology to detect the presence and location of these target molecules within cells and tissues. This technique utilizes antibodies that are specific to the protein or antigen of interest, which are then tagged with a detection system such as a chromogen or fluorophore. The stained tissue sections can be examined under a microscope, allowing for the visualization and analysis of the distribution and expression patterns of the target molecule in the context of the tissue architecture. Immunohistochemistry is widely used in diagnostic pathology to help identify various diseases, including cancer, infectious diseases, and immune-mediated disorders.
Neoplasms of connective and soft tissue are abnormal growths or tumors that develop in the body's supportive tissues, such as cartilage, tendons, ligaments, fascia, and fat. These neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign connective and soft tissue neoplasms include:
- Lipomas: slow-growing, fatty tumors that develop under the skin.
- Fibromas: firm, benign tumors that develop in connective tissue such as tendons or ligaments.
- Nevi (plural of nevus): benign growths made up of cells called melanocytes, which produce pigment.
Malignant connective and soft tissue neoplasms include:
- Sarcomas: a type of cancer that develops in the body's supportive tissues such as muscle, bone, fat, cartilage, or blood vessels. There are many different types of sarcomas, including liposarcoma (fatty tissue), rhabdomyosarcoma (muscle), and osteosarcoma (bone).
- Desmoid tumors: a rare type of benign tumor that can become aggressive and invade surrounding tissues. While not considered cancerous, desmoid tumors can cause significant morbidity due to their tendency to grow and infiltrate nearby structures.
Connective and soft tissue neoplasms can present with various symptoms depending on their location and size. Treatment options include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular follow-up care is essential to monitor for recurrence or metastasis (spread) of the tumor.
Appendiceal neoplasms refer to various types of tumors that can develop in the appendix, a small tube-like structure attached to the large intestine. These neoplasms can be benign or malignant and can include:
1. Adenomas: These are benign tumors that arise from the glandular cells lining the appendix. They are usually slow-growing and may not cause any symptoms.
2. Carcinoids: These are neuroendocrine tumors that arise from the hormone-producing cells in the appendix. They are typically small and slow-growing, but some can be aggressive and spread to other parts of the body.
3. Mucinous neoplasms: These are tumors that produce mucin, a slippery substance that can cause the appendix to become distended and filled with mucus. They can be low-grade (less aggressive) or high-grade (more aggressive) and may spread to other parts of the abdomen.
4. Adenocarcinomas: These are malignant tumors that arise from the glandular cells lining the appendix. They are relatively rare but can be aggressive and spread to other parts of the body.
5. Pseudomyxoma peritonei: This is a condition in which mucin produced by an appendiceal neoplasm leaks into the abdominal cavity, causing a jelly-like accumulation of fluid and tissue. It can be caused by both benign and malignant tumors.
Treatment for appendiceal neoplasms depends on the type and stage of the tumor, as well as the patient's overall health. Treatment options may include surgery, chemotherapy, or radiation therapy.
Plasma cell neoplasms are a type of cancer that originates from plasma cells, which are a type of white blood cell found in the bone marrow. These cells are responsible for producing antibodies to help fight off infections. When plasma cells become cancerous and multiply out of control, they can form a tumor called a plasmacytoma.
There are two main types of plasma cell neoplasms: solitary plasmacytoma and multiple myeloma. Solitary plasmacytoma is a localized tumor that typically forms in the bone, while multiple myeloma is a systemic disease that affects multiple bones and can cause a variety of symptoms such as bone pain, fatigue, and anemia.
Plasma cell neoplasms are diagnosed through a combination of tests, including blood tests, imaging studies, and bone marrow biopsy. Treatment options depend on the stage and extent of the disease, but may include radiation therapy, chemotherapy, and stem cell transplantation.
Ovarian neoplasms refer to abnormal growths or tumors in the ovary, which can be benign (non-cancerous) or malignant (cancerous). These growths can originate from various cell types within the ovary, including epithelial cells, germ cells, and stromal cells. Ovarian neoplasms are often classified based on their cell type of origin, histological features, and potential for invasive or metastatic behavior.
Epithelial ovarian neoplasms are the most common type and can be further categorized into several subtypes, such as serous, mucinous, endometrioid, clear cell, and Brenner tumors. Some of these epithelial tumors have a higher risk of becoming malignant and spreading to other parts of the body.
Germ cell ovarian neoplasms arise from the cells that give rise to eggs (oocytes) and can include teratomas, dysgerminomas, yolk sac tumors, and embryonal carcinomas. Stromal ovarian neoplasms develop from the connective tissue cells supporting the ovary and can include granulosa cell tumors, thecomas, and fibromas.
It is essential to diagnose and treat ovarian neoplasms promptly, as some malignant forms can be aggressive and potentially life-threatening if not managed appropriately. Regular gynecological exams, imaging studies, and tumor marker tests are often used for early detection and monitoring of ovarian neoplasms. Treatment options may include surgery, chemotherapy, or radiation therapy, depending on the type, stage, and patient's overall health condition.
Experimental neoplasms refer to abnormal growths or tumors that are induced and studied in a controlled laboratory setting, typically in animals or cell cultures. These studies are conducted to understand the fundamental mechanisms of cancer development, progression, and potential treatment strategies. By manipulating various factors such as genetic mutations, environmental exposures, and pharmacological interventions, researchers can gain valuable insights into the complex processes underlying neoplasm formation and identify novel targets for cancer therapy. It is important to note that experimental neoplasms may not always accurately represent human cancers, and further research is needed to translate these findings into clinically relevant applications.
Mucinous cystadenoma is a type of benign tumor that arises from the epithelial cells lining the mucous membranes of the body. It is most commonly found in the ovary, but can also occur in other locations such as the pancreas or appendix.
Mucinous cystadenomas are characterized by the production of large amounts of mucin, a slippery, gel-like substance that accumulates inside the tumor and causes it to grow into a cystic mass. These tumors can vary in size, ranging from a few centimeters to over 20 centimeters in diameter.
While mucinous cystadenomas are generally benign, they have the potential to become cancerous (mucinous cystadenocarcinoma) if left untreated. Symptoms of mucinous cystadenoma may include abdominal pain or swelling, bloating, and changes in bowel movements or urinary habits. Treatment typically involves surgical removal of the tumor.
Endocrine gland neoplasms refer to abnormal growths (tumors) that develop in the endocrine glands. These glands are responsible for producing hormones, which are chemical messengers that regulate various functions and processes in the body. Neoplasms can be benign or malignant (cancerous). Benign neoplasms tend to grow slowly and do not spread to other parts of the body. Malignant neoplasms, on the other hand, can invade nearby tissues and organs and may also metastasize (spread) to distant sites.
Endocrine gland neoplasms can occur in any of the endocrine glands, including:
1. Pituitary gland: located at the base of the brain, it produces several hormones that regulate growth and development, as well as other bodily functions.
2. Thyroid gland: located in the neck, it produces thyroid hormones that regulate metabolism and calcium balance.
3. Parathyroid glands: located near the thyroid gland, they produce parathyroid hormone that regulates calcium levels in the blood.
4. Adrenal glands: located on top of each kidney, they produce hormones such as adrenaline, cortisol, and aldosterone that regulate stress response, metabolism, and blood pressure.
5. Pancreas: located behind the stomach, it produces insulin and glucagon, which regulate blood sugar levels, and digestive enzymes that help break down food.
6. Pineal gland: located in the brain, it produces melatonin, a hormone that regulates sleep-wake cycles.
7. Gonads (ovaries and testicles): located in the pelvis (ovaries) and scrotum (testicles), they produce sex hormones such as estrogen, progesterone, and testosterone that regulate reproductive function and secondary sexual characteristics.
Endocrine gland neoplasms can cause various symptoms depending on the type and location of the tumor. For example, a pituitary gland neoplasm may cause headaches, vision problems, or hormonal imbalances, while an adrenal gland neoplasm may cause high blood pressure, weight gain, or mood changes.
Diagnosis of endocrine gland neoplasms typically involves a combination of medical history, physical examination, imaging studies such as CT or MRI scans, and laboratory tests to measure hormone levels. Treatment options may include surgery, radiation therapy, chemotherapy, or hormonal therapy, depending on the type and stage of the tumor.
Gastrointestinal (GI) neoplasms refer to abnormal growths in the gastrointestinal tract, which can be benign or malignant. The gastrointestinal tract includes the mouth, esophagus, stomach, small intestine, large intestine, rectum, and anus.
Benign neoplasms are non-cancerous growths that do not invade nearby tissues or spread to other parts of the body. They can sometimes be removed completely and may not cause any further health problems.
Malignant neoplasms, on the other hand, are cancerous growths that can invade nearby tissues and organs and spread to other parts of the body through the bloodstream or lymphatic system. These types of neoplasms can be life-threatening if not diagnosed and treated promptly.
GI neoplasms can cause various symptoms, including abdominal pain, bloating, changes in bowel habits, nausea, vomiting, weight loss, and anemia. The specific symptoms may depend on the location and size of the neoplasm.
There are many types of GI neoplasms, including adenocarcinomas, gastrointestinal stromal tumors (GISTs), lymphomas, and neuroendocrine tumors. The diagnosis of GI neoplasms typically involves a combination of medical history, physical examination, imaging studies, and biopsy. Treatment options may include surgery, radiation therapy, chemotherapy, targeted therapy, or immunotherapy.
Nose neoplasms refer to abnormal growths or tumors in the nasal cavity or paranasal sinuses. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow-growing and do not spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and have the potential to metastasize.
Nose neoplasms can cause various symptoms such as nasal congestion, nosebleeds, difficulty breathing through the nose, loss of smell, facial pain or numbness, and visual changes if they affect the eye. The diagnosis of nose neoplasms usually involves a combination of physical examination, imaging studies (such as CT or MRI scans), and biopsy to determine the type and extent of the growth. Treatment options depend on the type, size, location, and stage of the neoplasm and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Pancreatic ductal carcinoma (PDC) is a specific type of cancer that forms in the ducts that carry digestive enzymes out of the pancreas. It's the most common form of exocrine pancreatic cancer, making up about 90% of all cases.
The symptoms of PDC are often vague and can include abdominal pain, jaundice (yellowing of the skin and eyes), unexplained weight loss, and changes in bowel movements. These symptoms can be similar to those caused by other less serious conditions, which can make diagnosis difficult.
Pancreatic ductal carcinoma is often aggressive and difficult to treat. The prognosis for PDC is generally poor, with a five-year survival rate of only about 9%. Treatment options may include surgery, chemotherapy, radiation therapy, or a combination of these approaches. However, because PDC is often not detected until it has advanced, treatment is frequently focused on palliative care to relieve symptoms and improve quality of life.
Radiation-induced neoplasms are a type of cancer or tumor that develops as a result of exposure to ionizing radiation. Ionizing radiation is radiation with enough energy to remove tightly bound electrons from atoms or molecules, leading to the formation of ions. This type of radiation can damage DNA and other cellular structures, which can lead to mutations and uncontrolled cell growth, resulting in the development of a neoplasm.
Radiation-induced neoplasms can occur after exposure to high levels of ionizing radiation, such as that received during radiation therapy for cancer treatment or from nuclear accidents. The risk of developing a radiation-induced neoplasm depends on several factors, including the dose and duration of radiation exposure, the type of radiation, and the individual's genetic susceptibility to radiation-induced damage.
Radiation-induced neoplasms can take many years to develop after initial exposure to ionizing radiation, and they often occur at the site of previous radiation therapy. Common types of radiation-induced neoplasms include sarcomas, carcinomas, and thyroid cancer. It is important to note that while ionizing radiation can increase the risk of developing cancer, the overall risk is still relatively low, especially when compared to other well-established cancer risk factors such as smoking and exposure to certain chemicals.
A neoplasm of vascular tissue is an abnormal growth or mass of cells in the blood vessels or lymphatic vessels. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms, such as hemangiomas and lymphangiomas, are typically not harmful and may not require treatment. However, they can cause symptoms if they grow large enough to press on nearby organs or tissues. Malignant neoplasms, such as angiosarcomas, are cancerous and can invade and destroy surrounding tissue, as well as spread (metastasize) to other parts of the body. Treatment for vascular tissue neoplasms depends on the type, size, location, and stage of the growth, and may include surgery, radiation therapy, chemotherapy, or a combination of these.
Eye neoplasms, also known as ocular tumors or eye cancer, refer to abnormal growths of tissue in the eye. These growths can be benign (non-cancerous) or malignant (cancerous). Eye neoplasms can develop in various parts of the eye, including the eyelid, conjunctiva, cornea, iris, ciliary body, choroid, retina, and optic nerve.
Benign eye neoplasms are typically slow-growing and do not spread to other parts of the body. They may cause symptoms such as vision changes, eye pain, or a noticeable mass in the eye. Treatment options for benign eye neoplasms include monitoring, surgical removal, or radiation therapy.
Malignant eye neoplasms, on the other hand, can grow and spread rapidly to other parts of the body. They may cause symptoms such as vision changes, eye pain, floaters, or flashes of light. Treatment options for malignant eye neoplasms depend on the type and stage of cancer but may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
It is important to note that early detection and treatment of eye neoplasms can improve outcomes and prevent complications. Regular eye exams with an ophthalmologist are recommended for early detection and prevention of eye diseases, including eye neoplasms.
Salivary gland neoplasms refer to abnormal growths or tumors that develop in the salivary glands. These glands are responsible for producing saliva, which helps in digestion, lubrication of food and maintaining oral health. Salivary gland neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign neoplasms are slow-growing and typically do not spread to other parts of the body. They may cause symptoms such as swelling, painless lumps, or difficulty swallowing if they grow large enough to put pressure on surrounding tissues.
Malignant neoplasms, on the other hand, can be aggressive and have the potential to invade nearby structures and metastasize (spread) to distant organs. Symptoms of malignant salivary gland neoplasms may include rapid growth, pain, numbness, or paralysis of facial nerves.
Salivary gland neoplasms can occur in any of the major salivary glands (parotid, submandibular, and sublingual glands) or in the minor salivary glands located throughout the mouth and throat. The exact cause of these neoplasms is not fully understood, but risk factors may include exposure to radiation, certain viral infections, and genetic predisposition.
An adenoma is a benign (noncancerous) tumor that develops from glandular epithelial cells. These types of cells are responsible for producing and releasing fluids, such as hormones or digestive enzymes, into the surrounding tissues. Adenomas can occur in various organs and glands throughout the body, including the thyroid, pituitary, adrenal, and digestive systems.
Depending on their location, adenomas may cause different symptoms or remain asymptomatic. Some common examples of adenomas include:
1. Colorectal adenoma (also known as a polyp): These growths occur in the lining of the colon or rectum and can develop into colorectal cancer if left untreated. Regular screenings, such as colonoscopies, are essential for early detection and removal of these polyps.
2. Thyroid adenoma: This type of adenoma affects the thyroid gland and may result in an overproduction or underproduction of hormones, leading to conditions like hyperthyroidism (overactive thyroid) or hypothyroidism (underactive thyroid).
3. Pituitary adenoma: These growths occur in the pituitary gland, which is located at the base of the brain and controls various hormonal functions. Depending on their size and location, pituitary adenomas can cause vision problems, headaches, or hormonal imbalances that affect growth, reproduction, and metabolism.
4. Liver adenoma: These rare benign tumors develop in the liver and may not cause any symptoms unless they become large enough to press on surrounding organs or structures. In some cases, liver adenomas can rupture and cause internal bleeding.
5. Adrenal adenoma: These growths occur in the adrenal glands, which are located above the kidneys and produce hormones that regulate stress responses, metabolism, and blood pressure. Most adrenal adenomas are nonfunctioning, meaning they do not secrete excess hormones. However, functioning adrenal adenomas can lead to conditions like Cushing's syndrome or Conn's syndrome, depending on the type of hormone being overproduced.
It is essential to monitor and manage benign tumors like adenomas to prevent potential complications, such as rupture, bleeding, or hormonal imbalances. Treatment options may include surveillance with imaging studies, medication to manage hormonal issues, or surgical removal of the tumor in certain cases.
Carcinoma, papillary is a type of cancer that begins in the cells that line the glandular structures or the lining of organs. In a papillary carcinoma, the cancerous cells grow and form small finger-like projections, called papillae, within the tumor. This type of cancer most commonly occurs in the thyroid gland, but can also be found in other organs such as the lung, breast, and kidney. Papillary carcinoma of the thyroid gland is usually slow-growing and has a good prognosis, especially when it is diagnosed at an early stage.
Adenocarcinoma, papillary is a type of cancer that begins in the glandular cells and grows in a finger-like projection (called a papilla). This type of cancer can occur in various organs, including the lungs, pancreas, thyroid, and female reproductive system. The prognosis and treatment options for papillary adenocarcinoma depend on several factors, such as the location and stage of the tumor, as well as the patient's overall health. It is important to consult with a healthcare professional for an accurate diagnosis and personalized treatment plan.
Reproduction, in the context of biology and medicine, refers to the process by which organisms produce offspring. It is a complex process that involves the creation, development, and growth of new individuals from parent organisms. In sexual reproduction, this process typically involves the combination of genetic material from two parents through the fusion of gametes (sex cells) such as sperm and egg cells. This results in the formation of a zygote, which then develops into a new individual with a unique genetic makeup.
In contrast, asexual reproduction does not involve the fusion of gametes and can occur through various mechanisms such as budding, fragmentation, or parthenogenesis. Asexual reproduction results in offspring that are genetically identical to the parent organism.
Reproduction is a fundamental process that ensures the survival and continuation of species over time. It is also an area of active research in fields such as reproductive medicine, where scientists and clinicians work to understand and address issues related to human fertility, contraception, and genetic disorders.
Uterine neoplasms refer to abnormal growths in the uterus, which can be benign (non-cancerous) or malignant (cancerous). These growths can originate from different types of cells within the uterus, leading to various types of uterine neoplasms. The two main categories of uterine neoplasms are endometrial neoplasms and uterine sarcomas.
Endometrial neoplasms develop from the endometrium, which is the inner lining of the uterus. Most endometrial neoplasms are classified as endometrioid adenocarcinomas, arising from glandular cells in the endometrium. Other types include serous carcinoma, clear cell carcinoma, and mucinous carcinoma.
Uterine sarcomas, on the other hand, are less common and originate from the connective tissue (stroma) or muscle (myometrium) of the uterus. Uterine sarcomas can be further divided into several subtypes, such as leiomyosarcoma, endometrial stromal sarcoma, and undifferentiated uterine sarcoma.
Uterine neoplasms can cause various symptoms, including abnormal vaginal bleeding or discharge, pelvic pain, and difficulty urinating or having bowel movements. The diagnosis typically involves a combination of imaging tests (such as ultrasound, CT, or MRI scans) and tissue biopsies to determine the type and extent of the neoplasm. Treatment options depend on the type, stage, and patient's overall health but may include surgery, radiation therapy, chemotherapy, or hormone therapy.
Neoplasms in muscle tissue refer to abnormal and excessive growths of muscle cells that can be benign or malignant. These growths can arise from any of the three types of muscle tissue: skeletal, cardiac, or smooth muscle. Neoplasms in muscle tissue are classified based on their origin, behavior, and histological features.
Benign neoplasms in muscle tissue include leiomyomas (smooth muscle), rhabdomyomas (skeletal muscle), and myxomas (cardiac muscle). These tumors are usually slow-growing and do not invade surrounding tissues or spread to other parts of the body.
Malignant neoplasms in muscle tissue, also known as sarcomas, include leiomyosarcoma (smooth muscle), rhabdomyosarcoma (skeletal muscle), and angiosarcoma (cardiac muscle). These tumors are aggressive, invasive, and have the potential to metastasize to other parts of the body.
Symptoms of neoplasms in muscle tissue depend on their location, size, and type. They may include a painless or painful mass, weakness, fatigue, weight loss, and difficulty swallowing or breathing. Treatment options for neoplasms in muscle tissue include surgery, radiation therapy, chemotherapy, and targeted therapy. The choice of treatment depends on the type, stage, location, and patient's overall health condition.
Testicular neoplasms are abnormal growths or tumors in the testicle that can be benign (non-cancerous) or malignant (cancerous). They are a type of genitourinary cancer, which affects the reproductive and urinary systems. Testicular neoplasms can occur in men of any age but are most commonly found in young adults between the ages of 15 and 40.
Testicular neoplasms can be classified into two main categories: germ cell tumors and non-germ cell tumors. Germ cell tumors, which arise from the cells that give rise to sperm, are further divided into seminomas and non-seminomas. Seminomas are typically slow-growing and have a good prognosis, while non-seminomas tend to grow more quickly and can spread to other parts of the body.
Non-germ cell tumors are less common than germ cell tumors and include Leydig cell tumors, Sertoli cell tumors, and lymphomas. These tumors can have a variety of clinical behaviors, ranging from benign to malignant.
Testicular neoplasms often present as a painless mass or swelling in the testicle. Other symptoms may include a feeling of heaviness or discomfort in the scrotum, a dull ache in the lower abdomen or groin, and breast enlargement (gynecomastia).
Diagnosis typically involves a physical examination, imaging studies such as ultrasound or CT scan, and blood tests to detect tumor markers. Treatment options depend on the type and stage of the neoplasm but may include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular self-examinations of the testicles are recommended for early detection and improved outcomes.
Neoplasms are abnormal growths of cells or tissues that serve no purpose and can be benign (non-cancerous) or malignant (cancerous). Glandular and epithelial neoplasms refer to specific types of tumors that originate from the glandular and epithelial tissues, respectively.
Glandular neoplasms arise from the glandular tissue, which is responsible for producing and secreting substances such as hormones, enzymes, or other fluids. These neoplasms can be further classified into adenomas (benign) and adenocarcinomas (malignant).
Epithelial neoplasms, on the other hand, develop from the epithelial tissue that lines the outer surfaces of organs and the inner surfaces of cavities. These neoplasms can also be benign or malignant and are classified as papillomas (benign) and carcinomas (malignant).
It is important to note that while both glandular and epithelial neoplasms can become cancerous, not all of them do. However, if they do, the malignant versions can invade surrounding tissues and spread to other parts of the body, making them potentially life-threatening.
Neoplasm staging is a systematic process used in medicine to describe the extent of spread of a cancer, including the size and location of the original (primary) tumor and whether it has metastasized (spread) to other parts of the body. The most widely accepted system for this purpose is the TNM classification system developed by the American Joint Committee on Cancer (AJCC) and the Union for International Cancer Control (UICC).
In this system, T stands for tumor, and it describes the size and extent of the primary tumor. N stands for nodes, and it indicates whether the cancer has spread to nearby lymph nodes. M stands for metastasis, and it shows whether the cancer has spread to distant parts of the body.
Each letter is followed by a number that provides more details about the extent of the disease. For example, a T1N0M0 cancer means that the primary tumor is small and has not spread to nearby lymph nodes or distant sites. The higher the numbers, the more advanced the cancer.
Staging helps doctors determine the most appropriate treatment for each patient and estimate the patient's prognosis. It is an essential tool for communication among members of the healthcare team and for comparing outcomes of treatments in clinical trials.
Soft tissue neoplasms refer to abnormal growths or tumors that develop in the soft tissues of the body. Soft tissues include muscles, tendons, ligaments, fascia, nerves, blood vessels, fat, and synovial membranes (the thin layer of cells that line joints and tendons). Neoplasms can be benign (non-cancerous) or malignant (cancerous), and their behavior and potential for spread depend on the specific type of neoplasm.
Benign soft tissue neoplasms are typically slow-growing, well-circumscribed, and rarely spread to other parts of the body. They can often be removed surgically with a low risk of recurrence. Examples of benign soft tissue neoplasms include lipomas (fat tumors), schwannomas (nerve sheath tumors), and hemangiomas (blood vessel tumors).
Malignant soft tissue neoplasms, on the other hand, can grow rapidly, invade surrounding tissues, and may metastasize (spread) to distant parts of the body. They are often more difficult to treat than benign neoplasms and require a multidisciplinary approach, including surgery, radiation therapy, and chemotherapy. Examples of malignant soft tissue neoplasms include sarcomas, such as rhabdomyosarcoma (arising from skeletal muscle), leiomyosarcoma (arising from smooth muscle), and angiosarcoma (arising from blood vessels).
It is important to note that soft tissue neoplasms can occur in any part of the body, and their diagnosis and treatment require a thorough evaluation by a healthcare professional with expertise in this area.
Intestinal neoplasms refer to abnormal growths in the tissues of the intestines, which can be benign or malignant. These growths are called neoplasms and they result from uncontrolled cell division. In the case of intestinal neoplasms, these growths occur in the small intestine, large intestine (colon), rectum, or appendix.
Benign intestinal neoplasms are not cancerous and often do not invade surrounding tissues or spread to other parts of the body. However, they can still cause problems if they grow large enough to obstruct the intestines or cause bleeding. Common types of benign intestinal neoplasms include polyps, leiomyomas, and lipomas.
Malignant intestinal neoplasms, on the other hand, are cancerous and can invade surrounding tissues and spread to other parts of the body. The most common type of malignant intestinal neoplasm is adenocarcinoma, which arises from the glandular cells lining the inside of the intestines. Other types of malignant intestinal neoplasms include lymphomas, sarcomas, and carcinoid tumors.
Symptoms of intestinal neoplasms can vary depending on their size, location, and type. Common symptoms include abdominal pain, bloating, changes in bowel habits, rectal bleeding, weight loss, and fatigue. If you experience any of these symptoms, it is important to seek medical attention promptly.
Mucinous cystadenocarcinoma is a type of cancer that arises from the mucin-producing cells in the lining of a cyst. It is a subtype of cystadenocarcinoma, which is a malignant tumor that develops within a cyst. Mucinous cystadenocarcinomas are typically found in the ovary or pancreas but can also occur in other organs such as the appendix and the respiratory tract.
These tumors are characterized by the production of large amounts of mucin, a gel-like substance that can accumulate within the cyst and cause it to grow. Mucinous cystadenocarcinomas tend to grow slowly but can become quite large and may eventually spread (metastasize) to other parts of the body if left untreated.
Symptoms of mucinous cystadenocarcinoma depend on the location and size of the tumor, but they may include abdominal pain or discomfort, bloating, changes in bowel movements, or vaginal bleeding. Treatment typically involves surgical removal of the tumor, followed by chemotherapy or radiation therapy to kill any remaining cancer cells. The prognosis for mucinous cystadenocarcinoma depends on several factors, including the stage of the disease at diagnosis and the patient's overall health.
Hematologic neoplasms, also known as hematological malignancies, are a group of diseases characterized by the uncontrolled growth and accumulation of abnormal blood cells or bone marrow cells. These disorders can originate from the myeloid or lymphoid cell lines, which give rise to various types of blood cells, including red blood cells, white blood cells, and platelets.
Hematologic neoplasms can be broadly classified into three categories:
1. Leukemias: These are cancers that primarily affect the bone marrow and blood-forming tissues. They result in an overproduction of abnormal white blood cells, which interfere with the normal functioning of the blood and immune system. There are several types of leukemia, including acute lymphoblastic leukemia (ALL), chronic lymphocytic leukemia (CLL), acute myeloid leukemia (AML), and chronic myeloid leukemia (CML).
2. Lymphomas: These are cancers that develop from the lymphatic system, which is a part of the immune system responsible for fighting infections. Lymphomas can affect lymph nodes, spleen, bone marrow, and other organs. The two main types of lymphoma are Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL).
3. Myelomas: These are cancers that arise from the plasma cells, a type of white blood cell responsible for producing antibodies. Multiple myeloma is the most common type of myeloma, characterized by an excessive proliferation of malignant plasma cells in the bone marrow, leading to the production of abnormal amounts of monoclonal immunoglobulins (M proteins) and bone destruction.
Hematologic neoplasms can have various symptoms, such as fatigue, weakness, frequent infections, easy bruising or bleeding, weight loss, swollen lymph nodes, and bone pain. The diagnosis typically involves a combination of medical history, physical examination, laboratory tests, imaging studies, and sometimes bone marrow biopsy. Treatment options depend on the type and stage of the disease and may include chemotherapy, radiation therapy, targeted therapy, immunotherapy, stem cell transplantation, or a combination of these approaches.
A neoplasm is a tumor or growth that is formed by an abnormal and excessive proliferation of cells, which can be benign or malignant. Neoplasm proteins are therefore any proteins that are expressed or produced in these neoplastic cells. These proteins can play various roles in the development, progression, and maintenance of neoplasms.
Some neoplasm proteins may contribute to the uncontrolled cell growth and division seen in cancer, such as oncogenic proteins that promote cell cycle progression or inhibit apoptosis (programmed cell death). Others may help the neoplastic cells evade the immune system, allowing them to proliferate undetected. Still others may be involved in angiogenesis, the formation of new blood vessels that supply the tumor with nutrients and oxygen.
Neoplasm proteins can also serve as biomarkers for cancer diagnosis, prognosis, or treatment response. For example, the presence or level of certain neoplasm proteins in biological samples such as blood or tissue may indicate the presence of a specific type of cancer, help predict the likelihood of cancer recurrence, or suggest whether a particular therapy will be effective.
Overall, understanding the roles and behaviors of neoplasm proteins can provide valuable insights into the biology of cancer and inform the development of new diagnostic and therapeutic strategies.
Lymphoma is a type of cancer that originates from the white blood cells called lymphocytes, which are part of the immune system. These cells are found in various parts of the body such as the lymph nodes, spleen, bone marrow, and other organs. Lymphoma can be classified into two main types: Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL).
HL is characterized by the presence of a specific type of abnormal lymphocyte called Reed-Sternberg cells, while NHL includes a diverse group of lymphomas that lack these cells. The symptoms of lymphoma may include swollen lymph nodes, fever, night sweats, weight loss, and fatigue.
The exact cause of lymphoma is not known, but it is believed to result from genetic mutations in the lymphocytes that lead to uncontrolled cell growth and division. Exposure to certain viruses, chemicals, and radiation may increase the risk of developing lymphoma. Treatment options for lymphoma depend on various factors such as the type and stage of the disease, age, and overall health of the patient. Common treatments include chemotherapy, radiation therapy, immunotherapy, and stem cell transplantation.
Vascular neoplasms are a type of tumor that develops from cells that line the blood vessels or lymphatic vessels. These tumors can be benign (non-cancerous) or malignant (cancerous). Benign vascular neoplasms, such as hemangiomas and lymphangiomas, are usually harmless and may not require treatment unless they cause symptoms or complications. Malignant vascular neoplasms, on the other hand, are known as angiosarcomas and can be aggressive, spreading to other parts of the body and potentially causing serious health problems.
Angiosarcomas can develop in any part of the body but are most commonly found in the skin, particularly in areas exposed to radiation or chronic lymph edema. They can also occur in the breast, liver, spleen, and heart. Treatment for vascular neoplasms depends on the type, location, size, and stage of the tumor, as well as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Bone neoplasms are abnormal growths or tumors that develop in the bone. They can be benign (non-cancerous) or malignant (cancerous). Benign bone neoplasms do not spread to other parts of the body and are rarely a threat to life, although they may cause problems if they grow large enough to press on surrounding tissues or cause fractures. Malignant bone neoplasms, on the other hand, can invade and destroy nearby tissue and may spread (metastasize) to other parts of the body.
There are many different types of bone neoplasms, including:
1. Osteochondroma - a benign tumor that develops from cartilage and bone
2. Enchondroma - a benign tumor that forms in the cartilage that lines the inside of the bones
3. Chondrosarcoma - a malignant tumor that develops from cartilage
4. Osteosarcoma - a malignant tumor that develops from bone cells
5. Ewing sarcoma - a malignant tumor that develops in the bones or soft tissues around the bones
6. Giant cell tumor of bone - a benign or occasionally malignant tumor that develops from bone tissue
7. Fibrosarcoma - a malignant tumor that develops from fibrous tissue in the bone
The symptoms of bone neoplasms vary depending on the type, size, and location of the tumor. They may include pain, swelling, stiffness, fractures, or limited mobility. Treatment options depend on the type and stage of the tumor but may include surgery, radiation therapy, chemotherapy, or a combination of these treatments.
There is no medical definition for "dog diseases" as it is too broad a term. However, dogs can suffer from various health conditions and illnesses that are specific to their species or similar to those found in humans. Some common categories of dog diseases include:
1. Infectious Diseases: These are caused by viruses, bacteria, fungi, or parasites. Examples include distemper, parvovirus, kennel cough, Lyme disease, and heartworms.
2. Hereditary/Genetic Disorders: Some dogs may inherit certain genetic disorders from their parents. Examples include hip dysplasia, elbow dysplasia, progressive retinal atrophy (PRA), and degenerative myelopathy.
3. Age-Related Diseases: As dogs age, they become more susceptible to various health issues. Common age-related diseases in dogs include arthritis, dental disease, cancer, and cognitive dysfunction syndrome (CDS).
4. Nutritional Disorders: Malnutrition or improper feeding can lead to various health problems in dogs. Examples include obesity, malnutrition, and vitamin deficiencies.
5. Environmental Diseases: These are caused by exposure to environmental factors such as toxins, allergens, or extreme temperatures. Examples include heatstroke, frostbite, and toxicities from ingesting harmful substances.
6. Neurological Disorders: Dogs can suffer from various neurological conditions that affect their nervous system. Examples include epilepsy, intervertebral disc disease (IVDD), and vestibular disease.
7. Behavioral Disorders: Some dogs may develop behavioral issues due to various factors such as anxiety, fear, or aggression. Examples include separation anxiety, noise phobias, and resource guarding.
It's important to note that regular veterinary care, proper nutrition, exercise, and preventative measures can help reduce the risk of many dog diseases.
Neoplasms, adnexal and skin appendage refer to abnormal growths or tumors that develop in the sweat glands, hair follicles, or other structures associated with the skin. These growths can be benign (non-cancerous) or malignant (cancerous), and they can occur anywhere on the body.
Adnexal neoplasms are tumors that arise from the sweat glands or hair follicles, including the sebaceous glands, eccrine glands, and apocrine glands. These tumors can range in size and severity, and they may cause symptoms such as pain, itching, or changes in the appearance of the skin.
Skin appendage neoplasms are similar to adnexal neoplasms, but they specifically refer to tumors that arise from structures such as hair follicles, nails, and sweat glands. Examples of skin appendage neoplasms include pilomatricomas (tumors of the hair follicle), trichilemmomas (tumors of the outer root sheath of the hair follicle), and sebaceous adenomas (tumors of the sebaceous glands).
It is important to note that while many adnexal and skin appendage neoplasms are benign, some can be malignant and may require aggressive treatment. If you notice any unusual growths or changes in your skin, it is important to consult with a healthcare professional for further evaluation and care.
Sweat gland neoplasms are abnormal growths that develop in the sweat glands. These growths can be benign (noncancerous) or malignant (cancerous). Benign sweat gland neoplasms include hidradenomas and syringomas, which are usually slow-growing and cause little to no symptoms. Malignant sweat gland neoplasms, also known as sweat gland carcinomas, are rare but aggressive cancers that can spread to other parts of the body. They may cause symptoms such as a lump or mass under the skin, pain, swelling, and redness. Treatment typically involves surgical removal of the growth.
Palatal neoplasms refer to abnormal growths or tumors that occur on the palate, which is the roof of the mouth. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slower growing and less likely to spread, while malignant neoplasms are more aggressive and can invade nearby tissues and organs.
Palatal neoplasms can have various causes, including genetic factors, environmental exposures, and viral infections. They may present with symptoms such as mouth pain, difficulty swallowing, swelling or lumps in the mouth, bleeding, or numbness in the mouth or face.
The diagnosis of palatal neoplasms typically involves a thorough clinical examination, imaging studies, and sometimes biopsy to determine the type and extent of the growth. Treatment options depend on the type, size, location, and stage of the neoplasm but may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or spread of the neoplasm.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
Neoplasms are abnormal growths of cells or tissues in the body that can be benign (non-cancerous) or malignant (cancerous). When referring to "Complex and Mixed Neoplasms," it is typically used in the context of histopathology, where it describes tumors with a mixture of different types of cells or growth patterns.
A complex neoplasm usually contains areas with various architectural patterns, cell types, or both, making its classification challenging. It may require extensive sampling and careful examination to determine its nature and behavior. These neoplasms can be either benign or malignant, depending on the specific characteristics of the tumor cells and their growth pattern.
A mixed neoplasm, on the other hand, is a tumor that contains more than one type of cell or tissue component, often arising from different germ layers (the three primary layers of embryonic development: ectoderm, mesoderm, and endoderm). A common example of a mixed neoplasm is a teratoma, which can contain tissues derived from all three germ layers, such as skin, hair, teeth, bone, and muscle. Mixed neoplasms can also be benign or malignant, depending on the specific components of the tumor.
It's important to note that the classification and behavior of complex and mixed neoplasms can vary significantly based on their location in the body, cellular composition, and other factors. Accurate diagnosis typically requires a thorough examination by an experienced pathologist and may involve additional tests, such as immunohistochemistry or molecular analysis, to determine the appropriate treatment and management strategies.
Mandibular neoplasms refer to abnormal growths or tumors that develop in the mandible, which is the lower jawbone. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow-growing and rarely spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and may metastasize (spread) to distant sites.
Mandibular neoplasms can have various causes, including genetic mutations, exposure to certain chemicals or radiation, and infection with certain viruses. The symptoms of mandibular neoplasms may include swelling or pain in the jaw, difficulty chewing or speaking, numbness in the lower lip or chin, loose teeth, and/or a lump or mass in the mouth or neck.
The diagnosis of mandibular neoplasms typically involves a thorough clinical examination, imaging studies such as X-rays, CT scans, or MRI scans, and sometimes a biopsy to confirm the type and extent of the tumor. Treatment options depend on the type, stage, and location of the neoplasm, and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or metastasis.
Neoplasm antigens, also known as tumor antigens, are substances that are produced by cancer cells (neoplasms) and can stimulate an immune response. These antigens can be proteins, carbohydrates, or other molecules that are either unique to the cancer cells or are overexpressed or mutated versions of normal cellular proteins.
Neoplasm antigens can be classified into two main categories: tumor-specific antigens (TSAs) and tumor-associated antigens (TAAs). TSAs are unique to cancer cells and are not expressed by normal cells, while TAAs are present at low levels in normal cells but are overexpressed or altered in cancer cells.
TSAs can be further divided into viral antigens and mutated antigens. Viral antigens are produced when cancer is caused by a virus, such as human papillomavirus (HPV) in cervical cancer. Mutated antigens are the result of genetic mutations that occur during cancer development and are unique to each patient's tumor.
Neoplasm antigens play an important role in the immune response against cancer. They can be recognized by the immune system, leading to the activation of immune cells such as T cells and natural killer (NK) cells, which can then attack and destroy cancer cells. However, cancer cells often develop mechanisms to evade the immune response, allowing them to continue growing and spreading.
Understanding neoplasm antigens is important for the development of cancer immunotherapies, which aim to enhance the body's natural immune response against cancer. These therapies include checkpoint inhibitors, which block proteins that inhibit T cell activation, and therapeutic vaccines, which stimulate an immune response against specific tumor antigens.
Cystadenocarcinoma is a type of tumor that arises from the epithelial lining of a cyst, and it has the potential to invade surrounding tissues and spread (metastasize) to other parts of the body. It typically affects glandular organs such as the ovaries, pancreas, and salivary glands.
Cystadenocarcinomas can be classified into two types: serous and mucinous. Serous cystadenocarcinomas produce a watery fluid, while mucinous cystadenocarcinomas produce a thick, mucus-like fluid. Both types of tumors can be benign or malignant, but malignant cystadenocarcinomas are more aggressive and have a higher risk of metastasis.
Symptoms of cystadenocarcinoma depend on the location and size of the tumor. In some cases, there may be no symptoms until the tumor has grown large enough to cause pain or other problems. Treatment typically involves surgical removal of the tumor, along with any affected surrounding tissue. Chemotherapy and radiation therapy may also be used in some cases to help prevent recurrence or spread of the cancer.
Bile duct neoplasms, also known as cholangiocarcinomas, refer to a group of malignancies that arise from the bile ducts. These are the tubes that carry bile from the liver to the gallbladder and small intestine. Bile duct neoplasms can be further classified based on their location as intrahepatic (within the liver), perihilar (at the junction of the left and right hepatic ducts), or distal (in the common bile duct).
These tumors are relatively rare, but their incidence has been increasing in recent years. They can cause a variety of symptoms, including jaundice, abdominal pain, weight loss, and fever. The diagnosis of bile duct neoplasms typically involves imaging studies such as CT or MRI scans, as well as blood tests to assess liver function. In some cases, a biopsy may be necessary to confirm the diagnosis.
Treatment options for bile duct neoplasms depend on several factors, including the location and stage of the tumor, as well as the patient's overall health. Surgical resection is the preferred treatment for early-stage tumors, while chemotherapy and radiation therapy may be used in more advanced cases. For patients who are not candidates for surgery, palliative treatments such as stenting or bypass procedures may be recommended to relieve symptoms and improve quality of life.
Neoplasm invasiveness is a term used in pathology and oncology to describe the aggressive behavior of cancer cells as they invade surrounding tissues and organs. This process involves the loss of cell-to-cell adhesion, increased motility and migration, and the ability of cancer cells to degrade the extracellular matrix (ECM) through the production of enzymes such as matrix metalloproteinases (MMPs).
Invasive neoplasms are cancers that have spread beyond the original site where they first developed and have infiltrated adjacent tissues or structures. This is in contrast to non-invasive or in situ neoplasms, which are confined to the epithelial layer where they originated and have not yet invaded the underlying basement membrane.
The invasiveness of a neoplasm is an important prognostic factor in cancer diagnosis and treatment, as it can indicate the likelihood of metastasis and the potential effectiveness of various therapies. In general, more invasive cancers are associated with worse outcomes and require more aggressive treatment approaches.
Female condoms are a form of barrier contraception that provides protection against sexually transmitted infections (STIs) and pregnancy. They are made of soft, flexible nitrile rubber sheath that is inserted into the vagina before sexual intercourse. The closed end of the sheath covers the cervix, while the open end remains outside the vagina, covering the labia.
The female condom works by providing a physical barrier that prevents semen from entering the vagina and coming into contact with the cervix and internal reproductive organs. This helps to prevent pregnancy and also reduces the risk of STI transmission by preventing direct genital-to-genital contact.
Female condoms are an important option for individuals who cannot or do not wish to use male condoms, as they offer similar protection against STIs and pregnancy. They can be inserted up to eight hours before sexual intercourse, providing greater spontaneity and convenience compared to male condoms. Additionally, female condoms may be used during anal sex to reduce the risk of STI transmission.
It is important to note that female condoms should not be used in conjunction with male condoms, as this can increase friction and cause either condom to break or slip off. Proper use and handling of female condoms are essential for ensuring their effectiveness and preventing accidental pregnancy or STI transmission.
Heart neoplasms are abnormal growths or tumors that develop within the heart tissue. They can be benign (noncancerous) or malignant (cancerous). Benign tumors, such as myxomas and rhabdomyomas, are typically slower growing and less likely to spread, but they can still cause serious complications if they obstruct blood flow or damage heart valves. Malignant tumors, such as angiosarcomas and rhabdomyosarcomas, are fast-growing and have a higher risk of spreading to other parts of the body. Symptoms of heart neoplasms can include shortness of breath, chest pain, fatigue, and irregular heart rhythms. Treatment options depend on the type, size, and location of the tumor, and may include surgery, radiation therapy, or chemotherapy.
Colonic neoplasms refer to abnormal growths in the large intestine, also known as the colon. These growths can be benign (non-cancerous) or malignant (cancerous). The two most common types of colonic neoplasms are adenomas and carcinomas.
Adenomas are benign tumors that can develop into cancer over time if left untreated. They are often found during routine colonoscopies and can be removed during the procedure.
Carcinomas, on the other hand, are malignant tumors that invade surrounding tissues and can spread to other parts of the body. Colorectal cancer is the third leading cause of cancer-related deaths in the United States, and colonic neoplasms are a significant risk factor for developing this type of cancer.
Regular screenings for colonic neoplasms are recommended for individuals over the age of 50 or those with a family history of colorectal cancer or other risk factors. Early detection and removal of colonic neoplasms can significantly reduce the risk of developing colorectal cancer.
Splenic neoplasms refer to abnormal growths or tumors in the spleen, which can be benign (non-cancerous) or malignant (cancerous). These growths can arise from various cell types present within the spleen, including hematopoietic cells (red and white blood cells, platelets), stromal cells (supporting tissue), or lymphoid cells (part of the immune system).
There are several types of splenic neoplasms:
1. Hematologic malignancies: These are cancers that affect the blood and bone marrow, such as leukemias, lymphomas, and multiple myeloma. They often involve the spleen, causing enlargement (splenomegaly) and neoplastic infiltration of splenic tissue.
2. Primary splenic tumors: These are rare and include benign lesions like hemangiomas, lymphangiomas, and hamartomas, as well as malignant tumors such as angiosarcoma, littoral cell angiosarcoma, and primary splenic lymphoma.
3. Metastatic splenic tumors: These occur when cancer cells from other primary sites spread (metastasize) to the spleen. Common sources of metastasis include lung, breast, colon, and ovarian cancers, as well as melanomas and sarcomas.
Symptoms of splenic neoplasms may vary depending on the type and extent of the disease but often include abdominal pain or discomfort, fatigue, weight loss, and anemia. Diagnosis typically involves imaging studies (such as ultrasound, CT, or MRI scans) and sometimes requires a biopsy for confirmation. Treatment options depend on the type of neoplasm and may include surgery, chemotherapy, radiation therapy, targeted therapy, or immunotherapy.
Tumor markers are substances that can be found in the body and their presence can indicate the presence of certain types of cancer or other conditions. Biological tumor markers refer to those substances that are produced by cancer cells or by other cells in response to cancer or certain benign (non-cancerous) conditions. These markers can be found in various bodily fluids such as blood, urine, or tissue samples.
Examples of biological tumor markers include:
1. Proteins: Some tumor markers are proteins that are produced by cancer cells or by other cells in response to the presence of cancer. For example, prostate-specific antigen (PSA) is a protein produced by normal prostate cells and in higher amounts by prostate cancer cells.
2. Genetic material: Tumor markers can also include genetic material such as DNA, RNA, or microRNA that are shed by cancer cells into bodily fluids. For example, circulating tumor DNA (ctDNA) is genetic material from cancer cells that can be found in the bloodstream.
3. Metabolites: Tumor markers can also include metabolic products produced by cancer cells or by other cells in response to cancer. For example, lactate dehydrogenase (LDH) is an enzyme that is released into the bloodstream when cancer cells break down glucose for energy.
It's important to note that tumor markers are not specific to cancer and can be elevated in non-cancerous conditions as well. Therefore, they should not be used alone to diagnose cancer but rather as a tool in conjunction with other diagnostic tests and clinical evaluations.
Maxillary neoplasms refer to abnormal growths or tumors in the maxilla, which is the upper jaw bone. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are slow-growing and do not spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and spread to distant sites.
Maxillary neoplasms can cause various symptoms such as swelling, pain, numbness, loose teeth, or difficulty in chewing or swallowing. They may also cause nasal congestion, nosebleeds, or visual changes if they affect the eye or orbit. The diagnosis of maxillary neoplasms usually involves a combination of clinical examination, imaging studies such as CT or MRI scans, and biopsy to determine the type and extent of the tumor.
Treatment options for maxillary neoplasms depend on several factors, including the type, size, location, and stage of the tumor, as well as the patient's overall health and preferences. Treatment may include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular follow-up care is essential to monitor for recurrence or metastasis and ensure optimal outcomes.
Thymus neoplasms are abnormal growths in the thymus gland that result from uncontrolled cell division. The term "neoplasm" refers to any new and abnormal growth of tissue, also known as a tumor. Thymus neoplasms can be benign or malignant (cancerous).
Malignant thymus neoplasms are called thymomas or thymic carcinomas. Thymomas are the most common type and tend to grow slowly, invading nearby tissues and organs. They can also spread (metastasize) to other parts of the body. Thymic carcinomas are rarer and more aggressive, growing and spreading more quickly than thymomas.
Symptoms of thymus neoplasms may include coughing, chest pain, difficulty breathing, or swelling in the neck or upper chest. Treatment options for thymus neoplasms depend on the type, size, location, and stage of the tumor, as well as the patient's overall health. Treatment may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
A serous cystadenoma is a type of benign tumor that arises from the epithelial cells lining the serous glands, which are glands that produce a watery, lubricating fluid. This type of tumor typically develops in the ovary or the pancreas.
Serous cystadenomas of the ovary are usually filled with a clear, watery fluid and have multiple loculations (compartments). They can vary in size from a few millimeters to several centimeters in diameter. Although these tumors are benign, they can cause symptoms if they become large enough to press on surrounding organs or if they rupture and release their contents into the abdominal cavity.
Serous cystadenomas of the pancreas are less common than ovarian serous cystadenomas. They typically occur in the tail of the pancreas and can range in size from a few millimeters to several centimeters in diameter. These tumors are usually asymptomatic, but they can cause symptoms such as abdominal pain or discomfort if they become large enough to press on surrounding organs.
It is important to note that while serous cystadenomas are generally benign, there is a small risk that they may undergo malignant transformation and develop into a type of cancer known as a serous cystadenocarcinoma. For this reason, it is important for patients with these tumors to be followed closely by a healthcare provider and to have regular imaging studies and/or surgical excision to monitor for any changes in the tumor.
Anal gland neoplasms, also known as anal sac tumors, are abnormal growths that develop from the cells lining the anal glands. These glands are located on either side of the anus in dogs and some other animals, and they produce a scent used for marking territory.
Anal gland neoplasms can be benign or malignant (cancerous). Malignant tumors are more common and tend to grow quickly, invading surrounding tissues and spreading to other parts of the body (metastasis). Common symptoms of anal gland neoplasms include straining to defecate, bleeding from the rectum, and a firm mass that can be felt near the anus.
Treatment for anal gland neoplasms typically involves surgical removal of the tumor. In some cases, radiation therapy or chemotherapy may also be recommended. The prognosis for animals with anal gland neoplasms depends on several factors, including the size and location of the tumor, whether it has spread to other parts of the body, and the overall health of the animal.