Glomerulonephritis, Membranoproliferative
Glomerulonephritis
Complement C3 Nephritic Factor
Kidney Glomerulus
Glomerulonephritis, Membranous
Cryoglobulinemia
Nephrotic Syndrome
Glomerulonephritis, IGA
Complement C3
Cryoglobulins
Immune Complex Diseases
Biopsy
Complement Factor H
Properdin
Glomerulosclerosis, Focal Segmental
Kidney
Glomerular Basement Membrane
Complement System Proteins
Nephrosis, Lipoid
Complement Pathway, Alternative
Antigen-Antibody Complex
Anti-Glomerular Basement Membrane Disease
Nephritis, Interstitial
Hepatitis C
Hemolytic-Uremic Syndrome
Immunoglobulin G
Fluorescent Antibody Technique
Antibodies, Antineutrophil Cytoplasmic
Lupus Nephritis
Glomerular Mesangium
Immunosuppressive Agents
Microscopy, Electron
Basement Membrane
Hepacivirus
Vasculitis
Retrospective Studies
Autoantibodies
Serum Sickness
Blocking angiotensin II ameliorates proteinuria and glomerular lesions in progressive mesangioproliferative glomerulonephritis. (1/338)
BACKGROUND: The renin-angiotensin system is thought to be involved in the progression of glomerulonephritis (GN) into end-stage renal failure (ESRF) because of the observed renoprotective effects of angiotensin-converting enzyme inhibitors (ACEIs). However, ACEIs have pharmacological effects other than ACE inhibition that may help lower blood pressure and preserve glomerular structure. We previously reported a new animal model of progressive glomerulosclerosis induced by a single intravenous injection of an anti-Thy-1 monoclonal antibody, MoAb 1-22-3, in uninephrectomized rats. Using this new model of progressive GN, we examined the hypothesis that ACEIs prevent the progression to ESRF by modulating the effects of angiotensin II (Ang II) on the production of transforming growth factor-beta (TGF-beta) and extracellular matrix components. METHODS: We studied the effect of an ACEI (cilazapril) and an Ang II type 1 receptor antagonist (candesartan) on the clinical features and morphological lesions in the rat model previously reported. After 10 weeks of treatment with equihypotensive doses of cilazapril, cilazapril plus Hoe 140 (a bradykinin receptor B2 antagonist), candesartan, and hydralazine, we examined systolic blood pressure, urinary protein excretion, creatinine clearance, the glomerulosclerosis index, and the tubulointerstitial lesion index. We performed a semiquantitative evaluation of glomerular immunostaining for TGF-beta and collagen types I and III by immunofluorescence study and of these cortical mRNA levels by Northern blot analysis. RESULTS: Untreated rats developed massive proteinuria, renal dysfunction, and severe glomerular and tubulointerstitial injury, whereas uninephrectomized control rats did not. There was a significant increase in the levels of glomerular protein and cortical mRNA for TGF-beta and collagen types I and III in untreated rats. Cilazapril and candesartan prevented massive proteinuria, increased creatinine clearance, and ameliorated glomerular and tubulointerstitial injury. These drugs also reduced levels of glomerular protein and cortical mRNA for TGF-beta and collagen types I and III. Hoe 140 failed to blunt the renoprotective effect of cilazapril. Hydralazine did not exhibit a renoprotective effect. CONCLUSION: These results indicate that ACEIs prevent the progression to ESRF by modulating the effects of Ang II via Ang II type 1 receptor on the production of TGF-beta and collagen types I and III, as well as on intrarenal hemodynamics, but not by either increasing bradykinin activity or reducing blood pressure in this rat model of mesangial proliferative GN. (+info)Lysophosphatidic acid and mesangial cells: implications for renal diseases. (2/338)
The last decade has witnessed a phenomenal increase in our understanding of the biological role of lysophosphatidic acid (LPA) and has led to an appreciation of this critical serum-derived growth factor released from platelets. We herein summarize recent observations that collectively support the hypothesis that LPA may play a key role in the pathogenesis of initiation and progression of proliferative glomerulonephritis. LPA synergistically stimulates mesangial cell proliferation in combination with platelet-derived growth factor in primary culture. The mechanism of co-mitogenesis is likely to be mediated by the prolonged activation of mitogen-activated protein kinase which is stimulated by platelet-derived growth factor and LPA through different mechanisms. LPA contracts cultured mesangial cells and has properties in common with other pressor molecules including mobilization of intracellular Ca2+ and promotion of Ca2+ entry through dihydropyridine-sensitive calcium channels. LPA receptor mRNA has been identified in isolated glomeruli dissected from renal biopsy samples of patients with IgA nephropathy. All of these facts have led us to postulate that LPA is produced within glomeruli and that LPA's mitogenic as well as haemodynamic action contribute to the pathological process of mesangial proliferative glomerulonephritis. The possible production of LPA as an autocrine factor from mesangial cells themselves has also been discussed. (+info)Detection of urinary macrophages expressing the CD16 (Fc gamma RIII) molecule: a novel marker of acute inflammatory glomerular injury. (3/338)
BACKGROUND: The CD16 antigen is the Fc gamma receptor III. CD14+CD16+ cells are proinflammatory monocytes/macrophages (Mo/M phi) that constitute a minor population in the peripheral blood of healthy individuals. Little is known about the expression of CD16 antigen on Mo/M phi in glomerulonephritis. METHODS: Flow cytometric analyses were performed on urine and blood samples obtained from 209 patients with various renal diseases. Patients variously suffered from rapidly progressive crescentic glomerulonephritis (RPGN), membranoproliferative glomerulonephritis (MPGN), postinfectious acute glomerulonephritis (AGN), Henoch-Schonlein purpura nephritis (HSPN), IgA nephropathy (IgAN), membranous nephropathy (MN), minimal change nephrotic syndrome (MCNS), lupus nephritis (LN), acute interstitial nephritis, hereditary nephropathy, idiopathic renal hematuria (IRH), and renal stone. RESULTS: The CD16+ M phi population of cells was present in the urine of hematuria-positive patients with proliferative glomerulonephritis, including AGN, IgAN, RPGN, MPGN, and LN with acute inflammatory lesions, such as endocapillary proliferation, tuft necrosis, and cellular crescents. In contrast, the urinary CD16+ M phi population was negligible in hematuria-positive patients with nonproliferative renal disease, including hereditary nephropathy, IRH, and renal stone and also in patients with proliferative glomerulonephritis lacking acute inflammatory lesions. Total urinary M phi of these patients were much less than those of patients having proliferative glomerulonephritis with acute inflammatory lesions. Transient expansion of the CD16+ M phi population in urine was observed during the acute exacerbation of urinary abnormalities, whereas the disappearance of CD16+ M phi closely preceded the amelioration of urinary abnormalities in patients with proliferative glomerulonephritis. In 38 of the 98 patients positive for CD16+ M phi population in urine, the CD16+ Mo population was negligible in peripheral blood. Immunohistochemically, CD16+ M phi were present in the glomeruli of active proliferative glomerulonephritis, whereas such cells were absent in inactive proliferative glomerulonephritis or nonproliferative glomerular diseases. CONCLUSION: CD16+ M phi may be effector cells involved in the acute inflammation common to all types of proliferative glomerulonephritis. Furthermore, the detection of CD16+ M phi in urine, as well as urinary M phi counts, may serve as a useful indicator of the active stage of proliferative glomerulonephritis. (+info)Thrombospondin peptides are potent inhibitors of mesangial and glomerular endothelial cell proliferation in vitro and in vivo. (4/338)
BACKGROUND: Thrombospondin 1 (TSP1), a multifunctional, matricellular glycoprotein, is expressed de novo in many inflammatory disease processes, including glomerular disease. Short peptide fragments derived from the type I properdin repeats of the TSP1 molecule mimic anti-angiogenic and/or transforming growth factor-beta (TGF-beta)-activating properties of the whole TSP1 glycoprotein. We investigated the effects of D-reverse peptides derived from the type I domain of TSP1 in experimental mesangial proliferative glomerulonephritis in the rat (anti-Thy1 model), as well as their effects on cultured mesangial and glomerular endothelial cells. METHODS: Effects of TSP peptides on proliferation of mesangial or glomerular endothelial cells in culture after growth arrest or growth factor stimulation (fibroblast growth factor-2, platelet-derived growth factor-BB, 10% fetal calf serum) were measured by [3H]thymidine incorporation assay. Adhesion of rat mesangial cells (MCs) to a TSP-peptide matrix was assayed using an attachment-hexosaminidase assay. TSP peptides were intraperitoneally injected daily in rats that had received an intravenous injection of polyclonal anti-Thy1 antibody to induce mesangial proliferative glomerulonephritis. On biopsies from days 2, 5, and 8 of anti-Thy1 disease, mesangial and glomerular endothelial proliferation, matrix expansion, mesangial activation, and microaneurysm formation were assessed. Functional parameters such as blood pressure and proteinuria were also measured. RESULTS: An 18-amino acid peptide (type I peptide) with anti-angiogenic and TGF-beta-activating sequences decreased mesangial and glomerular endothelial cell proliferation in vitro and in vivo and reduced microaneurysm formation and proteinuria in experimental glomerulonephritis. Analogues lacking the TGF-beta-activating sequence mimicked most effects of the type I peptide. The mechanism of action of these peptides may include antagonism of fibroblast growth factor-2 and alteration of MC adhesion. The TGF-beta-activating sequence alone did not have significant effects on mesangial or glomerular endothelial cells in vitro or in experimental kidney disease in vivo. CONCLUSION: Peptides from TSP1 may be promising therapeutics in treating glomerular disease with mesangial and endothelial cell injury. (+info)Role of intron 1 in smooth muscle alpha-actin transcriptional regulation in activated mesangial cells in vivo. (5/338)
BACKGROUND: The activation of glomerular mesangial cells is one of the early, important features of progressive glomerular disease. Smooth muscle alpha-actin (SMalphaA) is an excellent marker of activated mesangial cells. However, the mechanisms of SMalphaA regulation are only available from in vitro investigation. METHODS: We examined in vivo promoter analysis of the SMalphaA gene-utilizing transgenic mice harboring different promoter regions of the SMalphaA gene fused to chloramphenicol acetyl transferase (CAT). CAT activities were tested in primary cultured mesangial cells and in glomerular legions of Habu venom glomerulonephritis. RESULTS: The DNA sequence -891 to +3828, which contains exon 1, intron 1, and the first 14 bp of exon 2 in addition to the 5'-flanking sequence of the SMalphaA gene, induced high levels of transcription in activated mesangial cells in in vivo habu venom glomerulonephritis and in cultured mesangial cells derived from transgenic mice. The DNA region -891 to -124 was a positive element in mesangial cells derived from transgenic mice. Deletions (3316 or 137 bp) in intron 1 reduced transcription to undetectable levels. The 137 bp sequence is highly conserved among several species, containing one CArG box element, which is one of the key motifs for transcriptional activation of contractile-related proteins. In vitro transfection analysis failed to demonstrate these positive effects of intron 1 and region -891 to -124. Conclusions. In vivo promoter analysis of the SMalphaA gene provided new information about the transcriptional regulation of SMalphaA in activated mesangial cells. The DNA region -891 to -124 has a positive effect on SMalphaA transcription in cultured mesangial cells. The intron 1 region (+1088 to +1224) plays a pivotal role in SMalphaA transcription in activated mesangial cells in vivo. Further analysis of this conserved region in intron 1, including the CArG motif, will be of great value in understanding the molecular mechanisms of mesangial activation. (+info)Hepatitis C virus-associated glomerular disease in patients with human immunodeficiency virus coinfection. (6/338)
Chronic infection with hepatitis C virus (HCV) has been linked to the development of glomerular disease. HCV infection is highly prevalent among intravenous drug users, a population that is also at risk for HIV coinfection. This study reports the clinical-pathologic features and outcome of HCV-associated glomerular disease (HCV-GD) in 14 patients with HIV coinfection. All were intravenous drug users and all but one were African-Americans. Renal presentations included renal insufficiency, microscopic hematuria with active urine sediment, hypertension, and nephrotic syndrome or nephrotic-range proteinuria without hypercholesterolemia. Hypocomplementemia and cryoglobulinemia were present in 46 and 33% of patients, respectively. The predominant renal biopsy findings were membranoproliferative glomerulonephritis type 1 or type 3 (Burkholder subtype) in 79% of patients and membranous glomerulopathy with atypical features in 21% (including overlap with collapsing glomerulopathy in one patient). The clinical course was characterized by rapid progression to renal failure requiring dialysis. The overall morbidity and mortality were high with median time of 5.8 mo to dialysis or death. Although most patients died in renal failure, cause of death was primarily attributable to long-term immunosuppression and advanced AIDS. Patients with AIDS had shorter survival than those without (median survival time of 6.1 mo versus 45.9 mo, log-rank test P = 0.02). Only two patients were alive with stable renal function at follow-up of 28.5 mo. In patients with HCV-GD, coinfection with HIV leads to an aggressive form of renal disease that can be easily confused with HIV-associated nephropathy. Although hypocomplementemia, cryoglobulinemia, and more prominent hypertension and microscopic hematuria may provide clues to the presence of HCV-GD, renal biopsy is essential to differentiate HCV-GD from HIV-associated nephropathy. (+info)Hyperimmunoglobulin E syndrome associated with nephrotic syndrome. (7/338)
A 21-year-old man was admitted to Kure National Hospital with nephrotic syndrome in September 1996. He had suffered from an intractable pruritic skin rash and recurrent subcutaneous abscesses caused by the hyperimmunoglobulin E syndrome since the age of 18 months. Renal biopsy gave a diagnosis of membranoproliferative glomerulonephritis. Steroid therapy decreased urinary protein loss and hypoproteinemia, and his pruritic skin rash was improved. Patients with hyperimmunoglobulin E syndrome have a defective immune response, especially to Staphylococcus aureus infection. Continuous antigen stimulation may have caused this patient's renal histological damage as in immune complex glomerulonephritis. (+info)Prediction in idiopathic membranous nephropathy. (8/338)
BACKGROUND: Results of the prognosis of idiopathic membranous nephropathy are conflictive and prevent an effective risk stratification. These conflicts are explained in part by insufficient consideration of methodological principles for prognostic research. This cohort study is aimed at identifying clinical predictors for risk stratification while paying particular attention to methodology. METHODS: We studied 120 patients with idiopathic membranous nephropathy. Baseline data were extracted at the time of diagnostic renal biopsy, and patients were followed prospectively. Predictors were identified for the end points end-stage renal failure (ESRF) and ESRF or death. RESULTS: From the 120 patients followed for a median of five years (1 to 24 years), 19% developed end-stage renal failure or deterioration of renal function. Proteinuria of more than 3.5 g/day persisted in 34%, and 47% were in complete or partial remission. The Kaplan-Meier estimated probability of renal survival was 91 +/- 3% at five years and 75 +/- 6% at ten years. The predictors for the primary outcome, ESRF, identified in a Cox proportional hazards model, were histological stage (Ehrenreich-Churg) III-IV (hazard ratio 5.3, CI 1.9 to 15.0, P = 0.002) and nephrotic syndrome (hazard ratio 7.9, CI 1.1 to 61.5, P = 0.04); the predictors for the secondary outcome, ESRF or patient death, were histological stage III-IV (hazard ratio 2.8, CI 1.3 to 6.0, P = 0.008), nephrotic syndrome (hazard ratio 3.0, CI 1.1 to 8.0, P = 0.003) and comorbidity (hazard ratio 2.8, CI 1.3 to 5.9, P = 0.007). Nephrotic syndrome and histological stage III-IV allowed the demarcation of the high-risk group from the remaining patients (P < 0.0001). CONCLUSION: Histological stage, nephrotic syndrome, and comorbidity predict end-stage renal failure or death in idiopathic membranous nephropathy. Identification of the high-risk group at the time of diagnostic renal biopsy will permit appropriate treatment to be targeted to the patients who might benefit the most from the therapy in future clinical trials. (+info)Membranoproliferative Glomerulonephritis (MPGN) is a type of glomerulonephritis, which is a group of kidney disorders characterized by inflammation and damage to the glomeruli, the tiny blood vessels in the kidneys responsible for filtering waste and excess fluids from the blood.
MPGN is specifically characterized by thickening of the glomerular basement membrane and proliferation (increased number) of cells in the mesangium, a region within the glomerulus. This condition can be primary or secondary to other diseases such as infections, autoimmune disorders, or monoclonal gammopathies.
MPGN is typically classified into three types based on the pattern of injury seen on electron microscopy: Type I, Type II (Dense Deposit Disease), and Type III. Each type has distinct clinical features, laboratory findings, and treatment approaches. Symptoms of MPGN may include hematuria (blood in urine), proteinuria (protein in urine), hypertension (high blood pressure), edema (swelling), and eventually progress to chronic kidney disease or end-stage renal disease if left untreated.
Glomerulonephritis is a medical condition that involves inflammation of the glomeruli, which are the tiny blood vessel clusters in the kidneys that filter waste and excess fluids from the blood. This inflammation can impair the kidney's ability to filter blood properly, leading to symptoms such as proteinuria (protein in the urine), hematuria (blood in the urine), edema (swelling), hypertension (high blood pressure), and eventually kidney failure.
Glomerulonephritis can be acute or chronic, and it may occur as a primary kidney disease or secondary to other medical conditions such as infections, autoimmune disorders, or vasculitis. The diagnosis of glomerulonephritis typically involves a combination of medical history, physical examination, urinalysis, blood tests, and imaging studies, with confirmation often requiring a kidney biopsy. Treatment depends on the underlying cause and severity of the disease but may include medications to suppress inflammation, control blood pressure, and manage symptoms.
Complement C3 Nephritic Factor (C3NeF) is a type of autoantibody that activates the complement system and plays a significant role in the development of certain types of kidney diseases. The complement system is a part of the immune system that helps to eliminate pathogens and damaged cells from the body.
C3NeF is specifically directed against the C3 convertase enzyme complex, which is a critical component of the complement system's activation pathway. By binding to this enzyme complex, C3NeF stabilizes it and enhances its activity, leading to excessive complement activation and subsequent tissue damage.
In the context of kidney diseases, C3NeF has been associated with several forms of glomerulonephritis, including membranoproliferative glomerulonephritis (MPGN) type II, also known as dense deposit disease (DDD). The persistent activation of the complement system by C3NeF can result in the accumulation of complement components and immune complexes in the glomeruli, causing inflammation, tissue injury, and ultimately leading to kidney function impairment.
It is essential to diagnose and monitor C3NeF levels in patients with kidney diseases, as it may help guide treatment decisions and assess disease prognosis. Therapeutic strategies targeting the complement system, such as eculizumab, have shown promising results in managing C3NeF-associated kidney diseases.
A kidney glomerulus is a functional unit in the nephron of the kidney. It is a tuft of capillaries enclosed within a structure called Bowman's capsule, which filters waste and excess fluids from the blood. The glomerulus receives blood from an afferent arteriole and drains into an efferent arteriole.
The process of filtration in the glomerulus is called ultrafiltration, where the pressure within the glomerular capillaries drives plasma fluid and small molecules (such as ions, glucose, amino acids, and waste products) through the filtration membrane into the Bowman's space. Larger molecules, like proteins and blood cells, are retained in the blood due to their larger size. The filtrate then continues down the nephron for further processing, eventually forming urine.
Membranous glomerulonephritis (MGN) is a kidney disorder that leads to the inflammation and damage of the glomeruli, which are the tiny blood vessels in the kidneys responsible for filtering waste and excess fluids from the blood. In MGN, the membrane that surrounds the glomerular capillaries becomes thickened and damaged due to the deposit of immune complexes, primarily composed of antibodies and antigens.
The onset of membranous glomerulonephritis can be either primary (idiopathic) or secondary to various underlying conditions such as autoimmune diseases (like systemic lupus erythematosus), infections (hepatitis B or C, syphilis, endocarditis), medications, or malignancies.
The symptoms of membranous glomerulonephritis may include:
1. Proteinuria - the presence of excess protein, specifically albumin, in the urine. This can lead to nephrotic syndrome, characterized by heavy protein loss in urine, edema (swelling), hypoalbuminemia (low blood albumin levels), and hyperlipidemia (high blood lipid levels).
2. Hematuria - the presence of red blood cells in the urine, which can be visible or microscopic.
3. Hypertension - high blood pressure.
4. Edema - swelling in various body parts due to fluid retention.
5. Nephrotic range proteinuria (protein loss greater than 3.5 grams per day) and/or nephritic syndrome (a combination of hematuria, proteinuria, hypertension, and kidney dysfunction) can be observed in some cases.
The diagnosis of membranous glomerulonephritis typically involves a thorough medical history, physical examination, urinalysis, blood tests, and imaging studies. A definitive diagnosis often requires a kidney biopsy to assess the glomerular structure and the nature of the immune complex deposits. Treatment depends on the underlying cause and severity of the disease and may include corticosteroids, immunosuppressants, blood pressure management, and supportive care for symptoms like edema and proteinuria.
Cryoglobulinemia is a medical condition characterized by the presence of abnormal proteins called cryoglobulins in the blood. These proteins become insoluble at lower temperatures and can form immune complexes that can cause inflammation and damage to small blood vessels when they precipitate in cooler parts of the body.
Cryoglobulinemia is often associated with underlying conditions such as autoimmune diseases (such as rheumatoid arthritis or lupus), chronic infections (such as hepatitis C), and certain types of cancer (such as lymphoma). Symptoms can vary widely, but may include purpura (purple spots on the skin), joint pain, peripheral neuropathy (nerve damage causing numbness or weakness), fatigue, and kidney problems.
The diagnosis of cryoglobulinemia is typically made by detecting cryoglobulins in the blood through a special test that requires the blood sample to be kept at cold temperatures. Treatment for cryoglobulinemia depends on the underlying cause, but may include medications such as corticosteroids, immunosuppressants, or chemotherapy drugs.
Nephrotic syndrome is a group of symptoms that indicate kidney damage, specifically damage to the glomeruli—the tiny blood vessel clusters in the kidneys that filter waste and excess fluids from the blood. The main features of nephrotic syndrome are:
1. Proteinuria (excess protein in urine): Large amounts of a protein called albumin leak into the urine due to damaged glomeruli, which can't properly filter proteins. This leads to low levels of albumin in the blood, causing fluid buildup and swelling.
2. Hypoalbuminemia (low blood albumin levels): As albumin leaks into the urine, the concentration of albumin in the blood decreases, leading to hypoalbuminemia. This can cause edema (swelling), particularly in the legs, ankles, and feet.
3. Edema (fluid retention and swelling): With low levels of albumin in the blood, fluids move into the surrounding tissues, causing swelling or puffiness. The swelling is most noticeable around the eyes, face, hands, feet, and abdomen.
4. Hyperlipidemia (high lipid/cholesterol levels): The kidneys play a role in regulating lipid metabolism. Damage to the glomeruli can lead to increased lipid production and high cholesterol levels in the blood.
Nephrotic syndrome can result from various underlying kidney diseases, such as minimal change disease, membranous nephropathy, or focal segmental glomerulosclerosis. Treatment depends on the underlying cause and may include medications to control inflammation, manage high blood pressure, and reduce proteinuria. In some cases, dietary modifications and lifestyle changes are also recommended.
IGA glomerulonephritis (also known as Berger's disease) is a type of glomerulonephritis, which is a condition characterized by inflammation of the glomeruli, the tiny filtering units in the kidneys. In IgA glomerulonephritis, the immune system produces an abnormal amount of IgA antibodies, which deposit in the glomeruli and cause inflammation. This can lead to symptoms such as blood in the urine, protein in the urine, and swelling in the legs and feet. In some cases, it can also lead to kidney failure. The exact cause of IgA glomerulonephritis is not known, but it is often associated with other conditions such as infections, autoimmune diseases, and certain medications.
Complement C3 is a protein that plays a central role in the complement system, which is a part of the immune system that helps to clear pathogens and damaged cells from the body. Complement C3 can be activated through three different pathways: the classical pathway, the lectin pathway, and the alternative pathway. Once activated, it breaks down into two fragments, C3a and C3b.
C3a is an anaphylatoxin that helps to recruit immune cells to the site of infection or injury, while C3b plays a role in opsonization, which is the process of coating pathogens or damaged cells with proteins to make them more recognizable to the immune system. Additionally, C3b can also activate the membrane attack complex (MAC), which forms a pore in the membrane of target cells leading to their lysis or destruction.
In summary, Complement C3 is an important protein in the complement system that helps to identify and eliminate pathogens and damaged cells from the body through various mechanisms.
Cryoglobulins are immunoglobulins (a type of antibody) that precipitate or become insoluble at reduced temperatures, typically below 37°C (98.6°F), and re-dissolve when rewarmed. They can be found in various clinical conditions such as infections, inflammatory diseases, and lymphoproliferative disorders.
The presence of cryoglobulins in the blood can lead to a variety of symptoms, including purpura (a type of skin rash), arthralgias (joint pain), neuropathy (nerve damage), and glomerulonephritis (kidney inflammation). The diagnosis of cryoglobulinemia is made by detecting the presence of cryoglobulins in the serum, which requires special handling and processing of the blood sample. Treatment of cryoglobulinemia depends on the underlying cause and may include medications such as corticosteroids, immunosuppressive agents, or targeted therapies.
Proteinuria is a medical term that refers to the presence of excess proteins, particularly albumin, in the urine. Under normal circumstances, only small amounts of proteins should be found in the urine because the majority of proteins are too large to pass through the glomeruli, which are the filtering units of the kidneys.
However, when the glomeruli become damaged or diseased, they may allow larger molecules such as proteins to leak into the urine. Persistent proteinuria is often a sign of kidney disease and can indicate damage to the glomeruli. It is usually detected through a routine urinalysis and may be confirmed with further testing.
The severity of proteinuria can vary, and it can be a symptom of various underlying conditions such as diabetes, hypertension, glomerulonephritis, and other kidney diseases. Treatment for proteinuria depends on the underlying cause and may include medications to control blood pressure, manage diabetes, or reduce protein loss in the urine.
Immune complex diseases are medical conditions that occur when the immune system produces an abnormal response to certain antigens, leading to the formation and deposition of immune complexes in various tissues and organs. These immune complexes consist of antibodies bound to antigens, which can trigger an inflammatory reaction and damage the surrounding tissue.
Immune complex diseases can be classified into two categories: acute and chronic. Acute immune complex diseases include serum sickness and hypersensitivity vasculitis, while chronic immune complex diseases include systemic lupus erythematosus (SLE), rheumatoid arthritis, and membranoproliferative glomerulonephritis.
The symptoms of immune complex diseases depend on the location and extent of tissue damage. They can range from mild to severe and may include fever, joint pain, skin rashes, kidney dysfunction, and neurological problems. Treatment typically involves medications that suppress the immune system and reduce inflammation, such as corticosteroids, immunosuppressants, and anti-inflammatory drugs.
A biopsy is a medical procedure in which a small sample of tissue is taken from the body to be examined under a microscope for the presence of disease. This can help doctors diagnose and monitor various medical conditions, such as cancer, infections, or autoimmune disorders. The type of biopsy performed will depend on the location and nature of the suspected condition. Some common types of biopsies include:
1. Incisional biopsy: In this procedure, a surgeon removes a piece of tissue from an abnormal area using a scalpel or other surgical instrument. This type of biopsy is often used when the lesion is too large to be removed entirely during the initial biopsy.
2. Excisional biopsy: An excisional biopsy involves removing the entire abnormal area, along with a margin of healthy tissue surrounding it. This technique is typically employed for smaller lesions or when cancer is suspected.
3. Needle biopsy: A needle biopsy uses a thin, hollow needle to extract cells or fluid from the body. There are two main types of needle biopsies: fine-needle aspiration (FNA) and core needle biopsy. FNA extracts loose cells, while a core needle biopsy removes a small piece of tissue.
4. Punch biopsy: In a punch biopsy, a round, sharp tool is used to remove a small cylindrical sample of skin tissue. This type of biopsy is often used for evaluating rashes or other skin abnormalities.
5. Shave biopsy: During a shave biopsy, a thin slice of tissue is removed from the surface of the skin using a sharp razor-like instrument. This technique is typically used for superficial lesions or growths on the skin.
After the biopsy sample has been collected, it is sent to a laboratory where a pathologist will examine the tissue under a microscope and provide a diagnosis based on their findings. The results of the biopsy can help guide further treatment decisions and determine the best course of action for managing the patient's condition.
Complement Factor H is a protein involved in the regulation of the complement system, which is a part of the immune system that helps to clear pathogens and damaged cells from the body. Specifically, Complement Factor H helps to regulate the activation and deactivation of the complement component C3b, preventing excessive or unwanted activation of the complement system and protecting host tissues from damage.
Complement Factor H is a crucial protein in maintaining the balance between the protective effects of the complement system and the potential for harm to the body's own cells and tissues. Deficiencies or mutations in Complement Factor H have been associated with several diseases, including age-related macular degeneration (AMD), atypical hemolytic uremic syndrome (aHUS), and C3 glomerulopathy.
Hematuria is a medical term that refers to the presence of blood in urine. It can be visible to the naked eye, which is called gross hematuria, or detected only under a microscope, known as microscopic hematuria. The blood in urine may come from any site along the urinary tract, including the kidneys, ureters, bladder, or urethra. Hematuria can be a symptom of various medical conditions, such as urinary tract infections, kidney stones, kidney disease, or cancer of the urinary tract. It is essential to consult a healthcare professional if you notice blood in your urine to determine the underlying cause and receive appropriate treatment.
Properdin is defined as a positive regulatory protein in the complement system, which is a part of the immune system. It plays a crucial role in the alternative pathway of complement activation. Properdin stabilizes the C3 convertase (C3bBb), preventing its decay and increasing the efficiency of the alternative pathway. This results in the production of the membrane attack complex, which leads to the lysis of foreign cells or pathogens. Deficiencies in properdin can lead to an increased susceptibility to bacterial infections.
Focal segmental glomerulosclerosis (FSGS) is a pattern of kidney injury that involves scarring or sclerosis in some (segmental) areas of some (focal) glomeruli. Glomeruli are the tiny blood vessel clusters within the kidneys that filter waste and excess fluids from the blood.
In FSGS, the scarring occurs due to damage to the glomerular basement membrane, which can be caused by various factors such as genetic mutations, viral infections, or immune system disorders. The damage leads to the accumulation of extracellular matrix proteins and the formation of scar tissue, impairing the kidney's ability to filter blood effectively.
FSGS is characterized by proteinuria (protein in the urine), hematuria (blood in the urine), hypertension (high blood pressure), and declining kidney function, which can lead to end-stage renal disease if left untreated. The focal and segmental nature of the scarring means that not all glomeruli are affected, and only some areas of each affected glomerulus are damaged, making FSGS a highly variable condition with different clinical presentations and outcomes.
A kidney, in medical terms, is one of two bean-shaped organs located in the lower back region of the body. They are essential for maintaining homeostasis within the body by performing several crucial functions such as:
1. Regulation of water and electrolyte balance: Kidneys help regulate the amount of water and various electrolytes like sodium, potassium, and calcium in the bloodstream to maintain a stable internal environment.
2. Excretion of waste products: They filter waste products from the blood, including urea (a byproduct of protein metabolism), creatinine (a breakdown product of muscle tissue), and other harmful substances that result from normal cellular functions or external sources like medications and toxins.
3. Endocrine function: Kidneys produce several hormones with important roles in the body, such as erythropoietin (stimulates red blood cell production), renin (regulates blood pressure), and calcitriol (activated form of vitamin D that helps regulate calcium homeostasis).
4. pH balance regulation: Kidneys maintain the proper acid-base balance in the body by excreting either hydrogen ions or bicarbonate ions, depending on whether the blood is too acidic or too alkaline.
5. Blood pressure control: The kidneys play a significant role in regulating blood pressure through the renin-angiotensin-aldosterone system (RAAS), which constricts blood vessels and promotes sodium and water retention to increase blood volume and, consequently, blood pressure.
Anatomically, each kidney is approximately 10-12 cm long, 5-7 cm wide, and 3 cm thick, with a weight of about 120-170 grams. They are surrounded by a protective layer of fat and connected to the urinary system through the renal pelvis, ureters, bladder, and urethra.
The Glomerular Basement Membrane (GBM) is a part of the filtration barrier in the nephron of the kidney. It is a thin, porous sheet of extracellular matrix that lies between the glomerular endothelial cells and the visceral epithelial cells (podocytes). The GBM plays a crucial role in the process of ultrafiltration, allowing the passage of water and small molecules while preventing the loss of larger proteins into the urine. It is composed mainly of type IV collagen, laminin, nidogen, and heparan sulfate proteoglycans. Certain kidney diseases, such as Goodpasture's disease and some forms of glomerulonephritis, can involve damage to the GBM.
The complement system is a group of proteins found in the blood and on the surface of cells that when activated, work together to help eliminate pathogens such as bacteria, viruses, and fungi from the body. The proteins are normally inactive in the bloodstream. When they encounter an invading microorganism or foreign substance, a series of reactions take place leading to the activation of the complement system. Activation results in the production of effector molecules that can punch holes in the cell membranes of pathogens, recruit and activate immune cells, and help remove debris and dead cells from the body.
There are three main pathways that can lead to complement activation: the classical pathway, the lectin pathway, and the alternative pathway. Each pathway involves a series of proteins that work together in a cascade-like manner to amplify the response and generate effector molecules. The three main effector molecules produced by the complement system are C3b, C4b, and C5b. These molecules can bind to the surface of pathogens, marking them for destruction by other immune cells.
Complement proteins also play a role in the regulation of the immune response. They help to prevent excessive activation of the complement system, which could damage host tissues. Dysregulation of the complement system has been implicated in a number of diseases, including autoimmune disorders and inflammatory conditions.
In summary, Complement System Proteins are a group of proteins that play a crucial role in the immune response by helping to eliminate pathogens and regulate the immune response. They can be activated through three different pathways, leading to the production of effector molecules that mark pathogens for destruction. Dysregulation of the complement system has been linked to various diseases.
Lipoid nephrosis is a historical term for a kidney disorder now more commonly referred to as minimal change disease (MCD). It is a type of glomerulonephritis which is characterized by the loss of proteins in the urine (proteinuria) due to damage to the glomeruli, the tiny filtering units within the kidneys.
The term "lipoid" refers to the presence of lipids or fats in the glomeruli, which can be observed under a microscope. However, it's worth noting that not all cases of MCD involve lipid accumulation in the glomeruli.
MCD is typically idiopathic, meaning its cause is unknown, but it can also occur as a secondary condition related to other medical disorders such as allergies, infections, or medications. It primarily affects children, but can also occur in adults. Treatment usually involves corticosteroids and other immunosuppressive therapies to control proteinuria and prevent kidney damage.
Nephritis is a medical term that refers to inflammation of the kidneys, specifically affecting the glomeruli - the tiny filtering units inside the kidneys. The condition can cause damage to the glomeruli, leading to impaired kidney function and the leakage of protein and blood into the urine.
Nephritis can result from a variety of causes, including infections, autoimmune disorders, and exposure to certain medications or toxins. Depending on the severity and underlying cause, nephritis may be treated with medications, dietary modifications, or other therapies aimed at reducing inflammation and preserving kidney function. In severe cases, hospitalization and more intensive treatments may be necessary.
Kidney disease, also known as nephropathy or renal disease, refers to any functional or structural damage to the kidneys that impairs their ability to filter blood, regulate electrolytes, produce hormones, and maintain fluid balance. This damage can result from a wide range of causes, including diabetes, hypertension, glomerulonephritis, polycystic kidney disease, lupus, infections, drugs, toxins, and congenital or inherited disorders.
Depending on the severity and progression of the kidney damage, kidney diseases can be classified into two main categories: acute kidney injury (AKI) and chronic kidney disease (CKD). AKI is a sudden and often reversible loss of kidney function that occurs over hours to days, while CKD is a progressive and irreversible decline in kidney function that develops over months or years.
Symptoms of kidney diseases may include edema, proteinuria, hematuria, hypertension, electrolyte imbalances, metabolic acidosis, anemia, and decreased urine output. Treatment options depend on the underlying cause and severity of the disease and may include medications, dietary modifications, dialysis, or kidney transplantation.
The alternative complement pathway is one of the three initiating pathways of the complement system, which is a part of the innate immune system that helps to clear pathogens and damaged cells from the body. The other two pathways are the classical and lectin pathways.
The alternative pathway is continuously activated at a low level, even in the absence of infection or injury, through the spontaneous cleavage of complement component C3 into C3a and C3b by the protease factor D in the presence of magnesium ions. The generated C3b can then bind covalently to nearby surfaces, including pathogens and host cells.
On self-surfaces, regulatory proteins like decay-accelerating factor (DAF) or complement receptor 1 (CR1) help to prevent the formation of the alternative pathway convertase and thus further activation of the complement system. However, on foreign surfaces, the C3b can recruit more complement components, forming a complex called the alternative pathway convertase (C3bBb), which cleaves additional C3 molecules into C3a and C3b.
The generated C3b can then bind to the surface and participate in the formation of the membrane attack complex (MAC), leading to the lysis of the target cell. The alternative pathway plays a crucial role in the defense against gram-negative bacteria, fungi, and parasites, as well as in the clearance of immune complexes and apoptotic cells. Dysregulation of the alternative complement pathway has been implicated in several diseases, including autoimmune disorders and atypical hemolytic uremic syndrome (aHUS).
An antigen-antibody complex is a type of immune complex that forms when an antibody binds to a specific antigen. An antigen is any substance that triggers an immune response, while an antibody is a protein produced by the immune system to neutralize or destroy foreign substances like antigens.
When an antibody binds to an antigen, it forms a complex that can be either soluble or insoluble. Soluble complexes are formed when the antigen is small and can move freely through the bloodstream. Insoluble complexes, on the other hand, are formed when the antigen is too large to move freely, such as when it is part of a bacterium or virus.
The formation of antigen-antibody complexes plays an important role in the immune response. Once formed, these complexes can be recognized and cleared by other components of the immune system, such as phagocytes, which help to prevent further damage to the body. However, in some cases, the formation of large numbers of antigen-antibody complexes can lead to inflammation and tissue damage, contributing to the development of certain autoimmune diseases.
Anti-glomerular basement membrane (anti-GBM) disease, also known as Goodpasture's disease, is a rare autoimmune disorder in which the body produces antibodies that attack the glomerular basement membrane (GBM), a component of the filtering units (glomeruli) in the kidneys. This leads to inflammation and damage to the glomeruli, causing hematuria (blood in urine), proteinuria (protein in urine), and potentially kidney failure. In some cases, anti-GBM disease may also affect the lungs, leading to coughing up blood (hemoptysis). The exact cause of anti-GBM disease is not fully understood, but it is believed to be related to both genetic and environmental factors. Treatment typically involves a combination of immunosuppressive therapy and plasma exchange.
Interstitial nephritis is a condition characterized by inflammation in the interstitium (the tissue between the kidney tubules) of one or both kidneys. This inflammation can be caused by various factors, including infections, autoimmune disorders, medications, and exposure to certain toxins.
The inflammation may lead to symptoms such as hematuria (blood in the urine), proteinuria (protein in the urine), decreased urine output, and kidney dysfunction. In some cases, interstitial nephritis can progress to chronic kidney disease or even end-stage renal failure if left untreated.
The diagnosis of interstitial nephritis typically involves a combination of medical history, physical examination, laboratory tests (such as urinalysis and blood tests), and imaging studies (such as ultrasound or CT scan). A kidney biopsy may also be performed to confirm the diagnosis and assess the severity of the inflammation.
Treatment for interstitial nephritis depends on the underlying cause, but may include corticosteroids, immunosuppressive medications, or discontinuation of any offending medications. In some cases, supportive care such as dialysis may be necessary to manage kidney dysfunction until the inflammation resolves.
Hepatitis C is a liver infection caused by the hepatitis C virus (HCV). It's primarily spread through contact with contaminated blood, often through sharing needles or other equipment to inject drugs. For some people, hepatitis C is a short-term illness but for most — about 75-85% — it becomes a long-term, chronic infection that can lead to serious health problems like liver damage, liver failure, and even liver cancer. The virus can infect and inflame the liver, causing symptoms like jaundice (yellowing of the skin and eyes), abdominal pain, fatigue, and dark urine. Many people with hepatitis C don't have any symptoms, so they might not know they have the infection until they experience complications. There are effective treatments available for hepatitis C, including antiviral medications that can cure the infection in most people. Regular testing is important to diagnose and treat hepatitis C early, before it causes serious health problems.
Blood protein electrophoresis (BPE) is a laboratory test that separates and measures the different proteins in the blood, such as albumin, alpha-1 globulins, alpha-2 globulins, beta globulins, and gamma globulins. This test is often used to help diagnose or monitor conditions related to abnormal protein levels, such as multiple myeloma, macroglobulinemia, and other plasma cell disorders.
In this test, a sample of the patient's blood is placed on a special gel and an electric current is applied. The proteins in the blood migrate through the gel based on their electrical charge and size, creating bands that can be visualized and measured. By comparing the band patterns to reference ranges, doctors can identify any abnormal protein levels or ratios, which may indicate underlying medical conditions.
It's important to note that while BPE is a useful diagnostic tool, it should be interpreted in conjunction with other clinical findings and laboratory tests for accurate diagnosis and management of the patient's condition.
Hemolytic-Uremic Syndrome (HUS) is a serious condition that affects the blood and kidneys. It is characterized by three major features: the breakdown of red blood cells (hemolysis), the abnormal clotting of small blood vessels (microthrombosis), and acute kidney failure.
The breakdown of red blood cells leads to the release of hemoglobin into the bloodstream, which can cause anemia. The microthrombi can obstruct the flow of blood in the kidneys' filtering system (glomeruli), leading to damaged kidney function and potentially acute kidney failure.
HUS is often caused by a bacterial infection, most commonly Escherichia coli (E. coli) that produces Shiga toxins. This form of HUS is known as STEC-HUS or Stx-HUS. Other causes include infections with other bacteria, viruses, medications, pregnancy complications, and certain medical conditions such as autoimmune diseases.
Symptoms of HUS may include fever, fatigue, decreased urine output, blood in the stool, swelling in the face, hands, or feet, and irritability or confusion. Treatment typically involves supportive care, including dialysis for kidney failure, transfusions to replace lost red blood cells, and managing high blood pressure. In severe cases, a kidney transplant may be necessary.
Immunoglobulin G (IgG) is a type of antibody, which is a protective protein produced by the immune system in response to foreign substances like bacteria or viruses. IgG is the most abundant type of antibody in human blood, making up about 75-80% of all antibodies. It is found in all body fluids and plays a crucial role in fighting infections caused by bacteria, viruses, and toxins.
IgG has several important functions:
1. Neutralization: IgG can bind to the surface of bacteria or viruses, preventing them from attaching to and infecting human cells.
2. Opsonization: IgG coats the surface of pathogens, making them more recognizable and easier for immune cells like neutrophils and macrophages to phagocytose (engulf and destroy) them.
3. Complement activation: IgG can activate the complement system, a group of proteins that work together to help eliminate pathogens from the body. Activation of the complement system leads to the formation of the membrane attack complex, which creates holes in the cell membranes of bacteria, leading to their lysis (destruction).
4. Antibody-dependent cellular cytotoxicity (ADCC): IgG can bind to immune cells like natural killer (NK) cells and trigger them to release substances that cause target cells (such as virus-infected or cancerous cells) to undergo apoptosis (programmed cell death).
5. Immune complex formation: IgG can form immune complexes with antigens, which can then be removed from the body through various mechanisms, such as phagocytosis by immune cells or excretion in urine.
IgG is a critical component of adaptive immunity and provides long-lasting protection against reinfection with many pathogens. It has four subclasses (IgG1, IgG2, IgG3, and IgG4) that differ in their structure, function, and distribution in the body.
The Fluorescent Antibody Technique (FAT) is a type of immunofluorescence assay used in laboratory medicine and pathology for the detection and localization of specific antigens or antibodies in tissues, cells, or microorganisms. In this technique, a fluorescein-labeled antibody is used to selectively bind to the target antigen or antibody, forming an immune complex. When excited by light of a specific wavelength, the fluorescein label emits light at a longer wavelength, typically visualized as green fluorescence under a fluorescence microscope.
The FAT is widely used in diagnostic microbiology for the identification and characterization of various bacteria, viruses, fungi, and parasites. It has also been applied in the diagnosis of autoimmune diseases and certain cancers by detecting specific antibodies or antigens in patient samples. The main advantage of FAT is its high sensitivity and specificity, allowing for accurate detection and differentiation of various pathogens and disease markers. However, it requires specialized equipment and trained personnel to perform and interpret the results.
Antineutrophil cytoplasmic antibodies (ANCAs) are a type of autoantibody that specifically target certain proteins in the cytoplasm of neutrophils, which are a type of white blood cell. These antibodies are associated with several types of vasculitis, which is inflammation of the blood vessels.
There are two main types of ANCAs: perinuclear ANCAs (p-ANCAs) and cytoplasmic ANCAs (c-ANCAs). p-ANCAs are directed against myeloperoxidase, a protein found in neutrophil granules, while c-ANCAs target proteinase 3, another protein found in neutrophil granules.
The presence of ANCAs in the blood can indicate an increased risk for developing certain types of vasculitis, such as granulomatosis with polyangiitis (GPA), eosinophilic granulomatosis with polyangiitis (EGPA), and microscopic polyangiitis (MPA). ANCA testing is often used in conjunction with other clinical findings to help diagnose and manage these conditions.
It's important to note that while the presence of ANCAs can indicate an increased risk for vasculitis, not everyone with ANCAs will develop the condition. Additionally, ANCAs can also be found in some individuals without any associated disease, so their presence should be interpreted in the context of other clinical findings.
Kidney transplantation is a surgical procedure where a healthy kidney from a deceased or living donor is implanted into a patient with end-stage renal disease (ESRD) or permanent kidney failure. The new kidney takes over the functions of filtering waste and excess fluids from the blood, producing urine, and maintaining the body's electrolyte balance.
The transplanted kidney is typically placed in the lower abdomen, with its blood vessels connected to the recipient's iliac artery and vein. The ureter of the new kidney is then attached to the recipient's bladder to ensure proper urine flow. Following the surgery, the patient will require lifelong immunosuppressive therapy to prevent rejection of the transplanted organ by their immune system.
Lupus nephritis is a type of kidney inflammation (nephritis) that can occur in people with systemic lupus erythematosus (SLE), an autoimmune disease. In lupus nephritis, the immune system produces abnormal antibodies that attack the tissues of the kidneys, leading to inflammation and damage. The condition can cause a range of symptoms, including proteinuria (protein in the urine), hematuria (blood in the urine), hypertension (high blood pressure), and eventually kidney failure if left untreated. Lupus nephritis is typically diagnosed through a combination of medical history, physical examination, laboratory tests, and imaging studies. Treatment may include medications to suppress the immune system and control inflammation, such as corticosteroids and immunosuppressive drugs.
The glomerular mesangium is a part of the nephron in the kidney. It is the region located in the middle of the glomerular tuft, where the capillary loops of the glomerulus are surrounded by a network of extracellular matrix and mesangial cells. These cells and matrix play an important role in maintaining the structure and function of the filtration barrier in the glomerulus, which helps to filter waste products from the blood.
The mesangial cells have contractile properties and can regulate the flow of blood through the capillaries by constricting or dilating the diameter of the glomerular capillary loops. They also play a role in immune responses, as they can phagocytize immune complexes and release cytokines and growth factors that modulate inflammation and tissue repair.
Abnormalities in the mesangium can lead to various kidney diseases, such as glomerulonephritis, mesangial proliferative glomerulonephritis, and diabetic nephropathy.
Immunosuppressive agents are medications that decrease the activity of the immune system. They are often used to prevent the rejection of transplanted organs and to treat autoimmune diseases, where the immune system mistakenly attacks the body's own tissues. These drugs work by interfering with the immune system's normal responses, which helps to reduce inflammation and damage to tissues. However, because they suppress the immune system, people who take immunosuppressive agents are at increased risk for infections and other complications. Examples of immunosuppressive agents include corticosteroids, azathioprine, cyclophosphamide, mycophenolate mofetil, tacrolimus, and sirolimus.
Electron microscopy (EM) is a type of microscopy that uses a beam of electrons to create an image of the sample being examined, resulting in much higher magnification and resolution than light microscopy. There are several types of electron microscopy, including transmission electron microscopy (TEM), scanning electron microscopy (SEM), and reflection electron microscopy (REM).
In TEM, a beam of electrons is transmitted through a thin slice of the sample, and the electrons that pass through the sample are focused to form an image. This technique can provide detailed information about the internal structure of cells, viruses, and other biological specimens, as well as the composition and structure of materials at the atomic level.
In SEM, a beam of electrons is scanned across the surface of the sample, and the electrons that are scattered back from the surface are detected to create an image. This technique can provide information about the topography and composition of surfaces, as well as the structure of materials at the microscopic level.
REM is a variation of SEM in which the beam of electrons is reflected off the surface of the sample, rather than scattered back from it. This technique can provide information about the surface chemistry and composition of materials.
Electron microscopy has a wide range of applications in biology, medicine, and materials science, including the study of cellular structure and function, disease diagnosis, and the development of new materials and technologies.
The basement membrane is a thin, specialized layer of extracellular matrix that provides structural support and separates epithelial cells (which line the outer surfaces of organs and blood vessels) from connective tissue. It is composed of two main layers: the basal lamina, which is produced by the epithelial cells, and the reticular lamina, which is produced by the connective tissue. The basement membrane plays important roles in cell adhesion, migration, differentiation, and survival.
The basal lamina is composed mainly of type IV collagen, laminins, nidogens, and proteoglycans, while the reticular lamina contains type III collagen, fibronectin, and other matrix proteins. The basement membrane also contains a variety of growth factors and cytokines that can influence cell behavior.
Defects in the composition or organization of the basement membrane can lead to various diseases, including kidney disease, eye disease, and skin blistering disorders.
Hepacivirus is a genus of viruses in the family Flaviviridae. The most well-known member of this genus is Hepatitis C virus (HCV), which is a major cause of liver disease worldwide. HCV infection can lead to chronic hepatitis, cirrhosis, and liver cancer.
Hepaciviruses are enveloped viruses with a single-stranded, positive-sense RNA genome. They have a small icosahedral capsid and infect a variety of hosts, including humans, non-human primates, horses, and birds. The virus enters the host cell by binding to specific receptors on the cell surface and is then internalized through endocytosis.
HCV has a high degree of genetic diversity and is classified into seven major genotypes and numerous subtypes based on differences in its RNA sequence. This genetic variability can affect the virus's ability to evade the host immune response, making treatment more challenging.
In addition to HCV, other hepaciviruses have been identified in various animal species, including equine hepacivirus (EHCV), rodent hepacivirus (RHV), and bat hepacivirus (BtHepCV). These viruses are being studied to better understand the biology of hepaciviruses and their potential impact on human health.
Vasculitis is a group of disorders characterized by inflammation of the blood vessels, which can cause changes in the vessel walls including thickening, narrowing, or weakening. These changes can restrict blood flow, leading to organ and tissue damage. The specific symptoms and severity of vasculitis depend on the size and location of the affected blood vessels and the extent of inflammation. Vasculitis can affect any organ system in the body, and its causes can vary, including infections, autoimmune disorders, or exposure to certain medications or chemicals.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
Autoantibodies are defined as antibodies that are produced by the immune system and target the body's own cells, tissues, or organs. These antibodies mistakenly identify certain proteins or molecules in the body as foreign invaders and attack them, leading to an autoimmune response. Autoantibodies can be found in various autoimmune diseases such as rheumatoid arthritis, lupus, and thyroiditis. The presence of autoantibodies can also be used as a diagnostic marker for certain conditions.
Serum sickness is an immune-mediated hypersensitivity reaction that typically occurs within 1 to 3 weeks after the administration of foreign proteins or drugs, such as certain types of antibiotics, antiserums, or monoclonal antibodies. It is characterized by symptoms such as fever, rash, joint pain, and lymphadenopathy (swollen lymph nodes). These symptoms are caused by the formation of immune complexes, which deposit in various tissues and activate the complement system, leading to inflammation. Serum sickness can be treated with antihistamines, corticosteroids, and other immunomodulatory agents. It is important to note that serum sickness is different from anaphylaxis, which is a more severe, life-threatening allergic reaction that occurs immediately after exposure to an allergen.
 Membranoproliferative glomerulonephritis
Membranoproliferative glomerulonephritis
Complement deficiency
List of OMIM disorder codes
Cryoglobulinemia
Secondary hypertension
Nephritic syndrome
Kamala Balakrishnan
Barraquer-Simons syndrome
Monoclonal gammopathy of renal significance
Cryoglobulinemic vasculitis
Central serous chorioretinopathy
Shunt nephritis
Lymphadenopathy
Transplant glomerulopathy
Endocapillary proliferative glomerulonephritis
Hypoalbuminemia
Anaerococcus
Bowman's capsule
Proteinuria
Nephrotic syndrome
CFHR5
Hematuria
Complement component 3
Complement 3 deficiency
Glomerulonephritis
Acute proliferative glomerulonephritis
Diffuse proliferative nephritis
List of diseases (M)
Sickle cell nephropathy
List of MeSH codes (C12)
Tram track (medicine)
Membranoproliferative glomerulonephritis - Wikipedia
 Membranoproliferative glomerulonephritis: MedlinePlus Medical Encyclopedia
Membranoproliferative glomerulonephritis: MedlinePlus Medical Encyclopedia
 Membranoproliferative Glomerulonephritis: Practice Essentials, Pathophysiology, Etiology
Membranoproliferative Glomerulonephritis: Practice Essentials, Pathophysiology, Etiology
 Membranoproliferative glomerulonephritis - wikidoc
Membranoproliferative glomerulonephritis - wikidoc
 Membranoproliferative glomerulonephritis Information | Mount Sinai - New York
Membranoproliferative glomerulonephritis Information | Mount Sinai - New York
 Factor D Inhibition Blocks Complement Activation Induced by Mutant Factor B Associated With Atypical Hemolytic Uremic Syndrome...
Factor D Inhibition Blocks Complement Activation Induced by Mutant Factor B Associated With Atypical Hemolytic Uremic Syndrome...
 Membranoproliferative Glomerulonephritis (MPGN) in PEDSnet - PEDSnet
Membranoproliferative Glomerulonephritis (MPGN) in PEDSnet - PEDSnet
 Membranoproliferative glomerulonephritis: Video | Osmosis
Membranoproliferative glomerulonephritis: Video | Osmosis
 membranoproliferative glomerulonephritis · Communications · Lafayette College
membranoproliferative glomerulonephritis · Communications · Lafayette College
 Membranoproliferative Glomerulonephritis - Genitourinary Disorders - MSD Manual Professional Edition
Membranoproliferative Glomerulonephritis - Genitourinary Disorders - MSD Manual Professional Edition
 Membranoproliferative glomerulonephritis possibly associated with over-vaccination in a cocker spaniel
Membranoproliferative glomerulonephritis possibly associated with over-vaccination in a cocker spaniel
 John Niles, MD - Nephrology
John Niles, MD - Nephrology
![American Society of Nephrology | Kidney Week - [Session] Onconephrology: Immunological Cross-Talk (2023)](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAYAAAAf8/9hAAACYUlEQVQ4jW2TP0wTcRTHP7+7KyUq8TBgsYF4oRLBfxRDDCSS4HIxLoW4mgCjEyHerowmTZQwECdlcZS66bnAaBhkMhhsbUD0oFAOoXDttT2HHoFC3/TL+33f+35f3vcJaoUeV4FBQPUz85hGuhZUqVE4BHT7mY+AjWmk0ePfgFm/2dLZBnpc81ltYBLTsE+RDfv/VSFOFadzA9MaiBh4aWDq9pcnAONCiKjnebOp+sYEMAcMYxr2kQIbsHMD05oINryV1DaQZJZXN0ebz+Vpbm5VA4qEld0fFLZNMqjOAq+AMQk9HgWeYxoJECOS2oYcvoWi3WNm5Zr6MPRL7b/bzp2uVtrDlwgG5Bgwf6Rc8tl3K0K8JSQZUd/Ah585flNkPehiOyuo6gUCARkhSPsbWQA0xZ/9oj/KVCqTGX2/uaiu/PGw8Nh2i7CWprQucT5TsPNuacrHaoCtnFQQDXWiFep4tFNip+ix6kBduYzr5nEDDjvdGluBwNEANqAqQPrEVsZbLodUpaebUGoXZzFFIbBP181+wh29/FjbVjes7DgwAVwF5iW/QQw9rspCaEFJxi0XCXdeYa+jib+RJsIdvbhuEVkIZCGivuE0wJZJmg4RvQfoa7yR/Cp75SHFK7Ody0Jpwz507ju4wfp/uQLrewdk8oXJg6TdAuxiGp9kACJ6GhjJfo98Vq4vL1iHtrqW20pYpb0xa7/vjXXgYOUcK5MvvNx69vgdEX0G03h67MRjN85R8Xui5vHo8VFgBNN4UG3latAL3ygxKsek+e8J33BjJ+FnG1SzQWVdGqbxuhbsPxOb8qWHbiWHAAAAAElFTkSuQmCC) American Society of Nephrology | Kidney Week - [Session] Onconephrology: Immunological Cross-Talk (2023)
American Society of Nephrology | Kidney Week - [Session] Onconephrology: Immunological Cross-Talk (2023)
Rareshare
 Epidemiology of Pediatric Renal Diseases and its Histopathological Spectrum - A Single-Center Experience from India
Epidemiology of Pediatric Renal Diseases and its Histopathological Spectrum - A Single-Center Experience from India
 Ranjini Kudva | Department of Pathology | KMC Manipal, Manipal Academy of Higher Education
Ranjini Kudva | Department of Pathology | KMC Manipal, Manipal Academy of Higher Education
Pediatric Nephrology, Fifth Edition, by Elis D. Avner, William E. Harmon, Patrick Niaudet
 Apellis Pharmaceuticals Reports Third Quarter 2022 Financial Results | BioSpace
Apellis Pharmaceuticals Reports Third Quarter 2022 Financial Results | BioSpace
Dermatologic Manifestations of Renal Disease: Overview, Dermatologic Manifestations of Diseases Associated With ESRD,...
 Erowid.org: Erowid Reference 85 : Drugs of abuse and renal disease : Bakir AA, Dunea G
Erowid.org: Erowid Reference 85 : Drugs of abuse and renal disease : Bakir AA, Dunea G
 Rare Disease
Rare Disease
Rareshare
 World Journal of Gastroenterology - Baishideng Publishing Group
World Journal of Gastroenterology - Baishideng Publishing Group
Internal Medicine
 Incidence of glomerulonephritis in the western part of Switzerland over the last decade
| Swiss Medical Weekly
Incidence of glomerulonephritis in the western part of Switzerland over the last decade
| Swiss Medical Weekly
 Baby’s Pregnancy Calendar
Baby’s Pregnancy Calendar
 A Case Series of Gastrointestinal Tuberculosis in Renal Transplant Patients
A Case Series of Gastrointestinal Tuberculosis in Renal Transplant Patients
![Anti-C3d antibody [7C10] (ab17453) | Abcam](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAYAAAAf8/9hAAABm0lEQVQ4jaWTv0tbURTHP/cl75lqTIiNRFyEJIiUxNB2qf+D6NIuDg7WwcXFxU2yOznYte2klFIqpXVqoXQqgTYZKhURUURTlajJy++Xdx1eeJrmTc/vcuHc8/3cc869V8ileBZkClcSOcW9GUCmFPdmS16n4PfjKp/2KxQbJsmwxnwywOs/RUoNCcB0rI+xAbUb0DQls9tnbO7qHcC3OyWOigbn1RYA0aDXGbD8o8Dmro6qCOYS/Tx6qPHztMbGXx3Zzll5FuJppKe7hULNZD17jQA+TA0xGe21Nh4HmRj2sfjtAoDno36iQdUG2EPM5Gs0WpJ4SL01t7UwHqBPdZ63HTVMaxWOaWBK6Ri3AU8iPSgC9i6bfDmodCS9yhWpGs4AT3piIA3Qrykc6y1+ndV5v1cmX25xWGqy9vua1cyVbRh84GEk4CXk81gVy6WYja4YkpnP/9jaL3eckghrnOgGhZrV57vJCC9G/cB/19jrFXycHuLrUZXtgwpXdZPUoMbLZIA3dx5SMnx7jR0VuNG9/4ICIufaLWT2BlLHjkWr+SchAAAAAElFTkSuQmCC) Anti-C3d antibody [7C10] (ab17453) | Abcam
Anti-C3d antibody [7C10] (ab17453) | AbcamMPGN18
- Membranoproliferative glomerulonephritis (MPGN) is a type of glomerulonephritis caused by deposits in the kidney glomerular mesangium and basement membrane (GBM) thickening, activating complement and damaging the glomeruli. (wikipedia.org)
- Membranoproliferative glomerulonephritis (MPGN) is a form of glomerulonephritis caused by an abnormal immune response . (medlineplus.gov)
- Membranoproliferative glomerulonephritis (MPGN) is an uncommon cause of chronic nephritis that occurs primarily in children and young adults. (medscape.com)
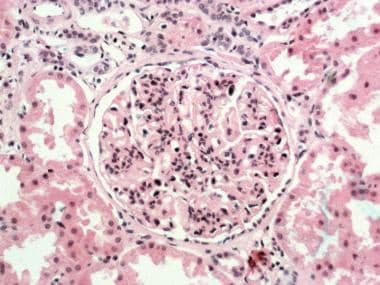
- Membranoproliferative glomerulonephritis (MPGN) type I. Glomerulus with lobular accentuation from increased mesangial cellularity. (medscape.com)
- Membranoproliferative glomerulonephritis (MPGN) type I. Immunofluorescent stained section. (medscape.com)
- Hypocomplementemia is a characteristic finding with all types of membranoproliferative glomerulonephritis (MPGN). (medscape.com)
- Complement factor B (FB) mutant variants are associated with excessive complement activation in kidney diseases such as atypical hemolytic uremic syndrome (aHUS), C3 glomerulopathy and membranoproliferative glomerulonephritis (MPGN). (lu.se)
- C3 Glomerulopathy (C3G) and Immune Complex-associated Membranoproliferative Glomerulonephritis (IC-MPGN) are diseases with distinct underlying pathophysiologic mechanisms. (pedsnet.org)
- Membranoproliferative glomerulonephritis , or MPGN, is a kidney disease triggered by immune deposits which end up in the walls of the glomerulus, which are the tufts of capillaries where blood is filtered. (osmosis.org)
- Membranoproliferative glomerulonephritis (MPGN) is characterized by a pattern of glomerular injury on light microscopy, including hypercellularity and thickening of the glomerular basement membrane. (msdmanuals.com)
- Membranoproliferative glomerulonephritis (MPGN) is characterized histologically by glomerular basement membrane (GBM) thickening and proliferative changes on light microscopy. (msdmanuals.com)
- Complement-mediated MPGN can be further categorized based on features observed on immunofluorescence and electron microscopy as C3 or C4 glomerulonephritis or dense deposition disease (DDD). (msdmanuals.com)
- Up until 2013, patients with C3G were diagnosed with membranoproliferative glomerulonephritis (MPGN) or mesangioproliferative glomerulonephritis. (rareshare.org)
- Histopathology, electron microscopy and immunohistochemistry were consistent with an immune-mediated membranoproliferative glomerulonephritis (MPGN). (vin.com)
- Although specific antigenic causes initiating glomerulonephritis were not determined in these pygmy marmosets, MPGN in humans can be triggered by chronic infections or parasitism. (vin.com)
- Membranoproliferative glomerulonephritis (MPGN) - This condition has been reported in about 20% of cases, and proteinuria, in 45% of cases. (medscape.com)
- 235400), membranoproliferative glomerulonephritis type II (MPGN II), and nonspecific hematuria or nephritis (Ault, 2000). (findzebra.com)
- This is a Phase 3 study to assess the efficacy and safety of twice-weekly subcutaneous (SC) doses of pegcetacoplan compared to placebo in patients with C3 glomerulopathy (C3G) or immune-complex membranoproliferative glomerulonephritis (IC-MPGN) on the basis of a reduction in proteinuria. (researcherprofiles.org)
Glomerulopathy2
- Acknowledgement of Membranoproliferative Glomerulonephritis (aka Complement 3 Glomerulopathy C3G) has not been added yet. (rareshare.org)
- The MHRA has received 13 Yellow Card reports of thrombotic microangioathy, haemolytic uraemic syndrome or thrombotic thrombocytopenic purpura and five Yellow Card reports of nephrotic syndromes (including collapsing focal segmental glomerulosclerosis, minimal-change disease, membranoproliferative glomerulonephritis and membranous glomerulopathy) linked to treatment with interferon beta . (mims.co.uk)
Acute glomerulonephritis8
- Infections with methicillin-resistant Staphylococcus aureus may cause acute glomerulonephritis by releasing bacterial superantigens. (erowid.org)
- The diagnosis of glomerular diseases: acute glomerulonephritis and the nephrotic syndrome. (smw.ch)
- Mice implanted with hybridoma secreting 6-19 IgG3 anti-IgG2a rheumatoid factor (RF) with cryoglobulin activity develop acute glomerulonephritis and cutaneous leukocytoclastic vasculitis. (unige.ch)
- IgA nephropathy also has no known cause, and can look like acute glomerulonephritis because of the blood seen in the urine. (childrenscolorado.org)
- Like acute glomerulonephritis, kidney function recovers in 85% of cases. (childrenscolorado.org)
- Acute glomerulonephritis usually presents with obvious blood (seen by the naked eye) in the urine. (childrenscolorado.org)
- Your child may not feel sick, but if you know that your child had a sore throat or some other infection a couple of weeks before this urine color change, your child may have acute glomerulonephritis. (childrenscolorado.org)
- However, if your child has blood in the urine that comes and goes, especially at times when he or she has an ongoing cold or some type of infection, they may not have acute glomerulonephritis, but IgA nephropathy instead. (childrenscolorado.org)
Renal disease1
- Glomerulonephritis is a rare yet serious group of diseases with a high risk of progression to end-stage renal disease. (smw.ch)
Membranous4
- It should not be confused with membranous glomerulonephritis, a condition in which the basement membrane is thickened, but the mesangium is not. (wikipedia.org)
- Membranous glomerulonephritis. (smw.ch)
- In patients presenting with nephrotic syndrome , distinguishing focal segmental glomerulosclerosis (FSGS) from other glomerular diseases (eg, minimal-change disease, mesangial proliferative glomerulonephritis, membranoproliferative glomerulonephritis, membranous glomerulonephritis) is clinically difficult. (medscape.com)
- The most common histological finding on kidney biopsy of patients with proteinuria owing to GVHD is membranous glomerulonephritis (MGN). (bvsalud.org)
Nephropathy1
- The same was true for the incidence of IgA nephropathy, lupus nephritis and pauci-immune glomerulonephritis. (smw.ch)
Vasculitis3
- Syed R, Rehman A, Valecha G, El-Sayegh S. Pauci-Immune Crescentic Glomerulonephritis: An ANCA-Associated Vasculitis. (smw.ch)
- More than 80% of patients with pauci-immune rapidly progressive glomerulonephritis were subsequently found to have circulating antineutrophil cytoplasmic antibodies (ANCAs), and, thus, this form of rapidly progressive glomerulonephritis is now termed ANCA-associated vasculitis. (medscape.com)
- In 1982, Davies et al first noted the presence of ANCAs in 8 patients with pauci-immune rapidly progressive glomerulonephritis and systemic vasculitis. (medscape.com)
Nephrotic syndrome2
- Okay so membranoproliferative glomerulonephritis is a type of nephrotic syndrome , got it. (osmosis.org)
- Serum immunoglobulins may be low in poorly selective proteinuric forms of nephrotic syndrome (focal glomerulonephritis). (mft.nhs.uk)
Cryoglobulinemia1
- Hepatitis C has supplanted hepatitis B and may give rise to membranoproliferative glomerulonephritis and cryoglobulinemia. (erowid.org)
Chronic4
- H-single and H/L-double transgenic mice displayed comparable high amounts of IgG3 cryoglobulins, but only H/L-double transgenic mice having 10-fold higher levels of IgG3 anti-IgG2a RF progressively developed chronic, lethal glomerulonephritis. (unige.ch)
- Membranoproliferative glomerulonephritis, a chronic (lifelong) condition. (childrenscolorado.org)
- In this special issue, Researchers and Specialist Registrars of University of Catania, Catanzaro and Messina (ITALY) focused on nephron-urological abnormalities in children, ranging from glomerular (nephrosic and Alport syndrome, chronic glomerulonephritis) and urologic diseases (multicystic dysplastic kidney, obstructive pathologies and stones). (biolifesas.org)
- Chronic glomerulonephritis characterized histologically by proliferation of MESANGIAL CELLS, increase in the MESANGIAL EXTRACELLULAR MATRIX, and a thickening of the glomerular capillary walls. (bvsalud.org)
Crescentic3
- p-ANCA associated glomerulonephritis is the common form of Necrotising crescentic glomerulonephritis, reflecting different vasculitic causes. (mft.nhs.uk)
- The ubiquitous pathological feature of crescentic glomerulonephritis is a focal rupture of glomerular capillary walls that can be seen by light microscopy and electron microscopy. (medscape.com)
- Several years later, the antiglomerular basement membrane (anti-GBM) antibody was discovered to produce a crescentic glomerulonephritis in sheep, and, following this discovery, the role of anti-GBM antibody in Goodpasture syndrome was elucidated. (medscape.com)
Complement2
- Complement 3 Glomerulonephritis (C3G) study is looking for volunteers. (rareshare.org)
- 1986) reported a consanguineous Algerian family in which 2 brothers had early-onset glomerulonephritis with C3 deposits and low levels (less than 10% of normal) of complement factor H . The factor H deficiency was defined by undetectable complement hemolytic activity by the classic (CH50) and alternate (AP50) pathways, and low levels of C3 and factor B (138470). (findzebra.com)
Dense2
- Most cases of dense deposit disease do not show a membranoproliferative pattern. (wikipedia.org)
- There are two types of C3G due to the two types of damage that can be done to the kidneys: dense deposit disease (DDD and C3 glomerulonephritis (C3GN). (rareshare.org)
Biopsy2
- Renal biopsy revealed membranoproliferative glomerulonephritis, with lobulated glomerular tufts, endocapillary proliferation, thickened basement membrane, and glomerular hyaline thrombi suggestive of cryoglobulin deposits. (who.int)
- A distinct feature of these cases was the virtual absence of antibody deposition after immunofluorescence staining of the biopsy specimens, which led to the label pauci-immune rapidly progressive glomerulonephritis. (medscape.com)
Pauci-immune1
- Rapidly progressive glomerulonephritis is classified pathologically into three categories, as follows: (1) anti-GBM antibody disease (approximately 3% of cases), (2) immune complex disease (45% of cases), and (3) pauci-immune disease (50% of cases). (medscape.com)
Patients4
- The incidence was calculated as the number of patients newly diagnosed with glomerulonephritis divided by the number of inhabitants of all the above-mentioned cantons during the year under review, as retrieved from the federal statistical office of Switzerland. (smw.ch)
- The term rapidly progressive glomerulonephritis was first used to describe a group of patients who had an unusually fulminant poststreptococcal glomerulonephritis and a poor clinical outcome. (medscape.com)
- In the mid 1970s, a group of patients was described who fit the clinical criteria for rapidly progressive glomerulonephritis but in whom no cause could be established. (medscape.com)
- [ 4 ] Patients with membranoproliferative glomerulonephritis are more likely to have low C3 levels and the presence of C3 nephritic factor (C3NeF). (medscape.com)
Diseases3
- [ 1 ] Hypertension accounts for approximately 26% of cases, and glomerulonephritis and cystic kidney diseases account for about 16%, although glomerulonephritis is not as prevalent as it was in the past. (medscape.com)
- There are other diseases that can involve the kidney filters and cause glomerulonephritis. (childrenscolorado.org)
- Glomerulonephritis can be seen in diseases such as Systemic Lupus Erythematosus (SLE) and Henoch-Schonlein Purpura (HSP) that affect other parts of the body. (childrenscolorado.org)
Hepatitis2
- Infectious causes of glomerulonephritis included streptococcal infections, human immunodeficiency virus (HIV) infection, and hepatitis viral infections, both hepatitis C (HCV) and hepatitis B (HBV). (medscape.com)
- Membranoproliferative glomerulonephritis associated with hepatitis B and C viral infections: from viruslike particles in the cryoprecipitate to viral localization in paramesangial deposits, problematic investigations prone to artifacts. (nih.gov)
Deposits2
- Membranoproliferative glomerulonephritis involves deposits at the intraglomerular mesangium. (wikipedia.org)
- Perivascular and glomerular immune complexes ( 2 , 4 , 5 ) can cause membranoproliferative glomerulonephritis ( 6 ) and segmental or circumferential arteritis ( 4 ) with mononuclear infiltration, fibrinoid necrosis and deposits, and increased intimal cellularity. (cdc.gov)
Kidney4
- Membranoproliferative glomerulonephritis is a kidney disorder that involves inflammation and changes to kidney cells. (medlineplus.gov)
- Glomerulonephritis is a condition in which the kidney filters become inflamed, causing blood to leak into urine. (childrenscolorado.org)
- In 85% of uncomplicated cases of post-strep glomerulonephritis, there is total kidney recovery. (childrenscolorado.org)
- Rapidly progressive glomerulonephritis (RPGN) is a disease of the kidney characterized clinically by a rapid decrease in the glomerular filtration rate (GFR) of at least 50% over a short period, from a few days to 3 months. (medscape.com)
20161
- Between 2007 and 2016, the incidence of all glomerulonephritis taken together remained stable. (smw.ch)
Diagnosis1
- Biopsies with a first diagnosis of primary glomerulonephritis were included in the analysis. (smw.ch)
Deficiency1
- 1982) reported 2 families with partial factor H deficiency and glomerulonephritis. (findzebra.com)
Type3
- A 2012 review considers DDD to be in a continuum with C3 glomerulonephritis, one reason the use of the type I to type III classification system is falling out of favour. (wikipedia.org)
- This study characterizes a specific type of glomerulonephritis in the pygmy marmoset ( Callithrix pygmaea ), which can progress to a hypertensive syndrome. (vin.com)
- Additional tests may help categorise the type of glomerulonephritis. (mft.nhs.uk)
Disease2
- C3 nephritic factor can cause membranoproliferative disease. (mft.nhs.uk)
- Soon afterward, the role of the anti-GBM antibody in rapidly progressive glomerulonephritis associated with Goodpasture disease was established. (medscape.com)
Inflammation1
- Glomerulonephritis is an inflammation of the glomeruli. (medlineplus.gov)
Clinical1
- Fakhouri F. Approche clinique des glomérulonéphrites membranoprolifératives primitives [Clinical approach to primary membranoproliferative glomerulonephritis]. (smw.ch)
Primary1
- The incidence of primary glomerulonephritis worldwide: a systematic review of the literature. (smw.ch)
Injury1
- Immunoglobulin-mediated glomerulonephritis with a membranoproliferative pattern of injury and cryoglobulinemic glomerulonephritis. (medlineplus.gov)
Adult2
- A retrospective study of adult pygmy marmosets (n=25) necropsied at the Smithsonian National Zoological Park, Washington, DC revealed a 56% prevalence of glomerulonephritis in this captive population. (vin.com)
- This article also only focuses on the adult population affected by rapidly progressive glomerulonephritis. (medscape.com)