Granuloma, Lethal Midline
Granuloma
Granuloma, Foreign-Body
Granuloma, Pyogenic
Eosinophilic Granuloma
Granuloma, Respiratory Tract
Granuloma Annulare
Sphenopalatine Ganglion Block
Headache
Pterygopalatine Fossa
Ganglia, Parasympathetic
Cluster Headache
Chicago
Midline destructive lesions of the sinonasal tract: simplified terminology based on histopathologic criteria. (1/16)
BACKGROUND AND PURPOSE: Destructive lesions of the sinonasal tract, lacking a discernible etiology and referred to as midline destructive disease, have been pathologically classified in accordance with a variety of confusing terms. Development of new pathologic concepts and immunohistochemical techniques has provided a fresh understanding of these lesions, and, as a result, they can be unified into two distinct pathologic groups: Wegener's granulomatosis and non-Hodgkin's T-cell lymphoma. METHODS: We retrospectively reviewed the imaging studies and pathologic specimens of seven patients with prior diagnoses included in the midline destructive disease group. The specimens were reviewed by an oral pathologist using currently accepted pathologic criteria and the newly available immunohistochemical markers CD20, CD45, and CD45RO. Lesions were classified as non-Hodgkin's T-cell lymphomas when positive for CD45 and CD45RO and negative for CD20, and as Wegener's granulomatosis in the presence of noncaseating multinucleated giant cell granulomas and necrotizing vasculitis. RESULTS: Three of the lesions were reclassified as Wegener's granulomatosis and four as T-cell lymphomas after applying these pathologic criteria. There were no distinguishing imaging findings between Wegener's granulomatosis and non-Hodgkin's T-cell lymphoma. CONCLUSION: The current pathologic classification for midline destructive disease should be incorporated into the radiologic lexicon and the use of terms from the old classification system, such as idiopathic midline granuloma and lethal midline granuloma, should be abandoned and no longer be used in radiologic reports. (+info)Characterization of novel natural killer (NK)-cell and gammadelta T-cell lines established from primary lesions of nasal T/NK-cell lymphomas associated with the Epstein-Barr virus. (2/16)
Studies on nasal T/natural killer (NK)-cell lymphoma have been hampered by its tendency to cause necrosis. Thus, the establishment of cell lines of this neoplasm would seem to be valuable. This study attempted to establish cell lines from primary lesions of this tumor, and successfully obtained 2 novel Epstein-Barr virus (EBV)-positive cell lines, SNK-6 and SNT-8, by means of high-dose recombinant interleukin 2. Flow cytometry showed that SNK-6 had an NK-cell phenotype, CD3- CD4- CD8- CD19- CD56+ T-cell receptor (TCR) alpha/beta- TCR gamma/delta-, whereas SNT-8 was CD3+ CD4- CD8- CD19- CD56+ TCR alpha/beta- TCR gamma/delta+. These were consistent with immunophenotypes of their original tumors, and the cell lines had monoclonal EBV clones identical to ones in their original tumors. Thus, the cell lines developed from cells forming the primary lesions. Genotypic analysis showed that SNK-6 had unrearranged TCR and immunoglobulin heavy-chain genes, supporting the conclusion that SNK-6 was of NK-cell lineage. On the other hand, SNT-8 had rearranged TCR beta-, gamma-, and delta-chain genes, and together with its phenotype, SNT-8 proved to be a gammadelta T-cell line. This is the first report of the establishment of cell lines from primary lesions of nasal T/NK cell lymphomas, and the results demonstrated that there are at least 2 lineages, NK- and gammadelta T-cell, in this neoplasm. Moreover, it has been suggested that nasal T/NK cell lymphomas of these lineages may belong to the same clinicopathologic entity because both types of cases shared common clinical and histopathologic features. (+info)Frequent mutations of Fas gene in nasal NK/T cell lymphoma. (3/16)
Fas (Apo-1/CD95) is a cell-surface receptor involved in cell death signaling through binding of Fas ligand. Mutation of Fas gene in lymphoid cells results in accumulation of these cells, which might thus contribute to lymphomagenesis. We examined the open reading frame of Fas cDNA in 14 cases of nasal NK/T-cell lymphoma. Mutations of Fas gene were detected in seven (50%) of 14 cases which comprised four frameshift, two missense, and one silent mutations. Frameshift mutations were caused by insertion of 1 bp (A) at nucleotide 1095 in two cases and by deletion of 1 bp at nucleotide 597 and at 704, respectively, in one each. Mouse T-cell lymphoma cells transfected with two missense mutated genes and frameshift mutations caused by insertion of 1 bp (A) at nucleotide 1095 were resistant to apoptosis induced by the anti-Fas antibody. These findings suggested that accumulation of lymphoid cells with Fas mutations provides a basis for the development of nasal NK/T-cell lymphoma. (+info)Re-irradiation of a second localization of idiopathic midline destructive disease in the head and neck area. (4/16)
Idiopathic midline destructive disease is a rare disease, characterized by a progressive ulceration and destruction of midline facial structures. We report a case with localization on the palate for which she received radiotherapy. Later she developed a second localization on the posterior pharyngeal wall for which she was re-irradiated, without severe sequels. Twice a complete regression was observed. (+info)Nasal NK/T cell lymphoma presenting as a lethal midline granuloma. (5/16)
Nasal NK/T cell lymphomas are aggressive, locally destructive, midfacial, necrotizing lesions. The nonspecific clinical symptoms constitute a major stumbling block in the early diagnosis and management of these lymphomas. We report here a case of probable nasal NK/T cell lymphoma in an apparently healthy male that progressed rapidly in a short span of time and was managed subsequently with chemotherapy and external beam irradiation with which the lesion regressed. (+info)Functional characterization of antineutrophil cytoplasmic antibodies in patients with cocaine-induced midline destructive lesions. (6/16)
(+info)Brain-derived neurotrophic factor Val/Met polymorphism and bipolar disorder. Association of the Met allele with suicidal behavior of bipolar patients. (7/16)
(+info)Erythematous indurated swelling on nose and upper lip. Cutaneous T cell lymphoma. (8/16)
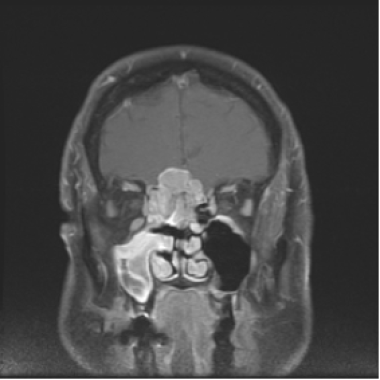
A 40-year-old man presented for diagnosis with nodules and plaques of the nose and upper lip, progessive over 1(1/2) years. (+info)A lethal midline granuloma (LMG) is a rare and aggressive form of necrotizing granulomatous inflammation that typically involves the nasopharynx, paranasal sinuses, and/or the central nervous system. It is called "lethal" because of its rapid progression and high mortality rate if left untreated.
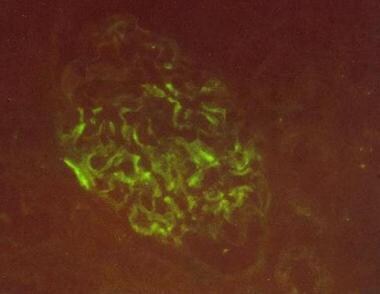
LMG is a type of granuloma, which is a collection of immune cells that form in response to chronic inflammation or infection. In LMG, the granulomas are characterized by extensive necrosis (tissue death) and vasculitis (inflammation of blood vessels).
The exact cause of LMG is not fully understood, but it is believed to be associated with a variety of factors, including infections (such as fungal or mycobacterial infections), autoimmune disorders, and lymphoproliferative diseases. Treatment typically involves a combination of surgical debridement, antimicrobial therapy, and immunosuppressive drugs. Despite treatment, the prognosis for LMG is generally poor, with a high rate of recurrence and significant morbidity and mortality.
Nose neoplasms refer to abnormal growths or tumors in the nasal cavity or paranasal sinuses. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow-growing and do not spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and have the potential to metastasize.
Nose neoplasms can cause various symptoms such as nasal congestion, nosebleeds, difficulty breathing through the nose, loss of smell, facial pain or numbness, and visual changes if they affect the eye. The diagnosis of nose neoplasms usually involves a combination of physical examination, imaging studies (such as CT or MRI scans), and biopsy to determine the type and extent of the growth. Treatment options depend on the type, size, location, and stage of the neoplasm and may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
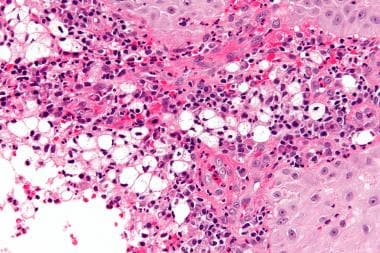
A granuloma is a small, nodular inflammatory lesion that occurs in various tissues in response to chronic infection, foreign body reaction, or autoimmune conditions. Histologically, it is characterized by the presence of epithelioid macrophages, which are specialized immune cells with enlarged nuclei and abundant cytoplasm, often arranged in a palisading pattern around a central area containing necrotic debris, microorganisms, or foreign material.
Granulomas can be found in various medical conditions such as tuberculosis, sarcoidosis, fungal infections, and certain autoimmune disorders like Crohn's disease. The formation of granulomas is a complex process involving both innate and adaptive immune responses, which aim to contain and eliminate the offending agent while minimizing tissue damage.
A granuloma is a type of organized immune response that occurs when the body encounters a foreign substance that it cannot eliminate. A "foreign-body" granuloma specifically refers to this reaction in response to an exogenous material, such as a splinter, suture, or other types of medical implants.
Foreign-body granulomas are characterized by the formation of a collection of immune cells, including macrophages and lymphocytes, which surround and attempt to isolate the foreign material. Over time, this collection of immune cells can become walled off and form a well-circumscribed mass or nodule.
Foreign-body granulomas may cause localized symptoms such as pain, swelling, or inflammation, depending on their location and size. In some cases, they may also lead to complications such as infection or tissue damage. Treatment typically involves removing the foreign body, if possible, followed by anti-inflammatory therapy to manage any residual symptoms or complications.
A pyogenic granuloma is not precisely a "granuloma" in the strict medical definition, which refers to a specific type of tissue reaction characterized by chronic inflammation and the formation of granulation tissue. Instead, a pyogenic granuloma is a benign vascular tumor that occurs most frequently on the skin or mucous membranes.
Pyogenic granulomas are typically characterized by their rapid growth, bright red to dark red color, and friable texture. They can bleed easily, especially when traumatized. Histologically, they consist of a mass of small blood vessels, surrounded by loose connective tissue and inflammatory cells.
The term "pyogenic" is somewhat misleading because these lesions are not actually associated with pus or infection, although they can become secondarily infected. The name may have originated from the initial mistaken belief that these lesions were caused by a bacterial infection.
Pyogenic granulomas can occur at any age but are most common in children and young adults. They can be caused by minor trauma, hormonal changes, or underlying medical conditions such as pregnancy or vasculitis. Treatment typically involves surgical excision, although other options such as laser surgery or cauterization may also be used.
Eosinophilic granuloma is a term used in pathology to describe a specific type of inflammatory lesion that is characterized by the accumulation of eosinophils, a type of white blood cell, and the formation of granulomas. A granuloma is a small nodular structure formed by the accumulation of immune cells, typically including macrophages, lymphocytes, and other inflammatory cells.
Eosinophilic granulomas can occur in various organs of the body, but they are most commonly found in the lungs, skin, and bones. In the lungs, eosinophilic granulomas are often associated with hypersensitivity reactions to inhaled antigens, such as dust mites or fungal spores. They can also be seen in association with certain diseases, such as Langerhans cell histiocytosis, an uncommon disorder characterized by the abnormal proliferation of a type of immune cell called Langerhans cells.
The symptoms of eosinophilic granuloma depend on the location and extent of the lesion. In the lungs, eosinophilic granulomas may cause cough, chest pain, or shortness of breath. In the skin, they may present as nodules, plaques, or ulcers. In the bones, they can cause pain, swelling, and fractures.
The diagnosis of eosinophilic granuloma is typically made based on a combination of clinical, radiological, and pathological findings. Treatment may include avoidance of known antigens, corticosteroids, or other immunosuppressive medications, depending on the severity and location of the lesion.
A granuloma in the respiratory tract refers to a small nodular lesion that forms in the lung tissue due to an ongoing immune response. It is typically composed of macrophages, lymphocytes, and other inflammatory cells that cluster together around a foreign substance or organism that the body cannot eliminate.
Granulomas can form in response to various stimuli, including infectious agents such as mycobacteria (tuberculosis, nontuberculous mycobacteria), fungi, and parasites, as well as non-infectious causes like inhaled particles (e.g., silica, beryllium) or autoimmune diseases (e.g., sarcoidosis).
These lesions can cause damage to the lung tissue over time, leading to symptoms such as cough, shortness of breath, chest pain, and fatigue. Diagnosis often involves imaging studies like chest X-rays or CT scans, followed by biopsy and microscopic examination to confirm the presence of granulomas and identify the underlying cause. Treatment depends on the underlying cause but may include antibiotics, corticosteroids, or other immunosuppressive medications.
Granuloma annulare is a chronic, inflammatory skin condition characterized by the formation of small, red or flesh-colored bumps that form rings or arcs. These lesions are usually found on the hands and feet but can occur anywhere on the body. The exact cause of granuloma annulare is unknown, but it may be associated with triggers such as insect bites, viral infections, sun exposure, or certain medications.
Histologically, granuloma annulare is characterized by a specific type of inflammatory cell infiltrate, consisting of histiocytes (a type of white blood cell) arranged in palisades around the edges of small collections of mucin (a glycoprotein). This distinctive pattern helps to differentiate granuloma annulare from other skin conditions.
Granuloma annulare is generally a benign condition that does not cause any symptoms or complications, although some people may experience itching or discomfort in the affected areas. In most cases, the lesions will resolve on their own within a few months to two years, although they can recur in some individuals. Treatment options for granuloma annulare include topical corticosteroids, phototherapy, and intralesional steroid injections, although observation is also a reasonable approach in many cases.
A Sphenopalatine Ganglion Block (SPG Block) is a medical procedure that involves the injection of a local anesthetic agent near the sphenopalatine ganglion, a collection of nerve cells located in the upper part of the nasopharynx, near the sphenoid bone. This procedure is typically used to diagnose or treat various types of headaches and facial pain, including cluster headaches, migraines, and trigeminal neuralgia.
The injection is usually administered through the nose using a long, thin needle, although it can also be performed via the roof of the mouth (greater palatine foramen) or the side of the face (via the infraorbital foramen). Once the needle is in position, the anesthetic agent is injected, which numbs the sphenopalatine ganglion and interrupts the transmission of pain signals to the brain.
The effects of the SPG Block can be immediate and may last for several hours or days, depending on the individual and the type of anesthetic used. Some people may require repeated blocks over time to achieve lasting relief from their symptoms. Potential risks and complications associated with this procedure are generally low but may include bleeding, infection, or trauma to surrounding tissues.
Bupivacaine is a long-acting local anesthetic drug, which is used to cause numbness or loss of feeling in a specific area of the body during certain medical procedures such as surgery, dental work, or childbirth. It works by blocking the nerves that transmit pain signals to the brain.
Bupivacaine is available as a solution for injection and is usually administered directly into the tissue surrounding the nerve to be blocked (nerve block) or into the spinal fluid (epidural). The onset of action of bupivacaine is relatively slow, but its duration of action is long, making it suitable for procedures that require prolonged pain relief.
Like all local anesthetics, bupivacaine carries a risk of side effects such as allergic reactions, nerve damage, and systemic toxicity if accidentally injected into a blood vessel or given in excessive doses. It should be used with caution in patients with certain medical conditions, including heart disease, liver disease, and neurological disorders.
A headache is defined as pain or discomfort in the head, scalp, or neck. It can be a symptom of various underlying conditions such as stress, sinus congestion, migraine, or more serious issues like meningitis or concussion. Headaches can vary in intensity, ranging from mild to severe, and may be accompanied by other symptoms such as nausea, vomiting, or sensitivity to light and sound. There are over 150 different types of headaches, including tension headaches, cluster headaches, and sinus headaches, each with their own specific characteristics and causes.
The pterygopalatine fossa is a small, irregularly shaped space located in the skull, lateral to the nasal cavity and inferior to the orbit. It serves as a critical communications center for several important nerves, arteries, and veins that provide sensory innervation, vasomotor control, and blood supply to various structures in the head and neck region.
The following are some key components of the pterygopalatine fossa:
1. Nerves: The pterygopalatine ganglion is a major component of this fossa, which contains postganglionic parasympathetic fibers, sympathetic fibers, and sensory fibers from various nerves, including the maxillary nerve (V2), greater petrosal nerve, deep petrosal nerve, and nerve of the pterygoid canal.
2. Arteries: The maxillary artery, a branch of the external carotid artery, enters the fossa through the foramen rotundum and divides into several branches that supply various structures in the head and neck region, such as the sphenopalatine artery, posterior superior alveolar artery, infraorbital artery, and greater palatine artery.
3. Veins: The pterygoid venous plexus is a complex network of veins located in and around the fossa that communicates with various venous systems, including the facial vein, cavernous sinus, and inferior ophthalmic vein.
The pterygopalatine fossa plays an essential role in several physiological functions, such as lacrimation, salivation, and vasodilation of blood vessels in the nasal cavity and paranasal sinuses. Additionally, it is a potential site for the spread of infection or neoplasm from the oral cavity, nasal cavity, or paranasal sinuses to other regions of the head and neck.
Parasympathetic ganglia are collections of neurons located outside the central nervous system (CNS) that serve as relay stations for parasympathetic nerve impulses. The parasympathetic nervous system is one of the two subdivisions of the autonomic nervous system, which controls involuntary physiological responses.
The parasympathetic ganglia receive preganglionic fibers from the brainstem and sacral regions of the spinal cord. After synapsing in these ganglia, postganglionic fibers innervate target organs such as the heart, glands, and smooth muscles. The primary function of the parasympathetic nervous system is to promote rest, digestion, and energy conservation.
Parasympathetic ganglia are typically located close to or within the target organs they innervate. Examples include:
1. Ciliary ganglion: Innervates the ciliary muscle and iris sphincter in the eye, controlling accommodation and pupil constriction.
2. Pterygopalatine (sphenopalatine) ganglion: Supplies the lacrimal gland, mucous membranes of the nasal cavity, and palate, regulating tear production and nasal secretions.
3. Otic ganglion: Innervates the parotid gland, controlling salivary secretion.
4. Submandibular ganglion: Supplies the submandibular and sublingual salivary glands, regulating salivation.
5. Sacral parasympathetic ganglia: Located in the sacrum, they innervate the distal colon, rectum, and genitourinary organs, controlling defecation, urination, and sexual arousal.
These parasympathetic ganglia play crucial roles in maintaining homeostasis by regulating various bodily functions during rest and relaxation.
A cluster headache is a type of primary headache disorder characterized by severe, one-sided headaches that occur in clusters, meaning they happen several times a day for several weeks or months and then go into remission for a period of time. The pain of a cluster headache is typically intense and often described as a sharp, stabbing, or burning sensation around the eye or temple on one side of the head.
Cluster headaches are relatively rare, affecting fewer than 1 in 1000 people. They tend to affect men more often than women and usually start between the ages of 20 and 50. The exact cause of cluster headaches is not fully understood, but they are thought to be related to abnormalities in the hypothalamus, a part of the brain that regulates various bodily functions, including hormone production and sleep-wake cycles.
Cluster headache attacks can last from 15 minutes to several hours and may be accompanied by other symptoms such as redness or tearing of the eye, runny nose, sweating, or swelling on the affected side of the face. During a cluster period, headaches typically occur at the same time each day, often at night or in the early morning.
Cluster headaches can be treated with various medications, including triptans, oxygen therapy, and local anesthetics. Preventive treatments such as verapamil, lithium, or corticosteroids may also be used to reduce the frequency and severity of cluster headache attacks during a cluster period.
I apologize, but "Chicago" is not a medical term or concept. Chicago is the largest city in the state of Illinois and the third-most populous city in the United States. It's known for its impressive architecture, vibrant arts scene, and significant contributions to American culture, including jazz music, improvisational theater, and culinary innovations like deep-dish pizza and the Chicago-style hot dog.
If you have any questions related to medical topics or definitions, please feel free to ask!
 Lethal midline granuloma
Lethal midline granuloma
Granulomatosis with polyangiitis
List of diseases (M)
List of MeSH codes (C23)
Indolent T cell lymphoproliferative disorder of the gastrointestinal tract
Ameloblastoma
List of skin conditions
Lethal midline granuloma - Wikipedia
 October 1976 - Volume 58 - Issue 4 : Plastic and Reconstructive Surgery
October 1976 - Volume 58 - Issue 4 : Plastic and Reconstructive Surgery
 Cutaneous Leishmaniasis: Recognition and Treatment | AAFP
Cutaneous Leishmaniasis: Recognition and Treatment | AAFP
 ICD-9 Code DISEASES OF ARTERIES, ARTERIOLES, AND CAPILLARIES 440-449- Codify By AAPC
ICD-9 Code DISEASES OF ARTERIES, ARTERIOLES, AND CAPILLARIES 440-449- Codify By AAPC
 The Presumptive Conditions List for Burn Pits Veterans Disability
The Presumptive Conditions List for Burn Pits Veterans Disability
 Lymphomatoid Papulosis: Background, Pathophysiology, Etiology
Lymphomatoid Papulosis: Background, Pathophysiology, Etiology
 Serous fluids and hematolymphoid disorders - CytoJournal
Serous fluids and hematolymphoid disorders - CytoJournal
 International Classification of Diseases - Diseases of the Circulatory System
International Classification of Diseases - Diseases of the Circulatory System
CDC/NIH Web Information Database|Home|PHGKB
 MeSH Browser
MeSH Browser
HuGE Navigator|Genopedia|PHGKB
Bio2Vec
VEGF165 Protein - ACROBiosystems
Bio2Vec
 Dentosphere : World of Dentistry: General Pathology MCQs - Cell in Health and Disease
Dentosphere : World of Dentistry: General Pathology MCQs - Cell in Health and Disease
 Characterization of novel natural killer (NK)-cell and γδ T-cell lines established from primary lesions of nasal T/NK-cell...
Characterization of novel natural killer (NK)-cell and γδ T-cell lines established from primary lesions of nasal T/NK-cell...
 Stomatitis - Dental Disorders - MSD Manual Professional Edition
Stomatitis - Dental Disorders - MSD Manual Professional Edition
Sphenopalatine Ganglion (SPG) Blocks | SPG Blocks | Chicago
 Granulomatosis with polyangiitis and microscopic polyangiitis: Respiratory tract involvement
Granulomatosis with polyangiitis and microscopic polyangiitis: Respiratory tract involvement
SAS VALUE LABELS FOR 1993 NHAMCS OUTPATIENT DEPARTMENT PUBLIC USE FILE
ICD Codes. ICD-10 Central Data Repository.. ICD10 Codes M300 (Polyarteritis nodosa) - M342 (Systemic sclerosis induced by drug...
Paranasal Sinus Diseases | Profiles RNS
 Rhinitis | Profiles RNS
Rhinitis | Profiles RNS
 Rhinosporidiosis - An overview | Capsule Health
Rhinosporidiosis - An overview | Capsule Health
 DeCS
DeCS
Archives of Head and Neck Surgery - Volume 49 / Issue
Sphenopalatine Ganglion (SPG) Blocks | SPG Blocks | Chicago
URBACH-WIETHE DISEASE: EXPERIENCE AT A TERTIARY CARE HOSPITAL IN ABBOTTABAD, PAKISTAN | Journal of Ayub Medical College...
 Namespace
Namespace
Granulomatosis with polyangiitis2
- Subsequent studies found that the cells infiltrating the midline tissues in cases of lethal midline granuloma that were not clearly diagnosed as granulomatosis with polyangiitis were: a) infected by the Epstein-Barr virus and b) consisted of malignant lymphocytes, usually NK cells or, rarely, cytotoxic T cells. (wikipedia.org)
- Since cases of LMG that were manifestations of granulomatosis with polyangiitis, a vascular inflammatory but not malignant disease, the term lethal midline granuloma is considered confusing and obsolete. (wikipedia.org)
Facial2
- Patients presenting with highly localized midline facial disease fit the historical definition of lethal midline granuloma. (wikipedia.org)
- A condition that is characterized by inflammation, ulceration, and perforation of the nose and the PALATE with progressive destruction of midline facial structures. (nih.gov)
Term2
- Lethal midline granuloma (LMG) is an historical term for a condition in which necrotic and highly destructive lesions develop progressively in the middle of the face, principally the nose and palate. (wikipedia.org)
- The term was used as a synonym for lethal midline granuloma. (nih.gov)
Malignant5
- Subsequent studies found that the cells infiltrating the midline tissues in cases of lethal midline granuloma that were not clearly diagnosed as granulomatosis with polyangiitis were: a) infected by the Epstein-Barr virus and b) consisted of malignant lymphocytes, usually NK cells or, rarely, cytotoxic T cells. (wikipedia.org)
- Since cases of LMG that were manifestations of granulomatosis with polyangiitis, a vascular inflammatory but not malignant disease, the term lethal midline granuloma is considered confusing and obsolete. (wikipedia.org)
- Biopsy findings in malignant histiocytosis presenting as lethal midline granuloma. (bmj.com)
- Nasal biopsy findings in malignant histiocytosis presenting clinically as lethal midline granuloma are characterised by necrosis and infiltration of atypical histiocytic cells with a diffuse positive reaction for non-specific esterase. (bmj.com)
- This cellular character was common to midline malignant reticulosis, and midline malignant reticulosis and malignant histiocytosis are thought to be the same disease. (bmj.com)
Lymphoma1
- 19. Extranodal natural killer/T-cell lymphoma, nasal type: 'midline lethal granuloma. (nih.gov)
Lesions2
- Lethal midline granuloma (LMG) is an historical term for a condition in which necrotic and highly destructive lesions develop progressively in the middle of the face, principally the nose and palate. (wikipedia.org)
- Destructive midline facial lesions have conventionally been referred to as lethal midline granuloma. (openpr.com)
Synonym1
- The term was used as a synonym for lethal midline granuloma. (nih.gov)