Hyperkalemia
Hypoaldosteronism
Pseudohypoaldosteronism
Potassium
Spironolactone
Hypokalemia
Mineralocorticoid Receptor Antagonists
Sodium Bicarbonate
Acidosis
Aldosterone
Cation Exchange Resins
Sodium Chloride Symporters
Succinylcholine
Polystyrenes
Angiotensin-Converting Enzyme Inhibitors
Enhanced exercise-induced hyperkalemia in patients with syndrome X. (1/356)
OBJECTIVES: The purpose of this study was to determine whether patients with syndrome X have altered potassium metabolism. BACKGROUND: Patients with syndrome X have angina pectoris and exercise induced ST segment depression on the electrocardiogram despite normal coronary angiograms. Increasing evidence suggests that myocardial ischemia is uncommon in these patients. Altered potassium metabolism causing interstitial potassium accumulation in the myocardium may be an alternative mechanism for chest pain and ST segment depression in syndrome X. METHODS: We compared the magnitude of exercise-induced hyperkalemia in 16 patients with syndrome X (12 female and four male, mean +/- SD age 53 +/- 6 years) and 15 matched healthy control subjects. The participants underwent a bicycle test at a fixed load of 75 W for 10 min, and blood samples were taken for analysis of potassium, catecholamines and lactate before, during and in the recovery period after exercise. In five patients with syndrome X, the test was repeated during alpha1 adrenoceptor blockade. RESULTS: Baseline concentrations of serum potassium, plasma catecholamines and plasma lactate were similar in patients and control subjects. The rate of exercise-induced increment of serum potassium was increased in the patients (70 +/- 29 vs. 30 +/- 21 micromol/liter/min in control subjects, p < 0.001). Six patients, who stopped before 10 min of exercise, showed very rapid increments in serum potassium concentration. Compared to the control subjects, patients also demonstrated larger increments in rate-pressure product, plasma norepinephrine and lactate concentrations during exercise. The rate of serum potassium increment correlated with the rate of plasma norepinephrine increment in the patients (r = 0.63, p < 0.02), but not in the control subjects (r = 0.01, p = 0.97). Blockade of alpha1 adrenoceptors decreased systolic blood pressure at baseline, but did not influence the increment of serum potassium, plasma catecholamines and lactate. CONCLUSIONS: Patients with syndrome X have enhanced exercise induced hyperkalemia in parallel with augmented increases of circulating norepinephrine and lactate. The prevailing mechanisms behind the abnormal potassium handling comprise sources distinct from alpha1-adrenoceptor activation. (+info)Familial pseudohyperkalemia maps to the same locus as dehydrated hereditary stomatocytosis (hereditary xerocytosis). (2/356)
Familial pseudohyperkalemia is a "leaky red blood cell" condition in which the cells show a temperature-dependent loss of potassium (K) from red blood cells when stored at room temperature, manifesting as apparent hyperkalemia. The red blood cells show a reduced lifespan in vivo but there is no frank hemolysis. Studies of cation content and transport show a marginal increase in permeability at 37 degrees C and a degree of cellular dehydration, qualitatively similar to the changes seen in dehydrated hereditary stomatocytosis (hereditary xerocytosis). Physiological studies have shown that the passive leak to K has an abnormal temperature dependence, such that the leak is less sensitive to temperature than that in normal cells. We performed genetic mapping on the original family and found that the condition in this kindred maps to the same locus (16q23-ter) that we have previously identified for an Irish family with dehydrated hereditary stomatocytosis, which does not show the same temperature effects. (+info)A case of aldosterone-producing adenoma with severe postoperative hyperkalemia. (3/356)
It is known that some patients with primary aldosteronism show postoperative hyperkalemia, which is due to inability of the adrenal gland to secrete sufficient amounts of aldosterone. However, hyperkalemia is generally neither severe nor prolonged, in which replacement therapy with mineralocorticoid is seldom necessary. We report a case of a 46-year-old woman with an aldosterone-producing adenoma associated with severe postoperative hyperkalemia. After unilateral adrenalectomy, the patient showed episodes of severe hyperkalemia for four months, which required not only cation-exchange resin, but also mineralocorticoid replacement. Plasma aldosterone concentration (PAC) was low, although PAC was increased after rapid ACTH test. Histological examination indicated the presence of adrenocortical tumor and paradoxical hyperplasia of zona glomerulosa in the adjacent adrenal. Immunohistochemistry demonstrated that the enzymes involved in aldosterone synthesis, such as cholesterol side chain cleavage (P-450scc), 3beta-hydroxysteroid dehydrogenase (3beta-HSD), and 21-hydroxylase (P-450c21), or the enzyme involved in glucocorticoid synthesis, 11beta-hydroxylase (P-450c11beta), were expressed in the tumor, but they were completely absent in zona glomerulosa of the adjacent adrenal. These findings were consistent with the patterns of primary aldosteronism. Serum potassium level was gradually decreased with concomitant increase in PAC. These results suggest that severe postoperative hyperkalemia of the present case was attributable to severe suppression of aldosterone synthesis in the adjacent and contralateral adrenal, which resulted in slow recovery of aldosterone secretion. It is plausible that aldosterone synthesis of adjacent and contralateral adrenal glands is severely impaired in some cases with primary aldosteronism, as glucocorticoid synthesis in Cushing syndrome. (+info)Hyperkalaemic paralysis--a bizarre presentation of renal failure. (4/356)
Paralysis due to hyperkalaemia is rare and the diagnosis may be overlooked in the first instance. However it is rapidly reversible and so long as electro-cardiography and serum potassium measurement are urgently done in all patients presenting with paralysis, it will not be missed. A case of hyperkalaemic paralysis is described and a review of the emergency management discussed. (+info)Activation and inactivation of the voltage-gated sodium channel: role of segment S5 revealed by a novel hyperkalaemic periodic paralysis mutation. (5/356)
Hyperkalaemic periodic paralysis, paramyotonia congenita, and potassium-aggravated myotonia are three autosomal dominant skeletal muscle disorders linked to the SCN4A gene encoding the alpha-subunit of the human voltage-sensitive sodium channel. To date, approximately 20 point mutations causing these disorders have been described. We have identified a new point mutation, in the SCN4A gene, in a family with a hyperkalaemic periodic paralysis phenotype. This mutation predicts an isoleucine-to-phenylalanine substitution at position 1495 located in the transmembrane segment S5 in the fourth homologous domain of the human alpha-subunit sodium channel. Introduction of the I1495F mutation into the wild-type channels disrupted the macroscopic current inactivation decay and shifted both steady-state activation and inactivation to the hyperpolarizing direction. The recovery from fast inactivation was slowed, and there was no effect on channel deactivation. Additionally, a significant enhancement of slow inactivation was observed in the I1495F mutation. In contrast, the T704M mutation, a hyperkalaemic periodic paralysis mutation located in the cytoplasmic interface of the S5 segment of the second domain, also shifted activation in the hyperpolarizing direction but had little effect on fast inactivation and dramatically impaired slow inactivation. These results, showing that the I1495F and T704M hyperkalaemic periodic paralysis mutations both have profound effects on channel activation and fast-slow inactivation, suggest that the S5 segment maybe in a location where fast and slow inactivation converge. (+info)Hyperkalemia in patients infected with the human immunodeficiency virus: involvement of a systemic mechanism. (6/356)
BACKGROUND: The appearance of hyperkalemia has been described in human immunodeficiency virus (HIV)-positive patients treated with drugs with amiloride-like properties. Recent in vitro data suggest that individuals infected with HIV have alterations in transcellular K+ transport. METHODS: With the objective of examining the presence of alterations in transmembrane K+ equilibrium in HIV-positive patients, we designed a prospective, interventional study involving 10 HIV-positive individuals and 10 healthy controls, all with normal renal function. An infusion of L-arginine (6%, intravenously, in four 30-min periods at 50, 100, 200, and 300 ml/hr) was administered, and plasma and urine electrolytes, creatinine, pH and osmolality, total and fractional sodium and potassium excretion, transtubular potassium gradient, plasma insulin, renin, aldosterone, and cortisol were measured. RESULTS: A primary disturbance consisting of a significant rise in plasma [K+] induced by L-arginine was detected in only the HIV patients but not in the controls (P < 0.001 between groups). A K+ redistribution origin of the hyperkalemia was supported by its rapid development (within 60 min) and the lack of significant differences between HIV-positive individuals and controls in the amount of K+ excreted in the urine. The fact that the HIV-positive individuals had an inhibited aldosterone response to the increase in plasma K+ suggested a putative mechanism for the deranged K+ response. CONCLUSIONS: These results reveal that HIV-infected individuals have a significant abnormality in systemic K+ equilibrium. This abnormality, which leads to the development of hyperkalemia after the L-arginine challenge, may be related, in part, to a failure in the aldosterone response to hyperkalemia. These results provide a new basis for understanding the pathogenesis of hyperkalemia in HIV individuals, and demonstrate that the risk of HIV-associated hyperkalemia exists even in the absence of amiloride-mimicking drugs or overt hyporeninemic hypoaldosteronism. (+info)The effect of potassium chloride infusion of parotid salivary flow and composition in conscious sheep. (7/356)
The composition and flow of parotid saliva in conscious sheep was measured before, during and after the intravenous infusion of 0-43 M-KCl or 0-43 M-NaCl at 2 ml./min for 2 hr. The salivary flow rate was depressed during the infusion of potassium chloride into both intact sheep and adrenalectomized sheep. As the salivary flow was unchanged by sodium chloride infusion it was concluded that the potassium ion was responsible for the decrease in flow and that this effect was not mediated through any of the adrenal hormones. The highly significant negative correlation between plasma potassium concentration and salivary flow throughout all potassium infusions indicated that the extent to which the salivary flow was depressed varied with the degree of hyperkalaemia. Except for situations where mineralocorticoid levels were likely to be elevated the concentrations of sodium and potassium in the saliva were positively correlated with the plasma concentrations of these ions. The salivary bicarbonate concentration of the saliva was negatively related to flow. The chloride concentration of the saliva was negatively correlated with salivary flow during all potassium chloride infusions. (+info)Changes in renal haemodynamics and electrolyte excretion during acute hyperkalemia in conscious adrenalectomized sheep. (8/356)
The p-aminohippurate (PAH) clearance, inulin clearance and the excretion of electrolytes by 10 adrenalectomized sheep were measured before, during and after the infusion of 0-43 M-KCl at 2 ml./min for 2 hr. The PAH clearance increased as the plasma potassium concentration increased up to approximately 6-0 m-mole/l. Further increases in plasma potassium were associated with a progressive return of the PAH clearance to or below the pre-infusion levels. At its maximum the PAH clearance was 1-228 +/- 0-032 (S.E. of mean) times the pre-infusion levels. The inulin clearance increased to reach a mazimum coincident with or subsequent to the maximum PAH clearance. The maximum level of inulin clearance during the hyperkalaemia was 1-158 +/- 0-020 times the pre-infusion clearance. The increments in the clearance of potassium and of bicarbonate rose rapidly to exceed the increment in inulin clearance during the hyperkalaemia in all experiments. The increments in the clearance of sodium and of chloride exceeded the increment in inulin clearance in more than half the experiments. It was concluded that although hyperkalaemia was associated with increased glomerular filtration much of the increased excretion of sodium, chloride and bicarbonate was derived from depressed tubular reabsorption of the ions. When the infusion experiments were repeated on the same animals the sheep demonstrated an improved ability to control the rise in plasma potassium concentration which was similar to potassium adaptation described in other species. There were no apparent differences between sheep maintained on 1-5 mg and 5 mg deoxycorticosterone acetate daily in their adaptation to potassium loading and the effect was tentatively attributed to the level of steroid maintenance being chronically high. The toxicity of hyperkalaemia was not lessened by this adaptation to potassium loading. (+info)Hyperkalemia is a medical condition characterized by an elevated level of potassium (K+) in the blood serum, specifically when the concentration exceeds 5.0-5.5 mEq/L (milliequivalents per liter). Potassium is a crucial intracellular ion that plays a significant role in various physiological processes, including nerve impulse transmission, muscle contraction, and heart rhythm regulation.
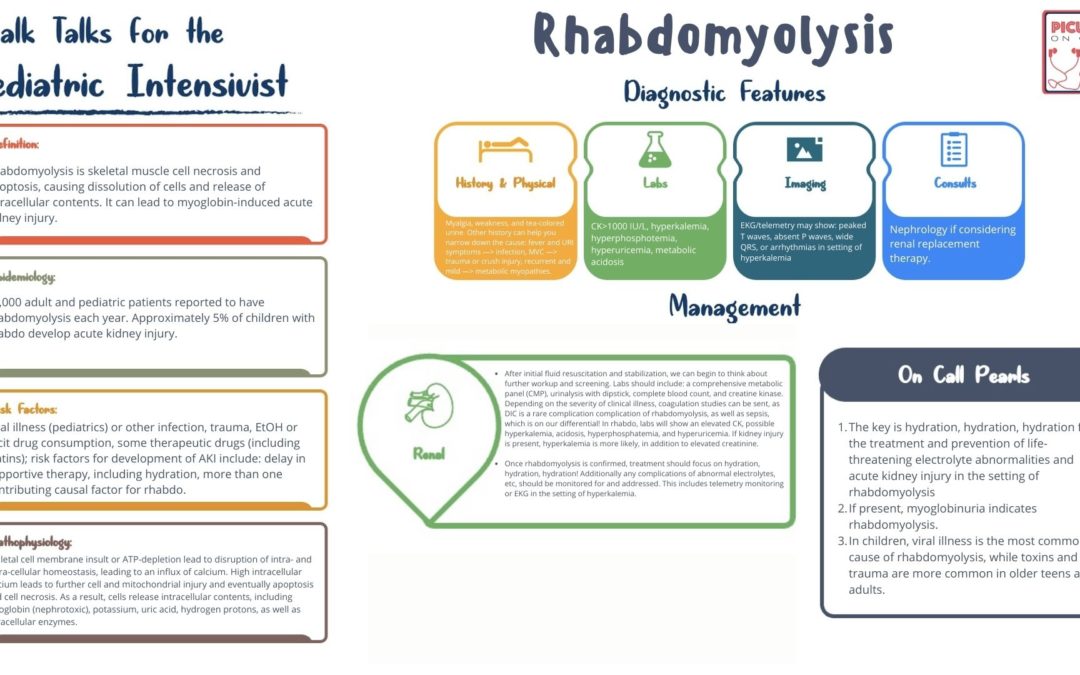
Mild to moderate hyperkalemia might not cause noticeable symptoms but can still have harmful effects on the body, particularly on the cardiovascular system. Severe cases of hyperkalemia (potassium levels > 6.5 mEq/L) can lead to potentially life-threatening arrhythmias and heart failure.
Hyperkalemia may result from various factors, such as kidney dysfunction, hormonal imbalances, medication side effects, trauma, or excessive potassium intake. Prompt identification and management of hyperkalemia are essential to prevent severe complications and ensure proper treatment.
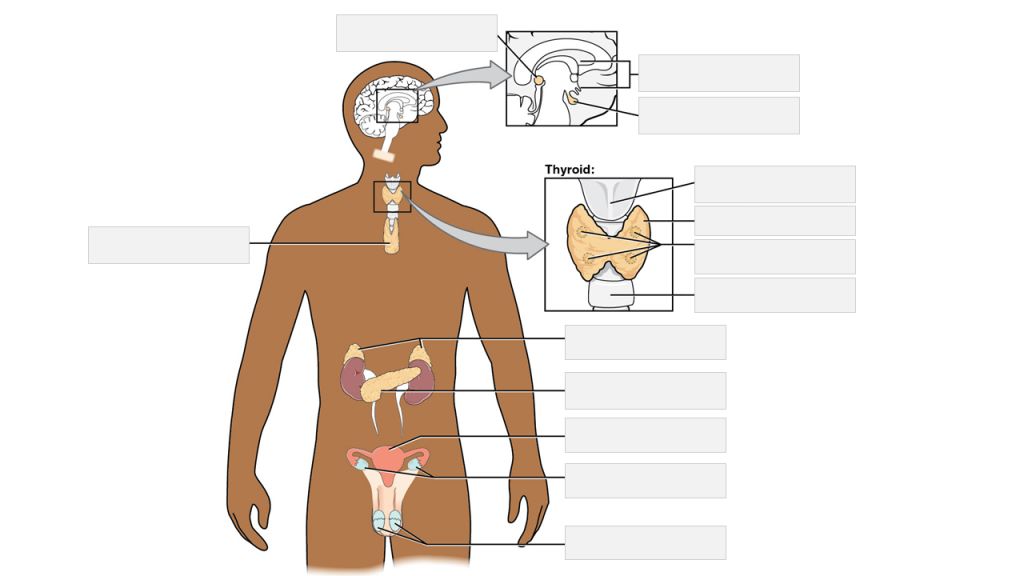
Hypoaldosteronism is a medical condition characterized by decreased levels or impaired function of the hormone aldosterone, which is produced by the adrenal gland. Aldosterone plays a crucial role in regulating electrolyte and fluid balance in the body by increasing the reabsorption of sodium and excretion of potassium in the kidneys.
Hypoaldosteronism can lead to low blood pressure, muscle weakness, and an imbalance of electrolytes, particularly low serum sodium levels and high serum potassium levels. This condition can be caused by various factors, including damage to the adrenal gland, impaired production or function of aldosterone, or decreased responsiveness of the kidneys to aldosterone.
Hypoaldosteronism can be primary or secondary. Primary hypoaldosteronism is caused by a problem with the adrenal glands themselves, such as damage to the gland or a genetic disorder that affects aldosterone production. Secondary hypoaldosteronism is caused by a problem outside of the adrenal glands, such as decreased production of renin (an enzyme produced by the kidneys) or certain medications that interfere with aldosterone production or function.
Treatment for hypoaldosteronism depends on the underlying cause and may include medication to replace missing aldosterone or correct electrolyte imbalances, as well as addressing any underlying conditions contributing to the development of the condition.
Pseudohypoaldosteronism is a group of disorders that are characterized by resistance to aldosterone, a hormone produced by the adrenal glands. Aldosterone plays a key role in regulating sodium and potassium balance in the body. In pseudohypoaldosteronism, the kidneys fail to respond to aldosterone, leading to an imbalance of electrolytes in the body.
There are two types of pseudohypoaldosteronism: type I and type II. Type I is further divided into two subtypes: severe neonatal or infantile forms, which are usually caused by genetic mutations that affect the function of the sodium-potassium pump in the kidney; and milder forms, which can be inherited or acquired and may be associated with other medical conditions.
Type II pseudohypoaldosteronism is a rare disorder that typically affects older children and adults. It is caused by genetic mutations that affect the function of the mineralocorticoid receptor in the kidney, which binds to aldosterone and triggers a response.
Symptoms of pseudohypoaldosteronism may include low sodium levels, high potassium levels, and metabolic acidosis (a buildup of acid in the body). Treatment typically involves supplementation with sodium and/or medications to help regulate electrolyte balance.
Potassium is a essential mineral and an important electrolyte that is widely distributed in the human body. The majority of potassium in the body (approximately 98%) is found within cells, with the remaining 2% present in blood serum and other bodily fluids. Potassium plays a crucial role in various physiological processes, including:
1. Regulation of fluid balance and maintenance of normal blood pressure through its effects on vascular tone and sodium excretion.
2. Facilitation of nerve impulse transmission and muscle contraction by participating in the generation and propagation of action potentials.
3. Protein synthesis, enzyme activation, and glycogen metabolism.
4. Regulation of acid-base balance through its role in buffering systems.
The normal serum potassium concentration ranges from 3.5 to 5.0 mEq/L (milliequivalents per liter) or mmol/L (millimoles per liter). Potassium levels outside this range can have significant clinical consequences, with both hypokalemia (low potassium levels) and hyperkalemia (high potassium levels) potentially leading to serious complications such as cardiac arrhythmias, muscle weakness, and respiratory failure.
Potassium is primarily obtained through the diet, with rich sources including fruits (e.g., bananas, oranges, and apricots), vegetables (e.g., leafy greens, potatoes, and tomatoes), legumes, nuts, dairy products, and meat. In cases of deficiency or increased needs, potassium supplements may be recommended under the guidance of a healthcare professional.
Fludrocortisone is a synthetic corticosteroid hormone, specifically a mineralocorticoid. It is often used to treat conditions associated with low levels of corticosteroids, such as Addison's disease. It works by helping the body retain sodium and lose potassium, which helps to maintain fluid balance and blood pressure.
In medical terms, fludrocortisone is defined as a synthetic mineralocorticoid with glucocorticoid activity used in the treatment of adrenogenital syndrome and Addison's disease, and as an adjunct in the treatment of rheumatoid arthritis. It is also used to treat orthostatic hypotension by helping the body retain sodium and water, thereby increasing blood volume and blood pressure.
It is important to note that fludrocortisone can have significant side effects, particularly if used in high doses or for long periods of time. These can include fluid retention, high blood pressure, increased risk of infection, and slowed growth in children. As with any medication, it should be used under the close supervision of a healthcare provider.
Spironolactone is a prescription medication that belongs to a class of drugs known as potassium-sparing diuretics. It works by blocking the action of aldosterone, a hormone that helps regulate sodium and potassium balance in your body. This results in increased urine production (diuresis) and decreased salt and fluid retention.
Spironolactone is primarily used to treat edema (fluid buildup) associated with heart failure, liver cirrhosis, or kidney disease. It's also prescribed for the treatment of high blood pressure and primary hyperaldosteronism, a condition where the adrenal glands produce too much aldosterone.
Furthermore, spironolactone is used off-label to treat conditions such as acne, hirsutism (excessive hair growth in women), and hormone-sensitive breast cancer in postmenopausal women.
It's important to note that spironolactone can cause increased potassium levels in the blood (hyperkalemia) and should be used with caution in patients with kidney impairment or those taking other medications that affect potassium balance. Regular monitoring of electrolyte levels, including potassium and sodium, is essential during spironolactone therapy.
Hypokalemia is a medical condition characterized by abnormally low potassium levels in the blood, specifically when the concentration falls below 3.5 milliequivalents per liter (mEq/L). Potassium is an essential electrolyte that helps regulate heart function, nerve signals, and muscle contractions.
Hypokalemia can result from various factors, including inadequate potassium intake, increased potassium loss through the urine or gastrointestinal tract, or shifts of potassium between body compartments. Common causes include diuretic use, vomiting, diarrhea, certain medications, kidney diseases, and hormonal imbalances.
Mild hypokalemia may not cause noticeable symptoms but can still affect the proper functioning of muscles and nerves. More severe cases can lead to muscle weakness, fatigue, cramps, paralysis, heart rhythm abnormalities, and in rare instances, respiratory failure or cardiac arrest. Treatment typically involves addressing the underlying cause and replenishing potassium levels through oral or intravenous (IV) supplementation, depending on the severity of the condition.
Mineralocorticoid receptor antagonists (MRAs) are a class of medications that block the action of aldosterone, a hormone produced by the adrenal glands. Aldosterone helps regulate sodium and potassium balance and blood pressure by binding to mineralocorticoid receptors in the kidneys, heart, blood vessels, and brain.
When aldosterone binds to these receptors, it promotes sodium retention and potassium excretion, which can lead to an increase in blood volume and blood pressure. MRAs work by blocking the binding of aldosterone to its receptors, thereby preventing these effects.
MRAs are primarily used to treat heart failure, hypertension, and kidney disease. By reducing sodium retention and increasing potassium excretion, MRAs can help lower blood pressure, reduce fluid buildup in the body, and improve heart function. Examples of MRAs include spironolactone and eplerenone.
Sodium bicarbonate, also known as baking soda, is a chemical compound with the formula NaHCO3. It is a white solid that is crystalline but often appears as a fine powder. It has a slightly salty, alkaline taste and is commonly used in cooking as a leavening agent.
In a medical context, sodium bicarbonate is used as a medication to treat conditions caused by high levels of acid in the body, such as metabolic acidosis. It works by neutralizing the acid and turning it into a harmless salt and water. Sodium bicarbonate can be given intravenously or orally, depending on the severity of the condition being treated.
It is important to note that sodium bicarbonate should only be used under the supervision of a healthcare professional, as it can have serious side effects if not used properly. These may include fluid buildup in the body, electrolyte imbalances, and an increased risk of infection.
Acidosis is a medical condition that occurs when there is an excess accumulation of acid in the body or when the body loses its ability to effectively regulate the pH level of the blood. The normal pH range of the blood is slightly alkaline, between 7.35 and 7.45. When the pH falls below 7.35, it is called acidosis.
Acidosis can be caused by various factors, including impaired kidney function, respiratory problems, diabetes, severe dehydration, alcoholism, and certain medications or toxins. There are two main types of acidosis: metabolic acidosis and respiratory acidosis.
Metabolic acidosis occurs when the body produces too much acid or is unable to eliminate it effectively. This can be caused by conditions such as diabetic ketoacidosis, lactic acidosis, kidney failure, and ingestion of certain toxins.
Respiratory acidosis, on the other hand, occurs when the lungs are unable to remove enough carbon dioxide from the body, leading to an accumulation of acid. This can be caused by conditions such as chronic obstructive pulmonary disease (COPD), asthma, and sedative overdose.
Symptoms of acidosis may include fatigue, shortness of breath, confusion, headache, rapid heartbeat, and in severe cases, coma or even death. Treatment for acidosis depends on the underlying cause and may include medications, oxygen therapy, fluid replacement, and dialysis.
Aldosterone is a hormone produced by the adrenal gland. It plays a key role in regulating sodium and potassium balance and maintaining blood pressure through its effects on the kidneys. Aldosterone promotes the reabsorption of sodium ions and the excretion of potassium ions in the distal tubules and collecting ducts of the nephrons in the kidneys. This increases the osmotic pressure in the blood, which in turn leads to water retention and an increase in blood volume and blood pressure.
Aldosterone is released from the adrenal gland in response to a variety of stimuli, including angiotensin II (a peptide hormone produced as part of the renin-angiotensin-aldosterone system), potassium ions, and adrenocorticotropic hormone (ACTH) from the pituitary gland. The production of aldosterone is regulated by a negative feedback mechanism involving sodium levels in the blood. High sodium levels inhibit the release of aldosterone, while low sodium levels stimulate its release.
In addition to its role in maintaining fluid and electrolyte balance and blood pressure, aldosterone has been implicated in various pathological conditions, including hypertension, heart failure, and primary hyperaldosteronism (a condition characterized by excessive production of aldosterone).
Cation exchange resins are a type of ion exchange resin that are positively charged and used to remove cations (positively charged ions) from aqueous solutions. They are often used in water treatment to soften water by removing calcium and magnesium ions, which can cause scale buildup in pipes and appliances. Cation exchange resins can also be used to remove heavy metals and other contaminants from water.
The resin itself is typically made of a cross-linked polymer matrix, such as polystyrene or polyacrylate, which contains functional groups that give the resin its ion exchange properties. The most common type of cation exchange resin is the sulfonated styrene divinylbenzene copolymer (SSDVB), in which the functional group is a sulfonic acid (-SO3H) group. When this resin comes into contact with a solution containing cations, such as a water supply, the cations in the solution will replace the hydrogen ions on the resin, causing the resin to become positively charged and the solution to become deionized.
Cation exchange resins can be regenerated by washing them with a strong acid, which replaces the captured cations with hydrogen ions, allowing the resin to be reused. The regeneration process must be done carefully to avoid damaging the resin and to ensure that it is properly rinsed of any residual acid before being put back into service.
Cation exchange resins are widely used in various industries such as pharmaceuticals, food and beverage, power generation, chemical processing and metal finishing for purification of water and wastewater treatment.
Dietary Potassium is a mineral and an essential electrolyte that is required in the human body for various physiological processes. It is primarily obtained through dietary sources. The recommended daily intake of potassium for adults is 4700 milligrams (mg).
Potassium plays a crucial role in maintaining normal blood pressure, heart function, and muscle and nerve activity. It also helps to balance the body's fluids and prevent kidney stones. Foods that are rich in dietary potassium include fruits such as bananas, oranges, and melons; vegetables such as leafy greens, potatoes, and tomatoes; legumes such as beans and lentils; dairy products such as milk and yogurt; and nuts and seeds.
It is important to maintain a balanced intake of dietary potassium, as both deficiency and excess can have negative health consequences. A deficiency in potassium can lead to muscle weakness, fatigue, and heart arrhythmias, while an excess can cause hyperkalemia, which can result in serious cardiac complications.
Sodium chloride symporters are membrane transport proteins that actively co-transport sodium and chloride ions into a cell. They are also known as sodium-chloride cotransporters or NCCs. These transporters play a crucial role in regulating the electrolyte balance and water homeostasis in various tissues, particularly in the kidney's distal convoluted tubule.
The primary function of sodium chloride symporters is to reabsorb sodium and chloride ions from the filtrate in the nephron back into the bloodstream. By doing so, they help maintain the body's sodium concentration and control water balance through osmosis.
Mutations in the gene encoding for the NCC can lead to various kidney disorders, such as Gitelman syndrome or Bartter syndrome type III, which are characterized by electrolyte imbalances, low blood pressure, and metabolic alkalosis.
Cathartics are a type of medication that stimulates bowel movements and evacuates the intestinal tract. They are often used to treat constipation or to prepare the bowel for certain medical procedures, such as colonoscopies. Common cathartic medications include laxatives, enemas, and suppositories.
Cathartics work by increasing the muscle contractions of the intestines, which helps to move stool through the digestive tract more quickly. They may also increase the amount of water in the stool, making it softer and easier to pass. Some cathartics, such as bulk-forming laxatives, work by absorbing water and swelling in the intestines, which helps to bulk up the stool and stimulate a bowel movement.
While cathartics can be effective at relieving constipation, they should be used with caution. Overuse of cathartics can lead to dependence on them for bowel movements, as well as electrolyte imbalances and other complications. It is important to follow the instructions carefully when using cathartic medications and to speak with a healthcare provider if constipation persists or worsens.
Succinylcholine is a neuromuscular blocking agent, a type of muscle relaxant used in anesthesia during surgical procedures. It works by inhibiting the transmission of nerve impulses at the neuromuscular junction, leading to temporary paralysis of skeletal muscles. This facilitates endotracheal intubation and mechanical ventilation during surgery. Succinylcholine has a rapid onset of action and is metabolized quickly, making it useful for short surgical procedures. However, its use may be associated with certain adverse effects, such as increased heart rate, muscle fasciculations, and potentially life-threatening hyperkalemia in susceptible individuals.
I'm sorry for any confusion, but "Polystyrenes" is not a medical term. Polystyrene is a type of synthetic aromatic hydrocarbon polymer that is used in a variety of commercial and industrial products, such as packaging materials, insulation, and disposable cutlery. It's important to note that some polystyrene products may contain potentially harmful chemicals, such as styrene, which can leach out into food or drink, posing potential health risks. However, the medical community primarily deals with the health effects of exposure to these chemicals rather than defining the material itself.
Angiotensin-Converting Enzyme (ACE) inhibitors are a class of medications that are commonly used to treat various cardiovascular conditions, such as hypertension (high blood pressure), heart failure, and diabetic nephropathy (kidney damage in people with diabetes).
ACE inhibitors work by blocking the action of angiotensin-converting enzyme, an enzyme that converts the hormone angiotensin I to angiotensin II. Angiotensin II is a potent vasoconstrictor, meaning it narrows blood vessels and increases blood pressure. By inhibiting the conversion of angiotensin I to angiotensin II, ACE inhibitors cause blood vessels to relax and widen, which lowers blood pressure and reduces the workload on the heart.
Some examples of ACE inhibitors include captopril, enalapril, lisinopril, ramipril, and fosinopril. These medications are generally well-tolerated, but they can cause side effects such as cough, dizziness, headache, and elevated potassium levels in the blood. It is important for patients to follow their healthcare provider's instructions carefully when taking ACE inhibitors and to report any unusual symptoms or side effects promptly.
Lisinopril is an angiotensin-converting enzyme (ACE) inhibitor, which is a type of medication used to treat various cardiovascular conditions. It works by blocking the conversion of angiotensin I to angiotensin II, a potent vasoconstrictor, resulting in relaxation and widening of blood vessels, decreased blood pressure, and increased blood flow.
Lisinopril is primarily used to treat hypertension (high blood pressure), congestive heart failure, and to improve survival after a heart attack. It may also be used to protect the kidneys from damage due to diabetes or high blood pressure. Additionally, it has been shown to reduce proteinuria (excess protein in urine) in patients with diabetic nephropathy.
Common side effects of Lisinopril include dizziness, headache, fatigue, and cough. More serious side effects may include angioedema (rapid swelling of the face, lips, tongue, or throat), hyperkalemia (elevated potassium levels), and impaired kidney function.
It is important to follow the prescribing physician's instructions carefully when taking Lisinopril and to report any unusual symptoms promptly. Regular monitoring of blood pressure, kidney function, and electrolyte levels may be necessary during treatment with this medication.
 Hyperkalemia
Hyperkalemia
Tumor lysis syndrome
T wave
Kidney failure
Calcium gluconate
P wave (electrocardiography)
Candesartan
Hypoaldosteronism
Kentice Tikolo
Reperfusion injury
Rhabdomyolysis
Pseudohypoaldosteronism
Beta blocker
Convallatoxin
Trandolapril
Sodium zirconium cyclosilicate
Clofarabine
Amiloride
Patiromer
List of dog diseases
Salbutamol
Crush injury
Regular insulin
Insulin (medication)
Nafarelin
Coconut water
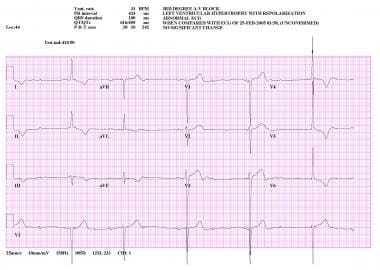
Third-degree atrioventricular block
Monosodium tartrate
Indometacin
Potassium bitartrate
Hyperkalemia - Wikipedia
 High potassium (hyperkalemia): Symptoms, causes, and prevention
High potassium (hyperkalemia): Symptoms, causes, and prevention
 Hyperkalemia (High Potassium): Symptoms, Causes, Treatment
Hyperkalemia (High Potassium): Symptoms, Causes, Treatment
 Dual RAAS Blockade in Diabetic Kidney Disease: Weighing the Benefits - Hyperkalemia Updates
Dual RAAS Blockade in Diabetic Kidney Disease: Weighing the Benefits - Hyperkalemia Updates
In CKD, We Need to Work Harder to Prevent the Preventable - Hyperkalemia Updates
 Hyperkalemia (High Potassium) | American Stroke Association
Hyperkalemia (High Potassium) | American Stroke Association
 Positive results for AZ' Lokelma in hyperkalaemia - PharmaTimes
Positive results for AZ' Lokelma in hyperkalaemia - PharmaTimes
Images in cardiology. ECG changes of severe hyperkalaemia. | Heart
 Perfusion Policies 101: HyperKalemia - Perfusion.com
Perfusion Policies 101: HyperKalemia - Perfusion.com
 NSAID risk of AKI or hyperkalemia | QxMD
NSAID risk of AKI or hyperkalemia | QxMD
 Hyperkalemia in the Emergency Room: Improving Long-Term Outcomes With Effective Discharge
Hyperkalemia in the Emergency Room: Improving Long-Term Outcomes With Effective Discharge
 EIA : Management of Acute Hyperkalaemia in Adults - Kingston Hospital
EIA : Management of Acute Hyperkalaemia in Adults - Kingston Hospital
 Investigation of a potassium adsorber for the treatment of hyperkalemia induced by traumatic injury and acute kidney injury in...
Investigation of a potassium adsorber for the treatment of hyperkalemia induced by traumatic injury and acute kidney injury in...
 The Co-occurrence of Hypertension and Hyperkalemia, Gordon's Syndrome: A Case Report | West Indian Medical Journal
The Co-occurrence of Hypertension and Hyperkalemia, Gordon's Syndrome: A Case Report | West Indian Medical Journal
 UKidney - Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study
UKidney - Rates of hyperkalemia after publication of the Randomized Aldactone Evaluation Study
Safety & Efficacy of Zirconium Silicate Dosed for 28 Days in Hyperkalemia.
Microangiographic Study of the Effects of Hyperkalaemia and Radiographic Contrast Media on Coronary Artery Calibre in the...
 Prevalence and factors associated with false hyperkalaemia in Asians in primary care: a cross-sectional study (the Unlysed...
Prevalence and factors associated with false hyperkalaemia in Asians in primary care: a cross-sectional study (the Unlysed...
 Bolus administration of intravenous glucose in the treatment of hyperkalemia : a randomized controlled trial
Bolus administration of intravenous glucose in the treatment of hyperkalemia : a randomized controlled trial
 Hyperkalemia
Hyperkalemia
Hyperkalemia Differential Diagnoses
 A cost-effectiveness analysis of patiromer in the UK: evaluation of hyperkalaemia treatment and lifelong RAASi maintenance in...
A cost-effectiveness analysis of patiromer in the UK: evaluation of hyperkalaemia treatment and lifelong RAASi maintenance in...
 hyperkalemia | HealthPlexus.net
hyperkalemia | HealthPlexus.net
Fluid, Electrolyte, and Nutrition Management of the Newborn: Overview, Prevalence and Loss of Body Water, Assessing Fluid and...
Hyperkalemia after the publication of RALES<...
 Klor-Con M: Package Insert - Drugs.com
Klor-Con M: Package Insert - Drugs.com
Mmol9
- Normal potassium levels are between 3.5 and 5.0 mmol/L (3.5 and 5.0 mEq/L) with levels above 5.5 mmol/L defined as hyperkalemia. (wikipedia.org)
- Most sources suggest that normal potassium serum levels are between 3.6-5 millimoles per liter, and levels above 5 mmol/l indicate hyperkalemia. (medicalnewstoday.com)
- For most people, their potassium level should be between 3.5 and 5.0 millimoles per liter (mmol/L). Hyperkalemia is a potassium level of greater than 5.5. (stroke.org)
- In the trial, 41.2% of patients with hyperkalaemia on stable haemodialysis receiving Lokelma maintained pre-dialysis normal potassium levels (4-5 mmol/L) on at least three out of four dialysis treatments after the long interdialytic interval and did not require urgent rescue therapy, compared to 1.0% of patients receiving placebo. (pharmatimes.com)
- Hyperkalemia was defined as serum potassium concentration of 5.5 mmol/L or greater. (qxmd.com)
- Approximately 275 subjects with hyperkalemia (two consecutive i-STAT potassium levels ≥ 5.1 mmol/l, taken 60 minutes apart at baseline) will be enrolled in the Open-label Acute Phase to provide 232 subjects in the Double Blind Randomized Maintenance Phase. (astrazenecaclinicaltrials.com)
- If repeat potassium level was ≤5.5 mmol/L within 8 days, the case was defined as false hyperkalaemia. (bmj.com)
- C .The patient has severe hyperkalemia (K = 6.9mmol/L) and requires urgent treatment. (mcgill.ca)
- 2) The normal range of serum K is 3.5-5.0 mmol/L. Hyperkalemia is defined as a serum potassium concentration of >5-5.5 mmol/L. (3) The large potassium gradient is maintained by Na-K ATPase pumps that drive sodium out of cells and potassium into cells. (mcgill.ca)
High potassium5
- Hyperkalemia is the medical term for high potassium levels. (medicalnewstoday.com)
- This is called hyperkalemia, or high potassium. (healthline.com)
- Hyperkalemia, also known as high potassium or hyperpotassemia, is a condition resulting from abnormally high levels of potassium in the blood, which can be cause health risks and be potentially life threatening. (columbia.edu)
- High potassium levels in the blood are called hyperkalemia. (suppcoupon.com)
- However, drug-induced hyperkalemia is considered the most important cause of high potassium in everyday clinical practice. (kidney.org)
Management of hyperkalemia1
- The management of hyperkalemia depends on the underlying cause and the level of potassium. (lu.se)
Diagnose hyperkalemia3
- A doctor will typically diagnose hyperkalemia when an individual's potassium levels are greater than 5.0-5.5 milliequivalents per liter. (medicalnewstoday.com)
- A blood test can help your doctor diagnose hyperkalemia. (healthline.com)
- It can be difficult to diagnose hyperkalemia. (stroke.org)
Severe9
- It is associated with an increased mortality, whether due to hyperkalaemia itself or as a marker of severe illness, especially in those without chronic kidney disease. (wikipedia.org)
- Whether you have mild or severe hyperkalemia, you should get prompt medical attention to prevent possible complications. (healthline.com)
- Although mild cases may not produce symptoms and may be easy to treat, severe cases of hyperkalemia that are left untreated can lead to fatal cardiac arrhythmias , which are abnormal heart rhythms. (stroke.org)
- ECG changes of severe hyperkalaemia. (bmj.com)
- Severe hyperkalemia (7.0mEq/L), especially with EKG manifestations, requires immediate therapy. (perfusion.com)
- Emergency cardiac pacing if severe hyperkalemia is causing arrhythmia's. (perfusion.com)
- Severe hyperkalemia can result in dangerous and potentially life-threatening manifestations, mainly cardiac in nature. (mcgill.ca)
- This approach article provides an overview of potassium homeostasis, diagnostic strategies, and treatment guidelines for patients with mild, moderate, and severe hyperkalemia. (mcgill.ca)
- When sufficient potassium chloride is rapidly ingested or given parenterally, severe hyperkalemia may result even when renal function is normal, but hyperkalemia is usually temporary. (msdmanuals.com)
Potential causes of hyperkalemia2
- There are a number of potential causes of hyperkalemia. (columbia.edu)
- There are many potential causes of hyperkalemia which may be divided into three main categories. (mcgill.ca)
Drug-Induced Hyperkalemia1
- This kind of hyperkalemia is known as Drug-Induced Hyperkalemia. (healthtian.com)
Sodium polystyre3
- For an earlier discussion about the use of sodium polystyrene sulfonate in managing hyperkalemia , click on the link. (hughesmedicine.com)
- Treatment of pediatric hyperkalemia with sodium polystyrene sulfonate. (madwirebuild.com)
- Sodium Polystyrene Sulfonate (SPS) is a commonly prescribed treatment for hyperkalemia. (ajkdblog.org)
Life-threatening2
- One implication of the delay is that complications of combat injury, including life-threatening hyperkalemia, will be more frequently managed in the far forward deployed setting where RRT is not practicable. (sbir.gov)
- 16 It should not be used as an emergency treatment for life-threatening hyperkalemia because of its delayed onset of action. (kidney.org)
Contribute to hyperkalemia2
- CKD, heart failure) can contribute to hyperkalemia. (kidney.org)
- There are a number of factors that can contribute to hyperkalemia, and in most cases some level of kidney failure is present. (lu.se)
Symptoms3
- Typically hyperkalemia does not cause symptoms. (wikipedia.org)
- There are often no symptoms of hyperkalemia, but it can be a sign of kidney disease, dehydration, diabetes complications, and many other health conditions. (medicalnewstoday.com)
- For patients with heart failure on these drugs, if any symptoms are experienced as above, you should tell your health care professional to make sure that the symptoms are not related to hyperkalemia. (stroke.org)
Angiotensin receptor2
- Examples of medications that can cause hyperkalemia include ACE inhibitors, angiotensin receptor blockers, non-selective beta blockers, and calcineurin inhibitor immunosuppressants such as ciclosporin and tacrolimus. (wikipedia.org)
- Drugs that are used to regulate blood pressure such as Angiotensin Converting Enzyme (ACE) inhibitors, Beta Blockers and Angiotensin Receptor Blockers (ARBs) can all cause hyperkalemia. (healthtian.com)
Hemodialysis3
- Hemodialysis for persistent hyperkalemia. (perfusion.com)
- Methods: A randomized, crossover study was conducted in 10 chronic hemodialysis patients who were prone to hyperkalemia. (sun.ac.za)
- Renin-angiotensin system blockade is not associated with hyperkalemia in chronic hemodialysis patients. (medscape.com)
Acute hyperkalemia4
- In acute hyperkalemia, which often results from a particular event, such as trauma, doctors may use dialysis and intravenous medications to flush the potassium from the body. (medicalnewstoday.com)
- Acute hyperkalemia may be due to redistribution of cellular potassium. (mcgill.ca)
- 5 Acute hyperkalemia represents a single event, occurring over hours to days and usually requires emergency treatment. (kidney.org)
- Treatment for acute hyperkalemia involves stabilzing heart function, shifting potassium to the intracellular space [using a combination of IV insulin plus glucose (to offset hypoglycemia), albuterol and sodium bicarbonate], and removing potassium with potassium binders, diuretics, or dialysis. (kidney.org)
Treat hyperkalemia3
- To address this unmet medical need for the military, we are developing a forward care intra-abdominal mesh packing device to reduce systemic potassium levels in austere medical treatment environments to treat hyperkalemia. (sbir.gov)
- Today, we will delve into the comparison between two drugs that are commonly used to treat hyperkalemia - Lokelma vs Kayexalate. (healthlinear.com)
- Lokelma is a selective potassium binder used to treat hyperkalemia. (healthlinear.com)
Hypotension2
- This means that inhibition of the RAAS, in susceptible individuals and settings in which RAAS activation is critical, is associated with an increased risk of acute kidney injury, hypotension, and hyperkalemia. (medpagetoday.com)
- Combination therapy with an ACE inhibitor and an ARB may improve morbidity and probably mortality, but with an increased incidence of hypotension, hyperkalemia, and azotemia. (healthplexus.net)
Medications6
- Consuming too much potassium through medications or diet can cause hyperkalemia. (medicalnewstoday.com)
- Several things can cause hyperkalemia, including health problems and the use of certain medications. (healthline.com)
- Most often the etiology of such disturbances is due to prescribed medications, but a number of clinical conditions exist which predispose people to both hyperkalemia and hypokalemia. (healthplexus.net)
- Heparin and low molecular weight heparins (LMWH) are some of the many medications that have been identified to cause hyperkalemia. (hughesmedicine.com)
- To manage hyperkalemia effectively, physicians often prescribe medications like Lokelma and Kayexalate, which are designed to lower potassium levels in the blood. (healthlinear.com)
- Management of chronic hyperkalemia requires confirmation, increased laboratory surveillance, dietary review and counseling, a review of medications (prescribed, over-the-counter and herbal), and, if needed, a potassium-lowering medication and/or a diuretic. (kidney.org)
Insulin2
- 5 Versus 10 Units of Insulin in Hyperkalemia Management: Multi-center, Prospective, Double-blind, Non-inferiority, Randomized Control Trial. (who.int)
- To study the efficacy of two intravenous insulin doses (5 units and 10 units) in reducing serum potassium level in patients receiving hyperkalemia treatment using the main laboratory measurements. (who.int)
Level of potassium3
- Hyperkalemia is an elevated level of potassium (K+) in the blood. (wikipedia.org)
- Hyperkalemia is a higher than normal level of potassium in the blood. (stroke.org)
- Asides kidney diseases, hyperkalemia also occurs when there is an increased level of potassium in one's diet. (healthtian.com)
Adrenal1
- Research has shown that the adrenal glands also has been seen to cause hyperkalemia. (healthtian.com)
Cardiac arrhythmias3
- The risk of death from hyperkalemia-induced cardiac arrhythmias is significant in the absence of renal replacement therapy (RRT). (sbir.gov)
- Background: Hyperkalemia is a common medical emergency that may result in serious cardiac arrhythmias. (sun.ac.za)
- On the other hand, hyperkalemia, marked by elevated potassium levels, can pose a risk of life-threatening cardiac arrhythmias. (healthlinear.com)
Occurs5
- In chronic kidney disease, hyperkalemia occurs as a result of reduced aldosterone responsiveness and reduced sodium and water delivery in distal tubules. (wikipedia.org)
- Hyperkalemia occurs when the body is unable to remove excess potassium. (medicalnewstoday.com)
- This occurs in response to various stimuli including angiotensin II, ACTH, hyperkalemia, low sodium intake, and decreased intravascular volume. (hughesmedicine.com)
- Hyperkalemia occurs when there is a problem with the functional process of the kidney. (healthtian.com)
- Hyperkalemia is a medical condition that occurs when there is an excessive amount of potassium in the bloodstream. (healthlinear.com)
Lokelma7
- AstraZeneca has announced a statistically significant and clinically meaningful improvement from its Phase IIIb DIALIZE trial, investigating the efficacy and safety of Lokelma (sodium zirconium cyclosilicate) for the treatment of hyperkalaemia in patients with end-stage renal disease (ESRD) on haemodialysis. (pharmatimes.com)
- Elisabeth Björk, senior vice president, said that the positive results show that "Lokelma can normalise potassium levels in between dialysis sessions for patients with hyperkalaemia who have end-stage renal disease. (pharmatimes.com)
- In this article you will learn about lokelma -the drug used for people with hyperkalemia that has proven its efficacy in clinical studies. (suppcoupon.com)
- Lokelma is a drug used in the treatment of hyperkalemia . (suppcoupon.com)
- Lokelma is usually taken in addition to dietary changes and other standard treatments for hyperkalemia. (suppcoupon.com)
- Lokelma can be an effective treatment for those suffering from hyperkalemia. (suppcoupon.com)
- Rapidly reducing potassium levels, Lokelma offers an effective solution for managing hyperkalemia. (healthlinear.com)
Levels of potassium3
- Hyperkalemia is a term that is used to describe a medical condition that arises as a result of high levels of potassium in the body. (healthtian.com)
- Hyperkalemia is when the levels of potassium in your blood are too high. (suppcoupon.com)
- High levels of potassium in the blood (called hyperkalemia) is unpredictable and can be life-threatening. (kidney.org)
Mild1
- Mild hyperkalemia (6.0mEQ/L), with normal renal function generally needs no treatment. (perfusion.com)
Severity2
- Treatment for hyperkalemia varies according to severity. (medicalnewstoday.com)
- The choice of treatment is determined by the patient's clinical presentation, how rapidly the disorder developed, severity of hyperkalemia, and by the presence or absence of ECG changes. (kidney.org)
Laboratory1
- This calculator to estimate patients' risk of acute kidney injury or hyperkalemia within 30 days following initiation of a prescription NSAID was developed in a large retrospective population-based study of adults 66 years and older using linked administrative and laboratory databases in Ontario, Canada. (qxmd.com)
Familial hypertension1
- Type IV renal tubular acidosis (aldosterone resistance of the kidney's tubules) Gordon's syndrome (pseudohypoaldosteronism type II) ("familial hypertension with hyperkalemia"), a rare genetic disorder caused by defective modulators of salt transporters, including the thiazide-sensitive Na-Cl cotransporter. (wikipedia.org)
Treatment12
- Chronic hyperkalemia usually means that a person's kidneys are not functioning correctly, and doctors will offer treatment to manage the condition. (medicalnewstoday.com)
- The drug is a highly-selective, oral potassium-removing agent currently approved and available in the US and EU for the treatment of adults with hyperkalaemia. (pharmatimes.com)
- If you're concerned that you may have hyperkalemia, your health care provider will likely order a blood test to diagnose and recommend an appropriate treatment plan. (columbia.edu)
- In the meantime, alert anesthesia to the possibility of true hyperkalemia, and the necessity for treatment of it. (perfusion.com)
- The goal of this activity is that learners will be better able to manage chronic kidney disease (CKD)-related hyperkalemia, learn about new evidence and guidance for initiating appropriate treatment, educate their patients, and plan long-term, team-based patient follow-up after discharge. (medscape.org)
- Hyperkalemia is a serious concern in the treatment of combat casualties as it is a common complication of acute kidney injury, which prevents the excretion of excessive plasma potassium released from damaged tissue. (sbir.gov)
- Rapid evacuation out of Iraq and Afghanistan ensured that most instances of hyperkalemia occurred further up the evacuation chain, thereby limiting the need for non-RRT hyperkalemia treatment options for austere conditions. (sbir.gov)
- The benefits of our forward care medical device are three-fold: 1) stabilizes hyperkalemia patients to endure prolonged field care and delayed evacuation, 2) is logistically feasible to implement for field use requiring nominal dialysate fluid and medical training, and 3) expands hyperkalemia treatment options to include transport on aircraft with limited medical capability. (sbir.gov)
- Successful completion of this project will be demonstrated by the production of an effective advanced prototype that is ready for manufacturing scale-up and subsequent clinical testing to provide a real-life solution for combat-related hyperkalemia treatment in austere environments. (sbir.gov)
- Resin Treatment for Hyperkalemia: Where Do We Stand? (ajkdblog.org)
- Diagnosis includes assessment of kidney and heart function, including blood tests and electrocardiogram (ECG) to determine whether the hyperkalemia requires immediate emergency treatment. (kidney.org)
- This paper briefly examines the pathophysiological mechanisms behind hyperkalemia, with a special focus on treatment. (lu.se)
Clinical5
- Results of large clinical trials dashed these hopes, finding increased risk of AKI and hyperkalemia without additional clinical benefit. (medpagetoday.com)
- To shed more light on this clinical conundrum, Whitlock and colleagues conducted a systematic review and meta-analysis of the risks of AKI and hyperkalemia associated with dual RAAS blockade in patients with DKD. (medpagetoday.com)
- In many cases, a hyperkalemia diagnosis must rely on clinical information such as a history of kidney failure or the use of medicines known to cause hyperkalemia. (stroke.org)
- Hyperkalemia is one of the most common electrolytic disorders encountered in clinical practice. (mcgill.ca)
- It has been studied in three double-blind, placebo controlled trials and in one ongoing 12-month open label clinical trial in patients with hyperkalaemia, which represents over 1,600 patients treated. (kidney.org)
Occur5
- If intake of potassium far outweighs the kidneys' ability to remove it, or if kidney function decreases, there can be too much potassium, and hyperkalemia can occur. (stroke.org)
- In pediatric patients, factitious hyperkalemia can occur because of "milking" of extremities (which can introduce a significant amount of interstitial fluid into the blood sample) during phlebotomy, especially with heel-poke and finger-stick phlebotomy, which are commonly performed in infants and small children. (medscape.com)
- However, when some diseases affect the level of production of this hormone, it will cause an imbalance and as such cause, hyperkalemia to occur. (healthtian.com)
- As such, there will be an accumulation within the bloodstream and as such hyperkalemia will occur. (healthtian.com)
- Hyperkalemia can also occur in metabolic acidosis (eg, as in diabetic ketoacidosis). (msdmanuals.com)
Hypertension5
- In the setting of CKD, hyperkalemia, malignant hypertension, volume overload, and heart failure are important ambulatory care-sensitive conditions (ACSCs), which refer to those health conditions that can be managed successfully with good outpatient care to potentially prevent hospitalizations. (medpagetoday.com)
- Primary outcomes included the CKD-specific ACSCs of hyperkalemia, malignant hypertension, volume overload, and heart failure, and patients with CKD were classified as having at least 1 ACSC-related hospitalization or no ACSC-related hospitalization during the follow-up period. (medpagetoday.com)
- Secondary hypertension co-occurrence with hyperkalaemia is not an expected finding. (uwi.edu)
- Gordon's syndrome is an autosomal dominant disease which is a rare cause of secondary hypertension and hyperkalaemia is the most important feature. (uwi.edu)
- A 33-year-old male patient presented with hypertension and hyperkalaemia. (uwi.edu)
Adults2
Haemolysis1
- Haemolysis is known to cause false hyperkalaemia. (bmj.com)
Renal function2
- Moderate hyperkalemia (6.0-7.0mEq/L), with normal renal function generally resolves with time and no therapy. (perfusion.com)
- Diabetes Mellitus: To minimise the risk of hyperkalaemia in known or suspected diabetic patients, the status of renal function should be determined before initiating therapy. (janusinfo.se)
Blockade1
- There is a population with chronic hyperkalemia, including those who require high dose renin-angiotensin blockade, patients with congestive failure, and those with diabetic nephropathy. (ajkdblog.org)
Electrolyte2
- Hyperkalemia is a relatively common electrolyte abnormality that in serious cases can lead to life-threatening arrhythmias. (lu.se)
- The elderly are more susceptible to electrolyte imbalance and are more likely to experience hyperkalaemia since renal reserve may be reduced. (janusinfo.se)
Dietary2
- Case notes were not reviewed for dietary assessment which could contribute to hyperkalaemia. (bmj.com)
- Overview of the symposium agenda followed by a discussion on the impact of hyperkalaemia on mortality, MACE outcomes,CKD progression and impairment of RAASi optimisation, and restriction of dietary K+. (radcliffecardiology.com)
RAASi3
- Therapeutic dilemmas and aspirations in hyperkalaemia management: interventional targets, RAASi optimisation, and low-K+diet. (radcliffecardiology.com)
- An overview of guidelines on the use of potassium bindersto manage hyperkalaemia and enable RAASi optimisation. (radcliffecardiology.com)
- People with chronic kidney disease, heart failure, diabetes mellitus, and those taking blood pressure medicines called renin-angiotensin-aldosterone system inhibitors (RAASi) have an estimated 2 to 3 times higher risk for hyperkalemia. (kidney.org)
Prevalence2
Diabetes3
- As a decrease in kidney function is a possible complication of diabetes, poorly managing the condition may result in hyperkalemia. (medicalnewstoday.com)
- Diabetes and Drug-Associated Hyperkalemia: Effect of Potassium Monitoring. (medscape.com)
- Risk factors for heparin-induced hyperkalemia include diabetes mellitus, renal impairment, hematomas, and other conditions that alter the balance of the renin-angiotensin aldosterone system. (hughesmedicine.com)
Mortality2
- Studies, however, have demonstrated increased risk of adverse events such as hyperkalemia and AKI with these combination therapies, while not finding any additional benefit on mortality or kidney disease progression. (medpagetoday.com)
- Chronic kidney disease (CKD) patients with and without heart failure (HF) often present with hyperkalaemia (HK) leading to increased risk of hospitalisations, cardiovascular related events and cardiovascular-related mortality. (biomedcentral.com)
Risk5
- A new systematic review and meta-analysis assessed the impact of dual renin-angiotensin-aldosterone system inhibition on risk of acute kidney injury and hyperkalemia in patients diagnosed with diabetic kidney disease. (medpagetoday.com)
- 2 On the contrary, in a number of studies, the combination of 2 RAAS blocking drugs was associated a greater risk of acute kidney injury (AKI) and hyperkalemia compared to single-drug therapy. (medpagetoday.com)
- Talk to your health care professional to understand any risk you might have for hyperkalemia. (stroke.org)
- The NSAID risk of AKI or hyperkalemia calculator is created by QxMD. (qxmd.com)
- Predicting the risk of hyperkalemia in patients with chronic kidney disease starting lisinopril. (medscape.com)
Kidney disease2
- The frequency of hyperkalemia and its significance in chronic kidney disease. (medscape.com)
- It is used for people with chronic kidney disease who have hyperkalemia. (suppcoupon.com)