Hypophosphatemia, Familial
Familial Hypophosphatemic Rickets
PHEX Phosphate Regulating Neutral Endopeptidase
Osteomalacia
Genetic Diseases, X-Linked
Sodium-Phosphate Cotransporter Proteins, Type IIc
Rickets
Fibroblast Growth Factors
Phosphorus
Sodium-Phosphate Cotransporter Proteins, Type IIa
Neoplasms, Connective Tissue
Refeeding Syndrome
Parathyroid Hormone
Sodium-Phosphate Cotransporter Proteins, Type II
Calcitriol
Mesenchymoma
Paraneoplastic Syndromes
Sodium-Phosphate Cotransporter Proteins
Hyperphosphatemia
Alkalosis, Respiratory
Fanconi Syndrome
Hypocalcemia
25-Hydroxyvitamin D3 1-alpha-Hydroxylase
Glucuronidase
Osteocytes
Vitamin D
Phosphorus, Dietary
Phosphorus Metabolism Disorders
Bone and Bones
Parturient Paresis
Hyperparathyroidism
Parathyroid Glands
Acidosis
Opossums
Calcification, Physiologic
Kidney
Parenteral Nutrition, Total
Calcium
Hereditary hypophosphataemic rickets: report of a family from the Indian subcontinent. (1/116)
Nutritional deficiency continues to be an important cause of rickets in the underdeveloped and developing parts of the world. In the western hemisphere, predominantly non-nutritional forms of rickets and osteomalacia are now seen. In this report we discuss a family with X-linked hypophosphataemic rickets from the Kashmir region of the Indian subcontinent (which is an uncommon entity here). (+info)Tertiary hyperparathyroidism in X-linked hypophosphatemic rickets. (2/116)
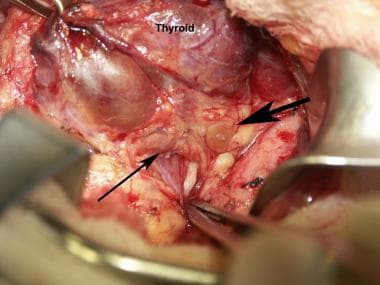
We report a case of tertiary hyperparathyroidism in an X-linked familial hypophosphatemic rickets (XLH) patient under regular calcitriol and self-adjusted large doses of oral phosphate salt (2.4-3.6 g/day in 4-5 divided doses) according to his serum phosphate level. Tertiary hyperparathyroidism is an unusual complication of XLH patients during treatment. As there is growing evidence that a high phosphate diet may induce hyperplasia of the parathyroid glands, it is important to avoid the stimulation of the parathyroid glands by high doses of phosphate administration in XLH patients. Serum calcium, phosphate, alkaline phosphatase, and also parathyroid hormone should be measured regularly in order to facilitate an early diagnosis of secondary hyperparathyroidism during the treatment of XLH patients, since this stage is reversible with calcitriol and reduced doses of phosphate salt. (+info)Final height of Japanese patients with X-linked hypophosphatemic rickets: effect of vitamin D and phosphate therapy. (3/116)
X-linked hypophosphatemic rickets (XLH) is one of the most common causes of rickets in infancy and childhood. Combination therapy of vitamin D and phosphate is generally used for patients with XLH. Effect of treatment of vitamin D and phosphate during childhood on final height of XLH has to be elucidated in Japanese. There have been only three Caucasian studies on final height of XLH with treatment since childhood. Purpose of this study is to report adult height and therapeutic effect of 22 Japanese participants (5 males, 17 females) with XLH who were treated with phosphate (33-200 mg/kg/day as phosphorus divided into 3 or 4 doses) and vitamin D (vitamin D2 or 1alpha-hydroxyvitamin D3) for more than five years and evaluate effect of the treatment on the final height retrospectively. Final height (FHt) for all participants was -1.69+/-11.11 SD. FHt (-1.69+/-1.11 SD) was significantly higher than height at the initiation of treatment (-2.38+/-0.88 SD) for all participants (P<0.01). In conclusion, combination therapy of vitamin D and phosphate improved final height of Japanese patients with XLH as is similar to previous Caucasian studies. (+info)Orthophosphate transport in the erythrocyte of normal subjects and of patients with X-linked hypophosphatemia. (4/116)
We have examined the mechanism of TCA-soluble orthophosphate (Pi) transfer across the membrane of mature human erythrocytes in normal subjects and in patients with X-linked hypophosphatemia (X-LH). The studies were carried out largely at pH 7.4 and 37 degrees C, in partial stimulation of conditions in vivo. (a) At physiological concentrations (1-2 mM) Pi enters the intact normal erythrocyte down its chemical gradient and under no conditions could we identify a steady-state trans-membrane gradient for Pi greater than 0.6. Calculations of the phosphate anion distribution ratio using the Nernst equation yield theoretical values that closely approximate observed values. (b) Glycolytic inhibitors have little effect on total entry of 32Pi inti erythrocytes but they do affect the intracellular distribution of Pi. In the presence of iodoacetamide, label accumulates almost exclusively in the orthophosphate pool and less than 1% enters the organic phosphate pool. (c) Specific activity measurements in unblocked cells indicate that Pi anion equilibrates first with its intracellular Pi pool. These initial findings imply that neither group translocation, nor energy coupling, influence Pi permeation into the human erythrocytes. (d) The relationship between 32P entry and extracellular Pi concentration is parabolic in the presence of chloride, and linear in the presence of sulfate. The kinetics of concentration dependent entrance cannot be examined and saturability of Pi entry cannot be identified under these conditions. (e) The competitive inhibitor arsenate partially inhibits the initial rate and steady-state flux of orthophosphate in erythrocytes treated with iodoacetamide to inhibit glycolysis. However, a significant portion of Pi transport escapes arsenate inhibition. (f) Activation energies for Pi entry, in nonglycolizing erythrocytes are much higher than those required by simple diffusion in an aqueous system. (g) Neither the inward or outward movement of Pi is modulated by trans-phosphate. These latter findings suggest that transport of phosphate across the human erythrocyte is compatible with slow facilitated diffusion with symmetry for influex and efflux. The transmembrane chemical distribution ratio, and the equilibrium flux of Pi were not different from normal in the X-LH erythrocyte. Nor did the extracellular Pi concentration, arsenate, or temperature affect Pi entry differently in the two types of cells. We dedjce that different gene products serve the diffusional type of Pi transport in the erythrocyte membrane and the saturable component of transepithelial absorption in the gut and kidney. Only the latter is affected by the X-LH mutation. The former is apparently present not only in erythrocytes but also in epithelial tissue, where it can serve the absorption of pharmacologic amounts of Pi in the therapeutic repair of the depleted phosphate pools in X-LH. (+info)Hereditary hypophosphatemic rickets with hypercalciuria is not caused by mutations in the Na/Pi cotransporter NPT2 gene. (5/116)
Hereditary hypophosphatemic rickets with hypercalciuria (HHRH), a renal phosphate (Pi) wasting disease first described in an extended Bedouin kindred, is characterized by hypophosphatemia, elevated serum 1,25-dihydroxyvitamin D levels, hypercalciuria, rickets, and osteomalacia. Correction of all abnormalities, except for renal Pi wasting, can be achieved by oral Pi supplementation. These findings and the demonstration that mice that are homozygous for the disrupted Na/Pi cotransporter gene Npt2 exhibit many of the biochemical features of HHRH suggested that mutations in the human orthologue NPT2 might be responsible for HHRH. The NPT2 gene in affected individuals from the Bedouin kindred and four small families was screened for mutations to test this hypothesis. No putative disease-causing mutation was found. Two single nucleotide polymorphisms (SNP), a silent substitution in exon 7 and a nucleotide substitution in intron 4, were identified, and neither consistently segregated with HHRH in the Bedouin kindred. Linkage analysis indicated that the two NPT2 intragenic SNP as well as five microsatellite markers in the NPT2 gene region were not linked to HHRH in the Bedouin kindred. Therefore, this is evidence to exclude NPT2 as a candidate gene for HHRH in the families that were studied. (+info)Autosomal recessive hypophosphataemic rickets with hypercalciuria is not caused by mutations in the type II renal sodium/phosphate cotransporter gene. (6/116)
BACKGROUND: At present the genetic defect for autosomal recessive and autosomal dominant hypophosphataemic rickets with hypercalciuria (HHRH) is unknown. Type II sodium/phosphate cotransporter (NPT2) gene is a serious candidate for being the causative gene in either or both autosomal recessive and autosomal dominant HHRH. In the present study we tested this hypothesis in one autosomal recessive family. METHODS: The gene structure of human NPT2 is known. We tested the complete open reading frame in the affected siblings by polymerase chain reaction in combination with automatic DNA sequencing for the presence of mutations. RESULTS: We did not observe disease-causing mutations in the NPT2 gene of the affected siblings. A T855C polymorphism resulting in a histidine to arginine transition was present in the open reading frame of NPT2. The polymorphism was present in both affected as well as unaffected family members. CONCLUSION: The hypothesis that a defect in the NPT2 gene could be an underlying cause for autosomal recessive HHRH could not be sustained in our study. (+info)A rationale for treatment of hereditary vitamin D-resistant rickets with analogs of 1 alpha,25-dihydroxyvitamin D(3). (7/116)
Hereditary vitamin D-resistant rickets (HVDRR) is caused by heterogeneous inactivating mutations in the vitamin D receptor (VDR). Treatment of HVDRR patients with high doses of oral calcium and supraphysiologic doses of 1 alpha,25-dihydroxyvitamin D(3) (1,25D(3)) has had limited success. In this study we explored the use of vitamin D analogs as a potential therapy for this disorder. The rationale for the use of vitamin D analogs is that they bind the VDR at different amino acid residues than 1,25D(3), and their ability to modulate VDR functions differs from that of the natural hormone. In this report, we examined the VDR from three HVDRR patients with mutations in the ligand-binding domain of the VDR (histidine 305 to glutamine, arginine 274 to leucine, and phenylalanine 251 to cysteine) for their responses to two vitamin D analogs, 20-epi-1,25D(3) and 1 beta-hydroxymethyl-3-epi-16-ene-26a,27a-bishomo-25D(3) (JK-1626-2). Our results reveal that vitamin D analogs partially or completely restore the responsiveness of the mutated VDR. Analog treatment seemed to be more successful when the mutation affects the amino acids directly involved in ligand binding rather than amino acids that contribute to a functional VDR interface with dimerization partners or coactivators of transcription. (+info)Disease-causing missense mutations in the PHEX gene interfere with membrane targeting of the recombinant protein. (8/116)
PHEX is homologous to the M13 zinc metallopeptidases, a class of type II membrane glycoproteins. Although more than 140 mutations in the PHEX gene have been identified in patients with X-linked hypophosphatemia (XLH), the most prevalent form of inherited rickets, the molecular consequences of disease-causing PHEX mutations have not yet been investigated. We examined the effect of PHEX missense mutations on cellular trafficking of the recombinant protein. Four mutant PHEX cDNAs were generated by PCR mutagenesis: C85R, G579R and S711R, identified in XLH patients, and E581V, previously engineered in neutral endopeptidase 24.11, where it abolished catalytic activity but not plasma membrane targeting. Wild-type and mutant PHEX cDNAs were transfected in HEK(293) cells and PHEX protein expression was characterized. In contrast to the wild-type and E581V PHEX proteins, the C85R, G579R and S711R mutants were completely sensitive to endoglycosidase H digestion, indicating that they were not fully glycosylated. Sequestration of the disease-causing mutant proteins in the endoplasmic reticulum (ER) and plasma membrane localization of wild-type and E581V PHEX proteins was demonstrated by immunofluorescence and cell surface biotinylation. Of the three mutant PHEX proteins, the S711R was the least stable and the only one that could be rescued from the ER to the plasma membrane in cells grown at 26 degrees C. The chemical chaperone glycerol failed to correct defective targeting of all three mutant proteins. Our data provide a mechanism for loss of PHEX function in XLH patients expressing the C85R, G579R and S711R mutations. (+info)Hypophosphatemia is a medical condition characterized by abnormally low levels of phosphate (phosphorus) in the blood, specifically below 2.5 mg/dL. Phosphate is an essential electrolyte that plays a crucial role in various bodily functions such as energy production, bone formation, and maintaining acid-base balance.
Hypophosphatemia can result from several factors, including malnutrition, vitamin D deficiency, alcoholism, hormonal imbalances, and certain medications. Symptoms of hypophosphatemia may include muscle weakness, fatigue, bone pain, confusion, and respiratory failure in severe cases. Treatment typically involves correcting the underlying cause and administering phosphate supplements to restore normal levels.
Familial Hypophosphatemia is a genetic disorder characterized by low levels of phosphate in the blood (hypophosphatemia) due to impaired absorption of phosphates in the gut. This condition results from mutations in the SLC34A3 gene, which provides instructions for making a protein called NaPi-IIc, responsible for reabsorbing phosphates from the filtrate in the kidney tubules back into the bloodstream.
In familial hypophosphatemia, the impaired function of NaPi-IIc leads to excessive loss of phosphate through urine, resulting in hypophosphatemia. This condition can cause rickets (a softening and weakening of bones) in children and osteomalacia (softening of bones) in adults. Symptoms may include bowed legs, bone pain, muscle weakness, and short stature.
Familial Hypophosphatemia is inherited as an autosomal recessive trait, meaning that an individual must inherit two copies of the mutated gene (one from each parent) to develop the condition.
Familial Hypophosphatemic Rickets (FHR) is a genetic disorder characterized by impaired reabsorption of phosphate in the kidneys, leading to low levels of phosphate in the blood (hypophosphatemia). This condition results in defective mineralization of bones and teeth, causing rickets in children and osteomalacia in adults.
FHR is typically caused by mutations in the PHEX gene, which encodes a protein that helps regulate phosphate levels in the body. In FHR, the mutation leads to an overproduction of a hormone called fibroblast growth factor 23 (FGF23), which increases phosphate excretion in the urine and decreases the activation of vitamin D, further contributing to hypophosphatemia.
Symptoms of FHR may include bowing of the legs, bone pain, muscle weakness, short stature, dental abnormalities, and skeletal deformities. Treatment typically involves oral phosphate supplements and active forms of vitamin D to correct the hypophosphatemia and improve bone mineralization. Regular monitoring of blood phosphate levels, kidney function, and bone health is essential for effective management of this condition.
PHEX (Phosphate Regulating Endopeptidase Homolog, X-Linked) is a gene that encodes for an enzyme called phosphate regulating neutral endopeptidase. This enzyme is primarily expressed in osteoblasts, which are cells responsible for bone formation.
The main function of the PHEX protein is to regulate the levels of a hormone called fibroblast growth factor 23 (FGF23) by breaking it down. FGF23 plays an essential role in maintaining phosphate homeostasis by regulating its reabsorption in the kidneys and its absorption from the gut.
Inactivating mutations in the PHEX gene can lead to X-linked hypophosphatemia (XLH), a genetic disorder characterized by low levels of phosphate in the blood, impaired bone mineralization, and rickets. In XLH, the production of FGF23 is increased due to the lack of regulation by PHEX, leading to excessive excretion of phosphate in the urine and decreased absorption from the gut. This results in hypophosphatemia, impaired bone mineralization, and other skeletal abnormalities.
Osteomalacia is a medical condition characterized by the softening of bones due to defective bone mineralization, resulting from inadequate vitamin D, phosphate, or calcium. It mainly affects adults and is different from rickets, which occurs in children. The primary symptom is bone pain, but muscle weakness can also occur. Prolonged osteomalacia may lead to skeletal deformities and an increased risk of fractures. Treatment typically involves supplementation with vitamin D, calcium, and sometimes phosphate.
Phosphates, in a medical context, refer to the salts or esters of phosphoric acid. Phosphates play crucial roles in various biological processes within the human body. They are essential components of bones and teeth, where they combine with calcium to form hydroxyapatite crystals. Phosphates also participate in energy transfer reactions as phosphate groups attached to adenosine diphosphate (ADP) and adenosine triphosphate (ATP). Additionally, they contribute to buffer systems that help maintain normal pH levels in the body.
Abnormal levels of phosphates in the blood can indicate certain medical conditions. High phosphate levels (hyperphosphatemia) may be associated with kidney dysfunction, hyperparathyroidism, or excessive intake of phosphate-containing products. Low phosphate levels (hypophosphatemia) might result from malnutrition, vitamin D deficiency, or certain diseases affecting the small intestine or kidneys. Both hypophosphatemia and hyperphosphatemia can have significant impacts on various organ systems and may require medical intervention.
X-linked genetic diseases refer to a group of disorders caused by mutations in genes located on the X chromosome. These conditions primarily affect males since they have only one X chromosome and therefore don't have a second normal copy of the gene to compensate for the mutated one. Females, who have two X chromosomes, are typically less affected because they usually have one normal copy of the gene on their other X chromosome.
Examples of X-linked genetic diseases include Duchenne and Becker muscular dystrophy, hemophilia A and B, color blindness, and fragile X syndrome. Symptoms and severity can vary widely depending on the specific condition and the nature of the genetic mutation involved. Treatment options depend on the particular disease but may include physical therapy, medication, or in some cases, gene therapy.
Sodium-phosphate cotransporter proteins, type IIc (NPTIIc), are a subtype of sodium-dependent phosphate transporters that play a crucial role in the regulation of phosphate homeostasis within the body. They are located primarily in the kidney's proximal tubule cells and intestinal epithelial cells.
NPTIIc proteins facilitate the active transport of inorganic phosphate (Pi) ions across the cell membrane, in conjunction with sodium ions (Na+). This symport mechanism allows for the movement of Pi against its concentration gradient, from areas of low concentration to high concentration. The energy required for this process is derived from the electrochemical gradient of sodium ions.
These transporters are essential for maintaining normal phosphate levels in the body, as they help reabsorb a significant portion of filtered phosphate in the kidneys and absorb dietary phosphate in the intestines. Dysregulation of NPTIIc proteins can lead to various disorders related to phosphate homeostasis, such as hypophosphatemia (low serum phosphate levels) or hyperphosphatemia (high serum phosphate levels), which can have detrimental effects on bone health, mineral metabolism, and overall body function.
Rickets is a medical condition characterized by the softening and weakening of bones in children, primarily caused by deficiency of vitamin D, calcium, or phosphate. It leads to skeletal deformities, bone pain, and growth retardation. Prolonged lack of sunlight exposure, inadequate intake of vitamin D-rich foods, or impaired absorption or utilization of vitamin D can contribute to the development of rickets.
Fibroblast Growth Factors (FGFs) are a family of growth factors that play crucial roles in various biological processes, including cell survival, proliferation, migration, and differentiation. They bind to specific tyrosine kinase receptors (FGFRs) on the cell surface, leading to intracellular signaling cascades that regulate gene expression and downstream cellular responses. FGFs are involved in embryonic development, tissue repair, and angiogenesis (the formation of new blood vessels). There are at least 22 distinct FGFs identified in humans, each with unique functions and patterns of expression. Some FGFs, like FGF1 and FGF2, have mitogenic effects on fibroblasts and other cell types, while others, such as FGF7 and FGF10, are essential for epithelial-mesenchymal interactions during organ development. Dysregulation of FGF signaling has been implicated in various pathological conditions, including cancer, fibrosis, and developmental disorders.
Phosphorus is an essential mineral that is required by every cell in the body for normal functioning. It is a key component of several important biomolecules, including adenosine triphosphate (ATP), which is the primary source of energy for cells, and deoxyribonucleic acid (DNA) and ribonucleic acid (RNA), which are the genetic materials in cells.
Phosphorus is also a major constituent of bones and teeth, where it combines with calcium to provide strength and structure. In addition, phosphorus plays a critical role in various metabolic processes, including energy production, nerve impulse transmission, and pH regulation.
The medical definition of phosphorus refers to the chemical element with the atomic number 15 and the symbol P. It is a highly reactive non-metal that exists in several forms, including white phosphorus, red phosphorus, and black phosphorus. In the body, phosphorus is primarily found in the form of organic compounds, such as phospholipids, phosphoproteins, and nucleic acids.
Abnormal levels of phosphorus in the body can lead to various health problems. For example, high levels of phosphorus (hyperphosphatemia) can occur in patients with kidney disease or those who consume large amounts of phosphorus-rich foods, and can contribute to the development of calcification of soft tissues and cardiovascular disease. On the other hand, low levels of phosphorus (hypophosphatemia) can occur in patients with malnutrition, vitamin D deficiency, or alcoholism, and can lead to muscle weakness, bone pain, and an increased risk of infection.
Sodium-phosphate cotransporter proteins, type IIa (NaPi-IIa), are a subtype of membrane transport proteins that facilitate the active transport of sodium and phosphate ions across the cell membrane. They play a crucial role in maintaining phosphate homeostasis within the body by regulating the reabsorption of phosphate in the kidney's proximal tubules.
NaPi-IIa proteins are located on the brush border membrane of the proximal tubule cells and function to couple the movement of sodium ions down its electrochemical gradient into the cell with the influx of phosphate ions against its concentration gradient, from the lumen into the cell. This process is driven by the sodium-potassium ATPase pump, which maintains a low intracellular sodium concentration and a negative membrane potential.
NaPi-IIa proteins are encoded by the SLC34A1 gene in humans and are subject to regulation by various hormonal and physiological factors, such as parathyroid hormone (PTH), fibroblast growth factor 23 (FGF23), and dietary phosphate intake. Dysregulation of NaPi-IIa function has been implicated in several kidney diseases and disorders of phosphate homeostasis, such as hyperphosphatemia and hypophosphatemic rickets.
Neoplasms of connective tissue are abnormal growths or tumors that develop from the cells that form the body's supportive framework, including bones, cartilage, tendons, ligaments, and other connective tissues. These neoplasms can be benign (non-cancerous) or malignant (cancerous), and they can cause various symptoms depending on their location and size.
There are several types of connective tissue neoplasms, including:
1. Fibroma: A benign tumor that arises from fibrous connective tissue.
2. Fibrosarcoma: A malignant tumor that develops from fibrous connective tissue.
3. Lipoma: A benign tumor that arises from fat cells.
4. Liposarcoma: A malignant tumor that develops from fat cells.
5. Chondroma: A benign tumor that arises from cartilage.
6. Chondrosarcoma: A malignant tumor that develops from cartilage.
7. Osteoma: A benign tumor that arises from bone.
8. Osteosarcoma: A malignant tumor that develops from bone.
9. Giant cell tumors: Benign or malignant tumors that contain many giant cells, which are large, multinucleated cells.
10. Synovial sarcoma: A malignant tumor that arises from the synovial tissue that lines joints and tendons.
Connective tissue neoplasms can cause various symptoms depending on their location and size. For example, a benign lipoma may cause a painless lump under the skin, while a malignant osteosarcoma may cause bone pain, swelling, and fractures. Treatment options for connective tissue neoplasms include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Hypercalciuria is a medical condition characterized by an excessive amount of calcium in the urine. It can occur when the body absorbs too much calcium from food, or when the bones release more calcium than usual. In some cases, it may be caused by certain medications, kidney disorders, or genetic factors.
Hypercalciuria can increase the risk of developing kidney stones and other kidney problems. It is often diagnosed through a 24-hour urine collection test that measures the amount of calcium in the urine. Treatment may include changes in diet, increased fluid intake, and medications to help reduce the amount of calcium in the urine.
Refeeding syndrome is a potentially fatal shift in fluid and electrolyte balance that may occur in malnourished individuals when they begin to receive nutrition. This occurs due to significant metabolic changes, including increased insulin secretion, which leads to shifts of fluids and electrolytes from the extracellular to intracellular space.
This shift can result in hypophosphatemia (low phosphate levels), hypokalemia (low potassium levels), hypomagnesemia (low magnesium levels), and fluid overload, which can cause serious complications such as heart failure, seizures, and even death if not properly managed. It's important to monitor and correct electrolyte imbalances and fluid status during refeeding to prevent these complications.
Parathyroid hormone (PTH) is a polypeptide hormone that plays a crucial role in the regulation of calcium and phosphate levels in the body. It is produced and secreted by the parathyroid glands, which are four small endocrine glands located on the back surface of the thyroid gland.
The primary function of PTH is to maintain normal calcium levels in the blood by increasing calcium absorption from the gut, mobilizing calcium from bones, and decreasing calcium excretion by the kidneys. PTH also increases phosphate excretion by the kidneys, which helps to lower serum phosphate levels.
In addition to its role in calcium and phosphate homeostasis, PTH has been shown to have anabolic effects on bone tissue, stimulating bone formation and preventing bone loss. However, chronic elevations in PTH levels can lead to excessive bone resorption and osteoporosis.
Overall, Parathyroid Hormone is a critical hormone that helps maintain mineral homeostasis and supports healthy bone metabolism.
Sodium-phosphate cotransporter proteins, type II (NPTII), are a group of membrane transport proteins that facilitate the active transport of inorganic phosphate (Pi) and sodium ions (Na+) across the cell membrane. They play a crucial role in maintaining intracellular phosphate homeostasis and regulating various physiological processes, including energy metabolism, signal transduction, and bone mineralization.
The type II sodium-phosphate cotransporters are further divided into three subtypes: NPT2a, NPT2b, and NPT2c. These subtypes differ in their tissue distribution, substrate affinity, and regulatory mechanisms. NPT2a is primarily expressed in the kidney proximal tubules and plays a major role in reabsorbing phosphate from the glomerular filtrate. NPT2b is predominantly found in the small intestine and contributes to phosphate absorption from the diet. NPT2c is widely distributed, with significant expression in the kidney, brain, and testis, although its specific functions are not as well understood as those of NPT2a and NPT2b.
Dysregulation of sodium-phosphate cotransporter proteins, type II, has been implicated in several pathological conditions, such as renal phosphate wasting disorders, tumoral calcinosis, and certain forms of hyperparathyroidism.
Calcitriol is the active form of vitamin D, also known as 1,25-dihydroxyvitamin D. It is a steroid hormone that plays a crucial role in regulating calcium and phosphate levels in the body to maintain healthy bones. Calcitriol is produced in the kidneys from its precursor, calcidiol (25-hydroxyvitamin D), which is derived from dietary sources or synthesized in the skin upon exposure to sunlight.
Calcitriol promotes calcium absorption in the intestines, helps regulate calcium and phosphate levels in the kidneys, and stimulates bone cells (osteoblasts) to form new bone tissue while inhibiting the activity of osteoclasts, which resorb bone. This hormone is essential for normal bone mineralization and growth, as well as for preventing hypocalcemia (low calcium levels).
In addition to its role in bone health, calcitriol has various other physiological functions, including modulating immune responses, cell proliferation, differentiation, and apoptosis. Calcitriol deficiency or resistance can lead to conditions such as rickets in children and osteomalacia or osteoporosis in adults.
Mesenchymoma is a very rare type of tumor that contains a mixture of different types of mesenchymal tissues, such as muscle, fat, bone, cartilage, or fibrous tissue. It typically occurs in children and young adults, and can be found in various parts of the body, including the head, neck, retroperitoneum (the area behind the abdominal cavity), and the limbs.
Mesenchymomas are usually slow-growing and may not cause any symptoms until they reach a large size. Treatment typically involves surgical removal of the tumor, but radiation therapy or chemotherapy may also be used in some cases. The prognosis for mesenchymoma depends on several factors, including the location and size of the tumor, the patient's age and overall health, and the specific types of tissue that are present in the tumor.
Paraneoplastic syndromes refer to a group of rare disorders that are caused by an abnormal immune system response to a cancerous (malignant) tumor. These syndromes are characterized by symptoms or signs that do not result directly from the growth of the tumor itself, but rather from substances produced by the tumor or the body's immune system in response to the tumor.
Paraneoplastic syndromes can affect various organs and systems in the body, including the nervous system, endocrine system, skin, and joints. Examples of paraneoplastic syndromes include Lambert-Eaton myasthenic syndrome (LEMS), which affects nerve function and causes muscle weakness; cerebellar degeneration, which can cause difficulty with coordination and balance; and dermatomyositis, which is an inflammatory condition that affects the skin and muscles.
Paraneoplastic syndromes can occur in association with a variety of different types of cancer, including lung cancer, breast cancer, ovarian cancer, and lymphoma. Treatment typically involves addressing the underlying cancer, as well as managing the symptoms of the paraneoplastic syndrome.
Sodium-phosphate cotransporter proteins are membrane transport proteins that facilitate the active transport of sodium and inorganic phosphate ions across biological membranes. These proteins play a crucial role in maintaining phosphate homeostasis within the body by regulating the absorption and excretion of phosphate in the kidneys and intestines. They exist in two major types, type I (NaPi-I) and type II (NaPi-II), each having multiple subtypes with distinct tissue distributions and regulatory mechanisms.
Type I sodium-phosphate cotransporters are primarily expressed in the kidney's proximal tubules and play a significant role in reabsorbing phosphate from the primary urine back into the bloodstream. Type II sodium-phosphate cotransporters, on the other hand, are found in both the kidneys and intestines. In the kidneys, they contribute to phosphate reabsorption, while in the intestines, they facilitate phosphate absorption from food.
These proteins function by coupling the passive downhill movement of sodium ions (driven by the electrochemical gradient) with the active uphill transport of phosphate ions against their concentration gradient. This coupled transport process enables cells to maintain intracellular phosphate concentrations within a narrow range, despite fluctuations in dietary intake and renal function.
Dysregulation of sodium-phosphate cotransporter proteins has been implicated in various pathological conditions, such as chronic kidney disease (CKD), tumoral calcinosis, and certain genetic disorders affecting phosphate homeostasis.
Hyperphosphatemia is a medical condition characterized by an excessively high level of phosphate (a form of the chemical element phosphorus) in the blood. Phosphate is an important component of various biological molecules, such as DNA, RNA, and ATP, and it plays a crucial role in many cellular processes, including energy metabolism and signal transduction.
In healthy individuals, the concentration of phosphate in the blood is tightly regulated within a narrow range to maintain normal physiological functions. However, when the phosphate level rises above this range (typically defined as a serum phosphate level greater than 4.5 mg/dL or 1.46 mmol/L), it can lead to hyperphosphatemia.
Hyperphosphatemia can result from various underlying medical conditions, including:
* Kidney dysfunction: The kidneys are responsible for filtering excess phosphate out of the blood and excreting it in the urine. When the kidneys fail to function properly, they may be unable to remove enough phosphate, leading to its accumulation in the blood.
* Hypoparathyroidism: The parathyroid glands produce a hormone called parathyroid hormone (PTH), which helps regulate calcium and phosphate levels in the body. In hypoparathyroidism, the production of PTH is insufficient, leading to an increase in phosphate levels.
* Hyperparathyroidism: In contrast, excessive production of PTH can also lead to hyperphosphatemia by increasing the release of phosphate from bones and decreasing its reabsorption in the kidneys.
* Excessive intake of phosphate-rich foods or supplements: Consuming large amounts of phosphate-rich foods, such as dairy products, nuts, and legumes, or taking phosphate supplements can raise blood phosphate levels.
* Tumor lysis syndrome: This is a complication that can occur after the treatment of certain types of cancer, particularly hematological malignancies. The rapid destruction of cancer cells releases large amounts of intracellular contents, including phosphate, into the bloodstream, leading to hyperphosphatemia.
* Rhabdomyolysis: This is a condition in which muscle tissue breaks down, releasing its contents, including phosphate, into the bloodstream. It can be caused by various factors, such as trauma, infection, or drug toxicity.
Hyperphosphatemia can have several adverse effects on the body, including calcification of soft tissues, kidney damage, and metabolic disturbances. Therefore, it is essential to diagnose and manage hyperphosphatemia promptly to prevent complications. Treatment options may include dietary modifications, medications that bind phosphate in the gastrointestinal tract, and dialysis in severe cases.
Respiratory alkalosis is a medical condition that occurs when there is an excess base (bicarbonate) and/or a decrease in carbon dioxide in the body. This leads to an increase in pH level of the blood, making it more alkaline than normal. Respiratory alkalosis is usually caused by conditions that result in hyperventilation, such as anxiety, lung disease, or high altitude. It can also be caused by certain medications and medical procedures. Symptoms of respiratory alkalosis may include lightheadedness, confusion, and tingling in the fingers and toes. Treatment typically involves addressing the underlying cause of the condition.
Fanconi syndrome is a medical condition that affects the proximal tubules of the kidneys. These tubules are responsible for reabsorbing various substances, such as glucose, amino acids, and electrolytes, back into the bloodstream after they have been filtered through the kidneys.
In Fanconi syndrome, there is a defect in the reabsorption process, causing these substances to be lost in the urine instead. This can lead to a variety of symptoms, including:
* Polyuria (excessive urination)
* Polydipsia (excessive thirst)
* Dehydration
* Metabolic acidosis (an imbalance of acid and base in the body)
* Hypokalemia (low potassium levels)
* Hypophosphatemia (low phosphate levels)
* Vitamin D deficiency
* Rickets (softening and weakening of bones in children) or osteomalacia (softening of bones in adults)
Fanconi syndrome can be caused by a variety of underlying conditions, including genetic disorders, kidney diseases, drug toxicity, and heavy metal poisoning. Treatment typically involves addressing the underlying cause, as well as managing symptoms such as electrolyte imbalances and acid-base disturbances.
Hypocalcemia is a medical condition characterized by an abnormally low level of calcium in the blood. Calcium is a vital mineral that plays a crucial role in various bodily functions, including muscle contraction, nerve impulse transmission, and bone formation. Normal calcium levels in the blood usually range from 8.5 to 10.2 milligrams per deciliter (mg/dL). Hypocalcemia is typically defined as a serum calcium level below 8.5 mg/dL or, when adjusted for albumin (a protein that binds to calcium), below 8.4 mg/dL (ionized calcium).
Hypocalcemia can result from several factors, such as vitamin D deficiency, hypoparathyroidism (underactive parathyroid glands), kidney dysfunction, certain medications, and severe magnesium deficiency. Symptoms of hypocalcemia may include numbness or tingling in the fingers, toes, or lips; muscle cramps or spasms; seizures; and, in severe cases, cognitive impairment or cardiac arrhythmias. Treatment typically involves correcting the underlying cause and administering calcium and vitamin D supplements to restore normal calcium levels in the blood.
Rhabdomyolysis is a medical condition characterized by the breakdown and degeneration of skeletal muscle fibers, leading to the release of their intracellular contents into the bloodstream. This can result in various complications, including electrolyte imbalances, kidney injury or failure, and potentially life-threatening conditions if not promptly diagnosed and treated.
The process of rhabdomyolysis typically involves three key components:
1. Muscle injury: Direct trauma, excessive exertion, prolonged immobilization, infections, metabolic disorders, toxins, or medications can cause muscle damage, leading to the release of intracellular components into the bloodstream.
2. Release of muscle contents: When muscle fibers break down, they release various substances, such as myoglobin, creatine kinase (CK), lactate dehydrogenase (LDH), aldolase, and potassium ions. Myoglobin is a protein that can cause kidney damage when present in high concentrations in the bloodstream, particularly when it is filtered through the kidneys and deposits in the renal tubules.
3. Systemic effects: The release of muscle contents into the bloodstream can lead to various systemic complications, such as electrolyte imbalances (particularly hyperkalemia), acidosis, hypocalcemia, and kidney injury or failure due to myoglobin-induced tubular damage.
Symptoms of rhabdomyolysis can vary widely depending on the severity and extent of muscle damage but may include muscle pain, weakness, swelling, stiffness, dark urine, and tea-colored or cola-colored urine due to myoglobinuria. In severe cases, patients may experience symptoms related to kidney failure, such as nausea, vomiting, fatigue, and decreased urine output.
Diagnosis of rhabdomyolysis typically involves measuring blood levels of muscle enzymes (such as CK and LDH) and evaluating renal function through blood tests and urinalysis. Treatment generally focuses on addressing the underlying cause of muscle damage, maintaining fluid balance, correcting electrolyte imbalances, and preventing or managing kidney injury.
25-Hydroxyvitamin D3 1-alpha-Hydroxylase is an enzyme that is responsible for converting 25-hydroxyvitamin D3 (a precursor form of vitamin D) to its active form, 1,25-dihydroxyvitamin D3. This activation process occurs primarily in the kidneys and is tightly regulated by various factors such as calcium levels, parathyroid hormone, and vitamin D status.
The activated form of vitamin D, 1,25-dihydroxyvitamin D3, plays a crucial role in maintaining calcium homeostasis by increasing the absorption of calcium from the gut and promoting bone health. It also has various other functions, including modulation of immune function, cell growth regulation, and protection against cancer.
Deficiencies in 25-Hydroxyvitamin D3 1-alpha-Hydroxylase can lead to vitamin D deficiency and its associated symptoms, such as osteomalacia (softening of the bones) and osteoporosis (brittle bones). Conversely, overactivity of this enzyme can result in hypercalcemia (elevated levels of calcium in the blood), which can cause a range of symptoms including kidney stones, abdominal pain, nausea, and vomiting.
Glucuronidase is an enzyme that catalyzes the hydrolysis of glucuronic acid from various substrates, including molecules that have been conjugated with glucuronic acid as part of the detoxification process in the body. This enzyme plays a role in the breakdown and elimination of certain drugs, toxins, and endogenous compounds, such as bilirubin. It is found in various tissues and organisms, including humans, bacteria, and insects. In clinical contexts, glucuronidase activity may be measured to assess liver function or to identify the presence of certain bacterial infections.
Osteocytes are the most abundant cell type in mature bone tissue. They are star-shaped cells that are located inside the mineralized matrix of bones, with their processes extending into small spaces called lacunae and canaliculi. Osteocytes are derived from osteoblasts, which are bone-forming cells that become trapped within the matrix they produce.
Osteocytes play a crucial role in maintaining bone homeostasis by regulating bone remodeling, sensing mechanical stress, and modulating mineralization. They communicate with each other and with osteoblasts and osteoclasts (bone-resorbing cells) through a network of interconnected processes and via the release of signaling molecules. Osteocytes can also respond to changes in their environment, such as hormonal signals or mechanical loading, by altering their gene expression and releasing factors that regulate bone metabolism.
Dysfunction of osteocytes has been implicated in various bone diseases, including osteoporosis, osteogenesis imperfecta, and Paget's disease of bone.
Vitamin D is a fat-soluble secosteroid that is crucial for the regulation of calcium and phosphate levels in the body, which are essential for maintaining healthy bones and teeth. It can be synthesized by the human body when skin is exposed to ultraviolet-B (UVB) rays from sunlight, or it can be obtained through dietary sources such as fatty fish, fortified dairy products, and supplements. There are two major forms of vitamin D: vitamin D2 (ergocalciferol), which is found in some plants and fungi, and vitamin D3 (cholecalciferol), which is produced in the skin or obtained from animal-derived foods. Both forms need to undergo two hydroxylations in the body to become biologically active as calcitriol (1,25-dihydroxyvitamin D3), the hormonally active form of vitamin D. This activated form exerts its effects by binding to the vitamin D receptor (VDR) found in various tissues, including the small intestine, bone, kidney, and immune cells, thereby influencing numerous physiological processes such as calcium homeostasis, bone metabolism, cell growth, and immune function.
Dietary Phosphorus is a mineral that is an essential nutrient for human health. It is required for the growth, maintenance, and repair of body tissues, including bones and teeth. Phosphorus is also necessary for the production of energy, the formation of DNA and RNA, and the regulation of various physiological processes.
In the diet, phosphorus is primarily found in protein-containing foods such as meat, poultry, fish, dairy products, legumes, and nuts. It can also be found in processed foods that contain additives such as phosphoric acid, which is used to enhance flavor or as a preservative.
The recommended daily intake of phosphorus for adults is 700 milligrams (mg) per day. However, it's important to note that excessive intake of phosphorus, particularly from supplements and fortified foods, can lead to health problems such as kidney damage and calcification of soft tissues. Therefore, it's recommended to obtain phosphorus primarily from whole foods rather than supplements.
Hypercalcemia is a medical condition characterized by an excess of calcium ( Ca2+ ) in the blood. While the normal range for serum calcium levels is typically between 8.5 to 10.2 mg/dL (milligrams per deciliter) or 2.14 to 2.55 mmol/L (millimoles per liter), hypercalcemia is generally defined as a serum calcium level greater than 10.5 mg/dL or 2.6 mmol/L.
Hypercalcemia can result from various underlying medical disorders, including primary hyperparathyroidism, malignancy (cancer), certain medications, granulomatous diseases, and excessive vitamin D intake or production. Symptoms of hypercalcemia may include fatigue, weakness, confusion, memory loss, depression, constipation, nausea, vomiting, increased thirst, frequent urination, bone pain, and kidney stones. Severe or prolonged hypercalcemia can lead to serious complications such as kidney failure, cardiac arrhythmias, and calcification of soft tissues. Treatment depends on the underlying cause and severity of the condition.
Phosphorus metabolism disorders refer to a group of conditions that affect the body's ability to properly regulate the levels and utilization of phosphorus. Phosphorus is an essential mineral that plays a critical role in many biological processes, including energy production, bone formation, and nerve function.
Disorders of phosphorus metabolism can result from genetic defects, kidney dysfunction, vitamin D deficiency, or other medical conditions. These disorders can lead to abnormal levels of phosphorus in the blood, which can cause a range of symptoms, including muscle weakness, bone pain, seizures, and respiratory failure.
Examples of phosphorus metabolism disorders include:
1. Hypophosphatemia: This is a condition characterized by low levels of phosphorus in the blood. It can be caused by various factors, such as malnutrition, vitamin D deficiency, and kidney dysfunction.
2. Hyperphosphatemia: This is a condition characterized by high levels of phosphorus in the blood. It can be caused by kidney failure, tumor lysis syndrome, and certain medications.
3. Hereditary hypophosphatemic rickets: This is a genetic disorder that affects the body's ability to regulate vitamin D and phosphorus metabolism. It can lead to weakened bones and skeletal deformities.
4. Oncogenic osteomalacia: This is a rare condition that occurs when tumors produce substances that interfere with phosphorus metabolism, leading to bone pain and weakness.
Treatment for phosphorus metabolism disorders depends on the underlying cause of the disorder and may include dietary changes, supplements, medications, or surgery.
"Bone" is the hard, dense connective tissue that makes up the skeleton of vertebrate animals. It provides support and protection for the body's internal organs, and serves as a attachment site for muscles, tendons, and ligaments. Bone is composed of cells called osteoblasts and osteoclasts, which are responsible for bone formation and resorption, respectively, and an extracellular matrix made up of collagen fibers and mineral crystals.
Bones can be classified into two main types: compact bone and spongy bone. Compact bone is dense and hard, and makes up the outer layer of all bones and the shafts of long bones. Spongy bone is less dense and contains large spaces, and makes up the ends of long bones and the interior of flat and irregular bones.
The human body has 206 bones in total. They can be further classified into five categories based on their shape: long bones, short bones, flat bones, irregular bones, and sesamoid bones.
Parturient paresis, also known as Eclampsia or Puerperal eclampsia, is a serious condition that can occur during pregnancy or after childbirth. It is characterized by the onset of seizures (convulsions) and coma in a woman who has previously developed high blood pressure and proteinuria (protein in the urine) – a condition known as preeclampsia.
Eclampsia is considered a medical emergency, and it can lead to severe complications for both the mother and the baby if not promptly treated. The exact cause of eclampsia is not fully understood, but it is thought to be related to problems with the blood vessels that supply the placenta.
Symptoms of eclampsia include high blood pressure, severe headaches, visual disturbances, nausea and vomiting, and sudden weight gain. If left untreated, eclampsia can lead to serious complications such as brain damage, stroke, kidney failure, and even death for the mother and the baby.
Treatment typically involves close monitoring of the mother and the baby, medication to control seizures and lower blood pressure, and delivery of the baby if necessary. In some cases, eclampsia may occur after the baby has been delivered, in which case it is known as postpartum eclampsia.
Hyperparathyroidism is a condition in which the parathyroid glands produce excessive amounts of parathyroid hormone (PTH). There are four small parathyroid glands located in the neck, near or within the thyroid gland. They release PTH into the bloodstream to help regulate the levels of calcium and phosphorus in the body.
In hyperparathyroidism, overproduction of PTH can lead to an imbalance in these minerals, causing high blood calcium levels (hypercalcemia) and low phosphate levels (hypophosphatemia). This can result in various symptoms such as fatigue, weakness, bone pain, kidney stones, and cognitive issues.
There are two types of hyperparathyroidism: primary and secondary. Primary hyperparathyroidism occurs when there is a problem with one or more of the parathyroid glands, causing them to become overactive and produce too much PTH. Secondary hyperparathyroidism develops as a response to low calcium levels in the body due to conditions like vitamin D deficiency, chronic kidney disease, or malabsorption syndromes.
Treatment for hyperparathyroidism depends on the underlying cause and severity of symptoms. In primary hyperparathyroidism, surgery to remove the overactive parathyroid gland(s) is often recommended. For secondary hyperparathyroidism, treating the underlying condition and managing calcium levels with medications or dietary changes may be sufficient.
Muscular diseases, also known as myopathies, refer to a group of conditions that affect the functionality and health of muscle tissue. These diseases can be inherited or acquired and may result from inflammation, infection, injury, or degenerative processes. They can cause symptoms such as weakness, stiffness, cramping, spasms, wasting, and loss of muscle function.
Examples of muscular diseases include:
1. Duchenne Muscular Dystrophy (DMD): A genetic disorder that results in progressive muscle weakness and degeneration due to a lack of dystrophin protein.
2. Myasthenia Gravis: An autoimmune disease that causes muscle weakness and fatigue, typically affecting the eyes and face, throat, and limbs.
3. Inclusion Body Myositis (IBM): A progressive muscle disorder characterized by muscle inflammation and wasting, typically affecting older adults.
4. Polymyositis: An inflammatory myopathy that causes muscle weakness and inflammation throughout the body.
5. Metabolic Myopathies: A group of inherited disorders that affect muscle metabolism, leading to exercise intolerance, muscle weakness, and other symptoms.
6. Muscular Dystonias: Involuntary muscle contractions and spasms that can cause abnormal postures or movements.
It is important to note that muscular diseases can have a significant impact on an individual's quality of life, mobility, and overall health. Proper diagnosis and treatment are crucial for managing symptoms and improving outcomes.
Nephrolithiasis is a medical term that refers to the presence of stones or calculi in the kidney. These stones can form anywhere in the urinary tract, including the kidneys, ureters, bladder, and urethra. Nephrolithiasis is also commonly known as kidney stones.
Kidney stones are hard deposits made up of minerals and salts that crystallize in the urine. They can vary in size from tiny sand-like particles to larger pebble or even golf ball-sized masses. Kidney stones can cause pain, bleeding, and infection if they block the flow of urine through the urinary tract.
The formation of kidney stones is often associated with a variety of factors such as dehydration, high levels of calcium, oxalate, or uric acid in the urine, family history, obesity, and certain medical conditions like gout or inflammatory bowel disease. Treatment for nephrolithiasis depends on the size and location of the stone, as well as the severity of symptoms. Small stones may pass spontaneously with increased fluid intake, while larger stones may require medication, shock wave lithotripsy, or surgical removal.
The parathyroid glands are four small endocrine glands located in the neck, usually near or behind the thyroid gland. They secrete parathyroid hormone (PTH), which plays a critical role in regulating calcium and phosphate levels in the blood and bones. PTH helps maintain the balance of these minerals by increasing the absorption of calcium from food in the intestines, promoting reabsorption of calcium in the kidneys, and stimulating the release of calcium from bones when needed. Additionally, PTH decreases the excretion of calcium through urine and reduces phosphate reabsorption in the kidneys, leading to increased phosphate excretion. Disorders of the parathyroid glands can result in conditions such as hyperparathyroidism (overactive glands) or hypoparathyroidism (underactive glands), which can have significant impacts on calcium and phosphate homeostasis and overall health.
Acidosis is a medical condition that occurs when there is an excess accumulation of acid in the body or when the body loses its ability to effectively regulate the pH level of the blood. The normal pH range of the blood is slightly alkaline, between 7.35 and 7.45. When the pH falls below 7.35, it is called acidosis.
Acidosis can be caused by various factors, including impaired kidney function, respiratory problems, diabetes, severe dehydration, alcoholism, and certain medications or toxins. There are two main types of acidosis: metabolic acidosis and respiratory acidosis.
Metabolic acidosis occurs when the body produces too much acid or is unable to eliminate it effectively. This can be caused by conditions such as diabetic ketoacidosis, lactic acidosis, kidney failure, and ingestion of certain toxins.
Respiratory acidosis, on the other hand, occurs when the lungs are unable to remove enough carbon dioxide from the body, leading to an accumulation of acid. This can be caused by conditions such as chronic obstructive pulmonary disease (COPD), asthma, and sedative overdose.
Symptoms of acidosis may include fatigue, shortness of breath, confusion, headache, rapid heartbeat, and in severe cases, coma or even death. Treatment for acidosis depends on the underlying cause and may include medications, oxygen therapy, fluid replacement, and dialysis.
I'm sorry for any confusion, but "opossums" are not a medical term or a medical condition. Opossums are actually marsupials (pouched mammals) that are native to the Americas. They are often known for their "playing dead" behavior as a defense mechanism when threatened. If you have any questions about medical terminology or health-related topics, I'd be happy to help with those!
Physiologic calcification is the normal deposit of calcium salts in body tissues and organs. It is a natural process that occurs as part of the growth and development of the human body, as well as during the repair and remodeling of tissues.
Calcium is an essential mineral that plays a critical role in many bodily functions, including bone formation, muscle contraction, nerve impulse transmission, and blood clotting. In order to maintain proper levels of calcium in the body, excess calcium that is not needed for these functions may be deposited in various tissues as a normal part of the aging process.
Physiologic calcification typically occurs in areas such as the walls of blood vessels, the lungs, and the heart valves. While these calcifications are generally harmless, they can sometimes lead to complications, particularly if they occur in large amounts or in sensitive areas. For example, calcification of the coronary arteries can increase the risk of heart disease, while calcification of the lung tissue can cause respiratory symptoms.
It is important to note that pathologic calcification, on the other hand, refers to the abnormal deposit of calcium salts in tissues and organs, which can be caused by various medical conditions such as chronic kidney disease, hyperparathyroidism, and certain infections. Pathologic calcification is not a normal process and can lead to serious health complications if left untreated.
A kidney, in medical terms, is one of two bean-shaped organs located in the lower back region of the body. They are essential for maintaining homeostasis within the body by performing several crucial functions such as:
1. Regulation of water and electrolyte balance: Kidneys help regulate the amount of water and various electrolytes like sodium, potassium, and calcium in the bloodstream to maintain a stable internal environment.
2. Excretion of waste products: They filter waste products from the blood, including urea (a byproduct of protein metabolism), creatinine (a breakdown product of muscle tissue), and other harmful substances that result from normal cellular functions or external sources like medications and toxins.
3. Endocrine function: Kidneys produce several hormones with important roles in the body, such as erythropoietin (stimulates red blood cell production), renin (regulates blood pressure), and calcitriol (activated form of vitamin D that helps regulate calcium homeostasis).
4. pH balance regulation: Kidneys maintain the proper acid-base balance in the body by excreting either hydrogen ions or bicarbonate ions, depending on whether the blood is too acidic or too alkaline.
5. Blood pressure control: The kidneys play a significant role in regulating blood pressure through the renin-angiotensin-aldosterone system (RAAS), which constricts blood vessels and promotes sodium and water retention to increase blood volume and, consequently, blood pressure.
Anatomically, each kidney is approximately 10-12 cm long, 5-7 cm wide, and 3 cm thick, with a weight of about 120-170 grams. They are surrounded by a protective layer of fat and connected to the urinary system through the renal pelvis, ureters, bladder, and urethra.
Total Parenteral Nutrition (TPN) is a medical term used to describe a specialized nutritional support system that is delivered through a vein (intravenously). It provides all the necessary nutrients that a patient needs, such as carbohydrates, proteins, fats, vitamins, and minerals. TPN is typically used when a patient cannot eat or digest food through their gastrointestinal tract for various reasons, such as severe malabsorption, intestinal obstruction, or inflammatory bowel disease. The term "total" indicates that the nutritional support is complete and meets all of the patient's nutritional needs.
Calcium is an essential mineral that is vital for various physiological processes in the human body. The medical definition of calcium is as follows:
Calcium (Ca2+) is a crucial cation and the most abundant mineral in the human body, with approximately 99% of it found in bones and teeth. It plays a vital role in maintaining structural integrity, nerve impulse transmission, muscle contraction, hormonal secretion, blood coagulation, and enzyme activation.
Calcium homeostasis is tightly regulated through the interplay of several hormones, including parathyroid hormone (PTH), calcitonin, and vitamin D. Dietary calcium intake, absorption, and excretion are also critical factors in maintaining optimal calcium levels in the body.
Hypocalcemia refers to low serum calcium levels, while hypercalcemia indicates high serum calcium levels. Both conditions can have detrimental effects on various organ systems and require medical intervention to correct.
 Bone Mineralization and Related Disorders: Practice Essentials, Vitamin D Metabolism, Pathophysiology
Bone Mineralization and Related Disorders: Practice Essentials, Vitamin D Metabolism, Pathophysiology
Bone Mineralization and Related Disorders: Practice Essentials, Vitamin D Metabolism, Pathophysiology
 Article - Billing and Coding: Vitamin D Assay Testing (A57484)
Article - Billing and Coding: Vitamin D Assay Testing (A57484)
Calcijex, Rocaltrol (calcitriol) dosing, indications, interactions, adverse effects, and more
 X-linked hypophosphatemia - Wikipedia
X-linked hypophosphatemia - Wikipedia
 Hypophosphatemia (definition)
Hypophosphatemia (definition)
 Rocaltrol 0.5 microgram Capsules - Summary of Product Characteristics (SmPC) - (emc)
Rocaltrol 0.5 microgram Capsules - Summary of Product Characteristics (SmPC) - (emc)
Dental Abscess: Practice Essentials, Pathophysiology, Epidemiology
 International Classification of Diseases - Endocrine, Nutritional and Metabolic Diseases, and Immunity Disorders
International Classification of Diseases - Endocrine, Nutritional and Metabolic Diseases, and Immunity Disorders
KoreaMed
Shu-Hwa Chen - 研究成果 - 臺北醫學大學
 Division of Nephrology, Hypertension & Apheresis - Research output
- Research Profiles at Washington University School of...
Division of Nephrology, Hypertension & Apheresis - Research output
- Research Profiles at Washington University School of...
A Familial Case of a Whole Germline CDC73 Deletion Discordant for Primary Hyperparathyroidism<...
 Vitamin D 50000 Iu Benefits - VitaminProGuide.com
Vitamin D 50000 Iu Benefits - VitaminProGuide.com
Vitamin D 50000 Iu Daily - VitaminProGuide.com
 Ms-D3 Softgel Capsule 4's Price, Uses, Side Effects, Composition - Apollo Pharmacy
Ms-D3 Softgel Capsule 4's Price, Uses, Side Effects, Composition - Apollo Pharmacy
Familial hypocalciuric hypercalcemia with a de novo heterozygous mutation of calcium-sensing receptor in: Endocrinology,...
D3 Max 60K Softgel Capsule 4's Price, Uses, Side Effects, Composition - Apollo Pharmacy
 Hypophosphatemic Rickets | Bone and Spine
Hypophosphatemic Rickets | Bone and Spine
 How Vitamin D3 Essential Oil Help Us in Maintaining Optimum Health Condition?
How Vitamin D3 Essential Oil Help Us in Maintaining Optimum Health Condition?
paolo found 73 records - Provincial Hospitals Library Catalogue - Nova Scotia Health Authority
Phosphate (Phosphorus): Reference Range, Interpretation, Collection and Panels
![Arthralgia[Clinical Features] OR 13917[uid] - MedGen -...](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAYAAAAf8/9hAAAB1ElEQVQ4jaWSPWgTcRjGf/ehuWhobO2JxGJRY3taTTRV2yoqSpW6iIWO4iAoUsRBioNDKUWKLU7i4KA4OfhVREQnETRia03k7IdiS0LaQYKJQg3mLtfc30GySNUDn/V5nx/vy/vAf0pqad3db2xquiBJku93s2Tb2eEHdw1rTcsxol23sObTjN7oIp9KVmaU9kMdTxcLAyiqGtA0bfms+XKQULSdQG2EmnUx0q9ughAA8p/CFW0IN3Sv0vUI5p2zIMpUrd5JeP/Jii//80ZJUlrb9lyV8qn3zI5dB8A4MoBWtcITAKBmZe3eRmPzccYf9uIUsyzx6zQd7fMMAIjFdgxpkuPy4clFANbu6qa6fouybXtznxeAoqoBn0/zz5kvBqVQ5DBasJ5gXaPnDQAWFpwCkiwLZekyAMp2wTPAsqy5d8nEZcIHThPQo7jlIua9854BibdvekqKX8PouARAOn6F+c8pT4Bc7svz6U8f77O1cwDVV439PcPU4yHw8AUhhDPyOn4OfWOMuuZfBZp41INTLACorhC2/Jc2zsxMX8vl8lMcPBUHFL5mnpEZGa748sS42esKYS8WLtl2NjE22s/6fScIhtr48W2S5O0zIFwvp3vST6Z+myCvkaonAAAAAElFTkSuQmCC) "Arthralgia"[Clinical Features] OR 13917[uid] - MedGen -...
"Arthralgia"[Clinical Features] OR 13917[uid] - MedGen -...
 Identification of a second kindred with familial hypocalciuric hypercalcemia type 3 (FHH3) narrows localization to a |3.5...
Identification of a second kindred with familial hypocalciuric hypercalcemia type 3 (FHH3) narrows localization to a |3.5...
 SgIndrop D Capsules | Vitamin D3|Cholecalciferol | Fareed Pharma World
SgIndrop D Capsules | Vitamin D3|Cholecalciferol | Fareed Pharma World
Chiari malformation, syringomyelia and bulbar palsy in X linked hypophosphataemia. - Immunology
 Calcitriol: Uses, Interactions, Mechanism of Action | DrugBank Online
Calcitriol: Uses, Interactions, Mechanism of Action | DrugBank Online
 1674882789 - Passmed UK
1674882789 - Passmed UKLumped in with autosoma1
- X-linked hypophosphatemia may be lumped in with autosomal dominant hypophosphatemic rickets under general terms such as hypophosphatemic rickets. (wikipedia.org)
Hypoparathyroidism6
- This soft capsule can be used with other medications to treat hypocalcemia brought on by hypoparathyroidism, familial hypophosphatemia, or pseudohypoparathyroidism. (fareedpharma.com)
- Used to treat vitamin D deficiency or insufficiency, refractory rickets (vitamin D resistant rickets), familial hypophosphatemia and hypoparathyroidism, and in the management of hypocalcemia and renal osteodystrophy in patients with chronic renal failure undergoing dialysis. (drugbank.com)
- Vitamin D is also used with other medications to treat low levels of calcium or phosphate caused by certain disorders (such as hypoparathyroidism, pseudohypoparathyroidism, familial hypophosphatemia). (shelter.co.in)
- Vitamin D is additionally utilized with different prescriptions to treat low degrees of calcium or phosphate brought about by specific problems (like hypoparathyroidism, pseudohypoparathyroidism, familial hypophosphatemia). (medikartindia.com)
- Additionally, vitamin D supplements are sometimes used in combination with other medications to combat low levels of calcium or phosphate caused by specific disorders, such as hypoparathyroidism, pseudohypoparathyroidism, or familial hypophosphatemia. (arisoapp.com)
- Because vitamin D is involved in regulating the levels of minerals such as phosphorous and calcium, it is used for conditions caused by low levels of phosphorous (familial hypophosphatemia and Fanconi syndrome) and low levels of calcium (hypoparathyroidism and pseudohypoparathyroidism). (nutritioncy.com)
Rickets9
- X-linked hypophosphatemia (XLH) is an X-linked dominant form of rickets (or osteomalacia) that differs from most cases of dietary deficiency rickets in that vitamin D supplementation does not cure it. (wikipedia.org)
- An outstanding feature of familial hypophosphatemic rickets is disproportionate short stature. (boneandspine.com)
- Hypophosphatemic rickets is a genetic disorder characterized by hypophosphatemia, defective intestinal absorption of calcium, and rickets or osteomalacia unresponsive to vitamin D . It is usually hereditary. (msdmanuals.com)
- The disease manifests as a spectrum of abnormalities, from hypophosphatemia alone to growth retardation and short stature to severe rickets or osteomalacia. (msdmanuals.com)
- This review was conducted to study the diagnosis, treatment, and growth progression in infants and adolescents with familial hypophosphatemic rickets. (uky.edu)
- The bibliographic search was carried out utilizing the electronic databases MEDLINE, OVID, and LILACS and by direct research within the last 15 years using the keywords rickets, familial hypophosphatemia, vitamin D deficiency, stature growth, childhood, and adolescence. (uky.edu)
- Article selection was done by comparing the evaluation of the growth in patients with familial hypophosphatemic rickets, including the variables that might affect them, for possible future therapeutic proposals. (uky.edu)
- It is concluded that the most significant fact in the treatment of familial hypophosphatemic rickets in infancy was the magnitude of the final stature. (uky.edu)
- Overactivity of fibroblast growth factor 23 reduces phosphate reabsorption by the kidneys, leading to low levels of phosphate in the blood (hypophosphatemia) and related problems with bone growth in people with autosomal dominant hypophosphatemic rickets. (encyclopedia.pub)
Pseudohypoparathyroidism1
- Vitamin D3 supplements are often used to treat disorders such as pseudohypoparathyroidism and familial hypophosphatemia. (truehealingnaturals.com)
Hypercalcemia5
- Laboratory tests showed hypercalcemia (13.6 mg/dL), hypophosphatemia (2.4 mg/dL), and elevated intact PTH level (149 pg/mL). (elsevierpure.com)
- Familial hypocalciuric hypercalcemia and neonatal severe hyperparathyroidism also belong to this category. (medscape.com)
- CONTEXT: Familial hypocalciuric hypercalcemia (FHH) is a genetically heterogenous disorder that consists of three defined types, FHH1, FHH2, and FHH3 whose chromosomal locations are 3q21.1, 19p, and 19q13, respectively. (ox.ac.uk)
- BACKGROUND: Familial hypocalciuric hypercalcemia (FHH) is one of the conditions that should be considered in the differential diagnosis of hypercalcemia and normo-hypophosphatemia in childhood. (bvsalud.org)
- Primary hyperparathyroidism is characterized by hypercalcemia and hypophosphatemia, secondary hyperparathyroidism is characterized by hyperphosphatemia and mild hypocalcemia, and tertiary hyperparathyroidism is characterized by hypercalcemia. (washington.edu)
Phosphate4
- The overactivity of FGF-23 reduces vitamin D 1α-hydroxylation and phosphate reabsorption by the kidneys, leading to hypophosphatemia and the related features of ricket. (wikipedia.org)
- Ms-D3 Softgel Capsule 4's is also used in the treatment of familial hypophosphatemia (a group of rare inherited disorders characterized by impaired kidney conservation of phosphate and in some cases, altered vitamin D metabolism). (apollopharmacy.in)
- Defective phosphate transport and hypophosphatemia in this case result in appropriately increased 1,25-dihydroxyvitamin D3 levels, thus leading to hypercalciuria. (msdmanuals.com)
- At least seven mutations in the FGF23 gene have been found to cause hyperphosphatemic familial tumoral calcinosis (HFTC), a condition characterized by an increase in the levels of phosphate in the blood (hyperphosphatemia) and abnormal deposits of phosphate and calcium (calcinosis) in the body's tissues. (encyclopedia.pub)
Disorders3
- Introduction: Primary hyperparathyroidism (PHPT) occurs as part of familial syndromes, including CDC73-related disorders caused by germline pathogenic variants of the CDC73 gene, particularly in early adulthood. (elsevierpure.com)
- In addition to hypophosphatemia, these disorders all have normal glomerular filtration rate, normal serum levels of calcium. (boneandspine.com)
- Vitamin D supplements can be used to help treat inherited disorders resulting from an inability to absorb or process vitamin D, such as familial hypophosphatemia. (cloud9acuclinic.com)
Adenomatous polyposis1
- Incidental Finding of Attenuated Familial Adenomatous Polyposis. (cdc.gov)
Hypomagnesemia1
- Echinocytes occur in many conditions, including malnutrition associated with mild hemolysis due to hypomagnesemia and hypophosphatemia, uremia, hemolytic anemia in long-distance runners, and pyruvate kinase deficiency . (medscape.com)
Vitamin1
- an active form of vitamin D, used to treat kidney disease with low blood calcium, hyperparathyroidism due to kidney disease, osteoporosis, and familial hypophosphatemia. (what-i-believe.ca)
Hyperparathyroidism1
- Familial cases can occur as either part of the multiple endocrine neoplasia syndromes (MEN 1 or MEN 2a), hyperparathyroid-jaw tumor (HPT-JT) syndrome, or familial isolated hyperparathyroidism (FIHPT). (medscape.com)
Syndromes1
- Tumor-induced osteomalacia has similar clinical manifestations to the familial syndromes. (boneandspine.com)
Renal1
- Diagnosis is based on the presence of all three of the following criteria: low-molecular-weight proteinuria, hypercalciuria and at least one of the following: nephrocalcinosis, kidney stones, hematuria, hypophosphatemia or renal insufficiency. (ox.ac.uk)
Mediterranean1
- Familial Mediterranean fever (FMF) is divided into two phenotypes: type 1 and type 2. (beds.ac.uk)
Severe1
- The phenotypic spectrum of X-linked hypophosphatemia (XLH) ranges from isolated hypophosphatemia to severe lower-extremity bowing. (beds.ac.uk)
Mild1
- RESULTS: Sixteen members were hypercalcemic with normal or elevated serum PTH concentrations and mild hypophosphatemia, features consistent with FHH3. (ox.ac.uk)
Disease2
- No genotype-phenotype correlation has been described thus far, and there is considerable intra-familial variability in disease severity. (ox.ac.uk)
- It was first described by Jones in 1933 as a familial multilocular cystic disease of the jaws. (washington.edu)
Conditions1
- Developmental conditions include abnormal morphology of the crown (eg, dens invaginatus, dens evaginatus) and abnormal structure of the dentine (eg, dentine dysplasia, dentinogenesis imperfecta, osteogenesis imperfecta , familial hypophosphatemia). (medscape.com)
Case1
- Herein, we report a familial case of a whole germline CDC73 deletion discordant for PHPT. (elsevierpure.com)
Rare1
- X linked hypophosphataemia (XLH) is a rare condition with numerous musculoskeletal complications. (ox.ac.uk)
Review1
- Healthcare Transition from Pediatric- to Adult-Focused Care in X-Linked Hypophosphatemia: Review and Expert Consensus. (cdc.gov)
Hypoparathyroidism6
- Ergocalciferol is indicated for use in the treatment of hypoparathyroidism, refractory rickets, also known as vitamin D resistant rickets, and familial hypophosphatemia. (nih.gov)
- Ergocalciferol capsules are indicated for use in the treatment of hypoparathyroidism, refractory rickets, also known as vitamin D resistant rickets, and familial hypophosphatemia. (nih.gov)
- Ergocalciferol is used in the treatment of hypoparathyroidism (condition in which the body does not produce enough parathyroid hormone), refractory rickets (softening and weakening of bones that does not respond to treatment), and familial hypophosphatemia (rickets or osteomalacia caused by an inherited condition with a decreased ability to break down vitamin D in the body). (medlineplus.gov)
- It is also used to treat low levels of calcium or phosphate caused by hypoparathyroidism, pseudohypoparathyroidism and familial hypophosphatemia. (optionrx.com)
- Vitamin D is also used with other medications to treat low levels of calcium or phosphate caused by certain disorders (such as hypoparathyroidism, pseudohypoparathyroidism, familial hypophosphatemia). (shelter.co.in)
- Vitamin D is additionally utilized with different prescriptions to treat low degrees of calcium or phosphate brought about by specific problems (like hypoparathyroidism, pseudohypoparathyroidism, familial hypophosphatemia). (medikartindia.com)
Hereditary5
- Hypophosphatemic rickets is a genetic disorder characterized by hypophosphatemia, defective intestinal absorption of calcium, and rickets or osteomalacia unresponsive to vitamin D . It is usually hereditary. (msdmanuals.com)
- X-linked hypophosphatemia (XLH) is a hereditary, progressive, and lifelong rare disease that affects up to 1 in 20,000 people. (xlhlink.com)
- The remaining 20% of familial hypophosphatemia patients have autosomal dominant hypophosphatemic rickets from gain-of-function autosomal recessive hypophosphatemic rickets and hereditary hypophosphatemic rickets with hypercalciuria. (medscape.com)
- Hypophosphatemic rickets(HR),also known as familial hypophosphatemia,is a hereditary disease characterized by hypophosphatemia and renal phosphate loss,mainly manifested as bone mineralization disorders. (magtech.com.cn)
- 13] Rafaelsen S,Johansson S,Raeder H,et al.Hereditary hypophosphatemia in Norway:a retrospective population-based study of genotypes,phenotypes,and treatment complications[J].Eur J Endocrinol,2016,174(2):125-136. (magtech.com.cn)
Osteomalacia4
- Hyperphosphatemia and hypophosphatemia both lead to the development of diseases, such as hyperphosphatemic tumoral calcinosis and rickets/osteomalacia, respectively. (nih.gov)
- X-linked hypophosphatemia (XLH) is an X-linked dominant form of rickets (or osteomalacia) that differs from most cases of dietary deficiency rickets in that vitamin D supplementation does not cure it. (wikipedia.org)
- Calcitriol is also sometimes used to treat rickets (softening and weakening of bones in children caused by lack of vitamin D), osteomalacia (softening and weakening of bones in adults caused by lack of vitamin D), and familial hypophosphatemia (rickets or osteomalacia caused by decreased ability to break down vitamin D in the body). (medlineplus.gov)
- The disease manifests as a spectrum of abnormalities, from hypophosphatemia alone to growth retardation and short stature to severe rickets or osteomalacia. (msdmanuals.com)
Hyperphosphatemia1
- At least seven mutations in the FGF23 gene have been found to cause hyperphosphatemic familial tumoral calcinosis (HFTC), a condition characterized by an increase in the levels of phosphate in the blood (hyperphosphatemia) and abnormal deposits of phosphate and calcium (calcinosis) in the body's tissues. (nih.gov)
Genetic3
- Genetic counseling can be offered to family members of affected individuals and genetic screening for the CASR familial mutation. (orpha.net)
- With recent advances in the understanding of the genetic basis of familial hypophosphatemic rickets, the term X-linked hypophosphatemic rickets has become more commonly used. (medscape.com)
- Phosphate homeostasis and genetic mutations of familial hypophosphatemic rickets. (bredagenetics.com)
Tumoral calcinosis1
- Hyperphosphatemic familial tumoral calcinosis (HFTC) is a rare and disabling disorder of fibroblast growth factor 23 (FGF23) deficiency or resistance. (nih.gov)
Autosomal2
- Overactivity of fibroblast growth factor 23 reduces phosphate reabsorption by the kidneys, leading to low levels of phosphate in the blood (hypophosphatemia) and related problems with bone growth in people with autosomal dominant hypophosphatemic rickets. (nih.gov)
- 11] Menon LP,Weinstein RS.Iron replacement ameliorates hypophosphatemia in autosomal dominant hypophosphatemic rickets:A review of the role of iron. (magtech.com.cn)
Hypokalemia1
- Rhabdomyolysis following severe hypokalemia caused by familial hypokalemic periodic paralysis. (wjgnet.com)
Hypocalcemia1
- Hypocalcemia and hypophosphatemia have also been described. (tnwmovie.com)
Phosphorus5
- Hypophosphatemia (the H in XLH) is a condition caused by a low level of phosphorus in the blood. (xlhlink.com)
- Sodium Phosphates Injection, USP, 3mM P/mL, is indicated as a source of phosphorus, for addition to large volume intravenous fluids, to prevent or correct hypophosphatemia in patients with restricted or no oral intake. (ncats.io)
- Hypophosphatemia in the strict sense of the term refers to subnormal phosphorus concentrations in blood. (tnwmovie.com)
- It has been stated that 38% of hyperadrenocortical dogs have hypophosphatemia, but actual serum phosphorus concentrations were not reported. (tnwmovie.com)
- In practice, however, it is common to consider hypophosphatemia as a synonym for phosphorus deficiency, which is incorrect and potentially misleading, because blood phosphate concentration is a poor surrogate marker for the phosphorous level in the body. (tnwmovie.com)
Severe1
- The phenotypic spectrum of X-linked hypophosphatemia (XLH) ranges from isolated hypophosphatemia to severe lower-extremity bowing. (nih.gov)
Renal phosphate1
- Familial hypophosphatemic rickets (HR) is a rare inherited disorder characterized by renal phosphate wasting and inappropriately low levels of calcitriol causing hypophosphatemia and abnormal bone mineralization, first described by Albright [ 1 ]. (hindawi.com)
Hyperphosphaturia1
- X-linked hypophosphataemia is a rare condition that causes low phosphate levels in the blood (hypophosphataemia), associated high phosphate excretion in the urine (hyperphosphaturia), and symptoms of rickets such as bowed or knock-kneed legs. (contact.org.uk)
Disorder1
- [ 1 ] X-linked hypophosphatemia (XLH) is a dominant disorder and accounts for more than 80% of all familial hypophosphatemia. (medscape.com)
Diagnosis5
- At the age of 22 the patient was osteotomized in both tibiae and a diagnosis of familial hypophosphatemic rickets was suspected. (hindawi.com)
- Consensus Recommendations for the Diagnosis and Management of X-Linked Hypophosphatemia in Belgium. (nih.gov)
- Clinical practice recommendations for the diagnosis and management of X-linked hypophosphataemia. (nih.gov)
- Familial occurrence of this condition led to the diagnosis of familial hypophosphatemic rickets. (medscape.com)
- 12] Haffner D,Emma F,Eastwood DM,et al.Clinical practice recommendations for the diagnosis and management of X-linked hypophosphataemia[J].Nat Rev Nephrol,2019,15(7):435-455. (magtech.com.cn)
Concentrations1
- FHH type 3 exhibits mild hypophosphatemia and elevated plasma PTH concentrations. (orpha.net)
Short stature1
- An outstanding feature of familial hypophosphatemic rickets is short stature. (medscape.com)
Dominant1
- The prevailing form of HR is X-linked dominant hypophosphatemia (XLH) caused by an inactivating mutation of the PHEX gene [ 5 ]. (hindawi.com)
Disorders1
- These disorders may lead to either hyper- or hypophosphatemia, which can be caused by cellular shifts of phosphate. (ncats.io)
Chronic1
- Hypophosphatemia can be acute or chronic. (tnwmovie.com)
20171
- X-linked hypophosphatemia and growth[J]. Rev Endocr Metab Disord,2017,18(1):107-115. (magtech.com.cn)
Diseases1
- 6] Kinoshita Y,Fukumoto S. X-linked hypophosphatemia and FGF23-related hypophosphatemic diseases:prospect for new treatment[J]. Endocr Rev,2018,39(3):274-291. (magtech.com.cn)
Cellular1
- Causes of hypophosphatemia are shown in Table 1.Hypophosphatemia can occur when there are increased losses, decreased intake, or cellular shifts of phosphate. (tnwmovie.com)
Blood1
- Hypophosphatemia is a low level of phosphate in your blood. (tnwmovie.com)
Primary1
- The primary forms of osteoporosis in childhood are relatively rare, and some of them are familial or genetically determined (Table 1 ). (biomedcentral.com)
Levels2
- hypophosphatemia would normally cause elevated 1,25-dihydroxyvitamin D3 levels. (msdmanuals.com)
- Defective phosphate transport and hypophosphatemia in this case result in appropriately increased 1,25-dihydroxyvitamin D3 levels, thus leading to hypercalciuria. (msdmanuals.com)
Dietary1
- Patients with hypophosphatemia can be treated with dietary phosphate supplements (potassium phosphate, for example). (ncats.io)
Patients1
- Patients with non-synonymous allelic variants had an earlier onset of gout (42 vs 48 years, P = 0.0143) and a greater likelihood of a familial history of gout (41% vs 27%, odds ratio = 1.96, P = 0.053). (symptoma.com)