Immunoblastic Lymphadenopathy
Lymphoma, Large-Cell, Immunoblastic
Lymphoma, Non-Hodgkin
Lymphoma, AIDS-Related
Lymph Nodes
Lymphoma, Large B-Cell, Diffuse
Tuberculosis, Lymph Node
Lymphoma, B-Cell
Prednisone
Herpesvirus 4, Human
Histiocytosis, Sinus
Primary Sjogren's syndrome and its lymphoid malignancy: a report of four cases. (1/100)
OBJECTIVE: To evaluate the incidence and spectrum of malignancy of primary Sjogren's syndrome (pSS). METHODS: 250 pSS who were followed-up in Peking Union Medical College (PUMC) Hospital were analyzed. RESULTS: Four of them were diagnosed with histopathological findings of 2 non-Hodgkin Lymphoma, 1 AILD, 1 multiple myeloma. Two died of secondary infection while receiving chemotherapy for lymphoma, 2 remained remitted. CONCLUSIONS: The risk factors were persistent enlargement of major salivary glands, appearance of monoclonal serum lg, and disappearance of auto antibodies. (+info)Frequent T and B cell oligoclones in histologically and immunophenotypically characterized angioimmunoblastic lymphadenopathy. (2/100)
The identification of clonal rearrangements of T cell receptor (TCR) genes is central to the diagnosis of T cell lymphomas. However, in angioimmunoblastic lymphadenopathy (AILD), first described as a nonneoplastic proliferation associated with immunodeficiency, the heterogeneity of TCR and IgH gene rearrangements suggest that some cases may harbor multiple lymphoid clones. In this study we have isolated DNA from archival paraffin biopsy material from 22 cases of AILD identified on the basis of classical histological and immunohistochemical features with the aim of establishing the occurrence of clones and oligoclones, the frequency of TCR and immunoglobulin heavy chain (IgH) variable (v) gene use, and the relationship of these findings to the presence of Epstein-Barr virus. DNA extracted from the biopsies was amplified using the polymerase chain reaction (PCR) and sequenced to detect functional and nonfunctional gene rearrangements. Epstein-Barr virus-encoded short RNA species (EBERs) were detected using in situ hybridization combined with immunochemistry to identify the phenotype of the Epstein-Barr virus-infected cells. Fifty-seven clonal products were found in 20/22 patients: TCRgamma clonal products were identified in 16/22, TCRbeta clonal products in 16/22 and IgH clonal products in 6/22 cases. Oligoclonal PCR products were seen for TCR in 3/22 and for IgH in 3/22 cases. In one biopsy PCR products from all reactions were polyclonal. Sequence analysis revealed functional TCRgamma, TCRbeta, and IgH sequences in 6/12, 9/11, and 8/8 cases, respectively. Functional TCR and/or IgH oligoclones were detected in 6/20 (30%) cases. In addition, nonfunctional TCR and IgH sequences were found in 11 cases. EBERs were identified in 18/20 cases varying from occasional to 25 to 30% nuclei staining and were associated with both T and B cells, although the majority were of indeterminate phenotype. The presence of EBERs was not associated with all clonal IgH gene rearrangements but was associated with B cell oligoclones. Patterns of gene recombinations indicated that the majority of TCRgamma recombinations used GV1 and GJ1S3/2S3 genes. Six out of eleven cases used TCR BV4S1 or BV2S1 genes associated with various BJ and BD1/2 genes. No common IgH gene usage was identified, but 8 clones had varying degrees of replacement and silent mutations (0.6-10.1%), consistent with B cell clones having undergone somatic mutation in the germinal center, and 3 clones harbored unmutated V genes, consistent with naive B cells. Our data do not support the concept of AILD as a clearly defined peripheral T cell lymphoma (PTCL). Rather, they suggest that AILD as defined by histology and immunohistochemistry is either a heterogeneous entity or represents a lymphoproliferation associated with immunodeficiency in which clonal T cell or B cell proliferation may occur. (+info)Intravenous cyclosporine and tacrolimus caused anaphylaxis but oral cyclosporine capsules were tolerated in an allogeneic bone marrow transplant recipient. (3/100)
A Japanese female patient with angioimmunoblastic T cell lymphoma underwent allogeneic bone marrow transplantation (BMT) from her brother. Cyclosporine at a dose of 3 mg/kg was started by continuous infusion over 24 h on day -1 of BMT. Within a couple of minutes after the infusion was begun, she developed diffuse pruritic erythema on her whole body and tachycardia. The infusion was immediately stopped and corticosteroid was given, resulting in disappearance of the erythema gradually. She was then switched to intravenous tacrolimus. However, she suffered urticalial erythema again. Since polyoxyethylated castor oil, a solubilizer used in the injective formulation of both cyclosporine and tacrolimus, is considered to be responsible for the reaction, she was given oral capsules of cyclosporine (Sandimmun) in which polyoxyethylated castor oil was not contained. No further anaphylactic reaction was observed. The BM cells were successfully engrafted without causing severe GVHD. She was discharged on cyclosporine capsules without any further adverse effects. Anaphylaxis to intravenous cyclosporine and tacrolimus is a very rare but a serious complication. Our present case indicates that oral capsule of Sandimmun is a safe alternative to prevent GVHD in such a case of anaphylactic reaction against intravenous formulation. (+info)Survival and clonal expansion of mutating "forbidden" (immunoglobulin receptor-deficient) epstein-barr virus-infected b cells in angioimmunoblastic t cell lymphoma. (4/100)
Angioimmunoblastic lymphadenopathy with dysproteinemia (AILD) is a peculiar T cell lymphoma, as expanding B cell clones are often present besides the malignant T cell clones. In addition, large numbers of Epstein-Barr virus (EBV)-infected B cells are frequently observed. To analyze the differentiation status and clonal composition of EBV-harboring B cells in AILD, single EBV-infected cells were micromanipulated from lymph nodes of six patients with frequent EBV(+) cells and their rearranged immunoglobulin (Ig) genes analyzed. Most EBV-infected B cells carried mutated Ig genes, indicating that in AILD, EBV preferentially resides in memory and/or germinal center B cells. EBV(+) B cell clones observed in all six cases ranged from small polyclonal to large monoclonal expansions and often showed ongoing somatic hypermutation while EBV(-) B cells showed little tendency for clonal expansion. Surprisingly, many members of expanding B cell clones had acquired destructive mutations in originally functional V gene rearrangements and showed an unfavorable high load of replacement mutations in the framework regions, indicating that they accumulated mutations over repeated rounds of mutation and division while not being selected through their antigen receptor. This sustained selection-free accumulation of somatic mutations is unique to AILD. Moreover, the survival and clonal expansion of "forbidden" (i.e., Ig-deficient) B cells has not been observed before in vivo and thus represents a novel type of viral latency in the B cell compartment. It is likely the interplay between the microenvironment in AILD lymph nodes and the viral transformation that leads to the survival and clonal expansion of Ig-less B cells. (+info)Neoplastic T cells in angioimmunoblastic T-cell lymphoma express CD10. (5/100)
Angioimmunoblastic T-cell lymphoma (AITL) is a systemic disease involving lymph nodes, spleen, and bone marrow. Although the histologic features have been well described, the diagnosis is often challenging, as there are no specific phenotypic or molecular markers available. This study shows that the neoplastic cells of AITL can be identified by aberrant CD10 expression. Archival material from 30 cases of AITL, 10 cases of peripheral T-cell lymphoma unspecified (PTL), and 10 cases of reactive lymphoid hyperplasia were reviewed. Single and double immunostaining for CD3, CD4, CD8, CD20, CD21, CD10, BCL6, Ki67, and LMP-1 in situ hybridization for Epstein-Barr early region and polymerase chain reaction (PCR) for T-cell receptor gamma chain gene and immunoglobulin heavy chain gene were performed. Three overlapping histologic patterns with hyperplastic follicles, depleted follicles, or without follicles were identified in AITL. Of the 30 cases of AITL, 27 contained CD10(+) T cells. No CD10(+) T cells were present in the cases of PTL or reactive hyperplasia. PCR confirmed a monoclonal or oligoclonal T-cell population in 29 of 30 cases of AITL and a monoclonal B-cell population in 6 cases. Analysis of microdissected CD10(+) single cells showed that they belonged to the neoplastic clone. In conclusion CD10 is a phenotypic marker that specifically identifies the tumor cells in 90% of AITL, including the early cases. The presence of these cells distinguishes AITL from other PTLs. This finding provides an objective criterion for accurate and early diagnosis of AITL. (+info)Cytologic findings of angioimmunoblastic T-cell lymphoma: analysis of 16 fine-needle aspirates over 9-year period. (6/100)
BACKGROUND: Peripheral T-cell lymphoma often represents an important diagnostic pitfall in fine-needle aspiration biopsy due to the heterogeneous cell population present. A classic example of this group is angioimmunoblastic T-cell lymphoma (AILD-T). The fine-needle aspiration cytology of this relatively well-defined histologic subtype of T-cell lymphoma is rarely described in the literature. METHODS: The authors reviewed 16 fine-needle aspirates of AILD-T from 9 patients in Queen Mary Hospital and Pamela Youde Nethersole Eastern Hospital, Hong Kong, over a 9-year period from early 1993 to mid-2001. The morphologic features seen in cytology smears and/or cell block sections were correlated with histologic and immunohistochemical findings of excisional biopsy specimens. RESULTS: The smears and cytospin preparations showed a heterogeneous population of hematolymphoid cells, including small lymphocytes; nondescript, medium-sized lymphoid cells; immunoblasts; plasma cells; eosinophils; and reticulum cells, including follicular dendritic cells. In general, tingible body macrophages were not identified. Conversely, follicular dendritic cells were discernible easily in most cases and sometimes were admixed intimately with lymphoid cells, forming dendritic cell-lymphocyte complexes. There also were large lymphoid tissue fragments containing a scaffold of arborizing small vessels. Pleomorphic cells with high mitotic activity or lymphoid cells with clear cytoplasm were not identified. The cell block sections often showed an intimate admixture of small lymphocytes, plasma cells, eosinophils, and reticulum cells amid a background of reticulin fibers. Lymphoid follicles with well-developed germinal centers were never found. The features seen in cytologic preparations were reminiscent of those seen in histologic sections of the corresponding lymph node excisional biopsies. CONCLUSIONS: though ancillary investigative methods, including flow cytometry and molecular study, are of limited value in fine-needle aspiration cytology assessment of AILD-T due to the heterogeneous cell population present, recognition of the peculiar combination of cytologic features, especially in the right clinical setting, should provide a clue about the diagnosis. A high index of suspicion is essential to avoid a false negative diagnosis of reactive lymphadenopathy. (+info)Acute myocardial ischemia after high-dose therapy with BEAM regimen. (7/100)
We describe a case of acute myocardial ischemia following carmustine treatment during the BEAM regimen. Despite this, full completion of the autologous peripheral stem-cell transplant was possible. (+info)Successful treatment of post-transplant lymphoproliferative disorder in autologous blood stem cell transplant recipients. (8/100)
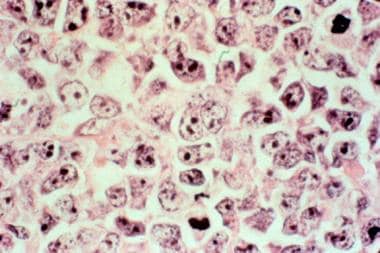
We report three cases of post-transplant lymphoproliferative disorder (PTLD) in the context of autologous stem cell transplantation (ASCT) for multiple myeloma (MM) and non-Hodgkin's lymphoma. The first two cases received ASCT for MM, one with a CD34-selected autograft and the other with an unmanipulated autograft. Both these cases of PTLD achieved a complete response following treatment with IVIG, gancyclovir, solumedrol and interferon (IFN). The third case received ASCT with an unmanipulated autograft for relapsed angioimmunoblastic lymphoma. He also achieved a complete response but only after rituximab was added to IVIG, gancyclovir, solumedrol and IFN. None of these patients experienced a relapse of their PTLD with follow-up ranging from 1.5 to 5 years. These cases highlight the importance of considering PTLD in the differential diagnosis of lymphadenopathy and fever post ASCT. They also demonstrate the possibility of durable complete remission of post-ASCT PTLD following antiviral and immune modulating therapy. (+info)Immunoblastic lymphadenopathy is a histopathological term used to describe the enlargement (or "adenopathy") of lymph nodes due to an abnormal proliferation or accumulation of immunoblasts, which are large, activated B cells. This condition can be seen in various reactive and neoplastic disorders, including certain infections, autoimmune diseases, and lymphomas.
In the context of lymphoma, immunoblastic lymphadenopathy is often associated with diffuse large B-cell lymphoma (DLBCL), a type of aggressive lymphoma characterized by the proliferation of malignant immunoblasts. The presence of immunoblastic lymphadenopathy in this setting suggests an advanced or more aggressive disease course, and it may warrant specific diagnostic workup and treatment approaches.
It is important to note that a definitive diagnosis of immunoblastic lymphadenopathy requires histological examination of tissue samples by a pathologist, who will assess the cellular morphology, immunophenotype, and genetic features of the cells involved.
Lymphatic diseases refer to a group of conditions that affect the lymphatic system, which is an important part of the immune and circulatory systems. The lymphatic system consists of a network of vessels, organs, and tissues that help to transport lymph fluid throughout the body, fight infection, and remove waste products.
Lymphatic diseases can be caused by various factors, including genetics, infections, cancer, and autoimmune disorders. Some common types of lymphatic diseases include:
1. Lymphedema: A condition that causes swelling in the arms or legs due to a blockage or damage in the lymphatic vessels.
2. Lymphoma: A type of cancer that affects the lymphatic system, including Hodgkin's and non-Hodgkin's lymphoma.
3. Infections: Certain bacterial and viral infections can affect the lymphatic system, such as tuberculosis, cat-scratch disease, and HIV/AIDS.
4. Autoimmune disorders: Conditions such as rheumatoid arthritis, lupus, and scleroderma can cause inflammation and damage to the lymphatic system.
5. Congenital abnormalities: Some people are born with abnormalities in their lymphatic system, such as malformations or missing lymph nodes.
Symptoms of lymphatic diseases may vary depending on the specific condition and its severity. Treatment options may include medication, physical therapy, surgery, or radiation therapy. It is important to seek medical attention if you experience symptoms of a lymphatic disease, as early diagnosis and treatment can improve outcomes.
Large B-cell lymphoma, immunoblastic variant, is a type of cancer that starts in the white blood cells called lymphocytes, which are part of the body's immune system. It is a subtype of diffuse large B-cell lymphoma (DLBCL), which is an aggressive (fast-growing) lymphoma.
Immunoblastic large B-cell lymphoma is characterized by the presence of large, immunoblastic cells that have a specific appearance under the microscope. These cells are typically found in the lymph nodes or other lymphoid tissues, such as the spleen or bone marrow.
This type of lymphoma can be aggressive and may require prompt treatment with chemotherapy, radiation therapy, or stem cell transplantation. The prognosis for immunoblastic large B-cell lymphoma varies depending on several factors, including the stage of the disease at diagnosis, the patient's age and overall health, and the specific features of the tumor.
It is important to note that a medical definition may vary based on different medical sources or guidelines, and it is always best to consult with a healthcare professional for accurate information.
Lymphoma is a type of cancer that originates from the white blood cells called lymphocytes, which are part of the immune system. These cells are found in various parts of the body such as the lymph nodes, spleen, bone marrow, and other organs. Lymphoma can be classified into two main types: Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL).
HL is characterized by the presence of a specific type of abnormal lymphocyte called Reed-Sternberg cells, while NHL includes a diverse group of lymphomas that lack these cells. The symptoms of lymphoma may include swollen lymph nodes, fever, night sweats, weight loss, and fatigue.
The exact cause of lymphoma is not known, but it is believed to result from genetic mutations in the lymphocytes that lead to uncontrolled cell growth and division. Exposure to certain viruses, chemicals, and radiation may increase the risk of developing lymphoma. Treatment options for lymphoma depend on various factors such as the type and stage of the disease, age, and overall health of the patient. Common treatments include chemotherapy, radiation therapy, immunotherapy, and stem cell transplantation.
Non-Hodgkin lymphoma (NHL) is a type of cancer that originates in the lymphatic system, which is part of the immune system. It involves the abnormal growth and proliferation of malignant lymphocytes (a type of white blood cell), leading to the formation of tumors in lymph nodes, spleen, bone marrow, or other organs. NHL can be further classified into various subtypes based on the specific type of lymphocyte involved and its characteristics.
The symptoms of Non-Hodgkin lymphoma may include:
* Painless swelling of lymph nodes in the neck, armpits, or groin
* Persistent fatigue
* Unexplained weight loss
* Fever
* Night sweats
* Itchy skin
The exact cause of Non-Hodgkin lymphoma is not well understood, but it has been associated with certain risk factors such as age (most common in people over 60), exposure to certain chemicals, immune system deficiencies, and infection with viruses like Epstein-Barr virus or HIV.
Treatment for Non-Hodgkin lymphoma depends on the stage and subtype of the disease, as well as the patient's overall health. Treatment options may include chemotherapy, radiation therapy, immunotherapy, targeted therapy, stem cell transplantation, or a combination of these approaches. Regular follow-up care is essential to monitor the progression of the disease and manage any potential long-term side effects of treatment.
AIDS-related lymphoma (ARL) is a type of cancer that affects the lymphatic system and is associated with acquired immunodeficiency syndrome (AIDS). It is caused by the infection of the lymphocytes, a type of white blood cell, with the human immunodeficiency virus (HIV), which weakens the immune system and makes individuals more susceptible to developing lymphoma.
There are two main types of AIDS-related lymphomas: diffuse large B-cell lymphoma (DLBCL) and Burkitt lymphoma (BL). DLBCL is the most common type and tends to grow rapidly, while BL is a more aggressive form that can also spread quickly.
Symptoms of AIDS-related lymphoma may include swollen lymph nodes, fever, night sweats, fatigue, weight loss, and decreased appetite. Diagnosis typically involves a biopsy of the affected lymph node or other tissue, followed by various imaging tests to determine the extent of the disease.
Treatment for AIDS-related lymphoma usually involves a combination of chemotherapy, radiation therapy, and/or immunotherapy, along with antiretroviral therapy (ART) to manage HIV infection. The prognosis for ARL varies depending on several factors, including the type and stage of the disease, the patient's overall health, and their response to treatment.
Lymph nodes are small, bean-shaped organs that are part of the immune system. They are found throughout the body, especially in the neck, armpits, groin, and abdomen. Lymph nodes filter lymph fluid, which carries waste and unwanted substances such as bacteria, viruses, and cancer cells. They contain white blood cells called lymphocytes that help fight infections and diseases by attacking and destroying the harmful substances found in the lymph fluid. When an infection or disease is present, lymph nodes may swell due to the increased number of immune cells and fluid accumulation as they work to fight off the invaders.
Large B-cell lymphoma, diffuse is a type of cancer that starts in cells called B-lymphocytes, which are part of the body's immune system. "Large B-cell" refers to the size and appearance of the abnormal cells when viewed under a microscope. "Diffuse" means that the abnormal cells are spread throughout the lymph node or tissue where the cancer has started, rather than being clustered in one area.
This type of lymphoma is typically aggressive, which means it grows and spreads quickly. It can occur almost anywhere in the body, but most commonly affects the lymph nodes, spleen, and bone marrow. Symptoms may include swollen lymph nodes, fever, night sweats, weight loss, and fatigue.
Treatment for large B-cell lymphoma, diffuse typically involves chemotherapy, radiation therapy, or a combination of both. In some cases, stem cell transplantation or targeted therapy may also be recommended. The prognosis varies depending on several factors, including the stage and location of the cancer, as well as the patient's age and overall health.
Tuberculosis (TB) of the lymph node, also known as scrofula or tuberculous lymphadenitis, is a specific form of extrapulmonary tuberculosis. It involves the infection and inflammation of the lymph nodes (lymph glands) by the Mycobacterium tuberculosis bacterium. The lymph nodes most commonly affected are the cervical (neck) and supraclavicular (above the collarbone) lymph nodes, but other sites can also be involved.
The infection typically spreads to the lymph nodes through the bloodstream or via nearby infected organs, such as the lungs or intestines. The affected lymph nodes may become enlarged, firm, and tender, forming masses called cold abscesses that can suppurate (form pus) and eventually rupture. In some cases, the lymph nodes may calcify, leaving hard, stone-like deposits.
Diagnosis of tuberculous lymphadenitis often involves a combination of clinical evaluation, imaging studies (such as CT or MRI scans), and microbiological or histopathological examination of tissue samples obtained through fine-needle aspiration biopsy or surgical excision. Treatment typically consists of a standard anti-tuberculosis multi-drug regimen, which may include isoniazid, rifampin, ethambutol, and pyrazinamide for at least six months. Surgical intervention might be necessary in cases with complications or treatment failure.
B-cell lymphoma is a type of cancer that originates from the B-lymphocytes, which are a part of the immune system and play a crucial role in fighting infections. These cells can develop mutations in their DNA, leading to uncontrolled growth and division, resulting in the formation of a tumor.
B-cell lymphomas can be classified into two main categories: Hodgkin's lymphoma and non-Hodgkin's lymphoma. B-cell lymphomas are further divided into subtypes based on their specific characteristics, such as the appearance of the cells under a microscope, the genetic changes present in the cancer cells, and the aggressiveness of the disease.
Some common types of B-cell lymphomas include diffuse large B-cell lymphoma, follicular lymphoma, mantle cell lymphoma, and Burkitt lymphoma. Treatment options for B-cell lymphomas depend on the specific subtype, stage of the disease, and other individual factors. Treatment may include chemotherapy, radiation therapy, immunotherapy, targeted therapy, or stem cell transplantation.
Mediastinal diseases refer to a group of conditions that affect the mediastinum, which is the area in the chest separating the lungs and containing various vital structures such as the heart, esophagus, trachea, thymus gland, lymph nodes, blood vessels, and nerves. These diseases can be benign or malignant (cancerous) and may cause symptoms due to compression or invasion of surrounding tissues. Examples of mediastinal diseases include:
1. Mediastinal tumors: Abnormal growths in the mediastinum, which can be benign or malignant. Common types include thymomas, germ cell tumors, lymphomas, and neurogenic tumors.
2. Mediastinitis: Inflammation of the mediastinal tissues, often caused by infections, trauma, or complications from medical procedures.
3. Enlarged lymph nodes: Abnormal swelling of the lymph nodes in the mediastinum can be a sign of various conditions, including infections, cancer, and autoimmune disorders.
4. Mediastinal cysts: Fluid-filled sacs that develop in the mediastinum, which are usually benign but may cause symptoms due to compression or infection.
5. Aneurysms or dissections of the aorta: Abnormal weakening or tearing of the aortic wall within the mediastinum, which can lead to life-threatening complications if not treated promptly.
6. Esophageal diseases: Conditions affecting the esophagus, such as tumors, strictures, or motility disorders, may present with symptoms related to the mediastinum.
7. Thyroid disorders: Enlargement of the thyroid gland (goiter) can extend into the mediastinum and cause compression symptoms.
8. Hematomas or effusions: Accumulation of blood (hematoma) or fluid (effusion) in the mediastinal space due to trauma, surgery, or other underlying conditions.
Early diagnosis and appropriate treatment are crucial for managing mediastinal diseases and improving patient outcomes.
Prednisone is a synthetic glucocorticoid, which is a type of corticosteroid hormone. It is primarily used to reduce inflammation in various conditions such as asthma, allergies, arthritis, and autoimmune disorders. Prednisone works by mimicking the effects of natural hormones produced by the adrenal glands, suppressing the immune system's response and reducing the release of substances that cause inflammation.
It is available in oral tablet form and is typically prescribed to be taken at specific times during the day, depending on the condition being treated. Common side effects of prednisone include increased appetite, weight gain, mood changes, insomnia, and easy bruising. Long-term use or high doses can lead to more serious side effects such as osteoporosis, diabetes, cataracts, and increased susceptibility to infections.
Healthcare providers closely monitor patients taking prednisone for extended periods to minimize the risk of adverse effects. It is essential to follow the prescribed dosage regimen and not discontinue the medication abruptly without medical supervision, as this can lead to withdrawal symptoms or a rebound of the underlying condition.
Vincristine is an antineoplastic agent, specifically a vinca alkaloid. It is derived from the Madagascar periwinkle plant (Catharanthus roseus). Vincristine binds to tubulin, a protein found in microtubules, and inhibits their polymerization, which results in disruption of mitotic spindles leading to cell cycle arrest and apoptosis (programmed cell death). It is used in the treatment of various types of cancer including leukemias, lymphomas, and solid tumors. Common side effects include peripheral neuropathy, constipation, and alopecia.
Medical Definition of "Herpesvirus 4, Human" (Epstein-Barr Virus)
"Herpesvirus 4, Human," also known as Epstein-Barr virus (EBV), is a member of the Herpesviridae family and is one of the most common human viruses. It is primarily transmitted through saliva and is often referred to as the "kissing disease."
EBV is the causative agent of infectious mononucleosis (IM), also known as glandular fever, which is characterized by symptoms such as fatigue, sore throat, fever, and swollen lymph nodes. The virus can also cause other diseases, including certain types of cancer, such as Burkitt's lymphoma, Hodgkin's lymphoma, and nasopharyngeal carcinoma.
Once a person becomes infected with EBV, the virus remains in the body for the rest of their life, residing in certain white blood cells called B lymphocytes. In most people, the virus remains dormant and does not cause any further symptoms. However, in some individuals, the virus may reactivate, leading to recurrent or persistent symptoms.
EBV infection is diagnosed through various tests, including blood tests that detect antibodies against the virus or direct detection of the virus itself through polymerase chain reaction (PCR) assays. There is no cure for EBV infection, and treatment is generally supportive, focusing on relieving symptoms and managing complications. Prevention measures include practicing good hygiene, avoiding close contact with infected individuals, and not sharing personal items such as toothbrushes or drinking glasses.
Sinus histiocytosis is a rare condition characterized by an abnormal accumulation of histiocytes (a type of immune cell) in the sinuses. It is also known as Rosai-Dorfman disease when it occurs as a systemic disorder. In sinus histiocytosis, the histiocytes accumulate in the mucous membranes lining the sinuses, leading to their enlargement and possible obstruction. Symptoms may include nasal congestion, drainage, and pain. The exact cause of sinus histiocytosis is unknown, but it is not contagious or cancerous. Treatment typically involves monitoring and, in some cases, surgery to relieve symptoms caused by blockages.
Lymphadenitis is a medical term that refers to the inflammation of one or more lymph nodes, which are small, bean-shaped glands that are part of the body's immune system. Lymph nodes contain white blood cells called lymphocytes, which help fight infection and disease.
Lymphadenitis can occur as a result of an infection in the area near the affected lymph node or as a result of a systemic infection that has spread through the bloodstream. The inflammation causes the lymph node to become swollen, tender, and sometimes painful to the touch.
The symptoms of lymphadenitis may include fever, fatigue, and redness or warmth in the area around the affected lymph node. In some cases, the overlying skin may also appear red and inflamed. Lymphadenitis can occur in any part of the body where there are lymph nodes, including the neck, armpits, groin, and abdomen.
The underlying cause of lymphadenitis must be diagnosed and treated promptly to prevent complications such as the spread of infection or the formation of an abscess. Treatment may include antibiotics, pain relievers, and warm compresses to help reduce swelling and discomfort.
Histiocytic Necrotizing Lymphadenitis is a condition characterized by the inflammation and necrosis (death of tissue) of lymph nodes, caused by an abnormal proliferation and activation of histiocytes (a type of white blood cell). It is also known as Kikuchi's disease. The exact cause of this condition is unknown, but it is thought to be related to an immune response to viral infections or other antigens.
Histopathologically, it is characterized by the presence of necrotizing granulomatous inflammation with histiocytic predominance and absence of neutrophils. The condition is typically self-limiting, with symptoms resolving within a few months without specific treatment. However, in some cases, it can be associated with systemic symptoms or other autoimmune disorders.