Inferior Wall Myocardial Infarction
Myocardial Infarction
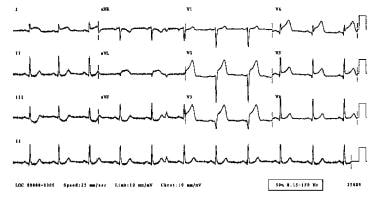
Electrocardiography
Anterior Wall Myocardial Infarction
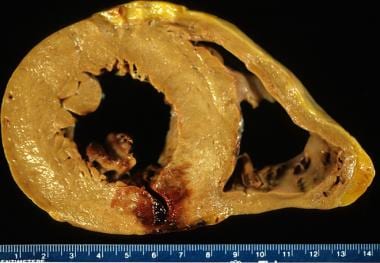
Heart Rupture, Post-Infarction
Coronary Angiography
Heart Ventricles
Ventricular Function, Left
Echocardiographic progression of a subepicardial aneurysm after inferior myocardial infarction. (1/26)
(+info)Predictors of inhospital outcome after acute inferior wall myocardial infarction. (2/26)
INTRODUCTION: Compared with anterior wall myocardial infarction, inferior wall myocardial infarction is generally regarded as being low risk. The aim of this study was to elucidate the clinical factors affecting its inhospital outcome. METHODS: From January 1997 to March 2006, 546 consecutive patients who suffered from their first inferior wall myocardial infarction were recruited for the study. The demographic, clinical, electrocardiographical and angiographical characteristics, treatment and medications, complications and inhospital deaths were subjected to univariate analysis. The factors that had a p-value of less than 0.1 were included for multivariate logistic regression analysis. A p-value of less than 0.05 was considered significant. The impact of thrombolysis on clinical outcome in various high-risk patient subsets was also examined. RESULTS: An advanced age of more than 74 years, female gender, lateral wall extension, complete atrioventricular block, bundle branch block, and cardiac free-wall rupture were found to be independent predictors of inhospital mortality, whereas the use of thrombolysis was associated with a favourable outcome. On the other hand, right ventricular infarction and precordial ST-segment depression are not predictive of poor outcome. In addition, thrombolysis reduced inhospital mortality in patients with an age above 64 years, male gender, lateral wall extension, haemodynamically-significant right ventricular infarction and complete atrioventricular block. CONCLUSION: In inferior wall myocardial infarction, independent predictors of poor inhospital outcome are advanced age, female gender, lateral wall extension, complete atrioventricular block, bundle branch block and cardiac free-wall rupture. The use of thrombolysis is generally beneficial, especially in those of the high-risk subsets. (+info)Posterior wall involvement attenuates predictive value of ST-segment elevation in lead V4R for right ventricular involvement in inferior acute myocardial infarction. (3/26)
(+info)Clinical and angiographic findings of complete atrioventricular block in acute inferior myocardial infarction. (4/26)
INTRODUCTION: The angiographic findings and prognosis of patients with complete atrioventricular block (AVB) complicating acute inferior myocardial infarction (MI) remain unclear. MATERIALS AND METHODS: The clinical and angiographic findings of 70 consecutive patients with complete AVB were compared with those of 319 patients with inferior MI without AVB (control group) admitted within the same study period. RESULTS: Patients with complete AVB were older (68 +/- 12 vs 63 +/- 13 years; P = 0.004) and clustered with clinical features indicative of larger infarct size, such as right ventricular infarction, cardiogenic shock, or low left ventricular ejection fraction (LVEF). The onset of the complete AVB was observed within 24 hours in 62 (88.6%), preceded by second-degree AVB in 26 (37.1%) and the escape QRS complex was wide in 8 (11.4%) patients. In patients with complete AVB, a dominant right coronary artery occlusion was found in >95% of cases and in-hospital mortality was increased (27.1% vs 10.7%; P = 0.000), especially in those with widen QRS escape rhythm (75.0%). Reperfusion therapy had a positive impact on the natural course of complete AVB. CONCLUSIONS: Complete AVB in acute inferior MI was associated with advanced age and larger infarct size. Complete AVB was virtually always caused by dominant right coronary artery occlusion. The in-hospital mortality was significantly higher, but improved by reperfusion therapy. No permanent pacemaker is performed at a mean follow-up of 47 months. (+info)Right ventricular infarction and tissue Doppler imaging - insights from acute inferior myocardial infarction after primary coronary intervention -. (5/26)
BACKGROUND: Tissue Doppler imaging (TDI) data for acute inferior myocardial infarction (MI) patients who have received primary percutaneous coronary intervention (PCI) are sparse. METHODS AND RESULTS: One hundred and sixty-five patients received primary PCI for acute inferior MI were enrolled. Right ventricular infarction (RVI) was defined as a culprit lesion proximal to the right ventricular branch of right coronary artery (RCA). Echocardiograms and TDI were obtained within 6 h after primary PCI. The prevalence of multi-vessel disease in the RCA-P culprit group (50%) was higher than that in other groups (39% of RCA-D culprit, 43% of left circumflex artery (LCX) culprit). The myocardial performance index (MPI) of the lateral tricuspid annulus provides discriminatory power for identifying RVI, whereas systolic velocity (Sm) of the lateral tricuspid annulus does not. Lateral mitral annular MPI divided by the lateral tricuspid annular MPI is a reliable index for identifying a culprit lesion (>1.06 predicts culprit over LCX; <0.96 predicts culprit over RCA-P and RVI). Kaplan-Meier survival curves revealed that late cardiovascular events were more likely in RVI patients. However, multivariate Cox proportional hazards analysis revealed that the most important factor in hard events and all cardiovascular events was multivessel disease. CONCLUSIONS: TDI is useful for identifying RVI and culprit lesions in inferior MI patients received primary PCI. RVI itself isn't associated with 1-year hard events and all cardiovascular events. (+info)Optimal positioning in the detection of inferior wall infarct size with myocardial perfusion scintigraphy: prone vs. supine. (6/26)
(+info)Post-infarction ventricular septal defect: triggered by Valsalva manoeuvre? (7/26)
(+info)Diffuse precordial ST-segment elevation in inferior-right myocardial infarction. (8/26)
A right ventricular (RV) myocardial infarction (MI) may yield precordial ST-segment elevation (STE). Accordingly, combined inferior and precordial STE may be produced during an inferior-RV MI. Such an electrocardiographic picture may be mistakenly regarded as showing wrapped left anterior descending artery (LADA) occlusion or double vessel occlusion. We present a patient with inferior-RV MI and STE in the inferior, all precordial and right chest leads, in whom the diffuse precordial STE was probably mistakenly regarded as showing anterior MI. However, the STE resolution in V1-V2 and late R' wave in V1, which were combined with a recanalized RV branch, favored the RV origin of this STE. Furthermore, the LADA was patent when V3-V6 showed severe ischemia, while its lesion was angiographically stable. Thus its simultaneous occlusion was unlikely. The late R' wave in V1 indicates RV transmural conduction delay;as highlighted herein, it is diagnostic of a RV myocardial infarction. (+info)An Inferior Wall Myocardial Infarction (MI) is a type of heart attack that occurs when there is a significant reduction or complete blockage of blood flow to the inferior (lower) region of the heart muscle, specifically the areas supplied by the right coronary artery or one of its branches. This reduction in blood flow, often caused by a blood clot forming around a ruptured plaque within the artery, can lead to ischemia and ultimately result in damage or death of the heart muscle cells (myocardial necrosis). Symptoms may include chest pain, shortness of breath, sweating, nausea, or vomiting. Diagnosis typically involves an electrocardiogram (ECG) and cardiac biomarker tests, such as troponin levels. Treatment includes medications, lifestyle changes, and possibly interventions like angioplasty or bypass surgery to restore blood flow.
Myocardial infarction (MI), also known as a heart attack, is a medical condition characterized by the death of a segment of heart muscle (myocardium) due to the interruption of its blood supply. This interruption is most commonly caused by the blockage of a coronary artery by a blood clot formed on the top of an atherosclerotic plaque, which is a buildup of cholesterol and other substances in the inner lining of the artery.
The lack of oxygen and nutrients supply to the heart muscle tissue results in damage or death of the cardiac cells, causing the affected area to become necrotic. The extent and severity of the MI depend on the size of the affected area, the duration of the occlusion, and the presence of collateral circulation.
Symptoms of a myocardial infarction may include chest pain or discomfort, shortness of breath, nausea, lightheadedness, and sweating. Immediate medical attention is necessary to restore blood flow to the affected area and prevent further damage to the heart muscle. Treatment options for MI include medications, such as thrombolytics, antiplatelet agents, and pain relievers, as well as procedures such as percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG).
Electrocardiography (ECG or EKG) is a medical procedure that records the electrical activity of the heart. It provides a graphic representation of the electrical changes that occur during each heartbeat. The resulting tracing, called an electrocardiogram, can reveal information about the heart's rate and rhythm, as well as any damage to its cells or abnormalities in its conduction system.
During an ECG, small electrodes are placed on the skin of the chest, arms, and legs. These electrodes detect the electrical signals produced by the heart and transmit them to a machine that amplifies and records them. The procedure is non-invasive, painless, and quick, usually taking only a few minutes.
ECGs are commonly used to diagnose and monitor various heart conditions, including arrhythmias, coronary artery disease, heart attacks, and electrolyte imbalances. They can also be used to evaluate the effectiveness of certain medications or treatments.
An anterior wall myocardial infarction (AMI) is a type of heart attack that occurs when there is a significant reduction or complete blockage of blood flow to the front wall of the heart muscle, also known as the anterior wall of the left ventricle. This reduction or blockage in blood flow is typically caused by a buildup of fatty deposits, called plaques, in the coronary arteries that supply oxygen-rich blood to the heart muscle.
When a plaque ruptures or breaks open, a blood clot forms around it, which can completely block the flow of blood to the heart muscle. This lack of blood flow causes the heart muscle to start to die, leading to a myocardial infarction or heart attack.
An anterior wall myocardial infarction is often associated with more severe symptoms and a higher risk of complications than other types of heart attacks because it affects a larger area of the heart muscle. Symptoms may include chest pain, shortness of breath, nausea, vomiting, sweating, and anxiety.
Immediate medical attention is necessary for an anterior wall myocardial infarction to restore blood flow to the heart muscle as quickly as possible and prevent further damage. Treatment options may include medications, such as clot-busting drugs or blood thinners, as well as procedures such as angioplasty or coronary artery bypass surgery.
Post-infarction heart rupture is a serious and potentially fatal complication that can occur after a myocardial infarction (heart attack). It is defined as the disruption or tearing of the heart muscle (myocardium) in the area that was damaged by the heart attack. This condition typically occurs within 1 to 7 days following a heart attack, and it's more common in elderly patients and those with large infarctions.
There are three main types of post-infarction heart rupture:
1. Ventricular free wall rupture: This is the most common type, where there is a tear in the left ventricular wall, leading to rapid bleeding into the pericardial sac (the space surrounding the heart). This can cause cardiac tamponade, which is a life-threatening situation characterized by increased pressure in the pericardial sac, compromising cardiac filling and reducing cardiac output.
2. Ventricular septal rupture: In this case, there is a tear in the interventricular septum (the wall separating the left and right ventricles), leading to a communication between the two chambers. This results in a shunt of blood from the high-pressure left ventricle to the low-pressure right ventricle, causing a sudden increase in pulmonary congestion and reduced systemic output.
3. Papillary muscle rupture: The papillary muscles are finger-like projections that attach the heart valves (mitral and tricuspid) to the ventricular walls. Rupture of these muscles can lead to severe mitral or tricuspid regurgitation, causing acute pulmonary edema and reduced cardiac output.
Symptoms of post-infarction heart rupture may include chest pain, shortness of breath, palpitations, hypotension, tachycardia, and signs of cardiogenic shock (such as cold sweats, weak pulse, and altered mental status). Diagnosis is typically made using echocardiography, CT angiography, or MRI. Treatment usually involves emergency surgical intervention to repair the rupture and stabilize the patient's hemodynamic condition.
Coronary angiography is a medical procedure that uses X-ray imaging to visualize the coronary arteries, which supply blood to the heart muscle. During the procedure, a thin, flexible catheter is inserted into an artery in the arm or groin and threaded through the blood vessels to the heart. A contrast dye is then injected through the catheter, and X-ray images are taken as the dye flows through the coronary arteries. These images can help doctors diagnose and treat various heart conditions, such as blockages or narrowing of the arteries, that can lead to chest pain or heart attacks. It is also known as coronary arteriography or cardiac catheterization.
The heart ventricles are the two lower chambers of the heart that receive blood from the atria and pump it to the lungs or the rest of the body. The right ventricle pumps deoxygenated blood to the lungs, while the left ventricle pumps oxygenated blood to the rest of the body. Both ventricles have thick, muscular walls to generate the pressure necessary to pump blood through the circulatory system.
Left ventricular function refers to the ability of the left ventricle (the heart's lower-left chamber) to contract and relax, thereby filling with and ejecting blood. The left ventricle is responsible for pumping oxygenated blood to the rest of the body. Its function is evaluated by measuring several parameters, including:
1. Ejection fraction (EF): This is the percentage of blood that is pumped out of the left ventricle with each heartbeat. A normal ejection fraction ranges from 55% to 70%.
2. Stroke volume (SV): The amount of blood pumped by the left ventricle in one contraction. A typical SV is about 70 mL/beat.
3. Cardiac output (CO): The total volume of blood that the left ventricle pumps per minute, calculated as the product of stroke volume and heart rate. Normal CO ranges from 4 to 8 L/minute.
Assessment of left ventricular function is crucial in diagnosing and monitoring various cardiovascular conditions such as heart failure, coronary artery disease, valvular heart diseases, and cardiomyopathies.
Coronary vessels refer to the network of blood vessels that supply oxygenated blood and nutrients to the heart muscle, also known as the myocardium. The two main coronary arteries are the left main coronary artery and the right coronary artery.
The left main coronary artery branches off into the left anterior descending artery (LAD) and the left circumflex artery (LCx). The LAD supplies blood to the front of the heart, while the LCx supplies blood to the side and back of the heart.
The right coronary artery supplies blood to the right lower part of the heart, including the right atrium and ventricle, as well as the back of the heart.
Coronary vessel disease (CVD) occurs when these vessels become narrowed or blocked due to the buildup of plaque, leading to reduced blood flow to the heart muscle. This can result in chest pain, shortness of breath, or a heart attack.
Echocardiography is a medical procedure that uses sound waves to produce detailed images of the heart's structure, function, and motion. It is a non-invasive test that can help diagnose various heart conditions, such as valve problems, heart muscle damage, blood clots, and congenital heart defects.
During an echocardiogram, a transducer (a device that sends and receives sound waves) is placed on the chest or passed through the esophagus to obtain images of the heart. The sound waves produced by the transducer bounce off the heart structures and return to the transducer, which then converts them into electrical signals that are processed to create images of the heart.
There are several types of echocardiograms, including:
* Transthoracic echocardiography (TTE): This is the most common type of echocardiogram and involves placing the transducer on the chest.
* Transesophageal echocardiography (TEE): This type of echocardiogram involves passing a specialized transducer through the esophagus to obtain images of the heart from a closer proximity.
* Stress echocardiography: This type of echocardiogram is performed during exercise or medication-induced stress to assess how the heart functions under stress.
* Doppler echocardiography: This type of echocardiogram uses sound waves to measure blood flow and velocity in the heart and blood vessels.
Echocardiography is a valuable tool for diagnosing and managing various heart conditions, as it provides detailed information about the structure and function of the heart. It is generally safe, non-invasive, and painless, making it a popular choice for doctors and patients alike.
 Left anterior fascicular block
Left anterior fascicular block First-Degree Atrioventricular Block: Background, Pathophysiology, Etiology
First-Degree Atrioventricular Block: Background, Pathophysiology, Etiology Related Articles | Annals Singapore
Related Articles | Annals Singapore Variants of arterial supply to the inferior (diaphragmatic) surface of the ventricles of the heart and the influence on age at...
Variants of arterial supply to the inferior (diaphragmatic) surface of the ventricles of the heart and the influence on age at... NCA - Magnetic Resonance Imaging (MRI) (CAG-00399R) - Decision Memo
NCA - Magnetic Resonance Imaging (MRI) (CAG-00399R) - Decision Memo Duration of DAPT in a Patient With PAD and ACS - American College of Cardiology
Duration of DAPT in a Patient With PAD and ACS - American College of Cardiology Ventricular pseudoaneurysm secondary to myocardial infarction - an exuberant presentation | Eurorad
Ventricular pseudoaneurysm secondary to myocardial infarction - an exuberant presentation | Eurorad Effect of thrombolytic therapy on the evolution of significant mitral regurgitation in patients with a first inferior...
Effect of thrombolytic therapy on the evolution of significant mitral regurgitation in patients with a first inferior... Digestive System | PPT
Digestive System | PPT Left Axis Deviation
Left Axis Deviation Clinical, Angiographic Profile and Immediate Outcome of COVID-19 Patients Presenting as Acute Coronary Syndrome: An...
Clinical, Angiographic Profile and Immediate Outcome of COVID-19 Patients Presenting as Acute Coronary Syndrome: An...![Ischemic heart diseases in Yemen [Archives:2007/1102/Health] - Yemen Times archives](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAUCAYAAACEYr13AAAB8UlEQVQ4jaXRv2sTYRzH8ffnLjFRaYW00VwG7eYgSqFgc4iza6E4CdKCg4OKmxSkOIiTKHQRweIgTi7+A0KhQ0mhFARBcXHQ2uaSFFtj08Z7vg71Ss0PoXrTw+f5PK/vFw7+81MlCF8Jtkz2EwCTjzicX8lcFXPNpGicORQF/S+F7ZjYlpE2GPKOxO6GYe9lTAhNSuQy37m+/zGAeLeTd40JxDehSWArpdaVvUIUlJ5ExdCiIPxk4Hdb10CVYrgcBaUXSeYlh6xtT5tZA3EqKpTGuwH1wui4sJMZz93uAPpWlyPQzO/0roHapvvO8+5jNtX/ZbHWAQBkGjzEbEPobC0Ix/bfVYPwGsbm4Nfys/35H8CxjYU64hGAE9PJFtHghT7D7nlxfEvgegIAXtMeg9UFw1GhdBlA6fiO4M1AZXGhva/2AKAShFMSD4APKdOlltyS37ThgXr5c8fAbkDeNWbMrAqcbuHmBLPdHvcEtPa24cFTAElD7LjZbr2eAIDQPABmbrC6+PHAADGbACa1BHZwQC75XT0f/xWQLx9ARuqfABcruyuRMkbSBwbwbSQ5rhfT53tu2h5UiqWbQmNgF0HJ5HWweXP2+vhq+flet1Ca6QDsxLmjAKzltmEu3k1HUlG+mcmns04rSz+Sbi032v8LRDW76rOJY1IAAAAASUVORK5CYII=) Ischemic heart diseases in Yemen [Archives:2007/1102/Health] - Yemen Times archives
Ischemic heart diseases in Yemen [Archives:2007/1102/Health] - Yemen Times archives Echocardiographic Parameters as Predictors of In-Hospital Mortality in Patients with Acute Coronary Syndrome Undergoing...
Echocardiographic Parameters as Predictors of In-Hospital Mortality in Patients with Acute Coronary Syndrome Undergoing... EMERGENCY MEDICAL SERVICES-ECG April Issue - Emergency Medical Services Agency
EMERGENCY MEDICAL SERVICES-ECG April Issue - Emergency Medical Services Agency Search | Global Index Medicus
Search | Global Index Medicus March 05, 2021<...
March 05, 2021<...