Kartagener Syndrome
Ciliary Motility Disorders
Encyclopedias as Topic
Cystic Fibrosis
Inflammation
Cough
Lung Diseases, Obstructive
Nasal nitric oxide concentration in paranasal sinus inflammatory diseases. (1/143)
In normal upper airways, nitric oxide is generated by the paranasal sinus epithelium and then diffuses into the nasal cavities. This study examined whether or not nasal NO concentration is affected by paranasal sinus inflammatory diseases. The influence of obstruction (nasal polyposis) and/or inflammation (allergy or chronic sinusitis) of the paranasal sinuses on nasal NO concentration was evaluated in nasal allergic (n=7 patients) or nonallergic (n=20) polyposis, nonallergic chronic sinusitis (n=10) and Kartagener's syndrome (n=6) and compared with control subjects (n=42). A score of alteration of the paranasal sinus (number of altered and occluded sinuses) was determined by a computed tomography scan. The nasal NO concentration in nasal nonallergic polyposis (150+/-20 parts per billion (ppb)) was significantly decreased compared with both controls (223+/-6 ppb, p=0.01) and polyposis with allergy (272+/-28 ppb, p<0.0001). In each group, the nasal NO concentration was inversely correlated with the extent of tomodensitometric alteration of the paranasal sinuses. In Kartagener's syndrome, the nasal NO concentration (14+/-2 ppb) was drastically decreased compared with all other groups, despite the presence of open paranasal sinuses. Thus, the nasal NO concentration in patients with nasal polyposis appeared to be dependent on both the allergic status and the degree of obstruction of the paranasal sinuses. (+info)Failure of fertilization after intracytoplasmic sperm injection in a patient with Kartagener's syndrome and totally immotile spermatozoa: case report. (2/143)
Patients with Kartagener's syndrome (KS) are invariably infertile with totally immotile spermatozoa. Intracytoplasmic sperm injection (ICSI) is considered to be the treatment of choice for patients with immotile spermatozoa. We report the second KS case in the literature from whom immotile spermatozoa from the ejaculate failed to fertilize mature oocytes after ICSI. The role of micromanipulation in the treatment of KS patients is discussed. (+info)Successful in-vitro fertilization pregnancy with spermatozoa from a patient with Kartagener's syndrome: case report. (3/143)
This paper reports on the successful treatment by in-vitro fertilization (IVF) of a couple in whom the male partner had Kartagener's syndrome. His spermatozoa were severely asthenozoospermic with deficient dynein arms and disordered microtubular configuration. On computer-assisted sperm analysis (CASA) motile spermatozoa displayed straight non-progressive motility with minimal amplitude of lateral head displacement and none were hyperactivated. This is the first case report in which spermatozoa with axonemal disruption in a man with immotile cilia syndrome (ICS) have been shown to be able to penetrate the zona pellucida and fertilize oocytes. IVF may be a suitable treatment for certain variants of ICS. (+info)Bronchiolitis in Kartagener's syndrome. (4/143)
The association of diffuse bronchiolitis in patients with Kartagener's syndrome (KS) has not been reported previously. The aim of this study was to present the morphological characteristics of bronchiolitis in patients with KS. Eight patients (four males, four females; mean age 37.9+/-18.7 yrs), clinically diagnosed as KS with the classical triad of chronic pansinusitis, bronchiectasis and situs in versus with dextrocardia, were evaluated. Routine chest radiography showed bronchiectasis and dextrocardia in all patients. Chest computed tomography (CT) showed diffuse centrilobular small nodules up to 2 mm in diameter throughout both lungs in six out of eight patients. Pulmonary function tests revealed marked obstructive impairment in all patients (forced expiratory volume in one second 57.0+/-11.3%, residual volume/total lung capacity 45.+/-12.7%, maximum midexpiratory flow 0.92+/-0.72 L x s(-1), forced vital capacity 74.1+/-12.2% (all mean +/- SD)). The examination of cilial movement of the bronchus revealed immotility in all of the five patients examined. The ultrastructure showed ciliary dynein arm defects in all patients. Histopathological examination of lung specimens obtained at autopsy or by video-assisted thoracoscopic surgery showed obliterative thickening of the walls of the membranous bronchioli with infiltration of lymphocytes, plasma cells and neutrophils, but most of the distal respiratory bronchioli were spared and alveolar spaces were overinflated. Pathologically, the diffuse centrilobular small nodules on the chest CT mainly corresponded to membranous bronchiolitis. This is the first report demonstrating that the association of diffuse bronchiolitis might be one of the characteristic features of the lung in Kartagener's syndrome. (+info)Axonemal dynein intermediate-chain gene (DNAI1) mutations result in situs inversus and primary ciliary dyskinesia (Kartagener syndrome). (5/143)
Kartagener syndrome (KS) is a trilogy of symptoms (nasal polyps, bronchiectasis, and situs inversus totalis) that is associated with ultrastructural anomalies of cilia of epithelial cells covering the upper and lower respiratory tracts and spermatozoa flagellae. The axonemal dynein intermediate-chain gene 1 (DNAI1), which has been demonstrated to be responsible for a case of primary ciliary dyskinesia (PCD) without situs inversus, was screened for mutation in a series of 34 patients with KS. We identified compound heterozygous DNAI1 gene defects in three independent patients and in two of their siblings who presented with PCD and situs solitus (i.e., normal position of inner organs). Strikingly, these five patients share one mutant allele (splice defect), which is identical to one of the mutant DNAI1 alleles found in the patient with PCD, reported elsewhere. Finally, this study demonstrates a link between ciliary function and situs determination, since compound mutation heterozygosity in DNAI1 results in PCD with situs solitus or situs inversus (KS). (+info)Primary ciliary dyskinesia syndrome associated with abnormal ciliary orientation in infants. (6/143)
Primary ciliary dyskinesia (PCD) syndrome associated with abnormal ciliary orientation but with normal ciliary ultrastructure has been described in adults, but there are no normal ranges for orientation in infants, despite the fact that half of all patients with PCD present in the new-born period. Nasal brush biopsies were obtained from eight infants (three males), mean age 13.1 months, range 7-23, in order to determine ciliary orientation. They had no upper or lower airway disease and normal organ arrangement and were undergoing general anaesthesia for other reasons. Two infants with typical PCD syndrome but normal ultrastructure of individual cilia also had orientation studies. In the eight normal subjects, a mean of 254 central pairs was examined, range 82-453. The mean ciliary orientation was 14.9 degrees, range 12.9-17.5. The two infants with PCD syndrome but normal ultrastructure of individual cilia had ciliary orientation of (Case 1) 44.5 degrees (range 10.6-64.5) in 218 central pairs; and on a second occasion, 28.9 degrees, (range 9.0-47.5) in 259 central pairs; for Case 2, 24.4 degrees, (range 13.1-38.4) in 196 central pairs. The normal range for ciliary orientation is similar in infants to that described in other work in adults. The two cases of phenotypic primary ciliary dyskinesia in the presence of normal ciliary ultrastructure but abnormal ciliary orientation in infants supports the contention that measurement of ciliary orientation should be part of the assessment of ciliary structure and function in cases of possible primary ciliary dyskinesia, in particular when the ultrastructure of individual cilia appear to be normal. (+info)Anaesthesia for Kartagener's syndrome. (7/143)
Kartagener's syndrome is a hereditary syndrome involving a combination of dextrocardia (situs inversus), bronchiectasis and sinusitis, transmitted as an autosomal recessive trait. We describe a patient who had three anaesthetics over a period of a few months. Discussion relates to anaesthetic considerations in the syndrome and to recent findings relating to the molecular mechanisms of left-right development. (+info)Loss of function of axonemal dynein Mdnah5 causes primary ciliary dyskinesia and hydrocephalus. (8/143)
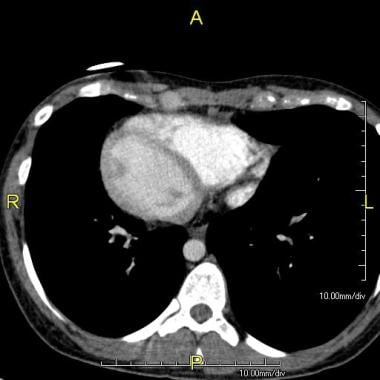
Primary ciliary dyskinesia (PCD), also known as Kartagener's syndrome, is a human syndrome that results from ciliary dysfunction. This syndrome is characterized by recurrent respiratory infections, situs inversus and infertility. In some cases, hydrocephalus is also observed. We have characterized an insertional mutation in a mouse axonemal dynein heavy chain gene (Mdnah5) that reproduces most of the classical features of PCD, including recurrent respiratory infections, situs inversus and ciliary immotility. These mice also suffer from hydrocephalus and die perinatally. Electron microscopic studies demonstrate the loss of axonemal outer arms. These results show that mutations in Mdnah5 are a primary cause of PCD and provide direct evidence that mutations in an axonemal dynein can cause hydrocephalus. Mutations in the human DNAH5 have recently been identified in PCD patients. Comparison of the mouse model and the human data suggests that the degree of ciliary dysfunction is causally related to the severity of human PCD, particularly the presence of hydrocephalus. (+info)Kartagener Syndrome is a rare genetic disorder that primarily affects the respiratory system. It is characterized by the triad of chronic sinusitis, bronchiectasis (damage and widening of the airways in the lungs), and situs inversus totalis - a condition where the major visceral organs are mirrored or reversed from their normal positions.
In Kartagener Syndrome, the cilia (tiny hair-like structures) lining the respiratory tract are abnormal or dysfunctional, which impairs their ability to clear mucus and other particles. This leads to recurrent respiratory infections, bronchiectasis, and ultimately, progressive lung damage.
The condition is inherited as an autosomal recessive trait, meaning that an individual must inherit two copies of the defective gene - one from each parent - to develop the syndrome. Kartagener Syndrome is a subtype of primary ciliary dyskinesia (PCD), a group of disorders affecting ciliary structure and function.
Ciliary motility disorders are a group of rare genetic conditions that affect the function of cilia, which are tiny hair-like structures on the surface of cells in the body. Cilia play an important role in moving fluids and particles across the cell surface, including the movement of mucus and other substances in the respiratory system, the movement of eggs and sperm in the reproductive system, and the movement of fluid in the inner ear.
Ciliary motility disorders are caused by mutations in genes that are responsible for the proper functioning of cilia. These mutations can lead to abnormalities in the structure or function of cilia, which can result in a range of symptoms depending on the specific disorder and the parts of the body that are affected.
Some common symptoms of ciliary motility disorders include recurrent respiratory infections, chronic sinusitis, hearing loss, infertility, and situs inversus, a condition in which the major organs are reversed or mirrored from their normal positions. There are several different types of ciliary motility disorders, including primary ciliary dyskinesia, Kartagener syndrome, and immotile cilia syndrome.
Treatment for ciliary motility disorders typically involves addressing the specific symptoms and underlying causes of the disorder. This may include antibiotics to treat respiratory infections, surgery to correct structural abnormalities, or assisted reproductive technologies to help with infertility.
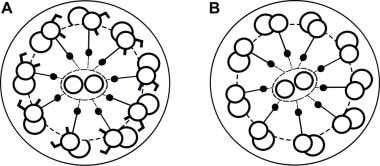
Axonemal dyneins are motor proteins that are located in the axoneme of eukaryotic cilia and flagella. The axoneme is the internal structure of these cellular appendages, and it is composed of nine microtubule doublets arranged in a ring around two central single microtubules.
Dyneins are large protein complexes that use the energy from ATP hydrolysis to move along microtubules, generating force and motion. Axonemal dyneins are responsible for the sliding of the microtubule doublets relative to each other, which leads to the bending and movement of cilia and flagella.
There are several types of axonemal dyneins, classified based on their structure and function. The outer dynein arms are larger complexes that generate the power stroke for ciliary beating, while the inner dynein arms are smaller complexes involved in regulating the beat pattern and frequency.
Defects in axonemal dyneins can lead to a variety of genetic disorders known as ciliopathies, which affect the structure and function of cilia and flagella. These disorders can cause a range of symptoms, including respiratory problems, infertility, and developmental abnormalities.
A syndrome, in medical terms, is a set of symptoms that collectively indicate or characterize a disease, disorder, or underlying pathological process. It's essentially a collection of signs and/or symptoms that frequently occur together and can suggest a particular cause or condition, even though the exact physiological mechanisms might not be fully understood.
For example, Down syndrome is characterized by specific physical features, cognitive delays, and other developmental issues resulting from an extra copy of chromosome 21. Similarly, metabolic syndromes like diabetes mellitus type 2 involve a group of risk factors such as obesity, high blood pressure, high blood sugar, and abnormal cholesterol or triglyceride levels that collectively increase the risk of heart disease, stroke, and diabetes.
It's important to note that a syndrome is not a specific diagnosis; rather, it's a pattern of symptoms that can help guide further diagnostic evaluation and management.
Bronchiectasis is a medical condition characterized by permanent, abnormal widening and thickening of the walls of the bronchi (the airways leading to the lungs). This can lead to recurrent respiratory infections, coughing, and the production of large amounts of sputum. The damage to the airways is usually irreversible and can be caused by various factors such as bacterial or viral infections, genetic disorders, immune deficiencies, or exposure to environmental pollutants. In some cases, the cause may remain unknown. Treatment typically includes chest physiotherapy, bronchodilators, antibiotics, and sometimes surgery.
An encyclopedia is a comprehensive reference work containing articles on various topics, usually arranged in alphabetical order. In the context of medicine, a medical encyclopedia is a collection of articles that provide information about a wide range of medical topics, including diseases and conditions, treatments, tests, procedures, and anatomy and physiology. Medical encyclopedias may be published in print or electronic formats and are often used as a starting point for researching medical topics. They can provide reliable and accurate information on medical subjects, making them useful resources for healthcare professionals, students, and patients alike. Some well-known examples of medical encyclopedias include the Merck Manual and the Stedman's Medical Dictionary.
Cystic fibrosis (CF) is a genetic disorder that primarily affects the lungs and digestive system. It is caused by mutations in the CFTR gene, which regulates the movement of salt and water in and out of cells. When this gene is not functioning properly, thick, sticky mucus builds up in various organs, leading to a range of symptoms.
In the lungs, this mucus can clog the airways, making it difficult to breathe and increasing the risk of lung infections. Over time, lung damage can occur, which may lead to respiratory failure. In the digestive system, the thick mucus can prevent the release of digestive enzymes from the pancreas, impairing nutrient absorption and leading to malnutrition. CF can also affect the reproductive system, liver, and other organs.
Symptoms of cystic fibrosis may include persistent coughing, wheezing, lung infections, difficulty gaining weight, greasy stools, and frequent greasy diarrhea. The severity of the disease can vary significantly among individuals, depending on the specific genetic mutations they have inherited.
Currently, there is no cure for cystic fibrosis, but treatments are available to help manage symptoms and slow the progression of the disease. These may include airway clearance techniques, medications to thin mucus, antibiotics to treat infections, enzyme replacement therapy, and a high-calorie, high-fat diet. Lung transplantation is an option for some individuals with advanced lung disease.
Inflammation is a complex biological response of tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. It is characterized by the following signs: rubor (redness), tumor (swelling), calor (heat), dolor (pain), and functio laesa (loss of function). The process involves the activation of the immune system, recruitment of white blood cells, and release of inflammatory mediators, which contribute to the elimination of the injurious stimuli and initiation of the healing process. However, uncontrolled or chronic inflammation can also lead to tissue damage and diseases.
A cough is a reflex action that helps to clear the airways of irritants, foreign particles, or excess mucus or phlegm. It is characterized by a sudden, forceful expulsion of air from the lungs through the mouth and nose. A cough can be acute (short-term) or chronic (long-term), and it can be accompanied by other symptoms such as chest pain, shortness of breath, or fever. Coughing can be caused by various factors, including respiratory infections, allergies, asthma, environmental pollutants, gastroesophageal reflux disease (GERD), and chronic lung diseases such as chronic obstructive pulmonary disease (COPD) and bronchitis. In some cases, a cough may be a symptom of a more serious underlying condition, such as heart failure or lung cancer.
Obstructive lung disease is a category of respiratory diseases characterized by airflow limitation that causes difficulty in completely emptying the alveoli (tiny air sacs) of the lungs during exhaling. This results in the trapping of stale air and prevents fresh air from entering the alveoli, leading to various symptoms such as coughing, wheezing, shortness of breath, and decreased exercise tolerance.
The most common obstructive lung diseases include:
1. Chronic Obstructive Pulmonary Disease (COPD): A progressive disease that includes chronic bronchitis and emphysema, often caused by smoking or exposure to harmful pollutants.
2. Asthma: A chronic inflammatory disorder of the airways characterized by variable airflow obstruction, bronchial hyperresponsiveness, and an underlying inflammation. Symptoms can be triggered by various factors such as allergens, irritants, or physical activity.
3. Bronchiectasis: A condition in which the airways become abnormally widened, scarred, and thickened due to chronic inflammation or infection, leading to mucus buildup and impaired clearance.
4. Cystic Fibrosis: An inherited genetic disorder that affects the exocrine glands, resulting in thick and sticky mucus production in various organs, including the lungs. This can lead to chronic lung infections, inflammation, and airway obstruction.
5. Alpha-1 Antitrypsin Deficiency: A genetic condition characterized by low levels of alpha-1 antitrypsin protein, which leads to uncontrolled protease enzyme activity that damages the lung tissue, causing emphysema-like symptoms.
Treatment for obstructive lung diseases typically involves bronchodilators (to relax and widen the airways), corticosteroids (to reduce inflammation), and lifestyle modifications such as smoking cessation and pulmonary rehabilitation programs. In severe cases, oxygen therapy or even lung transplantation may be considered.
Mucus is a viscous, slippery secretion produced by the mucous membranes that line various body cavities such as the respiratory and gastrointestinal tracts. It serves to lubricate and protect these surfaces from damage, infection, and foreign particles. Mucus contains water, proteins, salts, and other substances, including antibodies, enzymes, and glycoproteins called mucins that give it its characteristic gel-like consistency.
In the respiratory system, mucus traps inhaled particles such as dust, allergens, and pathogens, preventing them from reaching the lungs. The cilia, tiny hair-like structures lining the airways, move the mucus upward toward the throat, where it can be swallowed or expelled through coughing or sneezing. In the gastrointestinal tract, mucus helps protect the lining of the stomach and intestines from digestive enzymes and other harmful substances.
Excessive production of mucus can occur in various medical conditions such as allergies, respiratory infections, chronic lung diseases, and gastrointestinal disorders, leading to symptoms such as coughing, wheezing, nasal congestion, and diarrhea.
 Bronchiectasis
Bronchiectasis Primary Ciliary Dyskinesia (Kartagener Syndrome): Background, Pathophysiology, Etiology
Primary Ciliary Dyskinesia (Kartagener Syndrome): Background, Pathophysiology, Etiology A Case of Kartagener Syndrome With Pulmonary Hypertension | Ghewade | Journal of Medical Cases
A Case of Kartagener Syndrome With Pulmonary Hypertension | Ghewade | Journal of Medical Cases Kartagener Syndrome | Diseases & Conditions | 5MinuteConsult
Kartagener Syndrome | Diseases & Conditions | 5MinuteConsult Female infertility due to kartagener's syndrome
Female infertility due to kartagener's syndrome Aerobic exercise training in Kartagener's syndrome: case report
Aerobic exercise training in Kartagener's syndrome: case report Primary ciliary dyskinesia (Siewert's / Kartagener's Syndrome): Respiratory symptoms and psycho-social impact | BMC Pulmonary...
Primary ciliary dyskinesia (Siewert's / Kartagener's Syndrome): Respiratory symptoms and psycho-social impact | BMC Pulmonary... Shubhamoy Ghosh - Hpathy.com
Shubhamoy Ghosh - Hpathy.com Dextrocardia : MedlinePlus Medical Encyclopedia
Dextrocardia : MedlinePlus Medical Encyclopedia Primary ciliary dyskinesia. Recent advances in diagnostics, genetics, and characterization of clinical disease
Primary ciliary dyskinesia. Recent advances in diagnostics, genetics, and characterization of clinical disease Dyspnée récidivante révélatrice d'un syndrome de Kartagener: à propos d'un cas | Rev. Anesth.-Réanim. Med. Urg. Toxicol.;15(1...
Dyspnée récidivante révélatrice d'un syndrome de Kartagener: à propos d'un cas | Rev. Anesth.-Réanim. Med. Urg. Toxicol.;15(1... Clinical manifestations in primary ciliary dyskinesia: systematic review and meta-analysis | European Respiratory Society
Clinical manifestations in primary ciliary dyskinesia: systematic review and meta-analysis | European Respiratory Society Hong Kong College Of Radiologists: Answer of February 2007
Hong Kong College Of Radiologists: Answer of February 2007 Primary Ciliary Dyskinesia
Primary Ciliary Dyskinesia People Share Their Best Predictions For 2022 - George Takei
People Share Their Best Predictions For 2022 - George Takei Chronic Non-Cardiac Cough in Dogs - WSAVA2010 - VIN
Chronic Non-Cardiac Cough in Dogs - WSAVA2010 - VIN Pathoma - Respiratory Pathology Flashcards by Jon L | Brainscape
Pathoma - Respiratory Pathology Flashcards by Jon L | Brainscape Baby’s Pregnancy Calendar
Baby’s Pregnancy Calendar Primary Ciliary Dyskinesia - Old English Sheepdog Club of America
Primary Ciliary Dyskinesia - Old English Sheepdog Club of America Medizinische Hochschule Hannover : New treatment approach for incurable hereditary disease PCD
Medizinische Hochschule Hannover : New treatment approach for incurable hereditary disease PCD