Recurrent Laryngeal Nerve Injuries
Recurrent Laryngeal Nerve
Laryngeal Nerves
Vocal Cord Paralysis
Laryngeal Muscles
Cranial Nerve Injuries
Larynx
Sciatic Nerve
Optic Nerve Injuries
Wounds and Injuries
Facial Nerve Injuries
Peripheral Nerves
Spinal Nerves
Phrenic Nerve
Sciatic Neuropathy
Neuralgia
Trigeminal Nerve Injuries
Lingual Nerve Injuries
Trauma, Nervous System
Laryngoscopy
Voice Disorders
Brain Injuries
Optic Nerve
Hypoglossal Nerve
Nerve Fibers
Deglutition
Glossopharyngeal Nerve
Reflex
Spinal Cord Injuries
Axotomy
Hyperalgesia
Cats
Quantitative analysis of the anatomy of the epineurium of the canine recurrent laryngeal nerve. (1/21)
The purpose of this investigation was to determine the amount of epineurium surrounding the recurrent laryngeal nerve (RLN) compared with a limb nerve, that to flexor hallicus longus (NFHL). Nerve samples were obtained from 10 adult dogs and studied using scanning electron microscopy and light microscopy to measure the relative proportion of epineurium and the relative proportions of adipose and collagenous tissue comprising the epineurium in both nerves. Significantly greater relative epineurial cross-sectional areas and adipose content were found in the RLN than in the NFHL. Based on observations on noncranial peripheral nerves, the findings indicate that the RLN is better protected against deformational forces associated with compression than stretching forces. The RLN may not be structured well for successful reinnervation after injury. The patterns observed for adipose tissue in RLN epineurial tissue appeared unique compared with those previously reported in peripheral nerves. The primary role associated with adipose tissue is to 'package' the nerve for protection. The RLN is considered to be a vital nerve in the body, as are other cranial nerves. The large proportions of adipose tissue in the epineurium may relate to the importance of protecting this nerve from injury. (+info)Cranial and cervical nerve injuries after repeat carotid endarterectomy. (2/21)
BACKGROUND AND PURPOSE: The incidence of cranial and/or cervical nerve injuries after primary carotid endarterectomy (CEA) ranges from 3% to 48%; however, the clinical outcome of these injuries after repeat CEA has not been thoroughly analyzed in the English-language medical literature. This prospective study analyzes the incidence and outcome of cranial nerve injuries after repeat CEA. PATIENTS AND METHODS: This study includes 89 consecutive patients who had repeat CEAs. Preoperative and postoperative cranial nerve evaluations were performed, including clinical examinations (neurologic) and direct laryngoscopy. Patients with vagal or glossopharyngeal nerve injuries also underwent comprehensive speech evaluations, video stroboscopy, fluoroscopy, and methylene blue testing for aspiration. Patients with postoperative cranial nerve injuries were followed up for a long time to assess their recovery. RESULTS: Twenty-five cranial and/or cervical nerve injuries were identified in 19 patients (21%). They included 8 hypoglossal nerves (9%), 11 vagal nerves or branches (12%) (6 recurrent laryngeal nerves [7%], 3 superior laryngeal nerves [3%], and 2 complex vagal nerves [2%]), 3 marginal mandibular nerves (3%), 2 greater auricular nerves (2%), and 1 glossopharyngeal nerve (1%). Twenty-two (88%) of these injuries were transient with a complete healing time ranging from 2 weeks to 28 months (18 of 22 injuries healed within 12 months). The remaining three injuries (12%) were permanent (1 recurrent laryngeal nerve, 1 glossopharyngeal nerve, and 1 complex vagal nerve injury). The recurrent laryngeal nerve injury had a longer healing time than the other cranial nerve injuries. CONCLUSIONS: Repeat CEA is associated with a high incidence of cranial and/or cervical nerve injuries, most of which are transient. However, some of these have a long healing time, and a few can be permanent with significant disability. (+info)Injury to the superior laryngeal branch of the vagus during thyroidectomy: lesson or myth? (3/21)
OBJECTIVE: To examine the historical evidence that the thyroidectomy performed on operatic soprano Amelita Galli-Curci was responsible for the abrupt termination of her career. SUMMARY BACKGROUND DATA: The superior laryngeal branch of the vagus nerve may be injured during thyroidectomy, producing vocal defects more subtle than those found after recurrent nerve injury. It is widely believed that Galli-Curci suffered superior laryngeal nerve injury during her thyroidectomy by Arnold Kegel, MD, in 1935, resulting in the termination of her career. METHODS: The authors examined contemporary press reviews after surgery, conducted interviews with colleagues and relatives of the surgeon, and compared the career of Galli-Curci with that of other singers. RESULTS: Evidence against the prevailing view is to be found in the fact that she continued to perform acceptably after surgery, her continued friendly relationship with the surgeon for years afterward, the absence of the typical effects of superior laryngeal nerve injury, and the presence of other explanations for the gradual decline in her vocal abilities (documentation of deterioration before surgery, physiologic changes in the larynx comparable to those found in most other famous sopranos who retire at about the same age or earlier, and the possible development of myxedema). CONCLUSIONS: The story should no longer be perpetuated in surgical textbooks and papers. (+info)Prospective study of postoperative complications after total thyroidectomy for multinodular goiters by surgeons with experience in endocrine surgery. (4/21)
OBJECTIVES: (1) To show that total thyroidectomy (TT) can be performed in multinodular goiter (MG) by surgeons with experience in endocrine surgery with a definitive complication rate of 1% or less; and (2) to analyze the risk factors for complications in these patients. SUMMARY BACKGROUND DATA: There is current controversy over the role of TT in the treatment of MG; although there are potential benefits, high rates of complications are not acceptable in surgery for a benign pathology. PATIENTS AND METHOD: A prospective study was conducted on 301 MGs meeting the following criteria: (1) bilateral MG; (2) no prior cervical surgery; (3) operation by surgeons with experience in endocrine surgery; (4) no associated parathyroid pathology; (5) no initial thoracic approach; and (6) minimum follow-up of 1 year. Age, sex, time of evolution, symptoms, cervical goiter grade, intrathoracic component, thyroid weight, and presence of associated carcinoma were analyzed as risk factors for complications. The chi test and a logistic regression analysis were applied. RESULTS: Complications were presented by 62 patients (21%), corresponding to 29 hypoparathyroidisms, 26 recurrent laryngeal nerve injuries, 4 lesions of the superior laryngeal nerve, 3 cervical hematomas, and 1 infection of the cervicotomy. The variables associated with the presence of these complications were hyperthyroidism (P = 0.0033), compressive symptoms (P = 0.0455), intrathoracic component (P = 0.0366), goiter grade (P = 0.0195), and weight of excised specimen (P = 0.0302); hyperthyroidism (relative risk [RR] 2.5) and intrathoracic component (RR 1.5) persisted as independent risk factors. Definitive complications appeared in 3 patients (1%), corresponding to 2 hypoparathyroidisms and 1 recurrent laryngeal nerve injury. Two cases corresponded to a toxic goiter, and the third to an intrathoracic goiter with compressive symptoms. CONCLUSION: In endocrine surgery units, TT can be performed for MG with a definitive complication rate of around 1%; the main independent risk factors for the development of complications are hyperthyroidism and goiter size. (+info)Incidence of cranial nerve injuries after carotid eversion endarterectomy with a transverse skin incision under regional anaesthesia. (5/21)
OBJECTIVES: The objective of this prospective study was to evaluate the incidence and distribution of cranial nerve injuries after carotid eversion endarterectomy (EEA) performed under regional anaesthesia using a transverse skin incision. PATIENTS AND METHODS: The study included 165 patients and 180 carotid arteries. All patients had a standard pre-operative assessment performed by a neurologist and ENT specialist. All carotid endarterectomies were performed by the eversion technique under regional anaesthesia. RESULTS: Ten cranial nerve injuries were observed. Seven patients had injuries of the marginal mandibular branch of the facial nerve, two patients had lesions of the hypoglossal nerve, and one patient had an injury of the recurrent laryngeal nerve. Eleven patients developed hoarseness without cranial nerve injury. Injuries of the marginal mandibular branch recovered after 3-8 months (mean 5.2 months). Both hypoglossal nerve injuries recovered after 4 months. The patient with the recurrent laryngeal palsy had no improvement after 19 months. Patients with hoarseness secondary to laryngeal haematoma recovered within 1 month. CONCLUSION: The incidence of cranial nerves injury after carotid EEA under regional anaesthesia is comparable to that reported for conventional carotid surgery. Postoperative hoarseness is most frequently due to laryngeal haematoma. (+info)Surgical anatomy of the internal branch of the superior laryngeal nerve. (6/21)
The internal branch of the superior laryngeal nerve (ibSLN) may be injured during anterior approaches to the cervical spine, resulting in loss of laryngeal cough reflex, and, in turn, the risk of aspiration pneumonia. Such a risk dictates the knowledge regarding anatomical details of this nerve. In this study, 24 ibSLN of 12 formaldehyde fixed adult male cadavers were used. Linear and angular parameters were measured using a Vernier caliper, with a sensitivity of 0.1 mm, and a 1 degrees goniometer. The diameter and the length of the ibSLN were measured as 2.1+/-0.2 mm and 57.2+/-7.7 mm, respectively. The ibSLN originates from the vagus nerve at the C1 level in 5 cases (20.83%), at the C2 level in 14 cases (58.34%), and at the C2-3 intervertebral disc level in 5 cases (20.83%) of the specimens. The distance between the origin of ibSLN and the bifurcation of carotid artery was 35.2+/-12.9 mm. The distance between the ibSLN and midline was 24.2+/-3.3 mm, 20.2+/-3.6 mm, and 15.9+/-4.3 mm at the level of C2-3, C3-4, and at the C4-5 intervertebral disc level, respectively. The angles of ibSLN were mean 19.6+/-2.6 degrees medially with sagittal plane, and 23.6+/-2.6 degrees anteriorly with coronal plane. At the area between the thyroid cartilage and the hyoid bone the ibSLN is the only nerve which traverses lateral to medial. It is accompanied by the superior laryngeal artery, a branch of the superior thyroid artery. The ibSLN is under the risk of injury as a result of cutting or compression of the blades of the retractor at this level. The morphometric data regarding the ibSLN, information regarding the distances between the nerve, and the other consistent structures may help us identify this nerve, and to avoid the nerve injury. (+info)Transient palsy of peripheral cranial nerves following open heart surgery. (7/21)
A 32-year-old man developed hoarseness of voice, inability to swallow and restricted movement of the tongue after open heart surgery. Peripheral injury of the cranial nerves IX, X and XII was suspected, and it was thought that the duration of the surgery together with the endotracheal tube cuff and trans-oesophageal echocardiography probe pressure, as well as the head and neck position might have been the causes of this complication. (+info)The external laryngeal nerve in thyroid surgery: the 'no more neglected' nerve. (8/21)
AIMS: To describe a novel surgical technique of 'lateralization' of superior pole to identify and save external branch of superior laryngeal nerve (EBSLN) during thyroidectomy. SETTINGS AND DESIGN: Prospective, nonrandomized at a tertiary care hospital in a specialized unit. MATERIAL AND METHODS: Over 30 months, 46 patients underwent thyroidectomy using technique of 1) 'Lateralization' of upper pole and dissection of avascular cricothyroid space 2) identification of EBSLN 3) skeletonization and individual ligation of superior thyroid vessels. Identified nerves were classified according to Cernea's classification. Outcomes were number of nerves identified, number of 'at risk' nerves' bilateral asymmetry and incidence of injury assessed by subjective interview and indirect laryngoscopy. RESULTS: Of the 78 dissected superior poles, nerves could be identified in 72 (92.31%). There were 22 (28.2%) type I, 42 (53.54%) IIa and 8 (10.25%) IIb 'at risk' nerves. In 32 patients with bilateral dissections, asymmetry of nerve was noted in 15%. Injury to nerve was not recorded in any of the patients. Average weight of glands was 69.59 g. Thyroidectomy was performed for benign disease in 28, malignancy in 4 and thyrotoxicosis in 14 patients. CONCLUSIONS: With technique of 'lateralization' and 'skeletonization and individual ligation of the superior vessels,' EBSLN identification increases and injury can be prevented. These results relate to the utilization of specific surgical technique and it is reasonable to expect that most surgeons, once familiar with the technique, should be able to achieve similar outcomes. (+info)Recurrent laryngeal nerve injuries refer to damages or trauma inflicted on the recurrent laryngeal nerve, which is a branch of the vagus nerve that supplies motor function to the intrinsic muscles of the larynx, except for the cricothyroid muscle. This nerve plays a crucial role in controlling vocal fold movement and swallowing.
Injuries to this nerve can result in voice changes, hoarseness, or even complete loss of voice, depending on the severity and location of the injury. Additionally, it may also lead to breathing difficulties, coughing, and choking while swallowing due to impaired laryngeal function.
Recurrent laryngeal nerve injuries can occur due to various reasons, such as surgical complications (particularly during thyroid or neck surgeries), tumors, infections, inflammation, or direct trauma to the neck region. In some cases, these injuries may be temporary and resolve on their own or through appropriate treatment; however, severe or prolonged injuries might require medical intervention, including possible surgical repair.
Laryngeal nerve injuries refer to damages or injuries to the recurrent laryngeal nerve (RLN) and/or the superior laryngeal nerve (SLN), which are the primary nerves that supply the larynx, or voice box. These nerves play crucial roles in controlling the vocal cord movements and protecting the airway during swallowing.
The recurrent laryngeal nerve provides motor function to all intrinsic muscles of the larynx, except for the cricothyroid muscle, which is innervated by the superior laryngeal nerve. The RLN also carries sensory fibers from a small area of the mucous membrane below the vocal folds.
Injuries to these nerves can result in voice changes, breathing difficulties, and swallowing problems. Depending on the severity and location of the injury, patients may experience hoarseness, weak voice, breathy voice, coughing while swallowing, or even complete airway obstruction in severe cases. Laryngeal nerve injuries can occur due to various reasons, such as surgical complications (e.g., thyroid, esophageal, and cardiovascular surgeries), neck trauma, tumors, infections, or iatrogenic causes.
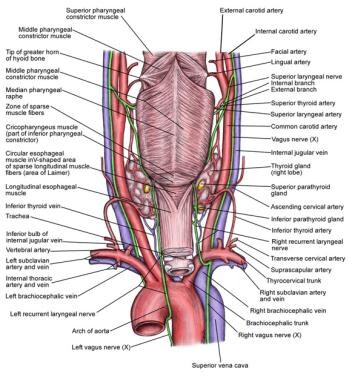
The Recurrent Laryngeal Nerve (RLN) is a branch of the vagus nerve (cranial nerve X), which is a mixed sensory, motor, and autonomic nerve. The RLN has important functions in providing motor innervation to the intrinsic muscles of the larynx, except for the cricothyroid muscle, which is supplied by the external branch of the superior laryngeal nerve.
The recurrent laryngeal nerve supplies all the muscles that are responsible for adduction (bringing together) of the vocal cords, including the vocalis muscle, lateral cricoarytenoid, thyroarytenoid, and interarytenoid muscles. These muscles play a crucial role in voice production, coughing, and swallowing.
The right recurrent laryngeal nerve has a longer course than the left one. It loops around the subclavian artery in the chest before ascending to the larynx, while the left RLN hooks around the arch of the aorta. This anatomical course makes them vulnerable to injury during various surgical procedures, such as thyroidectomy and neck dissection, leading to potential voice impairment or vocal cord paralysis.
The laryngeal nerves are a pair of nerves that originate from the vagus nerve (cranial nerve X) and provide motor and sensory innervation to the larynx. There are two branches of the laryngeal nerves: the superior laryngeal nerve and the recurrent laryngeal nerve.
The superior laryngeal nerve has two branches: the external branch, which provides motor innervation to the cricothyroid muscle and sensation to the mucous membrane of the laryngeal vestibule; and the internal branch, which provides sensory innervation to the mucous membrane of the laryngeal vestibule.
The recurrent laryngeal nerve provides motor innervation to all the intrinsic muscles of the larynx, except for the cricothyroid muscle, and sensation to the mucous membrane below the vocal folds. The right recurrent laryngeal nerve has a longer course than the left one, as it hooks around the subclavian artery before ascending to the larynx.
Damage to the laryngeal nerves can result in voice changes, difficulty swallowing, and respiratory distress.
Vocal cord paralysis is a medical condition characterized by the inability of one or both vocal cords to move or function properly due to nerve damage or disruption. The vocal cords are two bands of muscle located in the larynx (voice box) that vibrate to produce sound during speech, singing, and breathing. When the nerves that control the vocal cord movements are damaged or not functioning correctly, the vocal cords may become paralyzed or weakened, leading to voice changes, breathing difficulties, and other symptoms.
The causes of vocal cord paralysis can vary, including neurological disorders, trauma, tumors, surgery, or infections. The diagnosis typically involves a physical examination, including a laryngoscopy, to assess the movement and function of the vocal cords. Treatment options may include voice therapy, surgical procedures, or other interventions to improve voice quality and breathing functions.
Thyroidectomy is a surgical procedure where all or part of the thyroid gland is removed. The thyroid gland is a butterfly-shaped endocrine gland located in the neck, responsible for producing hormones that regulate metabolism, growth, and development.
There are different types of thyroidectomy procedures, including:
1. Total thyroidectomy: Removal of the entire thyroid gland.
2. Partial (or subtotal) thyroidectomy: Removal of a portion of the thyroid gland.
3. Hemithyroidectomy: Removal of one lobe of the thyroid gland, often performed to treat benign solitary nodules or differentiated thyroid cancer.
Thyroidectomy may be recommended for various reasons, such as treating thyroid nodules, goiter, hyperthyroidism (overactive thyroid), or thyroid cancer. Potential risks and complications of the procedure include bleeding, infection, damage to nearby structures like the parathyroid glands and recurrent laryngeal nerve, and hypoparathyroidism or hypothyroidism due to removal of or damage to the parathyroid glands or thyroid gland, respectively. Close postoperative monitoring and management are essential to minimize these risks and ensure optimal patient outcomes.
Peripheral nerve injuries refer to damage or trauma to the peripheral nerves, which are the nerves outside the brain and spinal cord. These nerves transmit information between the central nervous system (CNS) and the rest of the body, including sensory, motor, and autonomic functions. Peripheral nerve injuries can result in various symptoms, depending on the type and severity of the injury, such as numbness, tingling, weakness, or paralysis in the affected area.
Peripheral nerve injuries are classified into three main categories based on the degree of damage:
1. Neuropraxia: This is the mildest form of nerve injury, where the nerve remains intact but its function is disrupted due to a local conduction block. The nerve fiber is damaged, but the supporting structures remain intact. Recovery usually occurs within 6-12 weeks without any residual deficits.
2. Axonotmesis: In this type of injury, there is damage to both the axons and the supporting structures (endoneurium, perineurium). The nerve fibers are disrupted, but the connective tissue sheaths remain intact. Recovery can take several months or even up to a year, and it may be incomplete, with some residual deficits possible.
3. Neurotmesis: This is the most severe form of nerve injury, where there is complete disruption of the nerve fibers and supporting structures (endoneurium, perineurium, epineurium). Recovery is unlikely without surgical intervention, which may involve nerve grafting or repair.
Peripheral nerve injuries can be caused by various factors, including trauma, compression, stretching, lacerations, or chemical exposure. Treatment options depend on the type and severity of the injury and may include conservative management, such as physical therapy and pain management, or surgical intervention for more severe cases.
The laryngeal muscles are a group of skeletal muscles located in the larynx, also known as the voice box. These muscles play a crucial role in breathing, swallowing, and producing sounds for speech. They include:
1. Cricothyroid muscle: This muscle helps to tense the vocal cords and adjust their pitch during phonation (voice production). It is the only laryngeal muscle that is not innervated by the recurrent laryngeal nerve. Instead, it is supplied by the external branch of the superior laryngeal nerve.
2. Posterior cricoarytenoid muscle: This muscle is primarily responsible for abducting (opening) the vocal cords during breathing and speaking. It is the only muscle that can abduct the vocal cords.
3. Lateral cricoarytenoid muscle: This muscle adducts (closes) the vocal cords during phonation, swallowing, and coughing.
4. Transverse arytenoid muscle: This muscle also contributes to adduction of the vocal cords, working together with the lateral cricoarytenoid muscle. It also helps to relax and lengthen the vocal cords during quiet breathing.
5. Oblique arytenoid muscle: This muscle is involved in adducting, rotating, and shortening the vocal cords. It works together with the transverse arytenoid muscle to provide fine adjustments for voice production.
6. Thyroarytenoid muscle (Vocalis): This muscle forms the main body of the vocal cord and is responsible for its vibration during phonation. The vocalis portion of the muscle helps control pitch and tension in the vocal cords.
These muscles work together to enable various functions of the larynx, such as breathing, swallowing, and speaking.
Cranial nerve injuries refer to damages or trauma to one or more of the twelve cranial nerves (CN I through CN XII). These nerves originate from the brainstem and are responsible for transmitting sensory information (such as vision, hearing, smell, taste, and balance) and controlling various motor functions (like eye movement, facial expressions, swallowing, and speaking).
Cranial nerve injuries can result from various causes, including head trauma, tumors, infections, or neurological conditions. The severity of the injury may range from mild dysfunction to complete loss of function, depending on the extent of damage to the nerve. Treatment options vary based on the type and location of the injury but often involve a combination of medical management, physical therapy, surgical intervention, or rehabilitation.
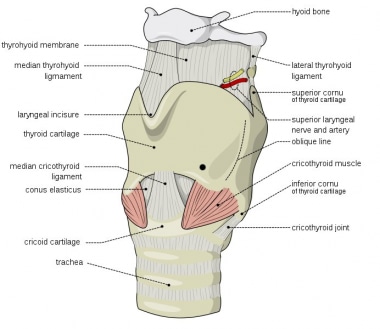
The larynx, also known as the voice box, is a complex structure in the neck that plays a crucial role in protection of the lower respiratory tract and in phonation. It is composed of cartilaginous, muscular, and soft tissue structures. The primary functions of the larynx include:
1. Airway protection: During swallowing, the larynx moves upward and forward to close the opening of the trachea (the glottis) and prevent food or liquids from entering the lungs. This action is known as the swallowing reflex.
2. Phonation: The vocal cords within the larynx vibrate when air passes through them, producing sound that forms the basis of human speech and voice production.
3. Respiration: The larynx serves as a conduit for airflow between the upper and lower respiratory tracts during breathing.
The larynx is located at the level of the C3-C6 vertebrae in the neck, just above the trachea. It consists of several important structures:
1. Cartilages: The laryngeal cartilages include the thyroid, cricoid, and arytenoid cartilages, as well as the corniculate and cuneiform cartilages. These form a framework for the larynx and provide attachment points for various muscles.
2. Vocal cords: The vocal cords are thin bands of mucous membrane that stretch across the glottis (the opening between the arytenoid cartilages). They vibrate when air passes through them, producing sound.
3. Muscles: There are several intrinsic and extrinsic muscles associated with the larynx. The intrinsic muscles control the tension and position of the vocal cords, while the extrinsic muscles adjust the position and movement of the larynx within the neck.
4. Nerves: The larynx is innervated by both sensory and motor nerves. The recurrent laryngeal nerve provides motor innervation to all intrinsic laryngeal muscles, except for one muscle called the cricothyroid, which is innervated by the external branch of the superior laryngeal nerve. Sensory innervation is provided by the internal branch of the superior laryngeal nerve and the recurrent laryngeal nerve.
The larynx plays a crucial role in several essential functions, including breathing, speaking, and protecting the airway during swallowing. Dysfunction or damage to the larynx can result in various symptoms, such as hoarseness, difficulty swallowing, shortness of breath, or stridor (a high-pitched sound heard during inspiration).
The sciatic nerve is the largest and longest nerve in the human body, running from the lower back through the buttocks and down the legs to the feet. It is formed by the union of the ventral rami (branches) of the L4 to S3 spinal nerves. The sciatic nerve provides motor and sensory innervation to various muscles and skin areas in the lower limbs, including the hamstrings, calf muscles, and the sole of the foot. Sciatic nerve disorders or injuries can result in symptoms such as pain, numbness, tingling, or weakness in the lower back, hips, legs, and feet, known as sciatica.
Hypoglossal nerve injuries refer to damages or impairments to the twelfth cranial nerve, also known as the hypoglossal nerve. This nerve is primarily responsible for controlling the movements of the tongue.
An injury to this nerve can result in various symptoms, depending on the severity and location of the damage. These may include:
1. Deviation of the tongue to one side when protruded (usually away from the side of the lesion)
2. Weakness or paralysis of the tongue muscles
3. Difficulty with speaking, swallowing, and articulation
4. Changes in taste and sensation on the back of the tongue (in some cases)
Hypoglossal nerve injuries can occur due to various reasons, such as trauma, surgical complications, tumors, or neurological disorders like stroke or multiple sclerosis. Treatment for hypoglossal nerve injuries typically focuses on managing symptoms and may involve speech and language therapy, exercises to strengthen the tongue muscles, and, in some cases, surgical intervention.
Optic nerve injuries refer to damages or trauma inflicted on the optic nerve, which is a crucial component of the visual system. The optic nerve transmits visual information from the retina to the brain, enabling us to see. Injuries to the optic nerve can result in various visual impairments, including partial or complete vision loss, decreased visual acuity, changes in color perception, and reduced field of view.
These injuries may occur due to several reasons, such as:
1. Direct trauma to the eye or head
2. Increased pressure inside the eye (glaucoma)
3. Optic neuritis, an inflammation of the optic nerve
4. Ischemia, or insufficient blood supply to the optic nerve
5. Compression from tumors or other space-occupying lesions
6. Intrinsic degenerative conditions affecting the optic nerve
7. Toxic exposure to certain chemicals or medications
Optic nerve injuries are diagnosed through a comprehensive eye examination, including visual acuity testing, slit-lamp examination, dilated fundus exam, and additional diagnostic tests like optical coherence tomography (OCT) and visual field testing. Treatment options vary depending on the cause and severity of the injury but may include medications, surgery, or vision rehabilitation.
A wound is a type of injury that occurs when the skin or other tissues are cut, pierced, torn, or otherwise broken. Wounds can be caused by a variety of factors, including accidents, violence, surgery, or certain medical conditions. There are several different types of wounds, including:
* Incisions: These are cuts that are made deliberately, often during surgery. They are usually straight and clean.
* Lacerations: These are tears in the skin or other tissues. They can be irregular and jagged.
* Abrasions: These occur when the top layer of skin is scraped off. They may look like a bruise or a scab.
* Punctures: These are wounds that are caused by sharp objects, such as needles or knives. They are usually small and deep.
* Avulsions: These occur when tissue is forcibly torn away from the body. They can be very serious and require immediate medical attention.
Injuries refer to any harm or damage to the body, including wounds. Injuries can range from minor scrapes and bruises to more severe injuries such as fractures, dislocations, and head trauma. It is important to seek medical attention for any injury that is causing significant pain, swelling, or bleeding, or if there is a suspected bone fracture or head injury.
In general, wounds and injuries should be cleaned and covered with a sterile bandage to prevent infection. Depending on the severity of the wound or injury, additional medical treatment may be necessary. This may include stitches for deep cuts, immobilization for broken bones, or surgery for more serious injuries. It is important to follow your healthcare provider's instructions carefully to ensure proper healing and to prevent complications.
Facial nerve injuries refer to damages or trauma inflicted on the facial nerve, also known as the seventh cranial nerve (CN VII). This nerve is responsible for controlling the muscles involved in facial expressions, eyelid movement, and taste sensation in the front two-thirds of the tongue.
There are two main types of facial nerve injuries:
1. Peripheral facial nerve injury: This type of injury occurs when damage affects the facial nerve outside the skull base, usually due to trauma from cuts, blunt force, or surgical procedures in the parotid gland or neck region. The injury may result in weakness or paralysis on one side of the face, known as Bell's palsy, and may also impact taste sensation and salivary function.
2. Central facial nerve injury: This type of injury occurs when damage affects the facial nerve within the skull base, often due to stroke, brain tumors, or traumatic brain injuries. Central facial nerve injuries typically result in weakness or paralysis only on the lower half of the face, as the upper motor neurons responsible for controlling the upper face receive innervation from both sides of the brain.
Treatment for facial nerve injuries depends on the severity and location of the damage. For mild to moderate injuries, physical therapy, protective eyewear, and medications like corticosteroids and antivirals may be prescribed. Severe cases might require surgical intervention, such as nerve grafts or muscle transfers, to restore function. In some instances, facial nerve injuries may heal on their own over time, particularly when the injury is mild and there is no ongoing compression or tension on the nerve.
Peripheral nerves are nerve fibers that transmit signals between the central nervous system (CNS, consisting of the brain and spinal cord) and the rest of the body. These nerves convey motor, sensory, and autonomic information, enabling us to move, feel, and respond to changes in our environment. They form a complex network that extends from the CNS to muscles, glands, skin, and internal organs, allowing for coordinated responses and functions throughout the body. Damage or injury to peripheral nerves can result in various neurological symptoms, such as numbness, weakness, or pain, depending on the type and severity of the damage.
Spinal nerves are the bundles of nerve fibers that transmit signals between the spinal cord and the rest of the body. There are 31 pairs of spinal nerves in the human body, which can be divided into five regions: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each spinal nerve carries both sensory information (such as touch, temperature, and pain) from the periphery to the spinal cord, and motor information (such as muscle control) from the spinal cord to the muscles and other structures in the body. Spinal nerves also contain autonomic fibers that regulate involuntary functions such as heart rate, digestion, and blood pressure.
A nerve crush injury is a type of peripheral nerve injury that occurs when there is excessive pressure or compression applied to a nerve, causing it to become damaged or dysfunctional. This can happen due to various reasons such as trauma from accidents, surgical errors, or prolonged pressure on the nerve from tight casts, clothing, or positions.
The compression disrupts the normal functioning of the nerve, leading to symptoms such as numbness, tingling, weakness, or pain in the affected area. In severe cases, a nerve crush injury can cause permanent damage to the nerve, leading to long-term disability or loss of function. Treatment for nerve crush injuries typically involves relieving the pressure on the nerve, providing supportive care, and in some cases, surgical intervention may be necessary to repair the damaged nerve.
Nerve regeneration is the process of regrowth and restoration of functional nerve connections following damage or injury to the nervous system. This complex process involves various cellular and molecular events, such as the activation of support cells called glia, the sprouting of surviving nerve fibers (axons), and the reformation of neural circuits. The goal of nerve regeneration is to enable the restoration of normal sensory, motor, and autonomic functions impaired due to nerve damage or injury.
The phrenic nerve is a motor nerve that originates from the cervical spine (C3-C5) and descends through the neck to reach the diaphragm, which is the primary muscle used for breathing. The main function of the phrenic nerve is to innervate the diaphragm and control its contraction and relaxation, thereby enabling respiration.
Damage or injury to the phrenic nerve can result in paralysis of the diaphragm, leading to difficulty breathing and potentially causing respiratory failure. Certain medical conditions, such as neuromuscular disorders, spinal cord injuries, and tumors, can affect the phrenic nerve and impair its function.
Sciatic neuropathy is a condition that results from damage or injury to the sciatic nerve, which is the largest nerve in the human body. The sciatic nerve originates from the lower spine (lumbar and sacral regions) and travels down through the buttocks, hips, and legs to the feet.
Sciatic neuropathy can cause various symptoms, including pain, numbness, tingling, weakness, or difficulty moving the affected leg or foot. The pain associated with sciatic neuropathy is often described as sharp, shooting, or burning and may worsen with movement, coughing, or sneezing.
The causes of sciatic neuropathy include compression or irritation of the nerve due to conditions such as herniated discs, spinal stenosis, bone spurs, tumors, or piriformis syndrome. Trauma or injury to the lower back, hip, or buttocks can also cause sciatic neuropathy.
Diagnosing sciatic neuropathy typically involves a physical examination and medical history, as well as imaging tests such as X-rays, MRI, or CT scans to visualize the spine and surrounding structures. Treatment options may include pain management, physical therapy, steroid injections, or surgery, depending on the severity and underlying cause of the condition.
Neuralgia is a type of pain that occurs along the pathway of a nerve, often caused by damage or irritation to the nerve. It is typically described as a sharp, stabbing, burning, or electric-shock like pain that can be severe and debilitating. Neuralgia can affect any nerve in the body, but it most commonly occurs in the facial area (trigeminal neuralgia) or in the nerves related to the spine (postherpetic neuralgia). The pain associated with neuralgia can be intermittent or constant and may be worsened by certain triggers such as touch, temperature changes, or movement. Treatment for neuralgia typically involves medications to manage pain, as well as other therapies such as nerve blocks, surgery, or lifestyle modifications.
Trigeminal nerve injuries refer to damages or traumas affecting the trigeminal nerve, also known as the fifth cranial nerve. This nerve is responsible for sensations in the face and motor functions such as biting and chewing. Trigeminal nerve injuries can result in various symptoms depending on the severity and location of the injury, including:
1. Loss or reduction of sensation in the face, lips, gums, teeth, or tongue.
2. Pain, often described as burning, aching, or stabbing, in the affected areas.
3. Numbness or tingling sensations.
4. Difficulty with biting, chewing, or performing other motor functions.
5. Impaired taste sensation.
6. Headaches or migraines.
7. Eye dryness or excessive tearing.
Trigeminal nerve injuries can occur due to various reasons, such as trauma during facial surgeries, accidents, tumors, infections, or neurological conditions like multiple sclerosis. Treatment options depend on the cause and severity of the injury and may include medication, physical therapy, surgical intervention, or pain management strategies.
A lingual nerve injury refers to damage or trauma to the lingual nerve, which is a branch of the mandibular nerve (itself a branch of the trigeminal nerve). The lingual nerve provides sensation to the anterior two-thirds of the tongue and the floor of the mouth. It also contributes to taste perception on the front two-thirds of the tongue through its connection with the chorda tympani nerve.
Lingual nerve injuries can result from various causes, such as surgical procedures (e.g., dental extractions, implant placements, or third molar surgeries), pressure from tumors or cysts, or direct trauma to the mouth and tongue area. The injury may lead to symptoms like numbness, altered taste sensation, pain, or difficulty speaking and swallowing. Treatment for lingual nerve injuries typically involves a combination of symptom management and possible surgical intervention, depending on the severity and cause of the injury.
Nervous system trauma, also known as neurotrauma, refers to damage or injury to the nervous system, including the brain and spinal cord. This type of trauma can result from various causes, such as vehicular accidents, sports injuries, falls, violence, or penetrating traumas. Nervous system trauma can lead to temporary or permanent impairments in sensory, motor, or cognitive functions, depending on the severity and location of the injury.
Traumatic brain injury (TBI) is a common form of nervous system trauma that occurs when an external force causes brain dysfunction. TBIs can be classified as mild, moderate, or severe, based on factors such as loss of consciousness, memory loss, and neurological deficits. Mild TBIs, also known as concussions, may not cause long-term damage but still require medical attention to ensure proper healing and prevent further complications.
Spinal cord injuries (SCI) are another form of nervous system trauma that can have severe consequences. SCI occurs when the spinal cord is damaged due to a sudden, traumatic blow or cut, causing loss of motor function, sensation, or autonomic function below the level of injury. The severity and location of the injury determine the extent of impairment, which can range from partial to complete paralysis.
Immediate medical intervention is crucial in cases of nervous system trauma to minimize secondary damage, prevent complications, and optimize recovery outcomes. Treatment options may include surgery, medication, rehabilitation, or a combination of these approaches.
Laryngoscopy is a medical procedure that involves the examination of the larynx, which is the upper part of the windpipe (trachea), and the vocal cords using a specialized instrument called a laryngoscope. The laryngoscope is inserted through the mouth or nose to provide a clear view of the larynx and surrounding structures. This procedure can be performed for diagnostic purposes, such as identifying abnormalities like growths, inflammation, or injuries, or for therapeutic reasons, such as removing foreign objects or taking tissue samples for biopsy. There are different types of laryngoscopes and techniques used depending on the reason for the examination and the patient's specific needs.
Voice disorders are conditions that affect the quality, pitch, or volume of a person's voice. These disorders can result from damage to or abnormalities in the vocal cords, which are the small bands of muscle located in the larynx (voice box) that vibrate to produce sound.
There are several types of voice disorders, including:
1. Vocal cord dysfunction: This occurs when the vocal cords do not open and close properly, resulting in a weak or breathy voice.
2. Vocal cord nodules: These are small growths that form on the vocal cords as a result of excessive use or misuse of the voice, such as from shouting or singing too loudly.
3. Vocal cord polyps: These are similar to nodules but are usually larger and can cause more significant changes in the voice.
4. Laryngitis: This is an inflammation of the vocal cords that can result from a viral infection, overuse, or exposure to irritants such as smoke.
5. Muscle tension dysphonia: This occurs when the muscles around the larynx become tense and constricted, leading to voice changes.
6. Paradoxical vocal fold movement: This is a condition in which the vocal cords close when they should be open, causing breathing difficulties and a weak or breathy voice.
7. Spasmodic dysphonia: This is a neurological disorder that causes involuntary spasms of the vocal cords, resulting in voice breaks and difficulty speaking.
Voice disorders can cause significant impairment in communication, social interactions, and quality of life. Treatment may include voice therapy, medication, or surgery, depending on the underlying cause of the disorder.
A brain injury is defined as damage to the brain that occurs following an external force or trauma, such as a blow to the head, a fall, or a motor vehicle accident. Brain injuries can also result from internal conditions, such as lack of oxygen or a stroke. There are two main types of brain injuries: traumatic and acquired.
Traumatic brain injury (TBI) is caused by an external force that results in the brain moving within the skull or the skull being fractured. Mild TBIs may result in temporary symptoms such as headaches, confusion, and memory loss, while severe TBIs can cause long-term complications, including physical, cognitive, and emotional impairments.
Acquired brain injury (ABI) is any injury to the brain that occurs after birth and is not hereditary, congenital, or degenerative. ABIs are often caused by medical conditions such as strokes, tumors, anoxia (lack of oxygen), or infections.
Both TBIs and ABIs can range from mild to severe and may result in a variety of physical, cognitive, and emotional symptoms that can impact a person's ability to perform daily activities and function independently. Treatment for brain injuries typically involves a multidisciplinary approach, including medical management, rehabilitation, and supportive care.
The optic nerve, also known as the second cranial nerve, is the nerve that transmits visual information from the retina to the brain. It is composed of approximately one million nerve fibers that carry signals related to vision, such as light intensity and color, from the eye's photoreceptor cells (rods and cones) to the visual cortex in the brain. The optic nerve is responsible for carrying this visual information so that it can be processed and interpreted by the brain, allowing us to see and perceive our surroundings. Damage to the optic nerve can result in vision loss or impairment.
The hypoglossal nerve, also known as the 12th cranial nerve (CN XII), is primarily responsible for innervating the muscles of the tongue, allowing for its movement and function. These muscles include the intrinsic muscles that alter the shape of the tongue and the extrinsic muscles that position it in the oral cavity. The hypoglossal nerve also has some minor contributions to the innervation of two muscles in the neck: the sternocleidomastoid and the trapezius. These functions are related to head turning and maintaining head position. Any damage to this nerve can lead to weakness or paralysis of the tongue, causing difficulty with speech, swallowing, and tongue movements.
Nerve fibers are specialized structures that constitute the long, slender processes (axons) of neurons (nerve cells). They are responsible for conducting electrical impulses, known as action potentials, away from the cell body and transmitting them to other neurons or effector organs such as muscles and glands. Nerve fibers are often surrounded by supportive cells called glial cells and are grouped together to form nerve bundles or nerves. These fibers can be myelinated (covered with a fatty insulating sheath called myelin) or unmyelinated, which influences the speed of impulse transmission.
Deglutition is the medical term for swallowing. It refers to the process by which food or liquid is transferred from the mouth to the stomach through a series of coordinated muscle movements and neural responses. The deglutition process involves several stages, including oral preparatory, oral transit, pharyngeal, and esophageal phases, each of which plays a critical role in ensuring safe and efficient swallowing.
Dysphagia is the medical term for difficulty with swallowing, which can result from various underlying conditions such as neurological disorders, structural abnormalities, or muscular weakness. Proper evaluation and management of deglutition disorders are essential to prevent complications such as aspiration pneumonia, malnutrition, and dehydration.
Hoarseness is a condition characterized by an abnormal change in the quality of voice, making it sound rough, breathy, strained, or weak. Medically, it's described as a disorder of phonation, which is the process of producing sound by vibrating the vocal cords in the larynx (voice box). Hoarseness can be caused by various factors, such as inflammation, irritation, or injury to the vocal cords, and may result in symptoms like altered voice pitch, volume, and clarity. It's essential to consult a healthcare professional if hoarseness persists for more than two weeks, especially if it's accompanied by other concerning symptoms like difficulty swallowing or breathing.
The glossopharyngeal nerve, also known as the ninth cranial nerve (IX), is a mixed nerve that carries both sensory and motor fibers. It originates from the medulla oblongata in the brainstem and has several functions:
1. Sensory function: The glossopharyngeal nerve provides general sensation to the posterior third of the tongue, the tonsils, the back of the throat (pharynx), and the middle ear. It also carries taste sensations from the back one-third of the tongue.
2. Special visceral afferent function: The nerve transmits information about the stretch of the carotid artery and blood pressure to the brainstem.
3. Motor function: The glossopharyngeal nerve innervates the stylopharyngeus muscle, which helps elevate the pharynx during swallowing. It also provides parasympathetic fibers to the parotid gland, stimulating saliva production.
4. Visceral afferent function: The glossopharyngeal nerve carries information about the condition of the internal organs in the thorax and abdomen to the brainstem.
Overall, the glossopharyngeal nerve plays a crucial role in swallowing, taste, saliva production, and monitoring blood pressure and heart rate.
A reflex is an automatic, involuntary and rapid response to a stimulus that occurs without conscious intention. In the context of physiology and neurology, it's a basic mechanism that involves the transmission of nerve impulses between neurons, resulting in a muscle contraction or glandular secretion.
Reflexes are important for maintaining homeostasis, protecting the body from harm, and coordinating movements. They can be tested clinically to assess the integrity of the nervous system, such as the knee-j jerk reflex, which tests the function of the L3-L4 spinal nerve roots and the sensitivity of the stretch reflex arc.
Dysphonia is a medical term that refers to difficulty or discomfort in producing sounds or speaking, often characterized by hoarseness, roughness, breathiness, strain, or weakness in the voice. It can be caused by various conditions such as vocal fold nodules, polyps, inflammation, neurological disorders, or injuries to the vocal cords. Dysphonia can affect people of all ages and may impact their ability to communicate effectively, causing social, professional, and emotional challenges. Treatment for dysphonia depends on the underlying cause and may include voice therapy, medication, surgery, or lifestyle modifications.
Spinal cord injuries (SCI) refer to damage to the spinal cord that results in a loss of function, such as mobility or feeling. This injury can be caused by direct trauma to the spine or by indirect damage resulting from disease or degeneration of surrounding bones, tissues, or blood vessels. The location and severity of the injury on the spinal cord will determine which parts of the body are affected and to what extent.
The effects of SCI can range from mild sensory changes to severe paralysis, including loss of motor function, autonomic dysfunction, and possible changes in sensation, strength, and reflexes below the level of injury. These injuries are typically classified as complete or incomplete, depending on whether there is any remaining function below the level of injury.
Immediate medical attention is crucial for spinal cord injuries to prevent further damage and improve the chances of recovery. Treatment usually involves immobilization of the spine, medications to reduce swelling and pressure, surgery to stabilize the spine, and rehabilitation to help regain lost function. Despite advances in treatment, SCI can have a significant impact on a person's quality of life and ability to perform daily activities.
Axotomy is a medical term that refers to the surgical cutting or severing of an axon, which is the long, slender projection of a neuron (nerve cell) that conducts electrical impulses away from the cell body and toward other cells. Axons are a critical component of the nervous system, allowing for communication between different parts of the body.
Axotomy is often used in research settings to study the effects of axonal injury on neuronal function and regeneration. This procedure can provide valuable insights into the mechanisms underlying neurodegenerative disorders and potential therapies for nerve injuries. However, it is important to note that axotomy can also have significant consequences for the affected neuron, including changes in gene expression, metabolism, and overall survival.
Hyperalgesia is a medical term that describes an increased sensitivity to pain. It occurs when the nervous system, specifically the nociceptors (pain receptors), become excessively sensitive to stimuli. This means that a person experiences pain from a stimulus that normally wouldn't cause pain or experiences pain that is more intense than usual. Hyperalgesia can be a result of various conditions such as nerve damage, inflammation, or certain medications. It's an important symptom to monitor in patients with chronic pain conditions, as it may indicate the development of tolerance or addiction to pain medication.
"Cat" is a common name that refers to various species of small carnivorous mammals that belong to the family Felidae. The domestic cat, also known as Felis catus or Felis silvestris catus, is a popular pet and companion animal. It is a subspecies of the wildcat, which is found in Europe, Africa, and Asia.
Domestic cats are often kept as pets because of their companionship, playful behavior, and ability to hunt vermin. They are also valued for their ability to provide emotional support and therapy to people. Cats are obligate carnivores, which means that they require a diet that consists mainly of meat to meet their nutritional needs.
Cats are known for their agility, sharp senses, and predatory instincts. They have retractable claws, which they use for hunting and self-defense. Cats also have a keen sense of smell, hearing, and vision, which allow them to detect prey and navigate their environment.
In medical terms, cats can be hosts to various parasites and diseases that can affect humans and other animals. Some common feline diseases include rabies, feline leukemia virus (FeLV), feline immunodeficiency virus (FIV), and toxoplasmosis. It is important for cat owners to keep their pets healthy and up-to-date on vaccinations and preventative treatments to protect both the cats and their human companions.
Athletic injuries are damages or injuries to the body that occur while participating in sports, physical activities, or exercise. These injuries can be caused by a variety of factors, including:
1. Trauma: Direct blows, falls, collisions, or crushing injuries can cause fractures, dislocations, contusions, lacerations, or concussions.
2. Overuse: Repetitive motions or stress on a particular body part can lead to injuries such as tendonitis, stress fractures, or muscle strains.
3. Poor technique: Using incorrect form or technique during exercise or sports can put additional stress on muscles, joints, and ligaments, leading to injury.
4. Inadequate warm-up or cool-down: Failing to properly prepare the body for physical activity or neglecting to cool down afterwards can increase the risk of injury.
5. Lack of fitness or flexibility: Insufficient strength, endurance, or flexibility can make individuals more susceptible to injuries during sports and exercise.
6. Environmental factors: Extreme weather conditions, poor field or court surfaces, or inadequate equipment can contribute to the risk of athletic injuries.
Common athletic injuries include ankle sprains, knee injuries, shoulder dislocations, tennis elbow, shin splints, and concussions. Proper training, warm-up and cool-down routines, use of appropriate protective gear, and attention to technique can help prevent many athletic injuries.
 Recurrent laryngeal nerve
Recurrent laryngeal nerve
Ortner's syndrome
Posterior cricoarytenoid muscle
Superior laryngeal nerve
Larynx
Thyroidectomy
Vocal cord paresis
Tracheotomy
Lung surgery
Hyperthyroidism
Thyroid disease
Clement Price Thomas
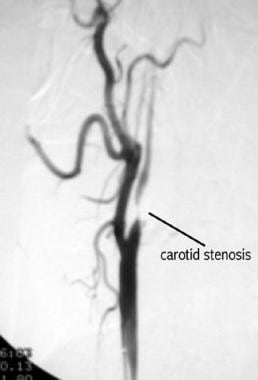
Carotid endarterectomy
Superior thyroid artery
Inferior thyroid artery
Double aortic arch
Thoracic aorta injury
Graves' disease
Bolam v Friern Hospital Management Committee
Amelita Galli-Curci
History of neurology and neurosurgery
Hoarse voice
Glossary of communication disorders
Ventral slot
Endoscopic laser cordectomy
Flexible Endoscopic Evaluation of Swallowing with Sensory Testing
Interrupted aortic arch
Trachea
Central pattern generator
Mediastinum
Vesalius Clinical Folios: Laryngeal Nerve Injury
 Recurrent laryngeal nerve injury - OpenAnesthesia
Recurrent laryngeal nerve injury - OpenAnesthesia
 Laryngeal nerve damage: MedlinePlus Medical Encyclopedia
Laryngeal nerve damage: MedlinePlus Medical Encyclopedia
 Management of Recurrent Laryngeal Nerve Injury | RGS Health
Management of Recurrent Laryngeal Nerve Injury | RGS Health
Recurrent laryngeal nerve - Wikipedia
 Complications of Thyroid Surgery: Practice Essentials, Overview, Bleeding
Complications of Thyroid Surgery: Practice Essentials, Overview, Bleeding
 Effects of early local administration of high-dose bFGF on a recurrent laryngeal nerve injury model | Journal of Otolaryngology...
Effects of early local administration of high-dose bFGF on a recurrent laryngeal nerve injury model | Journal of Otolaryngology...
 Iatrogenic bilateral recurrent laryngeal nerve injury: a retrospective study
| International Journal of...
Iatrogenic bilateral recurrent laryngeal nerve injury: a retrospective study
| International Journal of...
 Recurrent Laryngeal Nerve Injury Near the Nerve Entry Point in Total Endoscopic Thyroidectomy: A Retrospective Cohort Study -...
Recurrent Laryngeal Nerve Injury Near the Nerve Entry Point in Total Endoscopic Thyroidectomy: A Retrospective Cohort Study -...
 ATSDR - Oak Ridge Reservation - ORRHES Meeting Minutes
ATSDR - Oak Ridge Reservation - ORRHES Meeting Minutes
Hurthle Cell Carcinoma (Oncocytic Carcinoma) Treatment & Management: Medical Care, Surgical Care, Consultations
Atherosclerotic Disease of the Carotid Artery: Practice Essentials, Background, Anatomy
 Laryngeal nerve damage Information | Mount Sinai - New York
Laryngeal nerve damage Information | Mount Sinai - New York
 Thyroid | Centro Médico Teknon
Thyroid | Centro Médico Teknon
 Carolyn Dacey Seib, MD, MAS | Stanford Medicine
Carolyn Dacey Seib, MD, MAS | Stanford Medicine
 Accessories and Instruments for the NIM® 3.0 Nerve Monitoring Systems From Medtronic
Accessories and Instruments for the NIM® 3.0 Nerve Monitoring Systems From Medtronic
Hyperparathyroidism: Practice Essentials, Anatomy and Embryology, Primary Hyperparathyroidism
 RACGP - Thyroid disease Long term management of hyperthyroidism and hypothyroidism
RACGP - Thyroid disease Long term management of hyperthyroidism and hypothyroidism
 Amniotic Nerve Shield Decreases Vocal Cord Nerve Injury During Thyroid / Parathyroid Surgery
Amniotic Nerve Shield Decreases Vocal Cord Nerve Injury During Thyroid / Parathyroid Surgery
 Jason T. Rich, MD - Otolaryngology-Head & Neck Surgery
Jason T. Rich, MD - Otolaryngology-Head & Neck Surgery
 PPT - THYROID NODULES PowerPoint Presentation, free download - ID:2318535
PPT - THYROID NODULES PowerPoint Presentation, free download - ID:2318535
 Thyroid Surgery Cost in India by best ENT Surgeons | IndiCure
Thyroid Surgery Cost in India by best ENT Surgeons | IndiCure
 Vocal cord dysfunction in two patients after mitral valve replacement: consequences and mechanism. - Amrita Vishwa Vidyapeetham
Vocal cord dysfunction in two patients after mitral valve replacement: consequences and mechanism. - Amrita Vishwa Vidyapeetham
Internet Scientific Publications
 head and neck, endocrine and breast Flashcards by Bryce Haac | Brainscape
head and neck, endocrine and breast Flashcards by Bryce Haac | Brainscape
How Long Does a Supraclavicular Nerve Block Last? - Hdkino.org
 Clinical Characteristics of Recurrent Nasopharyngeal Carcinoma in High-Incidence Area
Clinical Characteristics of Recurrent Nasopharyngeal Carcinoma in High-Incidence Area
 Infrared neural stimulation markedly enhances nerve functionality assessment during nerve monitoring | Scientific Reports
Infrared neural stimulation markedly enhances nerve functionality assessment during nerve monitoring | Scientific Reports
Aintree - Ambulatory thyroidectomy: An anesthesiologist's perspective - Aintree and Walton Research
Larynx15
- The larynx is supported by a semi-rigid framework of cartilages (see laryngeal anatomy ). (vesalius.com)
- The recurrent laryngeal nerve (RLN) is a branch of the vagus nerve (cranial nerve X) that supplies all the intrinsic muscles of the larynx, with the exception of the cricothyroid muscles. (wikipedia.org)
- The recurrent laryngeal nerves supply sensation to the larynx below the vocal cords, give cardiac branches to the deep cardiac plexus, and branch to the trachea, esophagus and the inferior constrictor muscles. (wikipedia.org)
- The vagus nerves run down into the thorax, and the recurrent laryngeal nerves run up to the larynx. (wikipedia.org)
- 19 Unlike the other nerves supplying the larynx, the right and left RLNs lack bilateral symmetry. (wikipedia.org)
- These anastomoses include nerve connections between the superior laryngeal nerve (SLN) and RLN in the larynx. (biomedcentral.com)
- The Nerves of the Human Larynx. (ijorl.com)
- Damage to the nerves of the larynx can cause hoarseness, difficulty in swallowing or breathing, or the loss of voice. (mountsinai.org)
- Head anatomy1) Trigeminal nervea-branchesb-actions2) Facial nervea-branchesb-actions3) Glossopharyngeal nervea-actionsb-what does injury affect4) hypoglossal nervea-actionsb-findings in hypoglossal nerve injury5) recurrent laryngeal nerve- innervates all of larynx except what muscle? (brainscape.com)
- Several nerves in the larynx control these tasks. (medscape.com)
- The vagus nerves innervates the larynx. (medscape.com)
- The nerve provides sensation of the base of tongue, both surfaces of epiglottis, the aryepiglottic folds, and the vestibule of the larynx to the level of the vocal folds. (medscape.com)
- The left vocal cord is paralyzed more often than the right because the left recurrent nerve takes a longer course from the brain stem to the larynx, providing more opportunity for compression, traction, or surgical injuries. (msdmanuals.com)
- Overview of Laryngeal Disorders The larynx contains the vocal cords and serves as the opening to the tracheobronchial tree. (msdmanuals.com)
- The surgeon finds and takes care not to injure the parathyroid glands and the nerve which is attached to your larynx (voice box). (pdfdrugs.com)
Vagus nerve12
- Fibers cross over to and join the vagus nerve in the jugular foramen. (wikipedia.org)
- 86-88 Parasympathetic fibers to segments of the trachea and esophagus in the neck originate in the dorsal nucleus of the vagus nerve. (wikipedia.org)
- 318-323 In roughly 1 out of every 100-200 people, the right inferior laryngeal nerve is nonrecurrent, branching off the vagus nerve around the level of the cricoid cartilage. (wikipedia.org)
- Even experienced surgeons find it difficult to visually identify the recurrent laryngeal nerve (RLN) or vagus nerve during thyroid surgery and other neck dissections. (medtronic.com)
- Two sensory ganglia are associated with the vagus nerve: (1) superior (jugular) ganglion and (2) inferior (nodosum) ganglion. (medscape.com)
- Exiting the jugular foramen, the vagus nerve enlarges into the inferior (nodosum) ganglion. (medscape.com)
- In the neck, the vagus nerve lies posterior to, and in a groove between, the internal jugular vein and the internal carotid artery (see the image below). (medscape.com)
- Vagus Nerve Injuries" is a descriptor in the National Library of Medicine's controlled vocabulary thesaurus, MeSH (Medical Subject Headings) . (jefferson.edu)
- Traumatic injuries to the VAGUS NERVE. (jefferson.edu)
- Because the vagus nerve innervates multiple organs, injuries in the nerve fibers may result in any gastrointestinal organ dysfunction downstream of the injury site. (jefferson.edu)
- This graph shows the total number of publications written about "Vagus Nerve Injuries" by people in this website by year, and whether "Vagus Nerve Injuries" was a major or minor topic of these publications. (jefferson.edu)
- Below are the most recent publications written about "Vagus Nerve Injuries" by people in Profiles. (jefferson.edu)
Cervical9
- 1 The VCD can occur because of direct trauma after endotracheal intubation or it can be secondary to damage to the recurrent laryngeal nerve (RLN) in its cervical or intrathoracic course. (amrita.edu)
- 1) takes omohyoid, submandibular gland, sensory nerves C2-C5, cervical branch of facial nerve, and ipsilateral thyroid2) same as above + accessory nerve (CN XII), SCM, and internal jugular resection. (brainscape.com)
- These include cervical hematoma, bilateral recurrent laryngeal nerve injury and symptomatic hypocalcemia. (edgehill.ac.uk)
- Cervical radiculopathy is a clinical diagnosis defined by the presence of sensory or motor deficits and complaints caused by mechanical compression of the corresponding cervical nerve root. (biomedcentral.com)
- Another less common surgical cause for post-thyroidectomy voice change may be cervical strap muscle injury. (guidelinecentral.com)
- In operative births (cases where instruments were used), traumatic cranial and cervical spine injuries are still occurring. (abclawcenters.com)
- 2017. A Multicenter Review of Superior Laryngeal Nerve Injury Following Anterior Cervical Spine Surgery. . (cornell.edu)
- Hypoglossal Nerve Palsy After Cervical Spine Surgery. (cornell.edu)
- Their previous work suggested that by transferring a cervical spinal nerve from the unaffected side to the paralyzed side, a paralyzed hand could be functionally connected to the unimpaired cerebral hemisphere. (medscape.com)
Recurrent laryngeal nerve2
- Lo C, Kwok F, Yuen P. A prospective evaluation of recurrent laryngeal nerve paralysis during thyroidectomy. (medtronic.com)
- In recurrent laryngeal nerve paralysis, the cord may move with phonation but not with inspiration. (msdmanuals.com)
Bilateral8
- Bilateral recurrent laryngeal nerve injury is mostly iatrogenic following thyroidectomy. (ijorl.com)
- Our study aims at defining need for tracheostomy, timing of intervention and best method to achieve permanent treatment in cases of iatrogenic bilateral recurrent laryngeal nerve. (ijorl.com)
- 5 patients developed bilateral recurrent laryngeal nerve injury, of which 3 were multi nodular goiter cases and papillary carcinoma thyroid 2 cases. (ijorl.com)
- 5 out of 34 (14.7%) patients developed bilateral recurrent laryngeal nerve injury. (ijorl.com)
- 1 patient had bilateral abductor paresis and 1 patient had all bilateral recurrent laryngeal nerve and superior laryngeal nerve injury causing combined paralysis of vocal cord. (ijorl.com)
- In bilateral recurrent laryngeal nerve injury, Tracheostomy to be done if airway is compromised. (ijorl.com)
- A size 3 laryngeal mask airway was placed easily, with bilateral equal breath sounds. (ispub.com)
- The other nerves of major interest, and frequently less directly addressed during thyroid surgery, are the bilateral superior laryngeal nerves (SLN), injury to which can impair the ability to change pitch and reduce voice projection. (guidelinecentral.com)
Palsy8
- Recurrent nerve palsy after thyroid operations-principal nerve identification and a literature review. (ijorl.com)
- Recurrent laryngeal nerve injury (RLNI) is one of the common complications of thyroidectomy, which can lead to postoperative vocal cord palsy (VCP). (axisneuromonitoring.com)
- These include sore throat, laryngeal nerve palsy, lingual nerve palsy, alteration of taste/swallowing/ speech, rarely tongue cyanosis or tongue cyanosis with swelling. (ispub.com)
- Patient safety was monitored according to two indicators, which are immediately recognisable postoperative complications: recurrent laryngeal nerve palsy and hypocalcaemia. (bmj.com)
- The overall proportions of immediate recurrent laryngeal nerve palsy and hypocalcaemia were 7.4% and 20.5%, respectively. (bmj.com)
- The patients had hemiplegia due to a stroke, traumatic brain injury , cerebral palsy, or encephalitis, manifesting mainly as spasticity and weakness in the upper extremity contralateral to the cerebral lesion. (medscape.com)
- Cerebral palsy (CP) is characterized by nonprogressive brain injury, the most common cause of child disability. (bvsalud.org)
- Cerebral palsy (CP) is a general term that includes very different clinical manifestations that have in common motor difficulty due to a brain injury. (bvsalud.org)
Paralysis6
- Recurrent laryngeal nerve (RLN) injury results in true vocal-fold paresis or paralysis. (medscape.com)
- We previously reported that local administration of bFGF 1 month after recurrent laryngeal nerve (RLN) paralysis compensated for atrophy of the thyroarytenoid muscle. (biomedcentral.com)
- Unilateral vocal fold paralysis (UVFP) is caused by recurrent laryngeal nerve (RLN) dysfunction, including vagal nerve disorders. (biomedcentral.com)
- Vocal cord paralysis may result from lesions or dysfunction at the level of the nucleus ambiguus, its supranuclear tracts, the main trunk of the vagus, or the recurrent laryngeal nerves. (msdmanuals.com)
- In this single-center trial involving patients who had had unilateral arm paralysis due to chronic cerebral injury for more than 5 years, transfer of the C7 nerve from the nonparalyzed side to the side of the arm that was paralyzed was associated with a greater improvement in function and reduction of spasticity than rehabilitation alone over a period of 12 months," they conclude. (medscape.com)
- Spastic limb paralysis due to a stroke or other injury to the cerebral hemisphere causes long-term disability. (medscape.com)
Surgery26
- Potential major complications of thyroid surgery include bleeding, injury to the recurrent laryngeal nerve (see the first image below), hypoparathyroidism, hypothyroidism, thyrotoxic storm, injury to the superior laryngeal nerve (see the second image below), and infection. (medscape.com)
- Patients with pathological laryngeal electromyographic findings at least two months after the paresis need laryngeal framework surgery. (ijorl.com)
- Lamadé W, Renz K, Willeke F, Klar E, Herfarth C. Effect of training on the incidence of nerve damage in thyroid surgery. (ijorl.com)
- In thyroid surgery, the incidence of RLNI can be reduced by routine visual identification of the recurrent laryngeal nerve (RLN). (axisneuromonitoring.com)
- Why monitor the recurrent laryngeal nerve in thyroid surgery? (medtronic.com)
- Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. (medtronic.com)
- Dralle H. Intraoperative monitoring of the recurrent laryngeal nerve in thyroid surgery. (medtronic.com)
- New method may improve nerve healing after thyroid surgery. (parathyroid.com)
- The Recurrent Laryngeal Nerve Shield is the most important development in thyroid surgery in 50 years" Dr Gary Clayman. (parathyroid.com)
- But now there is something that can be done to potentially decrease the chance of a vocal cord nerve injury after thyroid and parathyroid surgery! (parathyroid.com)
- Dr Norman came up with the idea of using a piece of this membrane a few years ago to protect the vocal cord nerve (recurrent laryngeal nerve) and the normal parathyroid glands during thyroid and parathyroid surgery. (parathyroid.com)
- Several companies make human amniotic tissue available to use in surgery but nobody has used amnion/chorion before to see if it would shield and protect the vocal cord nerve from injury following thyroid and parathyroid surgery. (parathyroid.com)
- He has experience performing functional endoscopic sinus surgery (FESS), balloon sinuplasty, orbital decompression, optic nerve decompression, dacryocystorhinostomy (DCR), endoscopic closure of CSF leaks, and endoscopic pituitary tumor surgery, among other endoscopic nasal and sinus surgical procedures. (indicure.com)
- Supraclavicular nerve block performed before surgery and for post-surgical pain may involve hospitalization for a day or two, depending on the complexity of the surgery. (hdkino.org)
- Moreover, INIs are also a common source of medicolegal litigation with 60% of INI complications during thyroid surgery leading to malpractice lawsuits and 82% of cases of spinal accessory nerve injury resulting in patient compensation 17 , 18 . (nature.com)
- IONM seeks to preserve peripheral nerve function through electrical stimulation (ES) of at risk nerves throughout surgery and examining any changes in the amplitude and latency of the evoked signals that are indicative of damage. (nature.com)
- Prof. Gregory Randolph, Advances in prevention of recurrent laryngeal nerve injury during thyroid cancer surgery. (worldinfo.org)
- About 1 in 10 patients experience temporary laryngeal nerve injury after surgery, with longer lasting voice problems in ≤1 in 25. (guidelinecentral.com)
- Management of cranial nerve injury following surgery of the skull base. (jefferson.edu)
- Recurrent laryngeal nerve injury is a common complication of thyroid surgery that can cause communication disorders, aspiration, and swallowing difficulties. (ijthyroid.org)
- Only recently has increased awareness of the importance of voice outcomes in thyroid surgery led to the publication of a number of important papers on this topic, with several professional organizations starting to make reference to voice and laryngeal function in their guidelines for best practice. (elsevierpure.com)
- This chapter will discuss indications for laryngeal examination in thyroid surgery and current techniques available for voice and laryngeal examination. (elsevierpure.com)
- Laryngeal masks as airway management in major urological surgery - a safe alternative? (lmaco.com)
- If "bruised", the nerve does not work properly after surgery but recovers and returns to normal during the next few days or weeks. (pdfdrugs.com)
- Laryngeal injuries from intubation during surgery are believed to be confined to minor injuries. (slprandr.com)
- The patients were randomly assigned to undergo contralateral C7 nerve-transfer surgery followed by rehabilitation (n = 18) or to rehabilitation alone (n = 18). (medscape.com)
Main trunk of the vagus1
- The superior laryngeal nerve (SLN) branches from the main trunk of the vagus high in the neck. (medscape.com)
Thyroidectomy1
- The external branch of the SLN is vulnerable to injury during thyroidectomy as the surgeon dissects and ligates the superior thyroid vascular pedicle, especially for Cernea type 2b nerves. (medscape.com)
Innervates1
- An extension of the external superior laryngeal nerve that innervates the vocal cord. (ijorl.com)
Damage13
- Laryngeal nerve damage is injury to one or both of the nerves that cause the voice box to function. (medlineplus.gov)
- However, an experiment was conducted on a 44-year-old woman to improve symptoms of nerve damage. (rgshealthcare.com)
- Treatment depends on the cause and extent of the laryngeal nerve damage. (mountsinai.org)
- Damage to the laryngeal nerve can result in loss of voice or obstruction to breathing. (mountsinai.org)
- This membrane "shields" the nerve from further damage and promotes rapid healing. (parathyroid.com)
- However, a literature review of complication following the use of LMA's found reports of damage not only to recurrent laryngeal nerve but also to other adjacent nerves namely the hypoglossal and lingual nerve 3 . (ispub.com)
- In surgical procedures where the risk of accidental nerve damage is prevalent, surgeons commonly use electrical stimulation (ES) during intraoperative nerve monitoring (IONM) to assess a nerve's functional integrity. (nature.com)
- By assessing nerve functionality throughout a surgical procedure, the risk of INI is greatly reduced and timely interventions can be made if damage occurs. (nature.com)
- Currently, nerve auto-grafting is the gold standard for the treatment of recurrent laryngeal nerve damage. (ijthyroid.org)
- Nerve guide conduits are being increasingly considered as potential alternatives to nerve auto-grafts in the treatment of recurrent laryngeal nerve damage. (ijthyroid.org)
- Permanent damage to one of these nerves (risk 1:100) causes a hoarse, croaky and weak voice. (pdfdrugs.com)
- Permanent damage to both nerves is very rare but is a serious problem that may have to be treated by putting a permanent tracheostomy (breathing tube) into the windpipe in the neck. (pdfdrugs.com)
- Damage to one of these nerves results in a weak voice, although the sound of the voice in unchanged. (pdfdrugs.com)
Mask airway4
- We present a case report of a patient who developed cyanosis of the tongue during anesthesia using the laryngeal mask airway. (ispub.com)
- We are describing a case of tongue cyanosis after laryngeal mask airway insertion. (ispub.com)
- The laryngeal mask airway cuff was inflated with 20 ml air. (ispub.com)
- We believe that in our case the laryngeal mask airway was occluding the patients' lingual artery bilaterally. (ispub.com)
Superior14
- The nerve of the fourth arch gives rise to the superior laryngeal nerve. (wikipedia.org)
- 10, 48 In about four people out of five, there is a connecting branch between the inferior laryngeal nerve, a branch of the RLN, and the internal laryngeal nerve, a branch of the superior laryngeal nerve. (wikipedia.org)
- Superior laryngeal nerve (SLN). (medscape.com)
- Hydman J, Mattsson P. Collateral reinnervation by the superior laryngeal nerve after recurrent laryngeal nerve injury. (ijorl.com)
- Anatomy of the superior laryngeal nerve (SLN), left lateral view. (medscape.com)
- Right lateral view of the superior and recurrent laryngeal nerves. (medscape.com)
- Also passing through this foramen is the superior laryngeal artery. (medscape.com)
- Right lateral view of the superior and recurrent laryngeal nerve with the thyroid lamina removed. (medscape.com)
- Several cadaveric studies have shown that the nerve runs below the superior border of the thyroid gland in 40% of cases, with recent clinical studies confirming that the nerves most commonly course in this inferior, Cernea type 2b, position. (medscape.com)
- Thyroids that are larger than 50 grams or those with larger dimensions are correlated with nerves that run below the superior border of the thyroid gland. (medscape.com)
- In most cases, postoperative hoarseness is due to recurrent laryngeal nerve (RLN) injury, although injury to the external branch of the superior laryngeal nerve (EBSLN) can also result in significant vocal issues, including diminished vocal projection and inability to attain higher vocal registers. (elsevierpure.com)
- In The Recurrent and Superior Laryngeal Nerves (pp. 17-29). (elsevierpure.com)
- The external branch of the superior laryngeal nerve travels close to the vessels feeding the thyroid gland. (pdfdrugs.com)
- The surgical technique used in the study involves making an incision at the superior aspect of the sternum, mobilizing the donor C7 nerve on the nonparalyzed side, sectioning it as distally as possible but proximal to the point at which it combines with other nerves, and routing it between the spinal column and esophagus. (medscape.com)
Neck3
- 930-931 The vagus nerves, from which the recurrent laryngeal nerves branch, exit the skull at the jugular foramen and travel within the carotid sheath alongside the carotid arteries through the neck. (wikipedia.org)
- In an interscalene block, the injection is administered in the neck, closer to the nerve roots. (hdkino.org)
- Any operation on the neck can produce some change in the voice even when there is no injury to the nerves controlling movement of the vocal cords. (pdfdrugs.com)
Complications1
- There are few case reports of complications associated with the use of laryngeal mask airways LMA\'s. (ispub.com)
Endotracheal intubation1
- The purposes of this systematic review are to (1) evaluate the nature and severity of laryngeal injury after endotracheal intubation in ICU patients and (2) identify areas of inquiry for mitigation strategies and future intervention. (slprandr.com)
Inferior3
- The terminal branch is called the inferior laryngeal nerve. (wikipedia.org)
- A left nonrecurrent inferior laryngeal nerve is even more uncommon, requiring the aortic arch be on the right side, accompanied by an arterial variant which prevents the nerve from being drawn into the chest by the left subclavian. (wikipedia.org)
- In approximately 20% of individuals, the external branch is under the inferior constrictor muscle and cannot be visualized, but it can be stimulated using a nerve probe. (medscape.com)
Reinnervation2
- Considering that reinnervation of the TA muscle can occur even after UVFP through these anastomoses, it would be ideal if drugs that promote nerve regeneration could be used to treat UVFP. (biomedcentral.com)
- Intrinsic laryngeal muscle reinnervation using the muscle-nerve-muscle technique. (wustl.edu)
Anatomy2
- Anatomy of the recurrent laryngeal nerve (RLN). (medscape.com)
- Chapter 25: Surgical Anatomy of the Recurrent Laryngeal Nerve (p316). (medtronic.com)
Intubation1
- By comparison, critically ill patients intubated in ICU generally experience longer intubation resulting in laryngeal injuries that are more prevalent, potentially more severe, frequently overlooked, and often result in voice dysfunction (i.e., dysphonia) and/or swallowing dysfunction (i.e., dysphagia). (slprandr.com)
Hypoglossal nerve1
- This then joins the sublingual vein and passes with the hypoglossal nerve between hypoglossus and mylohyoid muscles to drain into the internal jugular, facial, or lingual vein. (ispub.com)
Nonrecurrent1
- The most common site of neural injury is the distal recurrent laryngeal nerve (RLN), which can be nonrecurrent in 0.5%-0.7% of cases (See figures below). (guidelinecentral.com)
Airway management1
- Nonsurgical causes may include laryngeal irritation, edema, or injury from airway management. (guidelinecentral.com)
Pharyngeal2
- The recurrent laryngeal nerves are the nerves of the sixth pharyngeal arch. (wikipedia.org)
- 1346-1347 The somatic motor fibers that innervate the laryngeal muscles, and pharyngeal muscles are located in the nucleus ambiguus and emerge from the medulla in the cranial root of the accessory nerve. (wikipedia.org)
Branch4
- Additionally, the nerves are among the few nerves that follow a recurrent course, moving in the opposite direction to the nerve they branch from, a fact from which they gain their name. (wikipedia.org)
- the term "recurrent" from Latin: re- (back) and currere (to run), indicates they run in the opposite direction to the vagus nerves from which they branch. (wikipedia.org)
- The recurrent laryngeal nerves branch off the vagus, the left at the aortic arch, and the right at the right subclavian artery. (wikipedia.org)
- Secretomotor fibers are also in the internal laryngeal branch of the SLN. (medscape.com)
Parathyroid1
- Injury to the recurrent laryngeal nerve (vocal cord nerve injury) is the biggest worry people have when they are told they need to have a thyroid or parathyroid operation. (parathyroid.com)
Fibers2
- In the medulla, the vagal fibers are connected to 4 nuclei: (1) spinal nucleus of the trigeminal nerve, (2) nucleus of the tractus solitarius, (3) nucleus ambiguus, and (4) dorsal vagal motor nucleus. (medscape.com)
- The C7 spinal nerve, one of five that give rise to the brachial plexus, contains thousands of nerve fibers. (medscape.com)
Thyroid gland1
- Cernea type 1 nerves cross greater than 1 cm above the upper border of the thyroid gland. (medscape.com)
Esophagus4
- After branching, the nerves typically ascend in a groove at the junction of the trachea and esophagus. (wikipedia.org)
- Electrocautery or ultrasonic dissectors should be used very sparingly in the region of the distal esophagus and the mediastinum to avoid injury. (sls.org)
- To investigate a potential esophageal injury, methylene blue can be placed into the distal esophagus via nasogastric tube, or an intraoperative upper endoscopy with air insufflation with the esophagus underwater can be performed. (sls.org)
- 1 At our centers, intraoperative endoscopy is a very sensitive and effective technique for identification of mucosal injury and adequate insufflation of the distal esophagus and is routinely used. (sls.org)
Patients5
- We began using the amniotic membrane on patients who had a thyroid cancer operation where the recurrent laryngeal nerve (vocal cord nerve) was completely dissected and exposed--and therefore at high risk for having a loss of voice post op. (parathyroid.com)
- We were amazed that the incidence of vocal cord injury and loss of voice went to zero in our first 50 patients. (parathyroid.com)
- We studied these tissues on vocal cord nerves in our patients and tried tissues that had amnion alone or amnion with chorion and the results were hugely different, with the membrane containing the chorion being much better. (parathyroid.com)
- However, recommendations in these guidelines vary, especially with regard to laryngeal examination for patients without voice impairments, with many surgeons using voice symptoms alone to guide the need for laryngeal examination. (elsevierpure.com)
- Transferring the C7 nerve from the nonparalyzed to the paralyzed side in patients with a stroke or other cerebral injury resulted in improved function and reduced spasticity in the affected arm, new research has shown. (medscape.com)
Resection1
- Hydman J, Svensson M, Kuylenstierna R, Ohlsson M, Mattsson P. Neuronal survival and glial reactions after recurrent laryngeal nerve resection in the rat. (ijorl.com)
Muscles1
- The posterior cricoarytenoid muscles, the only muscles that can open the vocal folds, are innervated by this nerve. (wikipedia.org)
Trauma3
- Laryngeal and esophageal trauma. (medlineplus.gov)
- C-section deliveries that are performed electively at 39 weeks reduce the risk of neonatal encephalopathy , permanent brachial plexus injury, physical trauma to the baby, long-term neurologic impairment, intrapartum death and intrauterine fetal demise. (abclawcenters.com)
- Objetivo: Generar recomendaciones basadas en la mejor evidencia disponible acerca del manejo de personas con trauma ocular. (bvsalud.org)
Uncommon1
- Injury to the laryngeal nerves is uncommon. (medlineplus.gov)
Edema1
- Death, if it occurs, usually results from airway obstruction caused by laryngeal edema or bronchospasm and may be associated with cardiovascular collapse. (cdc.gov)
Surgical2
- Our nerve monitoring products and accessories can be used in conjunction with NIM ® Nerve Monitoring Systems during a variety of surgical procedures. (medtronic.com)
- This narrative review describes the main applications of de la ultrasonografía en ultrasound in anesthesia, ultrasound-guided techniques, and current trends in the perioperative anesthetic management of anestesia the surgical patient. (bvsalud.org)
Brachial4
- An anesthetic injection is administered in the area above the collarbone (clavicle) close to the network of nerves (brachial plexus) that provides sensation to the upper extremities. (hdkino.org)
- A supraclavicular nerve block is the quickest and most effective block for the entire arm because the nerves are tightly packed in the targeted anatomical region (brachial plexus). (hdkino.org)
- Shoulder dystocia often causes brachial plexus, an injury to the nerves that control the shoulder, arm, hands and fingers. (abclawcenters.com)
- Brachial neuritis is defined as dysfunction limited to the upper extremity nerve plexus (i.e., its trunks, division, or cords) without involvement of other peripheral (e.g., nerve roots or a single peripheral nerve) or central (e.g., spinal cord) nervous system structures. (cdc.gov)
Symptoms2
- Diagnosis of INI is largely dependent on the surgeons' awareness of the injury and its symptoms that develop postoperatively 19 . (nature.com)
- True laryngeal function may be inaccurately predicted by voice symptoms, and thus controversy remains regarding need for routine laryngeal examination, timing of any such examination, and optimal examination technique(s). (elsevierpure.com)
Sensation1
- A supraclavicular nerve block is a procedure to block the sensation in the arm below the shoulder. (hdkino.org)
Intraoperative nerve2
- Studies show that the rate of RLN injury is under-estimated 1-6 and intraoperative nerve monitoring of the RLN is recommended as a risk-minimizing tool. (medtronic.com)
- NIM ® EMG Tubes provide an open airway for patient ventilation and intraoperative nerve monitoring of both vocal cords. (medtronic.com)
Phrenic nerve1
- This approach also carries less chances of blocking the phrenic nerve, which is responsible for the diaphragm 's function that is crucial for breathing . (hdkino.org)
Jugular foramen1
- This nerve emerges from the medulla of the brain stem and exits the skull through the jugular foramen. (medscape.com)