Mediastinal Emphysema
Pulmonary Emphysema
Barotrauma
Atmospheric Pressure
Encyclopedias as Topic
Pressure
Diving
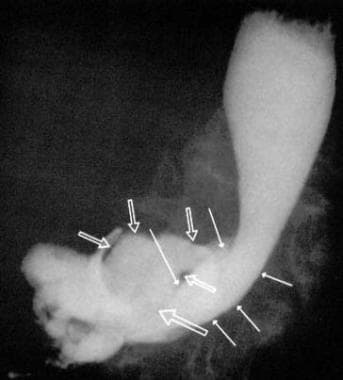
Spontaneous pneumomediastinum in an 18-year-old black Sudanese high school student. (1/128)
Spontaneous pneumomediastinum (SPM) is defined as pneumomediastinum in the absence of an underlying lung disease. It is the second most common cause of chest pain in young, healthy individuals (< 30 years) necessitating hospital visits. It is surpassed in frequency in this setting only by spontaneous pneumothorax. These two conditions may coexist in 18% of patients. The incidence of spontaneous pneumomediastinum varies in different communities and generally is relatively uncommon. Inhalational drug use (cocaine and cannabis) have been associated with a significant number of cases, although cases with no apparent etiologic or incriminating factors are well recognized. Also its recurrence, though uncommon, is worthy of note. It is a benign clinical condition with diverse clinical presentations. Physicians' knowledge of the presentation, treatment, and prognosis of SPM will guard against the need for expensive radiologic and laboratory tests. The differential diagnosis of chest pain, shortness of breath, and dysphagia include cardiac, pulmonary, and esophageal diseases. The tendency to pursue these entities may lead to laboratory investigations such as electrocardiograms, arterial blood gases, ventilation/perfusion scans, and contrast radiographic studies of the esophagus. (+info)Pneumomediastinum as a complication of extraperitoneal laparoscopic inguinal hernia repair. (2/128)
A 52-year-old man with left indirect groin hernia was admitted for elective inguinal repair using the totally extraperitoneal (TEP) approach. After an uneventful intubation, TEP repair of the hernia was performed with three midline trocars. Immediately after extubation, the patient noted severe chest pain. There was a decrease in PaO2 saturation, and neck subcutaneous emphysema was detected. There was no emphysema of the abdomen or of the back. A chest film and thoracic computed tomographic (CT) scan confirmed the presence of pneumomediastinum without pneumothorax. The patient was discharged without complications. (+info)Surgical emphysema and pneumomediastinum in a child following minor blunt injury to the neck. (3/128)
Largyngotracheal and pharyngoesophageal tears following minor blunt trauma to the neck are uncommon. A child with such an injury is reported and the modes of diagnosis and management are discussed. Patients may initially present with minimal signs and symptoms, but their condition may deteriorate rapidly or insidiously. In the absence of respiratory compromise, conservative management is appropriate, but all patients with significant blunt neck trauma should undergo early direct laryngoscopy under a general anaesthetic. (+info)Air leak syndrome as one of the manifestations of bronchiolitis obliterans organizing pneumonia. (4/128)
A 46-year-old man developed respiratory distress with air leak syndrome (ALS), including pneumothorax, pneumomediastinum, and subcutaneous emphysema. Open lung biopsy was performed and revealed the histopathologic evidence of bronchiolitis obliterans organizing pneumonia (BOOP), which responded well to steroid treatment. As far as we know, this appears to be the first case of BOOP presenting with ALS as one of its major complications. (+info)Pneumomediastinum in dermatomyositis: association with cutaneous vasculopathy. (5/128)
OBJECTIVES: To study the pathogenesis of pneumomediastinum in polymyositis/dermatomyositis (PM/DM). PATIENTS AND METHODS: The clinical records of 48 patients with PM/DM were reviewed, focusing mainly on the presence of pneumomediastinum and cutaneous vasculopathy, and the chest radiographic changes. A patient with pneumomediastinum with a characteristic change in his bronchus is described in detail. Case reports of pneumomediastinum in PM/DM in English publications are reviewed. RESULTS: Among the 48 patients with PM/DM, pneumomediastinum was observed as a complication in four patients with DM and none of the patients with PM. Three of the four patients with pneumomediastinum, but only six of the 44 patients without this complication, had associated cutaneous vasculopathy. There was a significant association of pneumomediastinum with cutaneous vasculopathy (p = 0.02) and younger age (p = 0.04), but not with the prevalence of lung disease. A 30 year old man (patient 1) with DM, who had interstitial pneumonitis and skin ulceration due to vasculopathy, developed pneumomediastinum. Fibreoptic bronchoscopy showed white plaques on the bronchial mucosa, which were confirmed by microscopic examination as representing subepithelial necrosis. A literature review showed 13 cases of DM but no patient with PM with pneumomediastinum. CONCLUSIONS: In patient 1, bronchial necrosis due to vasculopathy was strongly suspected as being responsible for the pneumomediastinum. The results suggest that pneumomediastinum was associated not with interstitial pneumonitis but with the complication of vasculopathy appearing as skin lesions in DM. (+info)Spontaneous pneumomediastinum in 33 patients: yield of chest computed tomography for the diagnosis of the mild type. (6/128)
BACKGROUND: Spontaneous pneumomediastinum (SPM) usually occurs in young people without an apparent precipitating factor or disease. Although there have been many studies focused on the clinical features and standard chest X-ray (CXR) findings of SPM, few have reviewed the chest computed-tomographic (CT) findings. OBJECTIVES: We assessed SPM using CXR and CT, and the relation between them. METHODS: We evaluated 33 patients (26 males) diagnosed with SPM on the basis of symptoms and chest radiological findings. RESULTS: Three patients showed normal CXR but a diagnostic CT scan. Seven showed mild pneumomediastinum on CXR. In these 10 patients, pneumomediastinum was easily detected by chest CT. Moderate and severe SPM were easily detected by both CXR and CT. CONCLUSIONS: These findings suggested that CXR alone poorly detected approximately 30% of SPM and that chest CT scan was needed to make the diagnosis in these cases. It seems likely that SPM is underdiagnosed by 30% or more in clinical practice. (+info)Pneumothorax in the newborn. Changing pattern. (7/128)
The clinical course of pneumothorax and its allied conditions was studied in 34 newborn infants who presented over a 2 1/2-year period. We found an overall incidence of 3/1000 live births. 11 term infants without obvious pulmonary pathology presented early (9 within minutes of birth); 6 of these had aspirated meconium or blood. The remaining 23 were preterm infants with hyaline membrane disease (HMD) and accounted for 68% of the infants in this series. In contrast, they presented late (mean 45 hours) and 16 were on continuous distending pressure (CDP) or intermittent positive pressure ventilation (IPPV) at the onset of pneumothorax. 15% of all infants with HMD who required CDP/IPPV developed pneumothorax; this increased incidence was most evident in infants who received CDP only. All except 2 of the 11 term infants in the first group were managed conservatively and all survived. Wehn pneumothorax occurred as a complication of HMD in preterm infants, 14 of the 16 infants required intrapleural drainage. Persistence or recurrence of pneumothorax occurred in 9 infants, 7 of whom were receiving CDP/IPPV at the time. Lung expansion was affected only after replacement with a patent chest drain through the same incision or insertion of a second drain on the same side of the chest. All 5 deaths occurred in the group of preterm infants with HMD. 3 resulted directly form respiratory failure due to severe HMD complicated by pneumothorax. We emphasize the increasing importance of pneumothorax as a complication of HMD in preterm infants, particularly in those receiving CDP. Successful management depends on prompt diagnosis and treatment of pneumothorax, which may occur as unexplained sudden deterioration at any time during the course of illness in this group of high risk infants. (+info)A case of spontaneous pneumomediastinum and pneumopericardium in a young adult. (8/128)
Spontaneous medialstinal emphysema (pneumomediastinum) and pneumopericardium may be defined as the presence of free air or gas in the mediastinal structures and in the pericardial sac without an apparent precipitating cause. It most frequently occurs in young healthy adults without serious underlying pulmonary disease. Although pneumomediastinum and pneumopericardium is often asymptomatic, it may cause pain in the neck and chest, dysphonia and shortness of breath. Treatment is supportive unless the patient has a history of trauma from foreign body aspiration. The course of spontaneous pneumomediastinum and pneumopericardium is usually benign and self-limited. A case of spontaneous pneumomediastinum, pneumopericardium and subcutaneous emphysema in a 20-year-old male is reported in this paper. (+info)Mediastinal emphysema is a medical condition characterized by the presence of air or gas within the mediastinum, which is the central compartment of the thorax that contains the heart, esophagus, trachea, bronchi, thymus gland, and other associated structures.
In mediastinal emphysema, the air accumulates in the mediastinal tissues and spaces, leading to their abnormal distention or swelling. This condition can result from various causes, including:
* Pulmonary trauma or barotrauma (e.g., mechanical ventilation, scuba diving)
* Infections that cause gas-forming organisms (e.g., pneumomediastinum)
* Air leakage from the lungs or airways (e.g., bronchial rupture, esophageal perforation)
* Certain medical procedures (e.g., mediastinoscopy, tracheostomy)
Mediastinal emphysema can cause symptoms such as chest pain, cough, difficulty breathing, and swallowing problems. In severe cases, it may lead to life-threatening complications, including tension pneumothorax or mediastinitis. Treatment depends on the underlying cause and severity of the condition.
Subcutaneous emphysema is a medical condition where air or gas collects in the subcutaneous tissue, which lies beneath the skin and above the muscle layer. This tissue covers the entire body, but the collection of air usually occurs in the chest wall, neck, or face. The accumulation of air can cause swelling, crepitus (a crackling or crunching sound when touched), and tightness in the affected area. Subcutaneous emphysema is often associated with underlying conditions such as trauma, pulmonary disease, or certain medical procedures that result in air leaks from the lungs or other structures into the subcutaneous tissue. It can be a serious condition if left untreated, as it may lead to complications like mediastinal emphysema or tension pneumothorax. Immediate medical attention is necessary for proper diagnosis and treatment.
Pulmonary emphysema is a chronic respiratory disease characterized by abnormal, permanent enlargement of the airspaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis. This results in loss of elastic recoil, which leads to trappling of air within the lungs and difficulty exhaling. It is often caused by cigarette smoking or long-term exposure to harmful pollutants. The disease is part of a group of conditions known as chronic obstructive pulmonary disease (COPD), which also includes chronic bronchitis.
Emphysema is a chronic respiratory disease characterized by abnormal, permanent enlargement of the airspaces called alveoli in the lungs, accompanied by destruction of their walls. This results in loss of elasticity and decreased gas exchange efficiency, causing shortness of breath and coughing. It is often caused by smoking or exposure to harmful pollutants. The damage to the lungs is irreversible, but quitting smoking and using medications can help alleviate symptoms and slow disease progression.
Barotrauma is a type of injury that occurs when there is a difference in pressure between the external environment and the internal body, leading to damage to body tissues. It commonly affects gas-filled spaces in the body, such as the lungs, middle ear, or sinuses.
In medical terms, barotrauma refers to the damage caused by changes in pressure that occur rapidly, such as during scuba diving, flying in an airplane, or receiving treatment in a hyperbaric chamber. These rapid changes in pressure can cause the gas-filled spaces in the body to expand or contract, leading to injury.
For example, during descent while scuba diving, the pressure outside the body increases, and if the diver does not equalize the pressure in their middle ear by swallowing or yawning, the increased pressure can cause the eardrum to rupture, resulting in barotrauma. Similarly, rapid ascent while flying can cause the air in the lungs to expand, leading to lung overexpansion injuries such as pneumothorax or arterial gas embolism.
Prevention of barotrauma involves equalizing pressure in the affected body spaces during changes in pressure and avoiding diving or flying with respiratory infections or other conditions that may increase the risk of injury. Treatment of barotrauma depends on the severity and location of the injury and may include pain management, antibiotics, surgery, or hyperbaric oxygen therapy.
Hydrostatic pressure is the pressure exerted by a fluid at equilibrium at a given point within the fluid, due to the force of gravity. In medical terms, hydrostatic pressure is often discussed in relation to body fluids and tissues. For example, the hydrostatic pressure in the capillaries (tiny blood vessels) is the force that drives the fluid out of the blood vessels and into the surrounding tissues. This helps to maintain the balance of fluids in the body. Additionally, abnormal increases in hydrostatic pressure can contribute to the development of edema (swelling) in the tissues.
Atmospheric pressure, also known as barometric pressure, is the force per unit area exerted by the Earth's atmosphere on objects. It is measured in units of force per unit area, such as pascals (Pa), pounds per square inch (psi), or, more commonly, millimeters of mercury (mmHg).
Standard atmospheric pressure at sea level is defined as 101,325 Pa (14.7 psi) or 760 mmHg (29.92 inches of mercury). Atmospheric pressure decreases with increasing altitude, as the weight of the air above becomes less. This decrease in pressure can affect various bodily functions, such as respiration and digestion, and may require adaptation for individuals living at high altitudes. Changes in atmospheric pressure can also be used to predict weather patterns, as low pressure systems are often associated with stormy or inclement weather.
An encyclopedia is a comprehensive reference work containing articles on various topics, usually arranged in alphabetical order. In the context of medicine, a medical encyclopedia is a collection of articles that provide information about a wide range of medical topics, including diseases and conditions, treatments, tests, procedures, and anatomy and physiology. Medical encyclopedias may be published in print or electronic formats and are often used as a starting point for researching medical topics. They can provide reliable and accurate information on medical subjects, making them useful resources for healthcare professionals, students, and patients alike. Some well-known examples of medical encyclopedias include the Merck Manual and the Stedman's Medical Dictionary.
In medical terms, pressure is defined as the force applied per unit area on an object or body surface. It is often measured in millimeters of mercury (mmHg) in clinical settings. For example, blood pressure is the force exerted by circulating blood on the walls of the arteries and is recorded as two numbers: systolic pressure (when the heart beats and pushes blood out) and diastolic pressure (when the heart rests between beats).
Pressure can also refer to the pressure exerted on a wound or incision to help control bleeding, or the pressure inside the skull or spinal canal. High or low pressure in different body systems can indicate various medical conditions and require appropriate treatment.
The term "diving" is generally not used in the context of medical definitions. However, when referring to diving in relation to a medical or physiological context, it usually refers to the act of submerging the body underwater, typically for activities such as swimming, snorkeling, or scuba diving.
In a medical or physiological sense, diving can have specific effects on the human body due to changes in pressure, temperature, and exposure to water. Some of these effects include:
* Changes in lung volume and gas exchange due to increased ambient pressure at depth.
* Decompression sickness (DCS) or nitrogen narcosis, which can occur when dissolved gases form bubbles in the body during ascent from a dive.
* Hypothermia, which can occur if the water is cold and the diver is not adequately insulated.
* Barotrauma, which can occur due to pressure differences between the middle ear or sinuses and the surrounding environment.
* Other medical conditions such as seizures or heart problems can also be exacerbated by diving.
It's important for divers to undergo proper training and certification, follow safe diving practices, and monitor their health before and after dives to minimize the risks associated with diving.
Blood pressure is the force exerted by circulating blood on the walls of the blood vessels. It is measured in millimeters of mercury (mmHg) and is given as two figures:
1. Systolic pressure: This is the pressure when the heart pushes blood out into the arteries.
2. Diastolic pressure: This is the pressure when the heart rests between beats, allowing it to fill with blood.
Normal blood pressure for adults is typically around 120/80 mmHg, although this can vary slightly depending on age, sex, and other factors. High blood pressure (hypertension) is generally considered to be a reading of 130/80 mmHg or higher, while low blood pressure (hypotension) is usually defined as a reading below 90/60 mmHg. It's important to note that blood pressure can fluctuate throughout the day and may be affected by factors such as stress, physical activity, and medication use.
 Barotrauma
Barotrauma Pneumomediastinum: MedlinePlus Medical Encyclopedia
Pneumomediastinum: MedlinePlus Medical Encyclopedia Esophageal Tear Imaging: Practice Essentials, Radiography, Computed Tomography
Esophageal Tear Imaging: Practice Essentials, Radiography, Computed Tomography Pathology
Pathology Pneumomediastinum | Johns Hopkins Medicine
Pneumomediastinum | Johns Hopkins Medicine Feasibility and effectiveness of prone position ventilation technique for postoperative acute lung injury in infants with...
Feasibility and effectiveness of prone position ventilation technique for postoperative acute lung injury in infants with... Overview of Idiopathic Interstitial Pneumonias - Pulmonary Disorders - Merck Manuals Professional Edition
Overview of Idiopathic Interstitial Pneumonias - Pulmonary Disorders - Merck Manuals Professional Edition Submucosal tunnel endoscopy: Peroral endoscopic myotomy and peroral endoscopic tumor resection
Submucosal tunnel endoscopy: Peroral endoscopic myotomy and peroral endoscopic tumor resection Synonyms
Synonyms Pneumomediastinum in COVID-19: a phenotype of severe COVID-19 pneumonitis? The results of the United Kingdom (POETIC) survey<...
Pneumomediastinum in COVID-19: a phenotype of severe COVID-19 pneumonitis? The results of the United Kingdom (POETIC) survey<... Turkiye Klinikleri Thoracic Surgery - Special Topics 2016 - Volume 7 Issue 2 | Journals | Türkiye Klinikleri
Turkiye Klinikleri Thoracic Surgery - Special Topics 2016 - Volume 7 Issue 2 | Journals | Türkiye Klinikleri Substance-Related Disorders - Page 3 | DADOSPDF
Substance-Related Disorders - Page 3 | DADOSPDF 2. Barotrauma Overview
2. Barotrauma Overview PADI IDC Exam Questions and Answers - How to Pass The PADI IE Exam - Scuba Diving Tips
PADI IDC Exam Questions and Answers - How to Pass The PADI IE Exam - Scuba Diving Tips Brian Wessman - Fingerprint
- Research Profiles at Washington University School of Medicine
Brian Wessman - Fingerprint
- Research Profiles at Washington University School of Medicine Number 1
Number 1