Mouth Breathing
Nasal Obstruction
Otorhinolaryngologic Diseases
Stomatognathic System
Respiration
Mouth
Work of Breathing
Oral airway resistance during wakefulness in patients with obstructive sleep apnoea. (1/93)
BACKGROUND: Patients with obstructive sleep apnoea (OSA) have a number of upper airway structural abnormalities which may influence the resistance of the oral airway to airflow. There have been no systematic studies of the flow dynamics of the oral cavity in such patients. METHODS: Inspiratory oral airway resistance to airflow (RO) was measured in 13 awake patients with OSA in both the upright and supine positions (neck position constant). Each subject breathed via a mouthpiece while the nasal airway was occluded with a nasal mask. RESULTS: In the upright position the mean (SE) RO was 1.26 (0. 19) cm H2O/l/s (at 0.4 l/s) which increased to 2.01 (0.43) cm H2O/l/s when supine (p<0.05, paired t test). The magnitude of this change correlated negatively with the respiratory disturbance index (r = -0.60, p = 0.03). CONCLUSION: In awake patients with OSA RO is normal when upright but abnormally raised when in the supine position. (+info)Longitudinal distribution of chlorine absorption in human airways: comparison of nasal and oral quiet breathing. (2/93)
The fraction of an inspired chlorine (Cl2) bolus absorbed during a single breath (Lambda) was measured as a function of bolus penetration (VP) into the respiratory system of five male and five female nonsmokers during both nasal and oral breathing at a quiet respiratory flow of 250 ml/s. The correspondence between VP and specific anatomic landmarks was found for each subject by a combination of acoustic reflection and nitrogen washout measurements. For both nasal and oral breathing, Lambda reached approximately 0. 95 at the distal end of the upper airways and reached 1.00 within the lower conducting airways. The values of a regional mass transfer parameter computed from the Lambda-VP data indicated that the resistance to Cl2 diffusion in the airway mucosa was negligible compared with the diffusion resistance in the respired gas. Changing the peak inhaled Cl2 concentration from 0.5 to 3.0 parts/million did not significantly affect the distribution of Cl2 absorption, suggesting that the underlying mass transport and chemical reaction processes were linear with respect to Cl2 concentration. (+info)Effect of mouth leak on effectiveness of nasal bilevel ventilatory assistance and sleep architecture. (3/93)
Mouth leak is common during nasal ventilatory assistance, but its effects on ventilatory support and on sleep architecture are unknown. The acute effect of sealing the mouth on sleep architecture and transcutaneous carbon dioxide tension (Ptc,CO2) was tested in 9 patients (7 hypercapnic) on longterm nasal bilevel ventilation with symptomatic mouth leak. Patients slept with nasal bilevel ventilation at their usual settings on two nights in random order. On one night, the mouth was taped closed. Leak was measured with a pneumotachograph. Median leak fell from 0.35+/-0.07 (mean +/- SEM) L x s(-1) untaped to 0.06+/-0.03 L x s(-1) taped. Ptc,CO2 fell in 8/9, including all hypercapnic patients. Across all patients, the mean Ptc,CO2 fell by 1.02+/-0.28 kPa (7.7+/-2.1 mm Hg) with taping (p = 0.007). Arousal index fell in every patient. Mean arousal index fell from 35.0+/-3.0 to 13.9+/-1.2 h(-1) (p<0.0001), and rapid eye movement (REM) sleep increased from 12.9+/-1.5% to 21.1+/-1.8% sleep time (p = 0.0016). Slow wave sleep changed inconsistently, from a mean of 13.1+/-1.6% to 19.5+/-2.2% of sleep (p = 0.09). Sleep latency and efficiency were unchanged. In four healthy volunteers ventilator-induced awake hypopharyngeal pressure swing during timed bilevel ventilation fell by 35+/-5% L(-1) x s(-1) of voluntary mouth leak (p<0.0001). Mouth leak reduces effective nasal bilevel ventilatory support, increases transcutaneous carbon dioxide tension, and disrupts sleep architecture. (+info)Influence of posture and breathing route on neural drive to upper airway dilator muscles during exercise. (4/93)
Our purpose was to determine the influence of posture and breathing route on electromyographic (EMG) activities of nasal dilator (NDM) and genioglossus (GG) muscles during exercise. Nasal and oral airflow rates and EMG activities of the NDM and GG were recorded in 10 subjects at rest and during upright and supine incremental cycling exercise to exhaustion. EMG activities immediately before and after the switch from nasal to oronasal breathing were also determined for those subjects who demonstrated a clear switch point (n = 7). NDM and GG EMG activities were significantly correlated with increases in nasal, oral, and total ventilatory rates during exercise, and these relationships were not altered by posture. In both upright and supine exercise, NDM activity rose more sharply as a function of nasal inspired ventilation compared with total or oral inspired ventilation (P < 0.01), but GG activity showed no significant breathing-route dependence. Peak NDM integrated EMG activity decreased (P = 0.008), and peak GG integrated EMG activity increased (P = 0.032) coincident with the switch from nasal to oronasal breathing. In conclusion, 1) neural drive to NDM and GG increases as a function of exercise intensity, but the increase is unaltered by posture; 2) NDM activity is breathing-route dependent in steady-state exercise, but GG activity is not; and 3) drive to both muscles changes significantly at the switch point, but the change in GG activity is more variable and is often transient. This suggests that factors other than the breathing route dominate drive to the GG soon after the initial changes in the configuration of the oronasal airway are made. (+info)Effects of intermaxillary fixation during orthognathic surgery on respiratory function after general anesthesia. (5/93)
I examined the relationship between preoperative breathing route (nasal and/or oral) and respiratory status in 29 patients who underwent orthognathic surgery and intermaxillary fixation (IMF) with general anesthesia and in 14 healthy, adult control volunteers who received IMF without surgery or anesthesia. The tidal volume (VT), minute respiratory volume (MV), respiratory rate, and end-tidal carbon dioxide concentration were measured for both nasal and oral breathing before and after IMF. Pulse oximetry recordings were also taken. There was no significant effect of IMF on any parameter in the volunteers. Fifteen patients engaged in nasal breathing only both before and after surgery with IMF (group pN), and 7 patients had combined nasal and oral breathing before but only nasal breathing after IMF (group pNO). VT and MV decreased (536-357 mL and 7.84-5.40 L, respectively) in group pNO after IMF. These results suggest that assessment of the preoperative breathing status is helpful in predicting postoperative respiratory function after IMF and indicate that patients with preoperative mouth breathing require greater respiratory care after general anesthesia with IMF. (+info)Cleft lip and palate: a review for dentists. (6/93)
The goals of primary closure of cleft lip and palate include not only re-establishing normal insertions for all of the nasolabial muscles but also restoring the normal position of all the other soft tissues, including the mucocutaneous elements. Conventional surgical wisdom, which recommends waiting until growth is complete before undertaking surgical correction of the postoperative sequelae of primary cheiloplasty, carries with it many disadvantages. If, after primary surgery of the lip, orolabial dysfunctions remain, they will exert their nefarious influences during growth and will themselves lead to long term dentofacial imbalances. These imbalances can significantly influence facial harmony. Unless accurate, symmetric and functional reconstruction of the nasolabial muscles is achieved during the primary surgery, not only will the existing dentoskeletal imbalances be exaggerated, but other deformities will be caused during subsequent growth, among which the most important are nasal obstruction and mouth breathing, reduced translation of the maxilla, dysymmetry of the nose and inability of the patient to symmetrically project the upper lip (+info)Lip seal study of Japanese adults with malocclusion. (7/93)
The purpose of this study to clarify the factors an effecting lip seal in Japanese adults with malocclusion. Sixty-three malocclusion patients aged 20 to 27 years were randomly selected and compared with fourteen normal occlusion controls aged 22 to 26 years old. The subjects were divided into a good seal group and a poor lip seal group by observing the distance between the upper and lower lip at rest. Results of this adult study were as follows; There were no poor lip seals in normal occlusion subjects. Significant differences were observed for tongue thrust (p < 0.05) and mouth breathing (p < 0.05) between the good lip seal group and poor lip seal group of malocclusion subjects. Adults with poor lip seal should be treated for their malocclusion prior to be other functional approaches to improving their lip seal. (+info)Partitioning of inhaled ventilation between the nasal and oral routes during sleep in normal subjects. (8/93)
The oral and nasal contributions to inhaled ventilation were simultaneously quantified during sleep in 10 healthy subjects (5 men, 5 women) aged 43 +/- 5 yr, with normal nasal resistance (mean 2.0 +/- 0.3 cmH(2)O. l(-1). s(-1)) by use of a divided oral and nasal mask. Minute ventilation awake (5.9 +/- 0.3 l/min) was higher than that during sleep (5.2 +/- 0.3 l/min; P < 0.0001), but there was no significant difference in minute ventilation between different sleep stages (P = 0.44): stage 2 5.3 +/- 0.3, slow-wave 5.2 +/- 0.2, and rapid-eye-movement sleep 5.2 +/- 0.2 l/min. The oral fraction of inhaled ventilation during wakefulness (7.6 +/- 4%) was not significantly different from that during sleep (4.3 +/- 2%; mean difference 3.3%, 95% confidence interval -2.1-8.8%, P = 0.19), and no significant difference (P = 0.14) in oral fraction was observed between different sleep stages: stage two 5.1 +/- 2.8, slow-wave 4.2 +/- 1.8, rapid-eye-movement 3.1 +/- 1.7%. Thus the inhaled oral fraction in normal subjects is small and does not change significantly with sleep stage. (+info)Mouth breathing is a condition characterized by the regular habit of breathing through the mouth instead of the nose during awake states and sometimes during sleep. This can occur due to various reasons such as nasal congestion, deviated septum, enlarged tonsils or adenoids, or structural abnormalities in the jaw or airway. Prolonged mouth breathing can lead to several oral and general health issues, including dry mouth, bad breath, gum disease, and orthodontic problems. It can also affect sleep quality and cognitive function.
Nasal obstruction is a medical condition that refers to any blockage or restriction in the normal flow of air through the nasal passages. This can be caused by various factors such as inflammation, swelling, or physical abnormalities in the nasal cavity. Common causes of nasal obstruction include allergies, sinusitis, deviated septum, enlarged turbinates, and nasal polyps. Symptoms may include difficulty breathing through the nose, nasal congestion, and nasal discharge. Treatment options depend on the underlying cause and may include medications, surgery, or lifestyle changes.
Otorhinolaryngologic diseases, also known as ear, nose, and throat (ENT) diseases, refer to a group of medical conditions that affect the ears, nose, and/or throat. These specialized areas are closely related both anatomically and functionally, and disorders in one area can often have impacts on the others.
Here are some examples of otorhinolaryngologic diseases categorized by the affected area:
1. Otologic diseases - affecting the ear:
* Otitis media (ear infection)
* Otitis externa (swimmer's ear)
* Tinnitus (ringing in the ears)
* Hearing loss
* Meniere's disease (inner ear disorder causing vertigo, tinnitus, and hearing loss)
* Acoustic neuroma (noncancerous tumor on the vestibular nerve)
2. Rhinologic diseases - affecting the nose:
* Allergic rhinitis (hay fever)
* Non-allergic rhinitis
* Sinusitis (sinus infection)
* Deviated septum
* Nasal polyps
* Epistaxis (nosebleed)
3. Laryngologic diseases - affecting the throat and voice box:
* Laryngitis (inflammation of the larynx, causing hoarseness or voice loss)
* Vocal cord nodules or polyps
* Reflux laryngitis (acid reflux irritating the throat)
* Subglottic stenosis (narrowing of the airway below the vocal cords)
* Laryngeal cancer
4. Common otorhinolaryngologic diseases:
* Tonsillitis (inflammation of the tonsils, often causing sore throat and difficulty swallowing)
* Adenoiditis (inflammation of the adenoids, commonly seen in children)
* Obstructive sleep apnea (OSA, a disorder characterized by pauses in breathing during sleep)
* Pharyngitis (inflammation of the pharynx or throat)
Otorhinolaryngologists, also known as ENT specialists, diagnose and treat these conditions. They may use various methods such as physical examination, imaging studies, endoscopy, and laboratory tests to determine the best course of treatment for each individual patient.
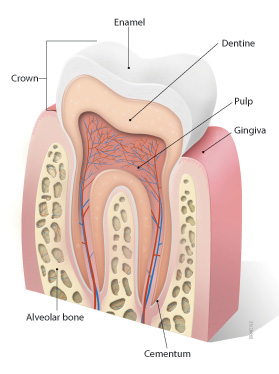
The stomatognathic system is a term used in medicine and dentistry to refer to the coordinated functions of the mouth, jaw, and related structures. It includes the teeth, gums, tongue, palate, lips, cheeks, salivary glands, as well as the muscles of mastication (chewing), swallowing, and speech. The stomatognathic system also involves the temporomandibular joint (TMJ) and associated structures that allow for movement of the jaw. This complex system works together to enable functions such as eating, speaking, and breathing. Dysfunction in the stomatognathic system can lead to various oral health issues, including temporomandibular disorders, occlusal problems, and orofacial pain.
Adenoids are a pair of masses of lymphoid tissue located in the nasopharynx, which is the upper part of the throat behind the nose. They are part of the immune system and help to protect against infection. Adenoids are largest in children and tend to shrink in size as people get older. In some cases, adenoids can become enlarged or infected, leading to problems such as breathing difficulties, ear infections, and sleep disorders. Treatment for enlarged or infected adenoids may include antibiotics, medications to reduce swelling, or surgical removal of the adenoids (adenoidectomy).
Medical Definition of Respiration:
Respiration, in physiology, is the process by which an organism takes in oxygen and gives out carbon dioxide. It's also known as breathing. This process is essential for most forms of life because it provides the necessary oxygen for cellular respiration, where the cells convert biochemical energy from nutrients into adenosine triphosphate (ATP), and releases waste products, primarily carbon dioxide.
In humans and other mammals, respiration is a two-stage process:
1. Breathing (or external respiration): This involves the exchange of gases with the environment. Air enters the lungs through the mouth or nose, then passes through the pharynx, larynx, trachea, and bronchi, finally reaching the alveoli where the actual gas exchange occurs. Oxygen from the inhaled air diffuses into the blood, while carbon dioxide, a waste product of metabolism, diffuses from the blood into the alveoli to be exhaled.
2. Cellular respiration (or internal respiration): This is the process by which cells convert glucose and other nutrients into ATP, water, and carbon dioxide in the presence of oxygen. The carbon dioxide produced during this process then diffuses out of the cells and into the bloodstream to be exhaled during breathing.
In summary, respiration is a vital physiological function that enables organisms to obtain the necessary oxygen for cellular metabolism while eliminating waste products like carbon dioxide.
Snoring is defined as the vibration of respiratory structures and the resulting sound, due to obstructed air movement during breathing while sleeping. It occurs when the tissues at the back of the throat relax and narrow during sleep, partially blocking the airway. The airflow causes these tissues to vibrate, leading to the snoring sound. Snoring can be a sign of various conditions such as obstructive sleep apnea or other respiratory disorders. It can also be influenced by factors such as alcohol consumption, obesity, and sleeping position.
In medical terms, the mouth is officially referred to as the oral cavity. It is the first part of the digestive tract and includes several structures: the lips, vestibule (the space enclosed by the lips and teeth), teeth, gingiva (gums), hard and soft palate, tongue, floor of the mouth, and salivary glands. The mouth is responsible for several functions including speaking, swallowing, breathing, and eating, as it is the initial point of ingestion where food is broken down through mechanical and chemical processes, beginning the digestive process.
Cephalometry is a medical term that refers to the measurement and analysis of the skull, particularly the head face relations. It is commonly used in orthodontics and maxillofacial surgery to assess and plan treatment for abnormalities related to the teeth, jaws, and facial structures. The process typically involves taking X-ray images called cephalograms, which provide a lateral view of the head, and then using various landmarks and reference lines to make measurements and evaluate skeletal and dental relationships. This information can help clinicians diagnose problems, plan treatment, and assess treatment outcomes.
Work of breathing (WOB) is a term used in respiratory physiology to describe the amount of energy expended by the respiratory muscles to overcome the elastic and resistive forces in the lungs and chest wall during breathing. It is usually measured in joules per liter (J/L) or in breaths per minute (BPM).
WOB can be increased in various lung diseases, such as chronic obstructive pulmonary disease (COPD), asthma, and interstitial lung disease, due to increased airway resistance or decreased lung compliance. Increased WOB can lead to respiratory muscle fatigue, decreased exercise tolerance, and reduced quality of life.
WOB can be measured noninvasively using techniques such as esophageal pressure monitoring or transdiaphragmatic pressure measurement, or invasively through the use of indwelling catheters in the pleural space or within the airways. These measurements are often used in research settings to evaluate the effectiveness of various treatments for respiratory disorders.
 Mouth breathing
Mouth breathing Nose Breathing vs. Mouth Breathing During Sleep - Which Is Better? - AskMen
Nose Breathing vs. Mouth Breathing During Sleep - Which Is Better? - AskMen Mouth Breathing | Harvard Catalyst Profiles | Harvard Catalyst
Mouth Breathing | Harvard Catalyst Profiles | Harvard Catalyst Positive Health Online | Article - Every Child Can Grow an Attractive Face - Mouth Breathing Causes Crooked Teeth
Positive Health Online | Article - Every Child Can Grow an Attractive Face - Mouth Breathing Causes Crooked Teeth Where did the myth that humans can automatically breathe through their mouths come from? | Sciforums
Where did the myth that humans can automatically breathe through their mouths come from? | Sciforums mouth breathing怎么读,"mouth breathing"的发音
mouth breathing怎么读,"mouth breathing"的发音 Clinical Trials on Mouth Breathing - Clinical Trials Registry - ICH GCP
Clinical Trials on Mouth Breathing - Clinical Trials Registry - ICH GCP Mouth breathing in Tursiops truncatus: | Centro Ricerca Cetacei
Mouth breathing in Tursiops truncatus: | Centro Ricerca Cetacei Stomach Ache, Smelly Stool, Bad Mouth Breathe, Gastric | Ask A Doctor 24x7
Stomach Ache, Smelly Stool, Bad Mouth Breathe, Gastric | Ask A Doctor 24x7 Mouth Breathing - Faceology
Mouth Breathing - Faceology Problems with Mouth Breathing
Problems with Mouth Breathing MOUTH BREATHING CREATES UNHEALTHY KIDS
MOUTH BREATHING CREATES UNHEALTHY KIDS Am I mouth breathing? | Apnea Board
Am I mouth breathing? | Apnea Board 3 Bad Breathing Habits and How They Affect Your Body - Areas of My Expertise
3 Bad Breathing Habits and How They Affect Your Body - Areas of My Expertise mouth breathing causes Archives - Dental Care Tips
mouth breathing causes Archives - Dental Care Tips MOUTH BREATHING - THE CONNECTION TO INSOMNIA. - sleepQ+
MOUTH BREATHING - THE CONNECTION TO INSOMNIA. - sleepQ+ Is Mouth Breathing Bad? - All About Smiles
Is Mouth Breathing Bad? - All About Smiles How Does Therapy Help Eliminate Mouth Breathing?
How Does Therapy Help Eliminate Mouth Breathing? Inspirewell-Buteyko and Myofunctional Therapy-Mouth Breathing-StroudUK
Inspirewell-Buteyko and Myofunctional Therapy-Mouth Breathing-StroudUK Mouth Breathing's Impact on Dental Health: Causes & Solutions
Mouth Breathing's Impact on Dental Health: Causes & Solutions Snoring/Mouth Breathing Archives - Good Night Sleep Site
Snoring/Mouth Breathing Archives - Good Night Sleep Site Chronic Mouth Breathing from Door County Dental Care
Chronic Mouth Breathing from Door County Dental Care Adenoid,Mouth Breathing and Dental Malocclusion | Dr Paulose
Adenoid,Mouth Breathing and Dental Malocclusion | Dr Paulose Myofunctional exercises for mouth breathing - Elite Dental 2021
Myofunctional exercises for mouth breathing - Elite Dental 2021 Kids Habit Breaking - Thumb Sucking and Mouth Breathing
Kids Habit Breaking - Thumb Sucking and Mouth Breathing