Neuromyelitis Optica
Aquaporin 4
Myelitis, Transverse
Autoantibodies
Demyelinating Autoimmune Diseases, CNS
Multiple Sclerosis
Optic Neuritis
Immunoglobulin G
Optic Nerve
Spinal Cord
Oligoclonal Bands
Area Postrema
Paraneoplastic Syndromes, Nervous System
Myelitis
Paraneoplastic Syndromes, Ocular
Magnetic Resonance Imaging
Astrocytes
Complement System Proteins
Bulbar Palsy, Progressive
Referral and Consultation
Hyperprolactinemia in optico-spinal multiple sclerosis. (1/195)
OBJECTIVE: To clarify the clinical features of MS patients with hyperprolactinemia. SUBJECTS AND METHODS: The serum prolactin level was measured in 67 Japanese patients (19 men and 48 women) with multiple sclerosis (MS) and in 16 patients (4 men and 12 women) with HTLV-I-associated myelopathy/tropical spastic paraparesis (HAM/TSP) using a two-site immunoradiometric assay. RESULTS: In the MS patients, 32 were classified as having Asian type MS showing a selective involvement of the optic nerves and spinal cord, while the other 35 were classified as having Western type MS which displayed disseminated central nervous system involvement. In women, the serum prolactin level was found to be significantly higher only in Asian type MS (mean=23.1 ng/ml, n=25) than in HAM/TSP (mean=6.9 ng/ml, n=12) (p=0.0297), while it did not differ significantly in men among the three groups. Hyperprolactinemia was significantly associated with acute relapse involving the optic nerves. All MS patients with hyperprolactinemia (7 women with Asian type MS and 2 women with Western type MS) showed recurrent opticomyelitis either throughout or in the early course of the disease, and also had a higher age of onset, a higher Expanded Disability Status Scale score, a greater visual impairment, and higher cell counts and protein contents in the cerebrospinal fluid than did the normoprolactinemic patients. CONCLUSION: Hyperprolactinemia may be one of the characteristic features of Asian patients with MS who preferentially show the optic nerve involvement. (+info)Matrix metalloproteinases and tissue inhibitors of metalloproteinases in cerebrospinal fluid differ in multiple sclerosis and Devic's neuromyelitis optica. (2/195)
Matrix metalloproteinases (MMPs) are increased in the CSF of patients with multiple sclerosis. Devic's neuromyelitis optica (DNO) is a demyelinating syndrome that involves the optic nerve and cervical cord but differs pathologically from multiple sclerosis. Therefore, we hypothesized that the type of inflammatory reaction that causes MMPs to be elevated in multiple sclerosis would be absent in patients with DNO. CSF was collected from 23 patients with relapsing-remitting or secondary progressive multiple sclerosis, all of whom were experiencing acute symptoms, from seven patients with DNO, and from seven normal volunteers. Diagnoses were made according to current criteria on the basis of clinical manifestations, imaging results and CSF studies. IgG synthesis was increased in the CSF of multiple sclerosis patients but not in that of DNO patients. Zymography, reverse zymography and ELISA (enzyme-linked immunosorbent assay) were used to measure gelatinase A (MMP-2), gelatinase B (MMP-9) and tissue inhibitors of metalloproteinases (TIMPs). Zymograms showed that multiple sclerosis patients had elevated MMP-9 compared with DNO patients and controls (P: < 0.05). TIMP-1 and TIMP-2 levels were similar in all three groups. We conclude that multiple sclerosis patients have higher MMP-9 levels in the CSF than patients with DNO, which supports the different pathological mechanisms of these diseases. (+info)A role for humoral mechanisms in the pathogenesis of Devic's neuromyelitis optica. (3/195)
Devic's disease [neuromyelitis optica (NMO)] is an idiopathic inflammatory demyelinating disease of the CNS, characterized by attacks of optic neuritis and myelitis. The mechanisms that result in selective localization of inflammatory demyelinating lesions to the optic nerves and spinal cord are unknown. Serological and clinical evidence of B cell autoimmunity has been observed in a high proportion of patients with NMO. The purpose of this study was to investigate the importance of humoral mechanisms, including complement activation, in producing the necrotizing demyelination seen in the spinal cord and optic nerves. Eighty-two lesions were examined from nine autopsy cases of clinically confirmed Devic's disease. Demyelinating activity in the lesions was immunocytochemically classified as early active (21 lesions), late active (18 lesions), inactive (35 lesions) or remyelinating (eight lesions) by examining the antigenic profile of myelin degradation products within macrophages. The pathology of the lesions was analysed using a broad spectrum of immunological and neurobiological markers, and lesions were defined on the basis of myelin protein loss, the geography and extension of plaques, the patterns of oligodendrocyte destruction and the immunopathological evidence of complement activation. The pathology was identical in all nine patients. Extensive demyelination was present across multiple spinal cord levels, associated with cavitation, necrosis and acute axonal pathology (spheroids), in both grey and white matter. There was a pronounced loss of oligodendrocytes within the lesions. The inflammatory infiltrates in active lesions were characterized by extensive macrophage infiltration associated with large numbers of perivascular granulocytes and eosinophils and rare CD3(+) and CD8(+) T cells. There was a pronounced perivascular deposition of immunoglobulins (mainly IgM) and complement C9neo antigen in active lesions associated with prominent vascular fibrosis and hyalinization in both active and inactive lesions. The extent of complement activation, eosinophilic infiltration and vascular fibrosis observed in the Devic NMO cases is more prominent compared with that in prototypic multiple sclerosis, and supports a role for humoral immunity in the pathogenesis of NMO. Based on this study, future therapeutic strategies designed to limit the deleterious effects of complement activation, eosinophil degranulation and neutrophil/macrophage/microglial activation are worthy of further investigation. (+info)Optic neuromyelitis syndrome in Brazilian patients. (4/195)
OBJECTIVES: To report the clinical features and outcome of 24 Brazilian patients with optic neuromyelitis syndrome (ONM); discuss the underlying pathological events associated with the ONM syndrome; review the nosological situation of ONM in the group of inflammatory and demyelinating diseases of the central nervous system. PATIENTS AND METHODS: Patients with ONM treated at the Hospital da Lagoa, Rio de Janeiro were studied. Demographic, clinical, magnetic resonance imaging, cerebrospinal fluid, and pathological data were analysed. RESULTS: The study consisted of 20 women, four men of whom 10 were white and 14 Afro-Brazilians. Clinical course was recurrent in 22 cases and monophasic in two. Neurological manifestations at inclusion were: sensory impairment (66%), bilateral (41.6%) or unilateral blindness (20.8%), paraplegia or quadriplegia (37.5%). The EDSS was moderate/severe in 70.8%. The underlying pathological events were respectively pulmonary tuberculosis and upper respiratory infection in the two monophasic cases; in the 22 recurrent ONM patients: pulmonary tuberculosis (3), neurocysticercosis (1), polyarteritis nodosa (1), antinuclear antibody and rheumatoid factor (1), antiphospholipid antibody primary syndrome (1), diabetes mellitus (1), hypothyroidism (1), and amenorrhea-galactorrhea (4). Normal cerebrospinal fluid was found in 52% and an inflammatory profile in 48%. Only four recurrent ONM white patients had brain and spinal cord magnetic resonance imaging and cerebrospinal fluid findings compatible with the diagnosis of multiple sclerosis. Large lesions were seen in 62% of spinal magnetic resonance images. Six of 12 recurrent ONM Afro-Brazilian died. There were no statistical differences in the demographic data of the two ethnic groups. Afro-Brazilians were significantly more severely impaired and had a higher mortality rate than the white patients. CONCLUSION: These cases were classified as follows: two monophasic acute disseminated encephalomyelitis; one recurrent disseminated encephalomyelitis; three recurrent ONM associated with Hughes syndrome, autoantibodies and polyarteritis nodosa; six recurrent ONM with endocrinopathies; and finally, four multiple sclerosis cases. The remaining cases were not associated with any other condition. It would seem clear that ONM is a syndrome rather than a single disease. (+info)Devic's neuromyelitis optica and Schilder's myelinoclastic diffuse sclerosis. (5/195)
An adult patient developed both Devic's neuromyelitis optica and Schilder's myelinoclastic diffuse sclerosis, suggesting that these entities represent rare topographical and aggressive variants within the spectrum of multiple sclerosis. (+info)Recurrent neuromyelitis optica with diffuse central nervous system involvement: case report. (6/195)
Several demyelinating disorders can affect children. The differential diagnosis between these diseases is usually an arduous task. Diagnostic criteria have been proposed for some of these disorders, however most of them have not yet been clinically and prospectively validated. Here we present a case of a ten year-old boy with recurrent bilateral optic neuritis and spinal cord involvement. Clinical and cerebrospinal fluid data have fulfilled diagnostic criteria for Devic's neuromyelitis optica (NMO). The differential diagnosis with multiple sclerosis (MS) has become troublesome since not only optic nerves and spinal cord were involved. In one of the relapses a left hemiparesis with facial involvement was registered. Magnetic resonance imaging was also compatible with MS. This case illustrates that CNS demyelinating disorders can fulfill diagnostic criteria for more than one demyelinating disease, making the clinical judgment an important tool in the management of these patients. (+info)Clinicopathological study of a myelin oligodendrocyte glycoprotein-induced demyelinating disease in LEW.1AV1 rats. (7/195)
Although multiple sclerosis is considered to be an autoimmune disease in the CNS, the immune responses that take place in the CNS and lymphoid organs remain to be elucidated. Here, we have successfully induced various subtypes of experimental autoimmune encephalitis (EAE) in LEW.1AV1 rats carrying RT1(av1) on the Lewis background genes by immunization with recombinant rat myelin oligodendrocyte glycoprotein (MOG) in various solutions with adjuvants. The purpose of the present study was to analyse in more detail the clinical and immunopathological features of MOG-induced EAE in LEW.1AV1 rats. Immunization with high doses of soluble MOG with pertussis toxin induced acute, frequently fatal EAE, whereas medium doses of partially aggregated MOG without pertussis toxin produced relapsing and remitting EAE. Secondary progressive EAE was induced in some rats by immunization with the immunization protocol having an intermediate nature between the above two. The optic nerve (approximately 60% of the immunized rats) and spinal cord (100%) were frequently involved and detectable both clinically and pathologically, while there was no lesion in the cerebrum. Histological examination revealed that, despite variety in the clinical subtypes, progression of the pathological processes was strikingly uniform, i.e. initial inflammation with minimal demyelination followed by predominant demyelination with minimal lymphocyte infiltration. These findings suggest that the lesion during the later stage is maintained by humoral factors. Taken together, this experimental system can serve as a model of neuromyelitis optica. Further analysis will provide useful information to elucidate the pathogenesis and to develop immunotherapy for neuromyelitis optica and multiple sclerosis. (+info)Intrathecal activation of the IL-17/IL-8 axis in opticospinal multiple sclerosis. (8/195)
There are two distinct subtypes of multiple sclerosis in Asians, opticospinal (OS-multiple sclerosis) and conventional (C-multiple sclerosis). In OS-multiple sclerosis, selective and severe involvement of the optic nerves and spinal cord is characteristic, though its mechanisms are unknown. The present study aimed to find out possible differences in the cytokine/chemokine profiles in CSF between OS-multiple sclerosis and C-multiple sclerosis and to delineate the relationships between these profiles and neuroimaging and pathological features. Sixteen cytokines/chemokines, namely interleukin (IL)-1beta, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-12 (p70), IL-13, IL-17, interferon (IFN)-gamma, tumour necrosis factor (TNF)-alpha, granulocyte colony-stimulating factor (G-CSF), monocyte chemoattractant protein-1 (MCP-1) and macrophage inflammatory protein-1beta (MIP-1beta), were measured simultaneously in CSF supernatants from 40 patients with relapsing-remitting multiple sclerosis (20 OS-multiple sclerosis and 20 C-multiple sclerosis) at relapse and 19 control patients with spinocerebellar degeneration (SCD), together with intracellular production of IFN-gamma and IL-4 in CSF CD4+ T cells. In CSF supernatants relative to controls, IL-17, MIP-1beta, IL-1beta and IL-13 were only significantly increased in OS-multiple sclerosis patients, while TNF-alpha was only significantly increased in C-multiple sclerosis patients, using a cut-off level of 1 pg/ml. IL-8 was significantly elevated in both OS-multiple sclerosis and C-multiple sclerosis patients. MCP-1 was significantly decreased in both OS-multiple sclerosis and C-multiple sclerosis patients, while IL-7 was only significantly decreased in C-multiple sclerosis patients. IL-17, IL-8 and IL-5 were significantly higher in OS-multiple sclerosis patients than in C-multiple sclerosis patients. The increases in IL-17 and IL-8 in OS-multiple sclerosis were still significant even after exclusion of the patients undergoing various immunomodulatory therapies. Assays of intracellular cytokine production revealed that both the IFN-gamma+IL-4- T-cell percentage and intracellular IFN-gamma/IL-4 ratio in CSF cells were significantly greater in C-multiple sclerosis patients than in controls. Contrarily, OS-multiple sclerosis patients showed not only a significantly greater percentage of IFN-gamma+IL-4- T cells than controls but also a significantly higher percentage of IFN-gamma-IL-4+ T cells than C-multiple sclerosis patients. Among the cytokines elevated in multiple sclerosis, only IL-8 showed a significant positive correlation with the Expanded Disability Status Scale of Kurtzke score. Both the length of the spinal cord lesions on MRI and the CSF/serum albumin ratio had a significant positive correlation with IL-8 and IL-17 in multiple sclerosis, in which the spinal cord lesions were significantly longer in OS-multiple sclerosis than in C-multiple sclerosis. Three of six spinal cord specimens from autopsied OS-multiple sclerosis cases demonstrated numerous myeloperoxidase-positive neutrophils infiltrating necrotic lesions. These findings strongly suggest that in OS-multiple sclerosis, in addition to the Th1 cell upregulation seen in C-multiple sclerosis, intrathecal activation of the IL-17/IL-8 axis inducing heavy neutrophil infiltration contributes to extensive spinal cord lesion formation. (+info)Neuromyelitis optica (NMO), also known as Devic's disease, is an autoimmune disorder that affects the central nervous system (CNS). It primarily causes inflammation and damage to the optic nerves (which transmit visual signals from the eye to the brain) and the spinal cord. This results in optic neuritis (inflammation of the optic nerve, causing vision loss) and myelitis (inflammation of the spinal cord, leading to motor, sensory, and autonomic dysfunction).
A key feature of NMO is the presence of autoantibodies against aquaporin-4 (AQP4-IgG), a water channel protein found in astrocytes (a type of glial cell) in the CNS. These antibodies play a crucial role in the development of the disease, as they target and damage the AQP4 proteins, leading to inflammation, demyelination (loss of the protective myelin sheath around nerve fibers), and subsequent neurological dysfunction.
NMO is distinct from multiple sclerosis (MS), another autoimmune disorder affecting the CNS, as it has different clinical features, radiological findings, and treatment responses. However, NMO can sometimes be misdiagnosed as MS due to overlapping symptoms in some cases. Accurate diagnosis of NMO is essential for appropriate management and treatment, which often includes immunosuppressive therapies to control the autoimmune response and prevent further damage to the nervous system.
Aquaporin 4 (AQP4) is a water channel protein that is primarily found in the membranes of astrocytes, which are a type of glial cell in the central nervous system. AQP4 plays a crucial role in the regulation of water homeostasis and the clearance of excess fluid from the brain and spinal cord. It also facilitates the rapid movement of water across the blood-brain barrier and between astrocytes, which is important for maintaining proper neuronal function and protecting the brain from edema or swelling.
Mutations in the AQP4 gene can lead to various neurological disorders, such as neurodegenerative diseases and neuromyelitis optica spectrum disorder (NMOSD), a severe autoimmune condition that affects the optic nerves and spinal cord. In NMOSD, the immune system mistakenly attacks AQP4 proteins, causing inflammation, demyelination, and damage to the nervous tissue.
Transverse Myelitis is a neurological disorder that involves inflammation of the spinal cord, leading to damage in both sides of the cord. This results in varying degrees of motor, sensory, and autonomic dysfunction, typically defined by the level of the spine that's affected. Symptoms may include a sudden onset of lower back pain, muscle weakness, paraesthesia or loss of sensation, and bowel/bladder dysfunction. The exact cause is often unknown but can be associated with infections, autoimmune disorders, or other underlying conditions.
Autoantibodies are defined as antibodies that are produced by the immune system and target the body's own cells, tissues, or organs. These antibodies mistakenly identify certain proteins or molecules in the body as foreign invaders and attack them, leading to an autoimmune response. Autoantibodies can be found in various autoimmune diseases such as rheumatoid arthritis, lupus, and thyroiditis. The presence of autoantibodies can also be used as a diagnostic marker for certain conditions.
Demyelinating autoimmune diseases of the central nervous system (CNS) are a group of disorders characterized by inflammation and damage to the myelin sheath, which is the protective covering that surrounds nerve fibers in the brain and spinal cord. This damage can result in various neurological symptoms, including muscle weakness, sensory loss, vision problems, and cognitive impairment.
The most common demyelinating autoimmune disease of the CNS is multiple sclerosis (MS), which affects approximately 2.3 million people worldwide. Other examples include neuromyelitis optica spectrum disorder (NMOSD), acute disseminated encephalomyelitis (ADEM), and transverse myelitis.
These conditions are thought to arise when the immune system mistakenly attacks the myelin sheath, leading to inflammation, damage, and scarring (sclerosis) in the CNS. The exact cause of this autoimmune response is not fully understood, but it is believed to involve a complex interplay between genetic, environmental, and immunological factors.
Treatment for demyelinating autoimmune diseases of the CNS typically involves a combination of medications to manage symptoms, reduce inflammation, and modify the course of the disease. These may include corticosteroids, immunosuppressive drugs, and disease-modifying therapies (DMTs) that target specific components of the immune system.
Multiple Sclerosis (MS) is a chronic autoimmune disease that affects the central nervous system (CNS), which includes the brain, spinal cord, and optic nerves. In MS, the immune system mistakenly attacks the protective covering of nerve fibers, called myelin, leading to damage and scarring (sclerosis). This results in disrupted communication between the brain and the rest of the body, causing a variety of neurological symptoms that can vary widely from person to person.
The term "multiple" refers to the numerous areas of scarring that occur throughout the CNS in this condition. The progression, severity, and specific symptoms of MS are unpredictable and may include vision problems, muscle weakness, numbness or tingling, difficulty with balance and coordination, cognitive impairment, and mood changes. There is currently no cure for MS, but various treatments can help manage symptoms, modify the course of the disease, and improve quality of life for those affected.
Optic neuritis is a medical condition characterized by inflammation and damage to the optic nerve, which transmits visual information from the eye to the brain. This condition can result in various symptoms such as vision loss, pain with eye movement, color vision disturbances, and pupillary abnormalities. Optic neuritis may occur in isolation or be associated with other underlying medical conditions, including multiple sclerosis, neuromyelitis optica, and autoimmune disorders. The diagnosis typically involves a comprehensive eye examination, including visual acuity testing, dilated funduscopic examination, and possibly imaging studies like MRI to evaluate the optic nerve and brain. Treatment options may include corticosteroids or other immunomodulatory therapies to reduce inflammation and prevent further damage to the optic nerve.
Immunoglobulin G (IgG) is a type of antibody, which is a protective protein produced by the immune system in response to foreign substances like bacteria or viruses. IgG is the most abundant type of antibody in human blood, making up about 75-80% of all antibodies. It is found in all body fluids and plays a crucial role in fighting infections caused by bacteria, viruses, and toxins.
IgG has several important functions:
1. Neutralization: IgG can bind to the surface of bacteria or viruses, preventing them from attaching to and infecting human cells.
2. Opsonization: IgG coats the surface of pathogens, making them more recognizable and easier for immune cells like neutrophils and macrophages to phagocytose (engulf and destroy) them.
3. Complement activation: IgG can activate the complement system, a group of proteins that work together to help eliminate pathogens from the body. Activation of the complement system leads to the formation of the membrane attack complex, which creates holes in the cell membranes of bacteria, leading to their lysis (destruction).
4. Antibody-dependent cellular cytotoxicity (ADCC): IgG can bind to immune cells like natural killer (NK) cells and trigger them to release substances that cause target cells (such as virus-infected or cancerous cells) to undergo apoptosis (programmed cell death).
5. Immune complex formation: IgG can form immune complexes with antigens, which can then be removed from the body through various mechanisms, such as phagocytosis by immune cells or excretion in urine.
IgG is a critical component of adaptive immunity and provides long-lasting protection against reinfection with many pathogens. It has four subclasses (IgG1, IgG2, IgG3, and IgG4) that differ in their structure, function, and distribution in the body.
The optic nerve, also known as the second cranial nerve, is the nerve that transmits visual information from the retina to the brain. It is composed of approximately one million nerve fibers that carry signals related to vision, such as light intensity and color, from the eye's photoreceptor cells (rods and cones) to the visual cortex in the brain. The optic nerve is responsible for carrying this visual information so that it can be processed and interpreted by the brain, allowing us to see and perceive our surroundings. Damage to the optic nerve can result in vision loss or impairment.
The spinal cord is a major part of the nervous system, extending from the brainstem and continuing down to the lower back. It is a slender, tubular bundle of nerve fibers (axons) and support cells (glial cells) that carries signals between the brain and the rest of the body. The spinal cord primarily serves as a conduit for motor information, which travels from the brain to the muscles, and sensory information, which travels from the body to the brain. It also contains neurons that can independently process and respond to information within the spinal cord without direct input from the brain.
The spinal cord is protected by the bony vertebral column (spine) and is divided into 31 segments: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each segment corresponds to a specific region of the body and gives rise to pairs of spinal nerves that exit through the intervertebral foramina at each level.
The spinal cord is responsible for several vital functions, including:
1. Reflexes: Simple reflex actions, such as the withdrawal reflex when touching a hot surface, are mediated by the spinal cord without involving the brain.
2. Muscle control: The spinal cord carries motor signals from the brain to the muscles, enabling voluntary movement and muscle tone regulation.
3. Sensory perception: The spinal cord transmits sensory information, such as touch, temperature, pain, and vibration, from the body to the brain for processing and awareness.
4. Autonomic functions: The sympathetic and parasympathetic divisions of the autonomic nervous system originate in the thoracolumbar and sacral regions of the spinal cord, respectively, controlling involuntary physiological responses like heart rate, blood pressure, digestion, and respiration.
Damage to the spinal cord can result in various degrees of paralysis or loss of sensation below the level of injury, depending on the severity and location of the damage.
Oligoclonal bands (OB) are a pattern of immunoglobulin (antibody) proteins found in the cerebrospinal fluid (CSF) when it is analyzed using a technique called electrophoresis. This pattern shows a limited number (oligo) of distinct protein bands, which are clonally expanded (clonal), indicating the presence of an intr Theatreaterathecal immunoglobulin synthesis, typically in response to some sort of central nervous system (CNS) antigenic stimulation or immune response.
The detection of oligoclonal bands is often associated with inflammatory conditions affecting the CNS, such as multiple sclerosis (MS), neuromyelitis optica spectrum disorder (NMOSD), and other infectious or autoimmune diseases. However, it's important to note that their presence alone does not confirm a specific diagnosis, but rather serves as a supportive finding in conjunction with other clinical and diagnostic data.
The area postrema is a small, chemoreceptive region located in the caudal part (the back) of the fourth ventricle in the brainstem. It is part of the vomiting center and is sensitive to various stimuli such as chemical substances, emotions, and vestibular signals that can trigger nausea and vomiting. The area postrema is not protected by the blood-brain barrier, allowing it to directly detect toxins and other harmful substances in the bloodstream. This region plays a crucial role in maintaining homeostasis by regulating fluid balance, electrolyte levels, and the elimination of potentially toxic substances from the body.
Methylprednisolone is a synthetic glucocorticoid drug, which is a class of hormones that naturally occur in the body and are produced by the adrenal gland. It is often used to treat various medical conditions such as inflammation, allergies, and autoimmune disorders. Methylprednisolone works by reducing the activity of the immune system, which helps to reduce symptoms such as swelling, pain, and redness.
Methylprednisolone is available in several forms, including tablets, oral suspension, and injectable solutions. It may be used for short-term or long-term treatment, depending on the condition being treated. Common side effects of methylprednisolone include increased appetite, weight gain, insomnia, mood changes, and increased susceptibility to infections. Long-term use of methylprednisolone can lead to more serious side effects such as osteoporosis, cataracts, and adrenal suppression.
It is important to note that methylprednisolone should be used under the close supervision of a healthcare provider, as it can cause serious side effects if not used properly. The dosage and duration of treatment will depend on various factors such as the patient's age, weight, medical history, and the condition being treated.
Paraneoplastic syndromes of the nervous system are a group of rare disorders that occur in some individuals with cancer. These syndromes are caused by an immune system response to the cancer tumor, which can lead to the damage or destruction of nerve cells. The immune system produces antibodies and/or activated immune cells that attack the neural tissue, leading to neurological symptoms.
Paraneoplastic syndromes can affect any part of the nervous system, including the brain, spinal cord, peripheral nerves, and muscles. Symptoms vary depending on the specific syndrome and the location of the affected nerve tissue. Some common neurological symptoms include muscle weakness, numbness or tingling, seizures, memory loss, confusion, difficulty speaking or swallowing, visual disturbances, and coordination problems.
Paraneoplastic syndromes are often associated with specific types of cancer, such as small cell lung cancer, breast cancer, ovarian cancer, and lymphoma. Diagnosis can be challenging because the symptoms may precede the discovery of the underlying cancer. A combination of clinical evaluation, imaging studies, laboratory tests, and sometimes a brain biopsy may be necessary to confirm the diagnosis.
Treatment typically involves addressing the underlying cancer with surgery, chemotherapy, or radiation therapy. Immunosuppressive therapies may also be used to manage the immune response that is causing the neurological symptoms. While treatment can help alleviate symptoms and improve quality of life, paraneoplastic syndromes are often difficult to cure completely.
Myelitis is a medical term that refers to inflammation of the spinal cord. This inflammation can cause damage to the myelin sheath, which is the protective covering of nerve fibers in the spinal cord. As a result, the transmission of nerve impulses along the spinal cord may be disrupted, leading to various neurological symptoms.
Myelitis can affect any part of the spinal cord and can have many different causes, including infections (such as viral or bacterial infections), autoimmune disorders (such as multiple sclerosis), and other conditions (such as spinal cord injuries or tumors). The specific symptoms of myelitis depend on the location and severity of the inflammation. They may include muscle weakness, numbness or tingling sensations, pain, bladder or bowel dysfunction, and difficulty with coordination and balance.
Myelitis can be a serious condition that requires prompt medical attention and treatment. Treatment typically focuses on addressing the underlying cause of the inflammation, as well as managing symptoms and supporting recovery.
Paraneoplastic syndromes are a group of rare disorders that occur in some individuals with cancer. These syndromes are caused by substances produced by the tumor or the body's immune response to the tumor, which can affect distant organs and cause various symptoms.
Ocular paraneoplastic syndromes refer to a subset of these disorders that specifically affect the eyes. They are caused by an abnormal immune response directed against antigens shared by both the tumor and the nervous tissue of the eye. This results in damage to the nerve cells and can lead to various visual symptoms, such as:
1. Visual loss or blurring
2. Double vision (diplopia)
3. Light sensitivity (photophobia)
4. Abnormalities in pupil size or reactivity
5. Jerky eye movements (nystagmus)
6. Loss of peripheral vision (visual field defects)
7. Impaired color vision
8. Deterioration of the optic nerve (optic neuropathy)
Some examples of ocular paraneoplastic syndromes include:
1. Paraneoplastic retinopathy: A condition characterized by damage to the light-sensitive cells in the retina, leading to visual loss and other visual disturbances.
2. Paraneoplastic optic neuropathy: Damage to the optic nerve that can result in visual loss and visual field defects.
3. Cancer-associated retinopathy (CAR): A condition characterized by progressive vision loss, night blindness, and abnormalities in the electroretinogram (ERG), a test used to assess retinal function.
4. Melanoma-associated retinopathy (MAR): Similar to CAR but specifically associated with melanoma, this condition can cause visual loss, night blindness, and abnormal ERG results.
5. Opsoclonus-myoclonus syndrome: A rare disorder characterized by rapid, involuntary eye movements (opsoclonus) and muscle jerks (myoclonus), which can be associated with various types of cancer, including breast, lung, and ovarian cancer.
It is important to note that these conditions are relatively rare but can significantly impact a patient's quality of life. Early diagnosis and treatment of the underlying cancer can help improve outcomes for patients with ocular paraneoplastic syndromes.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
Astrocytes are a type of star-shaped glial cell found in the central nervous system (CNS), including the brain and spinal cord. They play crucial roles in supporting and maintaining the health and function of neurons, which are the primary cells responsible for transmitting information in the CNS.
Some of the essential functions of astrocytes include:
1. Supporting neuronal structure and function: Astrocytes provide structural support to neurons by ensheathing them and maintaining the integrity of the blood-brain barrier, which helps regulate the entry and exit of substances into the CNS.
2. Regulating neurotransmitter levels: Astrocytes help control the levels of neurotransmitters in the synaptic cleft (the space between two neurons) by taking up excess neurotransmitters and breaking them down, thus preventing excessive or prolonged activation of neuronal receptors.
3. Providing nutrients to neurons: Astrocytes help supply energy metabolites, such as lactate, to neurons, which are essential for their survival and function.
4. Modulating synaptic activity: Through the release of various signaling molecules, astrocytes can modulate synaptic strength and plasticity, contributing to learning and memory processes.
5. Participating in immune responses: Astrocytes can respond to CNS injuries or infections by releasing pro-inflammatory cytokines and chemokines, which help recruit immune cells to the site of injury or infection.
6. Promoting neuronal survival and repair: In response to injury or disease, astrocytes can become reactive and undergo morphological changes that aid in forming a glial scar, which helps contain damage and promote tissue repair. Additionally, they release growth factors and other molecules that support the survival and regeneration of injured neurons.
Dysfunction or damage to astrocytes has been implicated in several neurological disorders, including Alzheimer's disease, Parkinson's disease, amyotrophic lateral sclerosis (ALS), and multiple sclerosis (MS).
Recurrence, in a medical context, refers to the return of symptoms or signs of a disease after a period of improvement or remission. It indicates that the condition has not been fully eradicated and may require further treatment. Recurrence is often used to describe situations where a disease such as cancer comes back after initial treatment, but it can also apply to other medical conditions. The likelihood of recurrence varies depending on the type of disease and individual patient factors.
The complement system is a group of proteins found in the blood and on the surface of cells that when activated, work together to help eliminate pathogens such as bacteria, viruses, and fungi from the body. The proteins are normally inactive in the bloodstream. When they encounter an invading microorganism or foreign substance, a series of reactions take place leading to the activation of the complement system. Activation results in the production of effector molecules that can punch holes in the cell membranes of pathogens, recruit and activate immune cells, and help remove debris and dead cells from the body.
There are three main pathways that can lead to complement activation: the classical pathway, the lectin pathway, and the alternative pathway. Each pathway involves a series of proteins that work together in a cascade-like manner to amplify the response and generate effector molecules. The three main effector molecules produced by the complement system are C3b, C4b, and C5b. These molecules can bind to the surface of pathogens, marking them for destruction by other immune cells.
Complement proteins also play a role in the regulation of the immune response. They help to prevent excessive activation of the complement system, which could damage host tissues. Dysregulation of the complement system has been implicated in a number of diseases, including autoimmune disorders and inflammatory conditions.
In summary, Complement System Proteins are a group of proteins that play a crucial role in the immune response by helping to eliminate pathogens and regulate the immune response. They can be activated through three different pathways, leading to the production of effector molecules that mark pathogens for destruction. Dysregulation of the complement system has been linked to various diseases.
Progressive bulbar palsy (PBP) is a form of motor neuron disease (MND), also known as Amyotrophic Lateral Sclerosis (ALS). It is characterized by the progressive degeneration of the motor neurons in the brainstem, which control vital functions such as swallowing, speaking, chewing, and breathing.
In PBP, these symptoms gradually worsen over time, often resulting in severe disability and ultimately death due to respiratory failure. The progression of the disease can vary from person to person, but it typically advances more slowly than other forms of ALS. There is currently no cure for PBP or any other form of MND, and treatment is focused on managing symptoms and maintaining quality of life.
**Referral:**
A referral in the medical context is the process where a healthcare professional (such as a general practitioner or primary care physician) sends or refers a patient to another healthcare professional who has specialized knowledge and skills to address the patient's specific health condition or concern. This could be a specialist, a consultant, or a facility that provides specialized care. The referral may involve transferring the patient's care entirely to the other professional or may simply be for a consultation and advice.
**Consultation:**
A consultation in healthcare is a process where a healthcare professional seeks the opinion or advice of another professional regarding a patient's medical condition. This can be done in various ways, such as face-to-face meetings, phone calls, or written correspondence. The consulting professional provides their expert opinion to assist in the diagnosis, treatment plan, or management of the patient's condition. The ultimate decision and responsibility for the patient's care typically remain with the referring or primary healthcare provider.
I'm sorry for any confusion, but "Suburban Population" is not a medical term. It refers to the people living in suburban areas, which are typically residential districts or communities that lie outside a city center. They are often characterized by single-family homes and less population density than in urban areas. If you have any questions related to medical terminology, I would be happy to help with those!
 Neuromyelitis optica spectrum disorder
Neuromyelitis optica spectrum disorder
MOG antibody disease
Anti-AQP4 disease
CCL17
Inflammatory demyelinating diseases of the central nervous system
Eugène Devic
Aquaporin-4
Satralizumab
Uhthoff's phenomenon
Multiple sclerosis
John F. Kurtzke
Chromosome 5 open reading frame 47
Pathophysiology of multiple sclerosis
Multiple sclerosis research
Lesional demyelinations of the central nervous system
Anti-neurofascin demyelinating diseases
Pathology of multiple sclerosis
Cholesterol 7 alpha-hydroxylase
Myelin oligodendrocyte glycoprotein
Optic neuritis
Acute disseminated encephalomyelitis
List of autoimmune diseases
Malignant multiple sclerosis
Tim Harris (biochemist)
Neuritis
Chronic relapsing inflammatory optic neuropathy
Classical complement pathway
Anti-NMDA receptor encephalitis
Interleukin 6
Tocilizumab
Neuromyelitis optica spectrum disorder - Wikipedia
 Brain abnormalities in neuromyelitis optica
Brain abnormalities in neuromyelitis optica
 Vaccines Tied to Relapses in Neuromyelitis Optica | MedPage Today
Vaccines Tied to Relapses in Neuromyelitis Optica | MedPage Today
 Alternative Treatment of Neuromyelitis optica spectrum Disorder or Devic's disease
Alternative Treatment of Neuromyelitis optica spectrum Disorder or Devic's disease
Cytokine and chemokine profiles in neuromyelitis optica: significance of interleukin-6
 Neuromyelitis Optica Spectrum Disorder (NMOSD) Medical Assistance - National Organization for Rare Disorders
Neuromyelitis Optica Spectrum Disorder (NMOSD) Medical Assistance - National Organization for Rare Disorders
 A Case Study of Intractable Vomiting with Final Diagnosis of Neuromyelitis Optica
A Case Study of Intractable Vomiting with Final Diagnosis of Neuromyelitis Optica
Neuromyelitis Optica Spectrum Disorder (NMOSD) Premium Copay Assistance - National Organization for Rare Disorders
 Eculizumab (Soliris) for Neuromyelitis Optica Spectrum Disorder | Cleveland Clinic
Eculizumab (Soliris) for Neuromyelitis Optica Spectrum Disorder | Cleveland Clinic
 New neuromyelitis optica spectrum disorder fund opens - PAN Foundation
New neuromyelitis optica spectrum disorder fund opens - PAN Foundation
 RNA profiles to distinguish multiple sclerosis and neuromyelitis optica in peripheral whole blood | Quest Diagnostics
RNA profiles to distinguish multiple sclerosis and neuromyelitis optica in peripheral whole blood | Quest Diagnostics
 Neuromyelitis Optica Archives - Hamilton Health Care System
Neuromyelitis Optica Archives - Hamilton Health Care System
 Astrazeneca's Inebilizumab Gains EU Orphan Designation in Neuromyelitis Optica Spectrum Disorder | 2017-04-12 | FDANews |...
Astrazeneca's Inebilizumab Gains EU Orphan Designation in Neuromyelitis Optica Spectrum Disorder | 2017-04-12 | FDANews |...
 Fighting friendly fire with fire: An antibody for treating neuromyelitis optica
Fighting friendly fire with fire: An antibody for treating neuromyelitis optica
 A review of cases of neuromyelitis optica - The GJCF
A review of cases of neuromyelitis optica - The GJCF
Establishment of a New Sensitive Assay for Anti-Human Aquaporin-4 Antibody in Neuromyelitis Optica
 Aquaporin 4-positive neuromyelitis optica spectrum disorder with meningoencephalitis-like onset: A case report. - International...
Aquaporin 4-positive neuromyelitis optica spectrum disorder with meningoencephalitis-like onset: A case report. - International...
A mathematical model of cellular swelling in Neuromyelitis optica - Nuffield Department of Clinical Neurosciences
 Neuromyelitis Optica Spectrum Disorder Pipeline Drugs Analysis Report, 2023: FDA Approvals, Clinical Trials, Therapies, ...
Neuromyelitis Optica Spectrum Disorder Pipeline Drugs Analysis Report, 2023: FDA Approvals, Clinical Trials, Therapies, ...
The evolving clinical spectrum of neuromyelitis optica - Nuffield Department of Clinical Neurosciences
 Life Expectancy Of Someone With Neuromyelitis Optica
Life Expectancy Of Someone With Neuromyelitis Optica
 Neuromyelitis Optica - Radiology Cases
Neuromyelitis Optica - Radiology Cases
 Forums | Neuromyelitis-Optica.net
Forums | Neuromyelitis-Optica.net
My story | Neuromyelitis-Optica.net
 Neuromyelitis Optica Spectrum Disorder - ENDECE
Neuromyelitis Optica Spectrum Disorder - ENDECE
 Ventricular Toxicity - 1549 Words | Bartleby
Ventricular Toxicity - 1549 Words | Bartleby
Sjogren myelopathy and neuromyelitis Optica - Immunology
 Serum chitinase 3-like 1 levels in patients with multiple sclerosis and neuromyelitis optica | AVESİS
Serum chitinase 3-like 1 levels in patients with multiple sclerosis and neuromyelitis optica | AVESİS
Neuromyelitis optica spectrum disorders - Fingerprint - Mayo Clinic
 Neuromyelitis Optica | Weill Cornell Medicine Multiple Sclerosis Center
Neuromyelitis Optica | Weill Cornell Medicine Multiple Sclerosis Center
NMOSD20
- Neuromyelitis optica spectrum disorders (NMOSD), including neuromyelitis optica (NMO), are autoimmune diseases characterized by acute inflammation of the optic nerve (optic neuritis, ON) and the spinal cord (myelitis). (wikipedia.org)
- PARIS - Vaccines may trigger relapses in patients with neuromyelitis optica spectrum disorder (NMOSD), but that risk is diminished if patients are on immunosuppressive therapy, researchers reported here. (medpagetoday.com)
- From numerous disorders of the central nervous system, Neuromyelitis optica spectrum disorder (NMOSD) is the one. (selfgrowth.com)
- Neuromyelitis optica spectrum disorder (NMOSD) is a disorder of the central nervous system that majorly affects the nerves of eyes (optic neuritis) and the spinal cord (myelitis). (selfgrowth.com)
- NMOSD is also known as Devic's disease or Neuromyelitis optica (NMO) . (selfgrowth.com)
- On June 27, 2019, eculizumab, or Soliris, became the first FDA approved treatment for anti-aquaporin-4 (AQP4) antibody positive neuromyelitis optica spectrum disorder (NMOSD) in adults. (clevelandclinic.org)
- Neuromyelitis optica spectrum disease (NMOSD) is a debilitating autoimmune inflammatory demyelinating disease of the central nervous system. (iasp-pain.org)
- In October 2022, detailed positive results from the Phase III CHAMPION-NMOSD trial showed that ULTOMIRIS®(ravulizumab-cwvz) significantly reduced relapse risk in adults with anti-aquaporin-4 (AQP4) antibody-positive (Ab+)neuromyelitis optica spectrum disorder (NMOSD), compared to the external placebo arm from the pivotal SOLIRIS®PREVENT clinical trial. (abnewswire.com)
- In June 2022, Alexion Pharmaceuticals initited a Phase II/III , open-label, historical-controlled,single-arm, multicenter study to evaluate the efficacy, pharmacokinetics, pharmacodynamics, and safety of ravulizumab inchildren and adolescents with aquaporin-4 antibody positive (AQP4-Ab [+]) Neuromyelitis Optica Spectrum Disorder(NMOSD). (abnewswire.com)
- In May 2022, Alexion Pharmaceuticals announced that ULTOMIRIS® (ravulizumab-cwvz) met primary endpoint inCHAMPION-NMOSD Phase III trial in adults with neuromyelitis optica spectrum disorder. (abnewswire.com)
- 2 3 4 5 6 ] However, a more recent population-based survey conducted in urban Mangalore has shown a prevalence of 8.3/100,000 for MS and 2.6/100,000 for neuromyelitis optic spectrum diseases (NMOSD). (lww.com)
- Neuromyelitis optica spectrum disorder (NMOSD) is one of the autoimmune demyelinating disorders, which is thought to be triggered by viral infection. (aku.edu)
- keywords = "Aquaporin 4 (AQP-4), Neuromyelitis optica spectrum disorder (NMOSD), Severe acute respiratory syndrome (SARS). (aku.edu)
- Satralizumab is an interleukin 6 (IL-6) receptor inhibitor that works by decreasing protocol-defined relapse (PDR) risk in patients diagnosed with neuromyelitis optica spectrum disorder (NMOSD). (mdnewsline.com)
- Here we investigated whether the brain structural and functional connectivity alterations were involved in fatigue related to neuromyelitis optica spectrum disorder (NMOSD). (biomedcentral.com)
- Neuromyelitis optica spectrum disorder (NMOSD) is an autoimmune disorder affecting the central nervous system and associated with the presence of aquaporin-4 immunoglobulin G antibodies (AQP4-IgG) [ 1 ]. (biomedcentral.com)
- Cognitive impairment in neuromyelitis optica spectrum disorder (NMOSD) is not uncommon occurring independent from attacks and lesions. (gccair.org)
- Although fatigue is a major symptom in patients with neuromyelitis optica spectrum disorder (NMOSD), the underlying mechanism remains unclear. (phoenixrising.me)
- Background: Optic neuritis is a frequent finding in multiple sclerosis (MS) and in neuromyelitis optica spectrum disorder (NMOSD), as well as in Myelin-Oligodendrocyte Glycoprotein (MOG) -positive disease. (tau.ac.il)
- Neuromyelitis optica spectrum disorder (NMOSD) is characterised by recurrent attacks of optic neuritis and transverse myelitis . (bvsalud.org)
Living with neuromyelitis optica spectrum disorder2
- The PAN Foundation today opened a new financial assistance program for people living with neuromyelitis optica spectrum disorder. (panfoundation.org)
- The National Organization for Rare Disorders estimates that between one and 10 of every 100,000 people are living with neuromyelitis optica spectrum disorder worldwide. (panfoundation.org)
Relapses in neuromyelitis optica1
- Because of these results, a subsequent randomized, double-blinded, placebo-controlled phase III time-to-event trial over 4 years, Prevention of Relapses in Neuromyelitis Optica (PREVENT), was performed. (clevelandclinic.org)
Antibody positive2
- Eculizumab was first studied in 14 AQP4 antibody positive neuromyelitis optica patients in an open-label trial. (clevelandclinic.org)
- Headache, nausea, and dizziness were the most common side effects reported in the open label trial of eculizumab in APQ4 antibody positive neuromyelitis optica patients. (clevelandclinic.org)
Disorders3
- Neuromyelitis optica spectrum disorders: a case of longitudinally extensive transverse myelitis. (ac.lk)
- Efficacy and safety of rituximab in myelin oligodendrocyte glycoprotein antibody-associated disorders compared with neuromyelitis optica spectrum disorder: a systematic review and meta-analysis. (ox.ac.uk)
- BackgroundRituximab (RTX) efficacy in patients with myelin oligodendrocyte glycoprotein (MOG) antibody-associated disorders (MOGADs) is still poorly understood, though it appears to be lower than in aquaporin-4-IgG-positive neuromyelitis optica spectrum disorders (AQP4-IgG+NMOSDs). (ox.ac.uk)
20231
- " Neuromyelitis Optica Spectrum Disorder Pipeline Insight, 2023 " report by DelveInsight outlines comprehensive insights into the present clinical development scenario and growth prospects across the Neuromyelitis Optica Spectrum Disorder Market. (abnewswire.com)
Myelin oligodendroc2
- We searched PubMed and Medline for studies published during the last 10 years with the general term "optic neuritis" and specific terms like "typical optic neuritis," "atypical optic neuritis," "multiple sclerosis," "neuromyelitis optic neuritis," and "myelin oligodendrocyte glycoprotein antibody. (lww.com)
- In neuromyelitis optica spectrum disorder, the immune system targets aquaporin 4, a protein that is present on astrocytes in the brain and particularly the spinal cord and optic nerves, or myelin oligodendrocyte glycoprotein (MOG), which is present on the myelin of oligodendrocytes in the same areas of the CNS and possibly other targets. (msdmanuals.com)
Neurology2
- In a study published this month in Annals of Neurology , researchers from Osaka University have revealed that treatment with an antibody to a protein called repulsive guidance molecule-a (RGMa) dramatically improves symptoms of neuromyelitis optica , a devastating autoimmune disorder, in an experimental rat model. (medicalxpress.com)
- One condition that had not been differentiated from MS was neuromyelitis optica, a condition that received minimal attention in textbooks of neurology, usually a footnote in chapters on MS. It was either believed to be very rare and many neurologists in western countries didn't believe that it was an independent disease, rather a severe form of MS. (sumairafoundation.org)
Acute1
- Although he did not propose any diagnostic criteria, a convention was established that lack of relapses was essential for making a diagnosis of "Devic's disease", a condition that he referred to as acute neuromyelitis optica. (sumairafoundation.org)
Optic9
- Neuromyelitis optica (NMO) is a severe demyelinating disease defined principally by its tendency to selectively affect optic nerves and the spinal cord causing recurrent attacks of blindness and paralysis. (nih.gov)
- Neuromyelitis optica spectrum disorder, also known as Devic's disease and neuromyelitis optica, is a rare autoimmune disease where an individual's immune system reacts against its own cells in the central nervous system, mainly in the optic nerves and spinal cord, but sometimes in the brain. (panfoundation.org)
- Neuromyelitis optica (NMO) is a devastating neurologic disease characterized by severe optic neuritis and transverse myelitis. (go.jp)
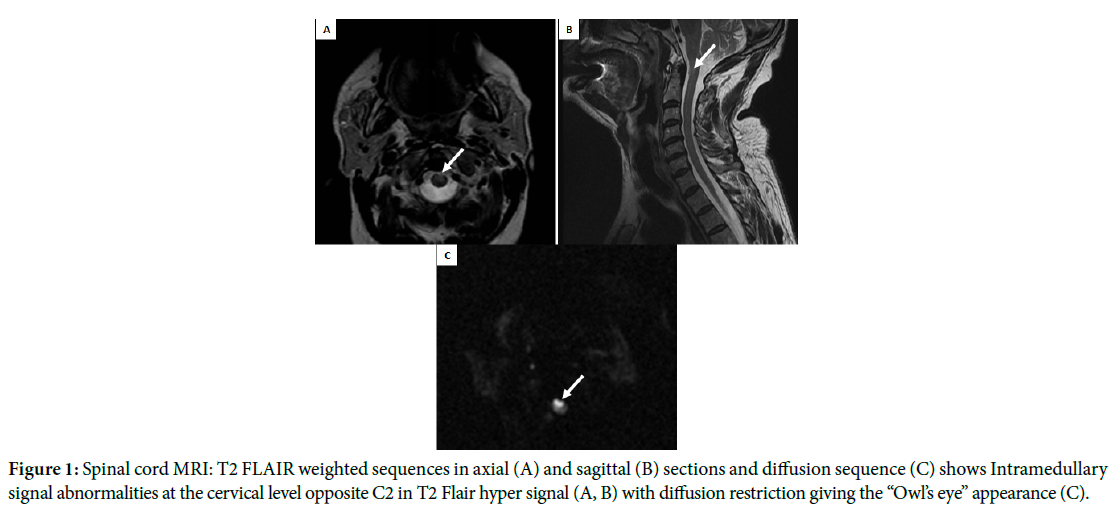
- Neuromyelitis Optica (NMO) is a severe form of demyelinating disease, characterized by involvement of the optic nerve and spinal cord and presence of highly specific anti-aquaporin-4 (AQP4) antibody in the CSF. (radiologycases.my)
- NeuroMyelitis Optica (NMO) is an autoimmune demyelinating disease that differs from multiple sclerosis in that the inflammatory attack is limited to the optic (eye) nerves and the spinal cord. (weillcornell.org)
- Neuromyelitis optica spectrum disorder is a rare CNS autoimmune disease, resulting in lesions throughout the optic nerves and spinal cord. (nursingrepository.org)
- Neuromyelitis optica (NMO) (and NMO spectrum disorder) is an autoimmune inflammatory disease of the CNS primarily affecting spinal cord and optic nerves. (duke.edu)
- can help differentiate neuromyelitis optica from other optic neuropathies. (msdmanuals.com)
- Optic neuritis (ON) is a demyelinating inflammation of the optic nerve that often occurs in association with multiple sclerosis (MS) and, much less commonly, neuromyelitis optica (NMO). (medscape.com)
Diagnosis1
- This antibody facilitated rapid and early diagnosis of neuromyelitis optica, and identified a series of other clinical syndromes, including sev ere vomiting and hiccups, to name but one, that was a syndrome of neuromyelitis optica previously unrecognized before discovery of the aquaporin-4 antibody. (sumairafoundation.org)
Middle Aged1
- My first contact with a patient who raised the issue of what neuromyelitis optica might be was a middle-aged Lebanese woman for whom I cared while practicing at the Ottawa General Hospital in Ottawa, Canada, the site of my first neurological practice. (sumairafoundation.org)
Findings2
- Findings in neuromyelitis optica spectrum disorder include reduced amplitudes or prolonged latencies. (msdmanuals.com)
- Seropositive findings for neuromyelitis optica (NMO)-immunoglobulin G (IgG) antibody occurring with SS/SLE (Sjogren syndrome/SLE overlap) or non-organ-specific antibodies favors coexisting NMO (Devin syndrome) rather than a vasculitic process. (medscape.com)
AQP41
- Long-term efficacy of satralizumab in AQP4-IGG-Seropositive Neuromyelitis Optica Spectrum Disorder from SAkuraSky and SAkuraStar. (mdnewsline.com)
Aquaporin3
- Aquaporin 4-positive neuromyelitis optica spectrum disorder with meningoencephalitis-like onset: A case report. (iasp-pain.org)
- Moreover, it was found that this Aquaporin 4 antibody was responsible for the Oriental form of Neuromyelitis optica. (diagnosticdetectives.com)
- Neuromyelitis optica spectrum disorder is a demyelinating disorder that predominantly affects the eyes and spinal cord but can affect other structures in the central nervous system (CNS) that contain aquaporin 4. (msdmanuals.com)
Inflammatory1
- Neuromyelitis optica (NMO) is an inflammatory disorder that can cause pain, paralysis, and even death. (medicalxpress.com)
Spinal Cord1
- Neuromyelitis optica affects several (typically ≥ 3) contiguous spinal segments of the spinal cord, whereas MS typically affects a single segment. (msdmanuals.com)
Patients3
- Patients who qualify are eligible to receive $9,600 per year in financial assistance to pay for the deductibles, copays, and coinsurance costs associated with their treatment for neuromyelitis optica spectrum disorder. (panfoundation.org)
- While some reports in the early 1900's including a few patients in a thesis by a student of Devic had relapsing forms of neuromyelitis optica, the possibility of relapse in this condition was ignored and it was suggested that such patients may have represented diagnostic errors. (sumairafoundation.org)
- The prevalence, incidence, and clinical assessment of neuromyelitis optica spectrum disorder in patients with demyelinating diseases. (bvsalud.org)
Multiple2
- Neuromyelitis optica (NMO) is assumed to be immunologically distinct from multiple sclerosis (MS). Adequate studies about cytokines and chemokines in NMO have been lacking. (nih.gov)
- Neuromyelitis optica responds to multiple sclerosis medications differently. (diagnosticdetectives.com)
Treatment5
- There is no cure for neuromyelitis optica spectrum disorder, but with proper treatment, long-term remission is sometimes possible. (panfoundation.org)
- Be getting treatment for neuromyelitis optica spectrum disorder. (panfoundation.org)
- The European Medicines Agency has granted orphan drug designation to inebilizumab (formerly MEDI-551) for the treatment of neuromyelitis optica spectrum disorder. (fdanews.com)
- Las Vegas, Nevada, United States) As per DelveInsight's assessment, globally, Neuromyelitis Optica Spectrum Disorder pipeline constitutes 15+ key companies continuously working towards developing 15+ Neuromyelitis Optica Spectrum Disorder treatment therapies, analysis of Clinical Trials, Therapies, Mechanism of Action, Route of Administration, and Developments analyzes DelveInsight. (abnewswire.com)
- Companies across the globe are diligently working toward developing novel Neuromyelitis Optica Spectrum Disorder treatment therapies with a considerable amount of success over the years. (abnewswire.com)
Syndromes1
- Neuromyelitis optica is a subgroup of syndromes. (diagnosticdetectives.com)
Symptoms2
- Symptoms of neuromyelitis optica spectrum disorder include visual loss, muscle spasms, paraparesis or quadriparesis, and incontinence. (msdmanuals.com)
- México: hallazgo del Amblyomma cajennense influenza-like symptoms, which continued after his return naturalmente infectado en Veracruz. (cdc.gov)
Clinical trials2
- Q. What did the clinical trials of eculizumab in neuromyelitis optica show? (clevelandclinic.org)
- Emerging Neuromyelitis Optica Spectrum Disorder therapies in the different phases of clinical trials are- NDC-1308, AIM Biologicals, B001, LP-168, HBM9161, SHR1459, Telitacicept, Ravulizumab, and others are expected to have a significant impact on the Neuromyelitis Optica Spectrum Disorder market in the coming years. (abnewswire.com)
Assessment2
- The Neuromyelitis Optica Spectrum Disorder Pipeline report embraces in-depth commercial and clinical assessment of the pipeline products from the pre-clinical developmental phase to the marketed phase. (abnewswire.com)
- Neuromyelitis Optica Spectrum Disorder pipeline report provides the therapeutic assessment of the pipeline drugs by the Route of Administration. (abnewswire.com)
Lesions1
- On MRI, cerebral white matter lesions are uncommon in neuromyelitis optica, unlike in MS. (msdmanuals.com)
Years3
- The report's author has thoroughly examined the market and concluded that the Neuromyelitis Optica Drug Market's growth will level off in the coming years. (timestechpharma.com)
- The global Neuromyelitis Optica Drug Market research report is the well-analyzed solution for the decision-makers and academicians who are seeking a detailed analysis in terms of both qualitative as well as quantitative, for the historic period and for the upcoming years forecast. (timestechpharma.com)
- Kevin O Neil was diagnosed with Neuro Myelitis Optica 5 years ago and know just how disabling the condition can be, during several attacks he lost vision in both eyes and was paralysed from the waist down. (nmouk.nhs.uk)
Prominent1
- In addition to that, the prominent qualitative information added in the report includes Neuromyelitis Optica Drug Market trends, segmentation, key companies, SWOT, PORTER and PEST analysis, market maturity, value chain analysis, and others. (timestechpharma.com)
Form2
- There is a specific oriental form of the Neuromyelitis optica [NMO]. (diagnosticdetectives.com)
- There is also the Caucasian form of Neuromyelitis optica. (diagnosticdetectives.com)
Discussion1
- Read conversations, start a discussion, and connect with others about neuromyelitis optica. (neuromyelitis-optica.net)
Trial1
- Dr. Hopkins would also like to disclose that she's the site principal investigator for clinical trial of SA237 in neuromyelitis optica spectrum disorder. (cdc.gov)
Market2
- According to Ameco Research's Neuromyelitis Optica Drug Market report, The analysts took this into account when estimating the Neuromyelitis Optica Drug Market size and CAGR for the respective industry. (timestechpharma.com)
- The Neuromyelitis Optica Drug Market is finely segmented by considering the most important and responsive aspects of the respective market. (timestechpharma.com)