Nociceptive Pain
Neuralgia
Pain
Pain Measurement
Nociceptors
Chronic Pain
Pain Management
Low Back Pain
Back Pain
Neck Pain
Pelvic Pain
Facial Pain
Acute Pain
Pain, Referred
Shoulder Pain
Studies on pharmacological properties of mucus and sting venom of Potamotrygon cf. henlei. (1/54)
(+info)Relevance of mast cell-nerve interactions in intestinal nociception. (2/54)
(+info)Activation characteristics of transient receptor potential ankyrin 1 and its role in nociception. (3/54)
(+info)Substance P and calcitonin gene related peptide mediate pain in chronic pancreatitis and their expression is driven by nerve growth factor. (4/54)
CONTEXT: Calcitonin gene-related peptide (CGRP), substance P and nerve growth factor play an important role in inflammatory pain in various somatic pain models but their role in chronic pancreatitis has not been well studied. OBJECTIVES: The aim of this study was to investigate the effects of intrathecal administration of calcitonin gene-related peptide antagonist and substance P receptor antagonist on pain behavior in a rat model of chronic pancreatitis and to determine whether nerve growth factor drives the up-regulation of expression of these neuropeptides in sensory neurons. METHODS: Pancreatitis was induced by retrograde infusion of trinitobenzene sulfonic acid into the pancreatic duct of adult rats. Three weeks post infusion continuous intrathecal infusion of the calcitonin gene-related peptide antagonist alpha CGRP8-37 or neurokinin-1 receptor antagonist CP-96345 or its inactive enantiomer CP-96344 was administered for seven days. The effects of treatment on pancreatic hyperalgesia were assessed by sensitivity of the abdominal wall to von Frey filament probing as well as by the nocifensive response to electrical stimulation of the pancreas. In a separate experiment chronic pancreatitis was induced and pancreas specific dorsal root ganglion neurons labeled with DiI were assessed for calcitonin gene-related peptide and substance P immunoreactivity. RESULTS: Intrathecal infusion of calcitonin gene-related peptide and neurokinin-1 receptor antagonists significantly attenuated behavioral pain responses in rats with chronic pancreatitis. Further, treatment of chronic pancreatitis rats with nerve growth factor antibody significantly reduced pancreas specific neurons expressing calcitonin gene-related peptide and substance P in thoracic dorsal root ganglion. CONCLUSIONS: Calcitonin gene-related peptide and substance P mediate pancreatic hyperalgesia in chronic pancreatitis and nerve growth factor in turn sustains the up-regulation of these neuropeptides in pancreatic sensory neurons. (+info)What makes osteoarthritis painful? The evidence for local and central pain processing. (5/54)
(+info)In vivo responses of cutaneous C-mechanosensitive neurons in mouse to punctate chemical stimuli that elicit itch and nociceptive sensations in humans. (6/54)
(+info)Canadian guideline for safe and effective use of opioids for chronic noncancer pain: clinical summary for family physicians. Part 2: special populations. (7/54)
OBJECTIVE: To provide family physicians with a practical clinical summary of opioid prescribing for specific populations based on recommendations from the Canadian Guideline for Safe and Effective Use of Opioids for Chronic Non-Cancer Pain. QUALITY OF EVIDENCE: Researchers for the guideline conducted a systematic review of the literature, focusing on reviews of the effectiveness and safety of opioids in specific populations. MAIN MESSAGE: Family physicians can minimize the risks of overdose, sedation, misuse, and addiction through the use of strategies tailored to the age and health status of patients. For patients at high risk of addiction, opioids should be reserved for well-defined nociceptive or neuropathic pain conditions that have not responded to first-line treatments. Opioids should be titrated slowly, with frequent dispensing and close monitoring for signs of misuse. Suspected opioid addiction is managed with structured opioid therapy, methadone or buprenorphine treatment, or abstinence-based treatment. Patients with mood and anxiety disorders tend to have a blunted analgesic response to opioids, are at higher risk of misuse, and are often taking sedating drugs that interact adversely with opioids. Precautions similar to those for other high-risk patients should be employed. The opioid should be tapered if the patient's pain remains severe despite an adequate trial of opioid therapy. In the elderly, sedation, falls, and overdose can be minimized through lower initial doses, slower titration, benzodiazepine tapering, and careful patient education. For pregnant women taking daily opioid therapy, the opioids should be slowly tapered and discontinued. If this is not possible, they should be tapered to the lowest effective dose. Opioid-dependent pregnant women should receive methadone treatment. Adolescents are at high risk of opioid overdose, misuse, and addiction. Patients with adolescents living at home should store their opioid medication safely. Adolescents rarely require long-term opioid therapy. CONCLUSION: Family physicians must take into consideration the patient's age, psychiatric status, level of risk of addiction, and other factors when prescribing opioids for chronic pain. (+info)Central corticotropin-releasing factor (CRF) may attenuate somatic pain sensitivity through involvement of glucocorticoids. (8/54)
Corticotropin-releasing factor (CRF) is an important regulator of physiological functions and behavior in stress. Analgesia is one of the characteristics of stress reaction and CRF is involved in providing stress-induced analgesia, however, the underlying mechanisms remain to be determined. Exogenous CRF mimics stress effects on pain sensitivity and causes analgesic effect. The present study was performed to investigate the participation of endogenous glucocorticoids in analgesic effects induced by central administration of CRF in anesthetized rats. The participation of glucocorticoids was studied by pharmacological suppression of the hypothalamic-pituitary-adrenocortical (HPA) axis as well as an occupation of glucocorticoid receptors by its antagonist RU 38486. Since CRF administration causes the release of beta-endorphin from the pituitary, the opioid antagonist naltrexone was used to determine the contribution of opioid-dependent mechanism to CRF-induced analgesia. An electrical current threshold test was applied for measurement of somatic pain sensitivity in anesthetized rats. Intracerebroventricular administration of CRF (2 mug/rat) caused analgesic effects (an increase of pain thresholds) and an increase in plasma corticosterone levels. Pretreatment with naltrexone did not change analgesic effects of central CRF as well as corticosterone levels in blood plasma. However, pharmacological suppression of the HPA axis leading to an inability of corticosterone release in response to CRF resulted in an elimination of CRF-induced analgesic effects. Pretreatment with RU 38486 also resulted in an elimination of CRF-induced effects. The data suggest that CRF-induced analgesic effects may be mediated by nonopioid mechanism associated with endogenous glucocorticoids released in response to central CRF administration. (+info)Nociceptive pain is a type of pain that results from the activation of nociceptors, which are specialized sensory receptors located in various tissues throughout the body. These receptors detect potentially harmful stimuli such as extreme temperatures, pressure, or chemical irritants and transmit signals to the brain, which interprets them as painful sensations.
Nociceptive pain can be further classified into two categories:
1. Somatic nociceptive pain: This type of pain arises from the activation of nociceptors in the skin, muscles, bones, and joints. It is often described as sharp, aching, or throbbing and may be localized to a specific area of the body.
2. Visceral nociceptive pain: This type of pain arises from the activation of nociceptors in the internal organs, such as the lungs, heart, and digestive system. It is often described as deep, cramping, or aching and may be more diffuse and difficult to localize.
Examples of conditions that can cause nociceptive pain include injuries, arthritis, cancer, and infections. Effective management of nociceptive pain typically involves a multimodal approach that includes pharmacologic interventions, such as non-opioid analgesics, opioids, and adjuvant medications, as well as non-pharmacologic therapies, such as physical therapy, acupuncture, and cognitive-behavioral therapy.
Neuralgia is a type of pain that occurs along the pathway of a nerve, often caused by damage or irritation to the nerve. It is typically described as a sharp, stabbing, burning, or electric-shock like pain that can be severe and debilitating. Neuralgia can affect any nerve in the body, but it most commonly occurs in the facial area (trigeminal neuralgia) or in the nerves related to the spine (postherpetic neuralgia). The pain associated with neuralgia can be intermittent or constant and may be worsened by certain triggers such as touch, temperature changes, or movement. Treatment for neuralgia typically involves medications to manage pain, as well as other therapies such as nerve blocks, surgery, or lifestyle modifications.
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. It is a complex phenomenon that can result from various stimuli, such as thermal, mechanical, or chemical irritation, and it can be acute or chronic. The perception of pain involves the activation of specialized nerve cells called nociceptors, which transmit signals to the brain via the spinal cord. These signals are then processed in different regions of the brain, leading to the conscious experience of pain. It's important to note that pain is a highly individual and subjective experience, and its perception can vary widely among individuals.
Pain measurement, in a medical context, refers to the quantification or evaluation of the intensity and/or unpleasantness of a patient's subjective pain experience. This is typically accomplished through the use of standardized self-report measures such as numerical rating scales (NRS), visual analog scales (VAS), or categorical scales (mild, moderate, severe). In some cases, physiological measures like heart rate, blood pressure, and facial expressions may also be used to supplement self-reported pain ratings. The goal of pain measurement is to help healthcare providers better understand the nature and severity of a patient's pain in order to develop an effective treatment plan.
Pain threshold is a term used in medicine and research to describe the point at which a stimulus begins to be perceived as painful. It is an individual's subjective response and can vary from person to person based on factors such as their pain tolerance, mood, expectations, and cultural background.
The pain threshold is typically determined through a series of tests where gradually increasing levels of stimuli are applied until the individual reports feeling pain. This is often used in research settings to study pain perception and analgesic efficacy. However, it's important to note that the pain threshold should not be confused with pain tolerance, which refers to the maximum level of pain a person can endure.
Nociceptors are specialized peripheral sensory neurons that detect and transmit signals indicating potentially harmful stimuli in the form of pain. They are activated by various noxious stimuli such as extreme temperatures, intense pressure, or chemical irritants. Once activated, nociceptors transmit these signals to the central nervous system (spinal cord and brain) where they are interpreted as painful sensations, leading to protective responses like withdrawing from the harmful stimulus or seeking medical attention. Nociceptors play a crucial role in our perception of pain and help protect the body from further harm.
Analgesics are a class of drugs that are used to relieve pain. They work by blocking the transmission of pain signals in the nervous system, allowing individuals to manage their pain levels more effectively. There are many different types of analgesics available, including both prescription and over-the-counter options. Some common examples include acetaminophen (Tylenol), ibuprofen (Advil or Motrin), and opioids such as morphine or oxycodone.
The choice of analgesic will depend on several factors, including the type and severity of pain being experienced, any underlying medical conditions, potential drug interactions, and individual patient preferences. It is important to use these medications as directed by a healthcare provider, as misuse or overuse can lead to serious side effects and potential addiction.
In addition to their pain-relieving properties, some analgesics may also have additional benefits such as reducing inflammation (like in the case of nonsteroidal anti-inflammatory drugs or NSAIDs) or causing sedation (as with certain opioids). However, it is essential to weigh these potential benefits against the risks and side effects associated with each medication.
When used appropriately, analgesics can significantly improve a person's quality of life by helping them manage their pain effectively and allowing them to engage in daily activities more comfortably.
Chronic pain is defined as pain that persists or recurs for a period of 3 months or longer, beyond the normal healing time for an injury or illness. It can be continuous or intermittent and range from mild to severe. Chronic pain can have various causes, such as nerve damage, musculoskeletal conditions, or chronic diseases like cancer. It can significantly impact a person's quality of life, causing limitations in mobility, sleep disturbances, mood changes, and decreased overall well-being. Effective management of chronic pain often involves a multidisciplinary approach, including medications, physical therapy, psychological interventions, and complementary therapies.
Pain management is a branch of medicine that focuses on the diagnosis and treatment of pain and improvement in the quality of life of patients with chronic pain. The goal of pain management is to reduce pain levels, improve physical functioning, and help patients cope mentally and emotionally with their pain. This may involve the use of medications, interventional procedures, physical therapy, psychological therapy, or a combination of these approaches.
The definition of pain management can vary depending on the medical context, but it generally refers to a multidisciplinary approach that addresses the complex interactions between biological, psychological, and social factors that contribute to the experience of pain. Pain management specialists may include physicians, nurses, physical therapists, psychologists, and other healthcare professionals who work together to provide comprehensive care for patients with chronic pain.
Postoperative pain is defined as the pain or discomfort experienced by patients following a surgical procedure. It can vary in intensity and duration depending on the type of surgery performed, individual pain tolerance, and other factors. The pain may be caused by tissue trauma, inflammation, or nerve damage resulting from the surgical intervention. Proper assessment and management of postoperative pain is essential to promote recovery, prevent complications, and improve patient satisfaction.
Low back pain is a common musculoskeletal disorder characterized by discomfort or pain in the lower part of the back, typically between the costal margin (bottom of the ribcage) and the gluteal folds (buttocks). It can be caused by several factors including strain or sprain of the muscles or ligaments, disc herniation, spinal stenosis, osteoarthritis, or other degenerative conditions affecting the spine. The pain can range from a dull ache to a sharp stabbing sensation and may be accompanied by stiffness, limited mobility, and radiating pain down the legs in some cases. Low back pain is often described as acute (lasting less than 6 weeks), subacute (lasting between 6-12 weeks), or chronic (lasting more than 12 weeks).
Back pain is a common symptom characterized by discomfort or soreness in the back, often occurring in the lower region of the back (lumbago). It can range from a mild ache to a sharp stabbing or shooting pain, and it may be accompanied by stiffness, restricted mobility, and difficulty performing daily activities. Back pain is typically caused by strain or sprain to the muscles, ligaments, or spinal joints, but it can also result from degenerative conditions, disc herniation, spinal stenosis, osteoarthritis, or other medical issues affecting the spine. The severity and duration of back pain can vary widely, with some cases resolving on their own within a few days or weeks, while others may require medical treatment and rehabilitation.
Abdominal pain is defined as discomfort or painful sensation in the abdomen. The abdomen is the region of the body between the chest and the pelvis, and contains many important organs such as the stomach, small intestine, large intestine, liver, gallbladder, pancreas, and spleen. Abdominal pain can vary in intensity from mild to severe, and can be acute or chronic depending on the underlying cause.
Abdominal pain can have many different causes, ranging from benign conditions such as gastritis, indigestion, or constipation, to more serious conditions such as appendicitis, inflammatory bowel disease, or abdominal aortic aneurysm. The location, quality, and duration of the pain can provide important clues about its cause. For example, sharp, localized pain in the lower right quadrant of the abdomen may indicate appendicitis, while crampy, diffuse pain in the lower abdomen may suggest irritable bowel syndrome.
It is important to seek medical attention if you experience severe or persistent abdominal pain, especially if it is accompanied by other symptoms such as fever, vomiting, or bloody stools. A thorough physical examination, including a careful history and a focused abdominal exam, can help diagnose the underlying cause of the pain and guide appropriate treatment.
Neck pain is discomfort or soreness in the neck region, which can extend from the base of the skull to the upper part of the shoulder blades, caused by injury, irritation, or inflammation of the muscles, ligaments, or nerves in the cervical spine. The pain may worsen with movement and can be accompanied by stiffness, numbness, tingling, or weakness in the neck, arms, or hands. In some cases, headaches can also occur as a result of neck pain.
In medicine, "intractable pain" is a term used to describe pain that is difficult to manage, control or relieve with standard treatments. It's a type of chronic pain that continues for an extended period, often months or even years, and does not respond to conventional therapies such as medications, physical therapy, or surgery. Intractable pain can significantly affect a person's quality of life, causing emotional distress, sleep disturbances, and reduced mobility. It is essential to distinguish intractable pain from acute pain, which is typically sharp and short-lived, resulting from tissue damage or inflammation.
Intractable pain may be classified as:
1. Refractory pain: Pain that persists despite optimal treatment with various modalities, including medications, interventions, and multidisciplinary care.
2. Incurable pain: Pain caused by a progressive or incurable disease, such as cancer, for which no curative treatment is available.
3. Functional pain: Pain without an identifiable organic cause that does not respond to standard treatments.
Managing intractable pain often requires a multidisciplinary approach involving healthcare professionals from various fields, including pain specialists, neurologists, psychiatrists, psychologists, and physical therapists. Treatment options may include:
1. Adjuvant medications: Medications that are not primarily analgesics but have been found to help with pain relief, such as antidepressants, anticonvulsants, and muscle relaxants.
2. Interventional procedures: Minimally invasive techniques like nerve blocks, spinal cord stimulation, or intrathecal drug delivery systems that target specific nerves or areas of the body to reduce pain signals.
3. Psychological interventions: Techniques such as cognitive-behavioral therapy (CBT), mindfulness meditation, and relaxation training can help patients cope with chronic pain and improve their overall well-being.
4. Physical therapy and rehabilitation: Exercise programs, massage, acupuncture, and other physical therapies may provide relief for some types of intractable pain.
5. Complementary and alternative medicine (CAM): Techniques like yoga, tai chi, hypnosis, or biofeedback can be helpful in managing chronic pain.
6. Lifestyle modifications: Dietary changes, stress management, and quitting smoking may also contribute to improved pain management.
Pelvic pain is defined as discomfort or unpleasant sensation in the lower abdominal region, below the belly button, and between the hips. It can be acute (sudden and lasting for a short time) or chronic (persisting for months or even years), and it may be steady or intermittent, mild or severe. The pain can have various causes, including musculoskeletal issues, nerve irritation, infection, inflammation, or organic diseases in the reproductive, urinary, or gastrointestinal systems. Accurate diagnosis often requires a thorough medical evaluation to determine the underlying cause and develop an appropriate treatment plan.
Pain perception refers to the neural and psychological processes involved in receiving, interpreting, and responding to painful stimuli. It is the subjective experience of pain, which can vary greatly among individuals due to factors such as genetics, mood, expectations, and past experiences. The perception of pain involves complex interactions between the peripheral nervous system (which detects and transmits information about tissue damage or potential harm), the spinal cord (where this information is processed and integrated with other sensory inputs), and the brain (where the final interpretation and emotional response to pain occurs).
Facial pain is a condition characterized by discomfort or pain felt in any part of the face. It can result from various causes, including nerve damage or irritation, injuries, infections, dental problems, migraines, or sinus congestion. The pain can range from mild to severe and may be sharp, dull, constant, or intermittent. In some cases, facial pain can also be associated with other symptoms such as headaches, redness, swelling, or changes in sensation. Accurate diagnosis and treatment of the underlying cause are essential for effective management of facial pain.
Acute pain is a type of pain that comes on suddenly and can be severe, but it typically lasts for a short period of time. It is often described as sharp or stabbing and can be caused by tissue damage, inflammation, or injury. Acute pain is the body's way of signaling that something is wrong and that action needs to be taken to address the underlying cause.
Acute pain is different from chronic pain, which is pain that persists for 12 weeks or longer. Chronic pain can be caused by a variety of factors, including ongoing medical conditions, nerve damage, or inflammation. It is important to seek medical attention if you are experiencing acute pain that does not improve or becomes severe, as it may be a sign of a more serious underlying condition.
Referred pain is a type of pain that is felt in a part of the body other than its actual source. This occurs because the brain incorrectly interprets nerve signals from damaged tissues or organs. In the case of referred pain, the brain misinterprets the location of the pain signal and attributes it to a different area of the body.
Referred pain is often described as a dull, aching sensation rather than a sharp, stabbing pain. It can be difficult to diagnose because the source of the pain may not be immediately apparent. Common examples of referred pain include:
* Heart attack pain that is felt in the left arm or jaw
* Gallbladder pain that is felt in the right shoulder blade
* Kidney stones that cause pain in the lower back and abdomen
* Appendicitis that causes pain in the lower right quadrant of the abdomen, but can sometimes be referred to the lower left quadrant in pregnant women or those with a longer colon.
Referred pain is thought to occur because the nerves carrying pain signals from different parts of the body converge on the same neurons in the spinal cord before traveling to the brain. If these neurons are stimulated by pain signals from multiple sources, the brain may have difficulty distinguishing between them and may interpret the pain as coming from a single location.
Shoulder pain is a condition characterized by discomfort or hurt in the shoulder joint, muscles, tendons, ligaments, or surrounding structures. The shoulder is one of the most mobile joints in the body, and this mobility makes it prone to injury and pain. Shoulder pain can result from various causes, including overuse, trauma, degenerative conditions, or referred pain from other areas of the body.
The shoulder joint is a ball-and-socket joint made up of three bones: the humerus (upper arm bone), scapula (shoulder blade), and clavicle (collarbone). The rotator cuff, a group of four muscles that surround and stabilize the shoulder joint, can also be a source of pain if it becomes inflamed or torn.
Shoulder pain can range from mild to severe, and it may be accompanied by stiffness, swelling, bruising, weakness, numbness, tingling, or reduced mobility in the affected arm. The pain may worsen with movement, lifting objects, or performing certain activities, such as reaching overhead or behind the back.
Medical evaluation is necessary to determine the underlying cause of shoulder pain and develop an appropriate treatment plan. Treatment options may include rest, physical therapy, medication, injections, or surgery, depending on the severity and nature of the condition.
Musculoskeletal pain is discomfort or pain that affects the muscles, bones, ligaments, tendons, and nerves. It can be caused by injury, overuse, or disease and can affect any part of the body, including the neck, back, shoulders, hips, and extremities. The pain can range from mild to severe and may be accompanied by stiffness, swelling, and decreased range of motion. Common causes of musculoskeletal pain include arthritis, fibromyalgia, tendinitis, bursitis, and muscle or ligament strain. Treatment for musculoskeletal pain depends on the underlying cause and may include physical therapy, medication, and in some cases, surgery.
 Nociceptive trigeminal inhibition tension suppression system
Nociceptive trigeminal inhibition tension suppression system Dual Piperidine-Based Histamine H and Sigma-1 Receptor Ligands in the Treatment of Nociceptive and Neuropathic Pain. -...
Dual Piperidine-Based Histamine H and Sigma-1 Receptor Ligands in the Treatment of Nociceptive and Neuropathic Pain. -... Widespread nociceptive maps in the human neonatal somatosensory cortex | eLife
Widespread nociceptive maps in the human neonatal somatosensory cortex | eLife The effect of a chromogranin A-derived peptide (CgA4-16) in the writhing nociceptive response induced by acetic acid in rats
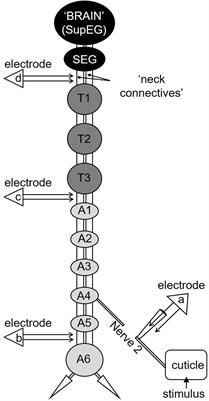
The effect of a chromogranin A-derived peptide (CgA4-16) in the writhing nociceptive response induced by acetic acid in rats Frontiers | Nociceptive Pathway in the Cockroach Periplaneta americana
Frontiers | Nociceptive Pathway in the Cockroach Periplaneta americana Nociceptive Pain
Nociceptive Pain Nociceptive Pain Archives - allvapestores.com
Nociceptive Pain Archives - allvapestores.com Nociceptive Sensitization Group | Berner Fachhochschule
Nociceptive Sensitization Group | Berner Fachhochschule Somatic and Visceral Nociceptive Pain | Clinique Sante & Physique
Somatic and Visceral Nociceptive Pain | Clinique Sante & Physique What is Nociceptive Pain? - Pain Patient Advocacy Australia
What is Nociceptive Pain? - Pain Patient Advocacy Australia Categories of Pain - Neuropathic vs. Nociceptive - YouTube | Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia...
Categories of Pain - Neuropathic vs. Nociceptive - YouTube | Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia... Low Back Pain: Nociceptive capacity of the thoracolumbar fascia
- Osteopathybooks
Low Back Pain: Nociceptive capacity of the thoracolumbar fascia
- Osteopathybooks Modulation of heat-evoked nociceptive withdrawal reflexes by painful intramuscular conditioning stimulation in man
-...
Modulation of heat-evoked nociceptive withdrawal reflexes by painful intramuscular conditioning stimulation in man
-... A new look at arthritis management: nociceptive reflex excitability as a pain biomarker | Arthritis Research & Therapy | Full...
A new look at arthritis management: nociceptive reflex excitability as a pain biomarker | Arthritis Research & Therapy | Full... Minimal Blocking Concentrations of Bupivacaine and Procaine in an Exclusively Nociceptive System in Humans | Regional...
Minimal Blocking Concentrations of Bupivacaine and Procaine in an Exclusively Nociceptive System in Humans | Regional... PDF) Critical review on pharmacological properties of Brahmi
PDF) Critical review on pharmacological properties of Brahmi A Peripherally Restricted Cannabinoid Receptor Agonist Produces Robust Anti-Nociceptive Effects In Rodent Models Of...
A Peripherally Restricted Cannabinoid Receptor Agonist Produces Robust Anti-Nociceptive Effects In Rodent Models Of... Influence of behavioral traits in the inter-individual variability of nociceptive, emotional and cognitive manifestations of...
Influence of behavioral traits in the inter-individual variability of nociceptive, emotional and cognitive manifestations of... Diabetic Neuropathy: Practice Essentials, Background, Anatomy
Diabetic Neuropathy: Practice Essentials, Background, Anatomy IJMS | Free Full-Text | Ion Channels Involved in Tooth Pain
IJMS | Free Full-Text | Ion Channels Involved in Tooth Pain Systemic desensitization through TRPA1 channels by capsazepine and mustard oil - a novel strategy against inflammation and pain...
Systemic desensitization through TRPA1 channels by capsazepine and mustard oil - a novel strategy against inflammation and pain...










![Buy Finalgon® [Nicoboxil, Nonivamide]](https://pillbuys.com/24086-large_default/finalgon-nicoboxil-nonivamide-.jpg)