Paraneoplastic Syndromes
Paraneoplastic Syndromes, Nervous System
Paraneoplastic Polyneuropathy
Paraneoplastic Cerebellar Degeneration
Lambert-Eaton Myasthenic Syndrome
Paraneoplastic Syndromes, Ocular
Osteoarthropathy, Secondary Hypertrophic
Inappropriate ADH Syndrome
Paraneoplastic Endocrine Syndromes
Encephalomyelitis
Myxosarcoma
Limbic Encephalitis
Cerebellar Diseases
Thymoma
Ocular Motility Disorders
Endocrine System Diseases
Polymyositis
Fatal Outcome
Nervous System Diseases
Recoverin
Parathyroid Hormone-Related Protein
Autoantibodies
Dermatomyositis
Carcinoma, Small Cell
Neuromuscular Diseases
Hu Paraneoplastic Encephalomyelitis Antigens
Stiff-Person Syndrome
Opsoclonus-Myoclonus Syndrome
Ma1, a novel neuron- and testis-specific protein, is recognized by the serum of patients with paraneoplastic neurological disorders. (1/335)
The identification of antineuronal antibodies has facilitated the diagnosis of paraneoplastic neurological disorders and the early detection of the associated tumours. It has also led to the cloning of possibly important neuron-specific proteins. In this study we wanted to identify novel antineuronal antibodies in the sera of patients with paraneoplastic neurological disorders and to clone the corresponding antigens. Serological studies of 1705 sera from patients with suspected paraneoplastic neurological disorders resulted in the identification of four patients with antibodies that reacted with 37 and 40 kDa neuronal proteins (anti-Ma antibodies). Three patients had brainstem and cerebellar dysfunction, and one had dysphagia and motor weakness. Autopsy of two patients showed loss of Purkinje cells, Bergmann gliosis and deep cerebellar white matter inflammatory infiltrates. Extensive neuronal degeneration, gliosis and infiltrates mainly composed of CD8+ T cells were also found in the brainstem of one patient. In normal human and rat tissues, the anti-Ma antibodies reacted exclusively with neurons and with testicular germ cells; the reaction was mainly with subnuclear elements (including the nucleoli) and to a lesser degree the cytoplasm. Anti-Ma antibodies also reacted with the cancers (breast, colon and parotid) available from three anti-Ma patients, but not with 66 other tumours of varying histological types. Preincubation of tissues with any of the anti-Ma sera abrogated the reactivity of the other anti-Ma immunoglobulins. Probing of a human complementary DNA library with anti-Ma serum resulted in the cloning of a gene that encodes a novel 37 kDa protein (Mal). Recombinant Mal was specifically recognized by the four anti-Ma sera but not by 337 control sera, including those from 52 normal individuals, 179 cancer patients without paraneoplastic neurological symptoms, 96 patients with paraneoplastic syndromes and 10 patients with non-cancer-related neurological disorders. The expression of Mal mRNA is highly restricted to the brain and testis. Subsequent analysis suggested that Mal is likely to be a phosphoprotein. Our study demonstrates that some patients with paraneoplastic neurological disorders develop antibodies against Mal, a new member of an expanding family of 'brain/testis' proteins. (+info)Anti-amphiphysin I antibodies in patients with paraneoplastic neurological disorders associated with small cell lung carcinoma. (2/335)
Patients with stiff man syndrome and breast cancer develop anti-amphiphysin I antibodies that primarily recognise the C terminus of the protein. Anti-amphiphysin I antibodies have also been identified in a few patients with paraneoplastic neurological disorders (PND) and small cell lung cancer (SCLC). The frequency of anti-amphiphysin I antibodies in patients with SCLC and PND was analysed and the epitope specificity of these antibodies was characterised. Anti-amphiphysin I antibodies were evaluated by immunohistochemistry on human and rat cerebellum and immunoblots of rat brain homogenates. Serum samples included 134 patients with PND and anti-Hu antibodies (83% had SCLC), 44 with SCLC and PND without anti-Hu-antibodies, 63 with PND and either Yo, Ri, or Tr antibodies, 146 with SCLC without PND, and 104 with non-PND. Positive serum samples were confirmed with immunoblots of recombinant human amphiphysin I and immunoreacted with five overlapping peptide fragments covering the full length of the molecule. Serum samples positive for anti-amphiphysin I antibodies included those from seven (2.9%) patients with PND and two (1.4%) with SCLC without PND. Six of the seven anti-amphiphysin I antibody positive patients with PND had SCLC (three with Hu-antibodies), and one had anti-Hu-antibodies but no detectable tumour. The PND included encephalomyelitis/sensory neuropathy (five patients), cerebellar degeneration (one), and opsoclonus (one). All anti-amphiphysin I antibodies reacted with the C terminus of amphiphysin I, but seven also recognised other fragments of the molecule. In conclusion, anti-amphiphysin I antibodies are present at low frequency in patients with SCLC irrespective of the presence of an associated PND. All anti-amphiphysin I antibody positive serum samples have in common reactivity with the C terminus of the protein. (+info)Envoplakin and periplakin are the paraneoplastic pemphigus antigens. (3/335)
Paraneoplastic pemphigus (PNP) sera have been reported to immunoprecipitate multiple proteins, including the 250 kDa and 210 kDa proteins believed to correspond to desmoplakins I/II, BP230, and two unidentified proteins of 190 kDa and 170 kDa. We have recently provided evidence that the presence of the 210 kDa and 190 kDa proteins is the most prominent feature of PNP, and have suggested that the major 210 kDa antigen may not correspond to desmoplakin II. Using immunoprecipitation and immunoblotting, we found that some PNP sera identified a doublet protein migrating at 210 kDa, with the larger protein corresponding to desmoplakin II, and the smaller protein corresponding to envoplakin, a recently described precursor of the keratinocyte cornified envelope. In contrast to desmoplakin II, envoplakin was detected by all PNP sera analyzed. Using immunoblotting and immunoprecipitation, we further showed that the 190 kDa PNP antigen is identical to periplakin, another recently identified envelope precursor that can form complexes with envoplakin. Like desmoplakin and BP230, envoplakin and periplakin belong to the plakin family of proteins. (+info)Small intestinal ulceration secondary to carcinoid tumour arising in a Meckel's diverticulum. (4/335)
A solitary small intestinal ulcer associated with a carcinoid tumour in a nearby Meckel's diverticulum was found in a 77 year old man presenting with massive rectal bleeding. Angiography and a radioisotope study localised the bleeding to the ileum. At operation, the Meckel's diverticulum was identified, with bleeding from an ulcer just distal to it. Pathological examination revealed a small carcinoid tumour confined to the Meckel's diverticulum. Close to the opening of the diverticulum, within the ileum, a well demarcated ulcer was present. Histology showed a non-specific ulcer which eroded a large blood vessel. This is the first documented occurrence of solitary small intestinal ulceration in association with a carcinoid tumour. Carcinoid tumour should be added to the list of possible causes of small intestinal ulceration. The ulceration may be secondary to release of cytokines by the tumour. (+info)Constrictive bronchiolitis obliterans and paraneoplastic pemphigus. (5/335)
Constrictive bronchiolitis obliterans is rare, and the pathogenesis of the disease often remains unknown. This study reports on the case of a 38 yr-old female with constrictive bronchiolitis obliterans and paraneoplastic pemphigus associated with malignant lymphoma. The patient developed progressive obstructive lung disease. The chest radiograph showed almost normal lungs. Paraneoplastic pemphigus is a newly described syndrome in which patients have autoantibodies binding to some epithelia, including in the respiratory tract. The disease develops in association with non-Hodgkin's lymphomas or other malignant neoplasms. The case presented here suggests that constrictive bronchiolitis obliterans associated with paraneoplastic pemphigus may be one of the facets of autoimmune responses in this context. (+info)A serologic marker of paraneoplastic limbic and brain-stem encephalitis in patients with testicular cancer. (6/335)
BACKGROUND: In patients with cancer, symptoms of limbic and brain-stem dysfunction may result from a paraneoplastic disorder. Paraneoplastic limbic or brain-stem encephalitis occurs more frequently with testicular cancer than with most other cancers. We sought antineuronal antibodies that might be used in a diagnostic test for this syndrome. METHODS: Immunohistochemical and immunoblotting techniques were used to detect serum and cerebrospinal fluid antibodies. Serologic screening of a complementary DNA library and Northern blotting were used to clone the target antigen and determine which tissues expressed it. RESULTS: Of 13 patients with testicular cancer and paraneoplastic limbic or brain-stem encephalitis (or both), 10 had antibodies in serum and cerebrospinal fluid against a 40-kd neuronal protein. These antibodies were used to clone a gene that we call Ma2, which codes for a protein (Ma2) that was recognized by serum from the 10 patients, but not by serum from 344 control subjects. Ma2 was selectively expressed by normal brain tissue and by the testicular tumors of the patients. Ma2 shares homology with Ma1, a "brain-testis-cancer" gene related to other paraneoplastic syndromes and tumors. CONCLUSIONS: The serum of patients with subacute limbic and brain-stem dysfunction and testicular cancer contains antibodies against a protein found in normal brain and in testicular tumors. Detection of these antibodies supports the paraneoplastic origin of the neurologic disorder and could be of diagnostic importance. (+info)Carcinoma associated paraneoplastic peripheral neuropathies in patients with and without anti-onconeural antibodies. (7/335)
OBJECTIVE: When to suspect a paraneoplastic disorder is a puzzling problem that has not recently been studied in a large series of patients referred for peripheral neuropathy. METHODS: From 422 consecutive patients with peripheral neuropathy, 26 were analysed who concomitantly had carcinoma but no tumorous infiltration, drug toxicity, or cachexia. Their clinical, pathological, and electrophysiological data were analysed according to the presence of anti-onconeural antibodies, the latency between presentation and cancer diagnosis, and the incidence of carcinoma in the corresponding types of neuropathy of the population of 422 patients. RESULTS: Seven patients (group I) had anti-onconeural antibodies (six anti-Hu, one anti-CV2) and 19 did not (groups IIA and B). In group I, subacute sensory neuropathy (SSN) was the most frequent but other neuropathies including demyelinating neuropathies were present. Patients in group II A had a short latency (mean 7.88 months), and a rapidly and usually severe neuropathy which corresponded in 11/14 to an established inflammatory disorder including neuropathy with encephalomyelitis, mononeuritis multiplex, and acute or chronic inflammatory demyelinating polyneuropathy (CIDP). Patients in group IIB had a long latency (mean 8.4 years) and a very chronic disorder corresponding in four of five to an axonal non-inflammatory polyneuropathy. In this population, the incidence of carcinoma occurring with a short latency was 47% in sensory neuronopathy, 1.7% in Guillain-Barre syndrome, 10% in mononeuritis multiplex and CIDP, and 4.5% in axonal polyneuropathy. CONCLUSIONS: Paraneoplastic neuropathies associated with carcinoma are heterogeneous disorders. Neuropathies occurring with a long latency with tumours probably resulted from a coincidental association. Neuropathies which occurred within a few years of the tumour evolved rapidly and corresponded mostly to inflammatory disorders. As dysimmune neuropathies are probably paraneoplastic in a limited number of cases, patients with these disorders should probably not be investigated systematically for carcinoma in the absence of anti-onconeural antibodies, except when the neuropathy is associated with encephalomyelitis and probably with vasculitis. Questions remain concerning CIDP. (+info)Cancer-associated retinopathy during treatment for small-cell lung carcinoma. (8/335)
A 70-year-old woman with small-cell lung carcinoma (c-T4N2M0) was treated by six courses of combination chemotherapy (carboplatin and etoposide). After two weeks, she complained of a sense of darkness and night blindness. A Western blot analysis showed that the patient's serum bound with the recombinant 23-kDa retinal cancer-associated retinopathy (CAR) antigen at 1:1,000 dilution. Her visual acuity became so poor that she could only recognise a hand motion at 50 cm despite treatment with corticosteroids and combination chemotherapy. The patient was diagnosed as having a rare type of CAR because CAR is usually found before the diagnosis of primary cancer. (+info)Paraneoplastic syndromes refer to a group of rare disorders that are caused by an abnormal immune system response to a cancerous (malignant) tumor. These syndromes are characterized by symptoms or signs that do not result directly from the growth of the tumor itself, but rather from substances produced by the tumor or the body's immune system in response to the tumor.
Paraneoplastic syndromes can affect various organs and systems in the body, including the nervous system, endocrine system, skin, and joints. Examples of paraneoplastic syndromes include Lambert-Eaton myasthenic syndrome (LEMS), which affects nerve function and causes muscle weakness; cerebellar degeneration, which can cause difficulty with coordination and balance; and dermatomyositis, which is an inflammatory condition that affects the skin and muscles.
Paraneoplastic syndromes can occur in association with a variety of different types of cancer, including lung cancer, breast cancer, ovarian cancer, and lymphoma. Treatment typically involves addressing the underlying cancer, as well as managing the symptoms of the paraneoplastic syndrome.
Paraneoplastic syndromes of the nervous system are a group of rare disorders that occur in some individuals with cancer. These syndromes are caused by an immune system response to the cancer tumor, which can lead to the damage or destruction of nerve cells. The immune system produces antibodies and/or activated immune cells that attack the neural tissue, leading to neurological symptoms.
Paraneoplastic syndromes can affect any part of the nervous system, including the brain, spinal cord, peripheral nerves, and muscles. Symptoms vary depending on the specific syndrome and the location of the affected nerve tissue. Some common neurological symptoms include muscle weakness, numbness or tingling, seizures, memory loss, confusion, difficulty speaking or swallowing, visual disturbances, and coordination problems.
Paraneoplastic syndromes are often associated with specific types of cancer, such as small cell lung cancer, breast cancer, ovarian cancer, and lymphoma. Diagnosis can be challenging because the symptoms may precede the discovery of the underlying cancer. A combination of clinical evaluation, imaging studies, laboratory tests, and sometimes a brain biopsy may be necessary to confirm the diagnosis.
Treatment typically involves addressing the underlying cancer with surgery, chemotherapy, or radiation therapy. Immunosuppressive therapies may also be used to manage the immune response that is causing the neurological symptoms. While treatment can help alleviate symptoms and improve quality of life, paraneoplastic syndromes are often difficult to cure completely.
Paraneoplastic polyneuropathy is a rare neurological disorder that can occur in some individuals with cancer. It's caused by the immune system producing antibodies or cells that attack the nervous system (neurons, nerve axons, or myelin sheath) as a response to the presence of a tumor or cancer in the body.
The term "polyneuropathy" refers to damage or dysfunction affecting multiple peripheral nerves simultaneously. This can lead to various symptoms such as numbness, tingling, muscle weakness, and pain, typically starting in the hands and feet and progressing upwards.
In paraneoplastic polyneuropathy, these symptoms are related to the immune system's response to the cancer rather than direct invasion of the nerves by the tumor itself. The specific type of polyneuropathy can vary between individuals, and it may present as sensorimotor polyneuropathy, autonomic neuropathy, or a combination of both.
Early diagnosis and treatment of the underlying cancer are crucial for managing paraneoplastic polyneuropathy. Immunotherapy, plasma exchange, and intravenous immunoglobulin may be used to help control the immune response and alleviate symptoms.
Paraneoplastic cerebellar degeneration (PCD) is a rare disorder characterized by progressive damage to the cerebellum, the part of the brain responsible for coordinating muscle movements. It is considered a paraneoplastic syndrome, which means it is caused by an abnormal immune system response to a cancerous tumor (neoplasm) located elsewhere in the body.
In PCD, antibodies produced by the immune system to fight the tumor mistakenly attack proteins in the cerebellum that are similar to those found in the tumor. This leads to inflammation and degeneration of the Purkinje cells, a type of neuron critical for maintaining balance and coordinating movements.
PCD can present with symptoms such as unsteady gait, loss of coordination, slurred speech, nystagmus (involuntary eye movement), and tremors. These symptoms often develop rapidly, over the course of days to weeks, and may progress even after the tumor has been removed or treated.
PCD is associated with several types of cancers, including small cell lung cancer, breast cancer, ovarian cancer, Hodgkin's lymphoma, and others. Early diagnosis and treatment of the underlying cancer are essential to slowing down the progression of PCD and improving outcomes.
Lambert-Eaton Myasthenic Syndrome (LEMS) is a rare autoimmune disorder characterized by muscle weakness and fatigability. It is caused by the presence of antibodies against voltage-gated calcium channels (VGCC) in the neuromuscular junction, which disrupts the normal transmission of signals between nerves and muscles.
The symptoms of LEMS include proximal muscle weakness, which may affect the legs more than the arms, and autonomic dysfunction such as dry mouth and constipation. The weakness tends to improve with exercise but worsens after periods of rest. In some cases, LEMS can be associated with cancer, particularly small cell lung cancer.
Diagnosis of LEMS typically involves a combination of clinical evaluation, electromyography (EMG) studies, and blood tests to detect VGCC antibodies. Treatment may include medications such as pyridostigmine, which improves neuromuscular transmission, or intravenous immunoglobulin and plasma exchange, which help to reduce the immune response. In cases where LEMS is associated with cancer, treatment of the underlying malignancy can also improve muscle strength and function.
Paraneoplastic syndromes are a group of rare disorders that occur in some individuals with cancer. These syndromes are caused by substances produced by the tumor or the body's immune response to the tumor, which can affect distant organs and cause various symptoms.
Ocular paraneoplastic syndromes refer to a subset of these disorders that specifically affect the eyes. They are caused by an abnormal immune response directed against antigens shared by both the tumor and the nervous tissue of the eye. This results in damage to the nerve cells and can lead to various visual symptoms, such as:
1. Visual loss or blurring
2. Double vision (diplopia)
3. Light sensitivity (photophobia)
4. Abnormalities in pupil size or reactivity
5. Jerky eye movements (nystagmus)
6. Loss of peripheral vision (visual field defects)
7. Impaired color vision
8. Deterioration of the optic nerve (optic neuropathy)
Some examples of ocular paraneoplastic syndromes include:
1. Paraneoplastic retinopathy: A condition characterized by damage to the light-sensitive cells in the retina, leading to visual loss and other visual disturbances.
2. Paraneoplastic optic neuropathy: Damage to the optic nerve that can result in visual loss and visual field defects.
3. Cancer-associated retinopathy (CAR): A condition characterized by progressive vision loss, night blindness, and abnormalities in the electroretinogram (ERG), a test used to assess retinal function.
4. Melanoma-associated retinopathy (MAR): Similar to CAR but specifically associated with melanoma, this condition can cause visual loss, night blindness, and abnormal ERG results.
5. Opsoclonus-myoclonus syndrome: A rare disorder characterized by rapid, involuntary eye movements (opsoclonus) and muscle jerks (myoclonus), which can be associated with various types of cancer, including breast, lung, and ovarian cancer.
It is important to note that these conditions are relatively rare but can significantly impact a patient's quality of life. Early diagnosis and treatment of the underlying cancer can help improve outcomes for patients with ocular paraneoplastic syndromes.
Secondary hyertrophic osteoarthropathy, also known as secondary musculoskeletal hypertrophy or Pierre Marie-Bamberger syndrome, is a condition characterized by the proliferation of new bone formation (osteophytes) and thickening of the bones (hyertrophy) in the joints, typically affecting the hands and feet. This condition is a reactive process that occurs as a secondary response to an underlying medical disorder, most commonly chronic hypoxia or ischemia due to conditions such as chronic obstructive pulmonary disease (COPD), cyanotic congenital heart disease, or malignancy.
The exact pathophysiology of this condition is not fully understood, but it is thought to be related to the release of growth factors and cytokines in response to the underlying medical disorder. The clinical manifestations of secondary hyertrophic osteoarthropathy include joint pain, swelling, stiffness, and limited range of motion, as well as characteristic radiographic findings such as periostitis, bone resorption, and new bone formation.
Treatment of this condition involves addressing the underlying medical disorder and providing supportive care for the musculoskeletal symptoms. This may include pain management, physical therapy, and orthopedic interventions as needed.
Inappropriate Antidiuretic Hormone (ADH) Syndrome, also known as the Syndrome of Inappropriate Antidiuresis (SIAD), is a condition characterized by the excessive release or action of antidiuretic hormone (ADH) leading to an imbalance of water and electrolytes in the body.
ADH is a hormone produced by the pituitary gland that helps regulate water balance in the body by controlling the amount of urine produced by the kidneys. In normal conditions, ADH levels increase in response to dehydration or decreased blood volume, causing the kidneys to retain water and decrease urine output.
However, in Inappropriate ADH Syndrome, there is an overproduction or inappropriate release of ADH, even when the body does not need it. This can lead to a condition called hyponatremia, which is low sodium levels in the blood. Hyponatremia can cause symptoms such as headache, confusion, seizures, and in severe cases, coma or death.
Inappropriate ADH Syndrome can be caused by various factors, including certain medications, brain tumors, lung diseases, and other medical conditions that affect the production or release of ADH. It is important to diagnose and treat Inappropriate ADH Syndrome promptly to prevent serious complications from hyponatremia. Treatment typically involves addressing the underlying cause and adjusting fluid intake and electrolyte levels as needed.
Paraneoplastic endocrine syndromes refer to a group of hormonal and related disorders that occur as remote effects of cancer. They are caused by substances (like hormones, peptides, or antibodies) produced by the tumor, which may be benign or malignant, and can affect various organs and systems in the body. These syndromes can occur before the cancer is diagnosed, making them an important consideration for early detection and treatment of the underlying malignancy.
Examples of paraneoplastic endocrine syndromes include:
1. Syndrome of Inappropriate Antidiuretic Hormone (SIADH): This occurs when a tumor, often small cell lung cancer, produces antidiuretic hormone (ADH), leading to excessive water retention and low sodium levels in the blood.
2. Cushing's Syndrome: Excessive production of adrenocorticotropic hormone (ACTH) by a tumor, often a small cell lung cancer or pancreatic neuroendocrine tumor, can lead to increased cortisol levels and symptoms such as weight gain, muscle weakness, and mood changes.
3. Ectopic Production of Parathyroid Hormone-Related Peptide (PTHrP): This occurs when a tumor, often a squamous cell carcinoma, produces PTHrP, leading to increased calcium levels in the blood and symptoms such as bone pain, kidney stones, and confusion.
4. Hypercalcemia of Malignancy: Excessive production of calcitriol (active vitamin D) by a tumor, often a lymphoma or myeloma, can lead to increased calcium levels in the blood and symptoms such as bone pain, kidney stones, and confusion.
5. Carcinoid Syndrome: This occurs when a neuroendocrine tumor, often in the gastrointestinal tract, produces serotonin and other substances, leading to symptoms such as flushing, diarrhea, and heart problems.
It is important to note that these syndromes can also be caused by non-cancerous conditions, so a thorough evaluation is necessary to make an accurate diagnosis.
Leukocytosis is a condition characterized by an increased number of leukocytes (white blood cells) in the peripheral blood. A normal white blood cell count ranges from 4,500 to 11,000 cells per microliter of blood in adults. Leukocytosis is typically considered present when the white blood cell count exceeds 11,000 cells/µL. However, the definition might vary slightly depending on the laboratory and clinical context.
Leukocytosis can be a response to various underlying conditions, including bacterial or viral infections, inflammation, tissue damage, leukemia, and other hematological disorders. It is essential to investigate the cause of leukocytosis through further diagnostic tests, such as blood smears, differential counts, and additional laboratory and imaging studies, to guide appropriate treatment.
Hypercalcemia is a medical condition characterized by an excess of calcium ( Ca2+ ) in the blood. While the normal range for serum calcium levels is typically between 8.5 to 10.2 mg/dL (milligrams per deciliter) or 2.14 to 2.55 mmol/L (millimoles per liter), hypercalcemia is generally defined as a serum calcium level greater than 10.5 mg/dL or 2.6 mmol/L.
Hypercalcemia can result from various underlying medical disorders, including primary hyperparathyroidism, malignancy (cancer), certain medications, granulomatous diseases, and excessive vitamin D intake or production. Symptoms of hypercalcemia may include fatigue, weakness, confusion, memory loss, depression, constipation, nausea, vomiting, increased thirst, frequent urination, bone pain, and kidney stones. Severe or prolonged hypercalcemia can lead to serious complications such as kidney failure, cardiac arrhythmias, and calcification of soft tissues. Treatment depends on the underlying cause and severity of the condition.
Encephalomyelitis is a medical term that refers to inflammation of both the brain (encephalitis) and spinal cord (myelitis). This condition can be caused by various infectious agents, such as viruses, bacteria, fungi, or parasites, or it can be due to an autoimmune response where the body's own immune system attacks the nervous tissue.
The symptoms of encephalomyelitis can vary widely depending on the extent and location of the inflammation, but they may include fever, headache, stiff neck, seizures, muscle weakness, sensory changes, and difficulty with coordination or walking. In severe cases, encephalomyelitis can lead to permanent neurological damage or even death.
Treatment for encephalomyelitis typically involves addressing the underlying cause, such as administering antiviral medications for viral infections or immunosuppressive drugs for autoimmune reactions. Supportive care, such as pain management, physical therapy, and rehabilitation, may also be necessary to help manage symptoms and promote recovery.
A syndrome, in medical terms, is a set of symptoms that collectively indicate or characterize a disease, disorder, or underlying pathological process. It's essentially a collection of signs and/or symptoms that frequently occur together and can suggest a particular cause or condition, even though the exact physiological mechanisms might not be fully understood.
For example, Down syndrome is characterized by specific physical features, cognitive delays, and other developmental issues resulting from an extra copy of chromosome 21. Similarly, metabolic syndromes like diabetes mellitus type 2 involve a group of risk factors such as obesity, high blood pressure, high blood sugar, and abnormal cholesterol or triglyceride levels that collectively increase the risk of heart disease, stroke, and diabetes.
It's important to note that a syndrome is not a specific diagnosis; rather, it's a pattern of symptoms that can help guide further diagnostic evaluation and management.
Myxosarcoma is a very rare type of soft tissue sarcoma, a cancer that develops in the soft tissues of the body, such as fat, muscle, nerves, blood vessels, and fibrous tissues. Myxosarcomas are characterized by the presence of mucoid or gelatinous material in the tumor, which is composed of an abnormal accumulation of acid mucopolysaccharides. These tumors typically affect adults, with a peak incidence in the sixth to seventh decade of life. They usually occur in the extremities, particularly the lower limbs, and can also arise in the retroperitoneum or other deep soft tissues. Myxosarcomas are classified into several subtypes based on their histological features, with the most common being the myxofibrosarcoma. Treatment typically involves surgical resection with wide margins, often followed by radiation therapy and/or chemotherapy. The prognosis for patients with myxosarcoma depends on several factors, including the size and location of the tumor, the histological grade, and the patient's age and overall health.
Limbic encephalitis is a rare type of inflammatory autoimmune disorder that affects the limbic system, which is a part of the brain involved in emotions, behavior, memory, and sense of smell. It is characterized by inflammation of the limbic system, leading to symptoms such as memory loss, confusion, seizures, changes in behavior and mood, and problems with autonomic functions.
Limbic encephalitis can be caused by a variety of factors, including viral infections, cancer, or autoimmune disorders. In some cases, the cause may remain unknown. Diagnosis typically involves a combination of clinical evaluation, imaging studies (such as MRI), and analysis of cerebrospinal fluid. Treatment usually involves immunosuppressive therapy to reduce inflammation, as well as addressing any underlying causes if they can be identified.
It is important to note that limbic encephalitis is a serious condition that requires prompt medical attention and treatment. If you or someone else experiences symptoms such as sudden confusion, memory loss, or seizures, it is essential to seek medical care immediately.
Cerebellar diseases refer to a group of medical conditions that affect the cerebellum, which is the part of the brain located at the back of the head, below the occipital lobe and above the brainstem. The cerebellum plays a crucial role in motor control, coordination, balance, and some cognitive functions.
Cerebellar diseases can be caused by various factors, including genetics, infections, tumors, stroke, trauma, or degenerative processes. These conditions can result in a wide range of symptoms, such as:
1. Ataxia: Loss of coordination and unsteady gait
2. Dysmetria: Inability to judge distance and force while performing movements
3. Intention tremors: Shaking or trembling that worsens during purposeful movements
4. Nystagmus: Rapid, involuntary eye movement
5. Dysarthria: Speech difficulty due to muscle weakness or incoordination
6. Hypotonia: Decreased muscle tone
7. Titubation: Rhythmic, involuntary oscillations of the head and neck
8. Cognitive impairment: Problems with memory, attention, and executive functions
Some examples of cerebellar diseases include:
1. Ataxia-telangiectasia
2. Friedrich's ataxia
3. Multiple system atrophy (MSA)
4. Spinocerebellar ataxias (SCAs)
5. Cerebellar tumors, such as medulloblastomas or astrocytomas
6. Infarctions or hemorrhages in the cerebellum due to stroke or trauma
7. Infections, such as viral encephalitis or bacterial meningitis
8. Autoimmune disorders, like multiple sclerosis (MS) or paraneoplastic syndromes
9. Metabolic disorders, such as Wilson's disease or phenylketonuria (PKU)
10. Chronic alcoholism and withdrawal
Treatment for cerebellar diseases depends on the underlying cause and may involve medications, physical therapy, surgery, or supportive care to manage symptoms and improve quality of life.
Thymoma is a type of tumor that originates from the thymus gland, which is a part of the immune system located in the chest behind the breastbone. Thymomas are typically slow-growing and often do not cause any symptoms until they have grown quite large or spread to other parts of the body.
Thymomas can be classified into different types based on their appearance under a microscope, such as type A, AB, B1, B2, and B3. These classifications are important because they can help predict how aggressive the tumor is likely to be and how it should be treated.
Symptoms of thymoma may include cough, chest pain, difficulty breathing, or swelling in the face or neck. Thymomas can also be associated with autoimmune disorders such as myasthenia gravis, which affects muscle strength and mobility. Treatment for thymoma typically involves surgical removal of the tumor, often followed by radiation therapy or chemotherapy to help prevent recurrence.
Ocular motility disorders refer to a group of conditions that affect the movement of the eyes. These disorders can result from nerve damage, muscle dysfunction, or brain injuries. They can cause abnormal eye alignment, limited range of motion, and difficulty coordinating eye movements. Common symptoms include double vision, blurry vision, strabismus (crossed eyes), nystagmus (involuntary eye movement), and difficulty tracking moving objects. Ocular motility disorders can be congenital or acquired and may require medical intervention to correct or manage the condition.
The endocrine system is a complex network of glands and organs that produce, store, and secrete hormones. It plays a crucial role in regulating various functions in the body, including metabolism, growth and development, tissue function, sexual function, reproduction, sleep, and mood.
Endocrine system diseases or disorders occur when there is a problem with the production or regulation of hormones. This can result from:
1. Overproduction or underproduction of hormones by the endocrine glands.
2. Impaired response of target cells to hormones.
3. Disruption in the feedback mechanisms that regulate hormone production.
Examples of endocrine system diseases include:
1. Diabetes Mellitus - a group of metabolic disorders characterized by high blood sugar levels due to insulin deficiency or resistance.
2. Hypothyroidism - underactive thyroid gland leading to slow metabolism, weight gain, fatigue, and depression.
3. Hyperthyroidism - overactive thyroid gland causing rapid heartbeat, anxiety, weight loss, and heat intolerance.
4. Cushing's Syndrome - excess cortisol production resulting in obesity, high blood pressure, and weak muscles.
5. Addison's Disease - insufficient adrenal hormone production leading to weakness, fatigue, and low blood pressure.
6. Acromegaly - overproduction of growth hormone after puberty causing enlargement of bones, organs, and soft tissues.
7. Gigantism - similar to acromegaly but occurs before puberty resulting in excessive height and body size.
8. Hypopituitarism - underactive pituitary gland leading to deficiencies in various hormones.
9. Hyperparathyroidism - overactivity of the parathyroid glands causing calcium imbalances and kidney stones.
10. Precocious Puberty - early onset of puberty due to premature activation of the pituitary gland.
Treatment for endocrine system diseases varies depending on the specific disorder and may involve medication, surgery, lifestyle changes, or a combination of these approaches.
Polymyositis is defined as a rare inflammatory disorder that causes muscle weakness and inflammation (swelling) of the muscles. It primarily affects the skeletal muscles, which are the muscles responsible for voluntary movements such as walking, talking, and swallowing. The onset of polymyositis can occur at any age but is most commonly seen in adults between 31 to 60 years old, with women being slightly more affected than men.
The exact cause of polymyositis remains unknown; however, it is believed to be an autoimmune disorder, where the body's immune system mistakenly attacks its own muscle tissue. Certain factors such as genetics, viral infections, and exposure to certain drugs may contribute to the development of this condition.
Polymyositis can cause various symptoms, including:
- Progressive muscle weakness and wasting, particularly affecting the proximal muscles (those closest to the trunk of the body) such as the hips, thighs, shoulders, and upper arms.
- Difficulty climbing stairs, lifting objects, or rising from a seated position.
- Fatigue and stiffness, especially after periods of inactivity.
- Joint pain and swelling.
- Difficulty swallowing or speaking.
- Shortness of breath due to weakened respiratory muscles.
Diagnosis of polymyositis typically involves a combination of medical history, physical examination, laboratory tests, electromyography (EMG), and muscle biopsy. Treatment usually includes medications such as corticosteroids and immunosuppressants to reduce inflammation and control the immune response. Physical therapy may also be recommended to help maintain muscle strength and flexibility.
If left untreated, polymyositis can lead to significant disability and complications, including respiratory failure, malnutrition, and cardiovascular disease. Early diagnosis and treatment are crucial for improving outcomes and preventing long-term complications.
Cachexia is a complex metabolic disorder characterized by severe weight loss, muscle wasting, and weakness. It is often associated with chronic diseases such as cancer, HIV/AIDS, heart failure, kidney disease, and chronic obstructive pulmonary disease (COPD). Cachexia differs from simple malnutrition or starvation in that it involves a significant loss of muscle mass and an imbalance in energy metabolism, even when adequate calories are consumed.
The hallmark features of cachexia include:
1. Weight loss: Unintentional loss of more than 5% of body weight over 12 months or less, or more than 2% in individuals already underweight.
2. Muscle wasting: Reduction in skeletal muscle mass and strength, leading to weakness and functional impairment.
3. Fatigue and anorexia: Decreased appetite and reduced food intake due to various factors such as inflammation, hormonal imbalances, and psychological distress.
4. Inflammation: Elevated levels of pro-inflammatory cytokines (e.g., TNF-α, IL-1, IL-6) that contribute to metabolic dysregulation and muscle wasting.
5. Insulin resistance: Impaired glucose uptake and utilization by cells, leading to increased blood glucose levels and altered energy metabolism.
6. Altered protein metabolism: Increased protein breakdown and decreased protein synthesis in skeletal muscles, contributing to muscle wasting.
7. Altered lipid metabolism: Increased lipolysis (breakdown of fat) and impaired lipogenesis (formation of fat), leading to loss of adipose tissue and altered energy storage.
Cachexia significantly impacts patients' quality of life, treatment outcomes, and overall survival. Currently, there is no single effective treatment for cachexia, and management typically involves addressing the underlying disease, nutritional support, exercise interventions, and pharmacological therapies to target specific aspects of the metabolic dysregulation associated with this condition.
A fatal outcome is a term used in medical context to describe a situation where a disease, injury, or illness results in the death of an individual. It is the most severe and unfortunate possible outcome of any medical condition, and is often used as a measure of the severity and prognosis of various diseases and injuries. In clinical trials and research, fatal outcome may be used as an endpoint to evaluate the effectiveness and safety of different treatments or interventions.
Hypophosphatemia is a medical condition characterized by abnormally low levels of phosphate (phosphorus) in the blood, specifically below 2.5 mg/dL. Phosphate is an essential electrolyte that plays a crucial role in various bodily functions such as energy production, bone formation, and maintaining acid-base balance.
Hypophosphatemia can result from several factors, including malnutrition, vitamin D deficiency, alcoholism, hormonal imbalances, and certain medications. Symptoms of hypophosphatemia may include muscle weakness, fatigue, bone pain, confusion, and respiratory failure in severe cases. Treatment typically involves correcting the underlying cause and administering phosphate supplements to restore normal levels.
Thymus neoplasms are abnormal growths in the thymus gland that result from uncontrolled cell division. The term "neoplasm" refers to any new and abnormal growth of tissue, also known as a tumor. Thymus neoplasms can be benign or malignant (cancerous).
Malignant thymus neoplasms are called thymomas or thymic carcinomas. Thymomas are the most common type and tend to grow slowly, invading nearby tissues and organs. They can also spread (metastasize) to other parts of the body. Thymic carcinomas are rarer and more aggressive, growing and spreading more quickly than thymomas.
Symptoms of thymus neoplasms may include coughing, chest pain, difficulty breathing, or swelling in the neck or upper chest. Treatment options for thymus neoplasms depend on the type, size, location, and stage of the tumor, as well as the patient's overall health. Treatment may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Nervous system diseases, also known as neurological disorders, refer to a group of conditions that affect the nervous system, which includes the brain, spinal cord, nerves, and muscles. These diseases can affect various functions of the body, such as movement, sensation, cognition, and behavior. They can be caused by genetics, infections, injuries, degeneration, or tumors. Examples of nervous system diseases include Alzheimer's disease, Parkinson's disease, multiple sclerosis, epilepsy, migraine, stroke, and neuroinfections like meningitis and encephalitis. The symptoms and severity of these disorders can vary widely, ranging from mild to severe and debilitating.
Recoverin is a protein found in the retina of the eye that plays a role in protecting photoreceptor cells from light-induced damage. It is a member of the neuronal calcium sensor family and functions as a calmodulin-binding protein, which means it can bind to calcium ions and regulate various cellular processes.
Recoverin is particularly important for the regulation of visual transduction, the process by which light is converted into electrical signals in the eye. When exposed to light, photoreceptor cells release calcium ions, which then bind to recoverin and cause it to change shape. This shape change allows recoverin to inhibit a key enzyme involved in the visual transduction cascade, helping to prevent excessive signaling and protect the photoreceptor cells from damage.
Mutations in the gene that encodes recoverin have been associated with certain inherited eye diseases, such as congenital stationary night blindness and retinitis pigmentosa. These mutations can disrupt the normal function of recoverin and lead to progressive vision loss.
Parathyroid Hormone-Related Protein (PTHrP) is a protein that is encoded by the PTHLH gene in humans. It is structurally similar to parathyroid hormone (PTH) and was initially identified due to its role in humoral hypercalcemia of malignancy, a condition characterized by high levels of calcium in the blood caused by certain types of cancer.
PTHrP has a variety of functions in the body, including regulation of calcium and phosphate homeostasis, cell growth and differentiation, and bone metabolism. It acts through a specific G protein-coupled receptor called the PTH/PTHrP receptor, which is found in many tissues throughout the body, including bone, kidney, and cartilage.
In contrast to PTH, which is primarily produced by the parathyroid glands and regulates calcium levels in the blood, PTHrP is produced by many different types of cells throughout the body. Its expression is regulated in a tissue-specific manner, and its functions can vary depending on the context in which it is produced.
Overall, PTHrP plays important roles in normal physiology as well as in various disease states, including cancer, bone disorders, and developmental abnormalities.
Maxillary neoplasms refer to abnormal growths or tumors in the maxilla, which is the upper jaw bone. These growths can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are slow-growing and do not spread to other parts of the body, while malignant neoplasms can invade surrounding tissues and spread to distant sites.
Maxillary neoplasms can cause various symptoms such as swelling, pain, numbness, loose teeth, or difficulty in chewing or swallowing. They may also cause nasal congestion, nosebleeds, or visual changes if they affect the eye or orbit. The diagnosis of maxillary neoplasms usually involves a combination of clinical examination, imaging studies such as CT or MRI scans, and biopsy to determine the type and extent of the tumor.
Treatment options for maxillary neoplasms depend on several factors, including the type, size, location, and stage of the tumor, as well as the patient's overall health and preferences. Treatment may include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular follow-up care is essential to monitor for recurrence or metastasis and ensure optimal outcomes.
Autoantibodies are defined as antibodies that are produced by the immune system and target the body's own cells, tissues, or organs. These antibodies mistakenly identify certain proteins or molecules in the body as foreign invaders and attack them, leading to an autoimmune response. Autoantibodies can be found in various autoimmune diseases such as rheumatoid arthritis, lupus, and thyroiditis. The presence of autoantibodies can also be used as a diagnostic marker for certain conditions.
Dermatomyositis is a medical condition characterized by inflammation and weakness in the muscles and skin. It is a type of inflammatory myopathy, which means that it causes muscle inflammation and damage. Dermatomyositis is often associated with a distinctive rash that affects the skin around the eyes, nose, mouth, fingers, and toes.
The symptoms of dermatomyositis can include:
* Progressive muscle weakness, particularly in the hips, thighs, shoulders, and neck
* Fatigue
* Difficulty swallowing or speaking
* Skin rash, which may be pink or purple and is often accompanied by itching
* Muscle pain and tenderness
* Joint pain and swelling
* Raynaud's phenomenon, a condition that affects blood flow to the fingers and toes
The exact cause of dermatomyositis is not known, but it is believed to be related to an autoimmune response in which the body's immune system mistakenly attacks healthy tissue. Treatment for dermatomyositis typically involves medications to reduce inflammation and suppress the immune system, as well as physical therapy to help maintain muscle strength and function.
Carcinoma, small cell is a type of lung cancer that typically starts in the bronchi (the airways that lead to the lungs). It is called "small cell" because the cancer cells are small and appear round or oval in shape. This type of lung cancer is also sometimes referred to as "oat cell carcinoma" due to the distinctive appearance of the cells, which can resemble oats when viewed under a microscope.
Small cell carcinoma is a particularly aggressive form of lung cancer that tends to spread quickly to other parts of the body. It is strongly associated with smoking and is less common than non-small cell lung cancer (NSCLC), which accounts for about 85% of all lung cancers.
Like other types of lung cancer, small cell carcinoma may not cause any symptoms in its early stages. However, as the tumor grows and spreads, it can cause a variety of symptoms, including coughing, chest pain, shortness of breath, hoarseness, and weight loss. Treatment for small cell carcinoma typically involves a combination of chemotherapy, radiation therapy, and sometimes surgery.
Lung neoplasms refer to abnormal growths or tumors in the lung tissue. These tumors can be benign (non-cancerous) or malignant (cancerous). Malignant lung neoplasms are further classified into two main types: small cell lung carcinoma and non-small cell lung carcinoma. Lung neoplasms can cause symptoms such as cough, chest pain, shortness of breath, and weight loss. They are often caused by smoking or exposure to secondhand smoke, but can also occur due to genetic factors, radiation exposure, and other environmental carcinogens. Early detection and treatment of lung neoplasms is crucial for improving outcomes and survival rates.
Neuromuscular diseases are a group of disorders that involve the peripheral nervous system, which includes the nerves and muscles outside of the brain and spinal cord. These conditions can affect both children and adults, and they can be inherited or acquired. Neuromuscular diseases can cause a wide range of symptoms, including muscle weakness, numbness, tingling, pain, cramping, and twitching. Some common examples of neuromuscular diseases include muscular dystrophy, amyotrophic lateral sclerosis (ALS), peripheral neuropathy, and myasthenia gravis. The specific symptoms and severity of these conditions can vary widely depending on the underlying cause and the specific muscles and nerves that are affected. Treatment for neuromuscular diseases may include medications, physical therapy, assistive devices, or surgery, depending on the individual case.
Hu paraneoplastic encephalomyelitis antigens are a group of neuronal intracellular antigens associated with paraneoplastic neurological disorders (PNDs). PNDs are a group of rare, degenerative conditions that affect the nervous system and can occur in patients with cancer. The Hu antigens are part of a family of proteins known as onconeural antigens, which are expressed in both cancer cells and normal neurons.
The Hu antigens include three main proteins: HuD, HuC, and Rb/p75. These proteins are involved in the regulation of gene expression and are found in the nucleus and cytoplasm of neuronal cells. In patients with PNDs associated with Hu antigens, the immune system mistakenly recognizes these antigens as foreign and mounts an immune response against them. This leads to inflammation and damage to the nervous system, resulting in various neurological symptoms such as muscle weakness, sensory loss, and autonomic dysfunction.
Paraneoplastic encephalomyelitis is a specific type of PND that affects both the brain (encephalitis) and spinal cord (myelitis). It is often associated with small cell lung cancer but can also occur in other types of cancer. The presence of Hu antibodies in the blood or cerebrospinal fluid is a useful diagnostic marker for this condition, although not all patients with Hu-associated PNDs will have detectable Hu antibodies.
Stiff-Person Syndrome (SPS) is a rare neurological disorder characterized by fluctuating muscle rigidity in the trunk and limbs and a heightened sensitivity to stimuli such as touch, sound, and emotional distress, which can trigger muscle spasms. The symptoms can significantly affect a person's ability to perform daily activities and can lead to frequent falls and injuries. SPS is often associated with antibodies against glutamic acid decarboxylase (GAD), an enzyme involved in the production of a neurotransmitter called gamma-aminobutyric acid (GABA) that helps regulate muscle movement. The exact cause of SPS remains unknown, but it is thought to involve both autoimmune and genetic factors.
Opsoclonus-Myoclonus Syndrome (OMS) is a rare neurological disorder characterized by rapid, involuntary, and chaotic eye movements (opsoclonus) and brief, shock-like jerks of the muscles (myoclonus). These symptoms can affect various parts of the body, including the limbs, trunk, and face. OMS is often associated with a variety of underlying causes, such as viral infections, tumors, or autoimmune disorders. In some cases, no specific cause can be identified, and this is referred to as idiopathic OMS.
The symptoms of OMS can significantly impact an individual's daily functioning and quality of life. Treatment typically involves a combination of medications to manage the symptoms and address any underlying causes. The prognosis for individuals with OMS varies depending on the severity of the condition and the effectiveness of treatment. Some people may experience significant improvement in their symptoms, while others may have persistent neurological impairments.
Pemphigus is a group of rare, autoimmune blistering diseases that affect the skin and mucous membranes. In these conditions, the immune system mistakenly produces antibodies against desmoglein proteins, which are crucial for maintaining cell-to-cell adhesion in the epidermis (outermost layer of the skin). This results in the loss of keratinocyte cohesion and formation of flaccid blisters filled with serous fluid.
There are several types of pemphigus, including:
1. Pemphigus vulgaris - The most common form, primarily affecting middle-aged to older adults, with widespread erosions and flaccid blisters on the skin and mucous membranes (e.g., mouth, nose, genitals).
2. Pemphigus foliaceus - A more superficial form, mainly involving the skin, causing crusted erosions and scaly lesions without mucosal involvement. It is more prevalent in older individuals and in certain geographical regions like the Middle East.
3. Paraneoplastic pemphigus - A rare type associated with underlying neoplasms (cancers), such as lymphomas or carcinomas, characterized by severe widespread blistering of both skin and mucous membranes, along with antibodies against additional antigens besides desmogleins.
4. IgA pemphigus - A less common form characterized by localized or generalized erosions and blisters, with IgA autoantibodies targeting the basement membrane zone.
Treatment for pemphigus typically involves high-dose systemic corticosteroids, often in combination with immunosuppressive agents (e.g., azathioprine, mycophenolate mofetil, rituximab) to control the disease activity and prevent complications. Regular follow-ups with dermatologists and oral specialists are essential for monitoring treatment response and managing potential side effects.
 Paraneoplastic syndrome
Paraneoplastic syndrome Paraneoplastic Syndromes: Practice Essentials, Pathophysiology, Etiology
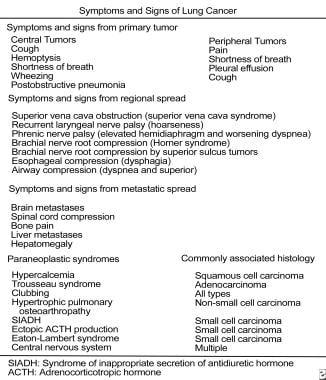
Paraneoplastic Syndromes: Practice Essentials, Pathophysiology, Etiology Paraneoplastic Syndromes Associated with Small Cell Lung Cancer
Paraneoplastic Syndromes Associated with Small Cell Lung Cancer Tumor induced osteomalacia: a forgotten paraneoplastic syndrome?
Tumor induced osteomalacia: a forgotten paraneoplastic syndrome? Paraneoplastic syndromes and oncological outcomes in renal cancer. - International Association for the Study of Pain (IASP)
Paraneoplastic syndromes and oncological outcomes in renal cancer. - International Association for the Study of Pain (IASP) Types of paraneoplastic syndromes - GPnotebook
Types of paraneoplastic syndromes - GPnotebook Quiz: Paraneoplastic Syndromes - MSD Manual Consumer Version
Quiz: Paraneoplastic Syndromes - MSD Manual Consumer Version Paraneoplastic Syndrome
Paraneoplastic Syndrome Paraneoplastic neurological syndromes<...
Paraneoplastic neurological syndromes<... A Case of Paraneoplastic Syndrome
A Case of Paraneoplastic Syndrome Home Remedies For Paraneoplastic Syndrome
Home Remedies For Paraneoplastic Syndrome Don't ignore these symptoms of kidney cancer | UCLA Health
Don't ignore these symptoms of kidney cancer | UCLA Health Paraneoplastic Dermatomyositis Syndrome Presenting as Dysphagia | Ofori | Gastroenterology Research
Paraneoplastic Dermatomyositis Syndrome Presenting as Dysphagia | Ofori | Gastroenterology Research Paraneoplastic Neurologic Syndromes- An Update on Current Understanding and Future Perspectives - touchNEUROLOGY
Paraneoplastic Neurologic Syndromes- An Update on Current Understanding and Future Perspectives - touchNEUROLOGY Medicine and Health - Page 164 - Nova Science Publishers
Medicine and Health - Page 164 - Nova Science Publishers Top 10 Rare Diseases | HowStuffWorks
Top 10 Rare Diseases | HowStuffWorks Paraneoplastic Syndromes: Endocrinologic/Hematologic | Harrison's Hematology and Oncology, 3e | AccessBiomedical Science |...
Paraneoplastic Syndromes: Endocrinologic/Hematologic | Harrison's Hematology and Oncology, 3e | AccessBiomedical Science |... Long-Range Tumor-Host Signaling Mechanisms Driving Paraneoplastic Syndromes | The Mark Foundation for Cancer Research
Long-Range Tumor-Host Signaling Mechanisms Driving Paraneoplastic Syndromes | The Mark Foundation for Cancer Research Autoimmune Diseases | Autoimmune Disease Symptoms | MedlinePlus
Autoimmune Diseases | Autoimmune Disease Symptoms | MedlinePlus Paraneoplastic Pemphigus (Paraneoplastic Autoimmune Multiorgan Syndrome) Screening Antibodies by IIF | ARUP Laboratories Test...
Paraneoplastic Pemphigus (Paraneoplastic Autoimmune Multiorgan Syndrome) Screening Antibodies by IIF | ARUP Laboratories Test...


![10 Best Clinics for Esophageal Cancer Treatment in Thailand [2023 Prices]](https://www.mymeditravel.com/cdn-cgi/image/f=auto,fit=contain,quality=75/uploads/property/gallery/5af2758efa6b7e04401f8c27/5af51dadfa6b7e4212052361/preview.jpg)