Radial Neuropathy
Diabetic Neuropathies
Radial Artery
Peripheral Nervous System Diseases
Hereditary Sensory and Motor Neuropathy
Radial Nerve
Hereditary Sensory and Autonomic Neuropathies
Optic Neuropathy, Ischemic
Polyneuropathies
Sural Nerve
Neural Conduction
Ulnar Neuropathies
Charcot-Marie-Tooth Disease
Cryosurgery for chronic injuries of the cutaneous nerve in the upper limb. Analysis of a new open technique. (1/29)
We have treated six patients with chronic pain following nerve injury using a cryosurgical probe. All had a significant return of hand function and improvement of pain during a mean follow-up of 13.5 months. Open visualisation of the injured nervous tissue is essential for patients undergoing this technique. Four patients regained normal sensation in the dermatome of the previously injured nerve. (+info)Ultrasonographic appearance of supinator syndrome. (2/29)
OBJECTIVE: To describe ultrasonographic findings in 4 patients with supinator syndrome (i.e., deep branch of the radial nerve). METHODS: Four patients with weakness and pain in their forearm underwent ultrasonographic examination with subsequent electroneurographic testing and surgical nerve inspection. Normal measurements of the deep branch of the radial nerve in 10 healthy volunteers served as comparison for measurements in the patients. RESULTS: An enlarged deep branch of the radial nerve was found in all 4 patients at the affected side. Electroneurographic testing and surgical inspection confirmed the ultrasonographic findings. The mean transverse diameter was 4.2 mm (range, 3.8-4.5 mm), and the anteroposterior diameter was 3.3 mm (range, 2.5-3.8 mm). In volunteers, the mean transverse diameter was 2.13 mm (range, 1.7-2.6 mm), and the mean anteroposterior diameter was 1.3 mm (range, 1.0-1.5 mm). CONCLUSIONS: The deep branch of the radial nerve appears enlarged in patients with supinator syndrome. (+info)Radial nerve palsy in an elite bodybuilder. (3/29)
A case is reported of high radial nerve palsy in an elite bodybuilder caused by an extrinsic mass effect of muscular hypertrophy. Surgical decompression resulted in complete clinical resolution. (+info)Radial nerve compression by a large cephalic vein aneurysm: case report. (4/29)
A 43-year-old man had weakness of the extensor muscles in the right forearm and could not extend the right wrist. The apparent disorder was caused by radial nerve compression by a large aneurysm in the cephalic vein in the antecubital fossa. Surgical resection of the aneurysm resolved the symptoms. This exceedingly rare complication of venous aneurysm is discussed. Venous aneurysm should be included in the differential diagnosis of a subcutaneous mass, and diagnosis is best made with Duplex ultrasound scanning. Surgical excision is the appropriate treatment. (+info)Radial nerve paralysis due to Kent retractor during upper abdominal operation. (5/29)
After general anesthesia, peripheral nerve paralysis is a rare complication. The frequently damaged nerves including: branches of the brachial plexus, the ulnar, radial and common peroneal nerves, and sometimes the facial nerve. The radial nerve is the most infrequently damaged one, accounting for only 3% of nerve damage. We report a case of radial nerve paralysis due to self retractor during abdominal operation, its clinical findings, and review of the literature on peripheral nerve paralysis. (+info)Investigation of two possible compression sites of the deep branch of the radial nerve and nerve supply of the extensor carpi radialis brevis muscle. (6/29)
The posterior interosseous nerve arises from the deep branch of the radial nerve, and compression by adjacent structures results in posterior interosseous nerve syndrome. Sixty upper limbs from 30 Turkish subjects (18 males and 12 females) were dissected to reveal the course of the posterior interosseous nerve and to examine possible compression sites at the proximal and distal edges of the supinator muscle, and the exit of the nerve from the extensor carpi radialis brevis muscle. Posterior interosseous nerve syndrome is most probably caused by the tendinous part of the supinator muscle at the proximal edge. (+info)Complications of treating distal radius fractures with external fixation: a community experience. (7/29)
OBJECTIVE: To analyze the immediate postoperative complications associated with treating distal radius fractures with external fixation. DESIGN: A retrospective chart review of data obtained from 24 consecutive patients who were treated with small AO external fixators in 1997. SETTING: Two community medical centers. INTERVENTION: Preoperative and postoperative radiograph measurements were taken of radial inclination, radial tilt, and radial length, and fractures were classified according to the AO system. Patient charts were reviewed to document demographics, type of fixator used, open or percutaneous technique for pin placement, use of augmentation, additional operations, and complications. MAIN OUTCOME MEASUREMENTS: Complications associated with treating distal radius fractures with one type of external fixator. RESULTS: Sixteen of the 24 patients had complications: 5 with neuropathies of the median or superficial radial nerve, 9 with pin track infections, 2 with pin loosening, one with a nonunion, 2 with malunion, and 4 patients each with radial shortening, loss of radial tilt, collapse of ulnar border or volar intercalated segment instability (VISI) of the lunate and rotatory subluxation of the scaphoid. CONCLUSIONS: Postoperative complications following distal radius fractures treated with external fixation are common. Their effect, however, on long term functional results and patient satisfaction is negligible, with the exception of those patients with complications intrinsic to the fracture itself, i.e., nonunion, malunion or carpal malalignment. (+info)Thrower's fracture of the humerus with radial nerve palsy: an unfamiliar softball injury. (8/29)
A fracture of the normal humerus in a healthy young adult most commonly results from significant direct trauma. Throwing sports have become increasingly popular outside of North America and bring with them a novel injury mechanism for clinicians. A 21 year old woman sustained a "thrower's fracture" of the distal humerus and radial nerve palsy while throwing a softball. She was treated by internal fixation. Her fracture united, and radial nerve neurapraxia resolved after 8 weeks. Clinicians should be aware of this entity so that prodromal symptoms can be recognised early and thrower's fractures are not investigated unnecessarily. (+info)Radial neuropathy, also known as radial nerve palsy, refers to damage or dysfunction of the radial nerve. The radial nerve provides motor function to the muscles in the back of the arm and sensation to the back of the hand and forearm. Damage to this nerve can result in weakness or paralysis of the wrist and finger extensors, causing difficulty with extending the wrist, fingers, and thumb. Additionally, there may be numbness or tingling sensations in the back of the hand and forearm. Radial neuropathy can occur due to various reasons such as trauma, compression, or certain medical conditions like diabetes.
Diabetic neuropathies refer to a group of nerve disorders that are caused by diabetes. High blood sugar levels can injure nerves throughout the body, but diabetic neuropathies most commonly affect the nerves in the legs and feet.
There are four main types of diabetic neuropathies:
1. Peripheral neuropathy: This is the most common type of diabetic neuropathy. It affects the nerves in the legs and feet, causing symptoms such as numbness, tingling, burning, or shooting pain.
2. Autonomic neuropathy: This type of neuropathy affects the autonomic nerves, which control involuntary functions such as heart rate, blood pressure, digestion, and bladder function. Symptoms may include dizziness, fainting, digestive problems, sexual dysfunction, and difficulty regulating body temperature.
3. Proximal neuropathy: Also known as diabetic amyotrophy, this type of neuropathy affects the nerves in the hips, thighs, or buttocks, causing weakness, pain, and difficulty walking.
4. Focal neuropathy: This type of neuropathy affects a single nerve or group of nerves, causing symptoms such as weakness, numbness, or pain in the affected area. Focal neuropathies can occur anywhere in the body, but they are most common in the head, torso, and legs.
The risk of developing diabetic neuropathies increases with the duration of diabetes and poor blood sugar control. Other factors that may contribute to the development of diabetic neuropathies include genetics, age, smoking, and alcohol consumption.
The radial artery is a key blood vessel in the human body, specifically a part of the peripheral arterial system. Originating from the brachial artery in the upper arm, the radial artery travels down the arm and crosses over the wrist, where it can be palpated easily. It then continues into the hand, dividing into several branches to supply blood to the hand's tissues and digits.
The radial artery is often used for taking pulse readings due to its easy accessibility at the wrist. Additionally, in medical procedures such as coronary angiography or bypass surgery, the radial artery can be utilized as a site for catheter insertion. This allows healthcare professionals to examine the heart's blood vessels and assess cardiovascular health.
Peripheral Nervous System (PNS) diseases, also known as Peripheral Neuropathies, refer to conditions that affect the functioning of the peripheral nervous system, which includes all the nerves outside the brain and spinal cord. These nerves transmit signals between the central nervous system (CNS) and the rest of the body, controlling sensations, movements, and automatic functions such as heart rate and digestion.
PNS diseases can be caused by various factors, including genetics, infections, toxins, metabolic disorders, trauma, or autoimmune conditions. The symptoms of PNS diseases depend on the type and extent of nerve damage but often include:
1. Numbness, tingling, or pain in the hands and feet
2. Muscle weakness or cramps
3. Loss of reflexes
4. Decreased sensation to touch, temperature, or vibration
5. Coordination problems and difficulty with balance
6. Sexual dysfunction
7. Digestive issues, such as constipation or diarrhea
8. Dizziness or fainting due to changes in blood pressure
Examples of PNS diseases include Guillain-Barre syndrome, Charcot-Marie-Tooth disease, diabetic neuropathy, and peripheral nerve injuries. Treatment for these conditions varies depending on the underlying cause but may involve medications, physical therapy, lifestyle changes, or surgery.
Hereditary Sensory and Motor Neuropathy (HSMN) is a group of inherited disorders that affect the peripheral nerves, which are the nerves outside the brain and spinal cord. These nerves transmit information between the brain and muscles, as well as sensations such as touch, pain, heat, and cold.
HSMN is characterized by progressive degeneration of these peripheral nerves, leading to muscle weakness, numbness, and tingling sensations, particularly in the hands and feet. The condition can also affect the autonomic nervous system, which controls involuntary functions such as heart rate, blood pressure, and digestion.
HSMN is caused by genetic mutations that are inherited from one or both parents. There are several types of HSMN, each with its own specific symptoms, severity, and pattern of inheritance. The most common form is Charcot-Marie-Tooth disease (CMT), which affects both motor and sensory nerves.
Treatment for HSMN typically focuses on managing the symptoms and preventing complications. This may include physical therapy, bracing or orthopedic surgery to support weakened muscles, pain management, and lifestyle modifications such as avoiding activities that aggravate symptoms. There is currently no cure for HSMN, but ongoing research is aimed at developing new treatments and therapies to slow or halt the progression of the disease.
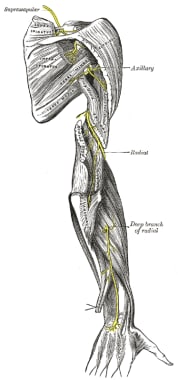
The Radial nerve is a major peripheral nerve in the human body that originates from the brachial plexus, which is a network of nerves formed by the union of the ventral rami (anterior divisions) of spinal nerves C5-T1. The radial nerve provides motor function to extensor muscles of the upper limb and sensation to parts of the skin on the back of the arm, forearm, and hand.
More specifically, the radial nerve supplies motor innervation to:
* Extensor muscles of the shoulder (e.g., teres minor, infraspinatus)
* Rotator cuff muscles
* Elbow joint stabilizers (e.g., lateral head of the triceps)
* Extensors of the wrist, fingers, and thumb
The radial nerve also provides sensory innervation to:
* Posterior aspect of the upper arm (from the lower third of the humerus to the elbow)
* Lateral forearm (from the lateral epicondyle of the humerus to the wrist)
* Dorsum of the hand (skin over the radial side of the dorsum, including the first web space)
Damage or injury to the radial nerve may result in various symptoms, such as weakness or paralysis of the extensor muscles, numbness or tingling sensations in the affected areas, and difficulty with extension movements of the wrist, fingers, and thumb. Common causes of radial nerve injuries include fractures of the humerus bone, compression during sleep or prolonged pressure on the nerve (e.g., from crutches), and entrapment syndromes like radial tunnel syndrome.
Hereditary Sensory and Autonomic Neuropathies (HSANs) are a group of inherited disorders that affect the sensory and autonomic nerves. These nerves are responsible for transmitting information about senses such as touch, pain, temperature, and vibration to the brain, as well as controlling automatic functions like blood pressure, heart rate, and digestion.
HSANs are caused by genetic mutations that result in damage to the peripheral nerves. There are several types of HSANs, each with its own specific symptoms and patterns of inheritance. Some common features include:
* Loss of sensation in the hands and feet
* Pain insensitivity
* Absent or reduced reflexes
* Autonomic dysfunction, such as abnormal sweating, blood pressure regulation, and digestive problems
The severity and progression of HSANs can vary widely depending on the specific type and individual factors. Treatment is generally focused on managing symptoms and preventing complications, such as injuries from lack of pain sensation or falls due to balance problems. Early diagnosis and intervention are important for optimizing outcomes.
Ischemic optic neuropathy (ION) is a medical condition that refers to the damage or death of the optic nerve due to insufficient blood supply. The optic nerve is responsible for transmitting visual information from the eye to the brain.
In ION, the blood vessels that supply the optic nerve become blocked or narrowed, leading to decreased blood flow and oxygen delivery to the nerve fibers. This results in inflammation, swelling, and ultimately, damage to the optic nerve. The damage can cause sudden, painless vision loss, often noticed upon waking up in the morning.
There are two types of ION: anterior ischemic optic neuropathy (AION) and posterior ischemic optic neuropathy (PION). AION affects the front part of the optic nerve, while PION affects the back part of the nerve. AION is further classified into arteritic and non-arteritic types, depending on whether it is caused by giant cell arteritis or not.
Risk factors for ION include age (most commonly occurring in people over 50), hypertension, diabetes, smoking, sleep apnea, and other cardiovascular diseases. Treatment options depend on the type and cause of ION and may include controlling underlying medical conditions, administering corticosteroids, or undergoing surgical procedures to improve blood flow.
Polyneuropathy is a medical condition that refers to the damage or dysfunction of peripheral nerves (nerves outside the brain and spinal cord) in multiple areas of the body. These nerves are responsible for transmitting sensory, motor, and autonomic signals between the central nervous system and the rest of the body.
In polyneuropathies, this communication is disrupted, leading to various symptoms depending on the type and extent of nerve damage. Commonly reported symptoms include:
1. Numbness or tingling in the hands and feet
2. Muscle weakness and cramps
3. Loss of reflexes
4. Burning or stabbing pain
5. Balance and coordination issues
6. Increased sensitivity to touch
7. Autonomic dysfunction, such as bowel, bladder, or digestive problems, and changes in blood pressure
Polyneuropathies can be caused by various factors, including diabetes, alcohol abuse, nutritional deficiencies, autoimmune disorders, infections, toxins, inherited genetic conditions, or idiopathic (unknown) causes. The treatment for polyneuropathy depends on the underlying cause and may involve managing underlying medical conditions, physical therapy, pain management, and lifestyle modifications.
The sural nerve is a purely sensory peripheral nerve in the lower leg and foot. It provides sensation to the outer ( lateral) aspect of the little toe and the adjacent side of the fourth toe, as well as a small portion of the skin on the back of the leg between the ankle and knee joints.
The sural nerve is formed by the union of branches from the tibial and common fibular nerves (branches of the sciatic nerve) in the lower leg. It runs down the calf, behind the lateral malleolus (the bony prominence on the outside of the ankle), and into the foot.
The sural nerve is often used as a donor nerve during nerve grafting procedures due to its consistent anatomy and relatively low risk for morbidity at the donor site.
Neural conduction is the process by which electrical signals, known as action potentials, are transmitted along the axon of a neuron (nerve cell) to transmit information between different parts of the nervous system. This electrical impulse is generated by the movement of ions across the neuronal membrane, and it propagates down the length of the axon until it reaches the synapse, where it can then stimulate the release of neurotransmitters to communicate with other neurons or target cells. The speed of neural conduction can vary depending on factors such as the diameter of the axon, the presence of myelin sheaths (which act as insulation and allow for faster conduction), and the temperature of the environment.
Ulnar neuropathies refer to conditions that cause damage or dysfunction to the ulnar nerve, which is one of the major nerves in the arm. The ulnar nerve runs down the forearm and through the wrist to the hand, where it provides sensation to the pinky finger and half of the ring finger, as well as motor function to the muscles that control finger movements.
Ulnar neuropathies can result from various causes, including trauma, compression, entrapment, or inflammation. Common symptoms include numbness, tingling, or weakness in the hand and fingers, particularly in the pinky and ring fingers. In more severe cases, muscle wasting and loss of dexterity may occur.
There are several types of ulnar neuropathies, depending on the location and cause of the nerve damage. For example, cubital tunnel syndrome is a type of ulnar neuropathy that results from compression of the ulnar nerve at the elbow, while ulnar nerve entrapment at the wrist (also known as Guyon's canal syndrome) can also cause ulnar neuropathies. Treatment options for ulnar neuropathies may include physical therapy, medication, or surgery, depending on the severity and underlying cause of the condition.
Charcot-Marie-Tooth disease (CMT) is a group of inherited disorders that cause nerve damage, primarily affecting the peripheral nerves. These are the nerves that transmit signals between the brain and spinal cord to the rest of the body. CMT affects both motor and sensory nerves, leading to muscle weakness and atrophy, as well as numbness or tingling in the hands and feet.
The disease is named after the three physicians who first described it: Jean-Martin Charcot, Pierre Marie, and Howard Henry Tooth. CMT is characterized by its progressive nature, meaning symptoms typically worsen over time, although the rate of progression can vary significantly among individuals.
There are several types of CMT, classified based on their genetic causes and patterns of inheritance. The two most common forms are CMT1 and CMT2:
1. CMT1: This form is caused by mutations in the genes responsible for the myelin sheath, which insulates peripheral nerves and allows for efficient signal transmission. As a result, demyelination occurs, slowing down nerve impulses and causing muscle weakness, particularly in the lower limbs. Symptoms usually begin in childhood or adolescence and include foot drop, high arches, and hammertoes.
2. CMT2: This form is caused by mutations in the genes responsible for the axons, the nerve fibers that transmit signals within peripheral nerves. As a result, axonal degeneration occurs, leading to muscle weakness and atrophy. Symptoms usually begin in early adulthood and progress more slowly than CMT1. They primarily affect the lower limbs but can also involve the hands and arms.
Diagnosis of CMT typically involves a combination of clinical evaluation, family history, nerve conduction studies, and genetic testing. While there is no cure for CMT, treatment focuses on managing symptoms and maintaining mobility and function through physical therapy, bracing, orthopedic surgery, and pain management.
 Radial neuropathy - Wikipedia
Radial neuropathy - Wikipedia Radial neuropathy - WikiProjectMed
Radial neuropathy - WikiProjectMed Marianne T. Luetmer, M.D. - الأطباء والفريق الطبي - Mayo Clinic (مايو كلينك)
Marianne T. Luetmer, M.D. - الأطباء والفريق الطبي - Mayo Clinic (مايو كلينك) Research | LHSC
Research | LHSC Radial Mononeuropathy: Background, Pathophysiology, Epidemiology
Radial Mononeuropathy: Background, Pathophysiology, Epidemiology Medical Abbreviations - R - GlobalRPH
Medical Abbreviations - R - GlobalRPH Pinched Nerve in Arm: Causes, Symptoms, Treatment, Prevention
Pinched Nerve in Arm: Causes, Symptoms, Treatment, Prevention![American Association of Neuromuscluar and Electrodiagnostic Medicine (AANEM) [2023] - CMEList](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAAPFBMVEVHcEwEHi8EHy8EHi8EHi8EHjAEHi8EHi8EHi8EHi8EHi8EHjAEHi8EHi8EHjAEHi8EHi8EHzAEHzAEHi9b+EGYAAAAFHRSTlMAypErID7d/oBWEkheaJ4F7LW3dja7mp4AAABVSURBVBiVtY7LFYBACMSGXWBg/2r/vWoT5pSXU4Bf2DOx+yfWzKxi048rBypTxAOPAFNJCDNTgbiAqpT7eJZlgLJcVDZ2H1FKfmWt1gIDs0ZE/2X8BVGBAoOhEgDhAAAAAElFTkSuQmCC) American Association of Neuromuscluar and Electrodiagnostic Medicine (AANEM) [2023] - CMEList
American Association of Neuromuscluar and Electrodiagnostic Medicine (AANEM) [2023] - CMEList WTS database | WHO FCTC
WTS database | WHO FCTC Nerve Conduction Studies
Nerve Conduction Studies Barton Branam, MD | UC Health Provider Profile
Barton Branam, MD | UC Health Provider Profile Peripheral Nerve Stimulator for Post-Surgical Pain Management
Peripheral Nerve Stimulator for Post-Surgical Pain Management Share this post
Share this post Serum micronutrients and prealbumin during development and recovery of chemotherapy-induced peripheral neuropathy
Serum micronutrients and prealbumin during development and recovery of chemotherapy-induced peripheral neuropathy Nerves & Circulation
Nerves & Circulation Wartenberg's Syndrome - Hand - Orthobullets
Wartenberg's Syndrome - Hand - Orthobullets Median Neuropathy; Median Nerve Diseases
Median Neuropathy; Median Nerve Diseases Is there a cure for hereditary neuropathy? - Leonieclaire.com
Is there a cure for hereditary neuropathy? - Leonieclaire.com DeCS - New terms
DeCS - New terms