Defecography
Rectal Prolapse
Cystocele
Intussusception
Pelvic Floor
Constipation
Hernia
Uterine Prolapse
Rectal Diseases
Surgical Stapling
Perineum
Surgical Staplers
Fecal Incontinence
Defecography in symptomatic older women living at home. (1/38)
BACKGROUND: complaints of defecation disorders in older patients living at home is an emerging problem. Little is known about radiological examination of this population. OBJECTIVE: this study aimed to analyse the yield of defecography in women older than 75 years, living at home and complaining of defecation disorders. DESIGN AND SETTINGS: prospective study of patients referred to a radiology department in a tertiary-care medical centre in Rouen, France. SUBJECTS AND METHODS: 52 women (mean age: 78, range: 75-93) complaining of constipation, faecal incontinence or pelvic pain underwent defecography. Defecography was performed after intake of a barium meal and vaginal opacification. Radiographs were analysed accordingly with the established criteria. RESULTS: defecography showed perineal descent in 27 patients, rectocele in 29, intussusception in 33 and enterocele in 14. A combination of abnormalities was found in 40 women. Only 3 studies were normal. There was no significant association between symptoms and pelvic disorders revealed by defecography. CONCLUSIONS: defecography in symptomatic women aged 75 years and over did not raise any technical difficulty. It revealed a 77% rate of abnormalities, but there was no relationship between the symptoms and the detected abnormalities. (+info)Incidence of pelvic organ prolapse in Nigerian women. (2/38)
OBJECTIVE: To establish the incidence and types of utero-vaginal prolapse. METHODS: Retrospective medical records analyses of women who were subjected to reconstructive pelvic surgery for various types of pelvic relaxation at the Nnamdi Azikiwe University Teaching Hospital, Nnewi and the University Of Nigeria Teaching Hospital, Enugu, Nigeria was carried out. The study was conducted from January 1996 to December 1999 during which there were 7515 surgical admissions. The inclusion criteria were those women who complained of feeling a mass in the vagina with demonAstrable descent of the anterior and/or posterior and/or apical vaginal walls and/or perineal descent. Excluded were patients who had other symptoms other than utero-vaginal prolapse and those whose grades and sites of prolapse were not determinable from the clinical or surgical notes. Also excluded were patients with nerve injury or disease, connective tissue disorders and neuromuscular diseases. The subjects were divided into two groups. Group I consisted of 54 women (age < or = 40 years), and group II included 105 women (age > or = 40 years). The findings between those two groups were compared with reference to sites, types and degree of prolapse. Also, coexistence of pelvic relaxation and underlying medical conditions were evaluated. RESULTS: A total of 159 subjects out of 492 charts studied met the inclusion criteria for the study. In group I, mean age was 32.839 with a standard deviation (SD) of +/- 6.012 years; and in group II the mean age was 56.543 with a SD of 8.094. Hypertrophic (elongated) cervix was determined in 15 (6.3%) subjects in group I for an incidence of 1.58% per year, cystocele (vaginal anterior wall descent) was present in 21 (8.9%) women for an incidence of 2.2% per year; rectocele (posterior vaginal wall descent) was identified in 15 (6.3%) women for an incidence of 1.58% per year; vaginal cough prolapse (apical descent) was present 21 (8.9%) women for an incidence of 2.2% per year. Perineal descent was absent in this group. In group II, there was no hypertrophic cervix; cystocele was present in 39 (16.5%) cases for an incidence of 4.13% per year; rectocele was identified in 27 (11.4%) women, amounting to an incidence of 2.85% per year; vaginal cough prolapse was present in 36 (15.%) women, an incidence of 3.75% per year; perineal descent was present in 63 (25.6%) women, for an incidence of 6.4% per year. CONCLUSION: (1) The incidence of hypertrophic cervix without any other abnormality amounted to 1.58% per year. This medical entity can present as uterine prolapse and was noted only in group I. (2) The annual incidence for hospital admission with a diagnosis of uterine prolapse was 2.1%. (3) The incidence of cystocele, and rectocele was not statistically different in the two groups; but the incidence of perineal descent and uterine prolapse were significantly more in group II than group I. (4) The etiology of hypertrophic cervix is not known, but it is of importance especially in the childbearing age when it may be related to prolonged pregnancy, cervical dystocia, etc. (+info)Dynamic MR imaging of outlet obstruction. (3/38)
The outlet obstruction syndrome encompasses all pelvic floor abnormalities which are responsible for an incomplete evacuation of fecal contents from the rectum. It has been estimated that outlet obstruction may be observed in half of constipated patients. A detailed clinical examination still represents the cornerstone of the diagnosis of these patients. However, there is general agreement that a reliable evaluation of the different pelvic floor abnormalities and the treatment decision highly depend on the imaging assessment. Traditionally, conventional defecography has played an important role in the radiological assessment of these patients but the technique is limited by its projectional nature and its inability to detect soft-tissue structures. Dynamic pelvic MR imaging using either closed-configuration or open-configuration MR systems is a rapidly evolving technique which has been gaining increased interest over the last years. The free selection of imaging planes, the good temporal resolution, and the excellent soft-tissue contrast have transformed this method into the preferred imaging modality in the evaluation of patients with pelvic floor dysfunction including rectocele, enterocele, internal rectal prolapse, and anismus. (+info)Management of disorders of the posterior pelvic floor. (4/38)
INTRODUCTION: Constipation is a relatively common problem affecting 15 percent of adults in the Western world, and over half of these cases are related to pelvic floor disorders. This article reviews the clinical presentation and diagnostic approach to posterior pelvic floor disorders, including how to image and treat them. METHODS: A Pubmed search using keywords "rectal prolapse," "rectocele," "perineal hernia," and "anismus" was performed, and bibliographies of the revealed articles were cross-referenced to obtain a representative cross-section of the literature, both investigational studies and reviews, that are currently available on posterior pelvic floor disorders. DISCUSSION: Pelvic floor disorders can occur with or without concomitant physical anatomical defects, and there are a number of imaging modalities available to detect such abnormalities in order to decide on the appropriate course of treatment. Depending on the nature of the disorder, operative or non-operative therapy may be indicated. CONCLUSION: Correctly diagnosing pelvic floor disorders can be complex and challenging, and the various imaging modalities as well as clinical history and exam must be considered together in order to arrive at a diagnosis. (+info)Tension free monofilament macropore polypropylene mesh (Gynemesh PS) in female genital prolapse repair. (5/38)
OBJECTIVES: To review intraoperative and postoperative complications associated to the correction of cystocele and rectocele with polypropylene mesh macropore monofilament (Gynemesh PS) using transvaginal free tension technique. MATERIALS AND METHODS: Prospective study of patients that have been submitted to correction of cystocele and/or rectocele between November 2004 and August 2005 in the Urogynecology and Vaginal Surgery Unit of Gynecology and Obstetrics Department, Las Condes Clinic. Mesh was used in 31 patients: 9 for cystocele, 11 for rectocele, and 11 for concomitant meshes. Total mesh used 42. Media age 55 years old, weight 64 kilograms. In 7 patients we used a third mesh for correction of urinary incontinence by TVT-O technique. RESULTS: They did not present intraoperative complications, neither in immediate or delayed postoperative time. We did not observe hematoma, infection, erosion or exposition mesh. Healing of cystocele and rectocele was obtained in 100% of patients, with a pursuit between 1 and 8 months. DISCUSSION: The use of prosthetic polypropylene monofilament macropore mesh in the correction of cystocele and/or rectocele, by transvaginal route with tension free technique seems to be a safe and effective surgery procedure. (+info)Sonomorphological evaluation of polypropylene mesh implants after vaginal mesh repair in women with cystocele or rectocele. (6/38)
OBJECTIVE: To investigate whether the sonographically measured size of the mesh implant in women who had undergone vaginal polypropylene mesh repair 6 weeks previously correlates with the original size of the mesh and whether the mesh ensures complete support of the anterior or posterior compartment. METHODS: Forty postmenopausal women with anterior or posterior vaginal wall prolapse and sonographically proven cystocele (n = 20) or rectocele (n = 20) were evaluated preoperatively and 6 weeks after vaginal mesh repair. Introital ultrasound was performed to identify the polypropylene mesh and measure its distal to proximal length and configuration as well as its thickness. The initial mesh length was compared with that measured by ultrasound 6 weeks postoperatively. Vaginal length was measured pre- and postoperatively. RESULTS: The mean +/- SD age of the women was 68 +/- 7 years. The 20 women with cystocele underwent repair by means of anterior transobturator mesh implantation; the initial mesh length was 6.8 +/- 1.1 cm versus 2.9 +/- 0.6 cm postoperatively. The 20 women with rectocele underwent repair by posterior transischioanal mesh implantation; the initial mesh length was 9.9 +/- 0.8 cm versus 3.3 +/- 0.5 cm postoperatively. The mesh supported 43.4% of the length of the anterior vaginal wall and this value was 53.7% for the posterior wall (P = 0.016). CONCLUSION: Sonography is recommended for postoperative evaluation of the anterior and posterior mesh positions after prolapse surgery. There is a considerable discrepancy between the implanted mesh size and the length measured 6 weeks later by postoperative ultrasound. Published by John Wiley & Sons, Ltd. (+info)Ultrasound assessment of pelvic organ prolapse: the relationship between prolapse severity and symptoms. (7/38)
OBJECTIVE: At present little information is available to help define whether a certain degree of pelvic organ prolapse is clinically relevant. We performed a retrospective study to define cut-offs for significant pelvic organ descent on the basis of prolapse symptoms. METHODS: At a tertiary urogynecological center, 735 women with symptoms of lower urinary tract dysfunction and prolapse were seen for interview, clinical examination, multi-channel urodynamics and ultrasound imaging, while supine and after voiding, for prolapse quantification. Women with multi-compartment prolapse, i.e. those in whom no compartment was clearly dominant were excluded. Receiver-operator statistics were used to test pelvic organ descent as a predictor of prolapse symptoms. RESULTS: Mean age was 55.1 years, mean parity 2.8 (range, 0-12). Symptoms of prolapse were reported by 188 women (25.6%). Seventy-four showed a symptomatic multi-compartment prolapse and were excluded, 56 symptomatic women had cystoceles and 48 had rectoceles. Symptomatic cystoceles descended on average to 23.8 mm below the symphysis pubis and symptomatic rectoceles to 21.4 mm below the symphysis pubis. Descent was strongly associated with symptoms of prolapse (both, P < 0.001). Receiver-operating characteristics (ROC) statistics suggested a cut-off of 10 mm below the symphysis pubis for cystocele, and 15 mm below the symphysis pubis for rectocele. ROC curves were similar for both compartments (area under the curve, 0.857 and 0.821, respectively). CONCLUSIONS: Descent of the bladder to > or = 10 mm and of the rectum to > or = 15 mm below the symphysis pubis are strongly associated with symptoms, and these values are proposed as cut-offs for the diagnosis of significant prolapse on the basis of ROC statistics. (+info)Posterior compartment anatomy as seen in magnetic resonance imaging and 3-dimensional reconstruction from asymptomatic nulliparas. (8/38)
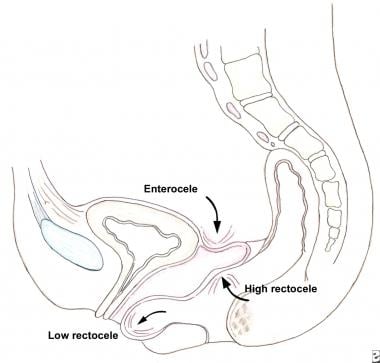
(+info)A rectocele is a type of pelvic organ prolapse, which occurs when the rectum (the lower end of the colon) bulges into the back wall of the vagina. This condition most commonly affects women who have gone through childbirth, although it can also occur in older women or those with long-term constipation or other conditions that put pressure on the pelvic floor muscles.
Rectoceles can cause a variety of symptoms, including difficulty having bowel movements, feeling like something is sticking out of the vagina, and pain during sexual intercourse. In some cases, rectoceles may not cause any symptoms at all. Treatment options for rectoceles include pelvic floor physical therapy, lifestyle changes (such as avoiding heavy lifting or straining), and in severe cases, surgery.
The exact medical definition of a rectocele is: "A herniation of the rectal wall into the vaginal wall, often associated with disruption of the rectovaginal septum." This means that there is a protrusion or bulge of the rectal wall into the vaginal wall, which can be caused by a weakening or tearing of the tissue that separates the two structures.
Defecography is a medical diagnostic procedure that involves taking X-ray images of the rectum and anus while a person is defecating. Also known as evacuation proctography, this test assesses how well the muscles and structures of the pelvic floor perform during a bowel movement. It can help identify issues such as rectal prolapse, intussusception, or abnormalities in muscle function that may be causing difficulties with defecation or fecal incontinence.
During the procedure, the individual is usually given an enema containing a contrast material, which makes the contents of the rectum visible on X-ray images. The person then sits on a special toilet seat placed within the X-ray machine, and is asked to strain and evacuate as if having a bowel movement. Fluoroscopic X-ray imaging is used to capture real-time images of the pelvic floor and surrounding structures during this process. The resulting images can help healthcare providers diagnose and treat various anorectal conditions.
Rectal prolapse is a medical condition where the rectum, which is the lower end of the colon, slips outside the anus, the opening through which stool leaves the body. This usually occurs due to weakened muscles and supporting structures in the pelvic area, often as a result of aging, childbirth, or long-term constipation or diarrhea.
The rectal prolapse can be partial, where only a small portion of the rectum slips outside the anus, or complete, where the entire rectum protrudes. This condition can cause discomfort, pain, bleeding, and difficulty with bowel movements. Treatment options may include dietary changes, medication, or surgical intervention.
A cystocele is a type of pelvic organ prolapse that occurs when the wall between the bladder and the vagina weakens and allows the bladder to bulge into the vagina. This condition is also sometimes referred to as a "prolapsed bladder." Cystoceles can cause various symptoms, including urinary incontinence, difficulty emptying the bladder completely, and discomfort or pain during sexual activity. The severity of a cystocele can vary, and treatment options may include lifestyle changes, pelvic floor exercises, or surgery.
Intussusception is a medical condition in which a part of the intestine telescopes into an adjacent section, leading to bowel obstruction and reduced blood flow. It often affects children under 3 years old but can also occur in adults. If not treated promptly, it can result in serious complications such as perforation, peritonitis, or even death. The exact cause is usually unknown, but it may be associated with infections, intestinal disorders, or tumors.
The pelvic floor is a group of muscles, ligaments, and connective tissues that form a sling or hammock across the bottom of the pelvis. It supports the organs in the pelvic cavity, including the bladder, rectum, and uterus or prostate. The pelvic floor helps control urination, defecation, and sexual function by relaxing and contracting to allow for the release of waste and during sexual activity. It also contributes to postural stability and balance. Weakness or damage to the pelvic floor can lead to various health issues such as incontinence, pelvic organ prolapse, and sexual dysfunction.
Constipation is a condition characterized by infrequent bowel movements or difficulty in passing stools that are often hard and dry. The medical definition of constipation varies, but it is generally defined as having fewer than three bowel movements in a week. In addition to infrequent bowel movements, other symptoms of constipation can include straining during bowel movements, feeling like you haven't completely evacuated your bowels, and experiencing hard or lumpy stools.
Constipation can have many causes, including a low-fiber diet, dehydration, certain medications, lack of physical activity, and underlying medical conditions such as irritable bowel syndrome or hypothyroidism. In most cases, constipation can be treated with lifestyle changes, such as increasing fiber intake, drinking more water, and getting regular exercise. However, if constipation is severe, persistent, or accompanied by other symptoms, it's important to seek medical attention to rule out any underlying conditions that may require treatment.
Defecation is the medical term for the act of passing stools (feces) through the anus. It is a normal bodily function that involves the contraction of muscles in the colon and anal sphincter to release waste from the body. Defecation is usually a regular and daily occurrence, with the frequency varying from person to person.
The stool is made up of undigested food, bacteria, and other waste products that are eliminated from the body through the rectum and anus. The process of defecation is controlled by the autonomic nervous system, which regulates involuntary bodily functions such as heart rate and digestion.
Difficulties with defecation can occur due to various medical conditions, including constipation, irritable bowel syndrome, and inflammatory bowel disease. These conditions can cause symptoms such as hard or painful stools, straining during bowel movements, and a feeling of incomplete evacuation. If you are experiencing any problems with defecation, it is important to speak with your healthcare provider for proper diagnosis and treatment.
A hernia is a protrusion of an organ or tissue through a weakened area in the abdominal wall, often appearing as a bulge beneath the skin. This condition can occur in various parts of the body such as the groin (inguinal hernia), navel (umbilical hernia), or site of a previous surgical incision (incisional hernia). Hernias may cause discomfort or pain, especially when straining, lifting heavy objects, or during bowel movements. In some cases, they may lead to serious complications like intestinal obstruction or strangulation, requiring immediate medical attention.
Uterine prolapse is a condition where the uterus descends or slips down from its normal position in the pelvic cavity into or through the cervix and sometimes even outside the vaginal opening. This occurs due to the weakening of the muscles and ligaments that support the uterus, often as a result of childbirth, aging, menopause, obesity, or prior hysterectomy. Uterine prolapse can lead to various symptoms such as a feeling of heaviness in the pelvis, difficulty in urinating or having bowel movements, and uncomfortable sexual intercourse. The severity of the condition may vary from mild to severe, and treatment options range from lifestyle changes and physical therapy to surgery.
Rectal diseases refer to conditions that affect the structure or function of the rectum, which is the lower end of the large intestine, just above the anus. The rectum serves as a storage area for stool before it is eliminated from the body. Some common rectal diseases include:
1. Hemorrhoids: Swollen veins in the rectum or anus that can cause pain, itching, bleeding, and discomfort.
2. Rectal cancer: Abnormal growth of cells in the rectum that can invade and destroy nearby tissue and spread to other parts of the body.
3. Anal fissures: Small tears in the lining of the anus that can cause pain, bleeding, and itching.
4. Rectal prolapse: A condition where the rectum slips outside the anus, causing discomfort, fecal incontinence, and other symptoms.
5. Inflammatory bowel disease (IBD): A group of chronic inflammatory conditions that affect the digestive tract, including the rectum, such as Crohn's disease and ulcerative colitis.
6. Rectal abscess: A collection of pus in the rectum caused by an infection, which can cause pain, swelling, and fever.
7. Fistula-in-ano: An abnormal connection between the rectum and the skin around the anus, which can cause drainage of pus or stool.
8. Rectal foreign bodies: Objects that are accidentally or intentionally inserted into the rectum and can cause injury, infection, or obstruction.
These are just a few examples of rectal diseases, and there are many other conditions that can affect the rectum. If you experience any symptoms related to the rectum, it is important to seek medical attention from a healthcare professional for proper diagnosis and treatment.
Surgical stapling is a medical technique that uses specialized staplers to place linear staple lines to close surgical incisions, connect or remove organs and tissues during surgical procedures. Surgical staples are made of titanium or stainless steel and can be absorbable or non-absorbable. They provide secure, fast, and accurate wound closure, reducing the risk of infection and promoting faster healing compared to traditional suturing methods.
The surgical stapler consists of a handle, an anvil, and a cartridge containing multiple staples. The device is loaded with staple cartridges and used to approximate tissue edges before deploying the staples. Once the staples are placed, the stapler is removed, leaving the staple line in place.
Surgical stapling has various applications, including gastrointestinal anastomosis, lung resection, vascular anastomosis, and skin closure. It is widely used in different types of surgeries, such as open, laparoscopic, and robotic-assisted procedures. The use of surgical stapling requires proper training and expertise to ensure optimal patient outcomes.
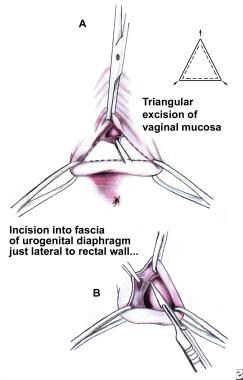
The perineum is the region between the anus and the genitals. In anatomical terms, it refers to the diamond-shaped area located in the lower part of the pelvis and extends from the coccyx (tailbone) to the pubic symphysis, which is the joint in the front where the two pubic bones meet. This region contains various muscles that support the pelvic floor and contributes to maintaining urinary and fecal continence. The perineum can be further divided into two triangular regions: the urogenital triangle (anterior) and the anal triangle (posterior).
Surgical staplers are medical devices used in various surgical procedures to create secure and precise connections between tissues, vessels, or organs. They function by placing sterile, disposable staple cartridges into the device that contain rows of stainless steel staples. The stapler then applies pressure to deform the staples, forming a B-shaped staple line that holds the tissue together.
These devices are often used in place of traditional suturing methods due to their speed, accuracy, and ability to reduce surgical trauma. They can be employed in various types of surgeries, including gastrointestinal, thoracic, gynecologic, and orthopedic procedures.
Surgical staplers come in different shapes and sizes, with some designed for specific applications such as linear or circular stapling. Linear staplers are used to create straight lines of staples, while circular staplers form a ring-shaped connection, often used in anastomosis procedures (the joining of two hollow organs or vessels).
It is essential to follow proper techniques and indications when using surgical staplers, as improper usage can lead to complications such as bleeding, infection, leakage, or even tissue necrosis.
The digestive system is a series of organs that work together to convert food into nutrients and energy. Digestive system surgical procedures involve operations on any part of the digestive system, including the esophagus, stomach, small intestine, large intestine, liver, pancreas, and gallbladder. These procedures can be performed for a variety of reasons, such as to treat diseases, repair damage, or remove cancerous growths.
Some common digestive system surgical procedures include:
1. Gastric bypass surgery: A procedure in which the stomach is divided into two parts and the smaller part is connected directly to the small intestine, bypassing a portion of the stomach and upper small intestine. This procedure is used to treat severe obesity.
2. Colonoscopy: A procedure in which a flexible tube with a camera on the end is inserted into the rectum and colon to examine the lining for polyps, cancer, or other abnormalities.
3. Colectomy: A procedure in which all or part of the colon is removed, often due to cancer, inflammatory bowel disease, or diverticulitis.
4. Gastrostomy: A procedure in which a hole is made through the abdominal wall and into the stomach to create an opening for feeding. This is often done for patients who have difficulty swallowing.
5. Esophagectomy: A procedure in which all or part of the esophagus is removed, often due to cancer. The remaining esophagus is then reconnected to the stomach or small intestine.
6. Liver resection: A procedure in which a portion of the liver is removed, often due to cancer or other diseases.
7. Pancreatectomy: A procedure in which all or part of the pancreas is removed, often due to cancer or chronic pancreatitis.
8. Cholecystectomy: A procedure in which the gallbladder is removed, often due to gallstones or inflammation.
These are just a few examples of digestive system surgical procedures. There are many other types of operations that can be performed on the digestive system depending on the specific needs and condition of each patient.
Fecal incontinence is the involuntary loss or leakage of stool (feces) from the rectum. It is also known as bowel incontinence. This condition can range from occasional leakage of stool when passing gas to a complete loss of bowel control. Fecal incontinence can be an embarrassing and distressing problem, but there are treatments available that can help improve symptoms and quality of life.
The causes of fecal incontinence can vary, but some common factors include:
* Damage to the muscles or nerves that control bowel function, such as from childbirth, surgery, spinal cord injury, or long-term constipation or diarrhea.
* Chronic digestive conditions, such as irritable bowel syndrome (IBS), inflammatory bowel disease (IBD), or celiac disease.
* Neurological conditions, such as multiple sclerosis, stroke, or spina bifida.
* Aging, which can lead to a decrease in muscle strength and control.
Treatment for fecal incontinence depends on the underlying cause of the condition. Treatments may include:
* Bowel training exercises to improve muscle strength and control.
* Changes in diet to help regulate bowel movements.
* Medications to treat constipation or diarrhea.
* Surgery to repair damaged muscles or nerves, or to create a new opening for stool to exit the body.
If you are experiencing symptoms of fecal incontinence, it is important to speak with your healthcare provider. They can help determine the cause of your symptoms and develop an appropriate treatment plan.
The rectum is the lower end of the digestive tract, located between the sigmoid colon and the anus. It serves as a storage area for feces before they are eliminated from the body. The rectum is about 12 cm long in adults and is surrounded by layers of muscle that help control defecation. The mucous membrane lining the rectum allows for the detection of stool, which triggers the reflex to have a bowel movement.
The anal canal is the terminal portion of the digestive tract, located between the rectum and the anus. It is a short tube-like structure that is about 1 to 1.5 inches long in adults. The main function of the anal canal is to provide a seal for the elimination of feces from the body while also preventing the leakage of intestinal contents.
The inner lining of the anal canal is called the mucosa, which is kept moist by the production of mucus. The walls of the anal canal contain specialized muscles that help control the passage of stool during bowel movements. These muscles include the internal and external sphincters, which work together to maintain continence and allow for the voluntary release of feces.
The anal canal is an important part of the digestive system and plays a critical role in maintaining bowel function and overall health.