Sphincter of Oddi Dysfunction
Sphincter of Oddi
Common Bile Duct Diseases
Sphincterotomy, Endoscopic
Postcholecystectomy Syndrome
Technetium Tc 99m Lidofenin
Cholangiopancreatography, Endoscopic Retrograde
Technetium Tc 99m Disofenin
Sphincterotomy, Transhepatic
Ampulla of Vater
Pancreatitis
Trimebutine
Anal Canal
Esophagogastric Junction
Esophageal Sphincter, Upper
Fecal Incontinence
Pressure
Urinary Sphincter, Artificial
Urethra
Prospective Studies
Opossums
Erectile Dysfunction
Ventricular Dysfunction, Left
Endoscopic sphincterotomy in the treatment of cholangiopancreatic diseases. (1/29)
AIM: To investigate the therapeutic effect of endoscopic sphincterotomy (EST) in the treatment of choledocholithiasis and stenosing papillitis. METHODS: A total of 1 026 patients undergoing EST during July 1983 to May 2003 at the institute were retrospectively analyzed. Chronic pancreatitis was diagnosed in 63 (6.1%), cholecystolithiasis and choledocholithiasis in 549 (53.5%), stones in residual biliary duct in 249 (24.3%), stenosing papillitis in 228 (22.2%). In patients with simple stenosing papillitis, most incisions were within 0.5-1 cm in length. As for patients with chronic pancreatitis simultaneously, selective pancreatic sphincterotomy was performed, and incision was within 0.5-0.8 cm in length. For stones less than 1 cm, incision was from 1 to 1.5 cm, and for those larger than 1 cm, incision ranged from 1.5 to 3 cm. For stones more than 2 cm in diameter, detritus basket rather than simple incision was chosen. RESULTS: Of the 798 patients with choledocholithiasis, 764 (93.5%) had successful stone clearance, 215 (94.3%) out of 228 cases of stenosing papillitis were cured totally, while 63 had chronic pancreatitis developed from stenosing papillitis, 57 (90.1%) had sound remission of symptoms, though membranous stenosis emerged in 13 of 57 which was treated with balloon dilatation. After the operation, only 21 cases (2.1%) had complications such as severe pancreatitis and incision bleeding. None of the patients died. CONCLUSION: EST is an ideal surgical management with mini-invasion in the treatment of choledocholithiasis and stenosing papillitis. (+info)The underestimated role of opiates in patients with suspected sphincter of Oddi dysfunction after cholecystectomy. (2/29)
AIMS: Pain recurrence after cholecystectomy is often attributed to sphincter of Oddi dysfunction, whose diagnostic criteria and treatments remain uncertain. We performed a retrospective study to assess the possible precipitating role of opiate ingestion in this setting. METHODS: The retrospective study of the files of 147 consecutive patients investigated for post-cholecystectomy syndrome by endoscopic ultrasonography and/or endoscopic retrograde cholangiography yielded 37 cases of suspected biliary-type sphincter of Oddi dysfunction. RESULTS: Thirteen patients (30%) with suspected sphincter of Oddi dysfunction had taken opiate-containing drugs 15 minutes to two hours (median 1 hr) before the onset of pain ("Opiate group"). When compared with the 23 patients having not taken opiates ("Non Opiate Group"), they were significantly younger (47 vs. 60 yrs), had a narrower common bile duct (5.0 vs. 7.7 mm), but had similar biochemical abnormalities and belonged to the same Milwaukee's classes, mainly class II. None of the patients in the "Opiate group" were submitted to retrograde cholangiography or endoscopic sphincterotomy vs. 52% and 39%, respectively of the patients of the "Non-Opiate Group". After a mean follow-up of 3.5 years, there were three recurrences of biliary-type pain (1 choledochal stone, and 2 suspected sphincter of Oddi dysfunction) in the "Opiate Group", and 2 (1 choledochal stone, 1 after codeine intake) in the "Non-Opiate Group". CONCLUSIONS: Opiate intake is a frequent cause of suspicion of sphincter of Oddi dysfunction after cholecystectomy, especially in young patients with a narrow common bile duct. A careful history taking is essential to avoid unnecessary and potentially harmful procedures. (+info)Evaluation of the biliary tract in patients with functional biliary symptoms. (3/29)
The aim of this paper was to describe functional biliary syndromes and methods for evaluation of the biliary tract in these patients. Functional biliary symptoms can be defined as biliary symptoms without demonstrable organic substrate. Two main syndromes exist: Gallbladder dysfunction and sphincter of Oddi dysfunction. The most important investigative tools are cholescintigraphy and endoscopic sphincter of Oddi manometry. In gallbladder dysfunction a scintigraphic gallbladder ejection fraction below 35% can select patients who will benefit from cholecystectomy. Endoscopic sphincter of Oddi manometry is considered the gold standard in sphincter of Oddi dysfunction but recent development in scintigraphic methods is about to change this. Thus, calculation of hilum-to-duodenum transit time and duodenal appearance time on cholescintigraphy have proven useful in these patients. In conclusion, ambient methods can diagnose functional biliary syndromes. However, there are still a number of issues where further knowledge is needed. Probably the next step forward will be in the area of sensory testing and impedance planimetric methods. (+info)Sphincter of Oddi dysfunction: managing the patient with chronic biliary pain. (4/29)
Sphincter of Oddi dysfunction (SOD) is a syndrome of chronic biliary pain or recurrent pancreatitis due to functional obstruction of pancreaticobiliary flow at the level of the sphincter of Oddi. The Milwaukee classification stratifies patients according to their clinical picture based on elevated liver enzymes, dilated common bile duct and presence of abdominal pain. Type I patients have pain as well as abnormal liver enzymes and a dilated common bile duct. Type II SOD consists of pain and only one objective finding, and Type III consists of biliary pain only. This classification is useful to guide diagnosis and management of sphincter of Oddi dysfunction. The current gold standard for diagnosis is manometry to detect elevated sphincter pressure, which correlates with outcome to sphincterotomy. However, manometry is not widely available and is an invasive procedure with a risk of pancreatitis. Non-invasive testing methods, including fatty meal ultrasonography and scintigraphy, have shown limited correlation with manometric findings but may be useful in predicting outcome to sphincterotomy. Endoscopic injection of botulinum toxin appears to predict subsequent outcome to sphincterotomy, and could be useful in selection of patients for therapy, especially in the setting where manometry is unavailable. (+info)Prospective comparison of secretin-stimulated magnetic resonance cholangiopancreatography with manometry in the diagnosis of sphincter of Oddi dysfunction types II and III. (5/29)
BACKGROUND: In sphincter of Oddi dysfunction (SOD), sphincter of Oddi manometry (SOM) predicts the response to sphincterotomy, but is invasive and associated with complications. AIM: To evaluate the role of secretin-stimulated magnetic resonance cholangiopancreatography (ss-MRCP) in predicting the results of SOM in patients with suspected type II or III SOD. METHODS: MRCP was performed at baseline and at 1, 3, 5 and 7 min after intravenous secretin. SOD was diagnosed when the mean basal sphincter pressure at SOM was >40 mm Hg. Long-term outcome after SOM, with or without endoscopic sphincterotomy, was assessed using an 11-point (0-10) Likert scale. RESULTS: Of 47 patients (male/female 9/38; mean age 46 years; range 27-69 years) referred for SOM, 27 (57%) had SOD and underwent biliary and/or pancreatic sphincterotomy. ss-MRCP was abnormal in 10/16 (63%) type II and 0/11 type III SOD cases. The diagnostic accuracy of ss-MRCP for SOD types II and III was 73% and 46%, respectively. During a mean follow-up of 31.6 (range 17-44) months, patients with normal SOM and SOD type II experienced a significant reduction in symptoms (mean Likert score 8 vs 4; p = 0.03, and 9 vs 1.6; p = 0.0002, respectively), whereas in patients with SOD type III, there was no improvement in pain scores. All patients with SOD and an abnormal ss-MRCP (n = 12) reported long-term symptom improvement (mean Likert score 9.2 v 1.2, p<0.001). CONCLUSIONS: ss-MRCP is insensitive in predicting abnormal manometry in patients with suspected type III SOD, but is useful in selecting patients with suspected SOD II who are most likely to benefit from endotherapy. (+info)Characterization of functional biliary pain and dyspeptic symptoms in patients with sphincter of Oddi dysfunction: effect of papillotomy. (6/29)
AIM: To characterize functional biliary pain and other gastrointestinal (GI) symptoms in postcholecystectomy syndrome (PCS) patients with and without sphincter of Oddi dysfunction (SOD) proved by endoscopic sphincter of Oddi manometry (ESOM), and to assess the post-endoscopic sphincterotomy (EST) outcome. METHODS: We prospectively investigated 85 cholecystectomized patients referred for ERCP because of PCS and suspected SOD. On admission, all patients completed our questionnaire. Physical examination, laboratory tests, abdominal ultrasound, quantitative hepatobiliary scintigraphy (QHBS), and ERCP were performed in all patients. Based on clinical and ERCP findings 15 patients had unexpected bile duct stone disease and 15 patients had SOD biliary type I. ESOM demonstrated an elevated basal pressure in 25 patients with SOD biliary-type III. In the remaining 30 cholecystectomized patients without SOD, the liver function tests, ERCP, QHBS and ESOM were all normal. As a control group, 30 'asymptomatic' cholecystectomized volunteers (attended to our hospital for general cardiovascular screening) completed our questionnaire, which is consisted of 50 separate questions on GI symptoms and abdominal pain characteristics. Severity of the abdominal pain (frequency and intensity) was assessed with a visual analogue scale (VAS). In 40 of 80 patients having definite SOD (i.e. patients with SOD biliary type I and those with elevated SO basal pressure on ESOM), an EST was performed just after ERCP. In these patients repeated questionnaires were filled at each follow-up visit (at 3 and 6 mo) and a second look QHBS was performed 3 mo after the EST to assess the functional response to EST. RESULTS: The analysis of characteristics of the abdominal pain demonstrated that patients with common bile duct stone and definite SOD had a significantly higher score of symptomatic agreement with previously determined biliary-like pain features than patient groups of PCS without SOD and controls. In contrary, no significant differences were found when the pain severity scores were compared in different groups of PCS patients. In patients with definite SOD, EST induced a significant acceleration of the transpapillary bile flow; and based on the comparison of VASs obtained from the pre- and post-EST questionnaires, the severity scores of abdominal pain were significantly improved, however, only 15 of 35 (43%) patients became completely pain free. Post-EST severity of abdominal pain by VASs was significantly higher in patients with predominant dyspepsia at initial presentation as compared to those without dyspeptic symptoms. CONCLUSION: Persistent GI symptoms and general patient dissatisfaction is a rather common finding after EST in patients with SOD, and correlated with the presence of predominant dyspeptic symptoms at the initial presentation, but does not depend on the technical and functional success of EST. (+info)ERCP in acute pancreatitis. (7/29)
BACKGROUND: The role of endoscopic retrograde cholangiopancreatography (ERCP) in the management of acute pancreatitis has evolved over years since its introduction in 1968. Its importance in diagnosing the etiology of pancreatitis has steadily declined with the advent of less invasive diagnostic tools. The therapeutic implications of ERCP in acute pancreatitis are many fold and are directed towards management of known etiological factors or its related complications. This article highlights the current status of ERCP in acute pancreatitis. DATA SOURCES: An English literature search using PubMed database was conducted on ERCP in acute pancreatitis, the etiologies and complications of pancreatitis amenable to endotherapy and other related subjects, which were reviewed. RESULTS: ERCP serves as a primary therapeutic modality for management of biliary pancreatitis in specific situations, pancreatitis due to microlithiasis, specific types of sphincter of Oddi dysfunction, pancreas divisum, ascariasis and malignancy. In recurrent acute pancreatitis and smoldering pancreatitis it has a definite therapeutic utility. Complications of acute pancreatitis including pancreatic-duct disruptions or leaks, benign pancreatic-fluid collections and pancreatic necrosis can be beneficially dealt with. Intraductal ultrasound and pancreatoscopy during ERCP are useful in detecting pancreatic malignancy. CONCLUSIONS: The role of ERCP in acute pancreatitis is predominantly therapeutic and occasionally diagnostic. Its role in the management continues to evolve and advanced invasive procedures should be undertaken only in centers dedicated to pancreatic care. (+info)Relationship between intraduodenal peri-ampullary diverticulum and biliary disease in 178 patients undergoing ERCP. (8/29)
BACKGROUND: The presence of intraduodenal peri-ampullary diverticulum is often observed during upper digestive tract barium meal studies and endoscopic retrograde cholangiopancreatography (ERCP). A few papers in China and overseas reported that the diverticulum had something to do with the incidence of cholelithiasis. This study was undertaken to further test this notion and ascertain the relationship between intraduodenal peri-ampullary diverticulum and biliary disease, especially the formation of bile duct pigment stones. METHODS: A total of 178 patients who had undergone ERCP or endoscopic sphincterotomy (EST) were studied retrospectively. They were divided into 6 groups according to the category of biliary disease, and the incidence rates of intraduodenal peri-ampullary diverticulum were calculated. RESULTS: There were 44 patients with intraduodenal peri-ampullary diverticulum in 81 patients with primary bile duct pigment stones (54.32%), 4 in 8 patients with bile duct stones and gallbladder stones (50%), 7 in 33 patients with bile duct stones secondary to gallbladder stones (21.21%), 3 in 21 patients with inflammation and stricture of the end of the bile duct and papilla (14.29%), 1 in 22 patients with carcinoma of the end of the bile duct and papilla (4.54%), and 5 in 13 patients with post-cholecystectomy syndrome or sphincter of Oddi dysfunction (38.46%). CONCLUSIONS: The incidence rate of intraduodenal peri-ampullary diverticulum in patients with primary bile duct pigment stones is higher than that in patients with bile duct stones secondary to gallbladder stones, patients with inflammation and stricture of the end of the bile duct and papilla, and patients with carcinoma of the end of the bile duct and papilla. These findings indicate that the anatomical abnormalities and malfunction of the sphincter of Oddi play an important role in the formation of bile duct pigment stones. (+info)Sphincter of Oddi dysfunction (SOD) is a condition characterized by abnormalities in the functioning of the Sphincter of Oddi, which is a muscular valve that controls the flow of bile and pancreatic juice from the pancreas and gallbladder into the duodenum (the first part of the small intestine).
In SOD, the sphincter may either fail to relax properly or become overactive, leading to a variety of symptoms such as abdominal pain, nausea, vomiting, bloating, and elevated liver enzymes. The condition can be classified into two types: Type I, which is associated with elevated liver enzymes and/or pancreatic enzymes, and Type II, which is characterized by abdominal pain without biochemical abnormalities.
The diagnosis of SOD typically involves a series of tests such as manometry (measuring the pressure inside the sphincter), endoscopic ultrasound, or magnetic resonance cholangiopancreatography (MRCP) to visualize the anatomy and function of the sphincter. Treatment options may include medications to relax the sphincter, endoscopic therapy to cut or stretch the muscle, or surgery in severe cases.
The Sphincter of Oddi is a muscular valve that controls the flow of bile and pancreatic juice from the pancreatic and bile ducts into the duodenum, which is the first part of the small intestine. It is named after Ruggero Oddi, an Italian physiologist who discovered it in 1887. The Sphincter of Oddi has two parts: the sphincter papillae, which surrounds the common opening of the pancreatic and bile ducts into the duodenum, and the sphincter choledochus, which is located more proximally in the bile duct. The contraction and relaxation of these muscles help regulate the release of digestive enzymes from the pancreas and the flow of bile from the liver to aid in digestion.
Common bile duct diseases refer to conditions that affect the common bile duct, a tube that carries bile from the liver and gallbladder into the small intestine. Some common examples of common bile duct diseases include:
1. Choledocholithiasis: This is the presence of stones (calculi) in the common bile duct, which can cause blockage, inflammation, and infection.
2. Cholangitis: This is an infection or inflammation of the common bile duct, often caused by obstruction due to stones, tumors, or strictures.
3. Common bile duct cancer (cholangiocarcinoma): This is a rare but aggressive cancer that arises from the cells lining the common bile duct.
4. Biliary strictures: These are narrowing or scarring of the common bile duct, which can be caused by injury, inflammation, or surgery.
5. Benign tumors: Non-cancerous growths in the common bile duct can also cause blockage and other symptoms.
Symptoms of common bile duct diseases may include abdominal pain, jaundice (yellowing of the skin and eyes), fever, chills, nausea, vomiting, and dark urine or light-colored stools. Treatment depends on the specific condition and severity but may include medications, endoscopic procedures, surgery, or a combination of these approaches.
Endoscopic sphincterotomy is a medical procedure that involves the use of an endoscope (a flexible tube with a light and camera) to cut the papilla of Vater, which contains the sphincter of Oddi muscle. This procedure is typically performed to treat gallstones or to manage other conditions related to the bile ducts or pancreatic ducts.
The sphincterotomy helps to widen the opening of the papilla, allowing stones or other obstructions to pass through more easily. It may also be used to relieve pressure and pain caused by spasms of the sphincter of Oddi muscle. The procedure is usually done under sedation or anesthesia and carries a risk of complications such as bleeding, infection, perforation, and pancreatitis.
Postcholecystectomy Syndrome is a condition that occurs in some patients following the surgical removal of the gallbladder (cholecystectomy). The syndrome encompasses a variety of symptoms such as abdominal pain, bloating, gas, indigestion, and diarrhea, which can be caused by several factors including:
1. Abnormal functioning or motility of the sphincter of Oddi (a muscle that controls the flow of bile and pancreatic juice into the small intestine)
2. Formation of gallstones in the bile ducts (choledocholithiasis)
3. Biliary dyskinesia (impaired functioning of the biliary tract muscles)
4. Persistent or recurrent infection or inflammation of the bile ducts (biliopathy)
5. Formation of abnormal bile-filled pouches (biliolethiasis or bile duct cysts)
6. Changes in bowel habits due to altered enterohepatic circulation of bile acids
The symptoms of Postcholecystectomy Syndrome can vary in severity and frequency, and they may appear soon after the surgery or develop months or even years later. The diagnosis of this condition typically involves a comprehensive medical evaluation, including a detailed history, physical examination, laboratory tests, and imaging studies such as ultrasound, CT scan, MRI, or endoscopic retrograde cholangiopancreatography (ERCP).
Treatment options for Postcholecystectomy Syndrome depend on the underlying cause of the symptoms and may include medications, dietary modifications, endoscopic procedures, or surgery. In some cases, the syndrome may resolve on its own without any specific treatment.
Manometry is a medical test that measures pressure inside various parts of the gastrointestinal tract. It is often used to help diagnose digestive disorders such as achalasia, gastroparesis, and irritable bowel syndrome. During the test, a thin, flexible tube called a manometer is inserted through the mouth or rectum and into the area being tested. The tube is connected to a machine that measures and records pressure readings. These readings can help doctors identify any abnormalities in muscle function or nerve reflexes within the digestive tract.
Technetium Tc 99m Lidofenin is a radiopharmaceutical used in nuclear medicine imaging procedures, specifically for hepatobiliary scintigraphy. It is a technetium-labeled compound, where the radioisotope technetium-99m (^99m^Tc) is bound to lidofenin, a liver-imaging agent.
The compound is used to assess the function and anatomy of the liver, gallbladder, and biliary system. After intravenous administration, Technetium Tc 99m Lidofenin is taken up by hepatocytes (liver cells) and excreted into the bile ducts and ultimately into the small intestine. The distribution and excretion of this radiopharmaceutical can be monitored using a gamma camera, providing functional information about the liver and biliary system.
It is essential to note that the use of Technetium Tc 99m Lidofenin should be under the guidance and supervision of healthcare professionals trained in nuclear medicine, as its administration and handling require specific expertise and safety measures due to the radioactive nature of the compound.
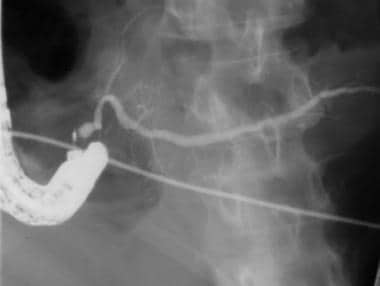
Endoscopic retrograde cholangiopancreatography (ERCP) is a medical procedure that combines upper gastrointestinal (GI) endoscopy and fluoroscopy to diagnose and treat certain problems of the bile ducts and pancreas.
During ERCP, a flexible endoscope (a long, thin, lighted tube with a camera on the end) is passed through the patient's mouth and throat, then through the stomach and into the first part of the small intestine (duodenum). A narrow plastic tube (catheter) is then inserted through the endoscope and into the bile ducts and/or pancreatic duct. Contrast dye is injected through the catheter, and X-rays are taken to visualize the ducts.
ERCP can be used to diagnose a variety of conditions affecting the bile ducts and pancreas, including gallstones, tumors, strictures (narrowing of the ducts), and chronic pancreatitis. It can also be used to treat certain conditions, such as removing gallstones from the bile duct or placing stents to keep the ducts open in cases of stricture.
ERCP is an invasive procedure that carries a risk of complications, including pancreatitis, infection, bleeding, and perforation (a tear in the lining of the GI tract). It should only be performed by experienced medical professionals in a hospital setting.
Technetium Tc 99m Disofenin is not a medical condition, but rather a radiopharmaceutical used in diagnostic imaging. It is a radioactive tracer used in nuclear medicine scans, specifically for liver and biliary system imaging. The compound consists of the radioisotope Technetium-99m (Tc-99m) bonded to the pharmaceutical Disofenin.
The Tc-99m is a gamma emitter with a half-life of 6 hours, making it ideal for diagnostic imaging. When administered to the patient, the compound is taken up by the liver and excreted into the bile ducts and gallbladder, allowing medical professionals to visualize these structures using a gamma camera. This can help detect various conditions such as tumors, gallstones, or obstructions in the biliary system.
It's important to note that Technetium Tc 99m Disofenin is used diagnostically and not for therapeutic purposes. The radiation exposure from this compound is generally low and considered safe for diagnostic use. However, as with any medical procedure involving radiation, the benefits and risks should be carefully weighed and discussed with a healthcare professional.
Cholecystectomy is a medical procedure to remove the gallbladder, a small pear-shaped organ located on the right side of the abdomen, just beneath the liver. The primary function of the gallbladder is to store and concentrate bile, a digestive fluid produced by the liver. During a cholecystectomy, the surgeon removes the gallbladder, usually due to the presence of gallstones or inflammation that can cause pain, infection, or other complications.
There are two primary methods for performing a cholecystectomy:
1. Open Cholecystectomy: In this traditional surgical approach, the surgeon makes an incision in the abdomen to access and remove the gallbladder. This method is typically used when there are complications or unique circumstances that make laparoscopic surgery difficult or risky.
2. Laparoscopic Cholecystectomy: This is a minimally invasive surgical procedure where the surgeon makes several small incisions in the abdomen, through which a thin tube with a camera (laparoscope) and specialized surgical instruments are inserted. The surgeon then guides these tools to remove the gallbladder while viewing the internal structures on a video monitor.
After the gallbladder is removed, bile flows directly from the liver into the small intestine through the common bile duct, and the body continues to function normally without any significant issues.
Transhepatic sphincterotomy is a medical procedure that involves the incision or cutting of the papilla of Vater, which is a small muscular structure located at the junction of the common bile duct and the main pancreatic duct, with the ampulla of Vater, within the second part of the duodenum. This procedure is performed using a special type of endoscope that is passed through the liver (transhepatically) to access the bile ducts.
The goal of transhepatic sphincterotomy is to relieve obstructions or blockages in the bile ducts, such as gallstones or tumors, that cannot be removed using other endoscopic techniques. This procedure is typically performed by an interventional radiologist or a gastroenterologist with specialized training in endoscopic retrograde cholangiopancreatography (ERCP).
Transhepatic sphincterotomy is considered a higher-risk procedure than traditional ERCP sphincterotomy due to the need for liver puncture and the potential complications associated with this approach, including bleeding, infection, and injury to surrounding organs. However, it may be necessary in certain situations where traditional ERCP is not feasible or has failed.
The ampulla of Vater, also known as hepatopancreatic ampulla, is a dilated portion of the common bile duct where it joins the main pancreatic duct and empties into the second part of the duodenum. It serves as a conduit for both bile from the liver and digestive enzymes from the pancreas to reach the small intestine, facilitating the digestion and absorption of nutrients. The ampulla of Vater is surrounded by a muscular sphincter, the sphincter of Oddi, which controls the flow of these secretions into the duodenum.
Pancreatitis is a medical condition characterized by inflammation of the pancreas, a gland located in the abdomen that plays a crucial role in digestion and regulating blood sugar levels. The inflammation can be acute (sudden and severe) or chronic (persistent and recurring), and it can lead to various complications if left untreated.
Acute pancreatitis often results from gallstones or excessive alcohol consumption, while chronic pancreatitis may be caused by long-term alcohol abuse, genetic factors, autoimmune conditions, or metabolic disorders like high triglyceride levels. Symptoms of acute pancreatitis include severe abdominal pain, nausea, vomiting, fever, and increased heart rate, while chronic pancreatitis may present with ongoing abdominal pain, weight loss, diarrhea, and malabsorption issues due to impaired digestive enzyme production. Treatment typically involves supportive care, such as intravenous fluids, pain management, and addressing the underlying cause. In severe cases, hospitalization and surgery may be necessary.
Trimebutine is an antispasmodic drug that is primarily used to treat functional gastrointestinal disorders, such as irritable bowel syndrome (IBS). It works by relaxing the smooth muscles in the intestines, which helps to reduce cramping, pain, and spasms.
Trimebutine is a derivative of the opioid alkaloid thebaine, but it does not have any significant analgesic or addictive properties. It is thought to exert its effects by acting on certain receptors in the intestinal muscles, including 5-HT3 and mu-opioid receptors.
Trimebutine is available in various forms, such as tablets, capsules, and syrup, and it is typically taken orally several times a day. The dosage may vary depending on the individual's age, weight, and medical condition.
It is important to note that trimebutine should only be used under the supervision of a healthcare provider, as it can have side effects and interact with other medications. Some common side effects of trimebutine include dizziness, dry mouth, and constipation.
The anal canal is the terminal portion of the digestive tract, located between the rectum and the anus. It is a short tube-like structure that is about 1 to 1.5 inches long in adults. The main function of the anal canal is to provide a seal for the elimination of feces from the body while also preventing the leakage of intestinal contents.
The inner lining of the anal canal is called the mucosa, which is kept moist by the production of mucus. The walls of the anal canal contain specialized muscles that help control the passage of stool during bowel movements. These muscles include the internal and external sphincters, which work together to maintain continence and allow for the voluntary release of feces.
The anal canal is an important part of the digestive system and plays a critical role in maintaining bowel function and overall health.
The esophagogastric junction (EGJ) is the region of the gastrointestinal tract where the esophagus (the tube that carries food from the mouth to the stomach) meets the stomach. It serves as a physiological sphincter, which helps control the direction of flow and prevent reflux of gastric contents back into the esophagus. The EGJ is also known as the gastroesophageal junction or cardia.
The upper esophageal sphincter (UES) is a band of muscle fibers located at the upper end of the esophagus, where it meets the throat or pharynx. The UES acts as a physiological barrier between the pharynx and the esophagus, helping to prevent the reflux of gastric contents into the upper airway.
During swallowing, the UES relaxes to allow the passage of food from the mouth into the esophagus, and then contracts again to prevent the backflow of food or stomach acid into the throat. The UES also plays a role in protecting the airway during activities such as coughing, sneezing, or vomiting, by closing to prevent the entry of foreign materials or fluids into the lungs.
Abnormalities in UES function can contribute to various swallowing disorders and respiratory symptoms, such as aspiration, coughing, and choking.
Fecal incontinence is the involuntary loss or leakage of stool (feces) from the rectum. It is also known as bowel incontinence. This condition can range from occasional leakage of stool when passing gas to a complete loss of bowel control. Fecal incontinence can be an embarrassing and distressing problem, but there are treatments available that can help improve symptoms and quality of life.
The causes of fecal incontinence can vary, but some common factors include:
* Damage to the muscles or nerves that control bowel function, such as from childbirth, surgery, spinal cord injury, or long-term constipation or diarrhea.
* Chronic digestive conditions, such as irritable bowel syndrome (IBS), inflammatory bowel disease (IBD), or celiac disease.
* Neurological conditions, such as multiple sclerosis, stroke, or spina bifida.
* Aging, which can lead to a decrease in muscle strength and control.
Treatment for fecal incontinence depends on the underlying cause of the condition. Treatments may include:
* Bowel training exercises to improve muscle strength and control.
* Changes in diet to help regulate bowel movements.
* Medications to treat constipation or diarrhea.
* Surgery to repair damaged muscles or nerves, or to create a new opening for stool to exit the body.
If you are experiencing symptoms of fecal incontinence, it is important to speak with your healthcare provider. They can help determine the cause of your symptoms and develop an appropriate treatment plan.
In medical terms, pressure is defined as the force applied per unit area on an object or body surface. It is often measured in millimeters of mercury (mmHg) in clinical settings. For example, blood pressure is the force exerted by circulating blood on the walls of the arteries and is recorded as two numbers: systolic pressure (when the heart beats and pushes blood out) and diastolic pressure (when the heart rests between beats).
Pressure can also refer to the pressure exerted on a wound or incision to help control bleeding, or the pressure inside the skull or spinal canal. High or low pressure in different body systems can indicate various medical conditions and require appropriate treatment.
An artificial urinary sphincter (AUS) is not a living tissue but a surgically implanted medical device used to help manage urinary incontinence, particularly for individuals with stress incontinence or overflow incontinence. The device consists of three main components: a cuff that encircles the urethra, a balloon regulator placed in the abdomen, and a control pump located in the scrotum (in men) or labia (in women).
The cuff is inflated with fluid, which constricts the urethra and prevents urine leakage. When the individual wants to urinate, they manually compress the control pump, which transfers the fluid from the cuff to the balloon regulator, allowing the urethra to open and enabling urination. After a short period, the fluid automatically flows back from the balloon to the cuff, re-establishing continence.
It is essential to note that an artificial urinary sphincter is not a native or biological tissue but a prosthetic device designed to mimic the function of the natural urinary sphincter.
The urethra is the tube that carries urine from the bladder out of the body. In males, it also serves as the conduit for semen during ejaculation. The male urethra is longer than the female urethra and is divided into sections: the prostatic, membranous, and spongy (or penile) urethra. The female urethra extends from the bladder to the external urethral orifice, which is located just above the vaginal opening.
Prospective studies, also known as longitudinal studies, are a type of cohort study in which data is collected forward in time, following a group of individuals who share a common characteristic or exposure over a period of time. The researchers clearly define the study population and exposure of interest at the beginning of the study and follow up with the participants to determine the outcomes that develop over time. This type of study design allows for the investigation of causal relationships between exposures and outcomes, as well as the identification of risk factors and the estimation of disease incidence rates. Prospective studies are particularly useful in epidemiology and medical research when studying diseases with long latency periods or rare outcomes.
I'm sorry for any confusion, but "opossums" are not a medical term or a medical condition. Opossums are actually marsupials (pouched mammals) that are native to the Americas. They are often known for their "playing dead" behavior as a defense mechanism when threatened. If you have any questions about medical terminology or health-related topics, I'd be happy to help with those!
Erectile dysfunction (ED) is the inability to achieve or maintain an erection sufficient for satisfactory sexual performance. It can have physical and psychological causes, such as underlying health conditions like diabetes, heart disease, obesity, and mental health issues like stress, anxiety, and depression. ED can also be a side effect of certain medications. Treatment options include lifestyle changes, medication, counseling, and in some cases, surgery.
Left ventricular dysfunction (LVD) is a condition characterized by the impaired ability of the left ventricle of the heart to pump blood efficiently during contraction. The left ventricle is one of the four chambers of the heart and is responsible for pumping oxygenated blood to the rest of the body.
LVD can be caused by various underlying conditions, such as coronary artery disease, cardiomyopathy, valvular heart disease, or hypertension. These conditions can lead to structural changes in the left ventricle, including remodeling, hypertrophy, and dilation, which ultimately impair its contractile function.
The severity of LVD is often assessed by measuring the ejection fraction (EF), which is the percentage of blood that is pumped out of the left ventricle during each contraction. A normal EF ranges from 55% to 70%, while an EF below 40% is indicative of LVD.
LVD can lead to various symptoms, such as shortness of breath, fatigue, fluid retention, and decreased exercise tolerance. It can also increase the risk of complications, such as heart failure, arrhythmias, and cardiac arrest. Treatment for LVD typically involves managing the underlying cause, along with medications to improve contractility, reduce fluid buildup, and control heart rate. In severe cases, devices such as implantable cardioverter-defibrillators (ICDs) or left ventricular assist devices (LVADs) may be required.
 Sphincter of Oddi dysfunction
Sphincter of Oddi dysfunction
Nardi test
Biliary endoscopic sphincterotomy
Jay Pasricha
Peripherally acting μ-opioid receptor antagonist
Peter B. Cotton
Endoscopic retrograde cholangiopancreatography
Sphincter of Oddi
Papillary stenosis
Postcholecystectomy syndrome
List of MeSH codes (C06)
Victor Rădulescu-Pogoneanu
Roemheld syndrome
Biliary colic
Sod (disambiguation)
Rome process
Functional gastrointestinal disorder
Human digestive system
ICD-9-CM Volume 3
Acute pancreatitis
Sphincter of Oddi dysfunction - Wikipedia
 Sphincter of Oddi Dysfunction - IFFGD
Sphincter of Oddi Dysfunction - IFFGD
Diarrhea Archives - IFFGD
 Гастрошколы. Clinical features and management of painless biliary type sphincter of Oddi dysfunction
Гастрошколы. Clinical features and management of painless biliary type sphincter of Oddi dysfunction
![Gasmi M[au] - Search Results - PubMed](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAARVBMVEVHcEwoU45gYmYAUpQAUpRPYGVgYmZLXnJgYmYAUZUAUpRJXnIAUpQAUpRgYmYAUpRgYmZgYmZhYmYAUpQAUpQAUpRgYmaDiPJuAAAAFXRSTlMADOJ+6QewGO8/uTRqtH7GdFJ11p1bCL3TAAAAZUlEQVQYlV2PVw7AIAxDTeney7n/UcsoldX3E+VJOAboEi7MBpHWMs1ADlG8u7UYWauwyZFeRQVPOhG2o+aiwhByJxUx91Jxhje3iJSqGfHuLKI0+0TpXvY1twCOPlFh5pa/++MB0vIOBm+1zaoAAAAASUVORK5CYII=) Gasmi M[au] - Search Results - PubMed
Gasmi M[au] - Search Results - PubMed
The Nardi test in sphincter of Oddi dysfunction: Is it still relevant? - Fingerprint - Manipal Academy of Higher Education...
 Will Ashwagandha Make My Dick Bigger, Penis Growth At 30 | Able UK
Will Ashwagandha Make My Dick Bigger, Penis Growth At 30 | Able UK
 Endoscopic retrograde cholangiopancreatography-related early perforations: A study of effects of procedure duration, complexity...
Endoscopic retrograde cholangiopancreatography-related early perforations: A study of effects of procedure duration, complexity...
 Biliary Tract Disorders, Gallbladder Disorders, & Gallstone Pancreatitis | ACG
Biliary Tract Disorders, Gallbladder Disorders, & Gallstone Pancreatitis | ACG
 Bile Duct Strictures: Background, Pathophysiology, Etiology
Bile Duct Strictures: Background, Pathophysiology, Etiology
 What is the treatment for uncontrolled recurrent RUQ pain?
What is the treatment for uncontrolled recurrent RUQ pain?
 A Healthy Eating Balanced Diet is Not Only Physically Beneficial - Zebra Nole Magicien
A Healthy Eating Balanced Diet is Not Only Physically Beneficial - Zebra Nole Magicien
Viberzi) eluxadoline dosing, indications, interactions, adverse effects, and more
 Andrew Seibert, MD
Andrew Seibert, MD
 Eluxadoline: MedlinePlus Drug Information
Eluxadoline: MedlinePlus Drug Information
 Postcholecystectomy Syndrome - Hepatic and Biliary Disorders - MSD Manual Professional Edition
Postcholecystectomy Syndrome - Hepatic and Biliary Disorders - MSD Manual Professional Edition
 Priya A. Jamidar, MD Gastroenterology | Yale New Haven Hospital
Priya A. Jamidar, MD Gastroenterology | Yale New Haven Hospital
 What Happens to Food When the Gallbladder Stops Working? | Healthfully
What Happens to Food When the Gallbladder Stops Working? | Healthfully
 Interventional Endoscopy Research - Digestive Diseases Research | UCLA Health
Interventional Endoscopy Research - Digestive Diseases Research | UCLA Health
 Gallstone Symptoms,Treatments, and Causes in San Antonio
Gallstone Symptoms,Treatments, and Causes in San Antonio
 October 2021 - Salon Marocain Decoration
October 2021 - Salon Marocain Decoration
Texas Viberzi® Lawyer | TX Pancreatitis Lawsuit
 September 2019 - Danieletdenise-stjean
September 2019 - Danieletdenise-stjean
KoreaMed Synapse
 Elevated liver enzymes after gallbladder removal | Mayo Clinic Connect
Elevated liver enzymes after gallbladder removal | Mayo Clinic Connect
 Volume 13(11) 2007 (20)
Volume 13(11) 2007 (20)
Travelers' diarrhea - Wikipedia
Budd-Chiari syndrome - Wikipedia
![MCQ] Acute and Chronic Pancreatitis- Part 2 - MedQuizzes](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAAn1BMVEX////yAADzExP4jIzzISH/+fn6ra32ZWX0Ozv2YGD4g4P3dnbzDw/zCgr6oaFiUgD7vr78xcX5p6f0Gxv5l5f6tLT0kYucm26PjVbvo5r+8vL3fX37ublrQgDCv6HT0LpeQwD3qqT+5uaLg0Tb2MeYkVy3uJuqpILHw6+poWrk4tSakU+zrH3+39/Mz7j2bW1tUQBsXQCBdjW8MwDQIQAQc8AHAAAAtklEQVQYlTVP5xqCQAxLDgQO2YoTPRXce7z/s9kDzY82zZcuQNDz/CDQxQw/eCTVQMKwq0Oqvs1ORN/mkm6cWFLRbT2MyNE4TSdTCp0h47wqF0vArNaVw0ImbHCrGxG2O7FraAL7w9Gczk0NuAH8VmiO5mJEGARweMVtYszp0rb4yHkvEhm6rx+jpE8PiFRs1z7Hr3es2INYfodlH9cagITqfgU284hh90yu2KH8v4vc0TrMWvoFIaIMJB1sQXYAAAAASUVORK5CYII=) MCQ] Acute and Chronic Pancreatitis- Part 2 - MedQuizzes
MCQ] Acute and Chronic Pancreatitis- Part 2 - MedQuizzes
Spasm3
- Sphincter of Oddi dysfunction (SOD) is not completely understood but it is thought the sphincter goes into spasm causing the back up of pancreatic and bile juices and in turn causes abdominal pain. (thegiconsultants.com)
- Traditional teaching dictates that morphine induces "spasm" in the sphincter of Oddi (SO) and should not be used in acute pancreatitis and that meperidine is the analgesic of choice because it does not elevate SO pressures. (nih.gov)
- Other opioid-induced effects may include a reduction in biliary and pancreatic secretions, spasm of sphincter of Oddi, and transient elevations in serum amylase. (clustermed.info)
Stenosis5
- Both stenosis and dyskinesia can obstruct flow through the sphincter of Oddi and can therefore cause retention of bile in the biliary tree and pancreatic juice in the pancreatic duct. (wikipedia.org)
- Two mechanisms are involved in the development of sphincter of Oddi dysfunction, either or both of which may be contributory to the condition: stenosis, or narrowing of the sphincter of Oddi (also termed papillary stenosis), and dyskinesia, or alteration in the function of the sphincter of Oddi (also termed biliary dyskinesia). (wikipedia.org)
- Papillary stenosis and biliary dyskinesia are 2 conditions affecting the sphincter. (thegiconsultants.com)
- Papillary stenosis, which is rare, is fibrotic narrowing around the sphincter, perhaps caused by trauma and inflammation due to pancreatitis, instrumentation (eg, endoscopic retrograde cholangiopancreatography), or prior passage of a stone. (msdmanuals.com)
- it may be due to stenosis at the ampulla, or it could be caused by sphincter of oddi hypertension (either due to hypertrophy, or increased smooth muscle response to stimuli) 2 . (sjrhem.ca)
Pancreatitis16
- Some have suggested avoiding manometry because of the risks, but several studies have shown that the likelihood of ERCP provoking pancreatitis is determined by the characteristics of the patient with "suspected SOD," and that sphincter manometry does not add to the risk. (medscape.com)
- Sphincter of Oddi dysfunction (SOD) is a functional gastrointestinal abnormality which commonly causes acute pancreatitis. (beatingpancreatitis.com)
- Even without the unfortunate occurrence of acute pancreatitis Sphincter of Oddi dysfunction is characterized by pancreatobiliary pain that can be debilitating and impair the patients quality of life. (beatingpancreatitis.com)
- 1. Sphincter of Oddi (pancreatic) hypertension and recurrent pancreatitis. (nih.gov)
- 3. Incidence and predictors of post-ERCP pancreatitis in patients with suspected sphincter of Oddi dysfunction undergoing biliary or dual sphincterotomy: results from the EPISOD prospective multicenter randomized sham-controlled study. (nih.gov)
- 5. [Sphincter of Oddi disfunction in "idiopathic" recurrent pancreatitis]. (nih.gov)
- 6. Pancreatic stenting prevents pancreatitis after biliary sphincterotomy in patients with sphincter of Oddi dysfunction. (nih.gov)
- 7. Sphincter of Oddi dysfunction: pancreaticobiliary sphincterotomy with pancreatic stent placement has a lower rate of pancreatitis than biliary sphincterotomy alone. (nih.gov)
- 11. ERCP, biliary crystal analysis, and sphincter of Oddi manometry in idiopathic recurrent pancreatitis. (nih.gov)
- 15. Secretin MRCP and endoscopic pancreatic manometry in the evaluation of sphincter of Oddi function: a comparative pilot study in patients with idiopathic recurrent pancreatitis. (nih.gov)
- 16. Evaluation of unexplained acute and acute recurrent pancreatitis using endoscopic retrograde cholangiopancreatography, sphincter of Oddi manometry and endoscopic ultrasound. (nih.gov)
- 17. Incidence of pancreatitis in patients undergoing sphincter of Oddi manometry (SOM). (nih.gov)
- 20. [Double sphincterostomy of pancreatic and choledochal sphincters in the treatment of chronic recurrent pancreatitis]. (nih.gov)
- The spectrum of conditions includes those due to cancer of the exocrine and endocrine pancreas, gallstones, sludge, pancreatic and biliary malignancy, trauma, anatomic problems (pancreas divisum), alcohol and drugs and idiopathic syndromes such as idiopathic pancreatitis and sphincter of Oddi dysfunction. (nih.gov)
- They did an recap and found no abnormalities they suspect sphincter of odi I recently happened again 3 months later and this time I had diarrhea I was nauseous lightheaded when the pain came on it was so severe bile duct is now dilated 14 mm not sure what to do they say maybe Ecco but that I could get pancreatitis. (dssurgery.com)
- Because Mr. X had pain that resembled biliary colic very closely, yet multiple previous imaging studies and lab studies showed no signs of acute cholecystitis, cholelithiasis, pancreatitis, or liver disease, it was thought that perhaps sphincter dysfunction could be the root cause of the problem. (sjrhem.ca)
Pancreatic sphincter4
- Sphincter of Oddi dysfunction refers to a group of functional disorders leading to abdominal pain due to dysfunction of the Sphincter of Oddi: functional biliary sphincter of Oddi and functional pancreatic sphincter of Oddi disorder. (wikipedia.org)
- and, functional pancreatic sphincter of Oddi disorder, where pancreatic enzyme measurements are elevated. (wikipedia.org)
- The criteria outline three variants of functional disorders of the gallbladder, bile duct and pancreas, termed functional gallbladder disorder, functional biliary sphincter of Oddi disorder and functional pancreatic sphincter of Oddi disorder. (wikipedia.org)
- 2. Hypertensive pancreatic sphincter. (nih.gov)
Manometry6
- The NIH conference recommended that testing should always include sphincter manometry. (medscape.com)
- Sphincter manometry is widely thought to be the "gold standard" for the diagnosis of SOD, but the evidence is very thin. (medscape.com)
- 8. Suspected sphincter of Oddi dysfunction type II: empirical biliary sphincterotomy or manometry-guided therapy? (nih.gov)
- 9. Frequency of abnormal pancreatic and biliary sphincter manometry compared with clinical suspicion of sphincter of Oddi dysfunction. (nih.gov)
- 12. Long-term outcome of endoscopic dual pancreatobiliary sphincterotomy in patients with manometry-documented sphincter of Oddi dysfunction and normal pancreatogram. (nih.gov)
- Later studies using endoscopic retrograde cholangiopancreatography with direct SO manometry demonstrated that the SO is exquisitely sensitive to all narcotics including meperidine and that a small increase in biliary sphincter pressure is seen with higher doses of morphine. (nih.gov)
Functional5
- If all of the above criteria are met, individuals are classified as having a functional biliary sphincter of Oddi disorder, if the testing of pancreatic enzymes (amylase and lipase) is normal. (wikipedia.org)
- However, more often can be functional, temporal spasms of the sphincter of Oddi without any abnormality in the tests. (dp.ua)
- sphincter of Oddi d. structural or functional abnormality of the sphincter of Oddi that interferes with bile or pancreatic duct drainage. (theodora.com)
- In about 10% of patients, biliary colic appears to result from functional or structural abnormalities of the sphincter of Oddi, resulting in altered biliary pressures or heightened sensitivity. (msdmanuals.com)
- Organic or functional motility disorder involving the SPHINCTER OF ODDI and associated with biliary COLIC . (nih.gov)
Lipase1
- elevated amylase and lipase suggest dysfunction of the sphincter's pancreatic portion. (msdmanuals.com)
Gallbladder and pancreas problems2
- The Sphincter of Oddi is a central gate to many liver, gallbladder and pancreas problems. (dp.ua)
- The online cialis prescriptions sphincter of Oddi dysfunction causes liver, gallbladder and pancreas problems. (longandshortreviews.com)
Cholecystectomy4
- The diagnosis of sphincter of Oddi dysfunction (SOD) is often considered in patients with recurrent pains after cholecystectomy. (medscape.com)
- 19. [Dysfunction of the sphincter of Oddi in cholecystectomy patients]. (nih.gov)
- Prior cholecystectomy was a requirement for inclusion and patients with primary CBD stones in the setting of an intact sphincter were excluded. (biomedcentral.com)
- Patients who presented with primary CBDS at least 6 months' post cholecystectomy with an intact sphincter were excluded from the analysis. (biomedcentral.com)
Bile11
- The sphincter of Oddi is a sphincter muscle, a circular band of muscle at the bottom of the biliary tree which controls the flow of pancreatic juices and bile into the second part of the duodenum. (wikipedia.org)
- Attempts have been made to demonstrate sphincter abnormalities with noninvasive tests, such as morphine-prostigmin provocation tests, dynamic isotope studies, and changes in bile duct diameter on scans after stimulation with fatty meals or cholecystokinin. (medscape.com)
- The sphincter of Oddi is a muscular valve that surrounds the exit of the bile duct and pancreatic duct. (thegiconsultants.com)
- The sphincter is usually closed but opens to allow drainage of bile and pancreatic juices to flow to aid in digestion of food. (thegiconsultants.com)
- Sphincter of Oddi dysfunction is a condition in which the muscle between the bile duct and pancreatic duct does not open like it should. (gastrohealthpartners.com)
- The sphincter of Oddi is a smooth muscle that surrounds the end of the common bile duct and the pancreatic duct. (gastrohealthpartners.com)
- Around the common bile duct, pancreatic duct and the duodenum wall there is a muscle valve called the Sphincter of Oddi. (dp.ua)
- The Sphincter of Oddi controls moving of the bile from the liver, and gallbladder and pancreatic juice from the pancreas into the duodenum. (dp.ua)
- When no food in the duodenum, sphincter of Oddi is closed so the bile from the liver is collected in the gallbladder. (dp.ua)
- The common reason for sphincter to be spasmodic is irritation of it by the "aggressive" bile and pancreatic juice. (dp.ua)
- Pathological changes are most often seen in the COMMON BILE DUCT sphincter, and less commonly the PANCREATIC DUCT sphincter. (nih.gov)
Abnormalities1
- The Sphincter of Oddi Dysfunction Awareness and Education Network, Inc. - The Sphincter of Oddi Dysfunction Awareness and Education Network - Sphincter of Oddi Dysfunction can cause abdominal and back pain, pancreas and liver abnormalities, nausea, vomiting, weight loss, and bowel issues. (solarisdentistryandmedical.com)
Liver2
- Sphincter of Oddi dysfunction may be suggested by pain which seems to come from a biliary origin, which may or may not be associated with transient increases of liver or pancreatic enzymes. (wikipedia.org)
- Laboratory Tests of the Liver and Gallbladder Laboratory tests are generally effective for the following: Detecting hepatic dysfunction Assessing the severity of liver injury Monitoring the course of liver diseases and the response to treatment. (msdmanuals.com)
Diagnosis2
- Sphincter of Oddi Dysfunction (SOD) is considered when the patient has severe attacks of abdominal pain persisting or recurring after gallbladder surgery and when all work up has failed to find an alternate diagnosis for the pain. (thegiconsultants.com)
- Sphincter of Oddi dysfunction (SOD) is within the differential diagnosis for patients who present with recurrent biliary pain, with no apparent source 1 . (sjrhem.ca)
Abdominal pain1
- Individuals with sphincter of Oddi dysfunction present with abdominal pain resembling that of structural or inflammatory disorders of the gallbladder, biliary tree or pancreas. (wikipedia.org)
Duodenum2
- Normally, when semi digestive food moves from the stomach into the duodenum sphincter of Oddi opens. (dp.ua)
- This opening is surrounded by the sphincter of Oddi, which helps to control the rate at which the pancreas and gallbladder elicit secretions into the duodenum ( 1 ). (drjockers.com)
Pancreas1
- Many scientists believe that the Sphincter of Oddi Dysfunction (SOD) is a culprit of the pancreas diseases and it is the common source of chronic pain after gallbladder removal. (dp.ua)
Morphine1
- The paper describes a case report of a patient with a significant history of opioid-induced dysfunction of the sphincter of Oddi, who required morphine sulfate to manage oral mucositis pain, and who was successfully treated with concomitant oral naloxegol (Moventig: Kyowa Kirin, Galashiels, UK). (nih.gov)
Disorders1
- Gallbladder and Sphincter of Oddi Disorders. (sjrhem.ca)
SignUp1
- http://www.sodae.org/email-signup.html SOD Awareness and Education Network Email Signup - The Sphincter of Oddi Dysfunction Awareness and Education Network, Inc. - Get up-to-date information on SOD by signing up for our email listserve. (solarisdentistryandmedical.com)
Doctors1
- Doctors diagnose sphincter of Oddi dysfunction in a few different ways. (gastrohealthpartners.com)
Disease1
- Gastroesophageal Reflux Disease (GERD) Incompetence of the lower esophageal sphincter allows reflux of gastric contents into the esophagus, causing burning pain. (msdmanuals.com)
Infertility1
- Chronic use of opioids may influence the hypothalamic-pituitary-gonadal axis, leading to androgen deficiency that may manifest as low libido, impotence, erectile dysfunction, amenorrhea, or infertility. (clustermed.info)
Patients1
- has years of experience treating patients with conditions like sphincter of Oddi dysfunction. (gastrohealthpartners.com)
Chronic1
- Sphincter of Oddi dysfunction: Managing the patient with chronic biliary pain [Internet]. (sjrhem.ca)
Commonly1
- The Roux-en-Y gastric bypass (RYGB) is one of the most commonly performed surgical procedures today in the United States. (basicmedicalkey.com)
Procedure1
- Urodynamic testing is any procedure that looks at how well the bladder, sphincters, and urethra are storing and releasing urine. (gourmandisesdecamille.com)
Pressure2
Articles1
- http://www.sodae.org/resources.html Sphincter of Oddi Dysfunction Support Information - The Sphincter of Oddi Dysfunction Awareness and Education Network, Inc. - This page is dedicated to Sphincter of Oddi Dysfunction resources, articles, stories, links, survey results, and anything else that may help an SOD patient. (solarisdentistryandmedical.com)
Condition1
- The old Milwaukee classification of biliary sphincter of Oddi dysfunction (SOD) used to divide the condition into three subtypes: but it is no longer in use. (wikipedia.org)