Syringomyelia
Arnold-Chiari Malformation
Arachnoiditis
Platybasia
Decompressive Craniectomy
Cerebrospinal Fluid Pressure
Encephalocele
Arachnoid Cysts
Fourth Ventricle
Myelography
Subarachnoid Space
Cranial Fossa, Posterior
Decompression, Surgical
Magnetic Resonance Imaging
Laminectomy
Arachnoid
Scoliosis
Cerebrospinal Fluid
Hydrocephalus
Spinal Cord
Arthropathy, Neurogenic
Dura Mater
Reflex, Abdominal
Cerebrospinal Fluid Shunts
Cerebellar Diseases
Spinal Cord Neoplasms
Hypohidrosis
Spinal Cord Injuries
Encyclopedias as Topic
Anterior Spinal Artery Syndrome
Focal (segmental) dyshidrosis in syringomyelia. (1/233)
The features or mechanisms of dyshidrosis have not been sufficiently clarified. Neither has the difference between hyperhidrosis and hypohidrosis. To clarify the features and mechanisms of dyshidrosis (hyperhidrosis and hypohidrosis) in syringomyelia, the clinical features focusing on hidrosis of 30 patients with syringomyelia and Chiari malformation located from a syringomyelia database were prospectively analysed. The patients were classified into three groups: eight patients (26.7%) had segmental hypohidrosis, 10 (33. 3%) had segmental hyperhidrosis, and 12 (40.0%) had normohidrosis. We found that the Karnofsky functional status for the hyperhydrosis and normohidrosis groups were significantly higher than for the hypohidrosis group (p=0.0012), with no significant differences between the hyperhidrosis and normohidrosis groups. The duration from the onset of syringomyelia to the current dyshidrosis was significantly longer in the hypohidrosis group than in the hyperhidrosis group (p=0.0027). A significant correlation was identified between the duration from the onset of syringomyelia to the time at study and the performance score (r=-0.599, p=0.0003). The results substantiate previous hypotheses that in its early stage syringomyelia causes segmental hyperactivity of the sympathetic preganglionic neurons, and hyperactivity of these gradually subsides as tissue damage progresses. Focal hyperhidrosis may be regarded as a hallmark of a relatively intact spinal cord, as well as normohidrosis. (+info)Arnold-Chiari malformation with syringomyelia in an elderly woman. (2/233)
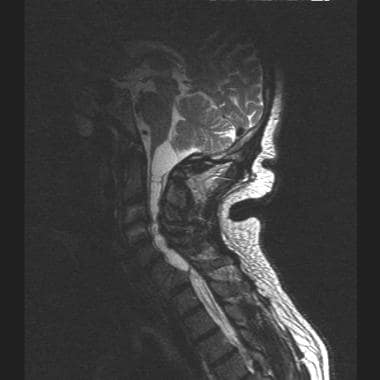
PRESENTATION: A 76-year-old woman, complaining of leg pain and unsteady gait for 3 years, presented with a spastic paraparetic gait, severe spasticity and touch, thermal and pain sensory loss limited to arms, lower thorax and upper abdomen. Brain and spinal cord magnetic resonance imaging showed a large loculated syrinx. Cerebellar tonsillar herniation into the foramen magnum was also seen (Arnold-Chiari malformation, type I). OUTCOME: The patient had successful cervico-spinal surgical decompression which resulted in marked reduction in hypertonia and weakness, normal gait and normal joint movement at 6 months. CONCLUSION: This unusual, late clinical presentation of a congenital disease underlines the importance of a comprehensive diagnostic work-up in the elderly patients with complex neurological signs. (+info)Spinal sonography and magnetic resonance imaging in patients with repaired myelomeningocele: comparison of modalities. (3/233)
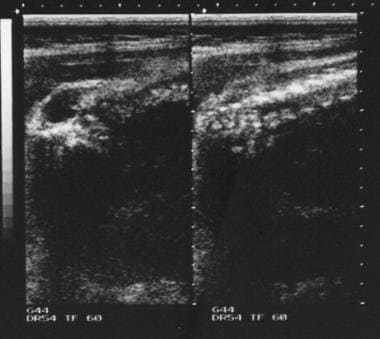
The goals of this study were to evaluate the feasibility of using ultrasonography of the spine in the follow-up evaluation of patients with repaired myelomeningocele at birth and to compare sonography with the accepted modality of magnetic resonance imaging. Over a period of 4 years we performed 165 sonographic studies in 101 patients; 107 sonographic studies had MR imaging results for comparison. We collected our data prospectively. The quality of the sonograms was good in 110 of 129 studies, acceptable in 17 of 129, and poor in two of 129. The sonographic examinations failed in 33 of 165 studies (20%). Concordant information was obtained between ultrasonography and magnetic resonance imaging in the following percentage of studies: level of the distal end of the cord in 82%, position of the cord in the canal in 59%, presence of hydromyelia in 63%, cord duplication in 96%, adhesions in 16%, intradural mass in 37%, cord measurements in 85%, and dural sac measurements in 83%. At the lumbosacral level, we saw no cord pulsation in 57% of the studies in patients with cord adhesions and in 20% of those without adhesions. At the lower thoracic level, we saw no pulsation in 35% of the studies in patients with cord adhesions and in 7% of those without adhesions. Postoperative studies of cord release surgery in eight patients showed varied findings. We conclude that in those patients who have a spinal defect or interlaminar space allowing proper visualization of the lumbosacral spinal canal, ultrasound can provide fairly similar information to that obtained with magnetic resonance imaging of that area with no need for sedation and at a reduced cost. Ultrasonography seems more sensitive than magnetic resonance imaging in the detection of cord adhesions, which is particularly relevant in the diagnosis of tethering. (+info)Diffusion-weighted MR imaging in a rat model of syringomyelia after excitotoxic spinal cord injury. (4/233)
BACKGROUND AND PURPOSE: Recent experimental data have shown that an increase of excitatory amino acids and the initiation of inflammatory responses within the injured spinal cord may play a role in post-traumatic syringomyelia. The purpose of this study was to determine whether diffusion-weighted MR imaging with apparent diffusion coefficient (ADC) maps could provide earlier evidence of spinal cord cavitation in a rat model of syringomyelia than available with conventional MR imaging. METHODS: The spinal cord gray matter of four rats was injected with the alpha-amino-3 hydroxy-5 methyl-4 isoxazole propionic acid/metabotropic receptor agonist quisqualic acid. Animals were sacrificed at 1, 4, or 8 weeks after injection, and the spinal cords were fixed in formalin for 1 week and imaged with T1-, T2-, and diffusion-weighted sequences. One control specimen was also imaged. ADC maps were constructed from the diffusion-weighted data. Histopathologic analyses of sections stained with cresyl violet were compared with the MR images. RESULTS: By 1 week after injection, ADC maps at the level of injection showed areas within the gray matter of increased intensity and increased ADC values as compared with the control specimen. These bright areas corresponded to cysts or cavities within the cord parenchyma on the histopathologic sections. The ADC values within affected gray matter areas progressively increased at 4 and 8 weeks, also corresponding to cyst formation. Conventional T1- and T2-weighted images showed corresponding lesions with cystic characteristics at 4 and 8 weeks, but not at 1 week. CONCLUSION: In an animal model of syringomyelia, diffusion-weighted imaging with ADC maps detected cystic lesions within spinal cord gray matter before they were seen on conventional T1- and T2-weighted images. (+info)Effect of cerebrospinal fluid shunting on experimental syringomyelia: magnetic resonance imaging and histological findings. (5/233)
The histological changes associated with syringomyelia after reduction of the syrinx size were investigated after cerebrospinal fluid shunting in experimental syringomyelia in the rabbit. Five weeks after syringomyelia was induced by the injection of kaolin into the cisterna magna in Japanese white rabbits, ventriculosubgaleal shunting or syringoepidural shunting were performed. After 1 week magnetic resonance (MR) imaging and histological examination were then carried out. Five of 11 shunted animals showed postoperative reduction of syrinx size on MR imaging. Grossly, some specimens showed cavity collapse and parenchymal healing, and others showed a small residual syrinx in the dorsal horn. The most dramatic histological changes occurred in the gray matter. Specimens with syrinx collapse showed rarefaction and tearing of the gray matter, with mild glial reaction. The edematous gray matter showed both degeneration and regeneration, with neuronal processes surrounded by edema fluid. Reactive astrocytes were observed mainly at the margin of the residual syrinx. Some astrocytic processes invested the extraaxonal space and gray matter lacked supportive tissue. Greater reduction of the syrinx after shunting operation was correlated with more regeneration and less degeneration, and the white matter was edematous and histological changes were milder. Syrinx shrinkage occurred after shunting in this experimental model of syringomyelia. The selective vulnerability of gray matter even after shunting may explain discrepancies between imaging findings and clinical features in this disease. The study supports the potential benefit from early treatment, considering the associated morphological findings of regeneration. (+info)Spinal dysraphism in a newborn Holstein-Friesian calf. (6/233)
Spinal dysraphism, not associated with vertebral defect or arthrogryposis, was found in a 3-day-old Holstein-Friesian calf that was clinically diagnosed as having encephalopathy. The dysraphic lesion occurred in the sixth (C6) and seventh (C7) segments of the cervical spinal cord. Microscopically, the lesion was characterized by hydromyelia, syringomyelia, anomaly of the ventral median fissure, abnormal running of the myelinated nerve fibers in the white column, and absence of the central canal due to a developmental defect of the ependymal cells. (+info)Retrocerebellar arachnoid cyst with syringomyelia: a case report. (7/233)
Association of syringomyelia with retrocerebellar arachnoid cysts is rare. A case of 14 year old female is being reported, who presented with hydrocephalus caused by a large midline retrocerebellar infravermal arachnoid cyst leading to obstruction of the outlet foramina of the fourth ventricle. There was associated syringomyelia. The pathogenesis of syringomyelia is discussed. The need to evaluate cervical spinal cord by taking T1 weighted sagittal sections in all the patients of large posterior fossa mass lesions causing obstruction to the outlet foramina of the fourth ventricle has been stressed, in order to detect associated syringomyelia. (+info)Chiari malformation and syringomyelia in monozygotic twins: birth injury as a possible cause of syringomyelia--case report. (8/233)
A 26-year-old female, the elder of monozygotic twins, presented with slow progressive numbness and pain in her left arm. Magnetic resonance (MR) imaging showed syringomyelia with Chiari malformation. The patient's birth had been difficult with prolonged delivery time, breech delivery, and neonatal asphyxia. MR imaging of the patient's twin sister showed mild tonsillar ectopia, but absence of syringomyelia. This younger sister was born without problems. The patient underwent syringosubarachnoid shunt at the C5-6 level. The syrinx was collapsed promptly, and her symptoms disappeared. This case of syringomyelia with Chiari malformation in one of twins suggests that birth injury is likely to be a cause of the pathogenesis of syringomyelia. (+info)Syringomyelia is a medical condition characterized by the formation of a fluid-filled cavity or cavities (syrinx) within the spinal cord. This syrinx can lead to various symptoms depending on its size and location, which may include pain, muscle weakness, numbness, and stiffness in the neck, back, shoulders, arms, or legs. In some cases, it may also affect bladder and bowel function, sexual performance, and the ability to maintain normal body temperature. Syringomyelia is often associated with Chiari malformation, a condition where the lower part of the brain extends into the spinal canal. However, other conditions such as spinal cord injuries, tumors, or infections may also cause syringomyelia.
Arnold-Chiari malformation is a structural abnormality of the brain and skull base, specifically the cerebellum and brainstem. It is characterized by the descent of the cerebellar tonsils and sometimes parts of the brainstem through the foramen magnum (the opening at the base of the skull) into the upper spinal canal. This can cause pressure on the brainstem and cerebellum, potentially leading to a range of symptoms such as headaches, neck pain, unsteady gait, swallowing difficulties, hearing or balance problems, and in severe cases, neurological deficits. There are four types of Arnold-Chiari malformations, with type I being the most common and least severe form. Types II, III, and IV are progressively more severe and involve varying degrees of hindbrain herniation and associated neural tissue damage. Surgical intervention is often required to alleviate symptoms and prevent further neurological deterioration.
Arachnoiditis is a medical condition that affects the arachnoid, one of the membranes that surround and protect the nerves of the central nervous system (the brain and spinal cord). The arachnoid becomes inflamed, often as a result of infection, direct injury, or complications from spinal surgery or chronic exposure to irritants such as steroids or contrast dyes.
The inflammation can cause the formation of scar tissue, which can lead to a variety of symptoms including:
1. Chronic pain in the back, legs, or arms
2. Numbness, tingling, or weakness in the limbs
3. Muscle cramps and spasms
4. Bladder and bowel dysfunction
5. Sexual dysfunction
In severe cases, arachnoiditis can cause permanent nerve damage and disability. Treatment typically focuses on managing symptoms and improving quality of life, as there is no cure for the condition.
Platybasia is a medical term that refers to a condition where the base of the skull is flattened or broadened, resulting in an abnormal increase in the angle between the clivus (a part of the sphenoid bone) and the posterior aspect of the upper surface of the palatine bone. This condition can be congenital or acquired and is often associated with other skeletal abnormalities. In some cases, platybasia may lead to neurological symptoms such as headaches, neck pain, or even brainstem compression.
The foramen magnum is the largest opening in the human skull, located at the base of the skull, through which the spinal cord connects to the brain. It is a crucial structure for the transmission of nerve impulses between the brain and the rest of the body. The foramen magnum also provides passage for blood vessels that supply the brainstem and upper spinal cord.
A decompressive craniectomy is a neurosurgical procedure in which a portion of the skull is removed to allow the swollen brain to expand and reduce intracranial pressure. This surgical intervention is typically performed as a last resort in cases where other treatments for increased intracranial pressure, such as hyperosmolar therapy or drainage of cerebrospinal fluid, have been unsuccessful.
During the procedure, the surgeon creates an opening in the skull (craniectomy) and removes a piece of bone (bone flap). This exposes the brain and creates additional space for it to expand without being compressed by the rigid skull. The dura mater, the outermost protective layer surrounding the brain, may also be opened to provide further room for brain swelling.
Once the swelling has subsided, a second procedure known as cranioplasty is performed to replace the removed bone flap or use an artificial implant to restore the skull's integrity and protect the underlying brain tissue. The timing of cranioplasty can vary depending on individual patient factors and clinical conditions.
Decompressive craniectomy is most commonly used in the management of traumatic brain injuries, stroke-induced malignant cerebral edema, and intracranial hypertension due to various causes, such as infection or inflammation. While this procedure can be lifesaving in some cases, it may also lead to complications like seizures, hydrocephalus, or neurological deficits. Therefore, the decision to perform a decompressive craniectomy should be made carefully and on an individual basis, considering both the potential benefits and risks.
Cerebrospinal Fluid Pressure (CSFP) is the pressure exerted by the cerebrospinal fluid (CSF), a clear, colorless fluid that surrounds and protects the brain and spinal cord. CSF acts as a cushion for the brain, allowing it to float within the skull and protecting it from trauma.
The normal range of CSFP is typically between 6 and 18 cm of water (cm H2O) when measured in the lateral decubitus position (lying on one's side). Elevated CSFP can be a sign of various medical conditions, such as hydrocephalus, meningitis, or brain tumors. Conversely, low CSFP may indicate dehydration or other underlying health issues.
It is important to monitor and maintain normal CSFP levels, as abnormal pressure can lead to serious neurological complications, including damage to the optic nerve, cognitive impairment, and even death in severe cases. Regular monitoring of CSFP may be necessary for individuals with conditions that affect CSF production or absorption.
An Encephalocele is a type of neural tube defect that occurs when the bones of the skull do not close completely during fetal development. This results in a sac-like protrusion of the brain and the membranes that cover it through an opening in the skull. The sac may be visible on the scalp, forehead, or back of the head, and can vary in size. Encephaloceles can cause a range of symptoms, including developmental delays, intellectual disabilities, vision problems, and seizures, depending on the severity and location of the defect. Treatment typically involves surgical repair of the encephalocele soon after birth to prevent further damage to the brain and improve outcomes.
An Arachnoid cyst is a type of abnormal fluid-filled sac that develops between the brain or spinal cord and the arachnoid membrane, which is one of the three layers that cover and protect the central nervous system. These cysts are filled with cerebrospinal fluid (CSF), which is the same fluid that surrounds and cushions the brain and spinal cord.
Arachnoid cysts can vary in size and may be present at birth or develop later in life due to trauma, infection, or other factors. While many arachnoid cysts are asymptomatic and do not cause any problems, larger cysts or those that grow or shift over time can put pressure on the brain or spinal cord, leading to a range of neurological symptoms such as headaches, seizures, hearing or vision changes, balance or coordination difficulties, and cognitive impairments.
Treatment for arachnoid cysts depends on their size, location, and associated symptoms. In some cases, observation and monitoring may be sufficient, while in others, surgical intervention may be necessary to drain the cyst or create a connection between it and the surrounding CSF space to relieve pressure.
The fourth ventricle is a part of the cerebrospinal fluid-filled system in the brain, located in the posterior cranial fossa and continuous with the central canal of the medulla oblongata and the cerebral aqueduct. It is shaped like a cavity with a roof, floor, and lateral walls, and it communicates rostrally with the third ventricle through the cerebral aqueduct and caudally with the subarachnoid space through the median and lateral apertures (foramina of Luschka and Magendie). The fourth ventricle contains choroid plexus tissue, which produces cerebrospinal fluid. Its roof is formed by the cerebellar vermis and the superior medullary velum, while its floor is composed of the rhomboid fossa, which includes several important structures such as the vagal trigone, hypoglossal trigone, and striae medullares.
Myelography is a medical imaging technique used to examine the spinal cord and surrounding structures, such as the spinal nerves, intervertebral discs, and the spinal column. This procedure involves the injection of a contrast dye into the subarachnoid space, which is the area surrounding the spinal cord filled with cerebrospinal fluid (CSF). The dye outlines the spinal structures, making them visible on X-ray or CT scan images.
The primary purpose of myelography is to diagnose various spinal conditions, including herniated discs, spinal stenosis, tumors, infection, and traumatic injuries. It can help identify any compression or irritation of the spinal cord or nerves that may be causing pain, numbness, weakness, or other neurological symptoms.
The procedure typically requires the patient to lie flat on their stomach or side while the radiologist inserts a thin needle into the subarachnoid space, usually at the lower lumbar level. Once the contrast dye is injected, the patient will be repositioned for various X-ray views or undergo a CT scan to capture detailed images of the spine. After the procedure, patients may experience headaches, nausea, or discomfort at the injection site, but these symptoms usually resolve within a few days.
The subarachnoid space is the area between the arachnoid mater and pia mater, which are two of the three membranes covering the brain and spinal cord (the third one being the dura mater). This space is filled with cerebrospinal fluid (CSF), which provides protection and cushioning to the central nervous system. The subarachnoid space also contains blood vessels that supply the brain and spinal cord with oxygen and nutrients. It's important to note that subarachnoid hemorrhage, a type of stroke, can occur when there is bleeding into this space.
The posterior cranial fossa is a term used in anatomy to refer to the portion of the skull that forms the lower, back part of the cranial cavity. It is located between the occipital bone and the temporal bones, and it contains several important structures including the cerebellum, pons, medulla oblongata, and the lower cranial nerves (IX-XII). The posterior fossa also contains the foramen magnum, which is a large opening through which the spinal cord connects to the brainstem. This region of the skull is protected by the occipital bone, which forms the base of the skull and provides attachment for several neck muscles.
Surgical decompression is a medical procedure that involves relieving pressure on a nerve or tissue by creating additional space. This is typically accomplished through the removal of a portion of bone or other tissue that is causing the compression. The goal of surgical decompression is to alleviate symptoms such as pain, numbness, tingling, or weakness caused by the compression.
In the context of spinal disorders, surgical decompression is often used to treat conditions such as herniated discs, spinal stenosis, or bone spurs that are compressing nerves in the spine. The specific procedure used may vary depending on the location and severity of the compression, but common techniques include laminectomy, discectomy, and foraminotomy.
It's important to note that surgical decompression is a significant medical intervention that carries risks such as infection, bleeding, and injury to surrounding tissues. As with any surgery, it should be considered as a last resort after other conservative treatments have been tried and found to be ineffective. A thorough evaluation by a qualified medical professional is necessary to determine whether surgical decompression is appropriate in a given case.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
A laminectomy is a surgical procedure that involves the removal of the lamina, which is the back part of the vertebra that covers the spinal canal. This procedure is often performed to relieve pressure on the spinal cord or nerves caused by conditions such as herniated discs, spinal stenosis, or tumors. By removing the lamina, the surgeon can access the affected area and alleviate the compression on the spinal cord or nerves, thereby reducing pain, numbness, or weakness in the back, legs, or arms.
Laminectomy may be performed as a standalone procedure or in combination with other surgical techniques such as discectomy, foraminotomy, or spinal fusion. The specific approach and extent of the surgery will depend on the patient's individual condition and symptoms.
Birth injuries refer to damages or injuries that a baby suffers during the birthing process. These injuries can result from various factors, such as mechanical forces during delivery, medical negligence, or complications during pregnancy or labor. Some common examples of birth injuries include:
1. Brachial plexus injuries: Damage to the nerves that control movement and feeling in the arms and hands, often caused by excessive pulling or stretching during delivery.
2. Cephalohematoma: A collection of blood between the skull and the periosteum (the membrane covering the bone), usually caused by trauma during delivery.
3. Caput succedaneum: Swelling of the soft tissues of the baby's scalp, often resulting from pressure on the head during labor and delivery.
4. Fractures: Broken bones, such as a clavicle or skull fracture, can occur due to mechanical forces during delivery.
5. Intracranial hemorrhage: Bleeding in or around the brain, which can result from trauma during delivery or complications like high blood pressure in the mother.
6. Perinatal asphyxia: A lack of oxygen supply to the baby before, during, or immediately after birth, which can lead to brain damage and other health issues.
7. Subconjunctival hemorrhage: Bleeding under the conjunctiva (the clear membrane covering the eye), often caused by pressure on the head during delivery.
8. Spinal cord injuries: Damage to the spinal cord, which can result in paralysis or other neurological issues, may occur due to excessive force during delivery or medical negligence.
It's important to note that some birth injuries are unavoidable and may not be a result of medical malpractice. However, if a healthcare provider fails to provide the standard of care expected during pregnancy, labor, or delivery, they may be held liable for any resulting injuries.
The arachnoid is one of the three membranes that cover the brain and the spinal cord, known as the meninges. It is located between the dura mater (the outermost layer) and the pia mater (the innermost layer). The arachnoid is a thin, delicate membrane that is filled with cerebrospinal fluid, which provides protection and nutrition to the central nervous system.
The arachnoid has a spider-web like appearance, hence its name, and it is composed of several layers of collagen fibers and elastic tissue. It is highly vascularized, meaning that it contains many blood vessels, and it plays an important role in regulating the flow of cerebrospinal fluid around the brain and spinal cord.
In some cases, the arachnoid can become inflamed or irritated, leading to a condition called arachnoiditis. This can cause a range of symptoms, including pain, muscle weakness, and sensory changes, and it may require medical treatment to manage.
Scoliosis is a medical condition characterized by an abnormal lateral curvature of the spine, which most often occurs in the thoracic or lumbar regions. The curvature can be "C" or "S" shaped and may also include rotation of the vertebrae. Mild scoliosis doesn't typically cause problems, but severe cases can interfere with breathing and other bodily functions.
The exact cause of most scoliosis is unknown, but it may be related to genetic factors. It often develops in the pre-teen or teenage years, particularly in girls, and is more commonly found in individuals with certain neuromuscular disorders such as cerebral palsy and muscular dystrophy.
Treatment for scoliosis depends on the severity of the curve, its location, and the age and expected growth of the individual. Mild cases may only require regular monitoring to ensure the curve doesn't worsen. More severe cases may require bracing or surgery to correct the curvature and prevent it from getting worse.
Cerebrospinal fluid (CSF) is a clear, colorless fluid that surrounds and protects the brain and spinal cord. It acts as a shock absorber for the central nervous system and provides nutrients to the brain while removing waste products. CSF is produced by specialized cells called ependymal cells in the choroid plexus of the ventricles (fluid-filled spaces) inside the brain. From there, it circulates through the ventricular system and around the outside of the brain and spinal cord before being absorbed back into the bloodstream. CSF analysis is an important diagnostic tool for various neurological conditions, including infections, inflammation, and cancer.
Hydrocephalus is a medical condition characterized by an abnormal accumulation of cerebrospinal fluid (CSF) within the brain, leading to an increase in intracranial pressure and potentially causing damage to the brain tissues. This excessive buildup of CSF can result from either overproduction or impaired absorption of the fluid, which typically causes the ventricles (fluid-filled spaces) inside the brain to expand and put pressure on surrounding brain structures.
The condition can be congenital, present at birth due to genetic factors or abnormalities during fetal development, or acquired later in life as a result of injuries, infections, tumors, or other disorders affecting the brain's ability to regulate CSF flow and absorption. Symptoms may vary depending on age, severity, and duration but often include headaches, vomiting, balance problems, vision issues, cognitive impairment, and changes in behavior or personality.
Treatment for hydrocephalus typically involves surgically implanting a shunt system that diverts the excess CSF from the brain to another part of the body where it can be absorbed, such as the abdominal cavity. In some cases, endoscopic third ventriculostomy (ETV) might be an alternative treatment option, creating a new pathway for CSF flow within the brain. Regular follow-ups with neurosurgeons and other healthcare professionals are essential to monitor the condition and make any necessary adjustments to the treatment plan.
The spinal cord is a major part of the nervous system, extending from the brainstem and continuing down to the lower back. It is a slender, tubular bundle of nerve fibers (axons) and support cells (glial cells) that carries signals between the brain and the rest of the body. The spinal cord primarily serves as a conduit for motor information, which travels from the brain to the muscles, and sensory information, which travels from the body to the brain. It also contains neurons that can independently process and respond to information within the spinal cord without direct input from the brain.
The spinal cord is protected by the bony vertebral column (spine) and is divided into 31 segments: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal. Each segment corresponds to a specific region of the body and gives rise to pairs of spinal nerves that exit through the intervertebral foramina at each level.
The spinal cord is responsible for several vital functions, including:
1. Reflexes: Simple reflex actions, such as the withdrawal reflex when touching a hot surface, are mediated by the spinal cord without involving the brain.
2. Muscle control: The spinal cord carries motor signals from the brain to the muscles, enabling voluntary movement and muscle tone regulation.
3. Sensory perception: The spinal cord transmits sensory information, such as touch, temperature, pain, and vibration, from the body to the brain for processing and awareness.
4. Autonomic functions: The sympathetic and parasympathetic divisions of the autonomic nervous system originate in the thoracolumbar and sacral regions of the spinal cord, respectively, controlling involuntary physiological responses like heart rate, blood pressure, digestion, and respiration.
Damage to the spinal cord can result in various degrees of paralysis or loss of sensation below the level of injury, depending on the severity and location of the damage.
Neurogenic arthropathy is a joint disease that occurs as a result of nerve damage or dysfunction. Also known as Charcot joint, this condition is characterized by joint destruction and deformity due to the loss of sensation and proprioception, which normally help protect the joint from excessive stress and injury.
Neurogenic arthropathy often affects people with diabetes, syphilis, leprosy, spinal cord injuries, or other conditions that damage nerves. The damage impairs the ability to feel pain, temperature, and position, making it difficult for individuals to notice or respond to joint injuries. Over time, this can lead to joint degeneration, fractures, dislocations, and severe deformities if left untreated.
Treatment typically involves managing the underlying nerve condition, immobilizing the affected joint with a brace or cast, and in some cases, surgical intervention to repair or replace damaged joints. Regular exercise, physical therapy, and maintaining a healthy lifestyle can also help manage symptoms and prevent further complications.
Dura Mater is the thickest and outermost of the three membranes (meninges) that cover the brain and spinal cord. It provides protection and support to these delicate structures. The other two layers are called the Arachnoid Mater and the Pia Mater, which are thinner and more delicate than the Dura Mater. Together, these three layers form a protective barrier around the central nervous system.
An abdominal reflex is a withdrawal response that occurs when the skin in the lower abdomen is stimulated, leading to contraction of the muscles in the same side of the abdomen. This reflex is mediated by the T10-L1 spinal cord segments and is typically tested during a physical examination to assess the integrity of the nervous system. A decreased or absent abdominal reflex may indicate damage to the peripheral nerves, spinal cord, or brain.
Cerebrospinal fluid (CSF) shunts are medical devices used to divert the flow of excess CSF from the brain and spinal cord to another part of the body, usually the abdominal cavity. The shunt consists of a catheter, a valve, and a reservoir.
The catheter is inserted into one of the ventricles in the brain or the subarachnoid space surrounding the spinal cord to drain the excess CSF. The valve regulates the flow of CSF to prevent over-drainage, which can cause complications such as low CSF pressure and brain sagging. The reservoir is a small chamber that allows for easy access to the shunt system for monitoring and adjusting the pressure settings.
CSF shunts are typically used to treat conditions associated with increased production or impaired absorption of CSF, such as hydrocephalus, communicating hydrocephalus, normal pressure hydrocephalus, and pseudotumor cerebri. By reducing the buildup of CSF in the brain, shunts can help alleviate symptoms such as headaches, nausea, vomiting, vision problems, and cognitive impairment.
It is important to note that while CSF shunts are effective in managing these conditions, they also carry risks of complications such as infection, obstruction, malfunction, and over-drainage. Regular monitoring and follow-up care are necessary to ensure proper functioning and minimize the risk of complications.
Cerebellar diseases refer to a group of medical conditions that affect the cerebellum, which is the part of the brain located at the back of the head, below the occipital lobe and above the brainstem. The cerebellum plays a crucial role in motor control, coordination, balance, and some cognitive functions.
Cerebellar diseases can be caused by various factors, including genetics, infections, tumors, stroke, trauma, or degenerative processes. These conditions can result in a wide range of symptoms, such as:
1. Ataxia: Loss of coordination and unsteady gait
2. Dysmetria: Inability to judge distance and force while performing movements
3. Intention tremors: Shaking or trembling that worsens during purposeful movements
4. Nystagmus: Rapid, involuntary eye movement
5. Dysarthria: Speech difficulty due to muscle weakness or incoordination
6. Hypotonia: Decreased muscle tone
7. Titubation: Rhythmic, involuntary oscillations of the head and neck
8. Cognitive impairment: Problems with memory, attention, and executive functions
Some examples of cerebellar diseases include:
1. Ataxia-telangiectasia
2. Friedrich's ataxia
3. Multiple system atrophy (MSA)
4. Spinocerebellar ataxias (SCAs)
5. Cerebellar tumors, such as medulloblastomas or astrocytomas
6. Infarctions or hemorrhages in the cerebellum due to stroke or trauma
7. Infections, such as viral encephalitis or bacterial meningitis
8. Autoimmune disorders, like multiple sclerosis (MS) or paraneoplastic syndromes
9. Metabolic disorders, such as Wilson's disease or phenylketonuria (PKU)
10. Chronic alcoholism and withdrawal
Treatment for cerebellar diseases depends on the underlying cause and may involve medications, physical therapy, surgery, or supportive care to manage symptoms and improve quality of life.
Spinal cord neoplasms refer to abnormal growths or tumors within the spinal cord. These can be benign (non-cancerous) or malignant (cancerous). They originate from the cells within the spinal cord itself (primary tumors), or they may spread to the spinal cord from other parts of the body (metastatic tumors). Spinal cord neoplasms can cause various symptoms depending on their location and size, including back pain, neurological deficits, and even paralysis. Treatment options include surgery, radiation therapy, and chemotherapy.
Hypohidrosis is a medical condition characterized by reduced or absent sweating. It's the opposite of hyperhidrosis, which is excessive sweating. Sweating is an essential function that helps regulate body temperature through the evaporation of sweat on the skin surface. When this process is impaired due to hypohidrosis, it can lead to difficulties in maintaining a normal body temperature, especially during physical exertion or in hot environments.
Hypohidrosis may be localized, affecting only certain areas of the body, or generalized, affecting the entire body. The causes of hypohidrosis are varied and include genetic factors, nerve damage, skin disorders, dehydration, burns, or the use of certain medications. Depending on its underlying cause, hypohidrosis can be managed through appropriate treatments, such as addressing nerve damage, managing skin conditions, or adjusting medication usage.
Hyperesthesia is a medical term that refers to an increased sensitivity to sensory stimuli, including touch, pain, or temperature. It can affect various parts of the body and can be caused by different conditions, such as nerve damage, multiple sclerosis, or complex regional pain syndrome. Hyperesthesia can manifest as a heightened awareness of sensations, which can be painful or uncomfortable, and may interfere with daily activities. It is essential to consult a healthcare professional for an accurate diagnosis and appropriate treatment if experiencing symptoms of hyperesthesia.
Spinal cord injuries (SCI) refer to damage to the spinal cord that results in a loss of function, such as mobility or feeling. This injury can be caused by direct trauma to the spine or by indirect damage resulting from disease or degeneration of surrounding bones, tissues, or blood vessels. The location and severity of the injury on the spinal cord will determine which parts of the body are affected and to what extent.
The effects of SCI can range from mild sensory changes to severe paralysis, including loss of motor function, autonomic dysfunction, and possible changes in sensation, strength, and reflexes below the level of injury. These injuries are typically classified as complete or incomplete, depending on whether there is any remaining function below the level of injury.
Immediate medical attention is crucial for spinal cord injuries to prevent further damage and improve the chances of recovery. Treatment usually involves immobilization of the spine, medications to reduce swelling and pressure, surgery to stabilize the spine, and rehabilitation to help regain lost function. Despite advances in treatment, SCI can have a significant impact on a person's quality of life and ability to perform daily activities.
An encyclopedia is a comprehensive reference work containing articles on various topics, usually arranged in alphabetical order. In the context of medicine, a medical encyclopedia is a collection of articles that provide information about a wide range of medical topics, including diseases and conditions, treatments, tests, procedures, and anatomy and physiology. Medical encyclopedias may be published in print or electronic formats and are often used as a starting point for researching medical topics. They can provide reliable and accurate information on medical subjects, making them useful resources for healthcare professionals, students, and patients alike. Some well-known examples of medical encyclopedias include the Merck Manual and the Stedman's Medical Dictionary.
Anterior Spinal Artery Syndrome (ASAS) is a medical condition that affects the blood supply to the anterior portion of the spinal cord. This results in a lack of oxygen and nutrients being delivered to the affected area, causing damage to the nerves and tissues.
The anterior spinal artery is responsible for supplying blood to the front two-thirds of the spinal cord, which includes the corticospinal tracts (responsible for motor function) and the spinothalamic tracts (responsible for pain, temperature, and touch sensation).
ASAS can be caused by various conditions that affect the blood flow in the anterior spinal artery, such as atherosclerosis, embolism, vasculitis, or trauma. The symptoms of ASAS depend on the severity and location of the injury but may include:
* Paralysis or weakness in the legs (paraplegia) or all four limbs (tetraplegia)
* Loss of pain and temperature sensation below the level of the injury
* Absent or reduced reflexes
* Autonomic dysfunction, such as bladder and bowel incontinence or sexual dysfunction
* Muscle spasticity or rigidity
The diagnosis of ASAS is typically made based on clinical examination, imaging studies (such as MRI or CT angiography), and sometimes cerebrospinal fluid analysis. Treatment for ASAS focuses on addressing the underlying cause, managing symptoms, and promoting rehabilitation and recovery.
 Syringomyelia
Syringomyelia
Syringobulbia
Scoliosis
Chiari malformation
Ehlers-Danlos syndromes
Tethered spinal cord syndrome
The Chiari Institute
Affenpinscher
Judson Sykes Bury
Canine Chiari-like malformation
Arachnoiditis
Ira Van Gieson
Failed back syndrome
Karin Muraszko
Ependymoma
Pseudoathletic appearance
Neuropathic arthropathy
Henry Head
Syrinx (medicine)
Cavalier King Charles Spaniel
Karlin Lillington
Otto Kahler
Cleidocranial dysostosis
Richard Kretz
Charles-Prosper Ollivier d'Angers
Griffon Bruxellois
Postural orthostatic tachycardia syndrome
Macrocephaly-capillary malformation
Molera
Central canal
Syringomyelia - Wikipedia
 Syringomyelia: MedlinePlus Medical Encyclopedia
Syringomyelia: MedlinePlus Medical Encyclopedia
 Syringomyelia: Background, Pathophysiology, Etiology
Syringomyelia: Background, Pathophysiology, Etiology
 Syringomyelia - Diagnosis and treatment - Mayo Clinic
Syringomyelia - Diagnosis and treatment - Mayo Clinic
 Syringomyelia Managed with Classi... preview & related info | Mendeley
Syringomyelia Managed with Classi... preview & related info | Mendeley
 BVA - Chiari Malformation/Syringomyelia Scheme
BVA - Chiari Malformation/Syringomyelia Scheme
 Syringomyelia | SCUBADOC - Diving Medicine Online
Syringomyelia | SCUBADOC - Diving Medicine Online
 Syringomyelia treatment - New Prague - Mayo Clinic Health System
Syringomyelia treatment - New Prague - Mayo Clinic Health System
ICD-9-CM Diagnosis Code 336.0 : Syringomyelia and syringobulbia
 Magiran | Traumatic Syringomyelias: A Critique on the Basis of the Vortex Effect Theory
Magiran | Traumatic Syringomyelias: A Critique on the Basis of the Vortex Effect Theory
Delayed presentation of syringomyelia after retrosigmoid craniectomy and resection of vestibular schwannoma: discussion of...
 Victoria Guerina "Pain, Weakness, and Uncertainty in the Time of Syringomyelia" - Art League RI
Victoria Guerina "Pain, Weakness, and Uncertainty in the Time of Syringomyelia" - Art League RI
 Go to New considerations about Chiari-like malformation, syringomyelia and their management.
Go to New considerations about Chiari-like malformation, syringomyelia and their management.
Syringomyelia | CRESSC
Noonan syndrome with syringomyelia and type I Chiari malformation<...
 syringomyelia - Hektoen International
syringomyelia - Hektoen International
Cbd ل syringomyelia
 Syringomyelia
Syringomyelia
Syringomyelia ('Syrinx) - Pietro Mortini
 Syringomyelia - THE URBAN BUZZ
Syringomyelia - THE URBAN BUZZ
 Syringomyelia - Wellness Veterinary Hospital
Syringomyelia - Wellness Veterinary Hospital
Chiari and Syringomyelia Australia
Posttraumatic Syringomyelia: Background, Pathophysiology, Epidemiology
 Syringomyelia - London Neurosurgery - Spine & Neurosurgery
Syringomyelia - London Neurosurgery - Spine & Neurosurgery
 Syringomyelia Treatment in India | Maurya
Syringomyelia Treatment in India | Maurya
 Stats Syringomyelia - Syringomyelia Map | Diseasemaps
Stats Syringomyelia - Syringomyelia Map | Diseasemaps
 Clinical Deterioration of Syringomyelia Symptoms Despite Syrinx Resolution After Chiari Decompression - Bobby Jones CSF
Clinical Deterioration of Syringomyelia Symptoms Despite Syrinx Resolution After Chiari Decompression - Bobby Jones CSF
 Syringomyelia: Video, Anatomy, Definition & Function | Osmosis
Syringomyelia: Video, Anatomy, Definition & Function | Osmosis
What is syringomyelia? - Bobby Jones CSF
 Chiari & Syringomyelia Foundation - Nonprofit Staten Island
Chiari & Syringomyelia Foundation - Nonprofit Staten IslandMalformation22
- The most common example is Arnold-Chiari malformation , which is also associated with communicating syringomyelia. (medscape.com)
- If syringomyelia is caused by Chiari malformation, surgery might involve removing a small section of bone at the back of your skull. (mayoclinic.org)
- Syringomyelia (SM) with Chiari malformation is a rare disease with an unpredictable course. (mendeley.com)
- The aim of this Scheme is to reduce and eliminate the incidence of chiari malformation and syringomyelia in dogs. (bva.co.uk)
- Read our chiari malformation/syringomyelia leaflet. (bva.co.uk)
- What is chiari malformation/syringomyelia? (bva.co.uk)
- For more information on the conditions, read our chiari malformation/syringomyelia leaflet . (bva.co.uk)
- There is no one specific treatment for chiari malformation/syringomyelia. (bva.co.uk)
- The scheme uses MRI images of the brain and cranial (upper) cervical spinal cord of dogs for changes indicative of chiari malformation (CM) and syringomyelia SM. (bva.co.uk)
- The certificate will show a grade for chiari-like malformation and a separate grade for syringomyelia. (bva.co.uk)
- Contact your veterinary surgeon and request that your dog be scanned for assessment under the Chiari Malformation/Syringomyelia Scheme. (bva.co.uk)
- We report a patient with Noonan syndrome who also had syringomyelia and a Chiari type I malformation. (psu.edu)
- We suggest that syringomyelia and Chiari I malformation are a rare manifestation of Noonan syndrome that should be sought for in the presence of scoliosis with or without long tract neurologic signs. (psu.edu)
- Miller, G & Ramer, J 1990, ' Noonan syndrome with syringomyelia and type I Chiari malformation ', Dysmorphology and Clinical Genetics , vol. 4, no. 4, pp. 141-144. (psu.edu)
- The causes of syringomyelia do include, damage and injury to the spinal cord, tumours and most commonly Chiari malformation. (lnpuk.com)
- Chiari 1 malformation is the main cause for syringomyelia. (lnpuk.com)
- Our understanding of Chiari-like malformation, and the associated disorder syringomyelia, has changed greatly in recent years. (hallmarq.net)
- Syringomyelia development is caused by a combination of brachycephaly and malformation of the craniocervical junction. (hallmarq.net)
- We invited Professor Clare Rusbridge , a leading expert on Chiari-like malformation and syringomyelia, to share her insights on the current understanding of these problems and their MR imaging interpretation. (hallmarq.net)
- When diagnosing syringomyelia, MRI becomes useful in ruling out other disorders which could be responsible for the clinical signs as well as documenting the multiple malformations which are a composite of the Chiari-like malformation diagnosis. (hallmarq.net)
- Chiari malformation and syringomyelia are complex disorders, but we're learning more about them every day. (hallmarq.net)
- This is the first report to have all the cause and effect mechanisms among syringomyelia, scoliosis and Chiari I malformation in 1 patient. (tmu.edu.tw)
Post-traumatic syringomyelia3
- The primary symptom of post-traumatic syringomyelia (often referred to using the abbreviation of PTS) is pain, which may spread upward from the site of injury. (wikipedia.org)
- The aim of the study was to evaluate the clinical and radiological follow-up of cases who had a history of spine trauma and were being followed up for a diagnosis of post-traumatic syringomyelia and to discuss the existing theories in the literature and the vortex effect in pathogenesis. (magiran.com)
- Records of 44 patients who had a history of high-energy spinal trauma and diagnosed post-traumatic syringomyelia after their follow-up were retrospectively evaluated. (magiran.com)
Syrinx10
- Syringomyelia is the development of a fluid-filled cavity or syrinx within the spinal cord. (medscape.com)
- Even after treatment, some signs and symptoms of syringomyelia can remain, as a syrinx can cause permanent spinal cord and nerve damage. (mayoclinic.org)
- Noncommunicating syringomyelia occurs as a complication of trauma, meningitis, hemorrhage or tumor, the cyst or syrinx developing in a segment of the spinal cord damaged by one or more of these conditions. (scuba-doc.com)
- Syringomyelia is a condition in which an abnormal fluid-filled cavity, or syrinx, develops within the central canal of the spinal cord. (amboss.com)
- Syringomyelia is a fluid filled cyst (syrinx) that has developed within the spinal cord. (lnpuk.com)
- Syringomyelia is an inflammatory condition that causes fluid filled cysts (syrinx) inside the spinal cord. (mauryaayurveda.com)
- Learn more about how syringomyelia (a syrinx in the spinal cord) is identified, diagnosed and treated. (bobbyjonescsf.org)
- Syringomyelia ( sear-IN-go-my-EEL-ya ) (SM) occurs when a cavity, sometimes called a " syrinx ", is formed inside the spinal cord. (bobbyjonescsf.org)
- Syringomyelia is treated based on its etiology , or the underlying cause of the syrinx. (bobbyjonescsf.org)
- Before you explore whether visible central canal dilation or syringomyelia corresponds with clinical signs, you should expect a syrinx width of about 4mm or more in Cavalier King Charles dogs and French bulldogs. (hallmarq.net)
Scoliosis1
- Clinically-relevant syringomyelia causes signs of spinal cord disease in the late stages but initially is associated with a phenomena called 'phantom scratching' as well as a deviation of the neck (termed scoliosis), which can in some cases appear similar to a head tilt. (hallmarq.net)
Symptoms13
- Syringomyelia has a prevalence estimated at 8.4 cases per 100,000 people, with symptoms usually beginning in young adulthood. (wikipedia.org)
- Syringomyelia causes a wide variety of neuropathic symptoms, due to damage to the spinal cord. (wikipedia.org)
- Symptoms of syringomyelia usually appear slowly and worsen over many years. (medlineplus.gov)
- Contact your provider if you have symptoms of syringomyelia. (medlineplus.gov)
- Treatment for syringomyelia depends on the severity and progression of your signs and symptoms. (mayoclinic.org)
- If syringomyelia isn't causing signs or symptoms, monitoring with periodic MRI and neurological exams might be all you need. (mayoclinic.org)
- If syringomyelia is causing signs and symptoms that interfere with your life, or if signs and symptoms rapidly worsen, your doctor will likely recommend surgery. (mayoclinic.org)
- If syringomyelia causes neurological problems that decrease your mobility and activity, such as muscle weakness, pain, fatigue or stiffness, a physical therapist might be able to create an exercise program for you that can help reduce these symptoms. (mayoclinic.org)
- Syringomyelia, The CBD Oil Experiment for symptoms of my Syringomyelia. (web.app)
- If a patient is presenting with the above symptoms associated with syringomyelia then their doctor talk through their medical history and perform a physical examination to look for signs of the condition. (lnpuk.com)
- Medication - although syringomyelia cannot be treated through medication, it can help some of relieve some of the symptoms that it is causing. (lnpuk.com)
- If you have any of the above symptoms and/or are suffering from syringomyelia and would like diagnosis and treatment then please do not hesitate to contact us . (lnpuk.com)
- Syringomyelia symptoms treatment that can be selected on the basis of cause, location, sensation, modalities and extension of the complaints. (rajeevclinic.com)
Neurological1
- Syringomyelia is a neurological condition whereby a fluid-filled cavity or cyst has formed within the spinal cord. (wellnessvet.com.hk)
Depends on the severity1
- There are a few different ways to treat syringomyelia and it all depends on the severity and whether it is affecting the patient's day to day life. (lnpuk.com)
Disorders1
- The 2019 Think Tank research meeting brought together thought leaders in the field of Chiari and related disorders, featuring presentations of novel research in Chiari, syringomyelia and more. (bobbyjonescsf.org)
Cavity2
- Syringomyelia is a generic term referring to a disorder in which a cyst or cavity forms within the spinal cord. (wikipedia.org)
- The fluid in a syringomyelia cavity is identical to CerebroSpinal Fluid ( CSF ). (cressc.org)
Managed with Classical Homeopathy1
- A case of syringomyelia managed with classical homeopathy is presented by Elena Rudakova, Seema. (hpathy.com)
Cyst4
- Syringomyelia is a cyst-like collection of cerebrospinal fluid (CSF) that forms in the spinal cord. (medlineplus.gov)
- First described by Bastian in 1867, posttraumatic syringomyelia (PTS) refers to the development and progression of a cyst filled with cerebrospinal fluid (CSF) within the spinal cord. (medscape.com)
- Watch and wait - this option would be for patients with a less disruptive syringomyelia and it may have been caught early on where the cyst is still very small. (lnpuk.com)
- Syringomyelia can sometimes be called something different, depending on the person-these other names may include hydromyelia, syringohydromyelia or spinal cord cyst. (bobbyjonescsf.org)
Idiopathic2
- Idiopathic syringomyelia has an unknown cause and cannot be classified under any of the previous categories. (medscape.com)
- Sometimes, there is no clear reason for the SM- this is often called idiopathic syringomyelia . (bobbyjonescsf.org)
Cervical5
- This is the most common cause of syringomyelia, where the anatomic abnormality, which may be due to a small posterior fossa, causes the lower part of the cerebellum to protrude from its normal location in the back of the head into the cervical or neck portion of the spinal canal. (wikipedia.org)
- 10 (58.8%) cases presented cervical, 4 (23.5%) cervicothoracic, and 3 (17.6%) thoracic syringomyelias due to axial trauma. (magiran.com)
- 6 (22.2%) cases presented cervical, 4 (14.8%) cases cervicothoracic, and 17 (62.9%) thoracic syringomyelias due to vertical forces. (magiran.com)
- Syringomyelias appeared most frequently in the cervical and cervicothoracic junction due to the vertebral column being affected by axial forces, whereas in the case of vertical forces, it appeared most frequently in the thoracic segments. (magiran.com)
- The neurolocalization corresponds to the damage done by the syringomyelia, which can extend from the cranial cervical vertebrae into the lumbar vertebral column. (hallmarq.net)
Dilation2
- Syringomyelia is an abnormal fluid-filled dilation of the central canal of the spinal cord occurring as a result of impaired CSF flow . (amboss.com)
- Syringomyelia can be categorized as "communicating" (dilation of the central canal) and "noncommunicating" (eccentrically located within the substance of the spinal cord). (medscape.com)
Symptomatic1
- A symptomatic or large syringomyelia is treated by surgery. (bobbyjonescsf.org)
Prevalence4
- Prevalence of asymptomatic syringomyelia in Cavalier King Charles spaniels. (tamu.edu)
- The prevalence of syringomyelia was investigated in a sample population of 555 Cavalier King Charles spaniels. (tamu.edu)
- Data were analysed by logistic regression to determine the effects of sex and age on the prevalence of syringomyelia. (tamu.edu)
- The prevalence of syringomyelia was 25 per cent in dogs aged 12 months, increasing to a peak of 70 per cent in dogs aged 72 months or more. (tamu.edu)
Cord9
- Classically, syringomyelia spares the dorsal column/medial lemniscus of the spinal cord, leaving pressure, vibration, touch and proprioception intact in the upper extremities. (wikipedia.org)
- This theory proposes that syringomyelia results from a "water hammer"-like transmission of pulsatile CSF pressure via a communication between the fourth ventricle and the central canal of the spinal cord through the obex. (medscape.com)
- An MRI of your spine and spinal cord is the most reliable tool for diagnosing syringomyelia. (mayoclinic.org)
- This surgery can reduce pressure on your brain and spinal cord, restore the normal flow of cerebrospinal fluid, and might improve or resolve syringomyelia. (mayoclinic.org)
- As a result, fluid-filled cavities called syrinxes can develop within the spinal cord, with the condition being called syringomyelia (SM). (bva.co.uk)
- The terms " Syringomyelia " refers to when a watery fluid builds up in the spinal cord. (cressc.org)
- Syringomyelia is a condition that causes a fluid filled space to grow inside of your spinal cord causing widespread pain and sometimes paralysis. (web.app)
- Compare this to industry giants like Google, Facebook, Instagram and Twitter who have been hesitant to reap… Spinal cysts, a condition called syringomyelia, are cerebrospinal-fluid-filled (CSF) sacs in the spinal cord. (web.app)
- The primary characteristic of syringomyelia is dilatation of the central canal of the spinal cord creating a variably sized cavitation filled with CSF. (hallmarq.net)
Posterior fossa1
- Obstruction of CSF circulation from the basal posterior fossa to the caudal space may cause syringomyelia of this type. (medscape.com)
Arachnoiditis1
- The second major form of syringomyelia occurs as a complication of trauma, meningitis, hemorrhage, a tumor, or arachnoiditis. (wikipedia.org)
Disorder4
- Syringomyelia is generally a chronic disorder that occurs over time, resulting in muscular atrophy. (wikipedia.org)
- Syringomyelia (SM) in dogs is a common condition that mostly affects Griffon Bruxellois and Cavalier King Charles Spaniels, leading experts to believe it is an inherited disorder. (web.app)
- Syringomyelia is a difficult, complex and fairly rare disorder. (bobbyjonescsf.org)
- The same is true for syringomyelia, although the identification of this disorder is more easily made and more objectively assessed, enabling long term monitoring and evaluation of treatment success. (hallmarq.net)
Weakness1
- It presents definition for terms related to Syringomyelia and medical issues (from Abduction to Weakness). (bvsalud.org)
Patients4
- Neuropathic arthropathy, also known as a Charcot joint, can occur, particularly in the shoulders, in patients with syringomyelia. (wikipedia.org)
- Our aim is to help the patients with Syringomyelia to lead a normal life without being a burden to the society. (mauryaayurveda.com)
- Our hospital brings together specially trained medical staff, advanced monitoring techniques, and specialized Physiotherapy and Ayurvedic treatments focused on improving the outcomes of patients with Syringomyelia. (mauryaayurveda.com)
- Dr. Shetty does a great job highlighting just how complicated syringomyelia treatment is, and explains how surgeons and patients can both better understand the risks and potential outcomes of some surgical treatments. (bobbyjonescsf.org)
Cavitation1
- Even with the spinal canal significantly affected by the cavitation that is syringomyelia, many dogs can still walk since they have enough white matter tracts preserved on the outside. (hallmarq.net)
Treatment3
- There is no known effective treatment for syringomyelia. (medlineplus.gov)
- Identification and treatment of associated dysraphism has the greatest impact on arresting progression of syringomyelia. (medscape.com)
- If you have chronic pain from your syringomyelia, talk to your doctor about treatment options. (mayoclinic.org)
Progression1
- You might have repeated MRI scans over time to monitor the progression of syringomyelia. (mayoclinic.org)
Congenital1
- Generally, there are two forms of syringomyelia: congenital and acquired. (wikipedia.org)
Mechanisms2
- Spinal dysraphism may cause syringomyelia through a variety of mechanisms, including those mentioned under the previous three categories. (medscape.com)
- When considered along with the mechanisms of syringomyelia development, the appearance of syringomyelias can be explained by a vortex effect inside the central canal. (magiran.com)
Clinical signs1
- All dogs, which were declared by their owners to be showing no clinical signs of syringomyelia, underwent MRI to determine the presence or absence of the condition. (tamu.edu)
Onset1
- Onset of syringomyelia is usually between 25 to 40 years old. (medlineplus.gov)
Cysts1
- This, in association with craniocervical junction malformations (deviated dens, C1 overlap with the foramen, quadrigeminal cysts, medullary kinking and dorsal atlantoaxial fibrous bands) is associated with the formation of syringomyelia. (hallmarq.net)
Cerebrospinal1
- Hydromyelia is a dilatation of the central canal by cerebrospinal fluid (CSF) and may be included within the definition of syringomyelia. (medscape.com)
Spine1
- In some cases, syringomyelia might be discovered incidentally during a spine MRI or CT scan conducted for other reasons. (mayoclinic.org)
Incidence1
- An emerging concern is syringomyelia, although the incidence is currently unknown. (wikipedia.org)
Tumors1
- The tumors most often associated with syringomyelia are ependymoma and hemangioblastoma. (medscape.com)
Etiology1
- Often, syringomyelia is used as a generic term before an etiology is determined. (wikipedia.org)
Condition1
- If syringomyelia isn't causing any problems, monitoring the condition may be all that's necessary. (mayoclinichealthsystem.org)
Complications1
- In some people, syringomyelia can progress and lead to serious complications. (rajeevclinic.com)
Develops1
- Syringomyelia mostly develops gradually over time. (mauryaayurveda.com)
Treatments1
- Looking for Syringomyelia Treatments? (mauryaayurveda.com)
Pain1
- CM-associated pain (CM-P) and syringomyelia are increasingly being diagnosed, due to the rising popularity of predisposed brachycephalic breeds and the availability of MRI in veterinary practices. (fitzpatrickreferrals.co.uk)