Testicular Neoplasms
Dysgerminoma
Seminoma
Pancreatic Neoplasms
Neoplasms
Incidence and occupational pattern of leukaemias, lymphomas, and testicular tumours in western Ireland over an 11 year period. (1/2042)
STUDY OBJECTIVE: To determine incidence of the following malignancies, testicular tumours, all leukaemias and all lymphomas in the West of Ireland in an 11 year period. Secondly, to examine the relation between disease patterns and available occupational data in male subjects of working age. DESIGN: A census survey of all cases occurring in the three counties in the Western Health Board (WHB) area, Galway, Mayo and Roscommon, for the 11 year period 1980 to 1990 inclusive. Average annual age standardised incidence rates for the period were calculated using the 1986 census data. Rates for the area are compared with rates from the southern region of Ireland, which had a tumour registry. Trends over the time period are evaluated. All male subjects for whom occupational data were available were categorised using the Irish socioeconomic group classification and incidence rates by occupation were compared using the standardised incidence ratio method. In one of the counties, Galway, a detailed occupational history of selected cases and an age matched control group was also elicited through patients' general practitioners. SETTING: All available case records in the West of Ireland. RESULTS: There are no national incidence records for the period. Compared with data from the Southern Tumour Registry, the number of cases of women with myeloid leukaemias was significantly lower. Male leukaemia rates were significantly lower as a group (SIR 84 (95% CI 74, 95) but not when considered as individual categories. Regression analysis revealed an increasing trend in the number of new cases of non-Hodgkin's lymphoma among both men (r = 0.47, p = 0.02) and women (r = 0.90, p = 0.0001) and of chronic lymphocytic leukaemia in men (r = 0.77, p = 0.005) and women (r = 0.68 p = 0.02) in the WHB region over the last decade. Four hundred and fifty six male cases over the age of 15 years were identified and adequate occupational information was available for 74% of these. Standardised incidence ratios of testicular tumours 100, 938) and agriworkers other than farmers (SIR 377, 95% CI 103, 967). There were also significantly increased incidence ratios for both non-Hodgkin's lymphoma (SIR 169, 95% CI 124, 266) and three categories of leukaemias among farmers. Hodgkin's disease and acute myeloid leukaemias were significantly increased among semi-skilled people. Interview data with 90 cases and 54 controls of both sexes revealed that among farmers, cases (n = 31) were significantly less likely than controls (n = 20) to use tractor mounted spraying techniques (OR = 0.19 (95% CI 0.04, 0.80)) and less likely to wear protective masks (OR 0.22 (95% CI 0.05, 0.84)). CONCLUSIONS: Trends of increase in non-Hodgkin's lymphoma and some leukaemias are consistent with studies elsewhere. The study provides further evidence of the relation between agricultural work and certain lymphoproliferative cancers. The possible carcinogenic role of chemicals used in agricultural industries must be considered as an explanation. (+info)Differential regulation of p21waf-1/cip-1 and Mdm2 by etoposide: etoposide inhibits the p53-Mdm2 autoregulatory feedback loop. (2/2042)
The Mdm2 protein is frequently overexpressed in human non-seminomatous germ cell tumours and transitional carcinoma of the bladder where it may contribute to tolerance of wtp53. Mdm2 forms an autoregulatory feedback loop with p53; the Mdm2 gene is responsive to transactivation by p53 and once synthesized the Mdm2 protein terminates the p53 response. We show here that the topoisomerase poison etoposide, like ultra violet irradiation, inhibits Mdm2 synthesis. Cytotoxic concentrations of etoposide (IC90 for > 3 h) result in inhibition of Mdm2 induction at both the RNA and protein level. Rapid apoptosis ensues. Global transcription is not inhibited: p21waf-1/cip1 and GADD45 expression increase in a dose dependent manner. Inhibition of Mdm2 synthesis depends on the continuous presence of etoposide, suggesting the DNA damage may prevent transcription. Downregulation of Mdm2 transcript occurs in cells expressing HPV16-E6 suggesting that inhibition of Mdm2 transcription is p53-independent. When cells are -treated with a pulse (1 h) of etoposide and reincubated in drug free medium, Mdm2 synthesis commences immediately after damage is repaired (3 h) and the p53 response is attenuated. Induction of apoptosis and loss of clonogenicity are 3-5-fold lower under pulse treatment conditions. This is the first observation of inhibition of Mdm2 transcription following treatment with topoisomerase (topo II) poisons, a feature that may be useful in tumour types where p53 is tolerated by overexpression of Mdm2. (+info)Mutational inactivation of the xeroderma pigmentosum group C gene confers predisposition to 2-acetylaminofluorene-induced liver and lung cancer and to spontaneous testicular cancer in Trp53-/- mice. (3/2042)
Mice that are genetically engineered to mimic the human hereditary cancer-prone DNA repair-defective disease xeroderma pigmentosum (XP) are highly predisposed to UV radiation-induced skin cancer. It is not clear, however, whether XP mice or humans are predisposed to cancers in other tissues associated with exposure to environmental carcinogens. To test the importance of nucleotide excision repair in protection against chemical carcinogenesis in internal organs, we treated XPC mutant (XPC-/-) mice with 2-acetylaminofluorene and NOH-2-acetylaminofluorene. We observed a significantly higher incidence of chemically induced liver and lung tumors in XPC-/- mice compared with normal and heterozygous littermates In addition, the progression of liver tumors in XPC-/- Trp53+/- mice is accelerated compared with XPC-/- Trp53+/+ animals. Finally, we demonstrate a higher incidence of spontaneous testicular tumors in XPC-/- TrpS3-/- double mutant mice compared with XPC+/+ Trp53-/- mice. (+info)Risk of testicular cancer in subfertile men: case-control study. (4/2042)
OBJECTIVE: To evaluate the association between subfertility in men and the subsequent risk of testicular cancer. DESIGN: Population based case-control study. SETTING: The Danish population. PARTICIPANTS: Cases were identified in the Danish Cancer Registry; controls were randomly selected from the Danish population with the computerised Danish Central Population Register. Men were interviewed by telephone; 514 men with cancer and 720 controls participated. OUTCOME MEASURE: Occurrence of testicular cancer. RESULTS: A reduced risk of testicular cancer was associated with paternity (relative risk 0.63; 95% confidence interval 0.47 to 0.85). In men who before the diagnosis of testicular cancer had a lower number of children than expected on the basis of their age, the relative risk was 1.98 (1.43 to 2.75). There was no corresponding protective effect associated with a higher number of children than expected. The associations were similar for seminoma and non-seminoma and were not influenced by adjustment for potential confounding factors. CONCLUSION: These data are consistent with the hypothesis that male subfertility and testicular cancer share important aetiological factors. (+info)Bcl-2 overexpression results in reciprocal downregulation of Bcl-X(L) and sensitizes human testicular germ cell tumours to chemotherapy-induced apoptosis. (5/2042)
Testicular germ cell tumours are hypersentive to chemotherapy and cell lines derived from these tumours are chemosensitive in vitro. We have previously shown that these cell lines express undetectable levels of the suppressor of apoptosis Bcl-2 and relatively high levels of the apoptosis inducer Bax (Chresta et al., 1996). To determine whether the absence of Bcl-2 in these cell lines makes them highly susceptible to drug-induced apoptosis, Bcl-2 was expressed ectopically in the 833K testicular germ cell tumour cell line. Stable overexpressing clones were isolated and three clones were studied further. Surprisingly, Bcl-2 overexpressing cells were sensitized to chemotherapy-induced apoptosis compared to the parental and vector control cells. Analysis of potential mechanisms of sensitization revealed there was a reciprocal downregulation of the endogenously expressed Bcl-X(L) in the Bcl-2 overexpressing clones. Downregulation of Bcl-X(L) to the same extent using antisense oligonucleotides enhanced etoposide-induced apoptosis by twofold. Our results indicate that Bcl-2 and Bcl-X(L) have different abilities to protect against chemotherapy-induced apoptosis in testicular germ cell tumours. In contrast to findings in some tumour cell types, Bcl-2 did not act as a gatekeeper to prevent entry of p53 to the nucleus. (+info)Expression of relaxin-like factor is down-regulated in human testicular Leydig cell neoplasia. (6/2042)
In addition to their role in steroidogenesis in the male, testicular Leydig cells constitutively express large amounts of the peptide relaxin-like factor (RLF), also known as Ley-IL. The Leydig cell-derived RLF belongs to the insulin-like superfamily, which also includes relaxin, insulin and the insulin-like growth factors, and within the testis is a specific marker of Leydig cells. Little information is available either on the regulation of gene expression or on the function of this Leydig cell-derived peptide. In the present study we have investigated the expression pattern of human RLF in patients with rare Leydig cell hyperplasia and adenoma. The expression of both mRNA and protein appear to be decreased in hyperplastic Leydig cells, whereas in the Leydig cell adenomas studied, large central areas of the adenoma were devoid of RLF mRNA and protein. Only Leydig cells located at the periphery of the adenoma displayed expression of RLF, with full agreement between in-situ hybridization and immunohistochemistry. It thus appears that the expression of the RLF gene and its products are down-regulated in Leydig cell hyperplasia and adenoma, consistent with a concomitant dedifferentiation of these cells. (+info)Testicular cancer: an oncological success story. (7/2042)
Testicular cancer has become a model for a curable neoplasm. Our studies with cisplatin combination chemotherapy allow us to conclude that: (a) short-duration intensive induction therapy with the most active agents in optimal dosage is more important than maintenance therapy; (b) modest dose escalation increases toxicity without improving therapeutic efficacy; (c) it is possible to develop curative salvage therapy for refractory germ cell tumors; and (d) preclinical models predicting synergism, such as vinblastine + bleomycin or cisplatin + etoposide have clinical relevance. Finally, testicular cancer has also become a model for new drug development. Cisplatin was approved by the Food and Drug Administration for testis and ovarian cancer, and etoposide and ifosfamide were approved for refractory germ cell tumors. The success of these studies confirms the importance of the continued search for new investigational drugs in all solid tumors. (+info)Semen quality and reproductive hormones before orchiectomy in men with testicular cancer. (8/2042)
PURPOSE: To obtain information about preorchiectomy gonadal function in patients with testicular germ cell cancer to improve the clinical management of fertility and other andrologic aspects in these men. PATIENTS AND METHODS: In group 1, a group of 83 consecutive patients with testicular germ cell cancer (TGCC) investigated before orchiectomy, semen analysis was carried out in 63 patients and hormonal investigations, including measurement of follicle-stimulating hormone, luteinizing hormone (LH), testosterone, estradiol, sex hormone-binding globulin (SHBG), inhibin B, and human chorionic gonadotropin (hCG), in 71 patients. Hormone levels in patients with elevated hCG (n = 41) were analyzed separately. To discriminate between general cancer effects and specific effects associated with TGCC, the same analyses were carried out in a group of 45 consecutive male patients with malignant lymphoma (group 2). Group 3 comprised 141 men employed in a Danish company who served as controls in the comparison of semen parameters. As a control group in hormone investigations, 193 men were selected randomly from the Danish National Personal Register to make up group 4. RESULTS: We found significantly lower sperm concentration (median, 15 x 10(6)/mL; range, 0 to 128 x 10(6)/mL) and total sperm count (median, 29 x 10(6)/mL; range, 0 to 589 x 10(6)) in patients with testicular cancer than in patients with malignant lymphomas (sperm concentration: median, 48 x 10(6)/mL; range, 0.04 to 250 x 10(6)/mL; sperm count: median, 146 x 10(6); range, 0.05 to 418 x 10(6)) (P < .001 and P < .001) and healthy men (sperm concentration: median, 48 x 10(6)/mL; range, 0 to 402 x 10(6)/mL; sperm count: median, 162 x 10(6); range, 0 to 1253 x 10(6)) (P < .001 and P < .001). FSH levels were increased in men with testicular cancer (median, 5.7 IU/L; range, 2.0 to 27 IU/L) compared with both men with malignant lymphomas (median, 3.3 IU/L; range, 1.01 to 12.0 IU/L) and healthy controls (median, 4.1 IU/L; range, 1.04 to 21 IU/L)(P = .001 and P = .007, respectively). Surprisingly, we found significantly lower LH in the group of men with TGCC (median, 3.6 IU/L; range, 1.12 to 11.9 IU/L) than in healthy men (median, 4.7 IU/L; range, 1.3 to 11.9 IU/L) (P = .01). We could not detect any differences between men with testicular cancer and men with malignant lymphomas and healthy men with regard to serum levels of testosterone, SHBG, and estradiol. Men with testicular cancer who had increased hCG levels had significantly lower LH and significantly higher testosterone and estradiol than those without detectable hCG levels. CONCLUSION: Spermatogenesis is already impaired in men with testicular cancer before orchiectomy. Neither local suppression of spermatogenesis by tumor pressure nor a general cancer effect seems to fully explain this impairment. The most likely explanation is preexisting impairment of spermatogenesis in the contralateral testis in men with testicular cancer. The question of whether also a pre-existing Leydig cell dysfunction is present in men with testicular cancer could not be answered in this study because the tumor seems to have a direct effect on the Leydig cells. Men with testicular cancer had low LH values as compared with controls. We speculate that increased intratesticular level of hCG also in men without measurable serum hCG may play a role by exerting LH-like effects on the Leydig cells, causing increased testosterone and estrogen levels and low LH values in the blood. (+info)Testicular neoplasms are abnormal growths or tumors in the testicle that can be benign (non-cancerous) or malignant (cancerous). They are a type of genitourinary cancer, which affects the reproductive and urinary systems. Testicular neoplasms can occur in men of any age but are most commonly found in young adults between the ages of 15 and 40.
Testicular neoplasms can be classified into two main categories: germ cell tumors and non-germ cell tumors. Germ cell tumors, which arise from the cells that give rise to sperm, are further divided into seminomas and non-seminomas. Seminomas are typically slow-growing and have a good prognosis, while non-seminomas tend to grow more quickly and can spread to other parts of the body.
Non-germ cell tumors are less common than germ cell tumors and include Leydig cell tumors, Sertoli cell tumors, and lymphomas. These tumors can have a variety of clinical behaviors, ranging from benign to malignant.
Testicular neoplasms often present as a painless mass or swelling in the testicle. Other symptoms may include a feeling of heaviness or discomfort in the scrotum, a dull ache in the lower abdomen or groin, and breast enlargement (gynecomastia).
Diagnosis typically involves a physical examination, imaging studies such as ultrasound or CT scan, and blood tests to detect tumor markers. Treatment options depend on the type and stage of the neoplasm but may include surgery, radiation therapy, chemotherapy, or a combination of these modalities. Regular self-examinations of the testicles are recommended for early detection and improved outcomes.
Testicular diseases refer to a range of conditions that affect the testicles, the male reproductive organs located in the scrotum. These diseases can affect either one or both testicles and may cause pain, swelling, or impact fertility. Here are some examples of testicular diseases:
1. Testicular cancer: A malignant tumor that develops in the testicle. It is a relatively rare cancer but is highly treatable if detected early.
2. Testicular torsion: A surgical emergency that occurs when the spermatic cord, which supplies blood to the testicle, becomes twisted, cutting off the blood flow.
3. Epididymitis: An infection or inflammation of the epididymis, a coiled tube that stores and carries sperm from the testicle.
4. Orchitis: An infection or inflammation of the testicle itself. It can occur on its own or as a complication of mumps.
5. Hydrocele: A fluid-filled sac that forms around the testicle, causing swelling.
6. Varicocele: Enlarged veins in the scrotum that can cause pain and affect fertility.
7. Inguinal hernia: A condition where a portion of the intestine or fat protrudes through a weakened area in the abdominal wall, often appearing as a bulge in the groin or scrotum.
8. Testicular trauma: Injury to the testicle, which can result from accidents, sports injuries, or other causes.
9. Undescended testicles: A condition where one or both testicles fail to descend from the abdomen into the scrotum before birth.
It is essential for men to perform regular self-examinations to check for any unusual lumps, swelling, or pain in the testicles and seek medical attention if they notice any changes.
Dysgerminoma is a type of germ cell tumor that develops in the ovaries. It is a malignant (cancerous) tumor that primarily affects girls and women of reproductive age, although it can occur at any age. Dysgerminomas are composed of large, round, or polygonal cells with clear cytoplasm and distinct cell borders, arranged in nests or sheets. They may also contain lymphoid aggregates and may produce hormones such as estrogen or testosterone.
Dysgerminomas are usually unilateral (affecting one ovary), but they can be bilateral (affecting both ovaries) in about 10-15% of cases. They tend to grow and spread rapidly, so early detection and treatment are crucial for a favorable prognosis.
The standard treatment for dysgerminoma is surgical removal of the affected ovary or ovaries, followed by chemotherapy with agents such as bleomycin, etoposide, and cisplatin (BEP). With appropriate treatment, the five-year survival rate for patients with dysgerminoma is high, ranging from 80% to 95%.
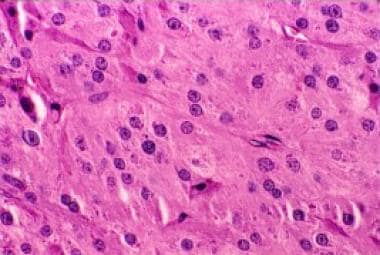
Seminoma is a type of germ cell tumor that develops in the testicle. It is a malignant tumor, meaning it can spread to other parts of the body if left untreated. Seminomas are typically slow-growing and tend to remain localized to the testicle for a longer period compared to other types of testicular cancer. They usually occur in men between the ages of 25 and 45 but can develop at any age.
Seminomas can be classified into two main subtypes: classical seminoma and spermatocytic seminoma. Classical seminoma is more common and typically responds well to treatment, while spermatocytic seminoma is rarer and tends to have a better prognosis with a lower risk of spreading.
Seminomas are usually treated with surgery to remove the affected testicle (orchiectomy), followed by radiation therapy or chemotherapy to kill any remaining cancer cells. The prognosis for seminoma is generally good, especially when caught and treated early. Regular self-examinations of the testicles can help detect any lumps or abnormalities that may indicate the presence of a seminoma or other type of testicular cancer.
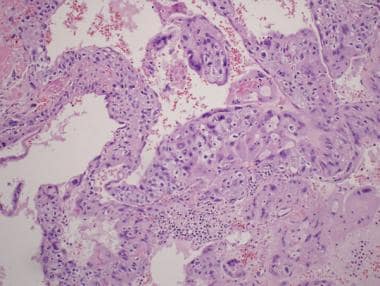
Pancreatic neoplasms refer to abnormal growths in the pancreas that can be benign or malignant. The pancreas is a gland located behind the stomach that produces hormones and digestive enzymes. Pancreatic neoplasms can interfere with the normal functioning of the pancreas, leading to various health complications.
Benign pancreatic neoplasms are non-cancerous growths that do not spread to other parts of the body. They are usually removed through surgery to prevent any potential complications, such as blocking the bile duct or causing pain.
Malignant pancreatic neoplasms, also known as pancreatic cancer, are cancerous growths that can invade and destroy surrounding tissues and organs. They can also spread (metastasize) to other parts of the body, such as the liver, lungs, or bones. Pancreatic cancer is often aggressive and difficult to treat, with a poor prognosis.
There are several types of pancreatic neoplasms, including adenocarcinomas, neuroendocrine tumors, solid pseudopapillary neoplasms, and cystic neoplasms. The specific type of neoplasm is determined through various diagnostic tests, such as imaging studies, biopsies, and blood tests. Treatment options depend on the type, stage, and location of the neoplasm, as well as the patient's overall health and preferences.
Neoplasms are abnormal growths of cells or tissues in the body that serve no physiological function. They can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow growing and do not spread to other parts of the body, while malignant neoplasms are aggressive, invasive, and can metastasize to distant sites.
Neoplasms occur when there is a dysregulation in the normal process of cell division and differentiation, leading to uncontrolled growth and accumulation of cells. This can result from genetic mutations or other factors such as viral infections, environmental exposures, or hormonal imbalances.
Neoplasms can develop in any organ or tissue of the body and can cause various symptoms depending on their size, location, and type. Treatment options for neoplasms include surgery, radiation therapy, chemotherapy, immunotherapy, and targeted therapy, among others.
Neoplasms: Neoplasms refer to abnormal growths of tissue that can be benign (non-cancerous) or malignant (cancerous). They occur when the normal control mechanisms that regulate cell growth and division are disrupted, leading to uncontrolled cell proliferation.
Cystic Neoplasms: Cystic neoplasms are tumors that contain fluid-filled sacs or cysts. These tumors can be benign or malignant and can occur in various organs of the body, including the pancreas, ovary, and liver.
Mucinous Neoplasms: Mucinous neoplasms are a type of cystic neoplasm that is characterized by the production of mucin, a gel-like substance produced by certain types of cells. These tumors can occur in various organs, including the ovary, pancreas, and colon. Mucinous neoplasms can be benign or malignant, and malignant forms are often aggressive and have a poor prognosis.
Serous Neoplasms: Serous neoplasms are another type of cystic neoplasm that is characterized by the production of serous fluid, which is a thin, watery fluid. These tumors commonly occur in the ovary and can be benign or malignant. Malignant serous neoplasms are often aggressive and have a poor prognosis.
In summary, neoplasms refer to abnormal tissue growths that can be benign or malignant. Cystic neoplasms contain fluid-filled sacs and can occur in various organs of the body. Mucinous neoplasms produce a gel-like substance called mucin and can also occur in various organs, while serous neoplasms produce thin, watery fluid and commonly occur in the ovary. Both mucinous and serous neoplasms can be benign or malignant, with malignant forms often being aggressive and having a poor prognosis.
 Leydig cell hypoplasia
Leydig cell hypoplasia Researchers interested in Testicular Neoplasms | Yale School of Medicine
Researchers interested in Testicular Neoplasms | Yale School of Medicine![PGS Catalog - testicular neoplasm [EFO:0004281] (Polygenic Trait)](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAYAAAAf8/9hAAACqUlEQVQ4jYXRT2hcVRTH8e+977730kknk3mZqfnjvzYNMcWooEIXSkREN7oRqwvBjW6L0m33FroXcevWrgSDqKBQiLZTqFEippHYIbZmmMn8y3t582bevcdFXEhbyVkezu+z+B3FA+bS8+8iIouPh1MXN9K7F0+Wpnc++P6TB52i712YyhgfnniZ+bHqq8+MPfxOcfn0x1dff+iNVUmZLE3cB6iPzp8Hpc44597XWhcByW3OK9ulF57Oq2e+fe049Tmz1bt64wdjjADKOdvxtPcZsG2arRZRufzeiysrF5aWlnAixO0e4ac3iFPBm5mgXBlfWDn31sJ0NIVSivX1dX5aW9vLhsPLph/HRFFUODU/z5PLywDsbmwTD27SKFn80jH8MCSamWX59CIAvX6fH9fWCnme398BwEG9iXeQ06/4+GMBngh3eh3EuaNLdAjZHw2cCMlcAWMMgUArS0kHg6OBdD/BbTaJC8LokQk0itAJic1p7/ePBtqbO/j1Po1HA3TlOCJCKCDWcrfb+X9AAcODAb0vb5KonPazVfwgQCmFrz1KFm7t3qGfxKj/ACZOYpxz1Go1fv/uOu52g+zsFF7JkDXbCKD+TfSzjC++XmXU6oAI1lpMEsdYa/nr9ibVqIh6zgeVYeu3wFkAPE/hi0aLMAR2/m6SW8sgG2CqUQ04xUtLGU/MZNjZgPr1LknRogcCSjFeCngs9ZBc0Erxm4u5sjsi2P8T8/ab8PPGiIWTFWbGQ9x0yOyiYktS0u4IpTXFcsBcYnC5QytF7hyFXxvMRTnmq2+eohyFndovXTonQmwcsHVtj3xSEeSHBRQ6PnHqIfYQ2GoMSNyx7l5cxpQnz+Jp8/nqtZby1MEERstw5COMUC4HFFpnGFEghw+zym+HxcqVQiHiHygLN77aGgUdAAAAAElFTkSuQmCC) PGS Catalog - testicular neoplasm [EFO:0004281] (Polygenic Trait)
PGS Catalog - testicular neoplasm [EFO:0004281] (Polygenic Trait) Testicular cancer: MedlinePlus Medical Encyclopedia
Testicular cancer: MedlinePlus Medical Encyclopedia Prepubertal Testicular and Paratesticular Tumors: Practice Essentials, Pathophysiology, Etiology
Prepubertal Testicular and Paratesticular Tumors: Practice Essentials, Pathophysiology, Etiology Identification of nine new susceptibility loci for testicular cancer, including variants near DAZL and PRDM14
Identification of nine new susceptibility loci for testicular cancer, including variants near DAZL and PRDM14 Pathology Case Reports, Elsevier E-Book on VitalSource, 1st Edition - 9780323754927
Pathology Case Reports, Elsevier E-Book on VitalSource, 1st Edition - 9780323754927 Testicular cancer Information | Mount Sinai - New York
Testicular cancer Information | Mount Sinai - New York Jonatan Axelsson - Fingerprint
- Lund University
Jonatan Axelsson - Fingerprint
- Lund University Analysis of gene expression profiles of microdissected cell populations indicates that testicular carcinoma in situ is an...
Analysis of gene expression profiles of microdissected cell populations indicates that testicular carcinoma in situ is an... Vinblastine - Side Effects, Uses, Dosage, Overdose, Pregnancy, Alcohol | RxWiki
Vinblastine - Side Effects, Uses, Dosage, Overdose, Pregnancy, Alcohol | RxWiki Book - Essentials of Pediatric Surgery
| Bentham Science
Book - Essentials of Pediatric Surgery
| Bentham Science Testicular Masses | AAFP
Testicular Masses | AAFP Testicular teratoma in an infant | Pediatric Oncall Journal
Testicular teratoma in an infant | Pediatric Oncall Journal Syndromes Associated with Mediastinal Nonseminomatour Germ Cell Tumors | health.am
Syndromes Associated with Mediastinal Nonseminomatour Germ Cell Tumors | health.am Simultaneously Detected Bilateral Testicular Cancer of Different Histopathological Origin
Simultaneously Detected Bilateral Testicular Cancer of Different Histopathological Origin Richard Barth's Profile | Stanford Profiles
Richard Barth's Profile | Stanford Profiles Christina Bøg Pedersen - Research output
- University of Southern Denmark
Christina Bøg Pedersen - Research output
- University of Southern Denmark 5-year-old male intact German Shepherd Dog - American College of Veterinary Radiology
5-year-old male intact German Shepherd Dog - American College of Veterinary Radiology Seminoma | Harvard Catalyst Profiles | Harvard Catalyst
Seminoma | Harvard Catalyst Profiles | Harvard Catalyst Giant Sertoli cell nodule of the testis: distinction from other Sertoli cell lesions | Journal of Clinical Pathology
Giant Sertoli cell nodule of the testis: distinction from other Sertoli cell lesions | Journal of Clinical Pathology Fetal Age & Pregnancy Test In Charlotte | Any Lab Test Now
Fetal Age & Pregnancy Test In Charlotte | Any Lab Test Now