Thoracic Duct
Chyle
Bile Ducts
Lymphography
Mediastinal Cyst
Pancreatic Ducts
Common Bile Duct
Cystic Duct
Lymphocytes
Salivary Ducts
Iodized Oil
Pericardial Effusion
Pericardial Window Techniques
Bile Duct Diseases
Thoracic Surgery, Video-Assisted
Wolffian Ducts
Lymphocele
Bile Ducts, Extrahepatic
Isolated primary chylopericardium. (1/245)
A 16-year-old man was found to have an enlarged cardiac silhouette. Primary chylopericardium was diagnosed when pericardiocentesis yielded the characteristic milky-white fluid. The thoracic duct was easily identified by giving milk and butter and an injection of ethylene blue immediately before the operation. Intraoperative thoracic ductography showed no abnormal findings. Mass ligation of the thoracic duct above the diaphragm and partial pericardiectomy were successfully performed through a right thoracotomy approach. In addition, many of the lymphatics were ligated above the diaphragm. The right thoracotomy approach was a useful method for resection and ligation of the thoracic duct just above the diaphragm. Follow-up showed no accumulation of pericardial fluid or pleural effusion. (+info)Lymph and pulmonary response to isobaric reduction in plasma oncotic pressure in baboons. (2/245)
Plasma colloid osmotic pressure was reduced by 76% (from 19.6 +/- 0.6 to 4.7 +/- 1.5 mm Hg) in five baboons while pulmonary capillary hydrostatic pressure was maintained at a normal level. This resulted in fluid retention, weight gain, peripheral edema and ascites, but no pulmonary edema. Thoracic duct lymph flow increased 6-fold and pulmonary lymph flow 7-fold. Thoracic duct lymph had a lower colloid osmotic pressure (2.0 +/- 0.7 mm Hg) than plasma (4.7 +/- 1.5 mm Hg), whereas the colloid osmotic pressure of pulmonary lymph (4.7 +/- 0.7 mm Hg) was the same as that of plasma. The lymph-plasma ratio for albumin fell in thoracic duct lymph but remained unchanged in pulmonary lymph. The difference between plasma colloid osmotic pressure and pulmonary artery wedge pressure decreased from 15.3 +/- 1.9 to -0.7 +/- 2.9 mm Hg. Despite this increase in filtration force, the lungs were protected from edema formation by a decrease of 11 mm Hg in pulmonary interstitial colloid osmotic pressure and a 7-fold increase in lymph flow. (+info)Identical T cell clones are located within the mouse gut epithelium and lamina propia and circulate in the thoracic duct lymph. (3/245)
Murine gut intraepithelial (IEL) T cell receptor (TCR)-alpha/beta lymphocytes bearing CD8alpha/13 or CD8alpha/alpha coreceptors have been shown previously to express different oligoclonal TCR beta chain repertoires in the same mouse, in agreement with other evidence indicating that these two populations belong to different ontogenic lineages, with only CD8alpha/beta+ IELs being fully thymus dependent. CD8alpha/beta+, but not CD8alpha/alpha+, T lymphocytes are also present in the lamina propria. Here, we show that CD8alpha/beta+ lymphocytes from the lamina propria and the epithelium are both oligoclonal, and that they share the same TCR-beta clonotypes in the same mouse, as is also the case for CD4alpha T cells. Furthermore, identical T cell clones were detected among CD8alpha/beta IELs and CD8alpha/beta+ blasts circulating into the thoracic duct (TD) lymph of the same mouse, whereas TD small lymphocytes are polyclonal. These findings must be considered in light of previous observations showing that T blasts, but not small T lymphocytes, circulating in the TD lymph have the capacity of homing into the gut epithelium and lamina propria. These combined observations have interesting implications for our understanding of the recirculation of gut thymus-dependent lymphocytes and their precursors, and of the events leading up to the selection of their restricted TCR repertoire. (+info)Computer analysis of defined populations of lymphocytes irradiated in vitro. II. Analysis of thymus-dependent versus bone marrow-dependent cells. (4/245)
Three uniform populations of T and B cells exposed to varying amounts of x-irradiation are examined utilizing computer-assisted morphometric analysis. These populations are: thoracic duct lymphocytes (TDL) from congenitally athymic (nude) mice (B cells); TDL from CBA mice treated with anti-Ig plus complement (T cells); and computer-selected untreated T cells from CBA TDL. Irradiated B cells show a more even dispersion of the nuclear chromatin and a dose-dependent increase in relative nuclear area beginning with the lowest dose evaluated (50 rads); no significan change in total optical density (OD) is demonstrable over the dose range evaluated (0 to 2000 rads). Anti-Ig-treated irradiated T cells demonstrate an initial shift toward lower OD values as a function of dose followed by a marked rise of OD values at 2000 rads, where numerous densely staining Feulgen-positive aggregates are identified. The relative nuclear area of this cell population also shows a biphasic response to radiation injury with an initial increase at the lower dose levels followed by a progressive decline to approximate control levels at 2000 rads. This effect is mirrored by the alteration in total OD which, after a decrease at low dose levels, approximates control values at 2000 rads. The computer-selected T cells show little change in OD values at the low-dose levels but show a marked increase in the more densely staining Feulgen-positive material following 2000 rads. This population reveals no apparent change in either relative nuclear area or total OD as a function of dose. Thus, untreated computer-selected T cells exhibit remarkably little evidence, morphologically, of radiation injury of doses associated with pronounced alterations on the part of B cells. In addition, treatment of a mixed cell population (CBA TDL) with anti-Ig plus complement to remove the B cells appears to alter the response of the residual T cells to radiation injury. These results, in conjunction with recent evidence to support the concept that T cells possess surface Ig, suggest that an Ig-anti-Ig interaction may alter the radiosensitivity of T cells. (+info)Myasthenia gravis: studies on HL-A antigens and lymphocyte subpopulations in patients with myasthenia gravis. (5/245)
Thirth-three patient with a clinical diagnosis of myasthenia gravis were tissue-typed for HL-A antigens. In agreement with earlier reports a significant increase in antigens HL-A1 and HL-A8 were found in this material. Two of the patients were treated with chronic thoracic duct drainage. Proportions of T and B lymphocytes in lymph and peripheral blood were estimated in these patients. In the lymph an initial decrease in the proportion of T cells occurred, which was accompanied by a subsequent increase in the proportion of B cells. Towards the end of the chronic drainage period this effect was reversed. A slightly different picture occurred in blood lymphocytes. Initially, there was an increase in both T and B cells, followed by a decrease in T-cells numbers in one patient, whereas in the second patient the proportion of T cells decreased from the onset of drainage while the proportion of B cells steadily increased. These studies showed that available markers for determination of T ANd B cells were useful for studies of lymphocyte subpopulations in blood and lymph. Lmyphocytes from the thoracic duct were also tested for their reactivity to various mitogens specific for either T or B cells. The B-cell mitogens which were used were dextran sulphate, lipopolysaccharide, purified protein derivative, as well as rabbit anti-human beta2-microglobulin serum. The T-cell mitogens investigated were concanavalin A and phytohaemagglutinin. No significant differences in the responsiveness of thoracic duct lymphocytes compared to normal peripheral blood lymphocytes were found. (+info)Lymphocutaneous fistula as a long-term complication of multiple central venous catheter placement. (6/245)
We report a case of a lymphocutaneous fistula in a 19-month-old boy who had been a premature neonate, born in the 23rd week of gestation. The fistula, an apparent complication of central venous line placement during the patient's first 5 months of life, was composed of a distinct lymphatic vessel bundle in the right supraclavicular region, with its exit point at the posterior aspect of the right shoulder. The drainage ceased immediately after resection and repair of a 1-cm obstruction in the superior vena cava. (+info)In vitro response of bovine thoracic duct lymphocyte to phytohaemagglutinin following adult thymectomy. (7/245)
The effect of adult thymectomy on the thoracic duct lymphocyte population of yearling calves has been investigated. Four to 6 weeks after thymectomy animals showed significantly reduced thoracic duct lymphocyte concentrations when compared to non-thymectomized controls. In addition, phytohaemagglutinin responsiveness of thoracic duct lymphocytes, measured by (3H) thymidine uptake, was significantly decreased following adult thymectomy. However, this decreased response to PHA was not accompanied by a change in spontaneous isotope incorporation. It is concluded that adult thymectomy in the bovine probably leads to a reduction in the number of PHA responsive T cells in the thoracic duct lymph. (+info)Fatal bilateral chylothorax in mice lacking the integrin alpha9beta1. (8/245)
Members of the integrin family of adhesion receptors mediate both cell-cell and cell-matrix interactions and have been shown to play vital roles in embryonic development, wound healing, metastasis, and other biological processes. The integrin alpha9beta1 is a receptor for the extracellular matrix proteins osteopontin and tenacsin C and the cell surface immunoglobulin vascular cell adhesion molecule-1. This receptor is widely expressed in smooth muscle, hepatocytes, and some epithelia. To examine the in vivo function of alpha9beta1, we have generated mice lacking expression of the alpha9 subunit. Mice homozygous for a null mutation in the alpha9 subunit gene appear normal at birth but develop respiratory failure and die between 6 and 12 days of age. The respiratory failure is caused by an accumulation of large volumes of pleural fluid which is rich in triglyceride, cholesterol, and lymphocytes. alpha9(-/-) mice also develop edema and lymphocytic infiltration in the chest wall that appears to originate around lymphatics. alpha9 protein is transiently expressed in the developing thoracic duct at embryonic day 14, but expression is rapidly lost during later stages of development. Our results suggest that the alpha9 integrin is required for the normal development of the lymphatic system, including the thoracic duct, and that alpha9 deficiency could be one cause of congenital chylothorax. (+info)The thoracic duct is the largest lymphatic vessel in the human body. It is a part of the lymphatic system, which helps to regulate fluid balance and immune function. The thoracic duct originates from the cisterna chyli, a dilated sac located in the abdomen near the aorta.
The thoracic duct collects lymph from the lower extremities, abdomen, pelvis, and left side of the thorax (chest). It ascends through the diaphragm and enters the chest, where it passes through the mediastinum (the central part of the chest between the lungs) and eventually drains into the left subclavian vein.
The thoracic duct plays a crucial role in transporting lymphatic fluid, which contains white blood cells, fats, proteins, and other substances, back into the circulatory system. Any obstruction or damage to the thoracic duct can lead to lymph accumulation in the surrounding tissues, causing swelling and other symptoms.
Chylothorax is a medical condition characterized by the accumulation of lymphatic fluid called chyle in the pleural space, which is the space between the lungs and the chest wall. Chyle is a milky-white fluid that contains nutrients, electrolytes, and immune cells, and it is normally transported through the thoracic duct to the bloodstream.
Chylothorax can occur due to various reasons, such as trauma, surgery, tumors, or congenital abnormalities that disrupt the normal flow of chyle. As a result, chyle leaks into the pleural space, causing symptoms such as cough, chest pain, difficulty breathing, and fever.
The diagnosis of chylothorax is usually made through imaging studies such as chest X-ray or CT scan, and confirmed by analyzing the fluid for the presence of chylomicrons, which are lipid particles found in chyle. The treatment options for chylothorax include dietary modifications, such as a low-fat diet with medium-chain triglycerides, chest tube drainage, and surgical interventions such as thoracic duct ligation or pleurodesis.
Lymph is a colorless, transparent fluid that circulates throughout the lymphatic system, which is a part of the immune and circulatory systems. It consists of white blood cells called lymphocytes, proteins, lipids, glucose, electrolytes, hormones, and waste products. Lymph plays an essential role in maintaining fluid balance, absorbing fats from the digestive tract, and defending the body against infection by transporting immune cells to various tissues and organs. It is collected from tissues through lymph capillaries and flows through increasingly larger lymphatic vessels, ultimately returning to the bloodstream via the subclavian veins in the chest region.
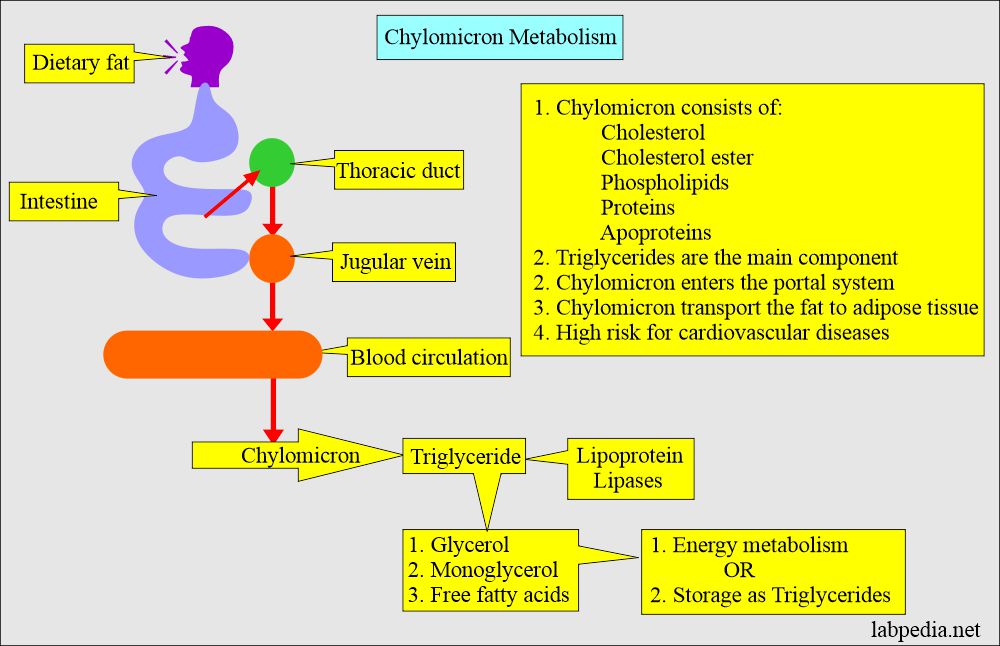
Chyle is a milky, slightly opaque fluid that is present in the lymphatic system. It is formed in the small intestine during the digestion of food, particularly fats. Chyle consists of emulsified fat droplets (chylomicrons), proteins, electrolytes, and lymphocytes suspended in a watery solution. It is transported through the lacteals in the villi of the small intestine into the cisterna chyli and then to the thoracic duct, where it empties into the left subclavian vein. From there, it mixes with blood and circulates throughout the body. Chyle formation plays a crucial role in fat absorption and transportation in the human body.
The lymphatic system is a complex network of organs, tissues, vessels, and cells that work together to defend the body against infectious diseases and also play a crucial role in the immune system. It is made up of:
1. Lymphoid Organs: These include the spleen, thymus, lymph nodes, tonsils, adenoids, and Peyer's patches (in the intestines). They produce and mature immune cells.
2. Lymphatic Vessels: These are thin tubes that carry clear fluid called lymph towards the heart.
3. Lymph: This is a clear-to-white fluid that contains white blood cells, mainly lymphocytes, which help fight infections.
4. Other tissues and cells: These include bone marrow where immune cells are produced, and lymphocytes (T cells and B cells) which are types of white blood cells that help protect the body from infection and disease.
The primary function of the lymphatic system is to transport lymph throughout the body, collecting waste products, bacteria, viruses, and other foreign substances from the tissues, and filtering them out through the lymph nodes. The lymphatic system also helps in the absorption of fats and fat-soluble vitamins from food in the digestive tract.
Bile ducts are tubular structures that carry bile from the liver to the gallbladder for storage or directly to the small intestine to aid in digestion. There are two types of bile ducts: intrahepatic and extrahepatic. Intrahepatic bile ducts are located within the liver and drain bile from liver cells, while extrahepatic bile ducts are outside the liver and include the common hepatic duct, cystic duct, and common bile duct. These ducts can become obstructed or inflamed, leading to various medical conditions such as cholestasis, cholecystitis, and gallstones.
Lymphography is not a commonly used term in current medical practice. However, historically, it referred to a radiographic imaging technique that involved the injection of a contrast material into the lymphatic system to visualize the lymph nodes and lymph vessels. This procedure was used primarily for diagnostic purposes, particularly in the evaluation of cancerous conditions like lymphoma or melanoma.
The process typically involved injecting a radiopaque substance into the interstitial tissue, which would then be taken up by the lymphatic vessels and transported to the regional lymph nodes. X-ray imaging was used to track the progression of the contrast material, creating detailed images of the lymphatic system.
Due to advancements in medical imaging technology, lymphography has largely been replaced by other non-invasive imaging techniques such as computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET) scans. These modern methods provide high-resolution images of the body's internal structures without requiring invasive procedures or the use of contrast materials.
A mediastinal cyst is a rare, abnormal fluid-filled sac located in the mediastinum, which is the central part of the chest cavity that separates the lungs and contains various organs such as the heart, esophagus, trachea, thymus gland, and lymph nodes. Mediastinal cysts can be congenital (present at birth) or acquired (develop later in life). They are usually asymptomatic but can cause symptoms depending on their size and location. Symptoms may include chest pain, cough, difficulty breathing, or swallowing. Treatment typically involves surgical removal of the cyst to prevent complications such as infection, bleeding, or pressure on surrounding structures.
The pancreatic ducts are a set of tubular structures within the pancreas that play a crucial role in the digestive system. The main pancreatic duct, also known as the duct of Wirsung, is responsible for transporting pancreatic enzymes and bicarbonate-rich fluid from the pancreas to the duodenum, which is the first part of the small intestine.
The exocrine portion of the pancreas contains numerous smaller ducts called interlobular ducts and intralobular ducts that merge and ultimately join the main pancreatic duct. This system ensures that the digestive enzymes and fluids produced by the pancreas are effectively delivered to the small intestine, where they aid in the breakdown and absorption of nutrients from food.
In addition to the main pancreatic duct, there is an accessory pancreatic duct, also known as Santorini's duct, which can sometimes join the common bile duct before emptying into the duodenum through a shared opening called the ampulla of Vater. However, in most individuals, the accessory pancreatic duct usually drains into the main pancreatic duct before entering the duodenum.
Thymectomy is a surgical procedure that involves the removal of the thymus gland. The thymus gland is a part of the immune system located in the upper chest, behind the sternum (breastbone), and above the heart. It is responsible for producing white blood cells called T-lymphocytes, which help fight infections.
Thymectomy is often performed as a treatment option for patients with certain medical conditions, such as:
* Myasthenia gravis: an autoimmune disorder that causes muscle weakness and fatigue. In some cases, the thymus gland may contain abnormal cells that contribute to the development of myasthenia gravis. Removing the thymus gland can help improve symptoms in some patients with this condition.
* Thymomas: tumors that develop in the thymus gland. While most thymomas are benign (non-cancerous), some can be malignant (cancerous) and may require surgical removal.
* Myasthenic syndrome: a group of disorders characterized by muscle weakness and fatigue, similar to myasthenia gravis. In some cases, the thymus gland may be abnormal and contribute to the development of these conditions. Removing the thymus gland can help improve symptoms in some patients.
Thymectomy can be performed using various surgical approaches, including open surgery (through a large incision in the chest), video-assisted thoracoscopic surgery (VATS, using small incisions and a camera to guide the procedure), or robotic-assisted surgery (using a robot to perform the procedure through small incisions). The choice of surgical approach depends on several factors, including the size and location of the thymus gland, the patient's overall health, and the surgeon's expertise.
The thoracic cavity is the medical term for the chest region that lies between the neck and the diaphragm. It is one of the main body cavities, enclosed by the ribcage and protected by the sternum in front and the vertebral column behind. This cavity contains vital organs such as the heart and lungs, along with the esophagus, trachea, thoracic aorta, and various nerves and blood vessels. The thoracic cavity is lined by a serous membrane called the pleura, which covers the lungs (visceral pleura) and lines the inner surface of the chest wall (parietal pleura). This cavity plays a crucial role in respiration and protection of vital organs.
The common bile duct is a duct that results from the union of the cystic duct (which drains bile from the gallbladder) and the common hepatic duct (which drains bile from the liver). The common bile duct transports bile, a digestive enzyme, from the liver and gallbladder to the duodenum, which is the first part of the small intestine.
The common bile duct runs through the head of the pancreas before emptying into the second part of the duodenum, either alone or in conjunction with the pancreatic duct, via a small opening called the ampulla of Vater. The common bile duct plays a crucial role in the digestion of fats by helping to break them down into smaller molecules that can be absorbed by the body.
The cystic duct is a short tube that connects the gallbladder to the common bile duct, which carries bile from the liver and gallbladder into the small intestine. The cystic duct allows bile to flow from the gallbladder into the common bile duct when it is needed for digestion. It is a part of the biliary system and plays an important role in the digestive process.
Lymphocytes are a type of white blood cell that is an essential part of the immune system. They are responsible for recognizing and responding to potentially harmful substances such as viruses, bacteria, and other foreign invaders. There are two main types of lymphocytes: B-lymphocytes (B-cells) and T-lymphocytes (T-cells).
B-lymphocytes produce antibodies, which are proteins that help to neutralize or destroy foreign substances. When a B-cell encounters a foreign substance, it becomes activated and begins to divide and differentiate into plasma cells, which produce and secrete large amounts of antibodies. These antibodies bind to the foreign substance, marking it for destruction by other immune cells.
T-lymphocytes, on the other hand, are involved in cell-mediated immunity. They directly attack and destroy infected cells or cancerous cells. T-cells can also help to regulate the immune response by producing chemical signals that activate or inhibit other immune cells.
Lymphocytes are produced in the bone marrow and mature in either the bone marrow (B-cells) or the thymus gland (T-cells). They circulate throughout the body in the blood and lymphatic system, where they can be found in high concentrations in lymph nodes, the spleen, and other lymphoid organs.
Abnormalities in the number or function of lymphocytes can lead to a variety of immune-related disorders, including immunodeficiency diseases, autoimmune disorders, and cancer.
Chylous ascites is a medical condition characterized by the accumulation of milky, fat-containing fluid in the peritoneal cavity, which is the space within the abdomen that contains the intestines, liver, and other organs. The fluid, called chyle, is normally found in the lymphatic system and is formed when dietary fats are absorbed from the small intestine.
Chylous ascites can occur as a result of damage to the lymphatic vessels that transport chyle from the intestines to the bloodstream. This damage can be caused by various conditions, such as trauma, surgery, tumors, inflammation, or congenital abnormalities. When the lymphatic vessels are damaged, chyle leaks into the peritoneal cavity and accumulates there, leading to ascites.
Symptoms of chylous ascites may include abdominal distension, pain, nausea, vomiting, and weight loss. The condition can be diagnosed through various tests, such as imaging studies or analysis of the fluid in the peritoneal cavity. Treatment typically involves addressing the underlying cause of the condition, as well as managing symptoms and preventing complications. This may include dietary modifications, medications to reduce lymphatic flow, or surgical interventions to repair damaged lymphatic vessels.
Salivary ducts are the excretory tubules that transport saliva from the major and minor salivary glands to the oral cavity. The main function of these ducts is to convey the salivary secretions, which contain enzymes and lubricants, into the mouth to aid in digestion, speech, and swallowing.
There are two pairs of major salivary glands: the parotid glands and the submandibular glands. Each pair has its own set of ducts. The parotid gland's saliva is drained through the parotid duct, also known as Stensen's duct, which opens into the oral cavity opposite the upper second molar tooth. The submandibular gland's saliva is transported through the submandibular duct, or Wharton's duct, which empties into the floor of the mouth near the base of the tongue.
Minor salivary glands are scattered throughout the oral cavity and pharynx, and their secretions are drained via small ducts directly into the oral mucosa.
Iodized oil is a type of oil, often sesame or soybean oil, that has been artificially enriched with the essential micromineral iodine. It is typically used as a medical treatment for iodine deficiency disorders, such as goiter and cretinism, and for preventing their occurrence.
The iodization process involves binding iodine to the oil molecules, which allows the iodine to be slowly released and absorbed by the body over an extended period of time. This makes it an effective long-term supplement for maintaining adequate iodine levels in the body. Iodized oil is usually administered via intramuscular injection, and its effects can last for several months to a year.
It's important to note that while iodized oil is a valuable tool in addressing iodine deficiency on an individual level, global public health initiatives have focused on adding iodine to table salt (known as iodization of salt) as a more widespread and sustainable solution for eliminating iodine deficiency disorders.
Ligation, in the context of medical terminology, refers to the process of tying off a part of the body, usually blood vessels or tissue, with a surgical suture or another device. The goal is to stop the flow of fluids such as blood or other substances within the body. It is commonly used during surgeries to control bleeding or to block the passage of fluids, gases, or solids in various parts of the body.
Thoracoscopy is a surgical procedure in which a thoracoscope, a type of endoscope, is inserted through a small incision between the ribs to examine the lungs and pleural space (the space surrounding the lungs). It allows the surgeon to directly view the chest cavity, take biopsies, and perform various operations. This procedure is often used in the diagnosis and treatment of pleural effusions, lung cancer, and other chest conditions.
Pericardial effusion is an abnormal accumulation of fluid in the pericardial space, which is the potential space between the two layers of the pericardium - the fibrous and serous layers. The pericardium is a sac that surrounds the heart to provide protection and lubrication for the heart's movement during each heartbeat. Normally, there is only a small amount of fluid (5-15 mL) in this space to ensure smooth motion of the heart. However, when an excessive amount of fluid accumulates, it can cause increased pressure on the heart, leading to various complications such as decreased cardiac output and even cardiac tamponade, a life-threatening condition that requires immediate medical attention.
Pericardial effusion may result from several causes, including infections (viral, bacterial, or fungal), inflammatory conditions (such as rheumatoid arthritis, lupus, or cancer), trauma, heart surgery, kidney failure, or iatrogenic causes. The symptoms of pericardial effusion can vary depending on the rate and amount of fluid accumulation. Slowly developing effusions may not cause any symptoms, while rapid accumulations can lead to chest pain, shortness of breath, cough, palpitations, or even hypotension (low blood pressure). Diagnosis is usually confirmed through imaging techniques such as echocardiography, CT scan, or MRI. Treatment depends on the underlying cause and severity of the effusion, ranging from close monitoring to drainage procedures or medications to address the root cause.
A pericardial window technique is a surgical procedure that creates an opening or window in the pericardium, which is the sac-like membrane surrounding the heart. This procedure is typically performed to relieve excessive pressure on the heart caused by excess fluid accumulation in the pericardial space (pericardial effusion) or to obtain tissue samples for diagnostic purposes.
There are two primary approaches to creating a pericardial window:
1. Surgical Pericardial Window: This is an open surgical procedure, usually performed under general anesthesia. The surgeon makes an incision in the chest wall and then opens the pericardium to create a window. Excess fluid is drained from the pericardial space, and the pericardial edges are sutured together to keep the window open. This technique allows for continuous drainage of any future fluid accumulation.
2. Percutaneous Pericardial Window: This is a minimally invasive procedure that involves inserting a needle or catheter through the skin and into the pericardial space under local anesthesia and image guidance (fluoroscopy, echocardiography, or CT scan). A guidewire is then passed through the needle, followed by a dilator and sheath. A drainage catheter is placed through the sheath into the pericardial space to remove excess fluid. The catheter may be left in place for several days to allow for continued drainage.
Pericardial window techniques are used to treat various conditions, including cardiac tamponade (life-threatening compression of the heart due to pericardial effusion), infectious pericarditis, malignant pericardial effusions, and inflammatory disorders affecting the pericardium.
Bile duct diseases refer to a group of medical conditions that affect the bile ducts, which are tiny tubes that carry bile from the liver to the gallbladder and small intestine. Bile is a digestive juice produced by the liver that helps break down fats in food.
There are several types of bile duct diseases, including:
1. Choledocholithiasis: This occurs when stones form in the common bile duct, causing blockage and leading to symptoms such as abdominal pain, jaundice, and fever.
2. Cholangitis: This is an infection of the bile ducts that can cause inflammation, pain, and fever. It can occur due to obstruction of the bile ducts or as a complication of other medical procedures.
3. Primary Biliary Cirrhosis (PBC): This is a chronic autoimmune disease that affects the bile ducts in the liver, causing inflammation and scarring that can lead to cirrhosis and liver failure.
4. Primary Sclerosing Cholangitis (PSC): This is another autoimmune disease that causes inflammation and scarring of the bile ducts, leading to liver damage and potential liver failure.
5. Bile Duct Cancer: Also known as cholangiocarcinoma, this is a rare form of cancer that affects the bile ducts and can cause jaundice, abdominal pain, and weight loss.
6. Benign Strictures: These are narrowing of the bile ducts that can occur due to injury, inflammation, or surgery, leading to blockage and potential infection.
Symptoms of bile duct diseases may include jaundice, abdominal pain, fever, itching, dark urine, and light-colored stools. Treatment depends on the specific condition and may involve medication, surgery, or other medical interventions.
Thoracic surgery, video-assisted (VATS) is a minimally invasive surgical technique used to diagnose and treat various conditions related to the chest cavity, including the lungs, pleura, mediastinum, esophagus, and diaphragm. In VATS, a thoracoscope, a type of endoscope with a camera and light source, is inserted through small incisions in the chest wall to provide visualization of the internal structures. The surgeon then uses specialized instruments to perform the necessary surgical procedures, such as biopsies, lung resections, or esophageal repairs. Compared to traditional open thoracic surgery, VATS typically results in less postoperative pain, shorter hospital stays, and quicker recoveries for patients.
The Wolffian ducts, also known as the mesonephric ducts, are a pair of embryological structures present in the developing urinary system of male fetuses. They originate from the intermediate mesoderm and descend towards the posterior end of the developing kidney, or the metanephros.
The Wolffian ducts play a crucial role in the formation of the male reproductive system. In males, these ducts give rise to the vas deferens, seminal vesicles, and ejaculatory ducts. They also contribute to the development of the kidneys, specifically the pronephros and mesonephros, which are transient structures that eventually give way to the permanent kidney, or metanephros.
In females, the Wolffian ducts regress due to the absence of testicular hormones, as they do not contribute to the formation of female reproductive organs. Instead, the paramesonephric ducts, also known as the Mullerian ducts, develop into the female reproductive structures such as the fallopian tubes, uterus, and vagina.
Drainage, in medical terms, refers to the removal of excess fluid or accumulated collections of fluids from various body parts or spaces. This is typically accomplished through the use of medical devices such as catheters, tubes, or drains. The purpose of drainage can be to prevent the buildup of fluids that may cause discomfort, infection, or other complications, or to treat existing collections of fluid such as abscesses, hematomas, or pleural effusions. Drainage may also be used as a diagnostic tool to analyze the type and composition of the fluid being removed.
A lymphocele is a localized collection or sac filled with lymph fluid, which usually forms as a result of surgical dissection or injury to the lymphatic vessels. The accumulation of lymph fluid occurs due to the disruption of normal lymphatic drainage in the affected area.
Lymphoceles are most commonly found following surgeries involving the lymph nodes, such as pelvic, groin, or abdominal procedures. They can also occur after radiotherapy treatments that damage the lymphatic vessels. In some cases, lymphoceles may develop spontaneously due to underlying medical conditions affecting the lymphatic system.
While lymphoceles are generally not harmful on their own, they can cause complications such as infection, delayed wound healing, or impaired limb function if they become large enough to put pressure on surrounding tissues and organs. Treatment options for lymphoceles include compression garments, percutaneous drainage, sclerosis (the injection of a substance that causes the sac to stick together), or surgical removal in severe cases.
Extrahepatic bile ducts refer to the portion of the biliary system that lies outside the liver. The biliary system is responsible for producing, storing, and transporting bile, a digestive fluid produced by the liver.
The extrahepatic bile ducts include:
1. The common hepatic duct: This duct is formed by the union of the right and left hepatic ducts, which drain bile from the corresponding lobes of the liver.
2. The cystic duct: This short duct connects the gallbladder to the common hepatic duct, allowing bile to flow into the gallbladder for storage and concentration.
3. The common bile duct: This is the result of the fusion of the common hepatic duct and the cystic duct. It transports bile from the liver and gallbladder to the duodenum, the first part of the small intestine, where it aids in fat digestion.
4. The ampulla of Vater (or hepatopancreatic ampulla): This is a dilated area where the common bile duct and the pancreatic duct join and empty their contents into the duodenum through a shared opening called the major duodenal papilla.
Extrahepatic bile ducts can be affected by various conditions, such as gallstones, inflammation (cholangitis), strictures, or tumors, which may require medical or surgical intervention.
Lymphatic vessels are thin-walled, valved structures that collect and transport lymph, a fluid derived from the interstitial fluid surrounding the cells, throughout the lymphatic system. They play a crucial role in immune function and maintaining fluid balance in the body. The primary function of lymphatic vessels is to return excess interstitial fluid, proteins, waste products, and immune cells to the bloodstream via the subclavian veins near the heart.
There are two types of lymphatic vessels:
1. Lymphatic capillaries: These are the smallest lymphatic vessels, found in most body tissues except for the central nervous system (CNS). They have blind ends and are highly permeable to allow the entry of interstitial fluid, proteins, and other large molecules.
2. Larger lymphatic vessels: These include precollecting vessels, collecting vessels, and lymphatic trunks. Precollecting vessels have valves that prevent backflow of lymph and merge to form larger collecting vessels. Collecting vessels contain smooth muscle in their walls, which helps to propel the lymph forward. They also have valves at regular intervals to ensure unidirectional flow towards the heart. Lymphatic trunks are large vessels that collect lymph from various regions of the body and eventually drain into the two main lymphatic ducts: the thoracic duct and the right lymphatic duct.
Overall, lymphatic vessels play a vital role in maintaining fluid balance, immune surveillance, and waste removal in the human body.
 Thoracic duct
Thoracic duct Mediastinal Thoracic Duct Cyst - An Unusual Finding
Mediastinal Thoracic Duct Cyst - An Unusual Finding LYSOSOMES IN RAT THORACIC DUCT LYMPHOCYTES FRACTIONATED BY ZONAL CENTRIFUGATION | Journal of Cell Biology | Rockefeller...
LYSOSOMES IN RAT THORACIC DUCT LYMPHOCYTES FRACTIONATED BY ZONAL CENTRIFUGATION | Journal of Cell Biology | Rockefeller... Acervo Digital: COLLATERAL LYMPHATIC CIRCULATION AFTER THORACIC-DUCT LIGATURE IN DOGS
Acervo Digital: COLLATERAL LYMPHATIC CIRCULATION AFTER THORACIC-DUCT LIGATURE IN DOGS thoracic duct Archives - CriticalCareDVM
thoracic duct Archives - CriticalCareDVM Supraomohyoid Neck Dissection: Background, History of the Procedure, Problem
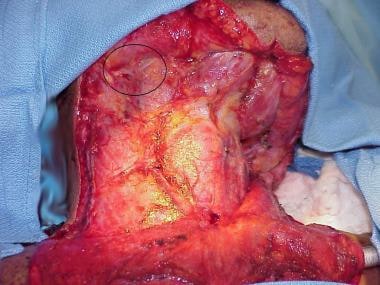
Supraomohyoid Neck Dissection: Background, History of the Procedure, Problem Download MBBS Lymphatic System and Thoracic Duct Lecture Notes : FirstRanker.com
Download MBBS Lymphatic System and Thoracic Duct Lecture Notes : FirstRanker.com Pneumocystis carinii pneumonia after thoracic duct ligation and leakage - ePrints - Newcastle University
Pneumocystis carinii pneumonia after thoracic duct ligation and leakage - ePrints - Newcastle University From Copenhagen to Yedo: the long journey of the thoracic duct<...
From Copenhagen to Yedo: the long journey of the thoracic duct<... submandibular lymph nodes
submandibular lymph nodes Lymphatic vessels and lymph nodes of the pelvis and spine, thoracic duct | Anatomia Collection: anatomical plates 1522-1867
Lymphatic vessels and lymph nodes of the pelvis and spine, thoracic duct | Anatomia Collection: anatomical plates 1522-1867 Lymphovenous Anastomoses Between Thoracic Duct and Azygos Vein in a Human Cadaver: A Case Report | Koutsouflianiotis | Acta...
Lymphovenous Anastomoses Between Thoracic Duct and Azygos Vein in a Human Cadaver: A Case Report | Koutsouflianiotis | Acta... Histamine-releasing activity. IV. Molecular heterogeneity of the activity from stimulated human thoracic duct lymphocytes -...
Histamine-releasing activity. IV. Molecular heterogeneity of the activity from stimulated human thoracic duct lymphocytes -... Combining non-contrast enhanced magnetic resonance thoracic ductography with vascular contrast-enhanced computed tomography to...
Combining non-contrast enhanced magnetic resonance thoracic ductography with vascular contrast-enhanced computed tomography to... Lymphocyte - New World Encyclopedia
Lymphocyte - New World Encyclopedia Full text of 'Are Inventions Inevitable? A Note on Social Evolution'
Full text of 'Are Inventions Inevitable? A Note on Social Evolution' Bassett Collection Large Image - Lane Medical Library, Stanford University Medical Center
Bassett Collection Large Image - Lane Medical Library, Stanford University Medical Center Metatalktail Hour: Other Science Facts | MetaTalk
Metatalktail Hour: Other Science Facts | MetaTalk A contemporary review of chylothorax
A contemporary review of chylothorax