Trigeminal Nerve Injuries
Trigeminal Neuralgia
Trigeminal Nerve
Trigeminal Nerve Diseases
Cranial Nerve Neoplasms
Sciatic Nerve
Cranial Nerve Injuries
Lingual Nerve Injuries
Maxillary Nerve
Optic Nerve Injuries
Peripheral Nerves
Effects of different types of injury to the inferior alveolar nerve on the behavior of Schwann cells during the regeneration of periodontal nerve fibers of rat incisor. (1/58)
The present study reports on different regeneration patterns of axons and Schwann cells in the periodontal ligament of the rat incisor using immunohistochemistry of protein gene product 9.5 (PGP 9.5) and S-100 protein. Three kinds of injury (transection, crush and segmental resection) were applied to the inferior alveolar nerve. In normal animals, PGP 9.5- and S-100-immunoreactivities were detected in the axons and Schwann cell elements of periodontal Ruffini endings, respectively. They were restricted to the alveolus-related part, occurring only rarely in the tooth-related part and in the shear zone (the border between the alveolus-related and tooth-related parts). Both transection and segmental resection caused the complete disappearance of PGP 9.5-immunoreactive nerve fibers in the periodontal ligament, while a small number of them could be found following the crush injury. Regenerating PGP 9.5-reactive nerve fibers appeared at 5 days and 21 days following the transection and segmental resection, respectively. The regeneration of periodontal nerve fibers completed in a period of 21-28 days and 14-21 days following the transection and crush, respectively, but was not completed even at 56 days following the segmental resection. The behavior of Schwann cells during regeneration was similar after the different nerve injuries; spindle-shaped S-100-immunoreactive cells, presumably Schwann cells, appeared in the shear zone and the tooth-related part. These cells disappeared 5-7 days prior to the completion of the regeneration of axonal elements of the periodontal ligament following the transection and crush. Following the segmental resection, in contrast, spindle-shaped S-100-positive cells disappeared from the tooth-related part at 42 days, although the axonal regeneration of periodontal Ruffini endings proceeded even until 56 days. We thus conclude that the duration of the migration of Schwann cells depends on the state of the regeneration of axons. (+info)Clinical evaluation of inferior alveolar nerve block by injection into the pterygomandibular space anterior to the mandibular foramen. (2/58)
The conventional inferior alveolar nerve block (conventional technique) has potential risks of neural and vascular injuries. We studied a method of inferior alveolar nerve block by injecting a local anesthetic solution into the pterygomandibular space anterior to the mandibular foramen (anterior technique) with the purpose of avoiding such complications. The insertion angle of the anterior technique and the estimation of anesthesia in the anterior technique were examined. The predicted insertion angle measured on computed tomographic images was 60.1 +/- 7.1 degrees from the median, with the syringe end lying on the contralateral mandibular first molar, and the insertion depth was approximately 10 mm. We applied the anterior technique to 100 patients for mandibular molar extraction and assessed the anesthetic effects. A success rate of 74% was obtained. This is similar to that reported for the conventional technique but without the accompanying risks for inferior alveolar neural and vascular complications. (+info)Links between anaesthetic modality and nerve damage during lower third molar surgery. (3/58)
OBJECTIVE: To investigate the relationships between eruption status, gender, social class, grade of operator, anaesthetic modality and nerve damage during third molar surgery. DESIGN: Two centre prospective longitudinal study. SETTING: The department of oral and maxillofacial surgery, University Hospital Birmingham NHS Trust and oral surgery outpatient clinics at Birmingham Dental Hospital. SUBJECTS: A total of 391 patients had surgical removal of lower third molars. Sensory disturbance was recorded at one week post operatively. Patients with altered sensation were followed up at one month, three months and six months following surgery. RESULTS: 614 lower third molars in 391 patients were removed. Forty-six procedures (7.5%) were associated with altered sensation at one week with three procedures (0.49%) showing persistent symptoms at six months. Of these 46 nerve injuries, 26 (4.23%) involved the lingual nerve and 20 (3.25%) the inferior dental nerve (IDN). All three persistent sensations were IDN related. A logistic regression model found that the use ofa lingual retractor chi2 = 11.559, p = 0.003 was more significant than eruption status chi2 = 12.935, p = 0.007. There was no significant relationship between anaesthetic modality, age, social class, sex and seniority of operator. CONCLUSIONS: There was no link between the choices of local or general anaesthesia and nerve damage during lower third molar removal when difficulty of surgery was taken into account. (+info)Reconstruction of the inferior alveolar nerve by autologous graft: a retrospective study of 20 cases examining donor nerve length. (4/58)
The purpose of this study was to confirm the length and kind of donor nerves used in nerve grafts for reconstruction of inferior alveolar nerve defects. The authors conducted a retrospective study of surgeries that were performed between 1977 and 1996. A total of 20 patients underwent nerve grafting procedures during this period. The greater auricular nerve was selected as the donor nerve in 16 cases, while the sural nerve was selected in 4. Mean lengths of donor nerves were 7.28 +/- 1.6 cm and 11.5 +/- 3.4 cm for the greater auricular and sural nerves, respectively. As indicated, the sural nerves were significantly longer (p < 0.01). Mean lengths of donor nerves grafted for partial resection and hemi-mandibulectomy were 7.23 +/- 1.6 cm and 10.8 +/- 3.4 cm, respectively. Statistical analysis indicated that grafts used in the hemi-mandibulectomy group were significantly longer (p < 0.05). In terms of types of donor nerve used in mandibulectomies, the greater auricular nerve was used in the majority of partial resections, and the sural nerve was employed for hemi-mandibulectomy. (+info)MR imaging of traumatic lesions of the inferior alveolar nerve in patients with fractures of the mandible. (5/58)
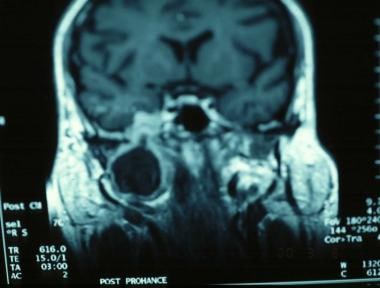
BACKGROUND AND PURPOSE: The objective of this study was to assess whether MR imaging can image the neurovascular bundle in patients with fractures of the mandible. In addition, an attempt was made to evaluate whether MR images provide information regarding the continuity of the inferior alveolar nerve before surgery and regarding signal intensity changes after trauma. METHODS: We analyzed preoperative MR images of 23 patients with mandibular fractures. Object-oriented sagittal view proton density- and T1-weighted sequences (before and after the administration of contrast agent) were used not only in an attempt to obtain purely qualitative information regarding nerve continuity in the neurovascular bundle (inferior alveolar nerve, artery, vein) but also to perform quantitative region-of-interest measurements of signal intensities at four defined measurement sites. The measurements were compared with those obtained for a patient population with healthy mandibles. RESULTS: It was possible to interpret MR images in 21 cases. MR imaging findings showed that the neurovascular bundle had been cut in two patients and was intact in the remaining 19 patients. These MR imaging findings were confirmed intraoperatively in all cases. Although we found no significant signal intensity differences between patients with intact nerves and patients with cut nerves, we found significant differences between patients with mandibular fractures and patients with unremarkable mandibles. CONCLUSION: It is possible to diagnose the interruption of nerve continuity by using MR imaging. Signal intensity measurements in the neurovascular bundle provide no information regarding nerve continuity. (+info)Inferior alveolar nerve paresthesia relieved by microscopic endodontic treatment. (6/58)
We experienced two cases of inferior alveolar nerve paresthesia caused by root canal medicaments, which were successfully relieved by microscopic endodontic treatment. In the first case, the paresthesia might have been attributable to infiltration of calcium hydroxide into the mandibular canal through the root canals of the mandibular left second molar tooth. In the second case, the paresthesia might have been attributable to infiltration of paraformaldehyde through the root canals of the mandibular right second molar tooth. The paresthesia was relieved in both cases by repetitive microscopic endodontic irrigation using physiological saline solution in combination with oral vitamin B12 and adenosine triphosphate. (+info)Inferior alveolar nerve injury caused by thermoplastic gutta-percha overextension. (7/58)
Injuries to the inferior alveolar nerve following trauma resulting in a mandibular fracture are well documented and are a well-known risk when surgical procedures are planned for the mandible in the region of the inferior alveolar canal. Such injuries are relatively rare following endodontic therapy. This article reports a case of combined thermal and pressure injury to the inferior alveolar nerve, reviews the pathogenesis of such an injury and makes suggestions for its management. (+info)Iatrogenic paresthesia in the third division of the trigeminal nerve: 12 years of clinical experience. (8/58)
BACKGROUND: Iatrogenic paresthesia in the third division of the trigeminal nerve remains a complex clinical problem with major medicolegal implications. However, most lawsuits can be prevented through better planning of procedures and by obtaining informed consent. The purpose of this article is to present the authors" clinical experience over the past 12 years, to review the principles of prevention and management of trigeminal paresthesia and to highlight the resulting medicolegal implications. METHODS: The files of all 165 patients referred to the oral and maxillofacial surgery department for evaluation of iatrogenic paresthesia in the third division of the trigeminal nerve were reviewed. The characteristics of the subgroup of patients who had taken an attending dentist to court were compared with those of the other patients. RESULTS: Surgical extraction of impacted molars was the main cause of paresthesia in 109 (66%) of the 165 subjects. The alveolar nerve was affected in 89 (54%) subjects, the lingual nerve in 67 (41%) subjects, and both nerves were affected in 9 (5%) subjects. There were more female than male patients (ratio 2.2:1). Lawsuits were initiated in 33 (20%) of the cases; patients who initiated lawsuits were younger, were more likely to have experienced anesthesia and were more likely to need microsurgery (all p < 0.001). Poor surgical planning and lack of informed consent were the most common errors on the part of the dentists. CONCLUSIONS: An accurate evaluation of surgical indications and risk, good surgical technique, preoperative informed consent and sufficient postoperative follow-up should help to reduce the frequency of neurosensory deficits after dental treatment and attendant lawsuits. (+info)Trigeminal nerve injuries refer to damages or traumas affecting the trigeminal nerve, also known as the fifth cranial nerve. This nerve is responsible for sensations in the face and motor functions such as biting and chewing. Trigeminal nerve injuries can result in various symptoms depending on the severity and location of the injury, including:
1. Loss or reduction of sensation in the face, lips, gums, teeth, or tongue.
2. Pain, often described as burning, aching, or stabbing, in the affected areas.
3. Numbness or tingling sensations.
4. Difficulty with biting, chewing, or performing other motor functions.
5. Impaired taste sensation.
6. Headaches or migraines.
7. Eye dryness or excessive tearing.
Trigeminal nerve injuries can occur due to various reasons, such as trauma during facial surgeries, accidents, tumors, infections, or neurological conditions like multiple sclerosis. Treatment options depend on the cause and severity of the injury and may include medication, physical therapy, surgical intervention, or pain management strategies.
Trigeminal neuralgia is a chronic pain condition that affects the trigeminal nerve, which is one of the largest nerves in the head. It carries sensations from the face to the brain.
Medically, trigeminal neuralgia is defined as a neuropathic disorder characterized by episodes of intense, stabbing, electric shock-like pain in the areas of the face supplied by the trigeminal nerve (the ophthalmic, maxillary, and mandibular divisions). The pain can be triggered by simple activities such as talking, eating, brushing teeth, or even touching the face lightly.
The condition is more common in women over 50, but it can occur at any age and in either gender. While the exact cause of trigeminal neuralgia is not always known, it can sometimes be related to pressure on the trigeminal nerve from a nearby blood vessel or other causes such as multiple sclerosis. Treatment typically involves medications, surgery, or a combination of both.
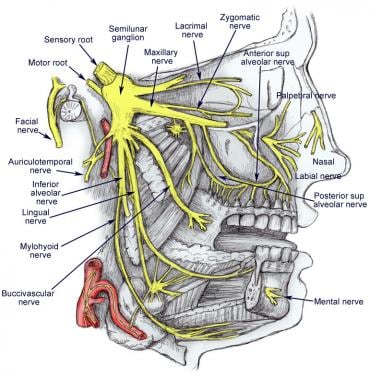
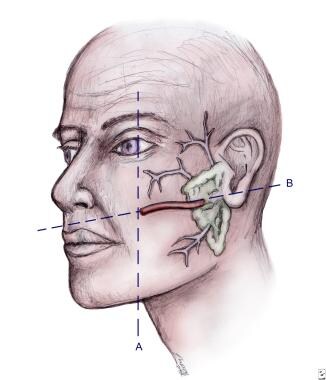
The trigeminal nerve, also known as the fifth cranial nerve or CNV, is a paired nerve that carries both sensory and motor information. It has three major branches: ophthalmic (V1), maxillary (V2), and mandibular (V3). The ophthalmic branch provides sensation to the forehead, eyes, and upper portion of the nose; the maxillary branch supplies sensation to the lower eyelid, cheek, nasal cavity, and upper lip; and the mandibular branch is responsible for sensation in the lower lip, chin, and parts of the oral cavity, as well as motor function to the muscles involved in chewing. The trigeminal nerve plays a crucial role in sensations of touch, pain, temperature, and pressure in the face and mouth, and it also contributes to biting, chewing, and swallowing functions.
Trigeminal nerve diseases refer to conditions that affect the trigeminal nerve, which is one of the cranial nerves responsible for sensations in the face and motor functions such as biting and chewing. The trigeminal nerve has three branches: ophthalmic, maxillary, and mandibular, which innervate different parts of the face and head.
Trigeminal nerve diseases can cause various symptoms, including facial pain, numbness, tingling, or weakness. Some common trigeminal nerve diseases include:
1. Trigeminal neuralgia: A chronic pain condition that affects the trigeminal nerve, causing intense, stabbing, or electric shock-like pain in the face.
2. Hemifacial spasm: A neuromuscular disorder that causes involuntary muscle spasms on one side of the face, often affecting the muscles around the eye and mouth.
3. Trigeminal neuropathy: Damage or injury to the trigeminal nerve, which can result in numbness, tingling, or weakness in the face.
4. Herpes zoster oticus (Ramsay Hunt syndrome): A viral infection that affects the facial nerve and geniculate ganglion of the trigeminal nerve, causing facial paralysis, ear pain, and a rash around the ear.
5. Microvascular compression: Compression of the trigeminal nerve by a blood vessel, which can cause symptoms similar to trigeminal neuralgia.
Treatment for trigeminal nerve diseases depends on the specific condition and its severity. Treatment options may include medication, surgery, or radiation therapy.
Peripheral nerve injuries refer to damage or trauma to the peripheral nerves, which are the nerves outside the brain and spinal cord. These nerves transmit information between the central nervous system (CNS) and the rest of the body, including sensory, motor, and autonomic functions. Peripheral nerve injuries can result in various symptoms, depending on the type and severity of the injury, such as numbness, tingling, weakness, or paralysis in the affected area.
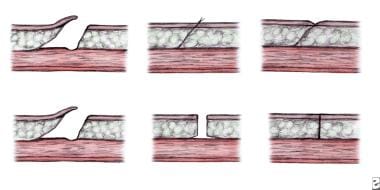
Peripheral nerve injuries are classified into three main categories based on the degree of damage:
1. Neuropraxia: This is the mildest form of nerve injury, where the nerve remains intact but its function is disrupted due to a local conduction block. The nerve fiber is damaged, but the supporting structures remain intact. Recovery usually occurs within 6-12 weeks without any residual deficits.
2. Axonotmesis: In this type of injury, there is damage to both the axons and the supporting structures (endoneurium, perineurium). The nerve fibers are disrupted, but the connective tissue sheaths remain intact. Recovery can take several months or even up to a year, and it may be incomplete, with some residual deficits possible.
3. Neurotmesis: This is the most severe form of nerve injury, where there is complete disruption of the nerve fibers and supporting structures (endoneurium, perineurium, epineurium). Recovery is unlikely without surgical intervention, which may involve nerve grafting or repair.
Peripheral nerve injuries can be caused by various factors, including trauma, compression, stretching, lacerations, or chemical exposure. Treatment options depend on the type and severity of the injury and may include conservative management, such as physical therapy and pain management, or surgical intervention for more severe cases.
Cranial nerve neoplasms refer to abnormal growths or tumors that develop within or near the cranial nerves. These nerves are responsible for transmitting sensory and motor information between the brain and various parts of the head, neck, and trunk. There are 12 pairs of cranial nerves, each with a specific function and location in the skull.
Cranial nerve neoplasms can be benign or malignant and may arise from the nerve itself (schwannoma, neurofibroma) or from surrounding tissues that invade the nerve (meningioma, epidermoid cyst). The growth of these tumors can cause various symptoms depending on their size, location, and rate of growth. Common symptoms include:
* Facial weakness or numbness
* Double vision or other visual disturbances
* Hearing loss or tinnitus (ringing in the ears)
* Difficulty swallowing or speaking
* Loss of smell or taste
* Uncontrollable eye movements or drooping eyelids
Treatment for cranial nerve neoplasms depends on several factors, including the type, size, location, and extent of the tumor, as well as the patient's overall health. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence or complications.
The sciatic nerve is the largest and longest nerve in the human body, running from the lower back through the buttocks and down the legs to the feet. It is formed by the union of the ventral rami (branches) of the L4 to S3 spinal nerves. The sciatic nerve provides motor and sensory innervation to various muscles and skin areas in the lower limbs, including the hamstrings, calf muscles, and the sole of the foot. Sciatic nerve disorders or injuries can result in symptoms such as pain, numbness, tingling, or weakness in the lower back, hips, legs, and feet, known as sciatica.
Cranial nerve injuries refer to damages or trauma to one or more of the twelve cranial nerves (CN I through CN XII). These nerves originate from the brainstem and are responsible for transmitting sensory information (such as vision, hearing, smell, taste, and balance) and controlling various motor functions (like eye movement, facial expressions, swallowing, and speaking).
Cranial nerve injuries can result from various causes, including head trauma, tumors, infections, or neurological conditions. The severity of the injury may range from mild dysfunction to complete loss of function, depending on the extent of damage to the nerve. Treatment options vary based on the type and location of the injury but often involve a combination of medical management, physical therapy, surgical intervention, or rehabilitation.
A lingual nerve injury refers to damage or trauma to the lingual nerve, which is a branch of the mandibular nerve (itself a branch of the trigeminal nerve). The lingual nerve provides sensation to the anterior two-thirds of the tongue and the floor of the mouth. It also contributes to taste perception on the front two-thirds of the tongue through its connection with the chorda tympani nerve.
Lingual nerve injuries can result from various causes, such as surgical procedures (e.g., dental extractions, implant placements, or third molar surgeries), pressure from tumors or cysts, or direct trauma to the mouth and tongue area. The injury may lead to symptoms like numbness, altered taste sensation, pain, or difficulty speaking and swallowing. Treatment for lingual nerve injuries typically involves a combination of symptom management and possible surgical intervention, depending on the severity and cause of the injury.
The maxillary nerve, also known as the second division of the trigeminal nerve (cranial nerve V2), is a primary sensory nerve that provides innervation to the skin of the lower eyelid, side of the nose, part of the cheek, upper lip, and roof of the mouth. It also supplies sensory fibers to the mucous membranes of the nasal cavity, maxillary sinus, palate, and upper teeth. Furthermore, it contributes motor innervation to the muscles involved in chewing (muscles of mastication), specifically the tensor veli palatini and tensor tympani. The maxillary nerve originates from the trigeminal ganglion and passes through the foramen rotundum in the skull before reaching its target areas.
Hypoglossal nerve injuries refer to damages or impairments to the twelfth cranial nerve, also known as the hypoglossal nerve. This nerve is primarily responsible for controlling the movements of the tongue.
An injury to this nerve can result in various symptoms, depending on the severity and location of the damage. These may include:
1. Deviation of the tongue to one side when protruded (usually away from the side of the lesion)
2. Weakness or paralysis of the tongue muscles
3. Difficulty with speaking, swallowing, and articulation
4. Changes in taste and sensation on the back of the tongue (in some cases)
Hypoglossal nerve injuries can occur due to various reasons, such as trauma, surgical complications, tumors, or neurological disorders like stroke or multiple sclerosis. Treatment for hypoglossal nerve injuries typically focuses on managing symptoms and may involve speech and language therapy, exercises to strengthen the tongue muscles, and, in some cases, surgical intervention.
Optic nerve injuries refer to damages or trauma inflicted on the optic nerve, which is a crucial component of the visual system. The optic nerve transmits visual information from the retina to the brain, enabling us to see. Injuries to the optic nerve can result in various visual impairments, including partial or complete vision loss, decreased visual acuity, changes in color perception, and reduced field of view.
These injuries may occur due to several reasons, such as:
1. Direct trauma to the eye or head
2. Increased pressure inside the eye (glaucoma)
3. Optic neuritis, an inflammation of the optic nerve
4. Ischemia, or insufficient blood supply to the optic nerve
5. Compression from tumors or other space-occupying lesions
6. Intrinsic degenerative conditions affecting the optic nerve
7. Toxic exposure to certain chemicals or medications
Optic nerve injuries are diagnosed through a comprehensive eye examination, including visual acuity testing, slit-lamp examination, dilated fundus exam, and additional diagnostic tests like optical coherence tomography (OCT) and visual field testing. Treatment options vary depending on the cause and severity of the injury but may include medications, surgery, or vision rehabilitation.
Peripheral nerves are nerve fibers that transmit signals between the central nervous system (CNS, consisting of the brain and spinal cord) and the rest of the body. These nerves convey motor, sensory, and autonomic information, enabling us to move, feel, and respond to changes in our environment. They form a complex network that extends from the CNS to muscles, glands, skin, and internal organs, allowing for coordinated responses and functions throughout the body. Damage or injury to peripheral nerves can result in various neurological symptoms, such as numbness, weakness, or pain, depending on the type and severity of the damage.
The ophthalmic nerve, also known as the first cranial nerve or CN I, is a sensory nerve that primarily transmits information about vision, including light intensity and color, and sensation in the eye and surrounding areas. It is responsible for the sensory innervation of the upper eyelid, conjunctiva, cornea, iris, ciliary body, and nasal cavity. The ophthalmic nerve has three major branches: the lacrimal nerve, frontal nerve, and nasociliary nerve. Damage to this nerve can result in various visual disturbances and loss of sensation in the affected areas.
 Central chromatolysis
Central chromatolysis
Tensor veli palatini muscle
Zygomatic branches of the facial nerve
Supratrochlear nerve
Impacted wisdom teeth
Trigeminal nerve
Inferior alveolar nerve
Supraclavicular nerves
Cavernous sinus
Trigeminal neuralgia
List of neuromuscular disorders
Neurological disorder
Lesser occipital nerve
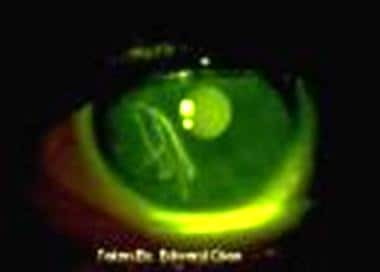
Cornea
Mosasaurus
Neurotrophic keratitis
Dental extraction
Headshaking
Epidural hematoma
Heterochromia iridum
Orbital blowout fracture
Harrison's Principles of Internal Medicine
Marcus Gunn phenomenon
Orofacial pain
Olfactory nerve
Peter J. Jannetta
Horse pain caused by the bit
Dysarthria
Hypoglossal nerve
William F. Windle
Ophthalmic division1
- The cornea is innervated primarily by the ophthalmic division of the trigeminal nerve and the oculomotor nerve. (medscape.com)
Cranial nerves3
- How long does it take for cranial nerves to heal? (greatgreenwedding.com)
- What do cranial nerves 9 and 10 do? (greatgreenwedding.com)
- The trigeminal nerve is the largest and most complex of the 12 cranial nerves (CNs). (medscape.com)
Mandibular7
- The mandibular nerve has sensory and motor functions. (medscape.com)
- It is characterized by unilateral pain following the sensory distribution of cranial nerve V (typically radiating to the maxillary or mandibular area in 35% of affected patients) and is often accompanied by a brief facial spasm or tic. (medscape.com)
- The aim of this study is to report a case of a 21-year-old patient, diagnosed with zoster, with commitment of the trigeminal nerve comprehending the ophthalmic, maxillary and mandibular branches. (bvsalud.org)
- The trigeminal nerve has three branches-ophthalmic, maxillary and mandibular-that together carry sensory information to or from the eye, check and jaw. (montefiore.org)
- The semilunar (gasserian or trigeminal) ganglion is the great sensory ganglion of CN V. It contains the sensory cell bodies of the 3 branches of the trigeminal nerve (the ophthalmic, mandibular, and maxillary divisions). (medscape.com)
- The motor root passes under the ganglion to join the sensory division of the mandibular nerve and exits the skull through foramen ovale. (medscape.com)
- A neurologic examination found diminished sensation to light touch over the distribution of her left trigeminal mandibular nerve. (cdc.gov)
Treating trigeminal neuralgia2
- Mayo Clinic doctors trained in brain and nervous system conditions (neurologists), brain and nervous system surgery (neurosurgeons), brain imaging (neuroradiology), and dental specialties have extensive experience diagnosing and treating trigeminal neuralgia. (greatgreenwedding.com)
- Glycerol is a mild neurolytic agent used for treating trigeminal neuralgia but may cause perineural damage. (medscape.com)
Ganglion4
- The trigeminal nerve ganglion (also referred to as the gasserian ganglion) lies in the trigeminal cave (also known as the Meckel cave), which is a dural invagination in the petrous part of the temporal bone. (medscape.com)
- This ganglion is formed by 2 roots that exit the ventral surface of the brainstem at the midpontine level and travel forwards and laterally to enter the trigeminal cave. (medscape.com)
- The dural pouch (trigeminal cistern) contains cerebrospinal fluid (CSF) and lies behind the ganglion. (medscape.com)
- The indications for gasserian ganglion block for trigeminal neuralgia. (medscape.com)
Damage12
- GM-CSF is also involved in bone cancer pain development by regulating tumor-nerve interactions, remodeling of peripheral nerves and sensitization of damage-sensing (nociceptive) nerves. (iasp-pain.org)
- Nerve damage from past injuries or facial surgery. (thenassauguardian.com)
- The body has limited ability to repair damage to the vestibular organs, although the body can often recover from vestibular injury by having the part of the brain that controls balance recalibrate itself to compensate. (greatgreenwedding.com)
- What causes damage to the 8th cranial nerve? (greatgreenwedding.com)
- How do you test for vagus nerve damage? (greatgreenwedding.com)
- Can auditory nerve damage be repaired? (greatgreenwedding.com)
- Gloria retained the services of attorney Relinda Louisy and brought a lawsuit against Dr. Mehrabian and his center for medical malpractice, dental malpractice, oral surgery malpractice, surgical error, negligent treatment, and nerve damage . (cohenandcohen.net)
- They also pointed out Gloria's complaints of numbness and pain decreased following the surgery, and claimed that Gloria had visited numerous dental specialists before finding one who would back up her claims of suffering nerve damage. (cohenandcohen.net)
- Neuralgia is a type of pain that's caused by a nerve problem, and neuropathy is a type of nerve damage. (healthline.com)
- Many people with diabetes have issues with their nerves, including neuralgia and neuropathy (nerve damage). (healthline.com)
- The excess glucose in the bloodstream may damage nerves . (healthline.com)
- With damage to the spinal and cervical nerves, neuritis of the shoulder occurs. (lonestarneurology.net)
Fibers7
- The postganglionic fibers are the sensory nerves to the face and exit via various foramina at the base of the skull. (medscape.com)
- More specifically, this invention relates to an implantable medical electrical lead having at least one stimulation electrode adapted to be implanted near the sacral nerves for stimulation of a bundle of sacral nerve fibers and a fixation mechanism for providing chronic stability of the stimulation electrode and lead. (justia.com)
- The glossopharyngeal nerve receives input from the general and special sensory fibers in the back of the throat. (greatgreenwedding.com)
- They achieve this by causing destruction of nerve fibers and wallerian degeneration of axonal fibers and Schwann cells. (medscape.com)
- It is the motor nerve for the muscles of mastication and contains proprioceptive fibers. (medscape.com)
- Usually, pain is felt when a stimulus, such as a pinch or an injury, causes electrical pulses to run along one of the cables of nerve fibers in our body and into the. (researchgate.net)
- The electrical stimuli on the skin preferentially activate low-threshold, myelinated nerve fibers. (medscape.com)
Anatomy1
- For more information about the relevant anatomy, see Trigeminal Nerve Anatomy . (medscape.com)
Douloureux1
- Trigeminal neuralgia (TN), also known as tic douloureux, is a distinctive facial pain syndrome that may become recurrent and chronic. (medscape.com)
Compression6
- Occasionally, tumor infiltration, vascular compression of the nerve, or diseases such as multiple sclerosis may be the causative factors. (medscape.com)
- Even the site of injury may impact underlying mechanisms, as indicated by the clinical finding that the antiseizure drug carbamazepine (CBZ) relieves pain because of compression injuries of trigeminal but not somatic nerves. (bvsalud.org)
- Compression or pressure on the trigeminal nerve. (thenassauguardian.com)
- 13. Ultrasound nerve compression in the elbow region. (klinika.lv)
- Pressure or compression of nerves may cause neuralgia. (healthline.com)
- Nerve related symptoms might occur as a result of nerve compression, trauma, inflammation, poor diets, lack of exercise, and also conditions such as diabetes, arthritis and others. (greenorganicsupplements.com)
Neuropathic pain2
- Different peripheral nerve injuries cause neuropathic pain through distinct mechanisms. (bvsalud.org)
- Our results suggest a novel therapeutic target for the treatment of trigeminal neuropathic pain .SIGNIFICANCE STATEMENT This study is based on evidence of differences in pain and its treatment depending on whether the pain is above (trigeminal) or below (somatic) the neck , as well as evidence that voltage-gated sodium channels (VGSCs) may contribute to these differences. (bvsalud.org)
Sensory4
- The trigeminal nerve is the fifth cranial nerve and supplies sensory innervations to the face via its branches (see the image below). (medscape.com)
- The ophthalmic and maxillary nerves are purely sensory. (medscape.com)
- Concentrations of 95% will reliably lyze sympathetic, sensory, and motor components of a nerve. (medscape.com)
- The trigeminal nerve is a type of sensory nerve. (healthline.com)
Commonly3
- The anti-convulsant drug most commonly prescribed for trigeminal neuralgia is carbamazepine (Tegretol), which can provide at least partial pain relief for up to 80 to 90 percent of patients. (greatgreenwedding.com)
- Transcutaneous electrical nerve stimulation (TENS) currently is one of the most commonly used forms of electroanalgesia. (medscape.com)
- Most attention has been devoted to the inferior alveolar nerve and lingual nerve as these nerves are commonly involved in routine dental procedures such as anesthetics block, root canal therapy, dental implant surgery and surgical removal of third molars or wisdom tooth. (iium.edu.my)
Infraorbital4
- CBZ diminished ongoing and evoked pain behavior in rats with chronic constriction injury (CCI) to the infraorbital nerve (ION) but had minimal effect in rats with sciatic nerve CCI. (bvsalud.org)
- The infraorbital nerve is a branch of the maxillary division of the trigeminal nerve . (radiopaedia.org)
- The infraorbital nerve divides off the maxillary division in the pterygopalatine fossa just after it gives off the the posterior superior alveolar nerve . (radiopaedia.org)
- Behavioral evidence of trigeminal pain following chronic constriction injury to the rat s infraorbital nerve. (bvsalud.org)
Pain22
- Trigeminal neuralgia is characterized by spontaneous, paroxysmal lancinating pain in the trigeminal nerve distribution. (medscape.com)
- Mechanisms Underlying the Selective Therapeutic Efficacy of Carbamazepine for Attenuation of Trigeminal Nerve Injury Pain. (bvsalud.org)
- Importantly, because the local block of NaV1.1 in the trigeminal nerve reverses nerve injury -induced mechanical hypersensitivity , the selective upregulation of NaV1.1 in trigeminal nerves suggests a novel therapeutic target for the treatment of pain associated with trigeminal nerve injury . (bvsalud.org)
- Other fairly common causes of facial pain include nerve conditions, jaw issues and other infections. (thenassauguardian.com)
- Pain caused by trigeminal neuralgia is considered one of the worst pains known to mankind. (thenassauguardian.com)
- The nerve becomes irritated and fires uncontrollably resulting in excruciating pain on one side of the face. (thenassauguardian.com)
- It is not until a definite diagnosis is made will the patient learn that the source of the pain is the fifth cranial nerve. (thenassauguardian.com)
- The nature and localization of pain directly depends on the type of injury. (ecureme.com)
- The jaw is one of the most used joints in the human body, and it makes sense for it to have wear and tear, overuse, injuries, and pain. (todaysrdh.com)
- Many people find relief from trigeminal neuralgia pain by applying heat to the affected area. (greatgreenwedding.com)
- Trigeminal nerve injuries not only causes significant neurosensory deficits and facial pain, but can cause significant comorbidities due to changes in eating habits from muscular denervation of masticator muscles or altered sensation of the oral mucosa. (greatgreenwedding.com)
- This makes the nerve transmit pain signals that are experienced as stabbing pains. (greatgreenwedding.com)
- Trigeminal neuralgia is a disorder that produces pain in one or more of these three areas. (montefiore.org)
- Clinical opinion discourages surgical resection of nerves proximal to the original injury site for fear of resurgence of ectopia and exacerbated pain. (researchgate.net)
- Neuralgia is a type of pain caused by a nerve that's irritated or damaged. (healthline.com)
- Neuralgia is a stabbing, burning, and often severe pain due to a nerve that's irritated or damaged. (healthline.com)
- For example, if you have an infection in a tooth, it may affect the nerve and cause pain. (healthline.com)
- Trigeminal neuralgia causes severe, recurrent pain in the face, usually on one side. (healthline.com)
- Because the pain always occurs along the path of a nerve , it's usually isolated to one side of the body. (healthline.com)
- Pain from the glossopharyngeal nerve , which is located in the throat, isn't very common. (healthline.com)
- Usually, the electrodes are initially placed on the skin over the painful area, but other locations (eg, over cutaneous nerves, trigger points, acupuncture sites) may give comparable or even better pain relief. (medscape.com)
- Neuropathy Pain Reliever a natural supplement for neuropathy is a natural formula to control symptoms of numbness, tingling, burning, nerve pain, pins and needles and peripheral neuropathy. (greenorganicsupplements.com)
Blood vessels3
- Her MRI revealed blood vessels that were close to the trigeminal nerve, and I was confident that in this situation an MVD would be a better option than radiation. (mayfieldclinic.com)
- The main cause of trigeminal neuralgia is blood vessels pressing on the root of the trigeminal nerve. (greatgreenwedding.com)
- Epinephrine prolongs the duration of the anesthetic effects from bupivacaine by causing vasoconstriction of the blood vessels surrounding the nerve axons. (medscape.com)
Surgical7
- With each athlete, physicians should obtain an ocular history, paying special attention to prior conditions such as a high degree of myopia, surgical aphakia, retinal detachment, eye surgery, and injury or infection. (aafp.org)
- neurological injury often occurs to the trigeminal nerve as well as facial nerve caused by trauma, pathology, infection, inflammatory, and other orofacial surgical procedures. (iium.edu.my)
- Various surgical and non-surgical options are available to treat the above said conditions in order to allow repair and regeneration of the peripheral branches of facial and trigeminal nerves so as to improve the quality of life for patients. (iium.edu.my)
- Non-surgical treatment is used as means to facilitate faster nerve end growth or axonal regeneration such as protein therapy, laser phototherapy and low frequency electric stimulation therapy. (iium.edu.my)
- Surgical treatment of brachial nerve inflammation can achieve effective results. (lonestarneurology.net)
- Treatment, when required, may involve decongestants, analgesics, and sometimes oral corticosteroids or surgical repair of serious inner or middle ear or sinus injuries. (msdmanuals.com)
- This narrative review describes the main applications of de la ultrasonografía en ultrasound in anesthesia, ultrasound-guided techniques, and current trends in the perioperative anesthetic management of anestesia the surgical patient. (bvsalud.org)
Glossopharyngeal nerve1
- The glossopharyngeal nerve (cranial nerve IX) is responsible for swallowing and the gag reflex, along with other functions. (greatgreenwedding.com)
Trauma3
- The most common mechanisms of eye trauma involve blunt, penetrating, and radiation injuries. (aafp.org)
- Blunt trauma accounts for most sports-related eye injuries. (aafp.org)
- The nerve of the tooth is damaged by trauma or bacterial infection caused by a cavity. (thenassauguardian.com)
Vestibulocochlear2
- What happens if the Vestibulocochlear nerve is damaged? (greatgreenwedding.com)
- The vestibulocochlear nerve sends balance and head position information from the inner ear (see left box) to the brain. (greatgreenwedding.com)
Traumatic Brain1
- Problems rooted in your brain, such as traumatic brain injury. (greatgreenwedding.com)
Abducens1
- My Trigeminal, Facial, Abducens and Vestibular cochlear nerve was badly damaged. (varunaraina.com)
20191
- Kayla felt her first stab of trigeminal neuralgia in the spring of 2019 while working her shift in a hospital emergency department. (mayfieldclinic.com)
Dura1
- Repeat brain and spine MRI revealed new enhancement of the dura, trigeminal nerve, and cauda equina, indicative of a central infiltrative process. (cdc.gov)
20231
- col. 1, line 45, through col. 5, line 44, which is focused on medical problems addressable by Case: 22-1451 AXONICS, INC. Document: 46 v. MEDTRONIC, INC. Page: 3 Filed: 07/10/2023 3 electrical stimulation of the sacral nerves, e.g., id. (justia.com)
Branch1
- Maxillary sinus overpressurization can compress the maxillary branch of the trigeminal nerve, causing hyperesthesia over the cheek. (msdmanuals.com)
Branches3
- The trigeminal nerve and its peripheral branches are susceptible to injury in the practice. (dentistrytoday.com)
- It receives ordinary sensations from the main 3 branches of the trigeminal. (medscape.com)
- The branches of this nerve merge and then travel from the face to the brain . (healthline.com)
Fractures1
- nerve is at risk of injury with orbital blowout fractures . (radiopaedia.org)
Vagus nerve2
- To test the vagus nerve, a doctor may check the gag reflex. (greatgreenwedding.com)
- If the person doesn't gag, this may be due to a problem with the vagus nerve. (greatgreenwedding.com)
Lower jaw1
- A dentist she visited three years later informed her that there could be a possible disturbance of her trigeminal nerve in the lower jaw, resulting in permanent numbness around the site. (cohenandcohen.net)
Brachial1
- The diagnosis, in most cases, is eminently clinical, usually determined by vesicle-bullous lesions involving the skin over the brachial nerve pathway. (bvsalud.org)
Disorders2
- The most common in a family of disorders, trigeminal neuralgia is caused by spontaneous, nontraumatic injury to a cranial nerve. (montefiore.org)
- Various diseases and injuries, including diseases associated with metabolic disorders, lead to this type of pathology development. (lonestarneurology.net)
Occurs1
- It is a localized acute musculoskeletal disorder that occurs from a traumatic or mechanical injury. (todaysrdh.com)
Multiple sclerosis1
- Pressure on this nerve may also be caused by a tumor or multiple sclerosis (MS). (greatgreenwedding.com)
Involves1
- Modern treatment of inflammation of the optic nerves involves the use of anti-inflammatory drugs and antibiotics. (lonestarneurology.net)
Infection3
- An infection , such as shingles , can affect your nerves. (healthline.com)
- An infection in a specific part of the body may also affect a nearby nerve. (healthline.com)
- Furthermore, temporal artery biopsy is associated with several complications and risks, such as injury to the facial nerve and the trigeminal nerve, peri- and postoperative hemorrhage, wound infection, scarring, and skin necrosis. (lu.se)
Skull2
- During surgery at The Jewish Hospital - Mercy Health, Dr. Gozal accessed the trigeminal nerve through a one-inch opening in Kayla's skull behind her right ear. (mayfieldclinic.com)
- The accident resulted in serious injuries, including a broken rib, a broken jaw, broken cheekbones, a fractured skull, and a ruptured left eye. (allenandallen.com)
Superficial1
- Minor and superficial nerve injuries will often heal themselves. (greatgreenwedding.com)
Treatment4
- Trigeminal nerve block provides hemifacial anesthesia and is used predominantly in the diagnosis and treatment of neuralgia. (medscape.com)
- trigeminal nerve block is reserved for patients who do not respond to medical treatment or patients in whom neurologic decompression of the canal is not feasible or has failed. (medscape.com)
- What is the most effective treatment for trigeminal neuralgia? (greatgreenwedding.com)
- There are also several different topical herbal plasters Dr. Wilson uses in her treatment to assist with acute injuries. (rootsacu.com)
Regeneration1
- This presentation attempts to discuss the use of different options of nerve regeneration therapy and its relevance in the field of oral and maxillofacial surgery. (iium.edu.my)