Trochlear Nerve
Trochlear Nerve Diseases
Optic Nerve Diseases
Abducens Nerve
Olfactory Nerve Diseases
Vagus Nerve Diseases
Cranial Nerve Diseases
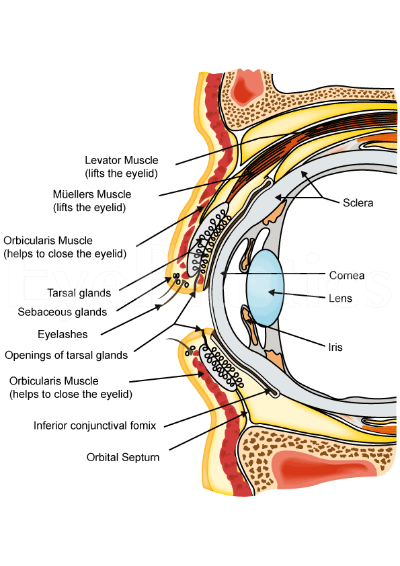
Ophthalmic Nerve
Diplopia
Cranial Sinuses
Tolosa-Hunt Syndrome
Cisterna Magna
Ophthalmoplegia
Hypoglossal Nerve Diseases
Oculomotor Muscles
Vestibulocochlear Nerve Diseases
Glossopharyngeal Nerve Diseases
Cavernous Sinus
Onchocerciasis, Ocular
Trigeminal Nerve Diseases
Accessory Nerve Diseases
Facial Nerve Diseases
Abducens Nerve Diseases
Oculomotor Nerve
Patellofemoral Joint
Neuroimaging
Oculomotor Nerve Diseases
Optic Neuritis
Mesencephalon
Sciatic Nerve
Traumatic trochlear nerve palsy following minor occipital impact--four case reports. (1/41)
Four patients presented with transient trochlear nerve palsy following occipital impact. The impact was slight in all patients, and neuroimaging found no lesions of the nerve. Three patients had delayed onset. Two patients did not complain of diplopia, but were only aware of blurred vision. In such patients, the head tilting test was useful for diagnosis. Minor occipital impact can cause trochlear nerve palsy, which requires careful neurological examinations to identify. (+info)Infundibulohypophysitis in a man presenting with diabetes insipidus and cavernous sinus involvement. (2/41)
Infundibulohypophysitis is an unusual inflammatory condition that affects the infundibulum, the pituitary stalk, and the neurohypophysis and may be part of a range that includes lymphocytic hypophysitis. Lymphocytic hypophysitis occurs mainly in women and most often presents in the later stages of pregnancy. Infundibulohypophysitis usually presents with diabetes insipidus and the cause remains unclear. The case of a 46 year old man with a 12 week history of polyuria and polydipsia is reported. Cranial diabetes insipidus was diagnosed on the basis of a water deprivation test. Initial cranial and pituitary imaging studies were normal. He subsequently developed symptoms of panhypopituitism over a period of 6-9 months and then, more acutely, developed diplopia secondary to a fourth nerve palsy. Further brain imaging studies disclosed an enhancing pituitary stalk and a left cavernous sinus lesion. An initial trial of immunosuppressive treatment did not help symptoms significantly. The diagnosis of infundibulohypophysitis was made on histological evidence. The patient was treated with prednisolone and methotrexate. At 9 months he is well, without symptoms, and the radiological abnormalities have resolved. (+info)Presigmoid transpetrosal approach for the treatment of a large trochlear nerve schwannoma--case report. (3/41)
A 61-year-old man presented with a rare, large trochlear nerve schwannoma manifesting as left-sided weakness and hypesthesia, bilateral bulbar pareses, and trochlear nerve paresis persisting for 3 months. T1-weighted magnetic resonance imaging with gadolinium revealed an intensely enhanced, well-circumscribed lesion with multicystic formation occupying the prepontine and interpeduncular cisterns and compressing the pons and midbrain with greater extension to the right. The mass was completely removed through the presigmoid transpetrosal approach with preservation of the posterior cerebral, superior cerebellar, and basilar arteries and their branches. Neuroradiological examination after 3 years demonstrated no recurrence. Enlargement of a tumor in the cisternal portion is inclined to involve and/or encase the adjacent major arteries and their branches. The presigmoid transpetrosal approach is one of the best surgical routes to remove a large trochlear nerve schwannoma safely and completely. (+info)Adaptive neural mechanism for listing's law revealed in patients with fourth nerve palsy. (4/41)
PURPOSE: During fixation and saccades, human eye movements obey Listing's law, which specifies the eye's torsional angle as a function of its horizontal and vertical position. Torsion of the eye is in part controlled by the fourth nerve. This study investigates whether the brain adapts to defective torsional control after fourth nerve palsy. METHODS: Thirteen patients with fourth nerve palsy (11 chronic, 2 acute), and 10 normal subjects were studied with scleral search coils. With the head immobile, subjects made saccades to a target that moved between straight ahead and eight eccentric positions. At each target position, fixation was maintained for 3 seconds before the next saccade. From the eye position data, we computed the plane of best fit, referred to as Listing's plane. Violations of Listing's law were quantified by computing the "thickness" of this plane, defined as the SD of the distances to the plane from the data points. RESULTS: Both the paretic and nonparetic eyes in patients with chronic fourth nerve palsy obeyed Listing's law during fixation and saccades. However, Listing's planes in both eyes had abnormal orientations, being rotated temporally, meaning the eye excyclotorted during downgaze and incyclotorted during upgaze. In contrast, the paretic eye of patients with acute fourth nerve palsy violated Listing's law during saccades. During downward saccades, transient torsional deviations moved the paretic eye out of Listing's plane. Torsional drifts returned the paretic eye to Listing's plane during subsequent fixation. CONCLUSIONS: During saccades, acute fourth nerve palsy violates Listing's law, whereas chronic palsy obeys it, indicating that neural adaptation can restore Listing's law by adjusting the innervations to the remaining extraocular muscles, even when one eye muscle remains paretic. The transient torsional deviations during downward saccades in acute palsy are attributed to pulse-step mismatch, as a result of lesions in the trochlear nerve that lead to an imbalance of phasic and tonic signals reaching the muscles. (+info)The vestibulo-ocular reflex in fourth nerve palsy: deficits and adaptation. (5/41)
The effects of fourth nerve palsy on the vestibulo-ocular reflex (VOR) had not been systematically investigated. We used the magnetic scleral search coil technique to study the VOR in patients with unilateral fourth nerve palsy during sinusoidal head rotations in yaw, pitch and roll at different frequencies. In darkness, VOR gains are reduced during incyclotorsion, depression and abduction of the paretic eye, as anticipated from paresis of the superior oblique muscle. VOR gains during excyclotorsion, elevation and adduction of the paretic eye are also reduced, whereas gains in the non-paretic eye remain normal, indicating a selective adjustment of innervation to the paretic eye. In light, torsional visually enhanced VOR (VVOR) gains in the paretic eye remain reduced; however, visual input increases vertical and horizontal VVOR gains to normal in the paretic eye, without a conjugate increase in VVOR gains in the non-paretic eye, providing further evidence of selective adaptation in the paretic eye. Motions of the eyes after fourth nerve palsy exemplify monocular adaptation of the VOR, in response to peripheral neuromuscular deficits. (+info)Primary position and listing's law in acquired and congenital trochlear nerve palsy. (6/41)
PURPOSE: In ocular kinematics, the primary position (PP) of the eye is defined by the position from which movements do not induce ocular rotations around the line of sight (Helmholtz). PP is mathematically linked to the orientation of Listing's plane. This study was conducted to determine whether PP is affected differently in patients with clinically diagnosed congenital (conTNP) and acquired (acqTNP) trochlear nerve palsy. METHODS: Patients with unilateral conTNP (n = 25) and acqTNP (n = 9) performed a modified Hess screen test. Three-dimensional eye positions were recorded with dual search coils. RESULTS: PP in eyes with acqTNP was significantly more temporal (mean: 21.2 degrees ) than in eyes with conTNP (6.8 degrees ) or healthy eyes (7.2 degrees ). In the pooled data of all patients, the horizontal location of PP significantly correlated with vertical noncomitance with the paretic eye in adduction (R = 0.59). Using a computer model, PP in acqTNP could be reproduced by a neural lesion of the superior oblique (SO) muscle. An additional simulated overaction of the inferior oblique (IO) muscle moved PP back to normal, as in conTNP. Lengthening the SO and shortening the IO muscles could also simulate PP in conTNP. CONCLUSIONS: The temporal displacement of PP in acqTNP is a direct consequence of the reduced force of the SO muscle. The reversal of this temporal displacement of PP, which occurs in some patients with conTNP, can be explained by a secondary overaction of the IO muscle. Alternatively, length changes in the SO and IO muscles, or other anatomic anomalies within the orbit, without a neural lesion, may also explain the difference in location of PP between conTNP and acqTNP. (+info)Ocular rotation axes during dynamic Bielschowsky head-tilt testing in unilateral trochlear nerve palsy. (7/41)
PURPOSE: To explain the positive Bielschowsky head-tilt (BHT) sign in unilateral trochlear nerve palsy (uTNP) by the kinematics of three-dimensional eye rotations. METHODS: Twelve patients with uTNP monocularly fixed on targets on a Hess screen were oscillated (+/- 35 degrees, 0.3 Hz) about the roll axis on a motorized turntable (dynamic BHT). Three-dimensional eye movements were recorded with dual search coils. Normal data were collected from 11 healthy subjects. RESULTS: The rotation axis of the viewing paretic or unaffected eye was nearly parallel to the line of sight. The rotation axis of the covered fellow eye, however, was tilted inward relative to the other axis. This convergence of axes increased with gaze toward the unaffected side. Over entire cycles of head roll, the rotation axis of either eye remained relatively stable in both the viewing and covered conditions. CONCLUSIONS: In patients with uTNP, circular gaze trajectories of the covered paretic or unaffected eye during dynamic BHT are a direct consequence of the nasal deviation of the rotation axis from the line of sight. This, in turn, is a geometrical result of decreased force by the superior oblique muscle (SO) of the covered paretic eye or, according to Hering's law, increased force parallel to the paretic SO in the covered unaffected eye. The horizontal incomitance of rotation axes along horizontal eye positions can be explained by the same mechanism. (+info)Transient isolated trochlear nerve palsy associated with Rathke's cleft cyst. (8/41)
We report the case of a 52-year-old woman who developed vertical diplopia of 1-days duration. Neuro-ophthalmological testing revealed left trochlear nerve palsy, and sellar MRI revealed a 1.5 cm-sized pituitary mass lesion, a Rathke's cleft cyst. The diplopia disappeared spontaneously after 6 days. (+info)The trochlear nerve, also known as the fourth cranial nerve (CN IV), is a nerve that originates in the midbrain and innervates the superior oblique muscle of the eye. This muscle helps with the downward and outward movement of the eye, playing a crucial role in controlling eye movements and maintaining binocular vision. The trochlear nerve's main function is to provide motor (efferent) innervation to the superior oblique muscle, enabling fine-tuning of eye movements during activities such as reading, writing, or driving. Damage to this nerve can result in vertical diplopia (double vision), strabismus (eye misalignment), and other visual impairments.
The trochlear nerve, also known as the fourth cranial nerve (CN IV), is responsible for controlling the movement of the eye. It innervates the superior oblique muscle, which helps in depressing and rotating the eye downwards and outwards. Trochlear nerve diseases refer to conditions that affect this nerve and impair its function, leading to symptoms such as double vision (diplopia), vertical misalignment of the eyes, and difficulty with depth perception.
Trochlear nerve diseases can be caused by various factors, including trauma, compression, inflammation, infection, or tumors. Some common conditions that affect the trochlear nerve include:
1. Trochlear nerve palsy: This is a weakness or paralysis of the trochlear nerve, which can cause vertical and torsional diplopia, especially when looking downwards or to the side. It can be congenital or acquired due to trauma, compression, or other causes.
2. Aneurysm: Aneurysms in the vicinity of the trochlear nerve can compress or damage it, leading to palsy and diplopia.
3. Meningitis: Inflammation of the meninges (the membranes surrounding the brain and spinal cord) due to infection or other causes can affect the trochlear nerve and cause palsy.
4. Multiple sclerosis (MS): This is a chronic autoimmune disease that affects the central nervous system, including the cranial nerves. MS can cause demyelination of the trochlear nerve, leading to palsy and diplopia.
5. Diabetes: People with diabetes are at risk of developing diabetic neuropathy, which can affect any peripheral nerve, including the trochlear nerve.
6. Tumors: Space-occupying lesions in the brain or skull base, such as meningiomas, schwannomas, or pituitary adenomas, can compress the trochlear nerve and cause palsy.
The diagnosis of trochlear nerve diseases involves a thorough neurological examination, including assessment of eye movements and alignment. Imaging studies such as MRI or CT scans may be ordered to identify any structural lesions causing compression or damage to the nerve. Treatment depends on the underlying cause and may involve surgical intervention, medication, or observation.
A Trochlear nerve injury, also known as Fourth cranial nerve palsy, refers to damage or dysfunction of the fourth cranial nerve (trochlear nerve). This nerve is responsible for controlling the movement of the eye's superior oblique muscle, which helps in downward and outward movement of the eye.
Trochlear nerve injuries can result in vertical diplopia (double vision), where images appear double when looking downwards or to the side. The diplopia may be worse when looking down and out, such as when walking down stairs or reading.
The injury can be caused by various factors including head trauma, increased intracranial pressure, tumors, aneurysms, or other neurological conditions. Treatment options depend on the severity and cause of the injury and may include eye patches, prism lenses, or surgical intervention in some cases.
Optic nerve diseases refer to a group of conditions that affect the optic nerve, which transmits visual information from the eye to the brain. These diseases can cause various symptoms such as vision loss, decreased visual acuity, changes in color vision, and visual field defects. Examples of optic nerve diseases include optic neuritis (inflammation of the optic nerve), glaucoma (damage to the optic nerve due to high eye pressure), optic nerve damage from trauma or injury, ischemic optic neuropathy (lack of blood flow to the optic nerve), and optic nerve tumors. Treatment for optic nerve diseases varies depending on the specific condition and may include medications, surgery, or lifestyle changes.
The abducens nerve, also known as the sixth cranial nerve (CN VI), is a motor nerve that controls the lateral rectus muscle of the eye. This muscle is responsible for moving the eye away from the midline (towards the temple) and enables the eyes to look towards the side while keeping them aligned. Any damage or dysfunction of the abducens nerve can result in strabismus, where the eyes are misaligned and point in different directions, specifically an adduction deficit, also known as abducens palsy or sixth nerve palsy.
Olfactory nerve diseases refer to conditions that affect the olfactory nerve, which is the first cranial nerve responsible for the sense of smell. These diseases can result in impaired or loss of smell (anosmia) and taste (ageusia), as well as distorted perception of smells (parosmia). The causes of olfactory nerve diseases can include trauma, infection, inflammation, neurological disorders, and exposure to certain chemicals. Some examples of specific olfactory nerve diseases include sinusitis, upper respiratory infections, head injuries, and neurodegenerative disorders such as Parkinson's disease and Alzheimer's disease. Treatment for these conditions depends on the underlying cause and may include medications, surgery, or lifestyle changes.
Vagus nerve diseases, also known as vagus nerve disorders, refer to conditions that affect the functioning of the vagus nerve. The vagus nerve is the tenth cranial nerve and extends from the brainstem to the abdomen, playing a crucial role in regulating various automatic functions of the body such as heart rate, digestion, respiratory rate, and sweating.
Diseases of the vagus nerve can result from various causes, including inflammation, infection, trauma, compression, or degeneration. Some common vagus nerve disorders include:
1. Vagus nerve dysfunction: This is a general term used to describe any abnormality in the functioning of the vagus nerve. Symptoms may vary depending on the specific functions affected but can include difficulty swallowing, hoarseness, voice changes, and abnormal heart rate or blood pressure.
2. Vagus nerve neuropathy: This is a condition that results from damage to the vagus nerve fibers. It can cause symptoms such as difficulty swallowing, voice changes, and abnormal digestive function.
3. Gastroparesis: This is a condition in which the stomach muscles fail to contract properly, leading to delayed gastric emptying. Vagus nerve dysfunction is a common cause of gastroparesis.
4. Orthostatic hypotension: This is a condition characterized by a drop in blood pressure when standing up from a sitting or lying down position. Vagus nerve dysfunction can contribute to this condition by causing an abnormal response in the heart rate and blood vessels.
5. Inflammatory disorders: Certain inflammatory conditions such as rheumatoid arthritis, lupus, and sarcoidosis can affect the vagus nerve and cause various symptoms.
Treatment for vagus nerve diseases depends on the underlying cause and may include medications, surgery, or lifestyle changes.
Cranial nerve diseases refer to conditions that affect the cranial nerves, which are a set of 12 pairs of nerves that originate from the brainstem and control various functions in the head and neck. These functions include vision, hearing, taste, smell, movement of the eyes and face, and sensation in the face.
Diseases of the cranial nerves can result from a variety of causes, including injury, infection, inflammation, tumors, or degenerative conditions. The specific symptoms that a person experiences will depend on which cranial nerve is affected and how severely it is damaged.
For example, damage to the optic nerve (cranial nerve II) can cause vision loss or visual disturbances, while damage to the facial nerve (cranial nerve VII) can result in weakness or paralysis of the face. Other common symptoms of cranial nerve diseases include pain, numbness, tingling, and hearing loss.
Treatment for cranial nerve diseases varies depending on the underlying cause and severity of the condition. In some cases, medication or surgery may be necessary to treat the underlying cause and relieve symptoms. Physical therapy or rehabilitation may also be recommended to help individuals regain function and improve their quality of life.
The ophthalmic nerve, also known as the first cranial nerve or CN I, is a sensory nerve that primarily transmits information about vision, including light intensity and color, and sensation in the eye and surrounding areas. It is responsible for the sensory innervation of the upper eyelid, conjunctiva, cornea, iris, ciliary body, and nasal cavity. The ophthalmic nerve has three major branches: the lacrimal nerve, frontal nerve, and nasociliary nerve. Damage to this nerve can result in various visual disturbances and loss of sensation in the affected areas.
Diplopia is a medical term that refers to the condition where a person sees two images of a single object. It is commonly known as double vision. This can occur due to various reasons, such as nerve damage or misalignment of the eyes. Diplopia can be temporary or chronic and can affect one or both eyes. If you're experiencing diplopia, it's essential to consult an eye care professional for proper evaluation and treatment.
Cranial sinuses are a part of the venous system in the human head. They are air-filled spaces located within the skull and are named according to their location. The cranial sinuses include:
1. Superior sagittal sinus: It runs along the top of the brain, inside the skull, and drains blood from the scalp and the veins of the brain.
2. Inferior sagittal sinus: It runs along the bottom of the brain and drains into the straight sinus.
3. Straight sinus: It is located at the back of the brain and receives blood from the inferior sagittal sinus and great cerebral vein.
4. Occipital sinuses: They are located at the back of the head and drain blood from the scalp and skull.
5. Cavernous sinuses: They are located on each side of the brain, near the temple, and receive blood from the eye and surrounding areas.
6. Sphenoparietal sinus: It is a small sinus that drains blood from the front part of the brain into the cavernous sinus.
7. Petrosquamosal sinuses: They are located near the ear and drain blood from the scalp and skull.
The cranial sinuses play an essential role in draining blood from the brain and protecting it from injury.
Tolosa-Hunt syndrome is a rare disorder characterized by the inflammation of the nerve structures (including the fifth and sixth cranial nerves) within the cavernous sinus, a venous space near the base of the skull. This inflammation can lead to various symptoms such as:
1. Unilateral or bilateral orbital pain, which may be severe and deep, often radiating around the eye and temple.
2. Ophthalmoplegia (paralysis of the eye muscles), causing double vision (diplopia) and limited eye movement in specific directions.
3. Ptosis (drooping of the eyelid).
4. Other possible symptoms include decreased sensation around the forehead, cheek, or upper jaw, and loss of taste on the anterior part of the tongue.
The exact cause of Tolosa-Hunt syndrome is unknown, but it's believed to be related to an autoimmune response or a non-specific inflammatory process. It can also occur in conjunction with other medical conditions like neoplasms (tumors) or infections. The diagnosis typically involves imaging studies such as MRI and CT scans, along with blood tests and a thorough neurological examination.
Treatment usually includes corticosteroids to reduce inflammation and alleviate symptoms. In some cases, immunosuppressive medications or radiation therapy may be necessary. If left untreated, Tolosa-Hunt syndrome can lead to permanent visual impairment or other neurological deficits.
The term "cisterna magna" is derived from Latin, where "cisterna" means "reservoir" or "receptacle," and "magna" means "large." In medical anatomy, the cisterna magna refers to a large, sac-like space located near the lower part of the brainstem. It is a subarachnoid cistern, which means it is a space that contains cerebrospinal fluid (CSF) between the arachnoid and pia mater membranes covering the brain and spinal cord.
More specifically, the cisterna magna is situated between the cerebellum (the lower part of the brain responsible for coordinating muscle movements and maintaining balance) and the occipital bone (the bone at the back of the skull). This space contains a significant amount of CSF, which serves as a protective cushion for the brain and spinal cord, helps regulate intracranial pressure, and facilitates the circulation of nutrients and waste products.
The cisterna magna is an essential structure in neurosurgical procedures and diagnostic imaging techniques like lumbar puncture (spinal tap) or myelograms, where contrast agents are introduced into the CSF to visualize the spinal cord and surrounding structures. Additionally, it serves as a crucial landmark for various surgical approaches to the posterior fossa (the lower part of the skull that houses the cerebellum and brainstem).
Ophthalmoplegia is a medical term that refers to the paralysis or weakness of the eye muscles, which can result in double vision (diplopia) or difficulty moving the eyes. It can be caused by various conditions, including nerve damage, muscle disorders, or neurological diseases such as myasthenia gravis or multiple sclerosis. Ophthalmoplegia can affect one or more eye muscles and can be partial or complete. Depending on the underlying cause, ophthalmoplegia may be treatable with medications, surgery, or other interventions.
The hypoglossal nerve, also known as the 12th cranial nerve (CN XII), is primarily responsible for controlling tongue movements. Hypoglossal nerve diseases refer to conditions that affect this nerve and result in various tongue-related symptoms. These disorders can be congenital or acquired, and they may stem from different causes such as trauma, tumors, infections, inflammation, or degenerative processes.
Hypoglossal nerve diseases can present with the following symptoms:
1. Weakness or paralysis of the tongue muscles on one or both sides.
2. Deviation of the tongue towards the affected side when protruded.
3. Fasciculations (involuntary muscle twitches) or atrophy (wasting) of the tongue muscles.
4. Difficulty with speaking, swallowing, and chewing due to tongue weakness.
5. Changes in taste and sensation on the back of the tongue and throat.
Some specific hypoglossal nerve diseases include:
1. Hypoglossal nerve palsy: A condition characterized by unilateral or bilateral weakness or paralysis of the tongue due to damage to the hypoglossal nerve. Causes can include trauma, tumors, stroke, multiple sclerosis, or other neurological disorders.
2. Hypoglossal neuritis: Inflammation of the hypoglossal nerve, often caused by viral infections or autoimmune processes, leading to tongue weakness and atrophy.
3. Congenital hypoglossal nerve anomalies: Abnormal development of the hypoglossal nerve during fetal growth can result in various tongue-related symptoms and difficulties with speech and swallowing.
4. Tumors affecting the hypoglossal nerve: Both benign and malignant tumors, such as schwannomas or neurofibromas, can compress or infiltrate the hypoglossal nerve, causing weakness or paralysis.
5. Hypoglossal-facial anastomosis: A surgical procedure that connects the hypoglossal nerve to the facial nerve to restore facial movement in cases of facial nerve palsy. This connection can lead to tongue weakness as a side effect.
The oculomotor muscles are a group of extraocular muscles that control the movements of the eye. They include:
1. Superior rectus: This muscle is responsible for elevating the eye and helping with inward rotation (intorsion) when looking downwards.
2. Inferior rectus: It depresses the eye and helps with outward rotation (extorsion) when looking upwards.
3. Medial rectus: This muscle adducts, or moves, the eye towards the midline of the face.
4. Inferior oblique: The inferior oblique muscle intorts and elevates the eye.
5. Superior oblique: It extorts and depresses the eye.
These muscles work together to allow for smooth and precise movements of the eyes, enabling tasks such as tracking moving objects, reading, and maintaining visual fixation on a single point in space.
The vestibulocochlear nerve, also known as the 8th cranial nerve, is responsible for transmitting sound and balance information from the inner ear to the brain. Vestibulocochlear nerve diseases refer to conditions that affect this nerve and can result in hearing loss, vertigo, and balance problems.
These diseases can be caused by various factors, including genetics, infection, trauma, tumors, or degeneration. Some examples of vestibulocochlear nerve diseases include:
1. Vestibular neuritis: an inner ear infection that causes severe vertigo, nausea, and balance problems.
2. Labyrinthitis: an inner ear infection that affects both the vestibular and cochlear nerves, causing vertigo, hearing loss, and tinnitus.
3. Acoustic neuroma: a benign tumor that grows on the vestibulocochlear nerve, causing hearing loss, tinnitus, and balance problems.
4. Meniere's disease: a inner ear disorder that causes vertigo, hearing loss, tinnitus, and a feeling of fullness in the ear.
5. Ototoxicity: damage to the inner ear caused by certain medications or chemicals that can result in hearing loss and balance problems.
6. Vestibular migraine: a type of migraine that is associated with vertigo, dizziness, and balance problems.
Treatment for vestibulocochlear nerve diseases varies depending on the specific condition and its severity. It may include medication, physical therapy, surgery, or a combination of these approaches.
The glossopharyngeal nerve, also known as the ninth cranial nerve (CN IX), is primarily responsible for providing motor innervation to the stylopharyngeus muscle and sensory innervation to parts of the pharynx, middle ear, and posterior tongue. It also plays a role in the reflexive control of heart rate via the baroreceptors located in the carotid sinus.
Glossopharyngeal nerve diseases refer to conditions that affect the function of this nerve, leading to various symptoms. These diseases can be classified into two main categories: peripheral and central. Peripheral disorders are caused by damage or injury to the nerve itself, while central disorders result from problems in the brainstem where the glossopharyngeal nerve originates.
Some examples of glossopharyngeal nerve diseases include:
1. Glossopharyngeal neuralgia: A rare condition characterized by severe, stabbing pain in the throat, ear, or tongue, often triggered by swallowing or talking. This disorder may be caused by compression of the nerve by blood vessels or other structures.
2. Infections: Bacterial and viral infections can cause inflammation and damage to the glossopharyngeal nerve, leading to dysfunction. Examples include Lyme disease, herpes zoster (shingles), and meningitis.
3. Tumors: Benign or malignant growths in the head and neck region can compress and injure the glossopharyngeal nerve, resulting in symptoms related to its dysfunction.
4. Trauma: Direct trauma to the neck or skull base can damage the glossopharyngeal nerve, causing various deficits depending on the severity of the injury.
5. Neurological disorders: Conditions such as multiple sclerosis and stroke can affect the central connections of the glossopharyngeal nerve in the brainstem, leading to dysfunction.
6. Genetic conditions: Rare genetic disorders like Moersch-Woltman syndrome (also known as stiff person syndrome) can involve the glossopharyngeal nerve and cause symptoms related to its dysfunction.
Symptoms of glossopharyngeal nerve dysfunction may include difficulty swallowing, hoarseness, loss of taste on the back of the tongue, decreased sensation in the throat or ear, and pain in the neck, throat, or ear. Treatment for these conditions depends on the underlying cause and may involve medications, surgery, or other interventions to address the specific problem.
The cavernous sinus is a venous structure located in the middle cranial fossa, which is a depression in the skull that houses several important nerves and blood vessels. The cavernous sinus is situated on either side of the sphenoid bone, near the base of the skull, and it contains several important structures:
* The internal carotid artery, which supplies oxygenated blood to the brain
* The abducens nerve (cranial nerve VI), which controls lateral movement of the eye
* The oculomotor nerve (cranial nerve III), which controls most of the muscles that move the eye
* The trochlear nerve (cranial nerve IV), which controls one of the muscles that moves the eye
* The ophthalmic and maxillary divisions of the trigeminal nerve (cranial nerve V), which transmit sensory information from the face and head
The cavernous sinus is an important structure because it serves as a conduit for several critical nerves and blood vessels. However, it is also vulnerable to various pathological conditions such as thrombosis (blood clots), infection, tumors, or aneurysms, which can lead to serious neurological deficits or even death.
Onchocerciasis, Ocular is a medical condition that specifically refers to the eye manifestations caused by the parasitic infection, Onchocerca volvulus. Also known as "river blindness," this disease is spread through the bite of infected blackflies.
Ocular onchocerciasis affects various parts of the eye, including the conjunctiva, cornea, iris, and retina. The infection can cause symptoms such as itching, burning, and redness of the eyes. Over time, it may lead to more serious complications like punctate keratitis (small, scattered opacities on the cornea), cataracts, glaucoma, and ultimately, blindness.
The infection is diagnosed through a skin snip or blood test, which can detect the presence of microfilariae (the larval stage of the parasite) or antibodies against the parasite. Treatment typically involves administering oral medications such as ivermectin, which kills the microfilariae and reduces the risk of eye damage. However, it does not kill the adult worms, so multiple doses are often required to control the infection. In some cases, surgery may be necessary to remove advanced ocular lesions.
Trigeminal nerve diseases refer to conditions that affect the trigeminal nerve, which is one of the cranial nerves responsible for sensations in the face and motor functions such as biting and chewing. The trigeminal nerve has three branches: ophthalmic, maxillary, and mandibular, which innervate different parts of the face and head.
Trigeminal nerve diseases can cause various symptoms, including facial pain, numbness, tingling, or weakness. Some common trigeminal nerve diseases include:
1. Trigeminal neuralgia: A chronic pain condition that affects the trigeminal nerve, causing intense, stabbing, or electric shock-like pain in the face.
2. Hemifacial spasm: A neuromuscular disorder that causes involuntary muscle spasms on one side of the face, often affecting the muscles around the eye and mouth.
3. Trigeminal neuropathy: Damage or injury to the trigeminal nerve, which can result in numbness, tingling, or weakness in the face.
4. Herpes zoster oticus (Ramsay Hunt syndrome): A viral infection that affects the facial nerve and geniculate ganglion of the trigeminal nerve, causing facial paralysis, ear pain, and a rash around the ear.
5. Microvascular compression: Compression of the trigeminal nerve by a blood vessel, which can cause symptoms similar to trigeminal neuralgia.
Treatment for trigeminal nerve diseases depends on the specific condition and its severity. Treatment options may include medication, surgery, or radiation therapy.
The accessory nerve, also known as the 11th cranial nerve (CN XI), has both a cranial and spinal root and innervates the sternocleidomastoid muscle and trapezius muscle. Accessory nerve diseases refer to conditions that affect the function of this nerve, leading to weakness or paralysis of the affected muscles.
Some examples of accessory nerve diseases include:
1. Traumatic injury: Direct trauma to the neck or posterior scalene region can damage the spinal root of the accessory nerve. This can result in weakness or paralysis of the trapezius muscle, leading to difficulty with shoulder movement and pain.
2. Neuralgia: Accessory nerve neuralgia is a condition characterized by painful spasms or shooting pains along the course of the accessory nerve. It can be caused by nerve compression, inflammation, or injury.
3. Tumors: Tumors in the neck region, such as schwannomas or neurofibromas, can compress or invade the accessory nerve, leading to weakness or paralysis of the affected muscles.
4. Infections: Viral infections, such as poliovirus or West Nile virus, can cause inflammation and damage to the accessory nerve, resulting in weakness or paralysis.
5. Neuropathy: Accessory nerve neuropathy is a condition characterized by degeneration of the accessory nerve fibers due to various causes such as diabetes, autoimmune disorders, or exposure to toxins. This can result in weakness or paralysis of the affected muscles.
6. Congenital defects: Some individuals may be born with congenital defects that affect the development and function of the accessory nerve, leading to weakness or paralysis of the affected muscles.
Treatment for accessory nerve diseases depends on the underlying cause and can include physical therapy, medications, surgery, or a combination of these approaches.
Facial nerve diseases refer to a group of medical conditions that affect the function of the facial nerve, also known as the seventh cranial nerve. This nerve is responsible for controlling the muscles of facial expression, and it also carries sensory information from the taste buds in the front two-thirds of the tongue, and regulates saliva flow and tear production.
Facial nerve diseases can cause a variety of symptoms, depending on the specific location and extent of the nerve damage. Common symptoms include:
* Facial weakness or paralysis on one or both sides of the face
* Drooping of the eyelid and corner of the mouth
* Difficulty closing the eye or keeping it closed
* Changes in taste sensation or dryness of the mouth and eyes
* Abnormal sensitivity to sound (hyperacusis)
* Twitching or spasms of the facial muscles
Facial nerve diseases can be caused by a variety of factors, including:
* Infections such as Bell's palsy, Ramsay Hunt syndrome, and Lyme disease
* Trauma or injury to the face or skull
* Tumors that compress or invade the facial nerve
* Neurological conditions such as multiple sclerosis or Guillain-Barre syndrome
* Genetic disorders such as Moebius syndrome or hemifacial microsomia
Treatment for facial nerve diseases depends on the underlying cause and severity of the symptoms. In some cases, medication, physical therapy, or surgery may be necessary to restore function and relieve symptoms.
The abducens nerve, also known as the sixth cranial nerve, is responsible for controlling the lateral rectus muscle of the eye, which enables the eye to move outward. Abducens nerve diseases refer to conditions that affect this nerve and can result in various symptoms, primarily affecting eye movement.
Here are some medical definitions related to abducens nerve diseases:
1. Abducens Nerve Palsy: A condition characterized by weakness or paralysis of the abducens nerve, causing difficulty in moving the affected eye outward. This results in double vision (diplopia), especially when gazing towards the side of the weakened nerve. Abducens nerve palsy can be congenital, acquired, or caused by various factors such as trauma, tumors, aneurysms, infections, or diseases like diabetes and multiple sclerosis.
2. Sixth Nerve Palsy: Another term for abducens nerve palsy, referring to the weakness or paralysis of the sixth cranial nerve.
3. Internuclear Ophthalmoplegia (INO): A neurological condition affecting eye movement, often caused by a lesion in the medial longitudinal fasciculus (MLF), a bundle of nerve fibers that connects the abducens nucleus with the oculomotor nucleus. INO results in impaired adduction (inward movement) of the eye on the side of the lesion and nystagmus (involuntary eye movements) of the abducting eye on the opposite side when attempting to look towards the side of the lesion.
4. One-and-a-Half Syndrome: A rare neurological condition characterized by a combination of INO and internuclear ophthalmoplegia with horizontal gaze palsy on the same side, caused by damage to both the abducens nerve and the paramedian pontine reticular formation (PPRF). This results in limited or no ability to move the eyes towards the side of the lesion and impaired adduction of the eye on the opposite side.
5. Brainstem Encephalitis: Inflammation of the brainstem, which can affect the abducens nerve and other cranial nerves, leading to various neurological symptoms such as diplopia (double vision), ataxia (loss of balance and coordination), and facial weakness. Brainstem encephalitis can be caused by infectious agents, autoimmune disorders, or paraneoplastic syndromes.
6. Multiple Sclerosis (MS): An autoimmune disorder characterized by inflammation and demyelination of the central nervous system, including the brainstem and optic nerves. MS can cause various neurological symptoms, such as diplopia, nystagmus, and INO, due to damage to the abducens nerve and other cranial nerves.
7. Wernicke's Encephalopathy: A neurological disorder caused by thiamine (vitamin B1) deficiency, often seen in alcoholics or individuals with malnutrition. Wernicke's encephalopathy can affect the brainstem and cause various symptoms such as diplopia, ataxia, confusion, and oculomotor abnormalities.
8. Pontine Glioma: A rare type of brain tumor that arises from the glial cells in the pons (a part of the brainstem). Pontine gliomas can cause various neurological symptoms such as diplopia, facial weakness, and difficulty swallowing due to their location in the brainstem.
9. Brainstem Cavernous Malformation: A benign vascular lesion that arises from the small blood vessels in the brainstem. Brainstem cavernous malformations can cause various neurological symptoms such as diplopia, ataxia, and facial weakness due to their location in the brainstem.
10. Pituitary Adenoma: A benign tumor that arises from the pituitary gland, located at the base of the brain. Large pituitary adenomas can compress the optic nerves and cause various visual symptoms such as diplopia, visual field defects, and decreased vision.
11. Craniopharyngioma: A benign tumor that arises from the remnants of the Rathke's pouch, a structure that gives rise to the anterior pituitary gland. Craniopharyngiomas can cause various neurological and endocrine symptoms such as diplopia, visual field defects, headaches, and hormonal imbalances due to their location near the optic nerves and pituitary gland.
12. Meningioma: A benign tumor that arises from the meninges, the protective covering of the brain and spinal cord. Meningiomas can cause various neurological symptoms such as diplopia, headaches, and seizures depending on their location in the brain or spinal cord.
13. Chordoma: A rare type of malignant tumor that arises from the remnants of the notochord, a structure that gives rise to the spine during embryonic development. Chordomas can cause various neurological and endocrine symptoms such as diplopia, visual field defects, headaches, and hormonal imbalances due to their location near the brainstem and spinal cord.
14. Metastatic Brain Tumors: Malignant tumors that spread from other parts of the body to the brain. Metastatic brain tumors can cause various neurological symptoms such as diplopia, headaches, seizures, and cognitive impairment depending on their location in the brain.
15. Other Rare Brain Tumors: There are many other rare types of brain tumors that can cause diplopia or other neurological symptoms, including gliomas, ependymomas, pineal region tumors, and others. These tumors require specialized diagnosis and treatment by neuro-oncologists and neurosurgeons with expertise in these rare conditions.
In summary, diplopia can be caused by various brain tumors, including pituitary adenomas, meningiomas, chordomas, metastatic brain tumors, and other rare types of tumors. It is important to seek medical attention promptly if you experience diplopia or other neurological symptoms, as early diagnosis and treatment can improve outcomes and quality of life.
The oculomotor nerve, also known as the third cranial nerve (CN III), is a motor nerve that originates from the midbrain. It controls the majority of the eye muscles, including the levator palpebrae superioris muscle that raises the upper eyelid, and the extraocular muscles that enable various movements of the eye such as looking upward, downward, inward, and outward. Additionally, it carries parasympathetic fibers responsible for pupillary constriction and accommodation (focusing on near objects). Damage to this nerve can result in various ocular motor disorders, including strabismus, ptosis, and pupillary abnormalities.
The patellofemoral joint is the articulation between the patella (kneecap) and the femur (thigh bone). It is a synovial joint, which means it is surrounded by a joint capsule containing synovial fluid to lubricate the joint. This joint is responsible for providing stability to the knee extensor mechanism and allows for smooth movement of the patella during activities like walking, running, and jumping. Pain or dysfunction in this joint can result in various conditions such as patellofemoral pain syndrome, chondromalacia patella, or patellar dislocation.
Neuroimaging is a medical term that refers to the use of various techniques to either directly or indirectly image the structure, function, or pharmacology of the nervous system. It includes techniques such as computed tomography (CT), magnetic resonance imaging (MRI), functional MRI (fMRI), positron emission tomography (PET), single-photon emission computed tomography (SPECT), and diffusion tensor imaging (DTI). These techniques are used to diagnose and monitor various neurological and psychiatric conditions, as well as to understand the underlying mechanisms of brain function in health and disease.
The oculomotor nerve, also known as the third cranial nerve (CN III), is responsible for controlling several important eye movements and functions. Oculomotor nerve diseases refer to conditions that affect this nerve and can lead to various symptoms related to eye movement and function. Here's a medical definition of oculomotor nerve diseases:
Oculomotor nerve diseases are a group of medical disorders characterized by the dysfunction or damage to the oculomotor nerve (CN III), resulting in impaired eye movements, abnormalities in pupillary response, and potential effects on eyelid position. These conditions can be congenital, acquired, or traumatic in nature and may lead to partial or complete paralysis of the nerve. Common oculomotor nerve diseases include oculomotor nerve palsy, third nerve ganglionopathies, and compressive oculomotor neuropathies caused by various pathologies such as aneurysms, tumors, or infections.
Optic neuritis is a medical condition characterized by inflammation and damage to the optic nerve, which transmits visual information from the eye to the brain. This condition can result in various symptoms such as vision loss, pain with eye movement, color vision disturbances, and pupillary abnormalities. Optic neuritis may occur in isolation or be associated with other underlying medical conditions, including multiple sclerosis, neuromyelitis optica, and autoimmune disorders. The diagnosis typically involves a comprehensive eye examination, including visual acuity testing, dilated funduscopic examination, and possibly imaging studies like MRI to evaluate the optic nerve and brain. Treatment options may include corticosteroids or other immunomodulatory therapies to reduce inflammation and prevent further damage to the optic nerve.
The mesencephalon, also known as the midbrain, is the middle portion of the brainstem that connects the hindbrain (rhombencephalon) and the forebrain (prosencephalon). It plays a crucial role in several important functions including motor control, vision, hearing, and the regulation of consciousness and sleep-wake cycles. The mesencephalon contains several important structures such as the cerebral aqueduct, tectum, tegmentum, cerebral peduncles, and several cranial nerve nuclei (III and IV).
Patellar dislocation is a medical condition characterized by the displacement of the patella (kneecap) from its normal position in the femoral groove, which is a part of the femur (thighbone). This displacement usually occurs laterally, meaning that the patella moves toward the outer side of the knee.
Patellar dislocation can happen as a result of direct trauma or due to various factors that increase the laxity of the medial patellofemoral ligament and tightness of the lateral structures, leading to abnormal tracking of the patella. These factors include anatomical variations, muscle imbalances, genetic predisposition, or degenerative changes in the knee joint.
Dislocation of the patella can cause pain, swelling, and difficulty in moving the knee. In some cases, it might be associated with other injuries such as fractures or damage to the articular cartilage and surrounding soft tissues. Immediate medical attention is required for proper diagnosis and treatment, which may involve reduction, immobilization, physical therapy, bracing, or even surgery in severe cases.
The sciatic nerve is the largest and longest nerve in the human body, running from the lower back through the buttocks and down the legs to the feet. It is formed by the union of the ventral rami (branches) of the L4 to S3 spinal nerves. The sciatic nerve provides motor and sensory innervation to various muscles and skin areas in the lower limbs, including the hamstrings, calf muscles, and the sole of the foot. Sciatic nerve disorders or injuries can result in symptoms such as pain, numbness, tingling, or weakness in the lower back, hips, legs, and feet, known as sciatica.
The patella, also known as the kneecap, is a sesamoid bone located at the front of the knee joint. It is embedded in the tendon of the quadriceps muscle and serves to protect the knee joint and increase the leverage of the extensor mechanism, allowing for greater extension force of the lower leg. The patella moves within a groove on the femur called the trochlea during flexion and extension of the knee.
 Nystagmus
Nystagmus
Cranial nerve disease
Brainstem
Ophthalmoparesis
Superior oblique myokymia
Trochlear nerve
Hypertropia
Eye movement
Recurrent painful ophthalmoplegic neuropathy
Torticollis
Diabetic neuropathy
Cranial nerves
Parinaud's syndrome
Idiopathic intracranial hypertension
Trochleitis
Pituitary apoplexy
Oculomotor nerve palsy
Abducens nerve
Joint
Synkinesis
Medial longitudinal fasciculus
Cavernous sinus
Extraocular muscles
Neurosarcoidosis
Motor neuron
Tropic cues involved in growth cone guidance
Brain herniation
Orbit (anatomy)
Alternating hemiplegia
Elbow
 Familial congenital palsy of trochlear nerve | Rare Diseases | RareGuru
Familial congenital palsy of trochlear nerve | Rare Diseases | RareGuru
 Trochlear Nerve Palsy (Fourth Nerve Palsy): Background, History of the Procedure, Problem
Trochlear Nerve Palsy (Fourth Nerve Palsy): Background, History of the Procedure, Problem
Nystagmus - Wikipedia
Trochlear nerve schwannoma with intratumoral hemorrhage: case report. - Fingerprint - Keio University
DeCS - New terms
DeCS - New terms
DeCS - New terms
DeCS - New terms
DeCS - New terms
DeCS - New terms
 DeCS - New terms
DeCS - New terms
DeCS - New terms
DeCS - New terms
DeCS - New terms
DeCS - New terms
DeCS - New terms
Bio2Vec
 Median Neuropathy; Median Nerve Diseases
Median Neuropathy; Median Nerve Diseases
 Houston Methodist Hospital - Research output
- Houston Methodist Scholars
Houston Methodist Hospital - Research output
- Houston Methodist Scholars
 Pesquisa | Portal Regional da BVS
Pesquisa | Portal Regional da BVS
Specific PHGKB|Rare Diseases PHGKB|PHGKB
 Fourth Cranial (Trochlear) Nerve Palsy - Neurologic Disorders - MSD Manual Professional Edition
Fourth Cranial (Trochlear) Nerve Palsy - Neurologic Disorders - MSD Manual Professional Edition
Guillain-Barre Syndrome: Practice Essentials, Background, Pathophysiology
 Clinical Services Offered
Clinical Services Offered
 Facial Nerve Diseases (medical concept explorer)
Facial Nerve Diseases (medical concept explorer)
Cantore, W. A.<...
 oh oh oh to touch and feel cranial nerves
oh oh oh to touch and feel cranial nerves
Scoliosis. Medical search. Definitions
 MeSH Browser
MeSH Browser
Guillain-Barre Syndrome: Practice Essentials, Background, Pathophysiology
OCULOMOTOR NERVE5
- All the extraocular muscles are innervated by the oculomotor nerve (CN III) except the superior oblique and lateral rectus muscles, which are innervated by the trochlear nerve (CN IV) and abducent nerve (CN VI), respectively. (brainmadesimple.com)
- This fasciculus connects the abducent nerve nucleus with the nuclei of the oculomotor nerve (CN III), trochlear nerve (CN IV), and vestibulocochlear nerve (CN VIII). (brainmadesimple.com)
- The cranial nerves that control eye movements (e.g., oculomotor nerve, trochlear nerve, abducens nerve) can be affected by neurological conditions, leading to eye movement abnormalities or double vision. (rthm.com)
- Benedict syndrome (BS) is caused by a stroke in the midbrain and usually presents as an ipsilateral oculomotor nerve palsy with contralateral hemi- tremor . (symptoma.com)
- The oculomotor nerve runs the ventral width of the tegmentum, emerging out of the nucleus. (databasefootball.com)
Nuclei12
- The nuclei of the cranial nerves are the collection of cell bodies of axons forming that cranial nerve. (brainmadesimple.com)
- Facial colliculi are actually rounded, bulged structures that are formed by the winding of fibers of the facial nerve around the nuclei of abducent nerves. (brainmadesimple.com)
- Diseases of the ninth cranial (glossopharyngeal) nerve or its nuclei in the medulla. (nih.gov)
- With the exception of the optic and olfactory nerves, this includes disorders of the brain stem nuclei from which the cranial nerves originate or terminate. (sdsu.edu)
- Underlying each of these are motor nuclei for the respective cranial nerves. (wikidoc.org)
- Each facial colliculus , contrary to their names, do not contain the facial nerve nuclei. (wikidoc.org)
- Instead, they have facial nerve axons traversing superficial to underlying abducens (CN VI) nuclei. (wikidoc.org)
- The cerebral aqueduct contains the nuclei of two pairs of cranial nerves , the oculomotor nuclei and the trochlear nuclei. (databasefootball.com)
- In contrast, the trochlear nuclei are found at the level of the inferior colliculus and they help refine vision, focusing the eyes on proximal objects. (databasefootball.com)
- Wilhelm His Sr. (18311904) combined, in an unprecedented way, (taste bud afferents of cranial nerves VII, IX, X to the solitary tract) and dorsolateral otic placode-derived afferents provide the sole sensory input to the special somatic column consisting of the vestibular/auditory nuclei. (spagades.com)
- Diseases of the facial nerve or nuclei. (nih.gov)
- Pontine disorders may affect the facial nuclei or nerve fascicle. (nih.gov)
Palsy38
- Connect with other caregivers and patients with Familial congenital palsy of trochlear nerve and get the support you need. (rareguru.com)
- Familial congenital palsy of trochlear nerve is a rare, genetic, neuro- ophthalmological disease characterized by congenital fourth cranial nerve palsy, manifesting with hypertropia in side gaze, unexplained head tilt, acquired vertical diplopia, and progressive increase in vertical fusional vergence amplitudes with prolonged occlusion. (rareguru.com)
- Trochlear nerve palsy is mentioned in ophthalmology texts dating to the mid nineteenth century. (medscape.com)
- In 1935, Bielschowsky correctly noted that trochlear nerve palsy was the most common cause of vertical diplopia and introduced his classic head-tilt test. (medscape.com)
- A fourth nerve palsy is a common cause of binocular vertical oblique diplopia in isolation. (medscape.com)
- An isolated fourth cranial nerve palsy usually can be diagnosed using the 3-step test. (medscape.com)
- Most cases of isolated fourth nerve palsy are believed to be congenital. (medscape.com)
- [ 5 ] However, estimating the true frequency of congenital fourth nerve palsy is difficult. (medscape.com)
- Some of the best information regarding the incidence of acquired fourth nerve palsy can be found in the Mayo Clinic series. (medscape.com)
- Trochlear nerve palsy was less common than abducens or oculomotor palsies. (medscape.com)
- Of 4,373 acquired cases of extraocular muscle palsy in adults, there were only 657 cases of isolated fourth nerve disease. (medscape.com)
- [ 6 ] Fourth nerve palsy also was the least frequent in a pediatric population. (medscape.com)
- In a similar Mayo Clinic study of 160 children, 19 of them had isolated fourth nerve palsy. (medscape.com)
- One must consider the possibility of underlying structural abnormalities (eg, skull based tumor) if fourth nerve palsy results after only minor trauma. (medscape.com)
- Microvasculopathy secondary to diabetes, atherosclerosis, or hypertension also may cause isolated fourth nerve palsy. (medscape.com)
- There are rare reports of thyroid ophthalmopathy and myasthenia gravis mimicking an isolated fourth nerve palsy. (medscape.com)
- Tumor, aneurysm, multiple sclerosis , or iatrogenic injury may present with isolated fourth nerve palsy that may evolve over time to include other cranial nerve palsies or neurologic symptoms. (medscape.com)
- Fourth nerve palsy may become manifest after cataract surgery. (medscape.com)
- Patients with underlying, well-controlled, and asymptomatic fourth nerve palsy may decompensate gradually as they lose binocular function resulting from cataract. (medscape.com)
- This syndrome was present in 73% of congenital trochlear nerve palsy cases and is characterized by absence of the trochlear nerve and secondary atrophy of the superior oblique muscle. (medscape.com)
- Fourth cranial nerve palsy impairs the superior oblique muscle, causing paresis of vertical gaze, mainly in adduction. (msdmanuals.com)
- Fourth cranial nerve palsy may affect one or both eyes. (msdmanuals.com)
- Childhood-onset of recurrent headaches with an oculomotor cranial nerve palsy. (nih.gov)
- During neurosurgery clinical analysis, the patient presented hypoesthesia of maxillary (V2) division of trigeminal nerve (V), associated with partial III and complete VI nerve palsy, on the right side. (surgicalneurologyint.com)
- Fourth nerve palsy, also known as superior oblique palsy or trochlear nerve palsy, occurs when the fourth cranial nerve becomes diseased or damaged. (optometrists.org)
- Idiopathic fourth nerve palsy occurs when there is no known cause for the nerve paralysis. (optometrists.org)
- What are the symptoms of fourth nerve palsy? (optometrists.org)
- Fourth nerve palsy generally affects only one eye, but it can affect both eyes as well. (optometrists.org)
- How is fourth nerve palsy diagnosed? (optometrists.org)
- To diagnose fourth nerve palsy, your eye doctor will first conduct a full medical history. (optometrists.org)
- How is fourth nerve palsy treated? (optometrists.org)
- The treatment options for fourth nerve palsy depend on the underlying cause of the condition. (optometrists.org)
- When fourth nerve palsy is idiopathic or caused by an injury to the nerve, it may improve on its own after several months. (optometrists.org)
- Vision therapy is an effective treatment option for some patients with fourth nerve palsy, as it can help to improve eye movements and binocular vision. (optometrists.org)
- The sooner fourth nerve palsy is diagnosed, the greater your chances of optimal treatment results. (optometrists.org)
- Aetiology: Trochlear nerve palsy can be divided into acute or congenital. (uk.com)
- Congenital trochlear nerve palsy is usually noted in childhood with development of abnormal head posture. (uk.com)
- Various pathologies can lead to acute IV nerve palsy, most commonly trauma. (uk.com)
Trigeminal nerve7
- Third division of trigeminal nerve innervates masseter and temporalis, so you should check for contraction of both muscles! (usc.edu)
- The trigeminal nerve provides sensory supply to the face and mouth. (usc.edu)
- The corneal reflex has two parts: the sensory, or afferent, part of the reflex is mediated by the ophthalmic branch of the trigeminal nerve, and the motor, or efferent, part of the reflex is mediated by the facial nerve. (usc.edu)
- At the level of the midpons, the large trigeminal nerve , CN V, emerges. (wikidoc.org)
- This manifestation is due to the involvement of the maxillary tier of the trigeminal nerve. (healthncare.info)
- A sudden, stabbing painassociated with this disease is known as tic douloureux Oct 24, 2015 - Explore Lory W's board "Trigeminal Neuralgia", followed by 212 people on Pinterest trigeminal neuralgia: Definition Trigeminal neuralgia is a disorder of the trigeminal nerve (the fifth cranial nerve) that causes episodes of sharp, An Introduction to the Brain and Cranial Nerves. (spagades.com)
- The syndrome is characterised by retro-orbital paralysis of extraocular muscles impairment of the branches of the 1st division of the trigeminal nerve and frequently extension to involve the optic nerve. (medicosnotes.com)
Disorders7
- Other common causes include diseases and disorders of the central nervous system, metabolic disorders and alcohol and drug toxicity. (wikipedia.org)
- thus, they can be considered cranial nerve disorders, neuro-ophthalmologic. (msdmanuals.com)
- Disorders of one or more of the twelve cranial nerves. (sdsu.edu)
- These disorders affect the intricate relationship between the eyes, optic nerves, and the brain, leading to various visual symptoms and eye-related abnormalities. (rthm.com)
- For example, whereas congenital or developmental diseases occur most often in young patients, neoplasia and degenerative disorders are more common in older patients. (merckvetmanual.com)
- Diseases that progress over several days include inflammatory and metabolic disorders, as well as some tumors. (merckvetmanual.com)
- Inflammatory disorders, and vasculitic ischaemic diseases. (medicosnotes.com)
Olfactory Nerve3
- Olfactory nerve - CN I. Sensory cranial nerves help a person see, smell, and hear. (spagades.com)
- The 12 cranial nerves are: I Olfactory Nerve. (spagades.com)
- In the first, we discuss the olfactory nerve, detailing its function and describing the anatomy of this The median plane, which divides the body into left and right. (spagades.com)
Ocular4
- Cranial nerves 3, 4 and 6 & extra ocular movements: Touch the sharp tip of the stick to the right and left side of the forehead, assessing the Ophthalmic branch. (spagades.com)
- The common abnormalities include brain tumor, hemorrhagic brain disease, stroke, and local eye disease damaging the muscles of ocular motion. (usc.edu)
- The inclusion of ocular motor nerves in the anatomical zone of the orbital apex causes ophthalmoplegia and visual loss which leads to orbital apex syndrome. (healthncare.info)
- Coronaviruses can cause severe ocular disease in animals, including anterior uveitis, retinitis, vasculitis, and optic neuritis in feline and murine species. (cov19longhaulfoundation.org)
Palsies4
- With greater clinical interest, the number of identified fourth nerve palsies has increased. (medscape.com)
- Several studies reported the incidence and etiology of acquired cranial nerve palsies in adult and pediatric patients. (medscape.com)
- A series of high-definition magnetic resonance imaging (MRI) studies by Yang et al have identified 2 etiologies of congenital trochlear nerve palsies, with the most common being congenital cranial dysinnervation syndrome. (medscape.com)
- We discussed in the first part some of these conditions including third cranial nerve palsies, giant cell. (uk.com)
Vestibular2
- vestibular disease. (myassignmentwriters.com)
- Cranial Nerve VIII (Vestibulocochlear Nerve): Sensory for hearing, motor for balance Vestibular branch (balance): Ask patient to march in place (Mittlemeyer Marching) with eyes closed. (spagades.com)
Abducent5
- For the internal strabismus, the defect sometimes is due to any damage to the abducent nerve, the sixth cranial nerve. (brainmadesimple.com)
- In the following text, we shall have a look at the origin, course, classification, and functional component(s) of the abducent nerve. (brainmadesimple.com)
- Last but not least, we shall have a look at the diseases caused by damage to the abducent nerve. (brainmadesimple.com)
- The abducent or abducent nerve is the sixth cranial nerve (CN VI). (brainmadesimple.com)
- There is only one nucleus for each of the abducent nerves that is present in the upper pons (seen in the cut section of upper pons) at the level of facial colliculi. (brainmadesimple.com)
Acute4
- Since December 2019, coronavirus disease 2019 (COVID-19) has become a global pandemic caused by the highly transmissible severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). (cov19longhaulfoundation.org)
- The posterior fossa tumor or skull base tumor may suppress the nerve supply to the neck and eventually cause acute torticollis . (frederickearlstein.com)
- Posterior pharyngeal infections can irritate the nerves that supply the neck muscles which may also cause acute torticollis . (frederickearlstein.com)
- Moving Beyond the Dura for Assessing Acute and Chronic cranial nerves boundless anatomy and physiology. (spagades.com)
Idiopathic1
- Types of early-onset nystagmus include the following, along with some of their causes: Infantile: Albinism Aniridia Bilateral congenital cataract Bilateral optic nerve hypoplasia Idiopathic Leber's congenital amaurosis Optic nerve or macular disease Persistent tunica vasculosa lentis Rod monochromatism Visual-motor syndrome of functional monophthalmus Latent nystagmus Noonan syndrome Nystagmus blockage syndrome X-linked infantile nystagmus is associated with mutations of the gene FRMD7, which is located on the X chromosome. (wikipedia.org)
Pathology1
- Clinical Anatomy of the Cranial Nerves combines anatomical knowledge, pathology, clinical examination, and explanation of clinical findings, drawing together material typically scattered throughout anatomical textbooks. (spagades.com)
Diplopia1
- and TROCHLEAR NERVE are involved with DIPLOPIA and BLEPHAROPTOSIS . (nih.gov)
Vestibulocochlear nerve2
- It also interacts with the third and fourth cranial nerves, oculomotor and trochlear, respectively, as well as with the eighth cranial nerve (vestibulocochlear nerve) to perform conjugate eye movements (discussed later). (brainmadesimple.com)
- These cranial nerves are the abducens nerve , facial nerve and the vestibulocochlear nerve , respectively. (wikidoc.org)
Pons4
- Abducens nerve emerges from the brain stem in the posterior cranial fossa from a groove at the junction of the pons and medulla oblongata medial to the facial nerve exit. (brainmadesimple.com)
- Between the basal pons, cranial nerve 6, 7 and 8 emerge (medial to lateral). (wikidoc.org)
- At the rostral pons, the occulomotor nerve emerges at the midline. (wikidoc.org)
- Laterally, the trochlear nerve has emerged after emerging out of the dorsal rostral pons and wrapping around to the anterior. (wikidoc.org)
Hypoglossal nerve2
- Emerging from the anterolateral sulci are the hypoglossal nerve (CN XII) rootlets. (wikidoc.org)
- Tongue deviation from unilateral hypoglossal nerve injury (CN XII). (wikem.org)
Paresis1
- Extraocular Paresis of cranial nerves III, IV, and VI causing ophthalmoplegia. (medicosnotes.com)
Neurodegenerative diseases1
- Neuro-ophthalmologists evaluate and manage various types of visual field abnormalities caused by conditions such as strokes, brain tumors, or neurodegenerative diseases. (rthm.com)
Superior oblique4
- The fourth cranial nerve innervates the superior oblique muscle, which intorts, depresses, and abducts the globe. (medscape.com)
- The remaining 27% had a normal trochlear nerve and superior oblique muscle size, but an abnormal superior oblique tendon, which may explain the variations in superior oblique tendon laxity encountered surgically. (medscape.com)
- The fourth cranial nerve controls the actions of the superior oblique eye muscle. (optometrists.org)
- the trochlear nerve supplies the superior oblique muscle in the eye. (frederickearlstein.com)
Spinal3
- The common abnormalities include disease of the muscle itself (myopathy), and motor nerve damage in peripheral/spinal cord/brain from cancer or trauma. (usc.edu)
- The latter is usually caused by Potted Disease or also known as spinal tuberculosis. (frederickearlstein.com)
- 1. The central nervous system includes the brain and spinal cord, while the peripheral nervous system includes the cranial and spinal nerves, as well as the ganglia. (spagades.com)
Symptoms7
- They include the nerves that transmit smell, those responsible for vision and the movement of the eyes, those that control facial movements, those responsible for hearing and balance, and those responsible for chewing, swallowing, vocalizing, and movement of the Other times a person's neurologic symptoms bring them to the doctors office. (spagades.com)
- Often associated with significant symptoms and disseminated systemic disease, nowadays radiosurgery is the first and less invasive strategy, offering low risk of new deficits, clinical improvement, and good local control. (surgicalneurologyint.com)
- ICD-9-CM codes are used in medical billing and coding to describe diseases, injuries, symptoms and conditions. (icd9data.com)
- These symptoms result due to the involvement of the optic and cranial nerves simultaneously. (healthncare.info)
- The visual system is intricately connected to the brain, and any abnormalities or diseases affecting the neurological pathways involved in vision can result in visual symptoms. (rthm.com)
- Conditions affecting the optic nerve, such as optic neuritis or optic neuropathy, can lead to visual symptoms such as reduced color vision, loss of peripheral vision (typically in a specific pattern, e.g., central scotoma), or visual field defects. (rthm.com)
- It is not a disease but a syndrome that is characterized by paroxysmal headache associated with other signs and symptoms. (medscape.com)
Hemorrhage2
- Trochlear nerve schwannoma with intratumoral hemorrhage: case report. (elsevierpure.com)
- Dive into the research topics of 'Trochlear nerve schwannoma with intratumoral hemorrhage: case report. (elsevierpure.com)
Movements4
- Electronystagmography is a test that looks at eye movements to see how well nerves in the brain are working. (medlineplus.gov)
- The patches record eye movements that occur when the inner ear and nearby nerves are stimulated by the water or air. (medlineplus.gov)
- Abnormal results may be a sign of damage to the nerve of the inner ear or other parts of the brain that control eye movements. (medlineplus.gov)
- They also help control certain eye movements and interact with fibers of the optic nerve. (databasefootball.com)
Sensory and motor2
- The sensory and motor innervation to the structures in the head and neck region of the body is exclusively provided by the cranial nerves. (brainmadesimple.com)
- It is commonly stated there are 12 to 13 cranial nerve pairs, Name the major brain regions, vesicles, and ventricles, and describe containing both sensory and motor fibers. (spagades.com)
Auditory1
- Near the superior colliculi are the inferior colliculi, which are responsible for the processing of auditory information and are found just above the trochlear nerve. (databasefootball.com)
Bilateral2
Posterior2
- Some of the diseases that present nystagmus as a pathological sign or symptom are as follows: Aniridia Benign paroxysmal positional vertigo Brain tumors (medulloblastoma, astrocytoma, or other tumors in the posterior fossa. (wikipedia.org)
- The nerve may be injured by diseases affecting the lower brain stem, floor of the posterior fossa, jugular foramen, or the nerve's extracranial course. (nih.gov)
Lateral1
- Lateral (and dorsal) to the olives are the rootlets for cranial nerves IX and X ( glossopharyngeal and vagus , respectively). (wikidoc.org)
Pairs1
- There are 12 pairs of cranial nerves Overview of the Cranial Nerves Twelve pairs of nervesthe cranial nerveslead directly from the brain to various parts of the head, neck, and trunk. (spagades.com)
Cavernous2
- The only difference between the orbital apex diseases such as OPS, CSS (Cavernous sinus syndrome), and SOFS (Superior orbital fissure syndrome) is the involvement of the optic nerve. (healthncare.info)
- Cavernous sinus syndrome (CSS) is characterized by deficits in more than one of the cranial nerves (CN) that traverse the cavernous sinus at the base of the cranial vault: CN III (oculomotor), IV (trochlear), VI (abducens), and the first two branches of CN V (trigeminal). (avmi.net)
Neurologic2
- When the patient cannot track motion this means neurologic damage involving cranial nerves III, IV, or VI. (usc.edu)
- Approach to the patient with neurologic disease. (medlineplus.gov)
Chronic2
- Patients with cancer and chronic kidney disease have higher treatment costs. (bvsalud.org)
- The inocula were prepared from pooled brain material from chronic wasting disease- affected elk from South Dakota, USA (CWDelk), and mule deer from Wyoming, USA (CWDmd), as described previously ( 2 ). (cdc.gov)
Vagus1
- The Vagus nerve is one exception that provides innervation to structures in the head and neck region as well as in the abdomen and chest cavity. (brainmadesimple.com)
Fibers2
- In this atlas you can view MRI sections through a living human brain as well as corresponding sections stained for cell bodies or for nerve fibers. (martindalecenter.com)
- The optic nerve contains only afferent (sensory) fibers, and like all cranial nerves is paired. (spagades.com)
Syndrome6
- Do you have information about a disease, disorder, or syndrome? (rareguru.com)
- Because the syndrome has multiple causes, the history of rapid progression and atypical image findings can arise suggesting metastatic diseases. (surgicalneurologyint.com)
- Orbital apex syndrome is a condition in which the cranial and optic nerves are involved and they do not work properly. (healthncare.info)
- Due to this, orbital apex syndrome is considered different from the other two diseases. (healthncare.info)
- The diagnosis of the disease becomes easy due to this feature of the orbital apex syndrome. (healthncare.info)
- Orbital Apex Syndrome is caused by various infections, inflammations, and tumors and the severity differs according to the origin of the disease. (healthncare.info)
Disorder2
- Is Alzheimer Disease an Autoimmune Disorder? (houstonmethodist.org)
- The test is used to determine whether a balance or nerve disorder is the cause of dizziness or vertigo. (medlineplus.gov)
Anatomy1
- MERP: Anatomy: Cranial Nerves. (spagades.com)
Basal1
- The olfactory is a sensory nerve, and damage in the nasal epithelium or the basal gangliamight impair the ability to discriminate different smells. (usc.edu)
Cerebellar2
- Directly rostral to the superior cerebellar peduncle, there is the superior medullary velum and then the two trochlear nerves. (wikidoc.org)
- Disruptions in the third cranial nerve, the red nucleus, the corticospinal tracts, the brachium conjunctivum, and the superior cerebellar peduncle decussation are normally associated with BS manifestations [1]. (symptoma.com)
Extraocular2
- It is a long, slender, motor nerve and supplies only one of the extraocular muscles of the eye and functions in the movement of the eyeball within the orbit. (brainmadesimple.com)
- Pathogenesis Thyroid eye disease (TED) is an auto-immune condition, in the initial phase there is lymphocytic infiltration and oedema of the extraocular muscles with deposition of glycosaminoglycans and hyaluronic acid and adipogenesis, which can lead to an increase in the. (uk.com)
Skull4
- Cranial nerves (CN) IX through XI all leave the skull together through the jugular foramen. (spagades.com)
- Increased pressure inside the skull that is pressing on the nerve. (optometrists.org)
- Cranial nerves are the 12 nerves of the peripheral nervous system that emerge from the foramina and fissures of the cranium.Their numerical order (1-12) is determined by their skull exit location (rostral to caudal). (spagades.com)
- They pass through skull foramina, fissures, or canals to exit 5th Cranial nerve. (spagades.com)
Lesion1
- lesion of cranial nerve IX. (myassignmentwriters.com)