Urachal Cyst
Urachus
Urinary Bladder Calculi
Clinical significance of first trimester umbilical cord cysts. (1/29)
A cystic mass of the umbilical cord was identified by transvaginal sonography in 10 first trimester pregnancies at a mean gestational age of 8 weeks 4 days (range, 8 weeks 1 day to 9 weeks 3 days) and at a mean crown-rump length of 20.5 mm (range, 15 to 25 mm). The cyst was solitary in all cases, the mean diameter was 4.6 mm (range, 3 to 6 mm), and the location was closer to the fetal insertion in two cases, in the middle of the cord in seven cases, and closer to the placental insertion in one case. Gestational sac and yolk sac diameters as well as the fetal heart rate were within normal ranges for gestational age in all cases. Information on detailed second trimester scans was available in nine cases, demonstrating complete resolution of the cyst and normal fetal anatomic survey in each case. These nine pregnancies were followed to delivery, and normal healthy infants were delivered at term in all cases. This series suggests that the incidental detection of umbilical cord cysts in early pregnancy is not associated with an adverse pregnancy outcome. (+info)Urachal adenocarcinoma in situ with pseudomyxoma peritonei: a case report. (2/29)
A 54 year old man presented with a six month history of abdominal pain. A computerised tomography scan showed a well defined intra-abdominal unilocular mass with a calcified wall just superior to the bladder. At laparotomy, pseudomyxoma peritonei was discovered, together with a midline abdominal mass adherent to the anterior abdominal wall originating from the fundus of the bladder. The specimen consisted of a cystic mass measuring 14 x 9.5 x 7 cm overall, which contained mucoid material. Histological examination revealed that the cyst was lined by mucinous epithelium, which in areas varied from having bland morphology to showing pronounced nuclear and architectural atypia. There was abundant extracellular mucin. The specimen was extensively sampled but there was no evidence of invasion. This tumour has many unusual features, namely: the absence of destructive invasion, association with pseudomyxoma peritonei, areas of dysplasia and cystadenoma, and stromal osseous metaplasia within the wall. (+info)Single and multiple umbilical cord cysts in early gestation: two different entities. (3/29)
OBJECTIVE: To investigate the prevalence of single and multiple umbilical cord cysts in the first trimester and to assess whether there is a difference in the pregnancy outcome between them. METHODS: A targeted sonographic morphological and morphometric evaluation of the umbilical cord was performed in consecutive patients between 7 and 14 weeks of gestation. Crown-rump length and umbilical cord diameter were measured in all cases. Nuchal translucency thickness was measured between 11 and 14 weeks' gestation. In pregnancies at very early gestational ages (7-10 weeks) an additional scan was performed between 11 and 14 weeks. RESULTS: A total of 1159 patients was screened. The prevalence of umbilical cord cysts was 2.1% (24/1159). The cysts were single and multiple in 18 and six cases, respectively. The median (range) largest umbilical cord cyst diameter was no different between multiple and single umbilical cord cysts (3.8 (2.1-18) mm vs. 3.05 (2.0-7.8) mm; P = 0.386). All women with a single umbilical cord cyst delivered an infant without structural abnormalities and without features suggestive of chromosomal abnormalities. Among the women with multiple umbilical cord cysts, four had a missed miscarriage and one had a fetus with obstructive uropathy. CONCLUSION: Single and multiple umbilical cord cysts in the first trimester of gestation represent two different entities. While single cysts in the first trimester are associated with a favorable pregnancy outcome, the presence of multiple umbilical cord cysts is associated with an increased risk of miscarriage and aneuploidy. (+info)Mucinous adenocarcinoma with superficial stromal invasion and villous adenoma of urachal remnants: a case report. (4/29)
This report describes a case of mucinous adenocarcinoma with superficial stromal invasion and villous adenoma originating in the dome of the urinary bladder. Although no urachal remnants were identified, the location suggested urachal derivation. Only two previous cases of urachal adenocarcinoma with features of early stromal invasion associated with a villous tumour have been described. (+info)Umbilical cord edema associated with patent urachus. (5/29)
Umbilical cord anomalies can often be detected prenatally by ultrasound, but a definitive prenatal diagnosis is not always possible. We present a case with increasing edema of the Wharton's jelly followed by the development of pseudocysts in the proximal umbilical cord due to a patent urachus. The first abnormal findings were detected by ultrasound in the 14th week of gestation. Differential diagnoses and their influence on surveillance and birth management are discussed. (+info)Treatment of urachal anomalies: a minimally invasive surgery technique. (6/29)
BACKGROUND: Urachal disease is uncommon. The surgical treatment consists of the resection of the urachus throughout its entire length. Our objective is to demonstrate the use of minimally invasive surgery to treat this disease. METHODS: Six patients were studied and diagnosed. The technique used three 10-mm ports on the right hemi abdomen, through which the dissection of the urachus was performed from the umbilical extreme to the bladder. We evaluated the perioperative records to assess morbidity and outcome. RESULTS: Most patients suffered from episodes of umbilical discharge. The diagnosis was made mainly through clinical history and confirmed during the laparoscopic procedure. The urachus was resected throughout its entire length, and we did not perform a segmentary bladder resection in any patient. The average operative time was 66 minutes (range, 42 to 123), and no operative complications were associated with the technique. DISCUSSION: Minimally invasive surgery is a safe and effective procedure that allows the dissection of the urachus through its entire length, providing optimal postoperative results. (+info)An unusual presentation of Crohn's disease. (7/29)
The first case of an inflamed, discharging urachal remnant associated with granulomatous appendicitis in which the patient was subsequently found to have Crohn's disease is described. (+info)Treatment of infected urachal cysts. (8/29)
The urachus is a fibrous cord that arises from the anterior bladder wall and extends cranially to the umbilicus. Traditionally, infection has been treated using a two-stage procedure that includes an initial incision and drainage which is then followed by elective excision. More recently, it has been suggested that a single-stage excision with improved antibiotics is a safe option. Thus, we intended to compare the effects of the two-stage procedure and the single-stage excision. We performed a retrospective review on nine patients treated between May 1990 and September 2005. The methods used in diagnosis were ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), and cystoscopy. The study group was comprised of three males and six females with a mean age of 28.2 years (with a range from three to 71 years). Symptoms consisted of abdominal pain, abdominal mass, fever, and dysuria. The primary incision and drainage followed by a urachal remnant excision with a bladder cuff excision (two-stage procedure) was performed in four patients. The mean postoperative hospitalization lasted 5.8 days (with a range of three to seven days), and there were no reported complications. A primary excision of the infected urachal cyst and bladder cuff (single-stage excision) was performed in the other five patients. These patients had a mean postoperative hospitalization time of 9.2 days (with a range of four to 15 days), and complications included an enterocutaneous fistula, which required additional operative treatment. The best method of treating an infected urachal cyst remains a matter of debate. However, based on our results, the two-stage procedure is associated with a shorter hospital stay and no complications. Thus, when infection is extensive and severe, we suggest that the two-stage procedure offers a more effective treatment option. (+info)A urachal cyst is a rare type of abdominal wall defect that results from the persistent embryonic remnant of the urachus, which is a canal-like structure that connects the bladder to the umbilicus (belly button) during fetal development. This canal normally obliterates and becomes a fibrous cord known as the median umbilical ligament after birth. However, if it fails to do so, it can result in the formation of various urachal anomalies, including a urachal cyst.
A urachal cyst is a fluid-filled sac that forms along any part of the urachus, usually located between the bladder and the umbilicus. These cysts are typically asymptomatic but can become infected or inflamed, leading to symptoms such as abdominal pain, tenderness, fever, and a palpable mass in the lower abdomen. In some cases, urachal cysts may also cause urinary tract infections or bladder irritation. Diagnosis is usually made through imaging studies such as ultrasound, CT scan, or MRI, and treatment typically involves surgical excision of the cyst to prevent complications.
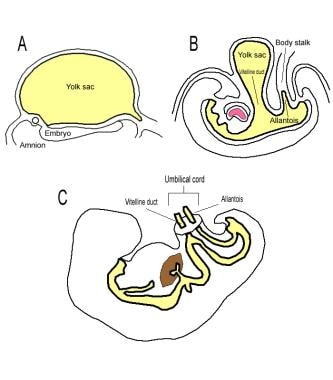
The urachus is a vestigial structure in humans, which is a fibrous cord that connects the umbilicus (navel or belly button) to the dome-shaped top of the bladder. In fetal development, the urachus is the passageway for urine to move from the developing bladder to the allantois, an outpouching of the hindgut that ultimately becomes part of the placenta.
After birth, the urachus usually obliterates and turns into a fibrous cord called the median umbilical ligament. However, in some cases, the urachus may not completely obliterate, leading to various congenital abnormalities such as urachal cysts, urachal sinuses, or urachal fistulas. These conditions can cause symptoms like lower abdominal pain, infection, and sometimes even sepsis if left untreated.
It's worth noting that the urachus is not a commonly discussed structure in routine medical practice, but it does have clinical significance in certain pediatric surgical cases and congenital anomalies.
Urinary bladder calculi, also known as bladder stones, refer to the formation of solid mineral deposits within the urinary bladder. These calculi develop when urine becomes concentrated, allowing minerals to crystallize and stick together, forming a stone. Bladder stones can vary in size, ranging from tiny sand-like particles to larger ones that can occupy a significant portion of the bladder's volume.
Bladder stones typically form as a result of underlying urinary tract issues, such as bladder infection, enlarged prostate, nerve damage, or urinary retention. Symptoms may include lower abdominal pain, difficulty urinating, frequent urination, blood in the urine, and sudden, strong urges to urinate. If left untreated, bladder stones can lead to complications like urinary tract infections and kidney damage. Treatment usually involves surgical removal of the stones or using other minimally invasive procedures to break them up and remove the fragments.
A cyst is a closed sac, having a distinct membrane and division between the sac and its surrounding tissue, that contains fluid, air, or semisolid material. Cysts can occur in various parts of the body, including the skin, internal organs, and bones. They can be caused by various factors, such as infection, genetic predisposition, or blockage of a duct or gland. Some cysts may cause symptoms, such as pain or discomfort, while others may not cause any symptoms at all. Treatment for cysts depends on the type and location of the cyst, as well as whether it is causing any problems. Some cysts may go away on their own, while others may need to be drained or removed through a surgical procedure.
 Urachal cyst
Urachal cyst
Urachus
Median umbilical ligament
Allantois
Urachal fistula
List of ICD-9 codes 740-759: congenital anomalies
List of diseases (U)
Urachal cyst - Wikipedia
 Necrotizing Fasciitis Due to an Infected Urachal Cyst in an Adult
Necrotizing Fasciitis Due to an Infected Urachal Cyst in an Adult
 CJU - Article Abstract: Benign multicystic mesothelioma masquerading as a urachal cyst
CJU - Article Abstract: Benign multicystic mesothelioma masquerading as a urachal cyst
Urachal Cyst | Profiles RNS
Granulosa-Theca Cell Tumors Differential Diagnoses
 Personalized nutrition diagnostics at the point-of-need - PubMed
Personalized nutrition diagnostics at the point-of-need - PubMed
Biomarkers Search
 NCIt Code NCIt PT Subset PT Subset SY NCIt Definition Subset Definition NCIt Code of First Parent First Parent NCIt Code of...
NCIt Code NCIt PT Subset PT Subset SY NCIt Definition Subset Definition NCIt Code of First Parent First Parent NCIt Code of...
 16cm X 12cm Mass - Cancer Survivors Network
16cm X 12cm Mass - Cancer Survivors Network
 Academic Learning Of Urology Procedures - TURP
Academic Learning Of Urology Procedures - TURP
 DeCS
DeCS
 MeSH Browser
MeSH Browser
MeSH Browser
Code System Concept
DeCS 2017 - July 04, 2017 version
Specific PHGKB|Rare Diseases PHGKB|PHGKB
Armenian-English Medical - Terms starting with 'ՈՒ' - MEDINDEX.AM
 Diverticula, Urachal Anomalies, and Utricles | Pediatric Urology Book
Diverticula, Urachal Anomalies, and Utricles | Pediatric Urology Book
Diverticula, Urachal Anomalies, and Utricles | Pediatric Urology Book
Carcinoma of Unknown Primary Associated with a Sister Mary Joseph's Nodule--A Case Report - Fingerprint - Keio University
 How To Get Rid Of Cottage Cheese Belly - CheeseProClub.com
How To Get Rid Of Cottage Cheese Belly - CheeseProClub.com
KoreaMed Synapse
 International Journal of Women's Health and Reproduction Sciences
International Journal of Women's Health and Reproduction Sciences
 Pesquisa | Portal Regional da BVS
Pesquisa | Portal Regional da BVS
DeCS 2013 - December 17, 2013 version
Abstracts in Posters - Educational, SPR 2022 Annual Meeting & Postgraduate Course - SPR Poster Archive
 Urachal mass<...
Urachal mass<...
 Subjects: Peritonitis -- surgery - Digital Collections - National Library of Medicine Search Results
Subjects: Peritonitis -- surgery - Digital Collections - National Library of Medicine Search Results
Disorders of the Umbilicus: Practice Essentials, Anatomy, Pathophysiology
Benign5
- The question of malignancy plays virtually no role in prenatal diagnosis because fetal ovarian cysts are almost always functional and benign tumors [2]. (degruyter.com)
- Breast cysts are a benign (not cancer) condition. (wellsprings-health.com)
- Diagnosis: Benign mesenteric cyst. (radiologycases.my)
- Benign, congenital, neuroepithelial cysts that are typically filled with a viscous mucus. (uams.edu)
- Mesenteric cysts are usually benign and can be very large fluid-filled (2000 mL) lesions. (uchicago.edu)
Urachus1
- This is a type of cyst occurring in a persistent portion of the urachus, presenting as an extraperitoneal mass in the umbilical region. (wikipedia.org)
Sinus3
- A urachal cyst is a sinus remaining from the allantois during embryogenesis. (wikipedia.org)
- Urachal cyst is a sinus that remains from the allantois during embryogenesis. (illnessopedia.org)
- Hi, I have been diagnosed by Umbilical Urachal Sinus. (practo.com)
Colloid Cysts3
- Colloid Cysts" is a descriptor in the National Library of Medicine's controlled vocabulary thesaurus, MeSH (Medical Subject Headings) . (uams.edu)
- This graph shows the total number of publications written about "Colloid Cysts" by people in UAMS Profiles by year, and whether "Colloid Cysts" was a major or minor topic of these publications. (uams.edu)
- Below are the most recent publications written about "Colloid Cysts" by people in Profiles over the past ten years. (uams.edu)
Bronchogenic Cyst3
- Bronchogenic Cyst" is a descriptor in the National Library of Medicine's controlled vocabulary thesaurus, MeSH (Medical Subject Headings) . (wakehealth.edu)
- This graph shows the total number of publications written about "Bronchogenic Cyst" by people in this website by year, and whether "Bronchogenic Cyst" was a major or minor topic of these publications. (wakehealth.edu)
- Below are the most recent publications written about "Bronchogenic Cyst" by people in Profiles. (wakehealth.edu)
Ovarian cyst3
- This case report describes the role of three-dimensional (3-D) ultrasonography as potential diagnostic method for ruling out adnexal torsion when an ovarian cyst is present. (degruyter.com)
- We report a case of fetal ovarian cyst using 3-D ultrasound in order to show how a better definition of the relationship between the ovary containing the cyst and its peduncle can be obtained and to introduce 3-D ultrasound as a method to rule out adnexal torsion when a fetal ovarian cyst is present. (degruyter.com)
- A 33-year-old woman, gravid 1, para 0, was referred to our prenatal center for suspected fetal ovarian cyst. (degruyter.com)
Abscess1
- Gabe was diagnosed with an urachal cyst with abscess. (nicklauschildrens.org)
Mesenteric2
- A left retroperitoneal mesenteric cyst. (radiologycases.my)
- Mesenteric and omental cysts: histologic classification with imaging correlation. (uchicago.edu)
Adenocarcinoma2
- Urachal cysts are usually silent clinically until infection, calculi or adenocarcinoma develop. (wikipedia.org)
- Occupying only 0.01% of all adult cancer patients, the rare entity urachal adenocarcinoma constitutes 22-35% of adenocarcinomas originating from urinary bladder. (2pressrelease.net)
Remnants2
- It is a cyst which occurs in the remnants between the umbilicus and bladder. (wikipedia.org)
- Then, the remnants of urachal tissue must be removed during surgery. (childrensmn.org)
Tract3
- Lower abdominal pain Pain on urination Persistent umbilical discharge Fever Urinary tract infection Lump Hematuria Urachal cysts are rare defects found mostly in young children and hence medical ultrasound of the abdomen, bladder and pelvis is the most used diagnostic tool combined with MRI scan and CT scan in older patients who can remain still during a scan. (wikipedia.org)
- Urachal Cancer is a rare form of bladder cancer that can occur at any site along the urachal tract. (illnessopedia.org)
- Children with urachal anomalies may have frequent urinary tract infections, blood in the urine, excessive discharge from the belly button, abdominal pain, or sometimes abdominal swelling. (childrensmn.org)
Congenital1
- Fetal ovarian cysts have been associated with pregnancies complicated by maternal diabetes, toxemia, and Rh isoimmunization, probably due to the increased production of hCG by the placenta and are rarely associated with other congenital anomalies [2, 4, 6, 12-14]. (degruyter.com)
Urinary1
- Fetal ovarian cysts can be suspected when an ultrasound scan shows intra-abdominal structures in female fetuses in the presence of normal bowel and urinary structures. (degruyter.com)
Inclusion1
- Masses associated with the skin include dermoid cysts, hemangiomas, and inclusion cysts. (medscape.com)
Lump3
- Basically it's a lump of fluid, air, or something else and you may need tests (like a CT scan, ultrasound, or biopsy) to confirm that it's a cyst. (wellsprings-health.com)
- You don't usually need to treat them, but see your doctor about any breast lump because it may be something more serious than a cyst. (wellsprings-health.com)
- If it doesn't close by the time you're born, a small lump of tissue and fluid (a cyst) can grow there. (wellsprings-health.com)
Epithelium2
- Cysts can arise from follicle epithelium, theca-lutein cells, corpus luteum, but some are without a known origin [12]. (degruyter.com)
- Microscopy: section of the cyst wall shows to be lined by ciliated pseudostratified epithelium. (radiologycases.my)
Malformations1
- applied an inversion mode for studying the relationship, size, and course of fluid collections in fetuses in the absence and presence of malformations, including fetal ovarian cysts, demonstrating the additional informative role of 3-D ultrasound [11]. (degruyter.com)
Cancer1
- It is natural to be concerned about any difference in your breasts, but important to know the difference between cancer and the many other types of cysts in the body. (wellsprings-health.com)
Resection1
- Laparoscopic Resection of the Urachal Cyst in. (medtube.net)
Masses1
- Ovarian cysts are among the most common abdominal masses in female fetuses, affecting around 1/2600 pregnancies [3]. (degruyter.com)
Symptoms1
- What are symptoms of urachal anomalies? (childrensmn.org)
Placental1
- The etiology of fetal ovarian cysts is still unknown, although a linkage with fetal gonadotrophin stimulation derived from maternal estrogens or placental human chorionic gonadotrophin (hCG) has been suggested. (degruyter.com)
Tissue1
- This surgery may be performed laparoscopically, which means that very small incisions are used to remove the urachal tissue. (childrensmn.org)
Drain3
- A good soak in the bath can help but in serious cases, your doctor might do surgery to create a permanent drain or remove the cyst. (wellsprings-health.com)
- Your doctor may give you antibiotics, drain or remove the cyst, and possibly repair the area with surgery. (wellsprings-health.com)
- Smaller ones usually go away on their own, but your doctor may need to drain or remove larger, swollen, or painful cysts. (wellsprings-health.com)
Colon1
- Macroscopy: specimen labelled as descending colon cyst consists of a cyst measuring 135x100x80 mm and weighing 500 gm. (radiologycases.my)
Infections1
- When this happens, the open area is vulnerable to infections, cysts, and other problems. (childrensmn.org)
Surgery1
- There is no standard treatment of fetal ovarian cysts, and their management varies widely among different centers, ranging from observation to intrauterine aspiration to neonatal surgery [2, 4, 6, 8, 12-14, 19]. (degruyter.com)
Case2
- Current information regarding the treatment of fetal ovarian cysts is based on personal experiences and some case series. (degruyter.com)
- g One case of urachal cyst an infection. (cell-signaling-pathways.com)
Shows1
- Cut section shows a unilocular cyst containing serous fluid. (radiologycases.my)
Small1
- They hatch in your gut and send small round "oncospheres" through your blood to the brain, muscles, liver, and other organs where they form cysts. (wellsprings-health.com)
Treatment1
- Often, cysts don't need treatment, but your doctor can let you know if yours does. (wellsprings-health.com)
Additional1
- Results -17 of the 50 (34%) dogs had vesicourachal diverticula, and 1 additional dog had a urachal cyst. (avma.org)