Abruptio Placentae
Monkey Diseases
Pregnancy
Placenta
Trophoblasts
Plasma total homocysteine, pregnancy complications, and adverse pregnancy outcomes: the Hordaland Homocysteine study. (1/87)
BACKGROUND: Total homocysteine (tHcy) measured in serum or plasma is a marker of folate status and a risk factor for cardiovascular disease. OBJECTIVE: Our objective was to investigate associations between tHcy and complications and adverse outcomes of pregnancy. DESIGN: Plasma tHcy values measured in 1992-1993 in 5883 women aged 40-42 y were compared with outcomes and complications of 14492 pregnancies in the same women that were reported to the Medical Birth Registry of Norway from 1967 to 1996. RESULTS: When we compared the upper with the lower quartile of plasma tHcy, the adjusted risk for preeclampsia was 32% higher [odds ratio (OR): 1. 32; 95% CI: 0.98, 1.77; P for trend = 0.02], that for prematurity was 38% higher (OR: 1.38; 95% CI: 1.09, 1.75; P for trend = 0.005), and that for very low birth weight was 101% higher (OR: 2.01; 95% CI: 1.23, 3.27; P for trend = 0.003). These associations were stronger during the years closest to the tHcy determination (1980-1996), when there was also a significant relation between tHcy concentration and stillbirth (OR: 2.03; 95% CI: 0.98, 4.21; P for trend = 0.02). Neural tube defects and clubfoot had significant associations with plasma tHcy. Placental abruption had no relation with tHcy quartile, but the adjusted OR when tHcy concentrations >15 micromol/L were compared with lower values was 3.13 (95% CI: 1.63, 6. 03; P = 0.001). CONCLUSION: Elevated tHcy concentration is associated with common pregnancy complications and adverse pregnancy outcomes. (+info)Primary aldosteronism in pregnancy. (2/87)
Aldosteronism is a rare complication of pregnancy. We report a case of a 26-year-old woman who became pregnant soon after a diagnosis of primary aldosteronism due to left adrenal adenoma was made. Only oral potassium supplementation was required in addition to routine prenatal care until 36 weeks' gestation. Subsequently, antihypertensive medication was needed to control elevated blood pressure. A healthy male infant was delivered by cesarean section because of abruptio placentae. The postoperative course was uneventful. Left adrenalectomy was conducted eight months after delivery under laparoscopic visualization. In this case report, we discuss management of aldosteronism in pregnancy and review the literature. (+info)Placental abruption and perinatal mortality in the United States. (3/87)
Placental abruption is an uncommon obstetric complication associated with high perinatal mortality rates. The authors explored the associations of abruption with fetal growth restriction, preterm delivery, and perinatal survival. The study was based on 7,508,655 singleton births delivered in 1995 and 1996 in the United States. Abruption was recorded in 6.5 per 1,000 births. Perinatal mortality was 119 per 1,000 births with abruption compared with 8.2 per 1,000 among all other births. The high mortality with abruption was due, in part, to its strong association with preterm delivery; 55% of the excess perinatal deaths with abruption were due to early delivery. Furthermore, babies in the lowest centile of weight (<1% adjusted for gestational age) were almost nine times as likely to be born with abruption than those in the heaviest (> or =90%) birth weight centiles. This relative risk progressively declined with higher birth weight centiles. After controlling for fetal growth restriction and early delivery, the high risk of perinatal death associated with abruption persisted. Even babies born at 40 weeks of gestation and birth weight of 3,500-3,999 g (where mortality was lowest) had a 25-fold higher mortality with abruption. The link between fetal growth restriction and abruption suggests that the origins of abruption lie at least in midpregnancy and perhaps even earlier. (+info)Social deprivation and the causes of stillbirth and infant mortality. (4/87)
AIMS: To investigate the relation between social deprivation and causes of stillbirth and infant mortality. METHODS: Stillbirths and infant deaths in 6347 enumeration districts in Wales were linked with the Townsend score of social deprivation. In 1993-98 there were 211 072 live births, 1147 stillbirths, and 1223 infant deaths. Poisson regression analysis was used to estimate the magnitude of effect for associations between the Townsend score and categories of death by age and the causes of death. The relative risk of death between most and least deprived enumeration districts was derived. RESULTS: Relative risk of combined stillbirth and infant death was 1.53 (95% CI 1.35 to 1.74) in the most deprived compared with the least deprived enumeration districts. The early neonatal mortality rate was not significantly associated with deprivation. Sudden infant death syndrome showed a 307% (95% CI 197% to 456%) increase in mortality across the range of deprivation. Deaths caused by specific conditions and infection were also associated with deprivation, but there was no evidence of a significant association with deaths caused by placental abruption, intrapartum asphyxia, and prematurity. CONCLUSIONS: Collaborative public health action at national and local level to target resources in deprived communities and reduce these inequalities in child health is required. Early neonatal mortality rates and deaths from intrapartum asphyxia and prematurity are not significantly associated with deprivation and may be more appropriate quality of clinical care indicators than stillbirth, perinatal, and neonatal mortality rates. (+info)Placental abruption among singleton and twin births in the United States: risk factor profiles. (5/87)
The authors performed a population-based epidemiologic study to evaluate and contrast risk factor profiles for placental abruption among singleton and twin gestations. Data were derived from linked US birth/infant death files for 1995 and 1996, comprising 7,465,858 singleton births and 193,266 twin births. The authors also evaluated effect modification between smoking and hypertension and the effect of a dose-response relation with number of cigarettes smoked daily on abruption risk. Abruption was recorded in 5.9 per 1,000 singleton births and 12.2 per 1,000 twin births. Risk factors for abruption among singleton and twin births, respectively, included preterm premature rupture of membranes (adjusted relative risks (RRs) = 4.89 and 2.01), eclampsia (RRs = 3.58 and 1.67), anemia (RRs = 2.23 and 2.33), hydramnios (RRs = 2.04 and 1.66), renal disorders (RRs = 1.54 and 2.56), and intrapartum fever (>100 degrees F) (RRs = 1.17 and 1.69). Chronic hypertension (RR = 2.38) and pregnancy-induced hypertension (RR = 2.34) were risk factors for abruption in singleton births but not in twin births. Number of cigarettes smoked daily demonstrated a dose-response trend for abruption risk in singletons and twins. Abruption was more likely to occur among smokers with chronic hypertension (RRs = 4.66 and 3.15) and eclampsia (RRs = 6.28 and 5.08). The authors conclude that abruption is twice as likely to occur in twins as in singletons with differing risk factor profiles. This suggests that abruption in twins may result from different pathophysiologic processes. (+info)Quantitative digital analysis of regional placental perfusion using power Doppler in placental abruption. (6/87)
PURPOSE: To apply digital imaging techniques to the quantification of placental vascularity using power Doppler. MATERIALS AND METHODS: Regional placental blood flow was measured in a case of large placental abruption, shortly after presentation and 1 week later. Images were stored digitally and analysed using purpose-designed software (CQ Analysis) to extract and measure vascular energy information. The integrated color energy (ICE) was determined in the main body of placental tissue and in a cotyledon isolated by the retroplacental clot. RESULTS: Initial assessment at 25 weeks showed only a small difference in integrated energy between normal placenta and the isolated cotyledon (ICE ratio 1.44, P < 0.04). One week later, perfusion in the isolated cotyledon had fallen both on qualitative and quantitative assessment (ICE ratio 3.98, P < 0.0001). This area subsequently became devascularized. CONCLUSION: Placental perfusion may be quantified using digital power Doppler analysis. Further studies are indicated to evaluate its role in assessing regional and/or global placental perfusion as well as fetal organ perfusion. (+info)Uterine artery Doppler velocimetry and the outcome of pregnancies resulting from ICSI. (7/87)
BACKGROUND: An increased incidence of pregnancy complications following assisted reproduction has been reported. The use of uterine artery Doppler ultrasound may aid the prediction of such complications. METHODS: Doppler was performed at 18-24 weeks gestation in 114 singleton and 32 twin pregnancies after intracytoplasmic sperm injection (ICSI) and compared with a control group matched for age, parity and plurality. Outcome variables included gestational age at delivery, prematurity, preterm premature rupture of membrane (PPROM), birth weight, birth weight discordance of >20% in twins, small for gestational age (SGA), mode of delivery, development of pre-eclampsia and placental abruption. RESULTS: Compared with the controls, there were no significant differences concerning uterine Doppler parameters, pregnancy complications and the neonatal outcome, either in singleton or in twin pregnancies. According to Doppler results and/or risk factors by medical history, 42% of singleton ICSI and 39% of spontaneous singleton pregnancies were considered as high risk. In singletons, abnormal Doppler findings were associated with pre-eclampsia in 22% and SGA in 26% of ICSI patients, compared with 33 and 21% in controls; in contrast, 0 and 10% in ICSI and 3 and 6% in controls showed these complications but no risk factors respectively. No correlation was found between PPROM, prematurity, the rate of Caesarean section and pathological Doppler results. CONCLUSIONS: Uterine Doppler examination holds the potential to identify patients with an increased risk for developing pregnancy complications. According to our results, this risk is not elevated after ICSI treatment, therefore the decision of offering an intensified antenatal care should be based on the results of Doppler examination or risks by medical history rather than the mode of conception. (+info)Review of unexplained infertility and obstetric outcome: a 10 year review. (8/87)
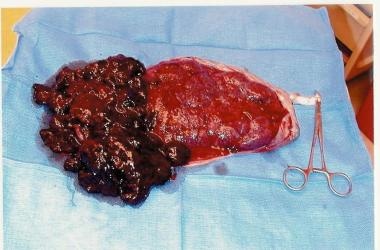
BACKGROUND: Increased maternal and fetal risks have been reported in pregnancies following unexplained infertility. Our aims were to examine the obstetric and perinatal outcome of singleton pregnancies in couples with unexplained infertility and explore the impact of fertility treatment. METHODS: Women with unexplained infertility were identified from the Aberdeen Fertility Clinic Database. Their unit numbers were matched against the Aberdeen Maternity and Neonatal Databank (AMND) in order to extract obstetric records of those women with subsequent pregnancy outcomes. The general obstetric population served as a control group. RESULTS: Women with unexplained infertility were older [30.8 versus 27.9 years, 95% confidence interval (CI) for difference = +2.4 to +3.4] and more likely to be primiparous (59 versus 40%, 95% CI = +1.3 to +1.9). After adjusting for age and parity they had a higher incidence of pre-eclampsia, abruptio placentae, preterm labour, emergency Caesarean section and induction of labour in comparison with the general population (P < 0.05). Perinatal outcome did not differ between women with unexplained infertility and those of the general population. The multiple pregnancy rate was 5.4% higher following fertility treatment than in women who conceived spontaneously (95% CI = +2.8 to +9.7). CONCLUSIONS: Women with unexplained infertility are at higher risk of obstetric complications which persist even after adjusting for age, parity and fertility treatment. The reasons are however unclear and merit further study. (+info)Abruptio placentae, also known as placental abruption, is a medical condition that occurs when the placenta separates from the uterus before the baby is born. The placenta is an organ that develops in the uterus during pregnancy to provide oxygen and nutrients to the growing fetus.
In abruptio placentae, the separation of the placenta from the uterus can cause bleeding, which can be serious or life-threatening for both the mother and the baby. The severity of the condition depends on how much of the placenta has separated from the uterus and how much bleeding has occurred.
Abruptio placentae can cause a range of symptoms, including vaginal bleeding, abdominal pain, contractions, and fetal distress. In severe cases, it can lead to preterm labor, low birth weight, and even stillbirth. The exact cause of abruptio placentae is not always known, but risk factors include high blood pressure, smoking, cocaine use, trauma to the abdomen, and advanced maternal age. Treatment may involve hospitalization, bed rest, medication to prevent contractions, or delivery of the baby if the pregnancy is at term.
There is no single medical definition for "Monkey Diseases." However, monkeys can carry and be infected with various diseases that are zoonotic, meaning they can be transmitted from animals to humans. Some examples include:
1. Simian Immunodeficiency Virus (SIV): A virus similar to Human Immunodeficiency Virus (HIV) that causes AIDS in monkeys. It is not typically harmful to monkeys but can cause AIDS in humans if transmitted, which is rare.
2. Herpes B Virus: Also known as Macacine herpesvirus 1 or Cercopithecine herpesvirus 1, it is a virus that commonly infects macaque monkeys. It can be transmitted to humans through direct contact with an infected monkey's saliva, eye fluid, or cerebrospinal fluid, causing a severe and potentially fatal illness called B encephalitis.
3. Tuberculosis (TB): Monkeys can contract and transmit tuberculosis to humans, although it is not common.
4. Simian Retrovirus (SRV): A virus that can infect both monkeys and great apes, causing immunodeficiency similar to HIV/AIDS in humans. It is not known to infect or cause disease in humans.
5. Various parasitic diseases: Monkeys can carry and transmit several parasites, including malaria-causing Plasmodium species, intestinal worms, and other parasites that can affect human health.
It's important to note that while monkeys can carry and transmit these diseases, the risk of transmission is generally low, and most cases occur in individuals who have close contact with monkeys, such as primatologists, zookeepers, or laboratory workers. Always follow safety guidelines when interacting with animals, including monkeys, to minimize the risk of disease transmission.
Fetal death, also known as stillbirth or intrauterine fetal demise, is defined as the death of a fetus at 20 weeks of gestation or later. The criteria for defining fetal death may vary slightly by country and jurisdiction, but in general, it refers to the loss of a pregnancy after the point at which the fetus is considered viable outside the womb.
Fetal death can occur for a variety of reasons, including chromosomal abnormalities, placental problems, maternal health conditions, infections, and umbilical cord accidents. In some cases, the cause of fetal death may remain unknown.
The diagnosis of fetal death is typically made through ultrasound or other imaging tests, which can confirm the absence of a heartbeat or movement in the fetus. Once fetal death has been diagnosed, medical professionals will work with the parents to determine the best course of action for managing the pregnancy and delivering the fetus. This may involve waiting for labor to begin naturally, inducing labor, or performing a cesarean delivery.
Experiencing a fetal death can be a very difficult and emotional experience for parents, and it is important for them to receive supportive care from their healthcare providers, family members, and friends. Grief counseling and support groups may also be helpful in coping with the loss.
Pregnancy is a physiological state or condition where a fertilized egg (zygote) successfully implants and grows in the uterus of a woman, leading to the development of an embryo and finally a fetus. This process typically spans approximately 40 weeks, divided into three trimesters, and culminates in childbirth. Throughout this period, numerous hormonal and physical changes occur to support the growing offspring, including uterine enlargement, breast development, and various maternal adaptations to ensure the fetus's optimal growth and well-being.
Placental diseases, also known as placental pathologies, refer to a group of conditions that affect the development and function of the placenta during pregnancy. The placenta is an organ that develops in the uterus during pregnancy and provides oxygen and nutrients to the developing fetus while removing waste products.
Placental diseases can have serious consequences for both the mother and the fetus, including preterm labor, growth restriction, stillbirth, and long-term health problems for the child. Some common placental diseases include:
1. Placental abruption: This occurs when the placenta separates from the uterine wall before delivery, causing bleeding and potentially harming the fetus.
2. Placental previa: This is a condition where the placenta implants in the lower part of the uterus, covering the cervix. It can cause bleeding and may require cesarean delivery.
3. Preeclampsia: This is a pregnancy-related disorder characterized by high blood pressure and damage to organs such as the liver and kidneys. Placental dysfunction is thought to play a role in its development.
4. Intrauterine growth restriction (IUGR): This occurs when the fetus does not grow properly due to poor placental function, leading to low birth weight and potential health problems.
5. Chorioamnionitis: This is an infection of the membranes surrounding the fetus, which can lead to preterm labor and other complications.
6. Placental infarction: This occurs when a portion of the placenta dies due to a lack of blood flow, which can lead to growth restriction or stillbirth.
Prompt diagnosis and treatment of placental diseases are essential for ensuring the best possible outcomes for both the mother and the fetus.
The placenta is an organ that develops in the uterus during pregnancy and provides oxygen and nutrients to the growing baby through the umbilical cord. It also removes waste products from the baby's blood. The placenta attaches to the wall of the uterus, and the baby's side of the placenta contains many tiny blood vessels that connect to the baby's circulatory system. This allows for the exchange of oxygen, nutrients, and waste between the mother's and baby's blood. After the baby is born, the placenta is usually expelled from the uterus in a process called afterbirth.
A Cesarean section, often referred to as a C-section, is a surgical procedure used to deliver a baby. It involves making an incision through the mother's abdomen and uterus to remove the baby. This procedure may be necessary when a vaginal delivery would put the mother or the baby at risk.
There are several reasons why a C-section might be recommended, including:
* The baby is in a breech position (feet first) or a transverse position (sideways) and cannot be turned to a normal head-down position.
* The baby is too large to safely pass through the mother's birth canal.
* The mother has a medical condition, such as heart disease or high blood pressure, that could make vaginal delivery risky.
* The mother has an infection, such as HIV or herpes, that could be passed to the baby during a vaginal delivery.
* The labor is not progressing and there are concerns about the health of the mother or the baby.
C-sections are generally safe for both the mother and the baby, but like any surgery, they do carry some risks. These can include infection, bleeding, blood clots, and injury to nearby organs. In addition, women who have a C-section are more likely to experience complications in future pregnancies, such as placenta previa or uterine rupture.
If you have questions about whether a C-section is necessary for your delivery, it's important to discuss your options with your healthcare provider.
Trophoblasts are specialized cells that make up the outer layer of a blastocyst, which is a hollow ball of cells that forms in the earliest stages of embryonic development. In humans, this process occurs about 5-6 days after fertilization. The blastocyst consists of an inner cell mass (which will eventually become the embryo) and an outer layer of trophoblasts.
Trophoblasts play a crucial role in implantation, which is the process by which the blastocyst attaches to and invades the lining of the uterus. Once implanted, the trophoblasts differentiate into two main layers: the cytotrophoblasts (which are closer to the inner cell mass) and the syncytiotrophoblasts (which form a multinucleated layer that is in direct contact with the maternal tissues).
The cytotrophoblasts proliferate and fuse to form the syncytiotrophoblasts, which have several important functions. They secrete enzymes that help to degrade and remodel the extracellular matrix of the uterine lining, allowing the blastocyst to implant more deeply. They also form a barrier between the maternal and fetal tissues, helping to protect the developing embryo from the mother's immune system.
Additionally, trophoblasts are responsible for the formation of the placenta, which provides nutrients and oxygen to the developing fetus and removes waste products. The syncytiotrophoblasts in particular play a key role in this process by secreting hormones such as human chorionic gonadotropin (hCG), which helps to maintain pregnancy, and by forming blood vessels that allow for the exchange of nutrients and waste between the mother and fetus.
Abnormalities in trophoblast development or function can lead to a variety of pregnancy-related complications, including preeclampsia, intrauterine growth restriction, and gestational trophoblastic diseases such as hydatidiform moles and choriocarcinomas.
 Alan Clemetson
Alan Clemetson
List of ICD-9 codes 630-679: complications of pregnancy, childbirth, and the puerperium
Couvelaire uterus
Cocaine intoxication
Alkali denaturation test
Vaginal bleeding
Eclampsia
Peter C. Klatsky
MTHFD1
Anemia in pregnancy
Maternal mortality in the United States
Placental alpha microglobulin-1 (PAMG-1)
Go Getters
Thyroid disease in pregnancy
Caesarean section
Thrombophilia
Dr. Jose Fabella Memorial Hospital
Childbirth
Ferguson v. City of Charleston
List of MeSH codes (C13)
Placental disease
Black Women's Health Imperative
Disseminated intravascular coagulation
Renal cortical necrosis
Prenatal cocaine exposure
Previa18
- Maternal cigarette smoking as a risk factor for placental abruption, placenta previa, and uterine bleeding in pregnancy. (medscape.com)
- Placentae previa and abruptio placentae. (medscape.com)
- Previous cesarean delivery and risks of placenta previa and placental abruption. (legehandboka.no)
- Ultrasonography helps to determine the location of the placenta in order to exclude placenta previa. (medscape.com)
- Ultrasonographic studies do help to quickly diagnose placenta previa as the etiology of bleeding, if present. (medscape.com)
- Perinatal outcome and near-miss morbidity between placenta previa versus abruptio placentae. (bvsalud.org)
- To compare perinatal outcome and near-miss morbidities between placenta previa versus abruptio placentae in patients of antepartum haemorrhage (APH). (bvsalud.org)
- Patients with APH diagnosed as placenta previa and abruptio placentae who delivered after 24 weeks of pregnancy were selected from labour room. (bvsalud.org)
- Abruptio placentae carry significantly higher perinatal mortality and near-miss morbidity than placenta previa . (bvsalud.org)
- Abruptio placenta Placenta previa Velamenous insertion Long - short cord: Umbilical cord length is determined by the amount of fetal movement. (ibis-birthdefects.org)
- Placenta previa at term occurs in about one in 200 births. (midwiferytoday.com)
- Matsuda Y, Hayashi K, Shiozaki A, Kawamichi Y, Satoh S, Saito S, 2011 Comparison of risk factors for placental abruption and placenta previa: case-cohort study. (springer.com)
- Placenta previa is a problem of pregnancy in which the placenta grows in the lowest part of the womb (uterus) and covers all or part of the opening to the cervix. (stlukes-stl.com)
- Placenta previa occurs in 1 out of 200 pregnancies. (stlukes-stl.com)
- The main symptom of placenta previa is sudden bleeding from the vagina . (stlukes-stl.com)
- Nearly all women with placenta previa need a C-section . (stlukes-stl.com)
- Placenta previa can be dangerous to both you and your baby. (stlukes-stl.com)
- The placental associations are umblical cord anomalies, single umblical artery, abruptio placente, placenta previa, amnion nodosum and villitis due to rubella, cytomegalovirus, syphilis and Bartonella infection. (ispub.com)
Placental abruption8
- Placenta abruptio (also called placental abruption) is when the placenta separates from the inner wall of the uterus before the baby is born. (medlineplus.gov)
- Placental abruption (abruptio placentae) is premature separation of the placenta from the uterus, usually after 20 weeks gestation. (msdmanuals.com)
- Placental abruption is a condition which occurs when the placenta prematurely separates from the wall of the uterus. (huggies.com.au)
- Women with SCH are at greater risk for placental abruption or abruptio placenta. (justmommies.com)
- Placental abruption is when the placenta tears away from the uterus. (justmommies.com)
- Placental abruption (abruptio placentae) is an uncommon yet serious complication of pregnancy. (theairambulanceservice.org.uk)
- Placental abruption occurs when the placenta partly or completely separates from the inner wall of the uterus before delivery. (theairambulanceservice.org.uk)
- Definition Abruptio placentae (also known as placental abruption) is the premature separation of the placenta that occurs late in the pregnancy.nurseslabs Pathophysiology The placenta has implanted in the correct location. (curejoy.com)
Separation of the placenta1
- Partial separation of the placenta (also called the afterbirth) from the wall of the uterus in the last 3 months of pregnancy. (nmihi.com)
Uterus11
- The placenta connects the fetus (unborn baby) to the mother's uterus. (medlineplus.gov)
- In a small number of pregnancies, the placenta detaches (pulls itself from the wall of the uterus) too early. (medlineplus.gov)
- A catheter is passed via the vagina through the cervix and into the uterus to the developing placenta under ultrasound guidance. (ibis-birthdefects.org)
- Ideally, this occurs as the uterus contracts down which helps the placenta to detach. (huggies.com.au)
- Bleeding can be concealed e.g. which occurs when the blood is trapped between the placenta and the uterus, effectively containing the blood within this space. (huggies.com.au)
- SCH or Subchorionic Hematoma is a gathering of blood between the membranes of the placenta and the uterus. (justmommies.com)
- The clot can release completely from the uterus and cause the fetus and placenta to miscarry. (justmommies.com)
- The placenta develops in the uterus during pregnancy. (theairambulanceservice.org.uk)
- The placenta is an organ in the mother's uterus that is responsible for providing necessary nutrition to the growing baby. (curejoy.com)
- It's mainly caused by uterus (Uterine Atony) and placenta (Placenta Percreta, Placenta Accreta, Placenta Increta). (curejoy.com)
- Placenta accreta , when the placenta embeds too deep within the uterus, is one such condition. (vbacfacts.com)
Hemorrhage1
- Blood may also remain behind the placenta (concealed hemorrhage). (msdmanuals.com)
Prematurely1
- If the placenta partially separates prematurely, the child's life will be endangered. (nmihi.com)
Pregnancy7
- We genotyped 62 women with a pregnancy history complicated by severe abruptio placentae and 184 control pregnancies. (nih.gov)
- A (R653Q) polymorphism are almost three times more likely to develop severe abruptio placentae during their pregnancy than women who are 'RQ' or 'RR. (nih.gov)
- 10 to 17% of patients have abruptio placentae in a future pregnancy. (nmihi.com)
- The placenta grows during pregnancy and feeds the developing baby. (stlukes-stl.com)
- During pregnancy, the placenta moves as the womb stretches and grows. (stlukes-stl.com)
- It is very common for the placenta to be low in the womb in early pregnancy. (stlukes-stl.com)
- But as the pregnancy continues, the placenta moves to the top of the womb. (stlukes-stl.com)
Fetal1
- The fetal surface of placenta showed grey white areas. (ispub.com)
Vaginal2
- On abdominal or vaginal ultrasound where the placenta can be seen sheared away from the uterine wall. (huggies.com.au)
- If the placenta covers all or part of the cervix, a vaginal delivery can cause severe bleeding. (stlukes-stl.com)
Separates1
- If the placenta separates from the uterine wall, the health of the fetus is in danger. (justmommies.com)
Uterine wall3
- In most pregnancies, the placenta stays attached to the upper part of the uterine wall. (medlineplus.gov)
- Sometimes the blood that collects when the placenta detaches stays between the placenta and uterine wall, so you may not have bleeding from your vagina. (medlineplus.gov)
- The placenta is the baby's main life line for oxygen and nutrients, and unless it is adhering firmly to the uterine wall there is an interruption in the flow of these vital elements. (huggies.com.au)
Abnormalities1
- The placenta did not show any gross or histopathologic abnormalities. (hindawi.com)
Maternal1
- We investigated the importance of maternal hypertension and cigarette smoking, and their interaction, as risk factors for abruptio placentae, using Massachusetts birth certificate data for 1987-1988. (nih.gov)
Perinatal outcome1
- Abu-Heija A, al-Chalabi H, el-Iloubani N. Abruptio placentae: risk factors and perinatal outcome. (medscape.com)
Coagulation1
- Women with PIH are at a greater risk of abruptio placentae, cerebrovascular events, organ failure and disseminated intravascular coagulation. (springer.com)
Pregnancies1
- A (R653Q) polymorphism showed increased frequency of the 'QQ' homozygote genotype in pregnancies affected by severe abruptio placentae compared to control pregnancies (odds ratio 2.85 (1.47-5.53), P = 0.002). (nih.gov)
Diagnosis1
- The diagnosis in these patients is made retrospectively by finding an organized blood clot or a depressed area on a delivered placenta. (medscape.com)
Trimester1
- By the third trimester, the placenta should be near the top of the womb, so the cervix is open for delivery. (stlukes-stl.com)
Fetus2
- The placenta is the lifeline of a fetus. (medlineplus.gov)
- Although often thought of as separate and distinct circulations, a baseline amount of bidirectional flow across the placenta between mother and fetus is considered physiologic. (hindawi.com)
Cervix3
- Sometimes, the placenta partly or completely covers the cervix. (stlukes-stl.com)
- Marginal: The placenta is next to the cervix but does not cover the opening. (stlukes-stl.com)
- the shortening and opening of the cervix during the first stage, descent and birth of the baby during the second, the delivery of the placenta during the third, and the recovery of the mother and infant during the fourth stage, which is referred to as the postpartum . (wikipedia.org)
Preterm1
- She delivered a preterm, healthy baby and bits of placenta was sent for routine examination and culture. (ispub.com)
Intravascular1
- Coagulopathy (disseminated intravascular coagulopathy [DIC])-certain elements of the placenta are released into the mother's circulation causing blood clotting defects. (nmihi.com)
Severe1
- C (E429A), and risk of severe abruptio placentae. (nih.gov)
Lesions1
- Villous capillary lesions of the placenta:distinctions between chorangioma, chorangiomatosis, and chorangioma. (ispub.com)
Unborn1
- The placenta carries all nourishment and oxygen to the unborn child. (nmihi.com)
Decidua1
- Separation results in bleeding into the decidua basalis behind the placenta (retroplacentally). (msdmanuals.com)
Partial1
- Partial: The placenta covers part of the cervical opening. (stlukes-stl.com)
Umbilical1
- The placenta weighed 650 gms and measured 21x13x2cms.There was an eccentrically attached umbilical cord measuring 15cms in length. (ispub.com)
Vascular3
- The hypoxic placenta then releases various placental factors such as soluble vascular endothelial growth factor receptor-1 (sVEGFR-1), which then binds vascular endothelial growth factor (VEGF) and placental growth factor (PGF), causing endothelial cell and placental dysfunction by preventing them from binding endothelial cell receptors. (medscape.com)
- Microscopically, the placenta showed enlarged villi with numerous vascular channels per villi, increased syncitial knots and areas of calcification (Fig 1). (ispub.com)
- In normal placenta, chorionic villi rarely contain more than 5 vascular channels. (ispub.com)
Hypertension1
- Chronic hypertension, cigarette smoking, and abruptio placentae. (nih.gov)
Genetic1
- Abruptio placentae risk and genetic variations in mitochondrial biogenesis and oxidative phosphorylation: replication of a candidate gene association study. (medscape.com)
Oxygen1
- When the placenta is not functioning properly, the baby is not getting essential oxygen and nutrients, and growth retardation is a real possibility. (healthy.net)
Risk factors1
- 11. Risk factors predisposing to abruptio placentae. (nih.gov)
Practice1
- However, eating the placenta has not been a traditional practice among most cultures, and no research has so far proved its health benefits. (curejoy.com)
Baby1
- The correct time for the placenta to separate is after the baby has been born. (huggies.com.au)
Pain2
- If more than half the placenta detaches, you may have belly pain and heavy bleeding. (medlineplus.gov)
- Celeb moms vouch for the benefits of eating their own placenta, such as relief from postpartum pain and depression, replenishment of the iron lost during childbirth, and enhanced milk production. (curejoy.com)
Multiple1
- We used multiple logistic regression procedures to model data from 943 abruptio placentae cases and 10,648 randomly selected births. (nih.gov)