Aortic Valve
Aortic Valve Stenosis
Aortic Valve Insufficiency
Heart Valve Diseases
Heart Valve Prosthesis Implantation
Heart Valve Prosthesis
Bioprosthesis
Tricuspid Valve
Cardiac Catheterization
Mitral Valve Insufficiency
Aortic Valve Prolapse
Endocarditis, Bacterial
Mitral Valve Prolapse
Mitral Valve Stenosis
Echocardiography, Transesophageal
Venous Valves
Echocardiography
Cardiac Valve Annuloplasty
Treatment Outcome
Endocarditis
Tricuspid Valve Insufficiency
Catheterization
Mitral Valve Annuloplasty
Echocardiography, Doppler
Reoperation
Heart Defects, Congenital
Prosthesis Failure
Dilatation, Pathologic
Echocardiography, Doppler, Color
Severity of Illness Index
Balloon Valvuloplasty
Postoperative Complications
Follow-Up Studies
Multidetector Computed Tomography
Hemodynamics
Prosthesis Fitting
Suture Techniques
Pulmonary Valve Stenosis
Phonocardiography
Echocardiography, Three-Dimensional
Retrospective Studies
Chordae Tendineae
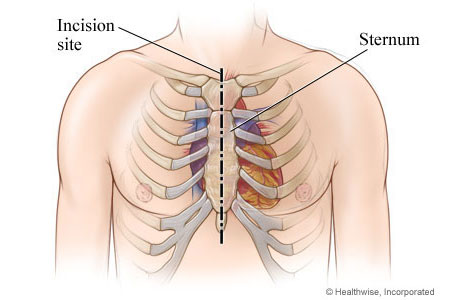
Sternum
Sclerosis
Heart Valves
Prospective Studies
Thoracic Surgery
Risk Factors
Pericardium
Cardiopulmonary Bypass
Risk Assessment
Heart Ventricles
Stroke Volume
Endocardial Fibroelastosis
Models, Cardiovascular
Ventricular Function, Left
Feasibility Studies
Chi-Square Distribution
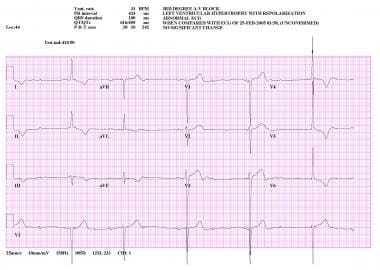
Atrioventricular Block
Aortic Coarctation
Aortic Stenosis, Subvalvular
Rheumatic Heart Disease
Polyethylene Terephthalates
Heart Arrest, Induced
Heart Neoplasms
Heart Septal Defects, Ventricular
Patient Selection
Coronary Artery Bypass
Tomography, X-Ray Computed
Surgical Procedures, Minimally Invasive
Embolism
Marfan Syndrome
Predictive Value of Tests
Ileocecal Valve
Aortography
Heart Sounds
Heart Murmurs
Kaplan-Meier Estimate
Hospital Mortality
Blood Flow Velocity
Pacemaker, Artificial
Swine
Cardiac Catheters
Glutaral
Thromboembolism
Aneurysm, Dissecting
Hypertrophy, Left Ventricular
Ventricular Dysfunction, Left
Prosthesis-Related Infections
Investigation of the theory and mechanism of the origin of the second heart sound. (1/2271)
To investigate further the origin of the second heart sound we studied human subjects, dogs, and a model in vitro of the cardiovascular system. Intra-arterial sound, pressure, and, where possible, flow and high speed cine (2,000 frames/sec) were utilized. The closure sound of the semilunar valves was of higher amplitude in be ventricles than in their respective arterial cavities. The direction of inscription of the main components of intra-arterial sound were opposite in direction to the components of intraventricular sound. Notches, representative of pressure increments, were noted on the ventricular pressure tracings and were coincident with the components of sound. The amplitude of the closure sound varied with diastolic pressure, but remained unchanged with augmentation of forward and retrograde aortic flow. Cines showed second sound to begin after complete valvular closure, and average leaflet closure rate was constant regardless of pressure. Hence, the semilunar valves, when closed, act as an elastic membrane and, when set into motion, generate compression and expansion of the blood, producing transient pressure changes indicative of sound. The magnitude of the initial stretch is related to the differential pressure between the arterial and ventricular chambers. Sound transients which follow the major components of the second sound appear to be caused by the continuing stretch and recoil of the leaflets. Clinically unexplained findings such as the reduced or absent second sound in calcific aortic stenosis and its paradoxical presence in congenital aortic stenosis may be explained by those observations. (+info)Acetylcholine-induced membrane potential changes in endothelial cells of rabbit aortic valve. (2/2271)
1. Using a microelectrode technique, acetylcholine (ACh)-induced membrane potential changes were characterized using various types of inhibitors of K+ and Cl- channels in rabbit aortic valve endothelial cells (RAVEC). 2. ACh produced transient then sustained membrane hyperpolarizations. Withdrawal of ACh evoked a transient depolarization. 3. High K+ blocked and low K+ potentiated the two ACh-induced hyperpolarizations. Charybdotoxin (ChTX) attenuated the ACh-induced transient and sustained hyperpolarizations; apamin inhibited only the sustained hyperpolarization. In the combined presence of ChTX and apamin, ACh produced a depolarization. 4. In Ca2+-free solution or in the presence of Co2+ or Ni2+, ACh produced a transient hyperpolarization followed by a depolarization. In BAPTA-AM-treated cells, ACh produced only a depolarization. 5. A low concentration of A23187 attenuated the ACh-induced transient, but not the sustained, hyperpolarization. In the presence of cyclopiazonic acid, the hyperpolarization induced by ACh was maintained after ACh removal; this maintained hyperpolarization was blocked by Co2+. 6. Both NPPB and hypertonic solution inhibited the membrane depolarization seen after ACh washout. Bumetanide also attenuated this depolarization. 7. It is concluded that in RAVEC, ACh produces a two-component hyperpolarization followed by a depolarization. It is suggested that ACh-induced Ca2+ release from the storage sites causes a transient hyperpolarization due to activation of ChTX-sensitive K+ channels and that ACh-activated Ca2+ influx causes a sustained hyperpolarization by activating both ChTX- and apamin-sensitive K+ channels. Both volume-sensitive Cl- channels and the Na+-K+-Cl- cotransporter probably contribute to the ACh-induced depolarization. (+info)Extent and severity of atherosclerotic involvement of the aortic valve and root in familial hypercholesterolaemia. (3/2271)
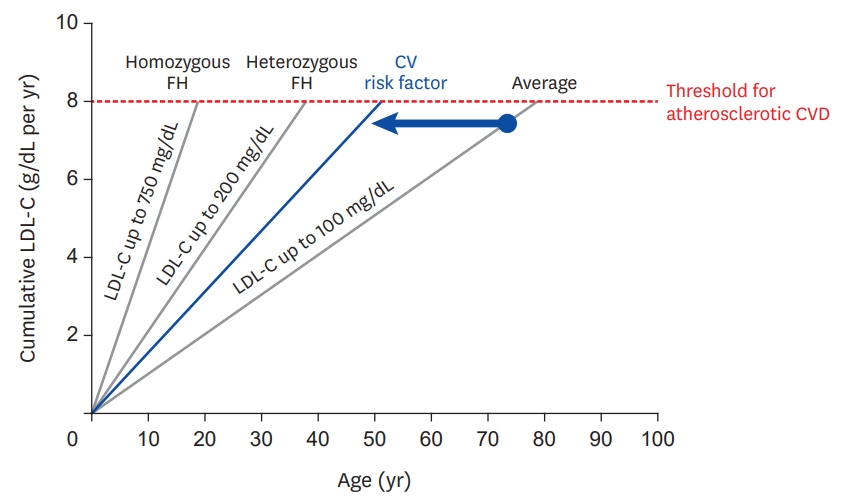
OBJECTIVE: To compare the frequency of valvar and supravalvar aortic stenosis in homozygous and heterozygous familial hypercholesterolaemia (FH). DESIGN: Analysis of life time cholesterol exposure and prevalence of aortic atherosclerosis in 84 consecutive cases attending a lipid clinic. SETTING: A tertiary referral centre in London. PATIENTS: Outpatients with FH (six homozygous, 78 heterozygous). INTERVENTIONS: Maintenance of lipid lowering treatment. MAIN OUTCOME MEASURES: Calculated cholesterol x years score (CYS) and echocardiographic measurement of aortic root diameter, aortic valve thickness, and transaortic gradient. RESULTS: Four homozygotes with a mean (SD) CYS of 387 (124) mmol/1 x years had severe aortic stenosis (treatment started after seven years of age), whereas the other two had echocardiographic evidence of supravalvar thickening but no aortic valve stenosis (treatment started before three years of age). On multivariate analysis, mean transaortic gradient correlated significantly with CYS (mean = 523 (175) mmol/1 x years) in heterozygotes (p = 0.0001), but only two had severe aortic valve and root involvement. CONCLUSIONS: In patients with familial hypercholesterolaemia, aortic stenosis is common in homozygotes, and aortic root involvement is always present despite the lower CYS than in heterozygotes. It appears to be determined by short term exposure to high cholesterol concentrations in early life. Conversely, aortic root and valve involvement are rare in heterozygotes and occur only with severe, prolonged hypercholesterolaemia, possibly accelerating age related degenerative effects. (+info)Bileaflet mechanical prostheses for aortic valve replacement in patients younger than 65 years and 65 years of age or older: major thromboembolic and hemorrhagic complications. (4/2271)
OBJECTIVE: To determine major thromboembolic and hemorrhagic complications and predictive risk factors associated with aortic valve replacement (AVR), using bileaflet mechanical prostheses (CarboMedics and St. Jude Medical). DESIGN: A case series. SETTING: Cardiac surgical services at the teaching institutions of the University of British Columbia. PATIENTS AND METHODS: Patients 2 age groups who had undergone AVR between 1989 and 1994 were studied. Group 1 comprised 384 patients younger than 65 years. Group 2 comprised 215 patients 65 years of age and older. RESULTS: The linearized rates of major thromboembolism (TE) occurring after AVR were 1.54%/patient-year for group 1 and 3.32%/patient-year for group 2; the rates for major TE occurring more than 30 days after AVR were 1.13%/patient-year for group 1 and 1.55%/patient-year for group 2. The crude rates for major TE occurring within 30 days of AVR were 1.04% for group 1 and 3.72% for group 2. The death rate from major TE in group 1 was 0.31%/patient-year and in group 2 was 0.88%/patient-year. Of the major TE events occurring within 30 days, 100% of patients in both age groups were inadequately anticoagulated at the time of the event, and for events occurring more than 30 days after AVR, 45% in group 1 and 57% in group 2 were inadequately anticoagulated (INR less than 2.0). The overall linearized rates of major hemorrhage were 1.54%/patient-year for group 1 and 2.21%/patient-year for group 2. There were no cases of prosthesis thrombosis in either group. The mean (and standard error) overall freedom from major TE for group 1 patients at 5 years was 95.6% (1.4%) and with exclusion of early events was 96.7% (1.3%); for group 2 patients the rates were 90.0% (3.2%) and 93.7% (3.0%), respectively. The mean (and SE) overall freedom from major and fatal TE and hemorrhage for group 1 patients was 90.1% (2.3%) and with exclusion of early events was 91.2% (2.3%); for group 2 patients the rates were 87.9% (3.1%) and 92.5% (2.9%), respectively. The 5-year rate for freedom from valve-related death for group 1 patients was 96.3% (2.1%) and for group 2 patients was 97.2% (1.2%). CONCLUSION: The thromboembolic and hemorrhagic complications after AVR with bileaflet mechanical prostheses occur more frequently and result in more deaths in patients 65 years of age and older than in patients years younger than 65 years. (+info)Minimally invasive aortic valve replacement through a transverse sternotomy: a word of caution. (5/2271)
OBJECTIVES: To compare aortic valve replacement (AVR) using a minimally invasive approach through a transverse sternotomy with the established approach of median sternotomy. DESIGN: Retrospective, case-control study. PATIENTS: Fourteen high risk patients (median age 78, Parsonnet score of 18%) who underwent AVR performed through a minimally invasive transverse sternotomy were compared with a historical group of patients matched for age, sex, and Parsonnet score who underwent AVR performed through a median sternotomy by the same surgeon. OUTCOME MEASURES: Cross clamp time, total bypass time, intensive care stay, postoperative in-hospital stay, morbidity, and mortality. RESULTS: There were two deaths in the minimally invasive group and none in the control group (NS). The cross clamp and total bypass times were longer in the minimally invasive group (67 and 92 minutes v 46 and 66 minutes, p < 0.001). There was a higher incidence of re-exploration for bleeding (14% v 0%) and paravalvar leaks (21% v 0%) in the minimally invasive group but these differences were not significant. The minimally invasive group had a longer postoperative in-hospital stay (p = 0.025). The incidence of mortality or major morbidity was 43% (six of 14) in the minimally invasive group and 7% (one of 14) in the matched pairs (p = 0.013). CONCLUSIONS: AVR can be performed through a transverse sternotomy but the operation takes longer and there is an unacceptably high incidence of morbidity and mortality. (+info)Role of glutaraldehyde in calcification of porcine aortic valve fibroblasts. (6/2271)
Glutaraldehyde-treated porcine aortic valve xenografts frequently fail due to calcification. Calcification in the prostheses begins intracellularly. In a previous study, various types of cell injury to canine valvular fibroblasts, including glutaraldehyde treatment, led to calcification. An influx of extracellular Ca2+ into the phosphate-rich cytosol was theorized to be the mechanism of calcification. To test the Ca2+ influx theory, cytosolic Ca2+ and Pi concentrations were assessed in glutaraldehyde-treated porcine aortic valve fibroblasts, and their relationship to a subsequent calcification was studied. Glutaraldehyde caused an immediate and sustained massive cytosolic Ca2+ increase that was dose dependent and a several-fold increase in Pi. Calcification of cells followed within a week. The earliest calcification was observed in blebs formed on glutaraldehyde-treated cells. Live control cells or cells fixed with glutaraldehyde in Ca2+-free solution did not calcify under the same conditions. Concomitant increases in Ca2+ and Pi in glutaraldehyde-treated cells appear to underlie the mechanism of calcification, and the presence of extracellular Ca2+ during glutaraldehyde fixation promotes calcification. (+info)Perivalvular abscesses associated with endocarditis; clinical features and prognostic factors of overall survival in a series of 233 cases. Perivalvular Abscesses French Multicentre Study. (7/2271)
AIMS: The purposes of this study were to determine the clinical features and to identify prognostic factors of abscesses associated with infective endocarditis. METHODS AND RESULTS: During a 5-year period from January 1989, 233 patients with perivalvular abscesses associated with infective endocarditis were enrolled in a retrospective multicentre study. Of the patients, 213 received medical surgical therapy and 20 medical therapy alone. No causative microorganism could be identified in 31% of cases. Sensitivity for the detection of abscesses was 36 and 80%, respectively using transthoracic and transoesophageal echocardiography. Surgical treatment consisted of primary suture of the abscess (38%), insertion of a felt aortic or mitral ring using Teflon or pericardium (42%), or debridment of the abscess cavity (20%). The 1 month operative mortality was 16%. Actuarial rates for overall survival at 3 and 27 months in operated patients were 75 +/- 10% and 59 +/- 11%, respectively. Increasing patient age, staphylococcal infection, and fistulization of the abscess were found to be independent risk factors in both 1 month and overall operative mortality. Renal failure was a risk factor predictive of operative mortality at 1 month, whereas uncontrolled infection and circumferential abscess were regarded as risk factors predictive of overall operative mortality. CONCLUSION: The data determined prognostic factors of abscesses associated with infective endocarditis. (+info)Syphilitic aortic regurgitation. An appraisal of surgical treatment. (8/2271)
During the 10 years from 1964 to 1973, fifteen patients with severe syphilitic aortic regurgitation were treated surgically at the National Heart Hospital. In thirteen the valve was replaced and in two it was repaired. In addition four had replacement of an aneurysmal ascending aorta with a Dacron graft and seven some form of plastic repair to the coronary ostia. Three patients died within 1 month of surgery and a further six during the follow-up period which varied from 1 to 55 months (mean 25-5). The six survivors have been followed-up for an average of 33 months. Factors contributing to this high mortality were analysed and it was found that the mean duration of effort dyspnoea was 22 months in the survivors compared with 48 months in those who had died. Similarly the average duration of nocturnal dyspnoea was 4 months in the survivors compared with a mean of 8 months in those who had died. Only six out of the fifteen patients had angina; this was present in two of the survivors and in four of the fatalities. The pulse pressure, heart size, and haemodynamic findings were similar in the two groups. The prognostic value of an elevated erythocyte sedimentation rate was also examined. It was concluded that preoperative investigations should include aortography, coronary arteriography, an assessment of left ventricular function, and whenever possible myocardial biopsy. These data were interpreted as suggesting that patients should be referred for surgery at an earlier stage in the disease--certainly before the onset of cardiac failure and--and that if this more aggresive attitude was adopted, as it has been in non-syphilitic cases of aortic valve disease, the present high mortality in this group would be reduced. (+info)The aortic valve is the valve located between the left ventricle (the lower left chamber of the heart) and the aorta (the largest artery in the body, which carries oxygenated blood from the heart to the rest of the body). It is made up of three thin flaps or leaflets that open and close to regulate blood flow. During a heartbeat, the aortic valve opens to allow blood to be pumped out of the left ventricle into the aorta, and then closes to prevent blood from flowing back into the ventricle when it relaxes. Any abnormality or damage to this valve can lead to various cardiovascular conditions such as aortic stenosis, aortic regurgitation, or infective endocarditis.
Aortic valve stenosis is a cardiac condition characterized by the narrowing or stiffening of the aortic valve, which separates the left ventricle (the heart's main pumping chamber) from the aorta (the large artery that carries oxygen-rich blood to the rest of the body). This narrowing or stiffening prevents the aortic valve from opening fully, resulting in reduced blood flow from the left ventricle to the aorta and the rest of the body.
The narrowing can be caused by several factors, including congenital heart defects, calcification (hardening) of the aortic valve due to aging, or scarring of the valve due to rheumatic fever or other inflammatory conditions. As a result, the left ventricle must work harder to pump blood through the narrowed valve, which can lead to thickening and enlargement of the left ventricular muscle (left ventricular hypertrophy).
Symptoms of aortic valve stenosis may include chest pain or tightness, shortness of breath, fatigue, dizziness or fainting, and heart palpitations. Severe aortic valve stenosis can lead to serious complications such as heart failure, arrhythmias, or even sudden cardiac death. Treatment options may include medications to manage symptoms, lifestyle changes, or surgical intervention such as aortic valve replacement.
Aortic valve insufficiency, also known as aortic regurgitation or aortic incompetence, is a cardiac condition in which the aortic valve does not close properly during the contraction phase of the heart cycle. This allows blood to flow back into the left ventricle from the aorta, instead of being pumped out to the rest of the body. As a result, the left ventricle must work harder to maintain adequate cardiac output, which can lead to left ventricular enlargement and heart failure over time if left untreated.
The aortic valve is a trileaflet valve that lies between the left ventricle and the aorta. During systole (the contraction phase of the heart cycle), the aortic valve opens to allow blood to be pumped out of the left ventricle into the aorta and then distributed to the rest of the body. During diastole (the relaxation phase of the heart cycle), the aortic valve closes to prevent blood from flowing back into the left ventricle.
Aortic valve insufficiency can be caused by various conditions, including congenital heart defects, infective endocarditis, rheumatic heart disease, Marfan syndrome, and trauma. Symptoms of aortic valve insufficiency may include shortness of breath, fatigue, chest pain, palpitations, and edema (swelling). Diagnosis is typically made through physical examination, echocardiography, and other imaging studies. Treatment options depend on the severity of the condition and may include medication, surgery to repair or replace the aortic valve, or a combination of both.
Heart valve diseases are a group of conditions that affect the function of one or more of the heart's four valves (tricuspid, pulmonic, mitral, and aortic). These valves are responsible for controlling the direction and flow of blood through the heart. Heart valve diseases can cause the valves to become narrowed (stenosis), leaky (regurgitation or insufficiency), or improperly closed (prolapse), leading to disrupted blood flow within the heart and potentially causing symptoms such as shortness of breath, fatigue, chest pain, and irregular heart rhythms. The causes of heart valve diseases can include congenital defects, age-related degenerative changes, infections, rheumatic heart disease, and high blood pressure. Treatment options may include medications, surgical repair or replacement of the affected valve(s), or transcatheter procedures.
The mitral valve, also known as the bicuspid valve, is a two-leaflet valve located between the left atrium and left ventricle in the heart. Its function is to ensure unidirectional flow of blood from the left atrium into the left ventricle during the cardiac cycle. The mitral valve consists of two leaflets (anterior and posterior), the chordae tendineae, papillary muscles, and the left atrial and ventricular myocardium. Dysfunction of the mitral valve can lead to various heart conditions such as mitral regurgitation or mitral stenosis.
Heart valve prosthesis implantation is a surgical procedure where an artificial heart valve is inserted to replace a damaged or malfunctioning native heart valve. This can be necessary for patients with valvular heart disease, including stenosis (narrowing) or regurgitation (leaking), who do not respond to medical management and are at risk of heart failure or other complications.
There are two main types of artificial heart valves used in prosthesis implantation: mechanical valves and biological valves. Mechanical valves are made of synthetic materials, such as carbon and metal, and can last a long time but require lifelong anticoagulation therapy to prevent blood clots from forming. Biological valves, on the other hand, are made from animal or human tissue and typically do not require anticoagulation therapy but may have a limited lifespan and may need to be replaced in the future.
The decision to undergo heart valve prosthesis implantation is based on several factors, including the patient's age, overall health, type and severity of valvular disease, and personal preferences. The procedure can be performed through traditional open-heart surgery or minimally invasive techniques, such as robotic-assisted surgery or transcatheter aortic valve replacement (TAVR). Recovery time varies depending on the approach used and individual patient factors.
A heart valve prosthesis is a medical device that is implanted in the heart to replace a damaged or malfunctioning heart valve. The prosthetic valve can be made of biological tissue (such as from a pig or cow) or artificial materials (such as carbon or polyester). Its function is to allow for the proper directional flow of blood through the heart, opening and closing with each heartbeat to prevent backflow of blood.
There are several types of heart valve prostheses, including:
1. Mechanical valves: These are made entirely of artificial materials and have a longer lifespan than biological valves. However, they require the patient to take blood-thinning medication for the rest of their life to prevent blood clots from forming on the valve.
2. Bioprosthetic valves: These are made of biological tissue and typically last 10-15 years before needing replacement. They do not require the patient to take blood-thinning medication, but there is a higher risk of reoperation due to degeneration of the tissue over time.
3. Homografts or allografts: These are human heart valves that have been donated and preserved for transplantation. They have similar longevity to bioprosthetic valves and do not require blood-thinning medication.
4. Autografts: In this case, the patient's own pulmonary valve is removed and used to replace the damaged aortic valve. This procedure is called the Ross procedure and has excellent long-term results, but it requires advanced surgical skills and is not widely available.
The choice of heart valve prosthesis depends on various factors, including the patient's age, overall health, lifestyle, and personal preferences.
A bioprosthesis is a type of medical implant that is made from biological materials, such as heart valves or tendons taken from animals (xenografts) or humans (allografts). These materials are processed and sterilized to be used in surgical procedures to replace damaged or diseased tissues in the body.
Bioprosthetic implants are often used in cardiac surgery, such as heart valve replacement, because they are less likely to cause an immune response than synthetic materials. However, they may have a limited lifespan due to calcification and degeneration of the biological tissue over time. Therefore, bioprosthetic implants may need to be replaced after several years.
Bioprostheses can also be used in other types of surgical procedures, such as ligament or tendon repair, where natural tissue is needed to restore function and mobility. These prostheses are designed to mimic the properties of native tissues and provide a more physiological solution than synthetic materials.
The pulmonary valve, also known as the pulmonic valve, is a semilunar valve located at the exit of the right ventricle of the heart and the beginning of the pulmonary artery. It has three cusps or leaflets that prevent the backflow of blood from the pulmonary artery into the right ventricle during ventricular diastole, ensuring unidirectional flow of blood towards the lungs for oxygenation.
The tricuspid valve is the heart valve that separates the right atrium and the right ventricle in the human heart. It is called "tricuspid" because it has three leaflets or cusps, which are also referred to as flaps or segments. These cusps are named anterior, posterior, and septal. The tricuspid valve's function is to prevent the backflow of blood from the ventricle into the atrium during systole, ensuring unidirectional flow of blood through the heart.
Cardiac catheterization is a medical procedure used to diagnose and treat cardiovascular conditions. In this procedure, a thin, flexible tube called a catheter is inserted into a blood vessel in the arm or leg and threaded up to the heart. The catheter can be used to perform various diagnostic tests, such as measuring the pressure inside the heart chambers and assessing the function of the heart valves.
Cardiac catheterization can also be used to treat certain cardiovascular conditions, such as narrowed or blocked arteries. In these cases, a balloon or stent may be inserted through the catheter to open up the blood vessel and improve blood flow. This procedure is known as angioplasty or percutaneous coronary intervention (PCI).
Cardiac catheterization is typically performed in a hospital cardiac catheterization laboratory by a team of healthcare professionals, including cardiologists, radiologists, and nurses. The procedure may be done under local anesthesia with sedation or general anesthesia, depending on the individual patient's needs and preferences.
Overall, cardiac catheterization is a valuable tool in the diagnosis and treatment of various heart conditions, and it can help improve symptoms, reduce complications, and prolong life for many patients.
Mitral valve insufficiency, also known as mitral regurgitation, is a cardiac condition in which the mitral valve located between the left atrium and left ventricle of the heart does not close properly, causing blood to flow backward into the atrium during contraction of the ventricle. This leads to an increased volume load on the left heart chamber and can result in symptoms such as shortness of breath, fatigue, and fluid retention. The condition can be caused by various factors including valve damage due to degenerative changes, infective endocarditis, rheumatic heart disease, or trauma. Treatment options include medication, mitral valve repair, or replacement surgery depending on the severity and underlying cause of the insufficiency.
Aortic valve prolapse is a cardiac condition in which the aortic valve leaflets bulge or billow into the left ventricle during systole, the phase of the heart cycle when the ventricles contract to pump blood out of the heart. The aortic valve typically has three leaflets that open and close to regulate the flow of blood between the left ventricle and the aorta. In aortic valve prolapse, one or more of these leaflets become floppy, allowing blood to leak back into the left ventricle, a condition known as aortic regurgitation.
Aortic valve prolapse can be congenital or acquired. Some people are born with abnormalities in the aortic valve that make it more prone to prolapse, while others may develop the condition due to degenerative changes in the valve tissue over time. Certain factors, such as Marfan syndrome, bicuspid aortic valve, and infective endocarditis, can increase the risk of aortic valve prolapse.
The symptoms of aortic valve prolapse can vary depending on the severity of the condition. Mild cases may not cause any noticeable symptoms, while more severe cases can lead to shortness of breath, fatigue, chest pain, and irregular heart rhythms. Treatment for aortic valve prolapse may include monitoring, medication, or surgical repair or replacement of the aortic valve.
Calcinosis is a medical condition characterized by the abnormal deposit of calcium salts in various tissues of the body, commonly under the skin or in the muscles and tendons. These calcium deposits can form hard lumps or nodules that can cause pain, inflammation, and restricted mobility. Calcinosis can occur as a complication of other medical conditions, such as autoimmune disorders, kidney disease, and hypercalcemia (high levels of calcium in the blood). In some cases, the cause of calcinosis may be unknown. Treatment for calcinosis depends on the underlying cause and may include medications to manage calcium levels, physical therapy, and surgical removal of large deposits.
Bacterial endocarditis is a medical condition characterized by the inflammation and infection of the inner layer of the heart, known as the endocardium. This infection typically occurs when bacteria enter the bloodstream and attach themselves to damaged or abnormal heart valves or other parts of the endocardium. The bacteria can then multiply and cause the formation of vegetations, which are clusters of infected tissue that can further damage the heart valves and lead to serious complications such as heart failure, stroke, or even death if left untreated.
Bacterial endocarditis is a relatively uncommon but potentially life-threatening condition that requires prompt medical attention. Risk factors for developing bacterial endocarditis include pre-existing heart conditions such as congenital heart defects, artificial heart valves, previous history of endocarditis, or other conditions that damage the heart valves. Intravenous drug use is also a significant risk factor for this condition.
Symptoms of bacterial endocarditis may include fever, chills, fatigue, muscle and joint pain, shortness of breath, chest pain, and a new or changing heart murmur. Diagnosis typically involves a combination of medical history, physical examination, blood cultures, and imaging tests such as echocardiography. Treatment usually involves several weeks of intravenous antibiotics to eradicate the infection, and in some cases, surgical intervention may be necessary to repair or replace damaged heart valves.
Mitral valve prolapse (MVP) is a heart condition where the mitral valve, which separates the left atrium and left ventricle in the heart, doesn't function properly. In MVP, one or both of the mitral valve flaps (known as leaflets) bulge or billow into the left atrium during the contraction of the left ventricle. This prolapse can cause a leakage of blood back into the atrium, known as mitral regurgitation. In many cases, MVP is asymptomatic and doesn't require treatment, but in some instances, it may lead to complications such as infective endocarditis or arrhythmias. The exact causes of MVP are not fully understood, but it can be associated with certain genetic factors, connective tissue disorders, and mitral valve abnormalities present at birth.
Prosthesis design is a specialized field in medical device technology that involves creating and developing artificial substitutes to replace a missing body part, such as a limb, tooth, eye, or internal organ. The design process typically includes several stages: assessment of the patient's needs, selection of appropriate materials, creation of a prototype, testing and refinement, and final fabrication and fitting of the prosthesis.
The goal of prosthesis design is to create a device that functions as closely as possible to the natural body part it replaces, while also being comfortable, durable, and aesthetically pleasing for the patient. The design process may involve collaboration between medical professionals, engineers, and designers, and may take into account factors such as the patient's age, lifestyle, occupation, and overall health.
Prosthesis design can be highly complex, particularly for advanced devices such as robotic limbs or implantable organs. These devices often require sophisticated sensors, actuators, and control systems to mimic the natural functions of the body part they replace. As a result, prosthesis design is an active area of research and development in the medical field, with ongoing efforts to improve the functionality, comfort, and affordability of these devices for patients.
Mitral valve stenosis is a cardiac condition characterized by the narrowing or stiffening of the mitral valve, one of the four heart valves that regulate blood flow through the heart. This narrowing prevents the mitral valve from fully opening during diastole (relaxation phase of the heart cycle), leading to restricted flow of oxygenated blood from the left atrium into the left ventricle.
The narrowing or stiffening of the mitral valve can be caused by various factors, such as rheumatic heart disease, congenital heart defects, aging, or calcium deposits on the valve leaflets. As a result, the left atrium has to work harder to pump blood into the left ventricle, causing increased pressure in the left atrium and pulmonary veins. This can lead to symptoms such as shortness of breath, fatigue, coughing, and heart palpitations.
Mitral valve stenosis is typically diagnosed through a combination of medical history, physical examination, and imaging techniques like echocardiography or cardiac catheterization. Treatment options may include medications to manage symptoms and prevent complications, as well as surgical interventions such as mitral valve repair or replacement to alleviate the stenosis and improve heart function.
Transesophageal echocardiography (TEE) is a type of echocardiogram, which is a medical test that uses sound waves to create detailed images of the heart. In TEE, a special probe containing a transducer is passed down the esophagus (the tube that connects the mouth to the stomach) to obtain views of the heart from behind. This allows for more detailed images of the heart structures and function compared to a standard echocardiogram, which uses a probe placed on the chest. TEE is often used in patients with poor image quality from a standard echocardiogram or when more detailed images are needed to diagnose or monitor certain heart conditions. It is typically performed by a trained cardiologist or sonographer under the direction of a cardiologist.
Venous valves are one-way flaps made of thin, flexible tissue that lie inside your veins. They allow blood to flow towards the heart but prevent it from flowing backward. These valves are especially important in the veins of the legs, where they help to counteract the force of gravity and ensure that blood flows back up to the heart. When venous valves become damaged or weakened, blood can pool in the veins, leading to conditions such as varicose veins or chronic venous insufficiency.
Echocardiography is a medical procedure that uses sound waves to produce detailed images of the heart's structure, function, and motion. It is a non-invasive test that can help diagnose various heart conditions, such as valve problems, heart muscle damage, blood clots, and congenital heart defects.
During an echocardiogram, a transducer (a device that sends and receives sound waves) is placed on the chest or passed through the esophagus to obtain images of the heart. The sound waves produced by the transducer bounce off the heart structures and return to the transducer, which then converts them into electrical signals that are processed to create images of the heart.
There are several types of echocardiograms, including:
* Transthoracic echocardiography (TTE): This is the most common type of echocardiogram and involves placing the transducer on the chest.
* Transesophageal echocardiography (TEE): This type of echocardiogram involves passing a specialized transducer through the esophagus to obtain images of the heart from a closer proximity.
* Stress echocardiography: This type of echocardiogram is performed during exercise or medication-induced stress to assess how the heart functions under stress.
* Doppler echocardiography: This type of echocardiogram uses sound waves to measure blood flow and velocity in the heart and blood vessels.
Echocardiography is a valuable tool for diagnosing and managing various heart conditions, as it provides detailed information about the structure and function of the heart. It is generally safe, non-invasive, and painless, making it a popular choice for doctors and patients alike.
Cardiac valve annuloplasty is a surgical procedure that involves repairing and reinforcing the ring-like structure (annulus) surrounding the heart valves, primarily the mitral or tricuspid valves. This procedure is often performed to correct valve leaks or regurgitation caused by various conditions such as valve disease or dilated cardiomyopathy.
During the annuloplasty procedure, the surgeon typically uses an artificial ring-like device (annuloplasty ring) made of fabric, metal, or a combination of both to reshape and stabilize the damaged annulus. The ring is sewn in place, reducing the size of the valve opening and helping the valve leaflets to coapt properly, thereby preventing valve leaks and improving heart function.
Annuloplasty can be performed as a standalone procedure or in combination with other cardiac surgeries such as valve replacement or repair. The specific technique and approach may vary depending on the individual patient's needs and the surgeon's preference.
Treatment outcome is a term used to describe the result or effect of medical treatment on a patient's health status. It can be measured in various ways, such as through symptoms improvement, disease remission, reduced disability, improved quality of life, or survival rates. The treatment outcome helps healthcare providers evaluate the effectiveness of a particular treatment plan and make informed decisions about future care. It is also used in clinical research to compare the efficacy of different treatments and improve patient care.
Endocarditis is an inflammation of the inner layer of the heart chambers and heart valves, called the endocardium. This inflammation typically results from a bacterial or, less commonly, fungal infection that travels through the bloodstream and attaches to damaged areas of the heart.
There are two main types of endocarditis:
1. Acute Endocarditis: Develops quickly and can be severe, causing fever, chills, shortness of breath, fatigue, and heart murmurs. It may lead to serious complications like heart failure, embolism (blood clots that travel to other parts of the body), and damage to heart valves.
2. Subacute Endocarditis: Develops more slowly, often causing milder symptoms that can be mistaken for a cold or flu. Symptoms may include fatigue, weakness, fever, night sweats, weight loss, joint pain, and heart murmurs. Subacute endocarditis is more likely to affect people with previously damaged heart valves or congenital heart conditions.
Treatment usually involves several weeks of intravenous antibiotics or antifungal medications, depending on the cause of the infection. In some cases, surgery may be required to repair or replace damaged heart valves. Preventive measures include good oral hygiene and prompt treatment of infections, especially in individuals at a higher risk for endocarditis, such as those with congenital heart defects, artificial heart valves, or previous history of endocarditis.
An aortic aneurysm is a medical condition characterized by the abnormal widening or bulging of the wall of the aorta, which is the largest artery in the body. The aorta carries oxygenated blood from the heart to the rest of the body. When the aortic wall weakens, it can stretch and balloon out, forming an aneurysm.
Aortic aneurysms can occur anywhere along the aorta but are most commonly found in the abdominal section (abdominal aortic aneurysm) or the chest area (thoracic aortic aneurysm). The size and location of the aneurysm, as well as the patient's overall health, determine the risk of rupture and associated complications.
Aneurysms often do not cause symptoms until they become large or rupture. Symptoms may include:
* Pain in the chest, back, or abdomen
* Pulsating sensation in the abdomen
* Difficulty breathing
* Hoarseness
* Coughing or vomiting
Risk factors for aortic aneurysms include age, smoking, high blood pressure, family history, and certain genetic conditions. Treatment options depend on the size and location of the aneurysm and may include monitoring, medication, or surgical repair.
Tricuspid valve insufficiency, also known as tricuspid regurgitation, is a cardiac condition in which the tricuspid valve located between the right atrium and right ventricle of the heart does not close properly, allowing blood to flow back into the right atrium during contraction of the right ventricle. This results in a portion of the blood being pumped inefficiently, which can lead to volume overload of the right side of the heart and potentially result in symptoms such as fatigue, weakness, shortness of breath, and fluid retention. The condition can be congenital or acquired, with common causes including dilated cardiomyopathy, infective endocarditis, rheumatic heart disease, and trauma.
Catheterization is a medical procedure in which a catheter (a flexible tube) is inserted into the body to treat various medical conditions or for diagnostic purposes. The specific definition can vary depending on the area of medicine and the particular procedure being discussed. Here are some common types of catheterization:
1. Urinary catheterization: This involves inserting a catheter through the urethra into the bladder to drain urine. It is often performed to manage urinary retention, monitor urine output in critically ill patients, or assist with surgical procedures.
2. Cardiac catheterization: A procedure where a catheter is inserted into a blood vessel, usually in the groin or arm, and guided to the heart. This allows for various diagnostic tests and treatments, such as measuring pressures within the heart chambers, assessing blood flow, or performing angioplasty and stenting of narrowed coronary arteries.
3. Central venous catheterization: A catheter is inserted into a large vein, typically in the neck, chest, or groin, to administer medications, fluids, or nutrition, or to monitor central venous pressure.
4. Peritoneal dialysis catheterization: A catheter is placed into the abdominal cavity for individuals undergoing peritoneal dialysis, a type of kidney replacement therapy.
5. Neurological catheterization: In some cases, a catheter may be inserted into the cerebrospinal fluid space (lumbar puncture) or the brain's ventricular system (ventriculostomy) to diagnose or treat various neurological conditions.
These are just a few examples of catheterization procedures in medicine. The specific definition and purpose will depend on the medical context and the particular organ or body system involved.
Mitral valve annuloplasty is a surgical procedure that involves repairing and reinforcing the mitral valve in the heart, which helps control blood flow between the left atrium and left ventricle. The procedure typically aims to reduce the size of the mitral valve's dilated or stretched opening (annulus) by implanting a prosthetic ring or band around it. This reinforcement helps restore normal valve function, preventing regurgitation or backflow of blood into the atrium during heart contractions.
The procedure is often performed to treat mitral valve regurgitation, which can be caused by various factors such as age-related degenerative changes, infective endocarditis, rheumatic heart disease, or congenital abnormalities. Mitral valve annuloplasty may be done alone or in combination with other cardiac surgeries like mitral valve replacement or repair of the valve leaflets.
Doppler echocardiography is a type of ultrasound test that uses high-frequency sound waves to produce detailed images of the heart and its blood vessels. It measures the direction and speed of blood flow in the heart and major blood vessels leading to and from the heart. This helps to evaluate various conditions such as valve problems, congenital heart defects, and heart muscle diseases.
In Doppler echocardiography, a small handheld device called a transducer is placed on the chest, which emits sound waves that bounce off the heart and blood vessels. The transducer then picks up the returning echoes, which are processed by a computer to create moving images of the heart.
The Doppler effect is used to measure the speed and direction of blood flow. This occurs when the frequency of the sound waves changes as they bounce off moving objects, such as red blood cells. By analyzing these changes, the ultrasound machine can calculate the velocity and direction of blood flow in different parts of the heart.
Doppler echocardiography is a non-invasive test that does not require any needles or dyes. It is generally safe and painless, although patients may experience some discomfort from the pressure applied by the transducer on the chest. The test usually takes about 30 to 60 minutes to complete.
A reoperation is a surgical procedure that is performed again on a patient who has already undergone a previous operation for the same or related condition. Reoperations may be required due to various reasons, such as inadequate initial treatment, disease recurrence, infection, or complications from the first surgery. The nature and complexity of a reoperation can vary widely depending on the specific circumstances, but it often carries higher risks and potential complications compared to the original operation.
Congenital heart defects (CHDs) are structural abnormalities in the heart that are present at birth. They can affect any part of the heart's structure, including the walls of the heart, the valves inside the heart, and the major blood vessels that lead to and from the heart.
Congenital heart defects can range from mild to severe and can cause various symptoms depending on the type and severity of the defect. Some common symptoms of CHDs include cyanosis (a bluish tint to the skin, lips, and fingernails), shortness of breath, fatigue, poor feeding, and slow growth in infants and children.
There are many different types of congenital heart defects, including:
1. Septal defects: These are holes in the walls that separate the four chambers of the heart. The two most common septal defects are atrial septal defect (ASD) and ventricular septal defect (VSD).
2. Valve abnormalities: These include narrowed or leaky valves, which can affect blood flow through the heart.
3. Obstruction defects: These occur when blood flow is blocked or restricted due to narrowing or absence of a part of the heart's structure. Examples include pulmonary stenosis and coarctation of the aorta.
4. Cyanotic heart defects: These cause a lack of oxygen in the blood, leading to cyanosis. Examples include tetralogy of Fallot and transposition of the great arteries.
The causes of congenital heart defects are not fully understood, but genetic factors and environmental influences during pregnancy may play a role. Some CHDs can be detected before birth through prenatal testing, while others may not be diagnosed until after birth or later in childhood. Treatment for CHDs may include medication, surgery, or other interventions to improve blood flow and oxygenation of the body's tissues.
Prosthesis failure is a term used to describe a situation where a prosthetic device, such as an artificial joint or limb, has stopped functioning or failed to meet its intended purpose. This can be due to various reasons, including mechanical failure, infection, loosening of the device, or a reaction to the materials used in the prosthesis.
Mechanical failure can occur due to wear and tear, manufacturing defects, or improper use of the prosthetic device. Infection can also lead to prosthesis failure, particularly in cases where the prosthesis is implanted inside the body. The immune system may react to the presence of the foreign material, leading to inflammation and infection.
Loosening of the prosthesis can also cause it to fail over time, as the device becomes less stable and eventually stops working properly. Additionally, some people may have a reaction to the materials used in the prosthesis, leading to tissue damage or other complications that can result in prosthesis failure.
In general, prosthesis failure can lead to decreased mobility, pain, and the need for additional surgeries or treatments to correct the problem. It is important for individuals with prosthetic devices to follow their healthcare provider's instructions carefully to minimize the risk of prosthesis failure and ensure that the device continues to function properly over time.
Pathologic dilatation refers to an abnormal and excessive widening or enlargement of a body cavity or organ, which can result from various medical conditions. This abnormal dilation can occur in different parts of the body, including the blood vessels, digestive tract, airways, or heart chambers.
In the context of the cardiovascular system, pathologic dilatation may indicate a weakening or thinning of the heart muscle, leading to an enlarged chamber that can no longer pump blood efficiently. This condition is often associated with various heart diseases, such as cardiomyopathy, valvular heart disease, or long-standing high blood pressure.
In the gastrointestinal tract, pathologic dilatation may occur due to mechanical obstruction, neuromuscular disorders, or inflammatory conditions that affect the normal motility of the intestines. Examples include megacolon in Hirschsprung's disease, toxic megacolon in ulcerative colitis, or volvulus (twisting) of the bowel.
Pathologic dilatation can lead to various complications, such as reduced organ function, impaired circulation, and increased risk of infection or perforation. Treatment depends on the underlying cause and may involve medications, surgery, or other interventions to address the root problem and prevent further enlargement.
Echocardiography, Doppler, color is a type of ultrasound test that uses sound waves to create detailed moving images of the heart and its blood vessels. In this technique, color Doppler is used to visualize the direction and speed of blood flow through the heart and great vessels. The movement of the red blood cells causes a change in frequency of the reflected sound waves (Doppler shift), which can be used to calculate the velocity and direction of the blood flow. By adding color to the Doppler image, it becomes easier for the interpreting physician to understand the complex three-dimensional motion of blood through the heart. This test is often used to diagnose and monitor various heart conditions, including valve disorders, congenital heart defects, and cardiac muscle diseases.
Cardiac surgical procedures are operations that are performed on the heart or great vessels (the aorta and vena cava) by cardiothoracic surgeons. These surgeries are often complex and require a high level of skill and expertise. Some common reasons for cardiac surgical procedures include:
1. Coronary artery bypass grafting (CABG): This is a surgery to improve blood flow to the heart in patients with coronary artery disease. During the procedure, a healthy blood vessel from another part of the body is used to create a detour around the blocked or narrowed portion of the coronary artery.
2. Valve repair or replacement: The heart has four valves that control blood flow through and out of the heart. If one or more of these valves become damaged or diseased, they may need to be repaired or replaced. This can be done using artificial valves or valves from animal or human donors.
3. Aneurysm repair: An aneurysm is a weakened area in the wall of an artery that can bulge out and potentially rupture. If an aneurysm occurs in the aorta, it may require surgical repair to prevent rupture.
4. Heart transplantation: In some cases, heart failure may be so severe that a heart transplant is necessary. This involves removing the diseased heart and replacing it with a healthy donor heart.
5. Arrhythmia surgery: Certain types of abnormal heart rhythms (arrhythmias) may require surgical treatment. One such procedure is called the Maze procedure, which involves creating a pattern of scar tissue in the heart to disrupt the abnormal electrical signals that cause the arrhythmia.
6. Congenital heart defect repair: Some people are born with structural problems in their hearts that require surgical correction. These may include holes between the chambers of the heart or abnormal blood vessels.
Cardiac surgical procedures carry risks, including bleeding, infection, stroke, and death. However, for many patients, these surgeries can significantly improve their quality of life and longevity.
A Severity of Illness Index is a measurement tool used in healthcare to assess the severity of a patient's condition and the risk of mortality or other adverse outcomes. These indices typically take into account various physiological and clinical variables, such as vital signs, laboratory values, and co-morbidities, to generate a score that reflects the patient's overall illness severity.
Examples of Severity of Illness Indices include the Acute Physiology and Chronic Health Evaluation (APACHE) system, the Simplified Acute Physiology Score (SAPS), and the Mortality Probability Model (MPM). These indices are often used in critical care settings to guide clinical decision-making, inform prognosis, and compare outcomes across different patient populations.
It is important to note that while these indices can provide valuable information about a patient's condition, they should not be used as the sole basis for clinical decision-making. Rather, they should be considered in conjunction with other factors, such as the patient's overall clinical presentation, treatment preferences, and goals of care.
Balloon valvuloplasty is a medical procedure used to treat heart valve stenosis or narrowing. It involves the use of a thin, flexible tube (catheter) with a balloon at its tip, which is guided through a blood vessel to the narrowed heart valve. Once in position, the balloon is inflated to stretch and widen the valve opening, improving blood flow. After the valve is widened, the balloon is deflated and the catheter is removed. This procedure can be performed on various heart valves, including the aortic, mitral, and pulmonary valves.
Postoperative complications refer to any unfavorable condition or event that occurs during the recovery period after a surgical procedure. These complications can vary in severity and may include, but are not limited to:
1. Infection: This can occur at the site of the incision or inside the body, such as pneumonia or urinary tract infection.
2. Bleeding: Excessive bleeding (hemorrhage) can lead to a drop in blood pressure and may require further surgical intervention.
3. Blood clots: These can form in the deep veins of the legs (deep vein thrombosis) and can potentially travel to the lungs (pulmonary embolism).
4. Wound dehiscence: This is when the surgical wound opens up, which can lead to infection and further complications.
5. Pulmonary issues: These include atelectasis (collapsed lung), pneumonia, or respiratory failure.
6. Cardiovascular problems: These include abnormal heart rhythms (arrhythmias), heart attack, or stroke.
7. Renal failure: This can occur due to various reasons such as dehydration, blood loss, or the use of certain medications.
8. Pain management issues: Inadequate pain control can lead to increased stress, anxiety, and decreased mobility.
9. Nausea and vomiting: These can be caused by anesthesia, opioid pain medication, or other factors.
10. Delirium: This is a state of confusion and disorientation that can occur in the elderly or those with certain medical conditions.
Prompt identification and management of these complications are crucial to ensure the best possible outcome for the patient.
The Sinus of Valsalva are three pouch-like dilations or outpouchings located at the upper part (root) of the aorta, just above the aortic valve. They are named after Antonio Maria Valsalva, an Italian anatomist and physician. These sinuses are divided into three parts:
1. Right Sinus of Valsalva: It is located to the right of the ascending aorta and usually gives rise to the right coronary artery.
2. Left Sinus of Valsalva: It is situated to the left of the ascending aorta and typically gives rise to the left coronary artery.
3. Non-coronary Sinus of Valsalva: This sinus is located in between the right and left coronary sinuses, and it does not give rise to any coronary arteries.
These sinuses play a crucial role during the cardiac cycle, particularly during ventricular contraction (systole). The pressure difference between the aorta and the ventricles causes the aortic valve cusps to be pushed into these sinuses, preventing the backflow of blood from the aorta into the ventricles.
Anatomical variations in the size and shape of the Sinuses of Valsalva can occur, and certain conditions like congenital heart diseases (e.g., aortic valve stenosis or bicuspid aortic valve) may affect their structure and function. Additionally, aneurysms or ruptures of the sinuses can lead to severe complications, such as cardiac tamponade, endocarditis, or stroke.
Follow-up studies are a type of longitudinal research that involve repeated observations or measurements of the same variables over a period of time, in order to understand their long-term effects or outcomes. In medical context, follow-up studies are often used to evaluate the safety and efficacy of medical treatments, interventions, or procedures.
In a typical follow-up study, a group of individuals (called a cohort) who have received a particular treatment or intervention are identified and then followed over time through periodic assessments or data collection. The data collected may include information on clinical outcomes, adverse events, changes in symptoms or functional status, and other relevant measures.
The results of follow-up studies can provide important insights into the long-term benefits and risks of medical interventions, as well as help to identify factors that may influence treatment effectiveness or patient outcomes. However, it is important to note that follow-up studies can be subject to various biases and limitations, such as loss to follow-up, recall bias, and changes in clinical practice over time, which must be carefully considered when interpreting the results.
In the field of medicine, "time factors" refer to the duration of symptoms or time elapsed since the onset of a medical condition, which can have significant implications for diagnosis and treatment. Understanding time factors is crucial in determining the progression of a disease, evaluating the effectiveness of treatments, and making critical decisions regarding patient care.
For example, in stroke management, "time is brain," meaning that rapid intervention within a specific time frame (usually within 4.5 hours) is essential to administering tissue plasminogen activator (tPA), a clot-busting drug that can minimize brain damage and improve patient outcomes. Similarly, in trauma care, the "golden hour" concept emphasizes the importance of providing definitive care within the first 60 minutes after injury to increase survival rates and reduce morbidity.
Time factors also play a role in monitoring the progression of chronic conditions like diabetes or heart disease, where regular follow-ups and assessments help determine appropriate treatment adjustments and prevent complications. In infectious diseases, time factors are crucial for initiating antibiotic therapy and identifying potential outbreaks to control their spread.
Overall, "time factors" encompass the significance of recognizing and acting promptly in various medical scenarios to optimize patient outcomes and provide effective care.
Multidetector computed tomography (MDCT) is a type of computed tomography (CT) scan that uses multiple rows of detectors to acquire several slices of images simultaneously, thereby reducing the total time required for the scan and improving the spatial resolution. This technology allows for faster scanning of moving organs, such as the heart, and provides high-resolution images with detailed information about various body structures, including bones, soft tissues, and blood vessels. MDCT has numerous applications in diagnostic imaging, interventional procedures, and cancer staging and treatment follow-up.
Hemodynamics is the study of how blood flows through the cardiovascular system, including the heart and the vascular network. It examines various factors that affect blood flow, such as blood volume, viscosity, vessel length and diameter, and pressure differences between different parts of the circulatory system. Hemodynamics also considers the impact of various physiological and pathological conditions on these variables, and how they in turn influence the function of vital organs and systems in the body. It is a critical area of study in fields such as cardiology, anesthesiology, and critical care medicine.
Prosthesis fitting is the process of selecting, designing, fabricating, and fitting a prosthetic device to replace a part of an individual's body that is missing due to congenital absence, illness, injury, or amputation. The primary goal of prosthesis fitting is to restore the person's physical function, mobility, and independence, as well as improve their overall quality of life.
The process typically involves several steps:
1. Assessment: A thorough evaluation of the patient's medical history, physical condition, and functional needs is conducted to determine the most appropriate type of prosthesis. This may include measurements, castings, or digital scans of the residual limb.
2. Design: Based on the assessment, a customized design plan is created for the prosthetic device, taking into account factors such as the patient's lifestyle, occupation, and personal preferences.
3. Fabrication: The prosthesis is manufactured using various materials, components, and techniques to meet the specific requirements of the patient. This may involve the use of 3D printing, computer-aided design (CAD), or traditional handcrafting methods.
4. Fitting: Once the prosthesis is fabricated, it is carefully fitted to the patient's residual limb, ensuring optimal comfort, alignment, and stability. Adjustments may be made as needed to achieve the best fit and function.
5. Training: The patient receives training on how to use and care for their new prosthetic device, including exercises to strengthen the residual limb and improve overall mobility. Follow-up appointments are scheduled to monitor progress, make any necessary adjustments, and provide ongoing support.
Suture techniques refer to the various methods used by surgeons to sew or stitch together tissues in the body after an injury, trauma, or surgical incision. The main goal of suturing is to approximate and hold the edges of the wound together, allowing for proper healing and minimizing scar formation.
There are several types of suture techniques, including:
1. Simple Interrupted Suture: This is one of the most basic suture techniques where the needle is passed through the tissue at a right angle, creating a loop that is then tightened to approximate the wound edges. Multiple stitches are placed along the length of the incision or wound.
2. Continuous Locking Suture: In this technique, the needle is passed continuously through the tissue in a zigzag pattern, with each stitch locking into the previous one. This creates a continuous line of sutures that provides strong tension and support to the wound edges.
3. Running Suture: Similar to the continuous locking suture, this technique involves passing the needle continuously through the tissue in a straight line. However, instead of locking each stitch, the needle is simply passed through the previous loop before being tightened. This creates a smooth and uninterrupted line of sutures that can be easily removed after healing.
4. Horizontal Mattress Suture: In this technique, two parallel stitches are placed horizontally across the wound edges, creating a "mattress" effect that provides additional support and tension to the wound. This is particularly useful in deep or irregularly shaped wounds.
5. Vertical Mattress Suture: Similar to the horizontal mattress suture, this technique involves placing two parallel stitches vertically across the wound edges. This creates a more pronounced "mattress" effect that can help reduce tension and minimize scarring.
6. Subcuticular Suture: In this technique, the needle is passed just below the surface of the skin, creating a smooth and barely visible line of sutures. This is particularly useful in cosmetic surgery or areas where minimizing scarring is important.
The choice of suture technique depends on various factors such as the location and size of the wound, the type of tissue involved, and the patient's individual needs and preferences. Proper suture placement and tension are crucial for optimal healing and aesthetic outcomes.
Pulmonary Valve Stenosis is a cardiac condition where the pulmonary valve, located between the right ventricle and the pulmonary artery, has a narrowed opening. This stenosis (narrowing) can cause obstruction of blood flow from the right ventricle to the lungs. The narrowing can be caused by a fusion of the valve leaflets, thickened or calcified valve leaflets, or rarely, a dysplastic valve.
The severity of Pulmonary Valve Stenosis is classified based on the gradient pressure across the valve, which is measured during an echocardiogram. A mild stenosis has a gradient of less than 30 mmHg, moderate stenosis has a gradient between 30-59 mmHg, and severe stenosis has a gradient of 60 mmHg or higher.
Mild Pulmonary Valve Stenosis may not require treatment, while more severe cases may need to be treated with balloon valvuloplasty or surgical valve replacement. If left untreated, Pulmonary Valve Stenosis can lead to right ventricular hypertrophy, heart failure, and other complications.
Phonocardiography is a non-invasive medical procedure that involves the graphical representation and analysis of sounds produced by the heart. It uses a device called a phonocardiograph to record these sounds, which are then displayed as waveforms on a screen. The procedure is often used in conjunction with other diagnostic techniques, such as electrocardiography (ECG), to help diagnose various heart conditions, including valvular heart disease and heart murmurs.
During the procedure, a specialized microphone called a phonendoscope is placed on the chest wall over the area of the heart. The microphone picks up the sounds generated by the heart's movements, such as the closing and opening of the heart valves, and transmits them to the phonocardiograph. The phonocardiograph then converts these sounds into a visual representation, which can be analyzed for any abnormalities or irregularities in the heart's function.
Phonocardiography is a valuable tool for healthcare professionals, as it can provide important insights into the health and functioning of the heart. By analyzing the waveforms produced during phonocardiography, doctors can identify any potential issues with the heart's valves or other structures, which may require further investigation or treatment. Overall, phonocardiography is an essential component of modern cardiac diagnostics, helping to ensure that patients receive accurate and timely diagnoses for their heart conditions.
Three-dimensional echocardiography (3DE) is a type of cardiac ultrasound that uses advanced technologies to create a real-time, detailed 3D image of the heart. This imaging technique provides a more comprehensive view of the heart's structure and function compared to traditional 2D echocardiography. By visualizing the heart from multiple angles, 3DE can help physicians better assess complex cardiac conditions, plan treatments, and monitor their effectiveness.
In a 3DE examination, a transducer (a handheld device that emits and receives sound waves) is placed on the chest to capture ultrasound data. This data is then processed by specialized software to create a 3D model of the heart. The procedure is non-invasive and typically takes less than an hour to complete.
Three-dimensional echocardiography has several clinical applications, including:
1. Evaluation of cardiac morphology and function in congenital heart disease
2. Assessment of valvular structure and function, such as mitral or aortic valve regurgitation or stenosis
3. Guidance during interventional procedures like transcatheter aortic valve replacement (TAVR)
4. Quantification of left ventricular volumes, ejection fraction, and mass
5. Assessment of right ventricular size and function
6. Detection and monitoring of cardiac tumors or other masses
7. Pre-surgical planning for complex heart surgeries
Overall, 3DE offers a more accurate and detailed view of the heart, allowing healthcare providers to make informed decisions about patient care and improve outcomes.
Replantation is a surgical procedure in which a body part that has been completely detached or amputated is reattached to the body. This procedure involves careful reattachment of bones, muscles, tendons, nerves, and blood vessels to restore function and sensation to the greatest extent possible. The success of replantation depends on various factors such as the level of injury, the condition of the amputated part, and the patient's overall health.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
The chordae tendineae are cord-like tendons that attach the heart's papillary muscles to the tricuspid and mitral valves in the heart. They play a crucial role in preventing the backflow of blood into the atria during ventricular contraction. The chordae tendineae ensure that the cusps of the atrioventricular valves close properly and maintain their shape during the cardiac cycle. Damage to these tendons can result in heart conditions such as mitral or tricuspid valve regurgitation.
The aorta is the largest artery in the human body, which originates from the left ventricle of the heart and carries oxygenated blood to the rest of the body. It can be divided into several parts, including the ascending aorta, aortic arch, and descending aorta. The ascending aorta gives rise to the coronary arteries that supply blood to the heart muscle. The aortic arch gives rise to the brachiocephalic, left common carotid, and left subclavian arteries, which supply blood to the head, neck, and upper extremities. The descending aorta travels through the thorax and abdomen, giving rise to various intercostal, visceral, and renal arteries that supply blood to the chest wall, organs, and kidneys.
A fibroma is a benign (non-cancerous) tumor that consists primarily of fibrous or connective tissue. It can occur in various parts of the body, including the skin, mouth, and internal organs. The term "fibroma" is often used to describe any benign fibrous growth, but there are specific types of fibromas such as dermatofibroma (found in the skin), oral fibroma (found in the mouth), and benign fibrous histiocytoma (found in soft tissues).
It's important to note that while fibromas are generally harmless, they can cause discomfort or problems depending on their size and location. If a fibroma is causing issues or there's concern about its growth or malignancy, it should be evaluated by a healthcare professional for potential removal or further assessment.
The sternum, also known as the breastbone, is a long, flat bone located in the central part of the chest. It serves as the attachment point for several muscles and tendons, including those involved in breathing. The sternum has three main parts: the manubrium at the top, the body in the middle, and the xiphoid process at the bottom. The upper seven pairs of ribs connect to the sternum via costal cartilages.
Sclerosis is a medical term that refers to the abnormal hardening or scarring of body tissues, particularly in the context of various degenerative diseases affecting the nervous system. The term "sclerosis" comes from the Greek word "skleros," which means hard. In these conditions, the normally flexible and adaptable nerve cells or their protective coverings (myelin sheath) become rigid and inflexible due to the buildup of scar tissue or abnormal protein deposits.
There are several types of sclerosis, but one of the most well-known is multiple sclerosis (MS). In MS, the immune system mistakenly attacks the myelin sheath surrounding nerve fibers in the brain and spinal cord, leading to scarring and damage that disrupts communication between the brain and the rest of the body. This results in a wide range of symptoms, such as muscle weakness, numbness, vision problems, balance issues, and cognitive impairment.
Other conditions that involve sclerosis include:
1. Amyotrophic lateral sclerosis (ALS): Also known as Lou Gehrig's disease, ALS is a progressive neurodegenerative disorder affecting motor neurons in the brain and spinal cord, leading to muscle weakness, stiffness, and atrophy.
2. Systemic sclerosis: A rare autoimmune connective tissue disorder characterized by thickening and hardening of the skin and internal organs due to excessive collagen deposition.
3. Plaque psoriasis: A chronic inflammatory skin condition marked by red, scaly patches (plaques) resulting from rapid turnover and accumulation of skin cells.
4. Adhesive capsulitis: Also known as frozen shoulder, this condition involves stiffening and thickening of the shoulder joint's capsule due to scarring or inflammation, leading to limited mobility and pain.
Heart valves are specialized structures in the heart that ensure unidirectional flow of blood through its chambers during the cardiac cycle. There are four heart valves: the tricuspid valve and the mitral (bicuspid) valve, located between the atria and ventricles, and the pulmonic (pulmonary) valve and aortic valve, located between the ventricles and the major blood vessels leaving the heart.
The heart valves are composed of thin flaps of tissue called leaflets or cusps, which are supported by a fibrous ring. The aortic and pulmonic valves have three cusps each, while the tricuspid and mitral valves have three and two cusps, respectively.
The heart valves open and close in response to pressure differences across them, allowing blood to flow forward into the ventricles during diastole (filling phase) and preventing backflow of blood into the atria during systole (contraction phase). A properly functioning heart valve ensures efficient pumping of blood by the heart and maintains normal blood circulation throughout the body.
Prospective studies, also known as longitudinal studies, are a type of cohort study in which data is collected forward in time, following a group of individuals who share a common characteristic or exposure over a period of time. The researchers clearly define the study population and exposure of interest at the beginning of the study and follow up with the participants to determine the outcomes that develop over time. This type of study design allows for the investigation of causal relationships between exposures and outcomes, as well as the identification of risk factors and the estimation of disease incidence rates. Prospective studies are particularly useful in epidemiology and medical research when studying diseases with long latency periods or rare outcomes.
Aortic diseases refer to conditions that affect the aorta, which is the largest and main artery in the body. The aorta carries oxygenated blood from the heart to the rest of the body. Aortic diseases can weaken or damage the aorta, leading to various complications. Here are some common aortic diseases with their medical definitions:
1. Aortic aneurysm: A localized dilation or bulging of the aortic wall, which can occur in any part of the aorta but is most commonly found in the abdominal aorta (abdominal aortic aneurysm) or the thoracic aorta (thoracic aortic aneurysm). Aneurysms can increase the risk of rupture, leading to life-threatening bleeding.
2. Aortic dissection: A separation of the layers of the aortic wall due to a tear in the inner lining, allowing blood to flow between the layers and potentially cause the aorta to rupture. This is a medical emergency that requires immediate treatment.
3. Aortic stenosis: A narrowing of the aortic valve opening, which restricts blood flow from the heart to the aorta. This can lead to shortness of breath, chest pain, and other symptoms. Severe aortic stenosis may require surgical or transcatheter intervention to replace or repair the aortic valve.
4. Aortic regurgitation: Also known as aortic insufficiency, this condition occurs when the aortic valve does not close properly, allowing blood to leak back into the heart. This can lead to symptoms such as fatigue, shortness of breath, and palpitations. Treatment may include medication or surgical repair or replacement of the aortic valve.
5. Aortitis: Inflammation of the aorta, which can be caused by various conditions such as infections, autoimmune diseases, or vasculitides. Aortitis can lead to aneurysms, dissections, or stenosis and may require medical treatment with immunosuppressive drugs or surgical intervention.
6. Marfan syndrome: A genetic disorder that affects the connective tissue, including the aorta. People with Marfan syndrome are at risk of developing aortic aneurysms and dissections, and may require close monitoring and prophylactic surgery to prevent complications.
Thoracic surgery, also known as cardiothoracic surgery, is a branch of medicine that specializes in the surgical treatment of diseases affecting the organs inside the thorax (chest), specifically the heart, lungs, esophagus, and major blood vessels. This can include procedures such as lung biopsies, lobectomies, pneumonectomies, esophagectomies, heart valve repairs or replacements, coronary artery bypass grafting, and treatment of chest injuries. Thoracic surgeons are medical doctors who have completed extensive training in this field, including a general surgery residency followed by a fellowship in thoracic surgery.
Medical Definition:
"Risk factors" are any attribute, characteristic or exposure of an individual that increases the likelihood of developing a disease or injury. They can be divided into modifiable and non-modifiable risk factors. Modifiable risk factors are those that can be changed through lifestyle choices or medical treatment, while non-modifiable risk factors are inherent traits such as age, gender, or genetic predisposition. Examples of modifiable risk factors include smoking, alcohol consumption, physical inactivity, and unhealthy diet, while non-modifiable risk factors include age, sex, and family history. It is important to note that having a risk factor does not guarantee that a person will develop the disease, but rather indicates an increased susceptibility.
The pericardium is the double-walled sac that surrounds the heart. It has an outer fibrous layer and an inner serous layer, which further divides into two parts: the parietal layer lining the fibrous pericardium and the visceral layer (epicardium) closely adhering to the heart surface.
The space between these two layers is filled with a small amount of lubricating serous fluid, allowing for smooth movement of the heart within the pericardial cavity. The pericardium provides protection, support, and helps maintain the heart's normal position within the chest while reducing friction during heart contractions.
Cardiopulmonary bypass (CPB) is a medical procedure that temporarily takes over the functions of the heart and lungs during major heart surgery. It allows the surgeon to operate on a still, bloodless heart.
During CPB, the patient's blood is circulated outside the body with the help of a heart-lung machine. The machine pumps the blood through a oxygenator, where it is oxygenated and then returned to the body. This bypasses the heart and lungs, hence the name "cardiopulmonary bypass."
CPB involves several components, including a pump, oxygenator, heat exchanger, and tubing. The patient's blood is drained from the heart through cannulas (tubes) and passed through the oxygenator, where it is oxygenated and carbon dioxide is removed. The oxygenated blood is then warmed to body temperature in a heat exchanger before being pumped back into the body.
While on CPB, the patient's heart is stopped with the help of cardioplegia solution, which is infused directly into the coronary arteries. This helps to protect the heart muscle during surgery. The surgeon can then operate on a still and bloodless heart, allowing for more precise surgical repair.
After the surgery is complete, the patient is gradually weaned off CPB, and the heart is restarted with the help of electrical stimulation or medication. The patient's condition is closely monitored during this time to ensure that their heart and lungs are functioning properly.
While CPB has revolutionized heart surgery and allowed for more complex procedures to be performed, it is not without risks. These include bleeding, infection, stroke, kidney damage, and inflammation. However, with advances in technology and technique, the risks associated with CPB have been significantly reduced over time.
Risk assessment in the medical context refers to the process of identifying, evaluating, and prioritizing risks to patients, healthcare workers, or the community related to healthcare delivery. It involves determining the likelihood and potential impact of adverse events or hazards, such as infectious diseases, medication errors, or medical devices failures, and implementing measures to mitigate or manage those risks. The goal of risk assessment is to promote safe and high-quality care by identifying areas for improvement and taking action to minimize harm.
Cardiovascular surgical procedures refer to a range of surgeries performed on the heart and blood vessels to treat or manage various cardiovascular conditions. These surgeries can be open or minimally invasive, and they aim to correct structural abnormalities, improve blood flow, or replace damaged or diseased parts of the cardiovascular system.
Some common types of cardiovascular surgical procedures include:
1. Coronary artery bypass grafting (CABG): This surgery involves taking a healthy blood vessel from another part of the body and using it to create a detour around a blocked or narrowed coronary artery, improving blood flow to the heart muscle.
2. Heart valve repair or replacement: When one or more heart valves become damaged or diseased, they may not open or close properly, leading to reduced blood flow or leakage of blood backward through the valve. In these cases, surgeons may repair or replace the affected valve with a mechanical or biological prosthetic valve.
3. Aneurysm repair: An aneurysm is a weakened area in the wall of an artery that can bulge and potentially rupture, causing severe bleeding. Surgeons can repair an aneurysm by reinforcing the weakened area with a graft or by replacing the affected section of the blood vessel.
4. Heart transplant: In cases where heart failure is irreversible and all other treatment options have been exhausted, a heart transplant may be necessary. This procedure involves removing the damaged heart and replacing it with a healthy donor heart.
5. Ventricular assist devices (VADs): These are mechanical pumps that can be implanted to help support heart function in patients with advanced heart failure who are not candidates for heart transplants. VADs can help improve blood flow, reduce symptoms, and increase the patient's quality of life.
6. Minimally invasive procedures: Advances in technology have led to the development of several minimally invasive cardiovascular surgical procedures, such as robotic-assisted heart surgery, video-assisted thoracoscopic surgery (VATS), and transcatheter aortic valve replacement (TAVR). These techniques typically involve smaller incisions, reduced blood loss, shorter hospital stays, and faster recovery times compared to traditional open-heart surgeries.
The heart ventricles are the two lower chambers of the heart that receive blood from the atria and pump it to the lungs or the rest of the body. The right ventricle pumps deoxygenated blood to the lungs, while the left ventricle pumps oxygenated blood to the rest of the body. Both ventricles have thick, muscular walls to generate the pressure necessary to pump blood through the circulatory system.
Thoracotomy is a surgical procedure that involves making an incision on the chest wall to gain access to the thoracic cavity, which contains the lungs, heart, esophagus, trachea, and other vital organs. The incision can be made on the side (lateral thoracotomy), back (posterolateral thoracotomy), or front (median sternotomy) of the chest wall, depending on the specific surgical indication.
Thoracotomy is performed for various indications, including lung biopsy, lung resection, esophagectomy, heart surgery, and mediastinal mass removal. The procedure allows the surgeon to directly visualize and access the organs within the thoracic cavity, perform necessary procedures, and control bleeding if needed.
After the procedure, the incision is typically closed with sutures or staples, and a chest tube may be placed to drain any accumulated fluid or air from the pleural space around the lungs. The patient will require postoperative care and monitoring in a hospital setting until their condition stabilizes.
A sternotomy is a surgical procedure that involves making an incision through the sternum, also known as the breastbone. This type of incision allows surgeons to access the thoracic cavity, which contains the heart and lungs. Sternotomies are often performed during open-heart surgery or other procedures that require access to the heart or major blood vessels. After the procedure, the sternum is typically wired or stapled back together to allow for proper healing.
Stroke volume is a term used in cardiovascular physiology and medicine. It refers to the amount of blood that is pumped out of the left ventricle of the heart during each contraction (systole). Specifically, it is the difference between the volume of blood in the left ventricle at the end of diastole (when the ventricle is filled with blood) and the volume at the end of systole (when the ventricle has contracted and ejected its contents into the aorta).
Stroke volume is an important measure of heart function, as it reflects the ability of the heart to pump blood effectively to the rest of the body. A low stroke volume may indicate that the heart is not pumping efficiently, while a high stroke volume may suggest that the heart is working too hard. Stroke volume can be affected by various factors, including heart disease, high blood pressure, and physical fitness level.
The formula for calculating stroke volume is:
Stroke Volume = End-Diastolic Volume - End-Systolic Volume
Where end-diastolic volume (EDV) is the volume of blood in the left ventricle at the end of diastole, and end-systolic volume (ESV) is the volume of blood in the left ventricle at the end of systole.
Endocardial fibroelastosis (EFE) is a rare heart condition characterized by the thickening and stiffening of the endocardium, which is the inner lining of the heart chambers. This thickening is caused by an overgrowth of fibrous tissue and elastic fibers in the endocardium, particularly affecting the left ventricle and atrium.
EFE can occur as a primary condition or secondary to other heart diseases, infections, or genetic disorders. In some cases, it may be associated with conditions such as congenital heart defects, metabolic disorders, or viral infections like coxsackievirus B.
The symptoms of EFE depend on the severity and underlying cause of the condition. They can include difficulty breathing, poor feeding, failure to thrive, fatigue, and irregular heart rhythms (arrhythmias). In severe cases, EFE can lead to heart failure and require medical intervention such as medications or even a heart transplant.
The exact cause of primary EFE is still unknown, but it is believed to involve genetic factors. Secondary EFE is usually a result of damage to the heart muscle due to various causes, including infections, inflammation, or other underlying conditions. Treatment for EFE focuses on addressing the underlying cause and managing symptoms to prevent further complications.
Cardiovascular models are simplified representations or simulations of the human cardiovascular system used in medical research, education, and training. These models can be physical, computational, or mathematical and are designed to replicate various aspects of the heart, blood vessels, and blood flow. They can help researchers study the structure and function of the cardiovascular system, test new treatments and interventions, and train healthcare professionals in diagnostic and therapeutic techniques.
Physical cardiovascular models may include artificial hearts, blood vessels, or circulation systems made from materials such as plastic, rubber, or silicone. These models can be used to study the mechanics of heart valves, the effects of different surgical procedures, or the impact of various medical devices on blood flow.
Computational and mathematical cardiovascular models use algorithms and equations to simulate the behavior of the cardiovascular system. These models may range from simple representations of a single heart chamber to complex simulations of the entire circulatory system. They can be used to study the electrical activity of the heart, the biomechanics of blood flow, or the distribution of drugs in the body.
Overall, cardiovascular models play an essential role in advancing our understanding of the human body and improving patient care.
Left ventricular function refers to the ability of the left ventricle (the heart's lower-left chamber) to contract and relax, thereby filling with and ejecting blood. The left ventricle is responsible for pumping oxygenated blood to the rest of the body. Its function is evaluated by measuring several parameters, including:
1. Ejection fraction (EF): This is the percentage of blood that is pumped out of the left ventricle with each heartbeat. A normal ejection fraction ranges from 55% to 70%.
2. Stroke volume (SV): The amount of blood pumped by the left ventricle in one contraction. A typical SV is about 70 mL/beat.
3. Cardiac output (CO): The total volume of blood that the left ventricle pumps per minute, calculated as the product of stroke volume and heart rate. Normal CO ranges from 4 to 8 L/minute.
Assessment of left ventricular function is crucial in diagnosing and monitoring various cardiovascular conditions such as heart failure, coronary artery disease, valvular heart diseases, and cardiomyopathies.
A feasibility study is a preliminary investigation or analysis conducted to determine the viability of a proposed project, program, or product. In the medical field, feasibility studies are often conducted before implementing new treatments, procedures, equipment, or facilities. These studies help to assess the practicality and effectiveness of the proposed intervention, as well as its potential benefits and risks.
Feasibility studies in healthcare typically involve several steps:
1. Problem identification: Clearly define the problem that the proposed project, program, or product aims to address.
2. Objectives setting: Establish specific, measurable, achievable, relevant, and time-bound (SMART) objectives for the study.
3. Literature review: Conduct a thorough review of existing research and best practices related to the proposed intervention.
4. Methodology development: Design a methodology for data collection and analysis that will help answer the research questions and achieve the study's objectives.
5. Resource assessment: Evaluate the availability and adequacy of resources, including personnel, time, and finances, required to carry out the proposed intervention.
6. Risk assessment: Identify potential risks and challenges associated with the implementation of the proposed intervention and develop strategies to mitigate them.
7. Cost-benefit analysis: Estimate the costs and benefits of the proposed intervention, including direct and indirect costs, as well as short-term and long-term benefits.
8. Stakeholder engagement: Engage relevant stakeholders, such as patients, healthcare providers, administrators, and policymakers, to gather their input and support for the proposed intervention.
9. Decision-making: Based on the findings of the feasibility study, make an informed decision about whether or not to proceed with the proposed project, program, or product.
Feasibility studies are essential in healthcare as they help ensure that resources are allocated efficiently and effectively, and that interventions are evidence-based, safe, and beneficial for patients.
A prolapse is a medical condition where an organ or tissue in the body slips from its normal position and drops down into a lower part of the body. This usually occurs when the muscles and ligaments that support the organ become weak or stretched. The most common types of prolapses include:
* Uterine prolapse: When the uterus slips down into or protrudes out of the vagina.
* Rectal prolapse: When the rectum (the lower end of the colon) slips outside the anus.
* Bladder prolapse (cystocele): When the bladder drops into the vagina.
* Small bowel prolapse (enterocele): When the small intestine bulges into the vagina.
Prolapses can cause various symptoms, such as discomfort, pain, pressure, and difficulty with urination or bowel movements. Treatment options depend on the severity of the prolapse and may include lifestyle changes, physical therapy, medication, or surgery.
The Chi-square distribution is a continuous probability distribution that is often used in statistical hypothesis testing. It is the distribution of a sum of squares of k independent standard normal random variables. The resulting quantity follows a chi-square distribution with k degrees of freedom, denoted as χ²(k).
The probability density function (pdf) of the Chi-square distribution with k degrees of freedom is given by:
f(x; k) = (1/ (2^(k/2) * Γ(k/2))) \* x^((k/2)-1) \* e^(-x/2), for x > 0 and 0, otherwise.
Where Γ(k/2) is the gamma function evaluated at k/2. The mean and variance of a Chi-square distribution with k degrees of freedom are k and 2k, respectively.
The Chi-square distribution has various applications in statistical inference, including testing goodness-of-fit, homogeneity of variances, and independence in contingency tables.
Atrioventricular (AV) block is a disorder of the electrical conduction system of the heart that causes a delay or interruption in the transmission of electrical signals from the atria (the upper chambers of the heart) to the ventricles (the lower chambers of the heart). This results in an abnormal heart rhythm, also known as an arrhythmia.
There are three degrees of AV block:
1. First-degree AV block: In this type of AV block, there is a delay in the conduction of electrical signals from the atria to the ventricles, but all signals are eventually conducted. This condition may not cause any symptoms and is often discovered during a routine electrocardiogram (ECG).
2. Second-degree AV block: In this type of AV block, some electrical signals from the atria are not conducted to the ventricles. There are two types of second-degree AV block: Mobitz type I and Mobitz type II. Mobitz type I is characterized by a progressive prolongation of the PR interval (the time between the electrical activation of the atria and ventricles) until a QRS complex (which represents the electrical activation of the ventricles) is dropped. Mobitz type II is characterized by a constant PR interval with occasional non-conducted P waves.
3. Third-degree AV block: In this type of AV block, no electrical signals are conducted from the atria to the ventricles. The atria and ventricles beat independently of each other, resulting in a slow heart rate (bradycardia) and an irregular rhythm. This condition can be life-threatening if not treated promptly.
The causes of AV block include aging, heart disease, medications, and certain medical conditions such as hypothyroidism and Lyme disease. Treatment depends on the severity of the condition and may include medication, a pacemaker, or surgery.
Aortic coarctation is a narrowing of the aorta, the largest blood vessel in the body that carries oxygen-rich blood from the heart to the rest of the body. This condition usually occurs in the part of the aorta that is just beyond where it arises from the left ventricle and before it divides into the iliac arteries.
In aortic coarctation, the narrowing can vary from mild to severe, and it can cause a variety of symptoms depending on the severity of the narrowing and the age of the individual. In newborns and infants with severe coarctation, symptoms may include difficulty breathing, poor feeding, and weak or absent femoral pulses (located in the groin area). Older children and adults with mild to moderate coarctation may not experience any symptoms until later in life, when high blood pressure, headaches, nosebleeds, leg cramps, or heart failure develop.
Aortic coarctation is typically diagnosed through physical examination, imaging tests such as echocardiography, CT angiography, or MRI, and sometimes cardiac catheterization. Treatment options include surgical repair or balloon dilation (also known as balloon angioplasty) to open the narrowed section of the aorta. If left untreated, aortic coarctation can lead to serious complications such as high blood pressure, heart failure, stroke, and rupture or dissection of the aorta.
Aortic stenosis, subvalvular is a medical condition that refers to the narrowing or obstruction of the outflow tract below the aortic valve in the heart. This abnormal narrowing can be caused by various factors such as a congenital heart defect, a tissue growth, or scarring from previous procedures. As a result, the left ventricle must work harder to pump blood through the narrowed opening, which can lead to thickening of the heart muscle (hypertrophy) and decreased cardiac output. Symptoms may include chest pain, shortness of breath, fatigue, and dizziness or fainting spells. Severe subvalvular aortic stenosis can lead to serious complications such as heart failure or even sudden death, and may require surgical intervention to correct the problem.
Rheumatic Heart Disease (RHD) is defined as a chronic heart condition caused by damage to the heart valves due to untreated or inadequately treated streptococcal throat infection (strep throat). The immune system's response to this infection can mistakenly attack and damage the heart tissue, leading to inflammation and scarring of the heart valves. This damage can result in narrowing, leakage, or abnormal functioning of the heart valves, which can further lead to complications such as heart failure, stroke, or infective endocarditis.
RHD is a preventable and treatable condition if detected early and managed effectively. It primarily affects children and young adults in developing countries where access to healthcare and antibiotics for strep throat infections may be limited. Long-term management of RHD typically involves medications, regular monitoring, and sometimes surgical intervention to repair or replace damaged heart valves.
I'm sorry for any confusion, but "Polyethylene Terephthalates" is not a medical term. It is a type of polymer used in the manufacturing of various products, such as plastic bottles and textile fibers. Medically, you might encounter the abbreviation "PET" or "PET scan," which stands for "Positron Emission Tomography." A PET scan is a type of medical imaging that provides detailed pictures of the body's interior. If you have any medical terms you would like defined, I'd be happy to help!
Induced heart arrest, also known as controlled cardiac arrest or planned cardiac arrest, is a deliberate medical intervention where cardiac activity is temporarily stopped through the use of medications or electrical disruption. This procedure is typically carried out during a surgical procedure, such as open-heart surgery, where the heart needs to be stilled to allow surgeons to work on it safely.
The most common method used to induce heart arrest is by administering a medication called potassium chloride, which stops the heart's electrical activity. Alternatively, an electrical shock may be delivered to the heart to achieve the same effect. Once the procedure is complete, the heart can be restarted using various resuscitation techniques, such as defibrillation or medication administration.
It's important to note that induced heart arrest is a carefully monitored and controlled medical procedure carried out by trained healthcare professionals in a hospital setting. It should not be confused with sudden cardiac arrest, which is an unexpected and often unpredictable event that occurs outside of a medical setting.
Heart neoplasms are abnormal growths or tumors that develop within the heart tissue. They can be benign (noncancerous) or malignant (cancerous). Benign tumors, such as myxomas and rhabdomyomas, are typically slower growing and less likely to spread, but they can still cause serious complications if they obstruct blood flow or damage heart valves. Malignant tumors, such as angiosarcomas and rhabdomyosarcomas, are fast-growing and have a higher risk of spreading to other parts of the body. Symptoms of heart neoplasms can include shortness of breath, chest pain, fatigue, and irregular heart rhythms. Treatment options depend on the type, size, and location of the tumor, and may include surgery, radiation therapy, or chemotherapy.
A ventricular septal defect (VSD) is a type of congenital heart defect that involves a hole in the wall separating the two lower chambers of the heart, the ventricles. This defect allows oxygenated blood from the left ventricle to mix with deoxygenated blood in the right ventricle, leading to inefficient oxygenation of the body's tissues. The size and location of the hole can vary, and symptoms may range from none to severe, depending on the size of the defect and the amount of blood that is able to shunt between the ventricles. Small VSDs may close on their own over time, while larger defects usually require medical intervention, such as medication or surgery, to prevent complications like pulmonary hypertension and heart failure.
Patient selection, in the context of medical treatment or clinical research, refers to the process of identifying and choosing appropriate individuals who are most likely to benefit from a particular medical intervention or who meet specific criteria to participate in a study. This decision is based on various factors such as the patient's diagnosis, stage of disease, overall health status, potential risks, and expected benefits. The goal of patient selection is to ensure that the selected individuals will receive the most effective and safe care possible while also contributing to meaningful research outcomes.
Coronary artery bypass surgery, also known as coronary artery bypass grafting (CABG), is a surgical procedure used to improve blood flow to the heart in patients with severe coronary artery disease. This condition occurs when the coronary arteries, which supply oxygen-rich blood to the heart muscle, become narrowed or blocked due to the buildup of fatty deposits, called plaques.
During CABG surgery, a healthy blood vessel from another part of the body is grafted, or attached, to the coronary artery, creating a new pathway for oxygen-rich blood to flow around the blocked or narrowed portion of the artery and reach the heart muscle. This bypass helps to restore normal blood flow and reduce the risk of angina (chest pain), shortness of breath, and other symptoms associated with coronary artery disease.
There are different types of CABG surgery, including traditional on-pump CABG, off-pump CABG, and minimally invasive CABG. The choice of procedure depends on various factors, such as the patient's overall health, the number and location of blocked arteries, and the presence of other medical conditions.
It is important to note that while CABG surgery can significantly improve symptoms and quality of life in patients with severe coronary artery disease, it does not cure the underlying condition. Lifestyle modifications, such as regular exercise, a healthy diet, smoking cessation, and medication therapy, are essential for long-term management and prevention of further progression of the disease.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
Minimally invasive surgical procedures are a type of surgery that is performed with the assistance of specialized equipment and techniques to minimize trauma to the patient's body. This approach aims to reduce blood loss, pain, and recovery time as compared to traditional open surgeries. The most common minimally invasive surgical procedure is laparoscopy, which involves making small incisions (usually 0.5-1 cm) in the abdomen or chest and inserting a thin tube with a camera (laparoscope) to visualize the internal organs.
The surgeon then uses long, slender instruments inserted through separate incisions to perform the necessary surgical procedures, such as cutting, coagulation, or suturing. Other types of minimally invasive surgical procedures include arthroscopy (for joint surgery), thoracoscopy (for chest surgery), and hysteroscopy (for uterine surgery). The benefits of minimally invasive surgical procedures include reduced postoperative pain, shorter hospital stays, quicker return to normal activities, and improved cosmetic results. However, not all surgeries can be performed using minimally invasive techniques, and the suitability of a particular procedure depends on various factors, including the patient's overall health, the nature and extent of the surgical problem, and the surgeon's expertise.
An embolism is a medical condition that occurs when a substance, such as a blood clot or an air bubble, blocks a blood vessel. This can happen in any part of the body, but it is particularly dangerous when it affects the brain (causing a stroke) or the lungs (causing a pulmonary embolism). Embolisms can cause serious harm by preventing oxygen and nutrients from reaching the tissues and organs that need them. They are often the result of underlying medical conditions, such as heart disease or deep vein thrombosis, and may require immediate medical attention to prevent further complications.
Marfan syndrome is a genetic disorder that affects the body's connective tissue. Connective tissue helps to strengthen and support various structures in the body, including the skin, ligaments, blood vessels, and heart. In Marfan syndrome, the body produces an abnormal amount of a protein called fibrillin-1, which is a key component of connective tissue. This leads to problems with the formation and function of connective tissue throughout the body.
The most serious complications of Marfan syndrome typically involve the heart and blood vessels. The aorta, which is the large artery that carries blood away from the heart, can become weakened and stretched, leading to an increased risk of aortic dissection or rupture. Other common features of Marfan syndrome include long, thin fingers and toes; tall stature; a curved spine; and eye problems such as nearsightedness and lens dislocation.
Marfan syndrome is usually inherited in an autosomal dominant pattern, which means that a child has a 50% chance of inheriting the gene mutation from a parent who has the condition. However, about 25% of cases are the result of a new mutation and occur in people with no family history of the disorder. There is no cure for Marfan syndrome, but treatment can help to manage the symptoms and reduce the risk of complications.
The Predictive Value of Tests, specifically the Positive Predictive Value (PPV) and Negative Predictive Value (NPV), are measures used in diagnostic tests to determine the probability that a positive or negative test result is correct.
Positive Predictive Value (PPV) is the proportion of patients with a positive test result who actually have the disease. It is calculated as the number of true positives divided by the total number of positive results (true positives + false positives). A higher PPV indicates that a positive test result is more likely to be a true positive, and therefore the disease is more likely to be present.
Negative Predictive Value (NPV) is the proportion of patients with a negative test result who do not have the disease. It is calculated as the number of true negatives divided by the total number of negative results (true negatives + false negatives). A higher NPV indicates that a negative test result is more likely to be a true negative, and therefore the disease is less likely to be present.
The predictive value of tests depends on the prevalence of the disease in the population being tested, as well as the sensitivity and specificity of the test. A test with high sensitivity and specificity will generally have higher predictive values than a test with low sensitivity and specificity. However, even a highly sensitive and specific test can have low predictive values if the prevalence of the disease is low in the population being tested.
"Device Removal" in a medical context generally refers to the surgical or nonsurgical removal of a medical device that has been previously implanted in a patient's body. The purpose of removing the device may vary, depending on the individual case. Some common reasons for device removal include infection, malfunction, rejection, or when the device is no longer needed.
Examples of medical devices that may require removal include pacemakers, implantable cardioverter-defibrillators (ICDs), artificial joints, orthopedic hardware, breast implants, cochlear implants, and intrauterine devices (IUDs). The procedure for device removal will depend on the type of device, its location in the body, and the reason for its removal.
It is important to note that device removal carries certain risks, such as bleeding, infection, damage to surrounding tissues, or complications related to anesthesia. Therefore, the decision to remove a medical device should be made carefully, considering both the potential benefits and risks of the procedure.
The ileocecal valve, also known as the Bauhin's valve, is a vital physiological structure in the gastrointestinal tract. It is a valve located at the junction between the ileum (the final portion of the small intestine) and the cecum (the first part of the large intestine or colon). This valve functions to control the flow of digesta from the small intestine into the large intestine, preventing backflow from the colon into the small intestine. It is an essential component in maintaining proper digestive function and gut health.
Aortography is a medical procedure that involves taking X-ray images of the aorta, which is the largest blood vessel in the body. The procedure is usually performed to diagnose or assess various conditions related to the aorta, such as aneurysms, dissections, or blockages.
To perform an aortography, a contrast dye is injected into the aorta through a catheter that is inserted into an artery, typically in the leg or arm. The contrast dye makes the aorta visible on X-ray images, allowing doctors to see its structure and any abnormalities that may be present.
The procedure is usually performed in a hospital or outpatient setting and may require sedation or anesthesia. While aortography can provide valuable diagnostic information, it also carries some risks, such as allergic reactions to the contrast dye, damage to blood vessels, or infection. Therefore, it is typically reserved for situations where other diagnostic tests have been inconclusive or where more invasive treatment may be required.
Heart sounds are the noises generated by the beating heart and the movement of blood through it. They are caused by the vibration of the cardiac structures, such as the valves, walls, and blood vessels, during the cardiac cycle.
There are two normal heart sounds, often described as "lub-dub," that can be heard through a stethoscope. The first sound (S1) is caused by the closure of the mitral and tricuspid valves at the beginning of systole, when the ventricles contract to pump blood out to the body and lungs. The second sound (S2) is produced by the closure of the aortic and pulmonary valves at the end of systole, as the ventricles relax and the ventricular pressure decreases, allowing the valves to close.
Abnormal heart sounds, such as murmurs, clicks, or extra sounds (S3 or S4), may indicate cardiac disease or abnormalities in the structure or function of the heart. These sounds can be evaluated through a process called auscultation, which involves listening to the heart with a stethoscope and analyzing the intensity, pitch, quality, and timing of the sounds.
A heart murmur is an abnormal sound heard during a heartbeat, which is caused by turbulent blood flow through the heart. It is often described as a blowing, whooshing, or rasping noise. Heart murmurs can be innocent (harmless and not associated with any heart disease) or pathological (indicating an underlying heart condition). They are typically detected during routine physical examinations using a stethoscope. The classification of heart murmurs includes systolic, diastolic, continuous, and functional murmurs, based on the timing and auscultatory location. Various heart conditions, such as valvular disorders, congenital heart defects, or infections, can cause pathological heart murmurs. Further evaluation with diagnostic tests like echocardiography is often required to determine the underlying cause and appropriate treatment.
Equipment design, in the medical context, refers to the process of creating and developing medical equipment and devices, such as surgical instruments, diagnostic machines, or assistive technologies. This process involves several stages, including:
1. Identifying user needs and requirements
2. Concept development and brainstorming
3. Prototyping and testing
4. Design for manufacturing and assembly
5. Safety and regulatory compliance
6. Verification and validation
7. Training and support
The goal of equipment design is to create safe, effective, and efficient medical devices that meet the needs of healthcare providers and patients while complying with relevant regulations and standards. The design process typically involves a multidisciplinary team of engineers, clinicians, designers, and researchers who work together to develop innovative solutions that improve patient care and outcomes.
The Kaplan-Meier estimate is a statistical method used to calculate the survival probability over time in a population. It is commonly used in medical research to analyze time-to-event data, such as the time until a patient experiences a specific event like disease progression or death. The Kaplan-Meier estimate takes into account censored data, which occurs when some individuals are lost to follow-up before experiencing the event of interest.
The method involves constructing a survival curve that shows the proportion of subjects still surviving at different time points. At each time point, the survival probability is calculated as the product of the conditional probabilities of surviving from one time point to the next. The Kaplan-Meier estimate provides an unbiased and consistent estimator of the survival function, even when censoring is present.
In summary, the Kaplan-Meier estimate is a crucial tool in medical research for analyzing time-to-event data and estimating survival probabilities over time while accounting for censored observations.
Hospital mortality is a term used to describe the number or rate of deaths that occur in a hospital setting during a specific period. It is often used as a measure of the quality of healthcare provided by a hospital, as a higher hospital mortality rate may indicate poorer care or more complex cases being treated. However, it's important to note that hospital mortality rates can be influenced by many factors, including the severity of illness of the patients being treated, patient demographics, and the availability of resources and specialized care. Therefore, hospital mortality rates should be interpreted with caution and in the context of other quality metrics.
The femoral artery is the major blood vessel that supplies oxygenated blood to the lower extremity of the human body. It is a continuation of the external iliac artery and becomes the popliteal artery as it passes through the adductor hiatus in the adductor magnus muscle of the thigh.
The femoral artery is located in the femoral triangle, which is bound by the sartorius muscle anteriorly, the adductor longus muscle medially, and the biceps femoris muscle posteriorly. It can be easily palpated in the groin region, making it a common site for taking blood samples, measuring blood pressure, and performing surgical procedures such as femoral artery catheterization and bypass grafting.
The femoral artery gives off several branches that supply blood to the lower limb, including the deep femoral artery, the superficial femoral artery, and the profunda femoris artery. These branches provide blood to the muscles, bones, skin, and other tissues of the leg, ankle, and foot.
Blood flow velocity is the speed at which blood travels through a specific part of the vascular system. It is typically measured in units of distance per time, such as centimeters per second (cm/s) or meters per second (m/s). Blood flow velocity can be affected by various factors, including cardiac output, vessel diameter, and viscosity of the blood. Measuring blood flow velocity is important in diagnosing and monitoring various medical conditions, such as heart disease, stroke, and peripheral vascular disease.
The postoperative period is the time following a surgical procedure during which the patient's response to the surgery and anesthesia is monitored, and any complications or adverse effects are managed. This period can vary in length depending on the type of surgery and the individual patient's needs, but it typically includes the immediate recovery phase in the post-anesthesia care unit (PACU) or recovery room, as well as any additional time spent in the hospital for monitoring and management of pain, wound healing, and other aspects of postoperative care.
The goals of postoperative care are to ensure the patient's safety and comfort, promote optimal healing and rehabilitation, and minimize the risk of complications such as infection, bleeding, or other postoperative issues. The specific interventions and treatments provided during this period will depend on a variety of factors, including the type and extent of surgery performed, the patient's overall health and medical history, and any individualized care plans developed in consultation with the patient and their healthcare team.
Aortitis is a medical condition characterized by inflammation of the aorta, which is the largest artery in the body that carries oxygenated blood from the heart to the rest of the body. The inflammation can cause damage to the aortic wall, leading to weakening, bulging (aneurysm), or tearing (dissection) of the aorta. Aortitis can be caused by various conditions, including infections, autoimmune diseases, and certain medications. It is essential to diagnose and treat aortitis promptly to prevent serious complications.
An artificial pacemaker is a medical device that uses electrical impulses to regulate the beating of the heart. It is typically used when the heart's natural pacemaker, the sinoatrial node, is not functioning properly and the heart rate is too slow or irregular. The pacemaker consists of a small generator that contains a battery and electronic circuits, which are connected to one or more electrodes that are placed in the heart.
The generator sends electrical signals through the electrodes to stimulate the heart muscle and cause it to contract, thereby maintaining a regular heart rhythm. Artificial pacemakers can be programmed to deliver electrical impulses at a specific rate or in response to the body's needs. They are typically implanted in the chest during a surgical procedure and can last for many years before needing to be replaced.
Artificial pacemakers are an effective treatment for various types of bradycardia, which is a heart rhythm disorder characterized by a slow heart rate. Pacemakers can significantly improve symptoms associated with bradycardia, such as fatigue, dizziness, shortness of breath, and fainting spells.
"Swine" is a common term used to refer to even-toed ungulates of the family Suidae, including domestic pigs and wild boars. However, in a medical context, "swine" often appears in the phrase "swine flu," which is a strain of influenza virus that typically infects pigs but can also cause illness in humans. The 2009 H1N1 pandemic was caused by a new strain of swine-origin influenza A virus, which was commonly referred to as "swine flu." It's important to note that this virus is not transmitted through eating cooked pork products; it spreads from person to person, mainly through respiratory droplets produced when an infected person coughs or sneezes.
A cardiac catheter is a thin, flexible tube that is inserted into the heart or adjacent blood vessels during a cardiac catheterization procedure. This procedure is typically performed to diagnose and treat various cardiovascular conditions such as heart disease, heart defects, or abnormal heart rhythms.
Cardiac catheters can be used for several purposes:
1. To measure the pressure and oxygen levels in different chambers of the heart and blood vessels.
2. To inject dye into the coronary arteries to visualize blockages or narrowing through angiography.
3. To perform interventions such as balloon angioplasty, stent placement, or valvuloplasty to open up blocked or narrowed blood vessels or repair damaged heart valves.
4. To collect samples of heart muscle tissue for biopsy, which can help diagnose conditions like cardiomyopathy or myocarditis.
There are various types of cardiac catheters, including:
1. Diagnostic catheters - used to measure pressure and oxygen levels in the heart and blood vessels.
2. Guiding catheters - used to guide other interventional devices like balloons or stents into place.
3. Angioplasty balloon catheters - used to inflate a balloon at the tip of the catheter, which helps open up blocked or narrowed blood vessels.
4. Thermodilution catheters - used to measure cardiac output and other hemodynamic parameters.
5. Microcatheters - smaller, more flexible catheters used for complex interventions or accessing difficult-to-reach areas of the heart and blood vessels.
Cardiac catheterization is a minimally invasive procedure that usually requires only local anesthesia and mild sedation. The recovery time is typically short, with most patients returning home within 24 hours after the procedure.
I believe there might be a misunderstanding in your question. "Glutaral" does not seem to be a recognized medical term or abbreviation in healthcare and biomedical sciences. It is possible that you may be looking for information on "glutaraldehyde," which is a disinfectant and sterilizing agent used in medical settings.
Glutaraldehyde is a chemical compound with the formula C5H8O2, and it's often used as a 2% solution. It's an effective agent against bacteria, viruses, and fungi, making it useful for sterilizing medical equipment. However, glutaraldehyde can cause respiratory issues and skin irritation in some individuals, so proper handling and use are essential to minimize exposure.
If you meant to ask about a different term or if this answer does not address your question, please provide more context or clarify your request, and I will be happy to help further.
Heart auscultation is a medical procedure in which a healthcare professional uses a stethoscope to listen to the sounds produced by the heart. The process involves placing the stethoscope on various locations of the chest wall to hear different areas of the heart.
The sounds heard during auscultation are typically related to the opening and closing of the heart valves, as well as the turbulence created by blood flow through the heart chambers. These sounds can provide important clues about the structure and function of the heart, allowing healthcare professionals to diagnose various cardiovascular conditions such as heart murmurs, valvular disorders, and abnormal heart rhythms.
Heart auscultation is a key component of a physical examination and requires proper training and experience to interpret the findings accurately.
Thromboembolism is a medical condition that refers to the obstruction of a blood vessel by a thrombus (blood clot) that has formed elsewhere in the body and then been transported by the bloodstream to a narrower vessel, where it becomes lodged. This process can occur in various parts of the body, leading to different types of thromboembolisms:
1. Deep Vein Thrombosis (DVT): A thrombus forms in the deep veins, usually in the legs or pelvis, and then breaks off and travels to the lungs, causing a pulmonary embolism.
2. Pulmonary Embolism (PE): A thrombus formed elsewhere, often in the deep veins of the legs, dislodges and travels to the lungs, blocking one or more pulmonary arteries. This can lead to shortness of breath, chest pain, and potentially life-threatening complications if not treated promptly.
3. Cerebral Embolism: A thrombus formed in another part of the body, such as the heart or carotid artery, dislodges and travels to the brain, causing a stroke or transient ischemic attack (TIA).
4. Arterial Thromboembolism: A thrombus forms in an artery and breaks off, traveling to another part of the body and blocking blood flow to an organ or tissue, leading to potential damage or loss of function. Examples include mesenteric ischemia (intestinal damage due to blocked blood flow) and retinal artery occlusion (vision loss due to blocked blood flow in the eye).
Prevention, early detection, and appropriate treatment are crucial for managing thromboembolism and reducing the risk of severe complications.
A dissecting aneurysm is a serious and potentially life-threatening condition that occurs when there is a tear in the inner layer of the artery wall, allowing blood to flow between the layers of the artery wall. This can cause the artery to bulge or balloon out, leading to a dissection aneurysm.
Dissecting aneurysms can occur in any artery, but they are most commonly found in the aorta, which is the largest artery in the body. When a dissecting aneurysm occurs in the aorta, it is often referred to as a "dissecting aortic aneurysm."
Dissecting aneurysms can be caused by various factors, including high blood pressure, atherosclerosis (hardening and narrowing of the arteries), genetic disorders that affect the connective tissue, trauma, or illegal drug use (such as cocaine).
Symptoms of a dissecting aneurysm may include sudden severe chest or back pain, which can feel like ripping or tearing, shortness of breath, sweating, lightheadedness, or loss of consciousness. If left untreated, a dissecting aneurysm can lead to serious complications, such as rupture of the artery, stroke, or even death.
Treatment for a dissecting aneurysm typically involves surgery or endovascular repair to prevent further damage and reduce the risk of rupture. The specific treatment approach will depend on various factors, including the location and size of the aneurysm, the patient's overall health, and their medical history.
Left ventricular hypertrophy (LVH) is a medical condition in which the left ventricle of the heart undergoes an enlargement or thickening of its muscle wall. The left ventricle is the main pumping chamber of the heart that supplies oxygenated blood to the rest of the body.
In response to increased workload, such as hypertension (high blood pressure), aortic valve stenosis, or athletic training, the left ventricular muscle may thicken and enlarge. This process is called "hypertrophy." While some degree of hypertrophy can be adaptive in athletes, significant or excessive hypertrophy can lead to impaired relaxation and filling of the left ventricle during diastole, reduced pumping capacity, and decreased compliance of the chamber.
Left ventricular hypertrophy is often asymptomatic initially but can increase the risk of various cardiovascular complications such as heart failure, arrhythmias, myocardial infarction (heart attack), and sudden cardiac death over time. It is typically diagnosed through imaging techniques like echocardiography or cardiac MRI and confirmed by measuring the thickness of the left ventricular wall.
Left ventricular dysfunction (LVD) is a condition characterized by the impaired ability of the left ventricle of the heart to pump blood efficiently during contraction. The left ventricle is one of the four chambers of the heart and is responsible for pumping oxygenated blood to the rest of the body.
LVD can be caused by various underlying conditions, such as coronary artery disease, cardiomyopathy, valvular heart disease, or hypertension. These conditions can lead to structural changes in the left ventricle, including remodeling, hypertrophy, and dilation, which ultimately impair its contractile function.
The severity of LVD is often assessed by measuring the ejection fraction (EF), which is the percentage of blood that is pumped out of the left ventricle during each contraction. A normal EF ranges from 55% to 70%, while an EF below 40% is indicative of LVD.
LVD can lead to various symptoms, such as shortness of breath, fatigue, fluid retention, and decreased exercise tolerance. It can also increase the risk of complications, such as heart failure, arrhythmias, and cardiac arrest. Treatment for LVD typically involves managing the underlying cause, along with medications to improve contractility, reduce fluid buildup, and control heart rate. In severe cases, devices such as implantable cardioverter-defibrillators (ICDs) or left ventricular assist devices (LVADs) may be required.
Prosthesis-related infections, also known as prosthetic joint infections (PJIs), are infections that occur around or within a prosthetic device, such as an artificial joint. These infections can be caused by bacteria, fungi, or other microorganisms and can lead to serious complications if not treated promptly and effectively.
Prosthesis-related infections can occur soon after the implantation of the prosthetic device (early infection) or months or even years later (late infection). Early infections are often caused by bacteria that enter the surgical site during the procedure, while late infections may be caused by hematogenous seeding (i.e., when bacteria from another source spread through the bloodstream and settle in the prosthetic device) or by contamination during a subsequent medical procedure.
Symptoms of prosthesis-related infections can include pain, swelling, redness, warmth, and drainage around the affected area. In some cases, patients may also experience fever, chills, or fatigue. Diagnosis typically involves a combination of clinical evaluation, laboratory tests (such as blood cultures, joint fluid analysis, and tissue biopsy), and imaging studies (such as X-rays, CT scans, or MRI).
Treatment of prosthesis-related infections usually involves a combination of antibiotics and surgical intervention. The specific treatment approach will depend on the type and severity of the infection, as well as the patient's overall health status. In some cases, it may be necessary to remove or replace the affected prosthetic device.
Body Surface Area (BSA) is a calculated value that is often used in medicine, pharmacology, and physiology to adjust dosages of medications or to estimate parameters based on body size. It is the total area of the exterior surface of the human body. The most widely used formula for estimating BSA in adults is the Mosteller formula:
BSA (m²) = √([height (cm)] x [weight (kg)] / 3600)
This formula uses the person's height and weight to estimate the body surface area. It's important to note that this formula, like all BSA formulas, is an approximation and may not be accurate for every individual. Other more complex formulas exist, such as the DuBois & DuBois formula or the Haycock formula, but the Mosteller formula is considered to be sufficiently accurate for most clinical purposes.
Cineangiography is a medical imaging technique used to visualize the blood flow in the heart and cardiovascular system. It involves the injection of a contrast agent into the bloodstream while X-ray images are taken in quick succession, creating a movie-like sequence that shows the movement of the contrast through the blood vessels and chambers of the heart. This technique is often used to diagnose and evaluate various heart conditions, such as coronary artery disease, valvular heart disease, and congenital heart defects.
The procedure typically involves threading a catheter through a blood vessel in the arm or leg and guiding it to the heart. Once in place, the contrast agent is injected, and X-ray images are taken using a specialized X-ray machine called a fluoroscope. The images captured during cineangiography can help doctors identify areas of narrowing or blockage in the coronary arteries, abnormalities in heart valves, and other cardiovascular problems.
Cineangiography is an invasive procedure that carries some risks, such as bleeding, infection, and reactions to the contrast agent. However, it can provide valuable information for diagnosing and treating heart conditions, and may be recommended when other diagnostic tests have been inconclusive.
Ventricular outflow obstruction is a term used in cardiology to describe a condition where there is an obstruction or narrowing in the flow of blood as it exits the heart's ventricles (the lower chambers of the heart). This obstruction can occur due to various reasons such as congenital heart defects, hypertrophic cardiomyopathy, or calcification of the aortic valve.
In a normal heart, the left ventricle pumps oxygenated blood into the aorta through the aortic valve, and the right ventricle pumps deoxygenated blood into the pulmonary artery through the pulmonic valve. Any obstruction in these outflow tracts can lead to increased pressure within the ventricles, which can result in various symptoms such as shortness of breath, chest pain, dizziness, or fatigue.
The severity of the obstruction and the resulting symptoms can vary depending on the location and extent of the narrowing. Treatment options may include medications, surgical procedures, or catheter-based interventions to alleviate the obstruction and improve blood flow.