Discrete Subaortic Stenosis
Aortic Stenosis, Subvalvular
Aortic Valve Insufficiency
Cardiac Valve Annuloplasty
Infant methylenetetrahydrofolate reductase 677TT genotype is a risk factor for congenital heart disease. (1/20)
OBJECTIVE: Recently, an association between the homozygous C677T mutation in the methylenetetrahydrofolate reductase (MTHFR) gene in infants with congenital neural tube defects or congenital oral clefts has been shown. However, no data are available so far with respect to the MTHFR 677TT genotype in children with underlying structural congenital heart disease (CHD). METHODS: We investigated the MTHFR genotype in 114 Caucasian CHD patients aged newborn to 16 years (median 0.6 years; 53% male) and in 228 age- and sex-matched healthy controls. RESULTS: In childhood patients with CHD the homozygous MTHFR 677TT genotype was found in 21 out of 114 subjects (18.4%) compared with 21 out of 228 controls (9.2%; odds ratio (OR) 2.2, 95%-confidence interval (CI) 1.2-4.3; P=0.027). In patients with pulmonary valve stenosis, hypoplastic left heart syndrome, coarctation of the aorta, aortic valve stenosis or subaortic stenosis the frequency of the TT genotype varied between 38 and 67% with corresponding ORs from 6.1 (CI, 1.4-27.5; P=0.034) to 20.4 (CI, 1.8-235.0; P=0.025), whereas in other structural CHD the frequency of this genotype was not significantly different from the controls. CONCLUSIONS: With the present study we can show for the first time that the embryonal MTHFR 677TT genotype is significantly associated with the development of structural congenital heart malformations during early pregnancy. It remains to be clarified, whether this genotype is at least a risk marker or a risk factor for structural congenital heart malformations. (+info)Discrete subaortic stenosis in adults: increased prevalence and slow rate of progression of the obstruction and aortic regurgitation. (2/20)
OBJECTIVES: We sought to determine the prevalence and rate of progression of left ventricular outflow tract obstruction (LVOTO) and aortic regurgitation (AR) in adults with discrete subaortic stenosis (DSS). BACKGROUND: Discrete subaortic stenosis is an uncommon form of LVOTO, with rapid hemodynamic progression in children, but the prevalence and rate of progression in adults have not been studied so far. METHODS: The prevalence of DSS was determined in 2,057 consecutive adults diagnosed with congenital heart disease (CHD). The relationship between LVOTO on Doppler echocardiography and patient age was analyzed. Sequential changes in LVOTO and AR were determined for patients with two or more Doppler echocardiograms obtained with at least a two-year interval. RESULTS: A total of 134 adults (mean age 31 +/- 17 years) were diagnosed with DSS. The prevalence was 6.5% for all adults with CHD. Sixty patients (44%) had other associated CHD. The mean age of 29 patients who had undergone an operation for DSS during their adult life (56 +/- 15 years) was significantly higher than that of 64 patients (27 +/- 13 years) who had not required a surgical intervention (p < 0.0001). A significant relationship between LVOTO and patient age (r = 0.61, p < 0.0001) was found: 21 +/- 16 mm Hg in patients <25 years old, 51 +/- 47 mm Hg for those between 25 and 50 years old, and 78 +/- 36 mm Hg for those >50 years old. The LVOTO increased from 39.2 +/- 28 to 46.8 +/- 34 mm Hg (p = 0.01) during a mean follow-up of 4.8 +/- 1.8 years in 25 patients. The slope of the change in LVOTO was 2.25 +/- 4.7 mm Hg per year of follow-up. Aortic regurgitation was detected by color Doppler imaging in 109 patients (81%), but it was hemodynamically significant in <20%. An increase in the mean degree of AR over time was not significant (baseline: 1.3 +/- 0.8; follow-up: 1.5 +/- 0.9; p = 0.096). CONCLUSIONS: The prevalence of DSS is increasing in adults due to the greater number of repaired CHDs that develop into evolutive DSS. In contrast to infants and children, adults with DSS show a slow rate of LVOTO progression. Aortic regurgitation is a common but usually mild and nonprogressive consequence. The current indications for surgical intervention should be revised. (+info)Rheology of discrete subaortic stenosis. (3/20)
The discrete form of subaortic stenosis is thought to be an acquired lesion, the aetiology of which may be a combination of factors which include an underlying genetic predisposition, turbulence in the left ventricular outflow tract, and various geometric and anatomical variations of the left ventricular outflow tract. A review of hypotheses relating to its aetiology is provided (+info)Discrete subaortic stenosis: surgical outcomes and follow-up results. (4/20)
Discrete subaortic stenosis, which is an obstructing lesion of the left ventricular outflow tract, remains a surgical challenge. The recurrence rate is high despite sufficient conventional resection. We retrospectively reviewed the results of surgery for discrete subaortic stenosis at our institution from September 1995 through March 2001. Twenty-one patients with this lesion underwent surgical treatment during this period. Excision of the fibromuscular membrane with myectomy was performed in all of the patients. Follow-up in all patients ranged from 7 to 67 months (mean follow-up period, 39.57 +/- 15.46 months). The mean systolic gradient between the left ventricle and the aorta decreased from 59.23 +/- 35.38 mmHg preoperatively to 9.47 +/- 9.91 mmHg postoperatively. There was no instance of heart block that required a permanent pacemaker, nor of bacterial endocarditis. There was no early or late postoperative death. A 22nd patient, who had 3+ aortic regurgitation, required aortic valve replacement and was excluded from the study. Two of the patients (9.5%) underwent reoperation because of recurrent gradient and residual ventricular septal defect. Our results suggest that fibromuscular membrane excision combined with myectomy in patients with discrete subaortic stenosis produces sufficient relief of obstruction with low morbidity. (+info)Subaortic obstruction and complete atrioventricular block in Behcet's disease. (5/20)
Left ventricular outflow tract obstruction may be dynamic, most commonly associated with hypertrophic cardiomyopathy, and, uncommonly, by congenital anomalies such as discrete subaortic stenosis. We describe a patient with Behcet's disease, presenting with a systolic murmur, fever, and syncope, in whom a diagnosis of subaortic obstruction caused by a pseudo-aneurysm dissecting the interventricular septum and associated with a complete atrioventricular block was made. (+info)Discrete subaortic stenosis in elderly women. (6/20)
Discrete subaortic stenosis (DSS) is likely an acquired cardiac disorder which requires anatomic precursors and a genetic background. DSS occurs usually within the first decade, provoking rapidly progressive left ventricular outflow tract obstruction and secondary aortic regurgitation. DSS has been considered for a long time exclusively a disease of infancy and childhood and few reports and small series have described DSS in adulthood and only two cases are reported in elderly. Our case describes a discrete subaortic membranous ridge in an elderly woman with recent onset of dyspnea. (+info)Risk factors for reoperation after repair of discrete subaortic stenosis in children. (7/20)
OBJECTIVES: This study aimed to identify independent predictors of reoperation after successful resection of discrete subaortic stenosis (DSS). BACKGROUND: Recurrence of DSS has been reported to range from 0% to 55% of patients. Factors associated with recurrence have not been adequately defined. METHODS: Patients were included if they had a diagnosis of DSS, normal segmental cardiac anatomy, previous resection of DSS, and at least 36 months' follow-up. Demographic, surgical, and echocardiographic data were analyzed. Primary outcome was repeat resection of DSS in patients after successful primary resection. RESULTS: Of 111 subjects who had successful surgical resection of DSS, 16 patients (14%) required reoperation. Median follow-up time was 8.2 years. Form of DSS and gender did not differ significantly between those with reoperation and those without. In multivariate analysis, independent predictors of reoperation that would be available before first surgery were <6 mm distance between the aortic valve (AoV) and the obstruction (hazard ratio [HR] 5.1; p = 0.013) and peak gradient by Doppler > or =60 mm Hg (HR 4.2; p = 0.016). If intraoperative variables are also considered, peeling of the membrane from the AoV or mitral valve at first surgery, <6 mm distance between the DSS and AoV, and peak gradient by Doppler > or =60 mm Hg were independent predictors of reoperation. CONCLUSIONS: Proximity of the obstructive lesion to the AoV and severe obstruction determined by preoperative echocardiography, as well as involvement of valve leaflets requiring surgical peeling, predict recurrent DSS requiring reoperation. (+info)The "1st septal unit" in hypertrophic obstructive cardiomyopathy: a newly recognized anatomo-functional entity, identified during recent alcohol septal ablation experience. (8/20)
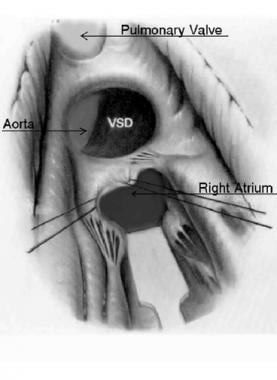
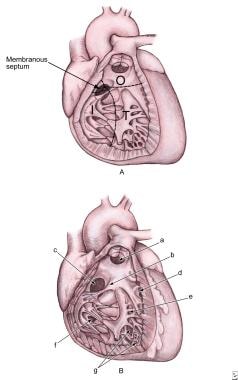
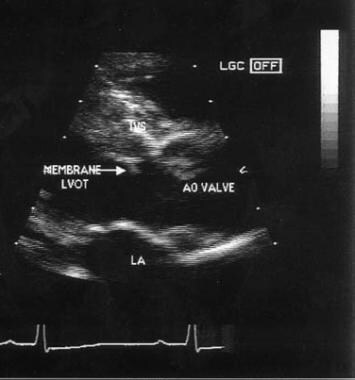
In hypertrophic obstructive cardiomyopathy, selective and asymmetric hypertrophy results in a stenotic subaortic channel, which is further narrowed by a Venturi effect (suctioning of the anterior leaflet, manifested by systolic anterior motion of the mitral valve). Better understanding of these essential pathophysiologic mechanisms has led to the definition of a new anatomo-functional entity, the 1st septal unit, which consists of the basal interventricular septal hypertrophy and its related septal arterial branches. As an alternative to surgical myomectomy, alcohol septal ablation is an effective method of reducing subaortic stenosis and improving mitral valve function. After alcohol ablation, global negative remodeling of the hypertrophied left ventricle eventually ensues. This review presents specific anatomic and functional features of a newly identified pathophysiologic entity (the 1st septal unit) in relation to the clinical manifestations and natural history of hypertrophic obstructive cardiomyopathy. This relationship is also relevant during the performance of alcohol septal ablation interventions: related operative suggestions are provided for optimizing subaortic stenosis relief during septal ablation and for preventing complications. (+info)Discrete subaortic stenosis is a medical condition that refers to a narrowing (stenosis) in the outflow tract below the aortic valve of the heart. This narrowing is usually caused by a fibrous ring or a discrete ridge of tissue that partially obstructs the flow of blood from the left ventricle into the aorta.
Discrete subaortic stenosis can cause various symptoms, including shortness of breath, chest pain, fatigue, and syncope (fainting). In severe cases, it can lead to heart failure or even sudden death. The condition is often diagnosed using echocardiography, which can help evaluate the severity of the narrowing and any associated abnormalities.
Treatment for discrete subaortic stenosis typically involves surgical intervention to remove the obstructive tissue and relieve the obstruction. In some cases, a mechanical valve may be implanted to replace the damaged aortic valve. Regular follow-up care is necessary to monitor for any potential complications or recurrence of the narrowing.
Aortic stenosis, subvalvular is a medical condition that refers to the narrowing or obstruction of the outflow tract below the aortic valve in the heart. This abnormal narrowing can be caused by various factors such as a congenital heart defect, a tissue growth, or scarring from previous procedures. As a result, the left ventricle must work harder to pump blood through the narrowed opening, which can lead to thickening of the heart muscle (hypertrophy) and decreased cardiac output. Symptoms may include chest pain, shortness of breath, fatigue, and dizziness or fainting spells. Severe subvalvular aortic stenosis can lead to serious complications such as heart failure or even sudden death, and may require surgical intervention to correct the problem.
Aortic valve insufficiency, also known as aortic regurgitation or aortic incompetence, is a cardiac condition in which the aortic valve does not close properly during the contraction phase of the heart cycle. This allows blood to flow back into the left ventricle from the aorta, instead of being pumped out to the rest of the body. As a result, the left ventricle must work harder to maintain adequate cardiac output, which can lead to left ventricular enlargement and heart failure over time if left untreated.
The aortic valve is a trileaflet valve that lies between the left ventricle and the aorta. During systole (the contraction phase of the heart cycle), the aortic valve opens to allow blood to be pumped out of the left ventricle into the aorta and then distributed to the rest of the body. During diastole (the relaxation phase of the heart cycle), the aortic valve closes to prevent blood from flowing back into the left ventricle.
Aortic valve insufficiency can be caused by various conditions, including congenital heart defects, infective endocarditis, rheumatic heart disease, Marfan syndrome, and trauma. Symptoms of aortic valve insufficiency may include shortness of breath, fatigue, chest pain, palpitations, and edema (swelling). Diagnosis is typically made through physical examination, echocardiography, and other imaging studies. Treatment options depend on the severity of the condition and may include medication, surgery to repair or replace the aortic valve, or a combination of both.
Cardiac valve annuloplasty is a surgical procedure that involves repairing and reinforcing the ring-like structure (annulus) surrounding the heart valves, primarily the mitral or tricuspid valves. This procedure is often performed to correct valve leaks or regurgitation caused by various conditions such as valve disease or dilated cardiomyopathy.
During the annuloplasty procedure, the surgeon typically uses an artificial ring-like device (annuloplasty ring) made of fabric, metal, or a combination of both to reshape and stabilize the damaged annulus. The ring is sewn in place, reducing the size of the valve opening and helping the valve leaflets to coapt properly, thereby preventing valve leaks and improving heart function.
Annuloplasty can be performed as a standalone procedure or in combination with other cardiac surgeries such as valve replacement or repair. The specific technique and approach may vary depending on the individual patient's needs and the surgeon's preference.
Aortic valve stenosis is a cardiac condition characterized by the narrowing or stiffening of the aortic valve, which separates the left ventricle (the heart's main pumping chamber) from the aorta (the large artery that carries oxygen-rich blood to the rest of the body). This narrowing or stiffening prevents the aortic valve from opening fully, resulting in reduced blood flow from the left ventricle to the aorta and the rest of the body.
The narrowing can be caused by several factors, including congenital heart defects, calcification (hardening) of the aortic valve due to aging, or scarring of the valve due to rheumatic fever or other inflammatory conditions. As a result, the left ventricle must work harder to pump blood through the narrowed valve, which can lead to thickening and enlargement of the left ventricular muscle (left ventricular hypertrophy).
Symptoms of aortic valve stenosis may include chest pain or tightness, shortness of breath, fatigue, dizziness or fainting, and heart palpitations. Severe aortic valve stenosis can lead to serious complications such as heart failure, arrhythmias, or even sudden cardiac death. Treatment options may include medications to manage symptoms, lifestyle changes, or surgical intervention such as aortic valve replacement.