Wounds and Injuries
Brain Injuries
Spinal Cord Injuries
Reperfusion Injury
Injury Severity Score
Lung Injury
Eye Injuries
The effect of using a tourniquet on the intensity of postoperative pain in forearm fractures. A randomized study in 32 surgically treated patients. (1/74)
We have analysed the relationship between the intensity of postoperative pain and the use of a pneumatic tourniquet in procedures for operative fixation of fractures of the forearm. Thirty-two patients were divided randomly into two groups as a control (NT) and tourniquet (T). The pain scores in the NT group were significantly lower. Patients over the age of 30 had notably more pain than those younger after the use of a tourniquet. Avoidance of the tourniquet gave better postoperative analgesia in male patients and in those with comminuted fractures. When a tourniquet was used the best results were obtained if it was kept inflated for less than one hour. (+info)Incidence and causes of tenosynovitis of the wrist extensors in long distance paddle canoeists. (2/74)
OBJECTIVES: To investigate the incidence and causes of acute tenosynovitis of the forearm of long distance canoeists. METHOD: A systematic sample of canoeists competing in four canoe marathons were interviewed. The interview included questions about the presence and severity of pain in the forearm and average training distances. Features of the paddles and canoes were determined. RESULTS: An average of 23% of the competitors in each race developed this condition. The incidence was significantly higher in the dominant than the nondominant hand but was unrelated to the type of canoe and the angle of the paddle blades. Canoeists who covered more than 100 km a week for eight weeks preceding the race had a significantly lower incidence of tenosynovitis than those who trained less. Environmental conditions during racing, including fast flowing water, high winds, and choppy waters, and the paddling techniques, especially hyperextension of the wrist during the pushing phase of the stroke, were both related to the incidence of tenosynovitis. CONCLUSION: Tenosynovitis is a common injury in long distance canoeists. The study suggests that development of tenosynovitis is not related to the equipment used, but is probably caused by difficult paddling conditions, in particular uneven surface conditions, which may cause an altered paddling style. However, a number of factors can affect canoeing style. Level of fitness and the ability to balance even a less stable canoe, thereby maintaining optimum paddling style without repeated eccentric loading of the forearm tendons to limit hyperextension of the wrist, would seem to be important. (+info)The wrist of the formula 1 driver. (3/74)
OBJECTIVES: During formula 1 driving, repetitive cumulative trauma may provoke nerve disorders such as nerve compression syndrome as well as osteoligament injuries. A study based on interrogatory and clinical examination of 22 drivers was carried out during the 1998 formula 1 World Championship in order to better define the type and frequency of these lesions. METHODS: The questions investigated nervous symptoms, such as paraesthesia and diminishment of sensitivity, and osteoligamentous symptoms, such as pain, specifying the localisation (ulnar side, dorsal aspect of the wrist, snuff box) and the effect of the wrist position on the intensity of the pain. Clinical examination was carried out bilaterally and symmetrically. RESULTS: Fourteen of the 22 drivers reported symptoms. One suffered cramp in his hands at the end of each race and one described a typical forearm effort compartment syndrome. Six drivers had effort "osteoligamentous" symptoms: three scapholunate pain; one medial hypercompression of the wrist; two sequellae of a distal radius fracture. Seven reported nerve disorders: two effort carpal tunnel syndromes; one typical carpal tunnel syndrome; one effort cubital tunnel syndrome; three paraesthesia in all fingers at the end of a race, without any objective signs. CONCLUSIONS: This appears to be the first report of upper extremity disorders in competition drivers. The use of a wrist pad to reduce the effects of vibration may help to prevent trauma to the wrist in formula 1 drivers. (+info)Use of a delayed cortical bone graft to treat diaphyseal defects in the forearm. (4/74)
The technique of delayed autogenous cortical bone grafting was used in 17 patients (6 women, 11 men, with an average age of 22 years) to treat diaphyseal defects resulting mainly from closed or compound fractures complicated by infection and bone tissue loss. Bones affected were the humerus in 1 case, the radius in 7 cases, the ulna in 4 cases, the radius and ulna in 2 cases, the first metacarpal in 1 case, and the femur in 2 cases. The average length of the defect was 5.7 cm and the graft, prepared from the anteromedial aspec of the tibia, was at least 1.5 cm longer than the defect. The graft application was combined with rigid internal fixation using an AO 3.5 mm DCP plate in most cases and this permitted early active movement. Union occurred without the need for any additional grafting procedure in 14 patients and within an average of 23 weeks. In most cases there was an increase in the thickness of the graft probably as a result of osteo-induction, with consequent restoration of the original diameter of the recipient bone diaphysis. The most frequent complication was infection (4 cases), and this was controlled by means of debridement, cleaning and antibiotics. A delayed graft provides mechanical support, incorporates quickly and is therefore a reasonable alternative method for treating diaphyseal defects of long bones, particularly in the upper limb. (+info)Ultrasound imaging of forearm fractures in children: a viable alternative? (5/74)
OBJECTIVE: A pilot study to investigate whether ultrasonography can be reliably used to demonstrate uncomplicated greenstick and torus fractures in children. METHOD: Children between the ages of 2 and 14 years with a high clinical suspicion of a non-articular, undisplaced forearm fracture were included. Ultrasound imaging of the injury was performed by a consultant radiologist who gave an immediate report. Standard radiographs of the forearm were then obtained and the patient treated in the normal way. The radiograph was formally reported on at a later date. RESULTS: 26 patients were included. There was an absolute correlation between the ultrasound and radiographic findings. The procedure was well tolerated. CONCLUSION: Ultrasound seems effective for detecting uncomplicated forearm fractures in children. The procedure is easy to perform and the images easy to interpret. A larger study will now be undertaken to confirm these initial findings. (+info)Lengthening of congenital below-elbow amputation stumps by the Ilizarov technique. (6/74)
Patients with short congenital amputations below the elbow often function as if they have had a disarticulation of the elbow. We have reviewed the results in six patients who had lengthening of such stumps by the Ilizarov technique to improve the fitting of prostheses. The mean lengthening was 5.6 cm (3.4 to 8.4), and in two patients flexion contractures of the elbows were corrected simultaneously. Additional lateral distraction was used in one patient to provide a better surface on the stump. There were no major complications. All six patients were able to use their prosthesis at the latest follow-up after 39 to 78 months. (+info)Evaluation of pressure beneath a split above elbow plaster cast. (7/74)
It has previously been shown that splitting a plaster cast after manipulation of, or surgery on, a limb leads to a decrease in pressure beneath the cast by accommodating the swelling that may occur. However, it is not known whether the axis along which the cast is split influences the amount of swelling that can occur before a critical pressure is reached. We investigated this with reference to above elbow plaster casts. (+info)Treatment of unstable fractures of the forearm in children. Is plating of a single bone adequate? (8/74)
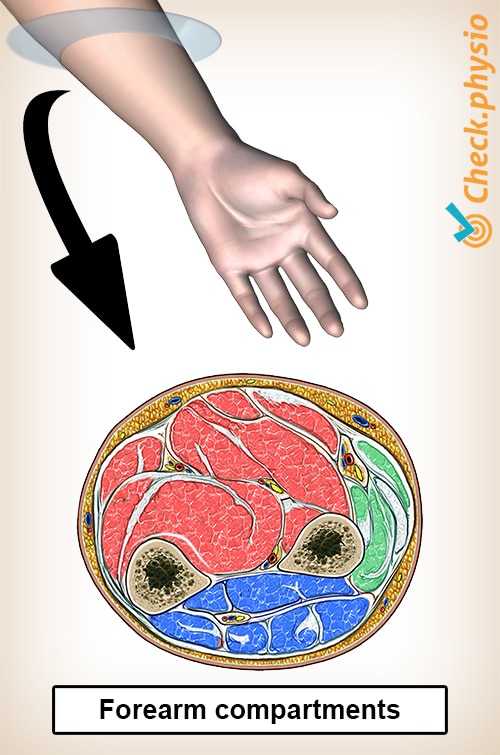
Unstable fractures of the forearm in children present problems in management and in the indications for operative treatment. In children, unlike adults, the fractures nearly always unite, and up to 10 degrees of angulation is usually considered to be acceptable. If surgical intervention is required the usual practice in the UK is to plate both bones as in an adult. We studied, retrospectively, 32 unstable fractures of the forearm in children treated by compression plating. Group A (20 children) had conventional plating of both forearm bones and group B (12 children) had plating of the ulna only. The mean age was 11 years in both groups and 23 (71%) of the fractures were in the midshaft. In group B an acceptable position of the radius was regarded as less than 10 degrees of angulation in both anteroposterior (AP) and lateral planes, and with the bone ends hitched. This was achieved by closed means in all except two cases, which were therefore included in group A. Union was achieved in all patients, the mean time being 9.8 weeks in group A and 11.5 weeks in B. After a mean interval of at least 12 months, 14 children in group A and nine in group B had their fixation devices removed. We analysed the results after the initial operation in all 32 children. The 23 who had the plate removed were assessed at final review. The results were graded on the ability to undertake physical activities and an objective assessment of loss of rotation of the forearm. In group A, complications were noted in eight patients (40%) after fixation and in six (42%) in relation to removal of the radial plate. No complications occurred in group B. The final range of movement and radiological appearance were compared in the two groups. There was a greater loss of pronation than supination in both. There was, however, no limitation of function in any patient and no difference in the degree of rotational loss between the two groups. The mean radiological angulation in both was less than 10 degrees in both AP and lateral views, which was consistent with satisfactory function. The final outcome for 23 patients was excellent or good in 12 of 14 (90%) in group A, despite the complications, and in eight of nine in group B (90%). If reduction and fixation of the fracture of the ulna alone restores acceptable alignment of the radius in unstable fractures of the forearm, operation on the radius can be avoided. (+info)Forearm injuries refer to damages or traumas that affect the anatomy and function of the forearm, which is the area between the elbow and wrist. This region consists of two long bones (the radius and ulna) and several muscles, tendons, ligaments, nerves, and blood vessels that enable movements such as flexion, extension, pronation, and supination of the hand and wrist.
Common forearm injuries include:
1. Fractures: Breaks in the radius or ulna bones can occur due to high-energy trauma, falls, or sports accidents. These fractures may be simple (stable) or compound (displaced), and might require immobilization, casting, or surgical intervention depending on their severity and location.
2. Sprains and Strains: Overstretching or tearing of the ligaments connecting the bones in the forearm or the muscles and tendons responsible for movement can lead to sprains and strains. These injuries often cause pain, swelling, bruising, and limited mobility.
3. Dislocations: In some cases, forceful trauma might result in the dislocation of the radioulnar joint, where the ends of the radius and ulna meet. This injury can be extremely painful and may necessitate immediate medical attention to realign the bones and stabilize the joint.
4. Tendonitis: Repetitive motions or overuse can cause inflammation and irritation of the tendons in the forearm, resulting in a condition known as tendonitis. This injury typically presents with localized pain, swelling, and stiffness that worsen with activity.
5. Nerve Injuries: Direct trauma, compression, or stretching can damage nerves in the forearm, leading to numbness, tingling, weakness, or paralysis in the hand and fingers. Common nerve injuries include radial nerve neuropathy and ulnar nerve entrapment.
6. Compartment Syndrome: Forearm compartment syndrome occurs when increased pressure within one of the forearm's fascial compartments restricts blood flow to the muscles, nerves, and tissues inside. This condition can result from trauma, bleeding, or swelling and requires immediate medical intervention to prevent permanent damage.
Accurate diagnosis and appropriate treatment are crucial for managing forearm injuries and ensuring optimal recovery. Patients should consult with a healthcare professional if they experience persistent pain, swelling, stiffness, weakness, or numbness in their forearms or hands.
A wound is a type of injury that occurs when the skin or other tissues are cut, pierced, torn, or otherwise broken. Wounds can be caused by a variety of factors, including accidents, violence, surgery, or certain medical conditions. There are several different types of wounds, including:
* Incisions: These are cuts that are made deliberately, often during surgery. They are usually straight and clean.
* Lacerations: These are tears in the skin or other tissues. They can be irregular and jagged.
* Abrasions: These occur when the top layer of skin is scraped off. They may look like a bruise or a scab.
* Punctures: These are wounds that are caused by sharp objects, such as needles or knives. They are usually small and deep.
* Avulsions: These occur when tissue is forcibly torn away from the body. They can be very serious and require immediate medical attention.
Injuries refer to any harm or damage to the body, including wounds. Injuries can range from minor scrapes and bruises to more severe injuries such as fractures, dislocations, and head trauma. It is important to seek medical attention for any injury that is causing significant pain, swelling, or bleeding, or if there is a suspected bone fracture or head injury.
In general, wounds and injuries should be cleaned and covered with a sterile bandage to prevent infection. Depending on the severity of the wound or injury, additional medical treatment may be necessary. This may include stitches for deep cuts, immobilization for broken bones, or surgery for more serious injuries. It is important to follow your healthcare provider's instructions carefully to ensure proper healing and to prevent complications.
A brain injury is defined as damage to the brain that occurs following an external force or trauma, such as a blow to the head, a fall, or a motor vehicle accident. Brain injuries can also result from internal conditions, such as lack of oxygen or a stroke. There are two main types of brain injuries: traumatic and acquired.
Traumatic brain injury (TBI) is caused by an external force that results in the brain moving within the skull or the skull being fractured. Mild TBIs may result in temporary symptoms such as headaches, confusion, and memory loss, while severe TBIs can cause long-term complications, including physical, cognitive, and emotional impairments.
Acquired brain injury (ABI) is any injury to the brain that occurs after birth and is not hereditary, congenital, or degenerative. ABIs are often caused by medical conditions such as strokes, tumors, anoxia (lack of oxygen), or infections.
Both TBIs and ABIs can range from mild to severe and may result in a variety of physical, cognitive, and emotional symptoms that can impact a person's ability to perform daily activities and function independently. Treatment for brain injuries typically involves a multidisciplinary approach, including medical management, rehabilitation, and supportive care.
Athletic injuries are damages or injuries to the body that occur while participating in sports, physical activities, or exercise. These injuries can be caused by a variety of factors, including:
1. Trauma: Direct blows, falls, collisions, or crushing injuries can cause fractures, dislocations, contusions, lacerations, or concussions.
2. Overuse: Repetitive motions or stress on a particular body part can lead to injuries such as tendonitis, stress fractures, or muscle strains.
3. Poor technique: Using incorrect form or technique during exercise or sports can put additional stress on muscles, joints, and ligaments, leading to injury.
4. Inadequate warm-up or cool-down: Failing to properly prepare the body for physical activity or neglecting to cool down afterwards can increase the risk of injury.
5. Lack of fitness or flexibility: Insufficient strength, endurance, or flexibility can make individuals more susceptible to injuries during sports and exercise.
6. Environmental factors: Extreme weather conditions, poor field or court surfaces, or inadequate equipment can contribute to the risk of athletic injuries.
Common athletic injuries include ankle sprains, knee injuries, shoulder dislocations, tennis elbow, shin splints, and concussions. Proper training, warm-up and cool-down routines, use of appropriate protective gear, and attention to technique can help prevent many athletic injuries.
Spinal cord injuries (SCI) refer to damage to the spinal cord that results in a loss of function, such as mobility or feeling. This injury can be caused by direct trauma to the spine or by indirect damage resulting from disease or degeneration of surrounding bones, tissues, or blood vessels. The location and severity of the injury on the spinal cord will determine which parts of the body are affected and to what extent.
The effects of SCI can range from mild sensory changes to severe paralysis, including loss of motor function, autonomic dysfunction, and possible changes in sensation, strength, and reflexes below the level of injury. These injuries are typically classified as complete or incomplete, depending on whether there is any remaining function below the level of injury.
Immediate medical attention is crucial for spinal cord injuries to prevent further damage and improve the chances of recovery. Treatment usually involves immobilization of the spine, medications to reduce swelling and pressure, surgery to stabilize the spine, and rehabilitation to help regain lost function. Despite advances in treatment, SCI can have a significant impact on a person's quality of life and ability to perform daily activities.
Reperfusion injury is a complex pathophysiological process that occurs when blood flow is restored to previously ischemic tissues, leading to further tissue damage. This phenomenon can occur in various clinical settings such as myocardial infarction (heart attack), stroke, or peripheral artery disease after an intervention aimed at restoring perfusion.
The restoration of blood flow leads to the generation of reactive oxygen species (ROS) and inflammatory mediators, which can cause oxidative stress, cellular damage, and activation of the immune system. This results in a cascade of events that may lead to microvascular dysfunction, capillary leakage, and tissue edema, further exacerbating the injury.
Reperfusion injury is an important consideration in the management of ischemic events, as interventions aimed at restoring blood flow must be carefully balanced with potential harm from reperfusion injury. Strategies to mitigate reperfusion injury include ischemic preconditioning (exposing the tissue to short periods of ischemia before a prolonged ischemic event), ischemic postconditioning (applying brief periods of ischemia and reperfusion after restoring blood flow), remote ischemic preconditioning (ischemia applied to a distant organ or tissue to protect the target organ), and pharmacological interventions that scavenge ROS, reduce inflammation, or improve microvascular function.
Regional blood flow (RBF) refers to the rate at which blood flows through a specific region or organ in the body, typically expressed in milliliters per minute per 100 grams of tissue (ml/min/100g). It is an essential physiological parameter that reflects the delivery of oxygen and nutrients to tissues while removing waste products. RBF can be affected by various factors such as metabolic demands, neural regulation, hormonal influences, and changes in blood pressure or vascular resistance. Measuring RBF is crucial for understanding organ function, diagnosing diseases, and evaluating the effectiveness of treatments.
Plethysmography is a non-invasive medical technique used to measure changes in volume or blood flow within an organ or body part, typically in the lungs or extremities. There are several types of plethysmography, including:
1. **Whole Body Plethysmography (WBP):** This type of plethysmography is used to assess lung function and volumes by measuring changes in pressure within a sealed chamber that contains the patient's entire body except for their head. The patient breathes normally while wearing a nose clip, allowing technicians to analyze respiratory patterns, airflow, and lung volume changes.
2. **Segmental or Local Plethysmography:** This technique measures volume or blood flow changes in specific body parts, such as the limbs or digits. It can help diagnose and monitor conditions affecting peripheral circulation, like deep vein thrombosis, arterial occlusive disease, or Raynaud's phenomenon.
3. **Impedance Plethysmography (IPG):** This non-invasive method uses electrical impedance to estimate changes in blood volume within an organ or body part. By applying a small electrical current and measuring the opposition to flow (impedance), technicians can determine variations in blood volume, which can help diagnose conditions like deep vein thrombosis or heart failure.
4. **Optical Plethysmography:** This technique uses light to measure changes in blood volume, typically in the skin or mucous membranes. By shining a light on the area and analyzing the reflected or transmitted light, technicians can detect variations in blood volume related to cardiac output, respiration, or other physiological factors.
Overall, plethysmography is an essential tool for diagnosing and monitoring various medical conditions affecting circulation, respiratory function, and organ volumes.
An ulna fracture is a break in the ulna bone, which is one of the two long bones in the forearm. The ulna is located on the pinky finger side of the forearm and functions to support the elbow joint and assist in rotation and movement of the forearm. Ulna fractures can occur at various points along the bone, including the shaft, near the wrist, or at the elbow end of the bone. Symptoms may include pain, swelling, bruising, tenderness, deformity, limited mobility, and in some cases, numbness or tingling in the fingers. Treatment typically involves immobilization with a cast or splint, followed by rehabilitation exercises to restore strength and range of motion. In severe cases, surgery may be required to realign and stabilize the fractured bone.
The Injury Severity Score (ISS) is a medical scoring system used to assess the severity of trauma in patients with multiple injuries. It's based on the Abbreviated Injury Scale (AIS), which classifies each injury by body region on a scale from 1 (minor) to 6 (maximum severity).
The ISS is calculated by summing the squares of the highest AIS score in each of the three most severely injured body regions. The possible ISS ranges from 0 to 75, with higher scores indicating more severe injuries. An ISS over 15 is generally considered a significant injury, and an ISS over 25 is associated with a high risk of mortality. It's important to note that the ISS has limitations, as it doesn't consider the number or type of injuries within each body region, only the most severe one.
Leg injuries refer to damages or harm caused to any part of the lower extremity, including the bones, muscles, tendons, ligaments, blood vessels, and other soft tissues. These injuries can result from various causes such as trauma, overuse, or degenerative conditions. Common leg injuries include fractures, dislocations, sprains, strains, contusions, and cuts. Symptoms may include pain, swelling, bruising, stiffness, weakness, or difficulty walking. The specific treatment for a leg injury depends on the type and severity of the injury.
Lung injury, also known as pulmonary injury, refers to damage or harm caused to the lung tissue, blood vessels, or air sacs (alveoli) in the lungs. This can result from various causes such as infection, trauma, exposure to harmful substances, or systemic diseases. Common types of lung injuries include acute respiratory distress syndrome (ARDS), pneumonia, and chemical pneumonitis. Symptoms may include difficulty breathing, cough, chest pain, and decreased oxygen levels in the blood. Treatment depends on the underlying cause and may include medications, oxygen therapy, or mechanical ventilation.
Eye injuries refer to any damage or trauma caused to the eye or its surrounding structures. These injuries can vary in severity and may include:
1. Corneal abrasions: A scratch or scrape on the clear surface of the eye (cornea).
2. Chemical burns: Occurs when chemicals come into contact with the eye, causing damage to the cornea and other structures.
3. Eyelid lacerations: Cuts or tears to the eyelid.
4. Subconjunctival hemorrhage: Bleeding under the conjunctiva, the clear membrane that covers the white part of the eye.
5. Hyphema: Accumulation of blood in the anterior chamber of the eye, which is the space between the cornea and iris.
6. Orbital fractures: Breaks in the bones surrounding the eye.
7. Retinal detachment: Separation of the retina from its underlying tissue, which can lead to vision loss if not treated promptly.
8. Traumatic uveitis: Inflammation of the uvea, the middle layer of the eye, caused by trauma.
9. Optic nerve damage: Damage to the optic nerve, which transmits visual information from the eye to the brain.
Eye injuries can result from a variety of causes, including accidents, sports-related injuries, violence, and chemical exposure. It is important to seek medical attention promptly for any suspected eye injury to prevent further damage and potential vision loss.
Hand injuries refer to any damage or harm caused to the structures of the hand, including the bones, joints, muscles, tendons, ligaments, nerves, blood vessels, and skin. These injuries can result from various causes such as trauma, overuse, or degenerative conditions. Examples of hand injuries include fractures, dislocations, sprains, strains, cuts, burns, and insect bites. Symptoms may vary depending on the type and severity of the injury, but they often include pain, swelling, stiffness, numbness, weakness, or loss of function in the hand. Proper diagnosis and treatment are crucial to ensure optimal recovery and prevent long-term complications.
 Medial epicondyle of the humerus
Medial epicondyle of the humerus Elbow and Forearm Overuse Injuries: Practice Essentials, Background, Epidemiology
Elbow and Forearm Overuse Injuries: Practice Essentials, Background, Epidemiology Harrison Bader forearm injury, to miss start of season
Harrison Bader forearm injury, to miss start of season Marlins' Alcantara confident of 2023 return despite forearm injury | theScore.com
Marlins' Alcantara confident of 2023 return despite forearm injury | theScore.com Pats put TE Gronkowski on IR with forearm injury | FOX Sports
Pats put TE Gronkowski on IR with forearm injury | FOX Sports Reverse radial forearm flap for doxorubicin induced extravasation injuries
Reverse radial forearm flap for doxorubicin induced extravasation injuries Injury Prevention Series: Forearms and Wrists - Albany CrossFit
Injury Prevention Series: Forearms and Wrists - Albany CrossFit A Segmental Fracture of Humerus with Ipsilateral Forearm Fracture: A Rare Variant of Pediatric Floating Elbow Injury
|...
A Segmental Fracture of Humerus with Ipsilateral Forearm Fracture: A Rare Variant of Pediatric Floating Elbow Injury
|... Max Fried on forearm injury, season outlook - Battery Power
Max Fried on forearm injury, season outlook - Battery Power Middle Forearm Fractures - Injuries and Poisoning - MSD Manual Consumer Version
Middle Forearm Fractures - Injuries and Poisoning - MSD Manual Consumer Version Prevent Cycling Injuries In Kids - Children's Health
Prevent Cycling Injuries In Kids - Children's Health Cowboys' injury horror story is no doubt much darker than the Eagles'
Cowboys' injury horror story is no doubt much darker than the Eagles' Hyun Jin Ryu injury MRI Toronto Blue Jays - TSN.ca
Hyun Jin Ryu injury MRI Toronto Blue Jays - TSN.ca Multimodal care for the management of musculoskeletal disorders of the elbow, forearm, wrist and hand: a systematic review by...
Multimodal care for the management of musculoskeletal disorders of the elbow, forearm, wrist and hand: a systematic review by... Adrian Houser, Milwaukee Brewers, SP - News, Stats, Bio - CBSSports.com
Adrian Houser, Milwaukee Brewers, SP - News, Stats, Bio - CBSSports.com What a team, Anushka Sharma lauds team CSK on IPL win
What a team, Anushka Sharma lauds team CSK on IPL win Jacob deGrom injury update: Mets SP placed on 10-day IL with forearm tightness - DraftKings Network
Jacob deGrom injury update: Mets SP placed on 10-day IL with forearm tightness - DraftKings Network 2021 ICD-10-CM Code S55.291: Other specified injury of vein at forearm level, right arm
2021 ICD-10-CM Code S55.291: Other specified injury of vein at forearm level, right arm S54.90XD - Injury of unspecified nerve at forearm level, unspecified arm, subsequent encounter - ICD List 2023
S54.90XD - Injury of unspecified nerve at forearm level, unspecified arm, subsequent encounter - ICD List 2023 Hardware removal - extremity: MedlinePlus Medical Encyclopedia
Hardware removal - extremity: MedlinePlus Medical Encyclopedia Emerging role of physiotherapy in management of crush injury over forearm
| International Journal of Advances in...
Emerging role of physiotherapy in management of crush injury over forearm
| International Journal of Advances in... Forearm Pain When Gripping | livestrong
Forearm Pain When Gripping | livestrong Injury Recovery and Prevention
Injury Recovery and Prevention Braves Injury List Today - October 12
Braves Injury List Today - October 12















![Are Squats Enough For Leg Day? [Answered] | Trainrightmuscle](https://trainrightmuscle.com/wp-content/uploads/2023/06/TRM-Feature-image-4.jpg)






