Germinoma
Pineal Gland
Brain Neoplasms
Dysgerminoma
Basal Ganglia Diseases
Cranial Irradiation
Chorionic Gonadotropin, beta Subunit, Human
Sella Turcica
Neoplasms, Germ Cell and Embryonal
Spinal Cord Neoplasms
Diabetes Insipidus
Diabetes Insipidus, Neurogenic
Giant Cells
Combined Modality Therapy
Pituitary Diseases
Histiocytes
Meningeal Neoplasms
Central Nervous System Neoplasms
Pituitary Neoplasms
Spinal Neoplasms
Femoral Neoplasms
Magnetic Resonance Imaging
Etoposide
Neoplasms, Multiple Primary
Medulla Oblongata
Corpus Callosum
Neoplasm Recurrence, Local
Chorionic Gonadotropin
Radiotherapy, Adjuvant
Trophoblasts
Bcl-2 overexpression results in reciprocal downregulation of Bcl-X(L) and sensitizes human testicular germ cell tumours to chemotherapy-induced apoptosis. (1/400)
Testicular germ cell tumours are hypersentive to chemotherapy and cell lines derived from these tumours are chemosensitive in vitro. We have previously shown that these cell lines express undetectable levels of the suppressor of apoptosis Bcl-2 and relatively high levels of the apoptosis inducer Bax (Chresta et al., 1996). To determine whether the absence of Bcl-2 in these cell lines makes them highly susceptible to drug-induced apoptosis, Bcl-2 was expressed ectopically in the 833K testicular germ cell tumour cell line. Stable overexpressing clones were isolated and three clones were studied further. Surprisingly, Bcl-2 overexpressing cells were sensitized to chemotherapy-induced apoptosis compared to the parental and vector control cells. Analysis of potential mechanisms of sensitization revealed there was a reciprocal downregulation of the endogenously expressed Bcl-X(L) in the Bcl-2 overexpressing clones. Downregulation of Bcl-X(L) to the same extent using antisense oligonucleotides enhanced etoposide-induced apoptosis by twofold. Our results indicate that Bcl-2 and Bcl-X(L) have different abilities to protect against chemotherapy-induced apoptosis in testicular germ cell tumours. In contrast to findings in some tumour cell types, Bcl-2 did not act as a gatekeeper to prevent entry of p53 to the nucleus. (+info)Phase II trial of primary chemotherapy followed by reduced-dose radiation for CNS germ cell tumors. (2/400)
PURPOSE: A prospective phase II study was initiated to assess the response rate, survival, and late effects of treatment in patients with newly diagnosed CNS germ cell tumors (GCT), using etoposide plus cisplatin followed by radiation therapy prescribed by extent of disease, histology, and response to chemotherapy. PATIENTS AND METHODS: Seventeen patients aged 8 to 24 years with histologically proven CNS GCT received etoposide (100 mg/m2/d) plus cisplatin (20 mg/m2/d) daily for 5 days every 3 weeks for four cycles, followed by radiation therapy. Nine patients had germinomas; eight had mixed GCT. Four patients (three with germinomas and one with mixed GCT) presented with leptomeningeal dissemination. RESULTS: Radiographically, 14 of 17 patients were assessable for response; 11 patients experienced complete regression, and three had major partial regression before radiation. Six of seven assessable patients with elevated CSF levels of alpha-fetoprotein or betahuman chorionic gonadotropin had normalization with chemotherapy alone; all normalized with combined chemotherapy and radiation therapy. All 17 patients are alive without evidence of disease (median follow-up, 51 months). One patient developed a relapse in the spinal leptomeninges and was rendered free of disease with spinal radiation more than 5 years ago. One patient developed carotid stenosis requiring surgery. Thus far, only minimal long-term deterioration in neurocognitive function has been detected as a consequence of protocol treatment. CONCLUSION: Conventional-dose intravenous chemotherapy with etoposide and cisplatin can effect tumor regression in a high proportion of patients with CNS GCT, including those with leptomeningeal metastases. Acute and long-term toxicities are acceptable. Progression-free survival and overall survival are excellent. (+info)Defective repair of cisplatin-induced DNA damage caused by reduced XPA protein in testicular germ cell tumours. (3/400)
Metastatic cancer in adults usually has a fatal outcome. In contrast, advanced testicular germ cell tumours are cured in over 80% of patients using cisplatin-based combination chemotherapy [1]. An understanding of why these cells are sensitive to chemotherapeutic drugs is likely to have implications for the treatment of other types of cancer. Earlier measurements indicate that testis tumour cells are hypersensitive to cisplatin and have a low capacity to remove cisplatin-induced DNA damage from the genome [2] [3]. We have investigated the nucleotide excision repair (NER) capacity of extracts from the well-defined 833K and GCT27 human testis tumour cell lines. Both had a reduced ability to carry out the incision steps of NER in comparison with extracts from known repair-proficient cells. Immunoblotting revealed that the testis tumour cells had normal amounts of most NER proteins, but low levels of the xeroderma pigmentosum group A protein (XPA) and the ERCC1-XPF endonuclease complex. Addition of XPA specifically conferred full NER capacity on the testis tumour extracts. These results show that a low XPA level in the testis tumour cell lines is sufficient to explain their poor ability to remove cisplatin adducts from DNA and might be a major reason for the high cisplatin sensitivity of testis tumours. Targeted inhibition of XPA could sensitise other types of cells and tumours to cisplatin and broaden the usefulness of this chemotherapeutic agent. (+info)Ki-A10, a germ cell nuclear antigen retained in a subset of germ cell-derived tumors. (4/400)
Monoclonal antibody Ki-A10 recognizes a nuclear antigen of 25 and 22 kd apparent molecular mass, which is abundantly expressed by immature gonocytes, spermatogonia, and spermatocytes, whereas it is absent in spermatids, spermatozoa, oocytes, and normal somatic tissues. In a broad spectrum of human cancers the antibody showed no reactivity except for a small subset of malignant lymphomas. Because of this restricted expression pattern, we examined 173 germ cell tumors and 18 sex cord stromal tumors immunohistochemically to assess the distribution of the Ki-A10 antigen. A strongly positive reaction was found in classic seminomas, dysgerminomas, spermatocytic seminomas, and the germ cell component of gonadoblastomas. Yolk sac tumors presented a heterogeneous reactivity pattern ranging from overall positivity to complete lack of antigen expression, and in three of eight choriocarcinomas, a few clusters of cytotrophoblast cells were strongly labeled. All other tumors, including Leydig and Sertoli cell tumors as well as placental tissue, were negative. Our findings suggest that specific germ cell antigens can be retained in germ cell tumors along particular differentiation pathways. Ki-A10 is the first marker that consistently labels spermatocytic seminoma, further confirming its germ cell origin and suggesting a close relationship to classic seminoma. The antibody may serve for diagnostic purposes and promises new insights into the process of germ cell differentiation and the development of germ cell-derived neoplasia. (+info)Phase II trial of gemcitabine in refractory germ cell tumors. (5/400)
PURPOSE: This phase II study was designed to determine the toxicity and activity of single-agent gemcitabine in heavily pretreated patients with germ cell tumors. PATIENTS AND METHODS: From March 1996 through November 1997, 21 patients were enrolled onto a phase II study of gemcitabine 1,200 mg/m2, given on days 1, 8, and 15 every 4 weeks. One patient was unassessable because he never received any gemcitabine. Thirteen of 20 patients had received three prior regimens, and 13 patients were platinum refractory (progression during or within 4 weeks of platinum treatment). There were five extragonadal cases and two patients with late relapse (relapse beyond 2 years). RESULTS: Gemcitabine was well tolerated. Only one patient had grade 3 or 4 nonhematologic toxicity (grade 3 nausea). Six of 20 patients had grade 3 leukopenia. There were no episodes of granulocytopenic fever, and no patient required platelet transfusion. Three (15%) of 20 patients achieved an objective response, including one complete remission. Three additional patients had a minor radiographic or serologic response. CONCLUSION: Gemcitabine had definite activity in this heavily pretreated germ cell tumor patient population. (+info)Gemcitabine in patients with relapsed or cisplatin-refractory testicular cancer. (6/400)
PURPOSE: Despite generally high cure rates in patients with metastatic testicular germ cell tumors, patients with incomplete response to cisplatin-based first-line therapy or with relapsed disease after high-dose salvage chemotherapy have a very poor prognosis. This phase II study evaluates the use of gemcitabine in patients with intensively pretreated or cisplatin-refractory testicular germ cell cancers. PATIENTS AND METHODS: Thirty-five patients (median age, 33 years) were enrolled; 31 patients were fully assessable. All patients had metastatic nonseminomatous germ cell tumors; eight patients had extragonadal primary tumors. Twenty patients (63%) had lung metastases, and 12 patients (39%) had liver metastases. The median number of prior cisplatin-based chemotherapy cycles was seven; 22 patients (71%) had received high-dose chemotherapy with autologous stem-cell transplantation, and 19 patients (61%) had received treatment with paclitaxel. Seventeen patients (54%) were considered refractory or absolutely refractory to chemotherapy. RESULTS: Six of 31 assessable patients (19%) responded favorably to gemcitabine, 11 patients (35%) displayed no change, and 14 patients (45%) had disease progression. The median time to treatment failure was 4 months (range, 2 to 9+ months), and the median survival was 6 months (range, 2 to 23 months). Patients received a median of six gemcitabine applications. Ten patients (32%) required dose reductions, mainly owing to hematologic toxicity. Grade 3/4 granulocytopenia occurred in four patients (13%) and grade 3/4 thrombocytopenia in seven patients (22%). One case of severe sepsis was observed. CONCLUSION: Gemcitabine displays antitumor activity in intensively pretreated and refractory germ cell tumors. Responses were observed in approximately 20% of patients, including three of 22 patients after previous high-dose chemotherapy and one of four patients with mediastinal tumors. Gemcitabine may be a reasonable palliative option for intensively pretreated patients and should be further investigated to define its role in the risk-adapted treatment strategies for germ cell tumors. (+info)Combined treatment modality for intracranial germinomas: results of a multicentre SFOP experience. Societe Francaise d'Oncologie Pediatrique. (7/400)
Conventional therapy for intracranial germinomas is craniospinal irradiation. In 1990, the Societe Francaise d'Oncologie Pediatrique initiated a study combining chemotherapy (alternating courses of etoposide-carboplatin and etoposide-ifosfamide for a recommended total of four courses) with 40 Gy local irradiation for patients with localized germinomas. Metastatic patients were allocated to receive low-dose craniospinal radiotherapy. Fifty-seven patients were enrolled between 1990 and 1996. Forty-seven had biopsy-proven germinoma. Biopsy was not performed in ten patients (four had diagnostic tumour markers and in six the neurosurgeon felt biopsy was contraindicated). Fifty-one patients had localized disease, and six leptomeningeal dissemination. Seven patients had bifocal tumour. All but one patient received at least four courses of chemotherapy. Toxicity was mainly haematological. Patients with diabetus insipidus (n = 25) commonly developed electrolyte disturbances during chemotherapy. No patient developed tumour progression during chemotherapy. Fifty patients received local radiotherapy with a median dose of 40 Gy to the initial tumour volume. Six metastatic patients, and one patient with localized disease who stopped chemotherapy due to severe toxicity, received craniospinal radiotherapy. The median follow-up for the group was 42 months. Four patients relapsed 9, 10, 38 and 57 months after diagnosis. Three achieved second complete remission following salvage treatment with chemotherapy alone or chemo-radiotherapy. The estimated 3-year survival probability is 98% (CI: 86.6-99.7%) and the estimated 3-year event-free survival is 96.4% (CI: 86.2-99.1%). This study shows that excellent survival rates can be achieved by combining chemotherapy and local radiotherapy in patients with non-metastatic intracranial germinomas. (+info)Human chorionic gonadotrophin in CSF, not serum, predicts outcome in germinoma. (8/400)
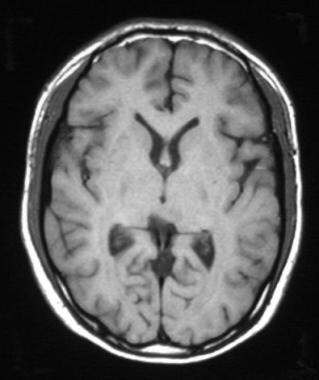
OBJECTIVES: Some intracranial germinomas, which may contain syncytiotrophoblastic giant cells (STGCs), are associated with a mildly to moderately increased human chorionic gonadotropin (HCG) concentration in serum, and patients with such germinomas are thus treated more aggressively than those with "pure" germinoma. However, the patients with germinoma and detectable HCG in CSF but not in serum have been classified and treated similarly to those with "pure" germinomas. The outcome of these patients and the relevance of HCG in the CSF were analysed. METHODS: The outcomes of patients with germinoma and increased serum HCG concentration (n=7) were compared with those of patients having detectable HCG titre in the CSF but not in the serum (n=5). RESULTS: Both groups in our series received similar treatments and also showed similar recurrence rates. The 40% recurrence rate in the group with HCG only in CSF did not correspond to the rate typical for "pure" germinoma: these tumours would be expected to have a better outcome. An additional patient whose CSF HCG were raised without increased serum HCG at recurrence is presented. CONCLUSIONS: It is recommended that patients with an increased HCG concentration in CSF should be considered to have "HCG producing germinoma", and they should be treated and followed up accordingly. (+info)A germinoma is a type of tumor that develops in the brain or the spine, primarily in the pituitary gland or pineal gland. It is a rare form of primary central nervous system (CNS) cancer and is classified as a type of germ cell tumor. These tumors arise from cells that normally develop into sperm or eggs, which can migrate to unusual locations during embryonic development.
Germinomas are highly sensitive to radiation therapy and chemotherapy, making them generally treatable and curable with appropriate medical intervention. Symptoms of a germinoma may include headaches, nausea, vomiting, visual disturbances, hormonal imbalances, and neurological deficits, depending on the location and size of the tumor. Diagnosis typically involves imaging studies like MRI or CT scans, followed by a biopsy to confirm the presence of malignant cells.
The pineal gland, also known as the epiphysis cerebri, is a small endocrine gland located in the brain. It is shaped like a pinecone, hence its name, and is situated near the center of the brain, between the two hemispheres, attached to the third ventricle. The primary function of the pineal gland is to produce melatonin, a hormone that helps regulate sleep-wake cycles and circadian rhythms in response to light and darkness. Additionally, it plays a role in the onset of puberty and has been suggested to have other functions related to cognition, mood, and reproduction, although these are not as well understood.
Brain neoplasms, also known as brain tumors, are abnormal growths of cells within the brain. These growths can be benign (non-cancerous) or malignant (cancerous). Benign brain tumors typically grow slowly and do not spread to other parts of the body. However, they can still cause serious problems if they press on sensitive areas of the brain. Malignant brain tumors, on the other hand, are cancerous and can grow quickly, invading surrounding brain tissue and spreading to other parts of the brain or spinal cord.
Brain neoplasms can arise from various types of cells within the brain, including glial cells (which provide support and insulation for nerve cells), neurons (nerve cells that transmit signals in the brain), and meninges (the membranes that cover the brain and spinal cord). They can also result from the spread of cancer cells from other parts of the body, known as metastatic brain tumors.
Symptoms of brain neoplasms may vary depending on their size, location, and growth rate. Common symptoms include headaches, seizures, weakness or paralysis in the limbs, difficulty with balance and coordination, changes in speech or vision, confusion, memory loss, and changes in behavior or personality.
Treatment for brain neoplasms depends on several factors, including the type, size, location, and grade of the tumor, as well as the patient's age and overall health. Treatment options may include surgery, radiation therapy, chemotherapy, targeted therapy, or a combination of these approaches. Regular follow-up care is essential to monitor for recurrence and manage any long-term effects of treatment.
Dysgerminoma is a type of germ cell tumor that develops in the ovaries. It is a malignant (cancerous) tumor that primarily affects girls and women of reproductive age, although it can occur at any age. Dysgerminomas are composed of large, round, or polygonal cells with clear cytoplasm and distinct cell borders, arranged in nests or sheets. They may also contain lymphoid aggregates and may produce hormones such as estrogen or testosterone.
Dysgerminomas are usually unilateral (affecting one ovary), but they can be bilateral (affecting both ovaries) in about 10-15% of cases. They tend to grow and spread rapidly, so early detection and treatment are crucial for a favorable prognosis.
The standard treatment for dysgerminoma is surgical removal of the affected ovary or ovaries, followed by chemotherapy with agents such as bleomycin, etoposide, and cisplatin (BEP). With appropriate treatment, the five-year survival rate for patients with dysgerminoma is high, ranging from 80% to 95%.
Basal ganglia diseases are a group of neurological disorders that affect the function of the basal ganglia, which are clusters of nerve cells located deep within the brain. The basal ganglia play a crucial role in controlling movement and coordination. When they are damaged or degenerate, it can result in various motor symptoms such as tremors, rigidity, bradykinesia (slowness of movement), and difficulty with balance and walking.
Some examples of basal ganglia diseases include:
1. Parkinson's disease - a progressive disorder that affects movement due to the death of dopamine-producing cells in the basal ganglia.
2. Huntington's disease - an inherited neurodegenerative disorder that causes uncontrolled movements, emotional problems, and cognitive decline.
3. Dystonia - a movement disorder characterized by sustained or intermittent muscle contractions that cause twisting and repetitive movements or abnormal postures.
4. Wilson's disease - a rare genetic disorder that causes excessive copper accumulation in the liver and brain, leading to neurological and psychiatric symptoms.
5. Progressive supranuclear palsy (PSP) - a rare brain disorder that affects movement, gait, and balance, as well as speech and swallowing.
6. Corticobasal degeneration (CBD) - a rare neurological disorder characterized by progressive loss of nerve cells in the cerebral cortex and basal ganglia, leading to stiffness, rigidity, and difficulty with movement and coordination.
Treatment for basal ganglia diseases varies depending on the specific diagnosis and symptoms but may include medication, surgery, physical therapy, or a combination of these approaches.
Cranial irradiation is a medical treatment that involves the use of radiation therapy to target the brain. It is often used to treat various conditions affecting the brain, such as brain tumors, leukemia, and certain neurological disorders. The radiation is directed at the skull and can be focused on specific areas of the brain or delivered more broadly, depending on the nature and location of the condition being treated.
The goal of cranial irradiation may be to destroy cancer cells, reduce the size of tumors, prevent the spread of cancer, or provide symptomatic relief for patients with advanced disease. However, it is important to note that cranial irradiation can have side effects, including hair loss, fatigue, memory problems, and cognitive changes, among others. These side effects can vary in severity and duration depending on the individual patient and the specific treatment regimen.
Chorionic Gonadotropin, beta Subunit, Human (β-hCG) is a protein that is produced by the placenta during pregnancy. It is a component of human chorionic gonadotropin (hCG), which is a hormone that is composed of two subunits: alpha and beta. The β-hCG subunit is specific to hCG and is not found in other hormones, making it a useful marker for pregnancy and certain medical conditions.
During early pregnancy, the levels of β-hCG increase rapidly and can be detected in the blood and urine. This has led to the development of pregnancy tests that detect the presence of β-hCG to confirm pregnancy. In addition to its role in pregnancy, β-hCG is also used as a tumor marker for certain types of cancer, such as germ cell tumors and choriocarcinoma.
Elevated levels of β-hCG may indicate the presence of a molar pregnancy, a condition in which a fertilized egg implants in the uterus but does not develop properly. In some cases, a molar pregnancy can become cancerous and require treatment. Therefore, monitoring β-hCG levels during pregnancy is important for detecting any potential complications.
The Sella Turcica, also known as the Turkish saddle, is a depression or fossa in the sphenoid bone located at the base of the skull. It forms a housing for the pituitary gland, which is a small endocrine gland often referred to as the "master gland" because it controls other glands and makes several essential hormones. The Sella Turcica has a saddle-like shape, with its anterior and posterior clinoids forming the front and back of the saddle, respectively. This region is of significant interest in neuroimaging and clinical settings, as various conditions such as pituitary tumors or other abnormalities may affect the size, shape, and integrity of the Sella Turcica.
Neoplasms, germ cell and embryonal are types of tumors that originate from the abnormal growth of cells. Here's a brief medical definition for each:
1. Neoplasms: Neoplasms refer to abnormal tissue growths or masses, which can be benign (non-cancerous) or malignant (cancerous). They result from uncontrolled cell division and may invade surrounding tissues or spread to other parts of the body through a process called metastasis.
2. Germ Cell Tumors: These are rare tumors that develop from the germ cells, which give rise to sperm and eggs in the reproductive organs (ovaries and testes). They can be benign or malignant and may occur in both children and adults. Germ cell tumors can also arise outside of the reproductive organs, a condition known as extragonadal germ cell tumors.
3. Embryonal Tumors: These are a type of malignant neoplasm that primarily affects infants and young children. They develop from embryonic cells, which are immature cells present during fetal development. Embryonal tumors can occur in various organs, including the brain (medulloblastomas), nervous system (primitive neuroectodermal tumors or PNETs), and other areas like the kidneys and liver.
It is essential to note that these conditions require professional medical evaluation and treatment by healthcare professionals with expertise in oncology and related fields.
Spinal cord neoplasms refer to abnormal growths or tumors within the spinal cord. These can be benign (non-cancerous) or malignant (cancerous). They originate from the cells within the spinal cord itself (primary tumors), or they may spread to the spinal cord from other parts of the body (metastatic tumors). Spinal cord neoplasms can cause various symptoms depending on their location and size, including back pain, neurological deficits, and even paralysis. Treatment options include surgery, radiation therapy, and chemotherapy.
Diabetes Insipidus is a medical condition characterized by the excretion of large amounts of dilute urine (polyuria) and increased thirst (polydipsia). It is caused by a deficiency in the hormone vasopressin (also known as antidiuretic hormone or ADH), which regulates the body's water balance.
In normal physiology, vasopressin is released from the posterior pituitary gland in response to an increase in osmolality of the blood or a decrease in blood volume. This causes the kidneys to retain water and concentrate the urine. In Diabetes Insipidus, there is either a lack of vasopressin production (central diabetes insipidus) or a decreased response to vasopressin by the kidneys (nephrogenic diabetes insipidus).
Central Diabetes Insipidus can be caused by damage to the hypothalamus or pituitary gland, such as from tumors, trauma, or surgery. Nephrogenic Diabetes Insipidus can be caused by genetic factors, kidney disease, or certain medications that interfere with the action of vasopressin on the kidneys.
Treatment for Diabetes Insipidus depends on the underlying cause. In central diabetes insipidus, desmopressin, a synthetic analogue of vasopressin, can be administered to replace the missing hormone. In nephrogenic diabetes insipidus, treatment may involve addressing the underlying kidney disease or adjusting medications that interfere with vasopressin action. It is important for individuals with Diabetes Insipidus to maintain adequate hydration and monitor their fluid intake and urine output.
Neurogenic diabetes insipidus is a condition characterized by the production of large amounts of dilute urine (polyuria) and increased thirst (polydipsia) due to deficiency of antidiuretic hormone (ADH), also known as vasopressin, which is produced by the hypothalamus and stored in the posterior pituitary gland.
Neurogenic diabetes insipidus can occur when there is damage to the hypothalamus or pituitary gland, leading to a decrease in ADH production or release. Causes of neurogenic diabetes insipidus include brain tumors, head trauma, surgery, meningitis, encephalitis, and autoimmune disorders.
In this condition, the kidneys are unable to reabsorb water from the urine due to the lack of ADH, resulting in the production of large volumes of dilute urine. This can lead to dehydration, electrolyte imbalances, and other complications if not properly managed. Treatment typically involves replacing the missing ADH with a synthetic hormone called desmopressin, which can be administered as a nasal spray, oral tablet, or injection.
Giant cells are large, multinucleated cells that result from the fusion of monocytes or macrophages. They can be found in various types of inflammatory and degenerative lesions, including granulomas, which are a hallmark of certain diseases such as tuberculosis and sarcoidosis. There are several types of giant cells, including:
1. Langhans giant cells: These have a horseshoe-shaped or crescentic arrangement of nuclei around the periphery of the cell. They are typically found in granulomas associated with infectious diseases such as tuberculosis and histoplasmosis.
2. Foreign body giant cells: These form in response to the presence of foreign material, such as a splinter or suture, in tissue. The nuclei are usually scattered throughout the cell cytoplasm.
3. Touton giant cells: These are found in certain inflammatory conditions, such as xanthomatosis and granulomatous slack skin. They have a central core of lipid-laden histiocytes surrounded by a ring of nuclei.
4. Osteoclast giant cells: These are multinucleated cells responsible for bone resorption. They can be found in conditions such as giant cell tumors of bone and Paget's disease.
It is important to note that the presence of giant cells alone does not necessarily indicate a specific diagnosis, and their significance must be interpreted within the context of the overall clinical and pathological findings.
Pituitary function tests are a group of diagnostic exams that evaluate the proper functioning of the pituitary gland, a small endocrine gland located at the base of the brain. The pituitary gland is responsible for producing and releasing several essential hormones that regulate various bodily functions, including growth, metabolism, stress response, reproduction, and lactation.
These tests typically involve measuring the levels of different hormones in the blood, stimulating or suppressing the pituitary gland with specific medications, and assessing the body's response to these challenges. Some common pituitary function tests include:
1. Growth hormone (GH) testing: Measures GH levels in the blood, often after a provocative test using substances like insulin, arginine, clonidine, or glucagon to stimulate GH release.
2. Thyroid-stimulating hormone (TSH) and free thyroxine (FT4) testing: Assesses the function of the thyroid gland by measuring TSH and FT4 levels in response to TRH (thyrotropin-releasing hormone) stimulation.
3. Adrenocorticotropic hormone (ACTH) and cortisol testing: Evaluates the hypothalamic-pituitary-adrenal axis by measuring ACTH and cortisol levels after a CRH (corticotropin-releasing hormone) stimulation test or an insulin tolerance test.
4. Prolactin (PRL) testing: Measures PRL levels in the blood, which can be elevated due to pituitary tumors or other conditions affecting the hypothalamus.
5. Follicle-stimulating hormone (FSH) and luteinizing hormone (LH) testing: Assesses reproductive function by measuring FSH and LH levels, often in conjunction with estradiol or testosterone levels.
6. Gonadotropin-releasing hormone (GnRH) stimulation test: Evaluates gonadal function by measuring FSH and LH levels after GnRH administration.
7. Growth hormone (GH) testing: Measures GH levels in response to various stimuli, such as insulin-like growth factor-1 (IGF-1), glucagon, or arginine.
8. Vasopressin (ADH) testing: Assesses the posterior pituitary function by measuring ADH levels and performing a water deprivation test.
These tests can help diagnose various pituitary disorders, such as hypopituitarism, hyperpituitarism, or pituitary tumors, and guide appropriate treatment strategies.
Combined modality therapy (CMT) is a medical treatment approach that utilizes more than one method or type of therapy simultaneously or in close succession, with the goal of enhancing the overall effectiveness of the treatment. In the context of cancer care, CMT often refers to the combination of two or more primary treatment modalities, such as surgery, radiation therapy, and systemic therapies (chemotherapy, immunotherapy, targeted therapy, etc.).
The rationale behind using combined modality therapy is that each treatment method can target cancer cells in different ways, potentially increasing the likelihood of eliminating all cancer cells and reducing the risk of recurrence. The specific combination and sequence of treatments will depend on various factors, including the type and stage of cancer, patient's overall health, and individual preferences.
For example, a common CMT approach for locally advanced rectal cancer may involve preoperative (neoadjuvant) chemoradiation therapy, followed by surgery to remove the tumor, and then postoperative (adjuvant) chemotherapy. This combined approach allows for the reduction of the tumor size before surgery, increases the likelihood of complete tumor removal, and targets any remaining microscopic cancer cells with systemic chemotherapy.
It is essential to consult with a multidisciplinary team of healthcare professionals to determine the most appropriate CMT plan for each individual patient, considering both the potential benefits and risks associated with each treatment method.
Pituitary diseases refer to a group of conditions that affect the pituitary gland, a small endocrine gland located at the base of the brain. The pituitary gland is responsible for producing and secreting several important hormones that regulate various bodily functions, including growth and development, metabolism, stress response, and reproduction.
Pituitary diseases can be classified into two main categories:
1. Pituitary tumors: These are abnormal growths in or around the pituitary gland that can affect its function. Pituitary tumors can be benign (non-cancerous) or malignant (cancerous), and they can vary in size. Some pituitary tumors produce excess hormones, leading to a variety of symptoms, while others may not produce any hormones but can still cause problems by compressing nearby structures in the brain.
2. Pituitary gland dysfunction: This refers to conditions that affect the normal function of the pituitary gland without the presence of a tumor. Examples include hypopituitarism, which is a condition characterized by decreased production of one or more pituitary hormones, and Sheehan's syndrome, which occurs when the pituitary gland is damaged due to severe blood loss during childbirth.
Symptoms of pituitary diseases can vary widely depending on the specific condition and the hormones that are affected. Treatment options may include surgery, radiation therapy, medication, or a combination of these approaches.
Histiocytes are a type of immune cell that are part of the mononuclear phagocyte system. They originate from monocytes, which are derived from hematopoietic stem cells in the bone marrow. Histiocytes play an important role in the immune system by engulfing and destroying foreign substances, such as bacteria and viruses, as well as removing dead cells and other debris from the body. They can be found in various tissues throughout the body, including the skin, lymph nodes, spleen, and liver.
Histiocytes include several different types of cells, such as macrophages, dendritic cells, and Langerhans cells. These cells have different functions but all play a role in the immune response. For example, macrophages are involved in inflammation and tissue repair, while dendritic cells are important for presenting antigens to T cells and initiating an immune response.
Abnormal accumulations or dysfunction of histiocytes can lead to various diseases, such as histiocytosis, which is a group of disorders characterized by the abnormal proliferation and accumulation of histiocytes in various tissues.
Meningeal neoplasms, also known as malignant meningitis or leptomeningeal carcinomatosis, refer to cancerous tumors that originate in the meninges, which are the membranes covering the brain and spinal cord. These tumors can arise primarily from the meningeal cells themselves, although they more commonly result from the spread (metastasis) of cancer cells from other parts of the body, such as breast, lung, or melanoma.
Meningeal neoplasms can cause a variety of symptoms, including headaches, nausea and vomiting, mental status changes, seizures, and focal neurological deficits. Diagnosis typically involves imaging studies (such as MRI) and analysis of cerebrospinal fluid obtained through a spinal tap. Treatment options may include radiation therapy, chemotherapy, or surgery, depending on the type and extent of the tumor. The prognosis for patients with meningeal neoplasms is generally poor, with a median survival time of several months to a year.
Central nervous system (CNS) neoplasms refer to a group of abnormal growths or tumors that develop within the brain or spinal cord. These tumors can be benign or malignant, and their growth can compress or disrupt the normal functioning of surrounding brain or spinal cord tissue.
Benign CNS neoplasms are slow-growing and rarely spread to other parts of the body. However, they can still cause significant problems if they grow large enough to put pressure on vital structures within the brain or spinal cord. Malignant CNS neoplasms, on the other hand, are aggressive tumors that can invade and destroy surrounding tissue. They may also spread to other parts of the CNS or, rarely, to other organs in the body.
CNS neoplasms can arise from various types of cells within the brain or spinal cord, including nerve cells, glial cells (which provide support and insulation for nerve cells), and supportive tissues such as blood vessels. The specific type of CNS neoplasm is often used to help guide treatment decisions and determine prognosis.
Symptoms of CNS neoplasms can vary widely depending on the location and size of the tumor, but may include headaches, seizures, weakness or paralysis, vision or hearing changes, balance problems, memory loss, and changes in behavior or personality. Treatment options for CNS neoplasms may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
Pituitary neoplasms refer to abnormal growths or tumors in the pituitary gland, a small endocrine gland located at the base of the brain. These neoplasms can be benign (non-cancerous) or malignant (cancerous), with most being benign. They can vary in size and may cause various symptoms depending on their location, size, and hormonal activity.
Pituitary neoplasms can produce and secrete excess hormones, leading to a variety of endocrine disorders such as Cushing's disease (caused by excessive ACTH production), acromegaly (caused by excessive GH production), or prolactinoma (caused by excessive PRL production). They can also cause local compression symptoms due to their size, leading to headaches, vision problems, and cranial nerve palsies.
The exact causes of pituitary neoplasms are not fully understood, but genetic factors, radiation exposure, and certain inherited conditions may increase the risk of developing these tumors. Treatment options for pituitary neoplasms include surgical removal, radiation therapy, and medical management with drugs that can help control hormonal imbalances.
Spinal neoplasms refer to abnormal growths or tumors found within the spinal column, which can be benign (non-cancerous) or malignant (cancerous). These tumors can originate in the spine itself, called primary spinal neoplasms, or they can spread to the spine from other parts of the body, known as secondary or metastatic spinal neoplasms. Spinal neoplasms can cause various symptoms, such as back pain, neurological deficits, and even paralysis, depending on their location and size. Early diagnosis and treatment are crucial to prevent or minimize long-term complications and improve the patient's prognosis.
Femoral neoplasms refer to abnormal growths or tumors that develop in the femur, which is the long thigh bone in the human body. These neoplasms can be benign (non-cancerous) or malignant (cancerous). Benign femoral neoplasms are slow-growing and rarely spread to other parts of the body, while malignant neoplasms are aggressive and can invade nearby tissues and organs, as well as metastasize (spread) to distant sites.
There are various types of femoral neoplasms, including osteochondromas, enchondromas, chondrosarcomas, osteosarcomas, and Ewing sarcomas, among others. The specific type of neoplasm is determined by the cell type from which it arises and its behavior.
Symptoms of femoral neoplasms may include pain, swelling, stiffness, or weakness in the thigh, as well as a palpable mass or limited mobility. Diagnosis typically involves imaging studies such as X-rays, CT scans, or MRI, as well as biopsy to determine the type and grade of the tumor. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches, depending on the type, size, location, and stage of the neoplasm.
Medical Definition:
Magnetic Resonance Imaging (MRI) is a non-invasive diagnostic imaging technique that uses a strong magnetic field and radio waves to create detailed cross-sectional or three-dimensional images of the internal structures of the body. The patient lies within a large, cylindrical magnet, and the scanner detects changes in the direction of the magnetic field caused by protons in the body. These changes are then converted into detailed images that help medical professionals to diagnose and monitor various medical conditions, such as tumors, injuries, or diseases affecting the brain, spinal cord, heart, blood vessels, joints, and other internal organs. MRI does not use radiation like computed tomography (CT) scans.
Etoposide is a chemotherapy medication used to treat various types of cancer, including lung cancer, testicular cancer, and certain types of leukemia. It works by inhibiting the activity of an enzyme called topoisomerase II, which is involved in DNA replication and transcription. By doing so, etoposide can interfere with the growth and multiplication of cancer cells.
Etoposide is often administered intravenously in a hospital or clinic setting, although it may also be given orally in some cases. The medication can cause a range of side effects, including nausea, vomiting, hair loss, and an increased risk of infection. It can also have more serious side effects, such as bone marrow suppression, which can lead to anemia, bleeding, and a weakened immune system.
Like all chemotherapy drugs, etoposide is not without risks and should only be used under the close supervision of a qualified healthcare provider. It is important for patients to discuss the potential benefits and risks of this medication with their doctor before starting treatment.
Multiple primary neoplasms refer to the occurrence of more than one primary malignant tumor in an individual, where each tumor is unrelated to the other and originates from separate cells or organs. This differs from metastatic cancer, where a single malignancy spreads to multiple sites in the body. Multiple primary neoplasms can be synchronous (occurring at the same time) or metachronous (occurring at different times). The risk of developing multiple primary neoplasms increases with age and is associated with certain genetic predispositions, environmental factors, and lifestyle choices such as smoking and alcohol consumption.
The medulla oblongata is a part of the brainstem that is located in the posterior portion of the brainstem and continues with the spinal cord. It plays a vital role in controlling several critical bodily functions, such as breathing, heart rate, and blood pressure. The medulla oblongata also contains nerve pathways that transmit sensory information from the body to the brain and motor commands from the brain to the muscles. Additionally, it is responsible for reflexes such as vomiting, swallowing, coughing, and sneezing.
The corpus callosum is the largest collection of white matter in the brain, consisting of approximately 200 million nerve fibers. It is a broad, flat band of tissue that connects the two hemispheres of the brain, allowing them to communicate and coordinate information processing. The corpus callosum plays a crucial role in integrating sensory, motor, and cognitive functions between the two sides of the brain. Damage to the corpus callosum can result in various neurological symptoms, including difficulties with movement, speech, memory, and social behavior.
Local neoplasm recurrence is the return or regrowth of a tumor in the same location where it was originally removed or treated. This means that cancer cells have survived the initial treatment and started to grow again in the same area. It's essential to monitor and detect any local recurrence as early as possible, as it can affect the prognosis and may require additional treatment.
Chorionic Gonadotropin (hCG) is a hormone that is produced during pregnancy. It is produced by the placenta after implantation of the fertilized egg in the uterus. The main function of hCG is to prevent the disintegration of the corpus luteum, which is a temporary endocrine structure that forms in the ovary after ovulation and produces progesterone during early pregnancy. Progesterone is essential for maintaining the lining of the uterus and supporting the pregnancy.
hCG can be detected in the blood or urine as early as 10 days after conception, and its levels continue to rise throughout the first trimester of pregnancy. In addition to its role in maintaining pregnancy, hCG is also used as a clinical marker for pregnancy and to monitor certain medical conditions such as gestational trophoblastic diseases.
Adjuvant radiotherapy is a type of cancer treatment that uses radiation therapy as an adjunct to a primary surgical procedure. The goal of adjuvant radiotherapy is to eliminate any remaining microscopic cancer cells that may be present in the surrounding tissues after surgery, thereby reducing the risk of local recurrence and improving the chances of cure.
Radiotherapy involves the use of high-energy radiation to destroy cancer cells and shrink tumors. In adjuvant radiotherapy, the radiation is usually delivered to the tumor bed and regional lymph nodes in order to target any potential sites of residual disease. The timing and dosing of adjuvant radiotherapy may vary depending on the type and stage of cancer being treated, as well as other factors such as patient age and overall health status.
Adjuvant radiotherapy is commonly used in the treatment of various types of cancer, including breast, colorectal, lung, head and neck, and gynecologic cancers. Its use has been shown to improve survival rates and reduce the risk of recurrence in many cases, making it an important component of comprehensive cancer care.
Trophoblasts are specialized cells that make up the outer layer of a blastocyst, which is a hollow ball of cells that forms in the earliest stages of embryonic development. In humans, this process occurs about 5-6 days after fertilization. The blastocyst consists of an inner cell mass (which will eventually become the embryo) and an outer layer of trophoblasts.
Trophoblasts play a crucial role in implantation, which is the process by which the blastocyst attaches to and invades the lining of the uterus. Once implanted, the trophoblasts differentiate into two main layers: the cytotrophoblasts (which are closer to the inner cell mass) and the syncytiotrophoblasts (which form a multinucleated layer that is in direct contact with the maternal tissues).
The cytotrophoblasts proliferate and fuse to form the syncytiotrophoblasts, which have several important functions. They secrete enzymes that help to degrade and remodel the extracellular matrix of the uterine lining, allowing the blastocyst to implant more deeply. They also form a barrier between the maternal and fetal tissues, helping to protect the developing embryo from the mother's immune system.
Additionally, trophoblasts are responsible for the formation of the placenta, which provides nutrients and oxygen to the developing fetus and removes waste products. The syncytiotrophoblasts in particular play a key role in this process by secreting hormones such as human chorionic gonadotropin (hCG), which helps to maintain pregnancy, and by forming blood vessels that allow for the exchange of nutrients and waste between the mother and fetus.
Abnormalities in trophoblast development or function can lead to a variety of pregnancy-related complications, including preeclampsia, intrauterine growth restriction, and gestational trophoblastic diseases such as hydatidiform moles and choriocarcinomas.
 Germinoma - Wikipedia
Germinoma - Wikipedia Central Nervous System Germinoma: Practice Essentials, Pathophysiology, Etiology
Central Nervous System Germinoma: Practice Essentials, Pathophysiology, Etiology GERMINOMA PINEAL - TnRelaciones - La vida misma
GERMINOMA PINEAL - TnRelaciones - La vida misma Germinoma caregiver: Why I wrote an open thank you note to MD Anderson | MD Anderson Cancer Center
Germinoma caregiver: Why I wrote an open thank you note to MD Anderson | MD Anderson Cancer Center Intracranial Germinoma: Successful Management by Chemotherapy and Intensity Modulated Radiation Therapy | Abstract
Intracranial Germinoma: Successful Management by Chemotherapy and Intensity Modulated Radiation Therapy | Abstract Gray Zone-Germination of Germinoma Treatment | ASTRO
Gray Zone-Germination of Germinoma Treatment | ASTRO PDF) The Mandelbrot Set as a Quasi-Black Hole
PDF) The Mandelbrot Set as a Quasi-Black Hole Gary M. Kupfer, MD| Pediatric Hematology Oncology, Pediatric Hematology | MedStar Health
Gary M. Kupfer, MD| Pediatric Hematology Oncology, Pediatric Hematology | MedStar Health Pituitary Tumors and Neuroendocrine Disorders - Brigham and Women's Hospital
Pituitary Tumors and Neuroendocrine Disorders - Brigham and Women's Hospital![BACHMAN DS[au] - Search Results - PubMed](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAMAAAAoLQ9TAAAARVBMVEVHcEwoU45gYmYAUpQAUpRPYGVgYmZLXnJgYmYAUZUAUpRJXnIAUpQAUpRgYmYAUpRgYmZgYmZhYmYAUpQAUpQAUpRgYmaDiPJuAAAAFXRSTlMADOJ+6QewGO8/uTRqtH7GdFJ11p1bCL3TAAAAZUlEQVQYlV2PVw7AIAxDTeney7n/UcsoldX3E+VJOAboEi7MBpHWMs1ADlG8u7UYWauwyZFeRQVPOhG2o+aiwhByJxUx91Jxhje3iJSqGfHuLKI0+0TpXvY1twCOPlFh5pa/++MB0vIOBm+1zaoAAAAASUVORK5CYII=) BACHMAN DS[au] - Search Results - PubMed
BACHMAN DS[au] - Search Results - PubMed Seminoma | Harvard Catalyst Profiles | Harvard Catalyst
Seminoma | Harvard Catalyst Profiles | Harvard Catalyst Testicular Cancer - EPIDEMIOLOGY AETIOLOGY PATHOLOGY - Uroweb
Testicular Cancer - EPIDEMIOLOGY AETIOLOGY PATHOLOGY - Uroweb Germ Cell Tumor Treatment Market Size & Share Analysis By 2030
Germ Cell Tumor Treatment Market Size & Share Analysis By 2030 Pathology Outlines - Atypical teratoid / rhabdoid tumor
Pathology Outlines - Atypical teratoid / rhabdoid tumor A. Lindsay Frazier, MD - Dana-Farber Cancer Institute | Boston, MA
A. Lindsay Frazier, MD - Dana-Farber Cancer Institute | Boston, MA Pediatric Brain Tumor Program | UCSF Benioff Children's Hospitals
Pediatric Brain Tumor Program | UCSF Benioff Children's Hospitals Ovarian teratoma | Radiology Reference Article | Radiopaedia.org
Ovarian teratoma | Radiology Reference Article | Radiopaedia.org Conditions Treated | Brain Tumor Center
Conditions Treated | Brain Tumor Center Student Publications | Investigative Medicine Program
Student Publications | Investigative Medicine Program Portal Regional da BVS
Portal Regional da BVS Congratulations Illyria Volcansek - Brain Tumour Foundation of Canada
Congratulations Illyria Volcansek - Brain Tumour Foundation of Canada Integrated Analysis of Serum Lymphocytes Develops a Nomogram for Predicting Prognosis of Intracranial Germ Cell Tumors to Chemo...
Integrated Analysis of Serum Lymphocytes Develops a Nomogram for Predicting Prognosis of Intracranial Germ Cell Tumors to Chemo...