Ear Auricle
Gingival Hypertrophy
Maxillofacial Abnormalities
Unilateral semicircular canal aplasia in Goldenhar's syndrome. (1/46)
A patient with Goldenhar's syndrome (oculoauriculovertebral dysplasia) and unilateral aplasia of all semicircular canals is presented. This is the first report of such a finding and may support the hypothesis that Goldenhar's syndrome and the CHARGE association have a common pathogenetic mechanism. (+info)Goldenhar's syndrome associated with occipital meningoencephalocele--case report. (2/46)
A male neonate presented with Goldenhar's syndrome (oculoauriculovertebral dysplasia), a combination of facial microsomia and auricular malformation, associated with occipital meningoencephalocele. Three-dimensional computed tomography images clearly showed a suboccipital cranial cleft extending to the foramen magnum and hypogenesis of the left temporal bone. The patient died of heart failure due to ventricular septal defect at age 5 months. (+info)Cervical spine instability in children with Goldenhar's syndrome. (3/46)
OBJECTIVE: To study the vertebral involvement of the cervical spine, in particular the stability of C1-C2, in children with proven Goldenhar's syndrome. DESIGN: A case review. SETTING: The Children's Hospital of Eastern Ontario, Ottawa. PATIENTS: Eight children who had a minimum of 2 out of 3 Goldenhar criteria plus other strong associations with the syndrome and for whom detailed radiographic spinal assessment, including flexion-extension views of the cervical spine and computed tomography of the congenital anomalies, were available. OUTCOME MEASURES: Radiographic findings. RESULTS: Seven children demonstrated cervical spine anomalies. Of particular concern was the high incidence of C1-C2 instability in 3 children, 2 of whom required occiput to C2 fusion. The presence of hemivertebrae and failures of segmentation were most common and resulted in thoracic scoliosis, leading to spinal fusion in 2 children. CONCLUSIONS: In patients with Goldenhar's syndrome the cervical spines must be monitored carefully for C1-C2 subluxation before any proposed surgery for other malformations associated with the syndrome, so that any instability can be identified to avoid cord impingement during a general anesthetic. (+info)Goldenhar's syndrome--case report. (4/46)
Goldenhar's syndrome is a rare condition described initially in the early 1950's. It is characterized by a combination of anomalies: dermal epibulbar cysts, auricular appendices and malformation of the ears. In 1963, Gorlin suggested the name oculo-auriculo-vertebral (OAV) dysplasia for this condition and also included vertebral anomalies as signs of the syndrome. The etiology of this rare disease is not fully understood, as it has shown itself variable genetically and of unclear causes. This work reports a case of Goldenhar's syndrome in an 11-year-old female, who presented all classical signs of this rare condition (+info)Ocular motility disturbances (Duane retraction syndrome and double elevator palsy) with congenital heart disease, a rare association with Goldenhar syndrome--a case report. (5/46)
This report is a case of a 4 year old male child who was admitted for meningitis. On clinical examination he was diagnosed as a case of oculo-suriculo-vertebral dysplasia with congenital heart disease, i.e., tetralogy of Fallots besides his presenting picture of meningitis. During his ophthalmic checkup for the conspicuous presence of epibulbar dermoid, he was discovered to have upper lid coloboma, double elevator palsy, and Grade 1 Duane retraction syndrome in his right eye while the pathognomic feature, a dermolipoma, was present in the left eye. The oculo-auriculo-vertebral dysplasia, as described by Goldenhar, is a disease complex of structures developed from the Ist and IInd branchial arch. The important feature of this case is the bilateral involvement of the disease complex over and above the presence of ocular motility disorders--Duane retraction syndrome and double elevator palsy. (+info)Goldenhar's Syndrome (oculo-auriculo-vertebral dysplasia) with congenital facial nerve palsy. (6/46)
Goldenhar's Syndrome (oculo-auriculo-vertebral dysplasia) is a wide spectrum of congenital anomalies that involves structures arising from the first and second branchial arches. In this report, a case of a male infant, with the features of hemi facial microsomia, anotia, vertebral anomalies, congenital facial nerve palsy and lagophthalmos is described. Although the syndrome itself is not uncommon, the presence of congenital facial nerve palsy, which has been reported in rare cases, prompted this case report. (+info)Prenatal diagnosis of hemifacial microsomia and ipsilateral cerebellar hypoplasia in a fetus with oculoauriculovertebral spectrum. (7/46)
Oculoauriculovertebral spectrum, or Goldenhar syndrome, is characterized by varying degrees of prevalently unilateral underdevelopment of craniofacial structures (orbit, ear, mandible) and spinal anomalies. We report the prenatal ultrasonographic diagnosis made at 24 weeks' gestation in a family with a negative history. The prenatal diagnosis was suspected due to the presence of marked hemifacial microsomia and moderate ipsilateral cerebellar hemisphere hypoplasia in the absence of facial clefting. (+info)Autism with ophthalmologic malformations: the plot thickens. (8/46)
PURPOSE: To review the association of autism spectrum disorder (ASD) in individuals manifesting thalidomide embryopathy and Mobius sequence and compare them with three new studies in which ASD was also associated with ocular and systemic malformations: (1) a Swedish study of individuals with CHARGE association (Coloboma, Heart, choanal Atresia, developmental or growth Retardation, Genital anomaly, and Ear involvement); (2) a Swedish study of Goldenhar syndrome; and (3) Brazilian Mobius syndrome (sequence) study. METHODS: In the Swedish CHARGE study, 31 patients met the inclusion criteria (3+ or 4 of the common characteristics of the CHARGE syndrome). The same team of investigators also evaluated 20 Swedish patients with Goldenhar syndrome. In the Brazilian Mobius study, 28 children with a diagnosis of Mobius sequence were studied; some children had a history of exposure during their mother's pregnancy to the abortifacient drug misoprostol in an unsuccessful abortion attempt. RESULTS: In the CHARGE study, five patients had the more severe autism disorder and five had autistic-like condition. In the Goldenhar study, two had autism disorder and one had autistic-like condition. In the Brazilian Mobius study, the systemic findings of the misoprostol-exposed and misoprostol-unexposed patients were almost undistinguishable, and ASD was present in both groups (autism disorder in five and autistic-like condition in three). CONCLUSION: Autism spectrum disorder has been reported in two conditions with known early pregnancy exposure to the teratogenic agents thalidomide and misoprostol. In the Brazilian Mobius study, autism also occurred in both the misoprostol-exposed and misoprostol-unexposed groups. Autism also was present in patients with both CHARGE association and Goldenhar syndrome. (+info)Goldenhar Syndrome, also known as Oculoauriculovertebral Spectrum (OAVS), is a rare congenital condition characterized by a combination of abnormalities affecting the development of the eyes, ears, jaw, and spine. The specific features of this syndrome can vary significantly from one individual to another, but they often include underdevelopment or absence of one ear (microtia) or both ears (anotia), benign growths or cysts in the ear (preauricular tags or sinuses), abnormalities in the formation of the jaw (hemifacial microsomia), and a variety of eye problems such as small eyes (microphthalmia) or anophthalmia (absence of one or both eyes). In addition, some individuals with Goldenhar Syndrome may have vertebral abnormalities, including scoliosis or spina bifida.
The exact cause of Goldenhar Syndrome is not fully understood, but it is believed to be related to disturbances in the development of the first and second branchial arches during embryonic development. These structures give rise to the facial bones, muscles, ears, and nerves. In some cases, genetic factors may play a role, but most cases appear to occur spontaneously, without a clear family history.
Treatment for Goldenhar Syndrome typically involves a multidisciplinary approach, with input from specialists such as plastic surgeons, ophthalmologists, audiologists, and orthodontists. Treatment may include reconstructive surgery to address facial asymmetry or ear abnormalities, hearing aids or other devices to improve hearing, and corrective lenses or surgery to address eye problems. Regular monitoring and follow-up care are also important to ensure optimal outcomes and to address any new issues that may arise over time.
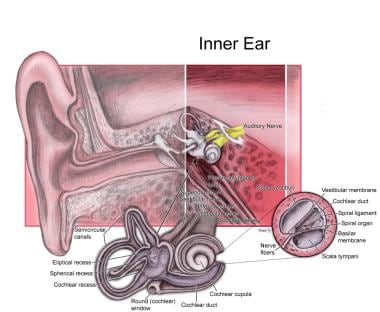
The ear auricle, also known as the pinna or outer ear, is the visible external structure of the ear that serves to collect and direct sound waves into the ear canal. It is composed of cartilage and skin and is shaped like a curved funnel. The ear auricle consists of several parts including the helix (the outer rim), antihelix (the inner curved prominence), tragus and antitragus (the small pointed eminences in front of and behind the ear canal opening), concha (the bowl-shaped area that directs sound into the ear canal), and lobule (the fleshy lower part hanging from the ear).
Facial asymmetry refers to a condition in which the facial features are not identical or proportionate on both sides of a vertical line drawn down the middle of the face. This can include differences in the size, shape, or positioning of facial features such as the eyes, ears, nose, cheeks, and jaw. Facial asymmetry can be mild and barely noticeable, or it can be more severe and affect a person's appearance and/or functionality of the mouth and jaw.
Facial asymmetry can be present at birth (congenital) or can develop later in life due to various factors such as injury, surgery, growth disorders, nerve damage, or tumors. In some cases, facial asymmetry may not cause any medical problems and may only be of cosmetic concern. However, in other cases, it may indicate an underlying medical condition that requires treatment.
Depending on the severity and cause of the facial asymmetry, treatment options may include cosmetic procedures such as fillers or surgery, orthodontic treatment, physical therapy, or medication to address any underlying conditions.
Gingival hypertrophy is a condition characterized by an abnormal enlargement or overgrowth of the gingiva (gum tissue). This can be caused due to various reasons such as inflammation from poor oral hygiene, certain medications like phenytoin and cyclosporine, or systemic conditions such as pregnancy, leukemia, and vitamin C deficiency.
The enlarged gums may appear swollen, red, and bleed easily. They can also cover the teeth, making cleaning difficult, which can further worsen the inflammation. Depending on the cause, treatment options may include improving oral hygiene, changing medications, or undergoing surgical procedures to remove the excess tissue.
Maxillofacial abnormalities, also known as craniofacial anomalies, refer to a broad range of structural and functional disorders that affect the development of the skull, face, jaws, and related soft tissues. These abnormalities can result from genetic factors, environmental influences, or a combination of both. They can vary in severity, from minor cosmetic issues to significant impairments of vital functions such as breathing, speaking, and eating.
Examples of maxillofacial abnormalities include cleft lip and palate, craniosynostosis (premature fusion of the skull bones), hemifacial microsomia (underdevelopment of one side of the face), and various other congenital anomalies. These conditions may require multidisciplinary treatment involving surgeons, orthodontists, speech therapists, and other healthcare professionals to address both functional and aesthetic concerns.
A dermoid cyst is a type of benign (non-cancerous) growth that typically develops during embryonic development. It is a congenital condition, which means it is present at birth, although it may not become apparent until later in life. Dermoid cysts are most commonly found in the skin or the ovaries of women, but they can also occur in other areas of the body, such as the spine or the brain.
Dermoid cysts form when cells that are destined to develop into skin and its associated structures, such as hair follicles and sweat glands, become trapped during fetal development. These cells continue to grow and multiply, forming a sac-like structure that contains various types of tissue, including skin, fat, hair, and sometimes even teeth or bone.
Dermoid cysts are usually slow-growing and may not cause any symptoms unless they become infected or rupture. In some cases, they may cause pain or discomfort if they press on nearby structures. Treatment typically involves surgical removal of the cyst to prevent complications and alleviate symptoms.
 Goldenhar syndrome - Wikipedia
Goldenhar syndrome - Wikipedia Goldenhar syndrome - Ontology Report - Rat Genome Database
Goldenhar syndrome - Ontology Report - Rat Genome Database Goldenhar syndrome | Pediatric Oncall Journal
Goldenhar syndrome | Pediatric Oncall Journal Goldenhar Syndrome - AboutFace
Goldenhar Syndrome - AboutFace Goldenhar Syndrome - EyeWiki
Goldenhar Syndrome - EyeWiki Manifestations of Craniofacial Syndromes: Overview, Classification, Apert Syndrome
Manifestations of Craniofacial Syndromes: Overview, Classification, Apert Syndrome Goldenhar Syndrome - Pictures, Symptoms, Deformities, Treatment
Goldenhar Syndrome - Pictures, Symptoms, Deformities, Treatment Child with Goldenhar syndrome shows off Baha 5 Sound Processor
Child with Goldenhar syndrome shows off Baha 5 Sound Processor Grave's disease in a case of Goldenhar syndrome - Karnataka Paediatric Journal
Grave's disease in a case of Goldenhar syndrome - Karnataka Paediatric Journal Goldenhar Syndrome in a pediatric patient: a case report and review of literature
Goldenhar Syndrome in a pediatric patient: a case report and review of literature Craniofacial microsomia: MedlinePlus Genetics
Craniofacial microsomia: MedlinePlus Genetics Blue corn may help prevent, treat metabolic syndrome
Blue corn may help prevent, treat metabolic syndrome Mandibular reconstruction in the growing patient with unilateral craniofacial microsomia: a systematic review
Mandibular reconstruction in the growing patient with unilateral craniofacial microsomia: a systematic review Kidshealth - Diseases & Conditions | Akron Children's Hospital
Kidshealth - Diseases & Conditions | Akron Children's Hospital Ear Tags (for Parents) - Nemours KidsHealth
Ear Tags (for Parents) - Nemours KidsHealth Waardenburg syndrome | Eurorad
Waardenburg syndrome | Eurorad Education and Training | Verathon
Education and Training | Verathon The Journal of Contemporary Dental Practice
The Journal of Contemporary Dental Practice Comments Archives - DIY Photography
Comments Archives - DIY Photography Dermoid Cyst - American Association for Pediatric Ophthalmology and Strabismus
Dermoid Cyst - American Association for Pediatric Ophthalmology and Strabismus Research Study to Find Connection Between ASD and Birth Defects - Kathy J. Marshack, Ph.D.
Research Study to Find Connection Between ASD and Birth Defects - Kathy J. Marshack, Ph.D. Congenital Anomalies of the Ear Microtia/Anotia | NCBDDD | CDC
Congenital Anomalies of the Ear Microtia/Anotia | NCBDDD | CDC Cauti92 - Swap-bot
Cauti92 - Swap-bot Otosclerosis - Ear, Nose, and Throat Disorders - MSD Manual Professional Edition
Otosclerosis - Ear, Nose, and Throat Disorders - MSD Manual Professional Edition