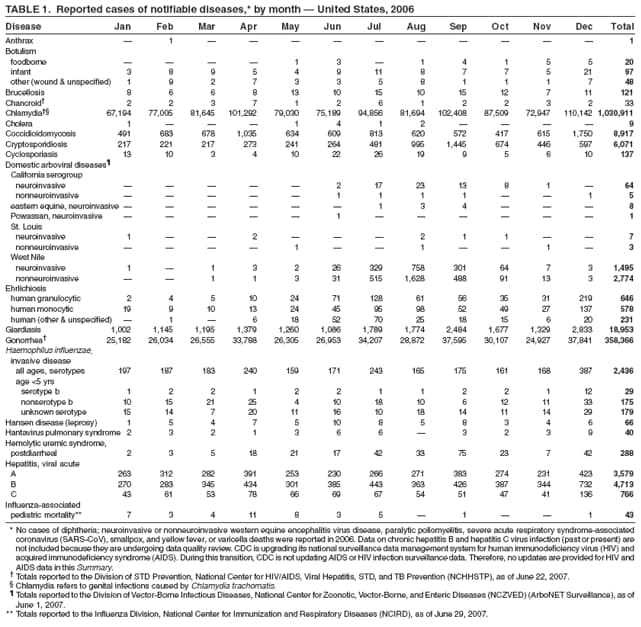
Leprosy
Leprosy, Lepromatous
Leprosy, Tuberculoid
Mycobacterium leprae
Leprosy, Borderline
Leprosy, Multibacillary
Leprostatic Agents
Leprosy, Paucibacillary
Erythema Nodosum
Lepromin
Armadillos
Clofazimine
Dapsone
Glycolipids
Neuritis
Skin
Brazil
Myanmar
Specificity and function of immunogenic peptides from the 35-kilodalton protein of Mycobacterium leprae. (1/1113)
We identified a T-cell determinant of the 35-kDa antigen of Mycobacterium leprae which is discriminatory against cross-sensitization by its closely related homologue in Mycobacterium avium. From synthetic peptides covering the entire sequence, those with the highest affinity and permissive binding to purified HLA-DR molecules were evaluated for the stimulation of proliferation of peripheral blood mononuclear cells (PBMCs) from leprosy patients and healthy sensitized controls. Responses to the peptide pair 206-224, differing by four residues between M. leprae and M. avium, involved both species-specific and cross-reactive T cells. Lymph node cell proliferation in HLA-DRB1*01 transgenic mice was reciprocally species specific, but only the response to the M. leprae peptide in the context of DR1 was immunodominant. Of the cytokines in human PBMC cultures, gamma interferon production was negligible, while interleukin 10 (IL-10) responses in both patients and controls were more pronounced. IL-10 was most frequently induced by the shared 241-255 peptide, indicating that environmental cross-sensitization may skew the response toward a potentially pathogenic cytokine phenotype. (+info)Candidate bacterial conditions. (2/1113)
This article provides background information on bacterial diseases and discusses those that are candidates for elimination or eradication. Only one disease, neonatal tetanus, is a strong candidate for elimination. Others, including Haemophilus influenzae b infection, leprosy, diphtheria, pertussis, tuberculosis, meningococcal disease, congenital syphilis, trachoma and syphilis are important causes of morbidity and mortality in industrialized and developing countries. For all these diseases, eradication/elimination is not likely because of the characteristics of the disease and limitations in the interventions. (+info)Neutrophils isolated from leprosy patients release TNF-alpha and exhibit accelerated apoptosis in vitro. (3/1113)
This study demonstrated that polymorphonuclear neutrophils (PMN) participate in the acute inflammatory response in leprosy as effector cells. Lepromatous patients present intense infiltrate of neutrophils in reactional (ENL) lesions. Circulating PMN of nonreactional patients, healthy donors, and reactional patients were purified and analyzed in vitro. The study confirmed the short lifespan of these cells in culture with progressive changes characteristic of apoptosis. Apoptosis was greatly accelerated in ENL patients as shown by cellular morphology, later confirmed by qualitative and quantitative analysis of fragmented DNA. It was observed that neutrophils stimulated with lipopolysaccharide, Mycobacterium leprae, and lipoarabinomannan secrete interleukin-8 and tumor necrosis factor alpha (TNF-alpha). Thalidomide, a drug known to inhibit TNF-alpha synthesis on monocytes, also exerted an inhibitory effect on TNF-alpha secretion in neutrophils. These data suggest that PMN can participate in the regulation of the immune response in leprosy and can contribute to the amplification of TNF-alpha production at the site of ENL lesion. (+info)Immune complexes and complement hypercatabolism in patients with leprosy. (4/1113)
The occurrence of immune complexes in the serum and the level of the C3 breakdown product C3d in the plasma from patients with leprosy were studied by quantitative methods and the results were compared in various forms of the disease. These studies were performed on sixty-two samples from twenty-six patients. The serum 125I-C1q binding activity was found to be increased by more than 2 s.d., as compared to the normal values, in most of the sera from patients with erythema nodosum leprosum (ENL) (80%) and uncomplicated lepromatous leprosy (82%), but also in the sera from patients with tuberculoid leprosy (58%). In vitro studies suggested that immune complexes involving mycobacterial antigens were present in leprosy sera. An increased C3d level (greater than 2s.d.) was also found in most of the plasma from patients with ENL (70%), but rarely in the plasma from patients with uncomplicated lepromatous leprosy (18%) and never in tuberculoid leprosy patients' plasma. The absence of a significant correlation between the 125I-C1q binding activity and the C3d level in leprosy patients may suggest that extravascular immune complexes are involved in the complement activation occurring in ENL. The quantitation of C3d in plasma may be of some practical interest in the early diagnosis of ENL complications of leprosy. (+info)IL-18 promotes type 1 cytokine production from NK cells and T cells in human intracellular infection. (5/1113)
We investigated the role of IL-18 in leprosy, a disease characterized by polar cytokine responses that correlate with clinical disease. In vivo, IL-18 mRNA expression was higher in lesions from resistant tuberculoid as compared with susceptible lepromatous patients, and, in vitro, monocytes produced IL-18 in response to Mycobacterium leprae. rIL-18 augmented M. leprae-induced IFN-gamma in tuberculoid patients, but not lepromatous patients, while IL-4 production was not induced by IL-18. Anti-IL-12 partially inhibited M. leprae-induced release of IFN-gamma in the presence of IL-18, suggesting a combined effect of IL-12 and IL-18 in promoting M. leprae-specific type 1 responses. IL-18 enhanced M. leprae-induced IFN-gamma production rapidly (24 h) by NK cells and in a more sustained manner (5 days) by T cells. Finally, IL-18 directly induced IFN-gamma production from mycobacteria-reactive T cell clones. These results suggest that IL-18 induces type 1 cytokine responses in the host defense against intracellular infection. (+info)Dominant recognition of a cross-reactive B-cell epitope in Mycobacterium leprae 10 K antigen by immunoglobulin G1 antibodies across the disease spectrum in leprosy. (6/1113)
Mycobacterium leprae-specific immunoglobulin G1 (IgG1) antibodies in patients with leprosy show a direct correlation with bacterial load (rho=0.748; P<0002) suggesting that IgG1 B-cell responses may be surrogate markers of disease progression. To investigate if this upregulation was a general feature of IgG1 responses to all M. leprae (ML) antigens, we analysed responses to several recombinant purified ML heat-shock proteins (HSP). Three recombinant HSPs (ML10 K, ML 18 K and ML 65 K) were tested for their ability to induce various IgG subclasses in patients with either the lepromatous (LL/BL, n=26) or tuberculoid form (BT/TT, n=39) of the disease as well as in healthy households (HC, n=14) and endemic controls (EC=19). Our major findings were: (1) selective augmentation of IgG1 antibody responses to ML10 K; (2) recognition of a restricted number of epitopes across the disease spectrum and healthy controls by IgG1 antibodies; (3) dominant recognition of cross-reactive epitopes which were common to both ML and MT 10 K. This response was not related to contamination with endotoxin. Epitope mapping using 15-mer overlapping peptides spanning the ML 10 000 MW revealed an immunodominant IgG1 binding peptide (aa41-55) in patients as well as healthy controls. This peptide is a shared epitope with M. tuberculosis 10 K suggesting that postswitched IgG1 B cells recognizing this epitope rather than naive B cells are being expanded. (+info)Species-specific identification of Mycobacterium leprae by PCR-restriction fragment length polymorphism analysis of the hsp65 gene. (7/1113)
PCR-restriction fragment length polymorphism analysis (PRA) of the hsp65 gene present in all mycobacteria was used in the present investigation to characterize Mycobacterium leprae. Bacilli were extracted and purified from different organs from experimentally infected armadillos and nude mice (Swiss mice of nu/nu origin). A total of 15 samples were assayed in duplicate, and the results were compared with those obtained for a total of 147 cultivable mycobacteria representing 34 species. Irrespective of its origin or viability, M. leprae strains from all the samples were uniformly characterized by two fragments of 315 and 135 bp upon BstEII digestion and two fragments of 265 and 130 bp upon HaeIII digestion. PRA is a relatively simple method and permits the conclusive identification of M. leprae to the species level. (+info)Use of a whole blood assay to evaluate in vitro T cell responses to new leprosy skin test antigens in leprosy patients and healthy subjects. (8/1113)
Development of an immunological tool to detect infection with Mycobacterium leprae would greatly benefit leprosy control programmes, as demonstrated by the contribution of the tuberculin test to tuberculosis control. In a new approach to develop a 'tuberculin-like' reagent for use in leprosy, two new fractions of M. leprae depleted of cross-reactive and immunomodulatory lipids- MLSA-LAM (cytosol-derived) and MLCwA (cell wall-derived)-have been produced in a form suitable for use as skin test reagents. T cell responses (interferon-gamma (IFN-gamma) and lymphoproliferation) to these two new fractions were evaluated in a leprosy-endemic area of Nepal using a simple in vitro whole blood test. The two fractions were shown to be highly potent T cell antigens in subjects exposed to M. leprae-paucibacillary leprosy patients and household contacts. Responses to the fractions decreased towards the lepromatous pole of leprosy. Endemic control subjects also showed high responses to the fractions, indicating high exposure to M. leprae, or cross-reactive mycobacterial antigens, in this Nepali population. The new fractions, depleted of lipids and lipoarabinomannan (LAM) gave enhanced responses compared with a standard M. leprae sonicate. The cell wall fraction appeared a more potent antigen than the cytosol fraction, which may be due to the predominance of the 65-kD GroEL antigen in the cell wall. The whole blood assay proved a robust field tool and a useful way of evaluating such reagents prior to clinical trials. (+info)Leprosy, also known as Hansen's disease, is a chronic infectious disease caused by the bacterium Mycobacterium leprae. It primarily affects the skin, peripheral nerves, mucosal surfaces of the upper respiratory tract, and the eyes. The disease mainly spreads through droplets from the nose and mouth of infected people.
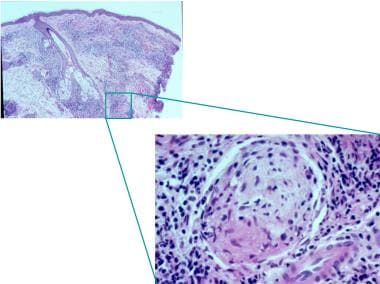
Leprosy is characterized by granulomatous inflammation, which leads to the formation of distinctive skin lesions and nerve damage. If left untreated, it can cause progressive and permanent damage to the skin, nerves, limbs, and eyes. However, with early diagnosis and multidrug therapy (MDT), the disease can be cured, and disability can be prevented or limited.
The World Health Organization (WHO) classifies leprosy into two types based on the number of skin lesions and bacteriological index: paucibacillary (one to five lesions) and multibacillary (more than five lesions). This classification helps determine the appropriate treatment regimen.
Although leprosy is curable, it remains a public health concern in many developing countries due to its stigmatizing nature and potential for social exclusion of affected individuals.
Lepromatous leprosy is a type of leprosy, a chronic infectious disease caused by the bacterium Mycobacterium leprae. In this form of the disease, there is a widespread and diffuse involvement of the skin, mucous membranes, and peripheral nerves. The bacteria multiply slowly and spread to the skin, upper respiratory tract, and peripheral nerves.
In lepromatous leprosy, the immune response is weak, allowing for extensive bacterial multiplication and widespread tissue damage. The skin lesions are typically numerous, pale, and have a smooth surface. Nerve involvement can lead to loss of sensation, muscle weakness, and deformities, particularly in the hands and feet.
Lepromatous leprosy is a more severe form of the disease compared to tuberculoid leprosy, which has a stronger immune response and localized skin lesions. Both forms of the disease are treatable with multidrug therapy (MDT), recommended by the World Health Organization (WHO) for all leprosy patients. Early diagnosis and treatment can prevent disability and reduce transmission.
Tuberculoid leprosy is a form of leprosy caused by the bacterium Mycobacterium leprae. It is one of the two major forms of the disease, with the other being lepromatous leprosy.
Tuberculoid leprosy typically presents with fewer lesions (generally less than five) that are well-defined, asymmetric, and dry. The lesions can be hypopigmented or erythematous and may have a raised border. Nerve involvement is common in tuberculoid leprosy, leading to symptoms such as numbness, muscle weakness, and paralysis.
The disease primarily affects the skin, peripheral nerves, and mucosa of the upper respiratory tract. Tuberculoid leprosy is characterized by a strong cell-mediated immune response, which can lead to the destruction of mycobacteria but may also cause tissue damage. It is generally a milder form of the disease compared to lepromatous leprosy and responds well to treatment with multidrug therapy (MDT).
"Mycobacterium leprae" is a slow-growing, rod-shaped, gram-positive bacterium that is the causative agent of leprosy, a chronic infectious disease that primarily affects the skin, peripheral nerves, and mucosal surfaces of the upper respiratory tract. The bacterium was discovered in 1873 by Gerhard Armauer Hansen, a Norwegian physician, and is named after him as "Hansen's bacillus."
"Mycobacterium leprae" has a unique cell wall that contains high amounts of lipids, which makes it resistant to many common disinfectants and antibiotics. It can survive and multiply within host macrophages, allowing it to evade the immune system and establish a chronic infection.
Leprosy is a treatable disease with multidrug therapy (MDT), which combines several antibiotics such as dapsone, rifampicin, and clofazimine. Early diagnosis and treatment can prevent the progression of the disease and reduce its transmission to others.
"Borderline leprosy," also known as "borderline tuberculoid leprosy (BT)," is a type of leprosy that falls in the middle of the clinical spectrum of the disease. It has features of both tuberculoid and lepromatous leprosy, but they are not well-defined. The immune response in borderline leprosy is unstable, which means that the condition can either improve or deteriorate over time.
In borderline leprosy, there are usually a few well-defined lesions with some sensory loss. The bacteria are present in the skin and nerves, but they have not yet caused extensive damage. Treatment for borderline leprosy is similar to that of other forms of leprosy, which typically involves multidrug therapy (MDT) recommended by the World Health Organization (WHO).
It's important to note that leprosy is a curable disease, and early diagnosis and treatment can prevent complications and reduce transmission.
Multibacillary (MB) leprosy, also known as lepromatous leprosy, is a type of leprosy that is characterized by the widespread dissemination of the bacterium Mycobacterium leprae throughout the body. It is one of two major forms of leprosy, with the other being paucibacillary (PB) leprosy.
In MB leprosy, there are typically numerous skin lesions that may be widespread and often have a symmetrical distribution. The lesions can appear as nodules, plaques, or macules and can be hypopigmented or erythematous. They may also have a characteristic appearance with loss of sensation due to nerve damage.
MB leprosy is characterized by the presence of large numbers of bacilli in the skin lesions and nasal mucosa, as well as involvement of multiple nerves leading to deformities and disabilities if left untreated. The diagnosis of MB leprosy is usually made based on clinical examination, skin smears, and/or biopsy.
MB leprosy is treated with a multidrug therapy (MDT) regimen recommended by the World Health Organization (WHO), which includes rifampicin, dapsone, and clofazimine for at least 12 months. Early diagnosis and treatment of MB leprosy can prevent disability and reduce transmission.
Leprosstatic agents are substances or drugs that have a specific effect on the bacterium that causes leprosy, also known as Mycobacterium leprae. These agents are used in the treatment and prevention of leprosy, a chronic infectious disease that primarily affects the skin, peripheral nerves, and mucosal surfaces of the upper respiratory tract.
The most common leprostatic agents are antibiotics, which target the bacterial cells and inhibit their growth or kill them. The two main antibiotics used to treat leprosy are dapsone and rifampicin, which are often given in combination with other drugs such as clofazimine to prevent the development of drug-resistant strains of the bacteria.
Leprosstatic agents are usually administered orally or by injection, and the duration of treatment can vary depending on the severity of the disease and the patient's response to therapy. It is important to note that early detection and treatment of leprosy can help prevent the progression of the disease and reduce the risk of transmission to others.
Paucibacillary leprosy is a type of leprosy that is characterized by the presence of fewer than 5 skin lesions and no bacterial growth in slit skin smears or biopsies. It is also known as tuberculoid leprosy and is caused by the Mycobacterium leprae bacteria. The condition primarily affects the nerves and skin, leading to numbness, muscle weakness, and disfigurement if left untreated. Paucibacillary leprosy tends to have a better prognosis compared to multibacillary leprosy, which is characterized by more numerous skin lesions and bacterial growth.
Erythema nodosum is a type of inflammation that occurs in the fatty layer of the skin, causing painful, red or purple bumps (nodules) to form. It is a type of panniculitis, which refers to any condition that causes inflammation of the fatty layer of tissue beneath the skin.
Erythema nodosum is often associated with a variety of underlying conditions, such as infections (e.g., streptococcus, tuberculosis), medications (e.g., sulfa drugs, oral contraceptives), inflammatory bowel disease (e.g., Crohn's disease, ulcerative colitis), and pregnancy.
The bumps associated with erythema nodosum typically appear on the shins, ankles, knees, or other areas of the legs, although they can also occur on the arms, hands, or face. The bumps may be tender to the touch, warm, and swollen, and they may cause pain or discomfort when walking or standing for prolonged periods.
In most cases, erythema nodosum resolves on its own within a few weeks to several months, although symptoms can be managed with medications such as nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroids. Treating the underlying condition is also important for resolving erythema nodosum and preventing recurrences.
Lepromin is not a medical condition but rather a diagnostic test used in the diagnosis and classification of leprosy, a chronic infectious disease caused by the bacterium Mycobacterium leprae. The Lepromin test measures the cell-mediated immunity of an individual to the bacteria that causes leprosy.
The test involves injecting two types of antigens derived from M. leprae, one more soluble and the other less soluble, into the skin of the forearm. The response of the immune system to these antigens is then observed after 24 hours (for the soluble antigen) and 48 hours (for the less soluble antigen).
A positive reaction to the more soluble antigen indicates a strong cell-mediated immunity, which is associated with tuberculoid leprosy, a milder form of the disease. A positive reaction to the less soluble antigen suggests a weaker cell-mediated immunity and is associated with lepromatous leprosy, a more severe form of the disease.
It's important to note that the Lepromin test has limited availability and is not widely used in many parts of the world due to its complexity and the need for specialized laboratory facilities.
An armadillo is not a medical condition or term. It is a type of mammal that is native to the Americas, known for its distinctive armor-like shell. If you have any questions about a specific medical condition or topic, I would be happy to help if you could provide more information.
Clofazimine is an antimycobacterial medication used mainly in the treatment of leprosy (Hansen's disease) and also has some activity against Mycobacterium avium complex (MAC) infections. It is an oral riminophenazine dye that accumulates in macrophages and bacterial cells, where it inhibits mycobacterial DNA-dependent RNA polymerase. Its side effects include skin discoloration, gastrointestinal symptoms, and potential eye toxicity.
Dapsone is a medication that belongs to a class of drugs called sulfones. It is primarily used to treat bacterial skin infections such as leprosy and dermatitis herpetiformis (a skin condition associated with coeliac disease). Dapsone works by killing the bacteria responsible for these infections.
In addition, dapsone has anti-inflammatory properties and is sometimes used off-label to manage inflammatory conditions such as vasculitis, bullous pemphigoid, and chronic urticaria. It is available in oral tablet form and topical cream or gel form.
Like all medications, dapsone can cause side effects, which may include nausea, loss of appetite, and headache. More serious side effects, such as methemoglobinemia (a blood disorder that affects the body's ability to transport oxygen), peripheral neuropathy (nerve damage that causes pain, numbness, or weakness in the hands and feet), and liver damage, can occur but are less common.
It is important for patients taking dapsone to be monitored by a healthcare provider to ensure safe and effective use of the medication.
Bacterial antigens are substances found on the surface or produced by bacteria that can stimulate an immune response in a host organism. These antigens can be proteins, polysaccharides, teichoic acids, lipopolysaccharides, or other molecules that are recognized as foreign by the host's immune system.
When a bacterial antigen is encountered by the host's immune system, it triggers a series of responses aimed at eliminating the bacteria and preventing infection. The host's immune system recognizes the antigen as foreign through the use of specialized receptors called pattern recognition receptors (PRRs), which are found on various immune cells such as macrophages, dendritic cells, and neutrophils.
Once a bacterial antigen is recognized by the host's immune system, it can stimulate both the innate and adaptive immune responses. The innate immune response involves the activation of inflammatory pathways, the recruitment of immune cells to the site of infection, and the production of antimicrobial peptides.
The adaptive immune response, on the other hand, involves the activation of T cells and B cells, which are specific to the bacterial antigen. These cells can recognize and remember the antigen, allowing for a more rapid and effective response upon subsequent exposures.
Bacterial antigens are important in the development of vaccines, as they can be used to stimulate an immune response without causing disease. By identifying specific bacterial antigens that are associated with virulence or pathogenicity, researchers can develop vaccines that target these antigens and provide protection against infection.
Glycolipids are a type of lipid (fat) molecule that contain one or more sugar molecules attached to them. They are important components of cell membranes, where they play a role in cell recognition and signaling. Glycolipids are also found on the surface of some viruses and bacteria, where they can be recognized by the immune system as foreign invaders.
There are several different types of glycolipids, including cerebrosides, gangliosides, and globosides. These molecules differ in the number and type of sugar molecules they contain, as well as the structure of their lipid tails. Glycolipids are synthesized in the endoplasmic reticulum and Golgi apparatus of cells, and they are transported to the cell membrane through vesicles.
Abnormalities in glycolipid metabolism or structure have been implicated in a number of diseases, including certain types of cancer, neurological disorders, and autoimmune diseases. For example, mutations in genes involved in the synthesis of glycolipids can lead to conditions such as Tay-Sachs disease and Gaucher's disease, which are characterized by the accumulation of abnormal glycolipids in cells.
Neuritis is a general term that refers to inflammation of a nerve or nerves, often causing pain, loss of function, and/or sensory changes. It can affect any part of the nervous system, including the peripheral nerves (those outside the brain and spinal cord) or the cranial nerves (those that serve the head and neck). Neuritis may result from various causes, such as infections, autoimmune disorders, trauma, toxins, or metabolic conditions. The specific symptoms and treatment depend on the underlying cause and the affected nerve(s).
In medical terms, the skin is the largest organ of the human body. It consists of two main layers: the epidermis (outer layer) and dermis (inner layer), as well as accessory structures like hair follicles, sweat glands, and oil glands. The skin plays a crucial role in protecting us from external factors such as bacteria, viruses, and environmental hazards, while also regulating body temperature and enabling the sense of touch.
I apologize, but "Brazil" is not a medical term or condition. It is the largest country in both South America and Latin America by land area and population. If you have any questions related to medical terminology or health concerns, please provide more information and I will do my best to help.
'Mycobacterium lepraemurium' is not typically associated with human leprosy or any medical conditions affecting humans. It is a species of mycobacteria that primarily infects rodents, particularly mice and rats. This bacterium is the causative agent of a form of leprosy-like disease in these animals, known as murine leprosy.
Human infections with 'Mycobacterium lepraemurium' are extremely rare and have only been reported in a handful of cases worldwide. When they do occur, they usually result from close contact with infected rodents or their excrement. The disease caused by this bacterium in humans is typically milder than human leprosy and often resolves on its own without specific treatment.
Therefore, 'Mycobacterium lepraemurium' should not be confused with the mycobacterial species that cause leprosy in humans, such as 'Mycobacterium leprae' or 'Mycobacterium lepromatosis'.
'Leper Colonies' are not a medical term per se, but rather a historical and sociological concept. They refer to communities that were established in many parts of the world, especially in the past, to isolate and care for individuals affected by leprosy or Hansen's disease. The intention was often to prevent the spread of the disease, which was not well understood at the time, and to provide a place for those afflicted to live. However, these colonies often led to social stigma, discrimination, and isolation of the individuals living there. It is important to note that leprosy is now well-controlled with multidrug therapy, and it is not as easily transmitted or as devastating a disease as it once was. The World Health Organization recommends that people affected by leprosy be treated in regular health facilities within their own communities to avoid stigma and promote early detection and treatment.
I'm sorry for any confusion, but "Myanmar" is not a medical term or condition. It is the name of a country in Southeast Asia, also known as Burma. If you have any questions about medical conditions or terminology, I would be happy to help clarify those for you.