Myoglobinuria
Glycogen Storage Disease Type V
Acute Kidney Injury
Myoglobin
Creatine Kinase
Non-traumatic acute rhabdomyolysis. (1/86)
A boy developed sudden severe generalized muscle stiffness, bulbar weakness and passed dark coloured urine. Laboratory tests revealed marked elevation of creatinine kinase(CK) levels and myoglobinuria. Histopathology of quadriceps muscle showed features of acute rhabdomyolysis. Patient made complete clinical recovery over a period of three weeks and CK returned to normal level. The possible aetiologies of non-traumatic rhabdomyolysis are discussed and the relevant literature reviewed. (+info)Renal cortical ceramide patterns during ischemic and toxic injury: assessments by HPLC-mass spectrometry. (2/86)
Ceramides are a class of signaling molecules that can acutely accumulate in tissues as part of a "stress response." They are classically measured by the diacylglycerol kinase assay, which, in general, measures total ceramide rather than individual moieties within the diverse ceramide family. The present study was undertaken to 1) adapt current HPLC-mass spectrometry technology for measuring individual renal ceramides, and 2) use this technique to more fully characterize the nature of the renal ceramide "stress" reaction. Renal cortical tissues were obtained from CD-1 mice under control conditions and 2 or 18 h after renal injury (ischemia-reperfusion and glycerol-mediated myohemoglobinuria). C24, C22, and C16 ceramides were identified in normal renal cortex, constituting 70, 10, and 20% of the total ceramide pool, respectively. Within each of these families, heterogeneity was apparent because of differing degrees of unsaturation (0-3 double bonds) in the constituent fatty acid of ceramide. Renal injury dramatically changed ceramide profiles: 1) total ceramide increased by approximately 300%; 2) although all ceramides participated in this reaction, they did so to differing degrees; 3) this caused pronounced changes in ceramide distribution patterns; 4) injury induced a striking shift toward unsaturated (vs. saturated) fatty acids within the C22 and C24 (but not the C16) ceramide pools; and 5) the extent of these qualitative changes differed according to the etiology of the initiating renal damage. Thus we conclude that ceramide stress response involves major qualitative (and not simply quantitative) changes in ceramide expression that are partially disease dependent. These findings underscore the fact that simply measuring total renal ceramide content (e.g., by diacylglycerol kinase assay) substantially oversimplifies the nature and, hence, the potential implications of the ceramide stress reaction. (+info)Acute alcoholic myopathy, rhabdomyolysis and acute renal failure: a case report. (3/86)
A case of middle aged male who developed swelling and weakness of muscles in the lower limbs following a heavy binge of alcohol is being reported. He had myoglobinuria and developed acute renal failure for which he was dialyzed. Acute alcoholic myopathy is not a well recognized condition and should be considered in any intoxicated patient who presents with muscle tenderness and weakness. (+info)Effects of LTB4 receptor antagonist on myonephropathic metabolic syndrome: an experimental study. (4/86)
The aims of this study were to determine the involvement of leukocytes in reperfusion injury following acute arterial occlusion and to evaluate the effect of the leukotriene B4 (LTB4), which is a chemical mediator of inflammation, receptor antagonist. We examined the usefulness of LTB4 receptor antagonist, ONO-4057, as a preventative drug for myonephropathic metabolic syndrome (MNMS). The experimental leg ischemic model was developed using Wistar strain rats. The rats were divided into 4 groups. In Group R3, the infra-renal abdominal aorta was clamped for 3 hrs and the right femoral muscle tissue was cut to block the development of a collateral artery. In Group R6, the infra-renal abdominal aorta was clamped for 6 hrs and the right femoral muscle tissue was cut. In Group C, the controls, there was no clamping of the abdominal aorta and the right femoral muscle tissue was cut. In Group M, the medicated group, rats were pretreated with an LTB4 receptor antagonist, ONO-4057, just before reperfusion. Blood serum interleukin-1 (IL-1), interleukin-8 (IL-8), creatine phosphokinase (CPK), and aldolase were measured and compared in each of those 4 groups. We also examined the intercellular adhesion molecule-1 (ICAM-1) expression in various organs (liver, heart and kidney) by immunohistochemistry. We found that IL-1 beta levels were low in all groups. CPK, aldolase and IL-8 levels after reperfusion in Group R6 significantly high compared with the levels in Group C (P < 0.03 about CPK, P < 0.05 about aldolase, and P < 0.05 about IL-8). The levels of CPK, aldolase, and IL-8 in Group M were significantly lower than those in Group R6 (P < 0.02 about CPK, P < 0.04 about aldolase, and P < 0.03 about IL-8). We determined immunohistochemically that the expression of ICAM-1 was positive on endothelial cells at the coronary artery and the small vein in Group R6 and that the expression of ICAM-1 was negative on endothelial cells in Group C. Those data suggested that ICAM-1 may play an important role in the progression of reperfusion injury, and the adhesion of neutrophilic leukocytes on endothelial cells may play a significant role in MNMS. LTB4 receptor antagonist may be useful for preventing reperfusion injury following acute aortic occlusion. (+info)Changes in free and esterified cholesterol: hallmarks of acute renal tubular injury and acquired cytoresistance. (5/86)
Acute tubular cell injury is accompanied by plasma membrane phospholipid breakdown. Although cholesterol is a dominant membrane lipid which interdigitates with, and impacts, phospholipid homeostasis, its fate during the induction and recovery phases of acute renal failure (ARF) has remained ill defined. The present study was performed to ascertain whether altered cholesterol expression is a hallmark of evolving tubular damage. Using gas chromatographic analysis, free cholesterol (FC) and esterified cholesterol (CE) were quantified in: 1) isolated mouse proximal tubule segments (PTS) after 30 minutes of hypoxic or oxidant (ferrous ammonium sulfate) injury; 2) cultured proximal tubule (HK-2) cells after 4 or 18 hours of either ATP depletion/Ca(2+) ionophore- or ferrous ammonium sulfate-mediated injury; and 3) in renal cortex 18 hours after induction of glycerol-induced myoglobinuric ARF, a time corresponding to the so-called "acquired cytoresistance" state (ie, resistance to further renal damage). Hypoxic and oxidant injury each induced approximately 33% decrements in CE (but not FC) levels in PTS, corresponding with lethal cell injury ( approximately 50 to 60% LDH release). When comparable CE declines were induced in normal PTS by exogenous cholesterol esterase treatment, proportionate lethal cell injury resulted. During models of slowly evolving HK-2 cell injury, progressive CE increments occurred: these were first noted at 4 hours, and reached approximately 600% by 18 hours. In vivo myoglobinuric ARF produced comparable renal cortical CE (and to a lesser extent FC) increments. Renal CE accumulation strikingly correlated with the severity of ARF (eg, blood urea nitrogen versus CE; r, 0.84). Mevastatin blocked cholesterol accumulation in injured HK-2 cells, indicating de novo synthesis was responsible. Acute tubule injury first lowers, then raises, tubule cholesterol content. Based on previous observations that cholesterol has cytoprotectant properties, the present findings have potential relevance for both the induction and maintenance phases of ARF. (+info)Acute cardiomyopathy with rhabdomyolysis in chronic alcoholism. (6/86)
Of five chronic alcoholics with acute skeletal muscle necrosis (rhabdomyolysis) three developed acute heart failure with disturbances of rhythm and conduction. Symptoms came on abruptly after a period of intensified drinking. Myocardial infarction, thiamine deficiency, and cobalt intoxication were excluded. Probably the whole spectrum of muscle disease in chronic alcoholism may be commoner than has been suspected. (+info)Altered cholesterol localization and caveolin expression during the evolution of acute renal failure. (7/86)
BACKGROUND: Renal cortical/proximal tubule cholesterol accumulation, with preferential localization within plasma membrane "detergent resistant microdomains" (DRMs: rafts/caveolae), is a hallmark of the maintenance phase of acute renal failure (ARF). This study addressed two related issues: (1) Are maintenance-phase cholesterol increases accompanied by an up-regulation of caveolin, a DRM/caveolar-associated cholesterol binding protein? (2) Is DRM cholesterol/caveolin homeostasis acutely altered during the induction phase of ARF? METHODS: Mouse kidneys were subjected to ischemia +/- reperfusion (I/R) followed by assessment of cholesterol DRM partitioning. Acute cell injury effects on potential caveolin release from isolated proximal tubules or into urine also were assessed. Finally, renal cortical/isolated proximal tubule caveolin levels were determined 18 hours after I/R or myoglobinuric ARF. RESULTS: Acute ischemia causes a rapid shift of cholesterol into cortical DRMs (>22%). Cholesterol migration into DRMs also was observed in ATP-depleted cultured proximal tubule (HK-2) cells. Acute hypoxic or toxic tubule injury induced plasma membrane caveolin release (Western blot). By the maintenance phase of ARF, marked renal cortical/proximal tubule caveolin increases resulted. CONCLUSIONS: Acute proximal tubular injury damages caveolar/DRM structures, as determined by cholesterol maldistribution and caveolin release. Post-injury, there is a dramatic up-regulation of renal cortical/proximal tubule caveolin, suggesting an increased caveolar mass. These findings indicate, to our knowledge for the first time, that dysregulation of caveolae/raft microdomain expression is a correlate of, and potential participant in, the induction and maintenance phases of ischemic and toxic forms of experimental ARF. (+info)A3 adenosine receptor knockout mice are protected against ischemia- and myoglobinuria-induced renal failure. (8/86)
A(3) adenosine receptor (AR) activation and inhibition worsen and improve, respectively, renal function after ischemia-reperfusion (I/R) injury in rats. We sought to further characterize the role of A(3) ARs in modulating renal function after either I/R or myoglobinuric renal injury. A(3) knockout mice had significantly lower plasma creatinines compared with C57 controls 24 h after I/R or myoglobinuric renal injury. C57 control mice pretreated with the A(3) AR antagonist [3-ethyl-5-benzyl-2-methyl-4-phenylethynyl-6-phenyl-1,4-(+/-)-dihydropyridine-3,5 dicarboxylate] or agonist [0.125 mg/kg N(6)-(3-iodobenzyl)-N-methyl-5'-carbamoyladenosine (IB-MECA)] demonstrated improved or worsened renal function, respectively, after I/R or myoglobinuric renal injury. Higher doses of IB-MECA were lethal in C57 mice subjected to renal ischemia. H(1) but not H(2) histamine receptor antagonist prevented death in mice pretreated with IB-MECA before renal ischemia. Improvement in renal function was associated with significantly improved renal histology. In conclusion, preischemic A(3) AR activation (0.125 mg/kg IB-MECA) exacerbated renal I/R injury in mice. Mice lacking A(3) ARs or blocking A(3) ARs in wild-type mice resulted in significant renal protection from ischemic or myoglobinuric renal failure. (+info)Myoglobinuria is a medical condition characterized by the presence of myoglobin in the urine. Myoglobin is a protein found in muscle cells that is released into the bloodstream when muscle tissue is damaged or broken down, such as during intense exercise, trauma, or muscle diseases like muscular dystrophy and rhabdomyolysis.
When myoglobin is present in high concentrations in the blood, it can damage the kidneys by causing direct tubular injury, cast formation, and obstruction, which can lead to acute kidney injury (AKI) or even renal failure if left untreated. Symptoms of myoglobinuria may include dark-colored urine, muscle pain, weakness, and swelling, as well as symptoms related to AKI such as nausea, vomiting, and decreased urine output.
Diagnosis of myoglobinuria is typically made by detecting myoglobin in the urine using a dipstick test or more specific tests like immunoassays or mass spectrometry. Treatment may involve aggressive fluid resuscitation, alkalization of the urine to prevent myoglobin precipitation, and management of any underlying conditions causing muscle damage.
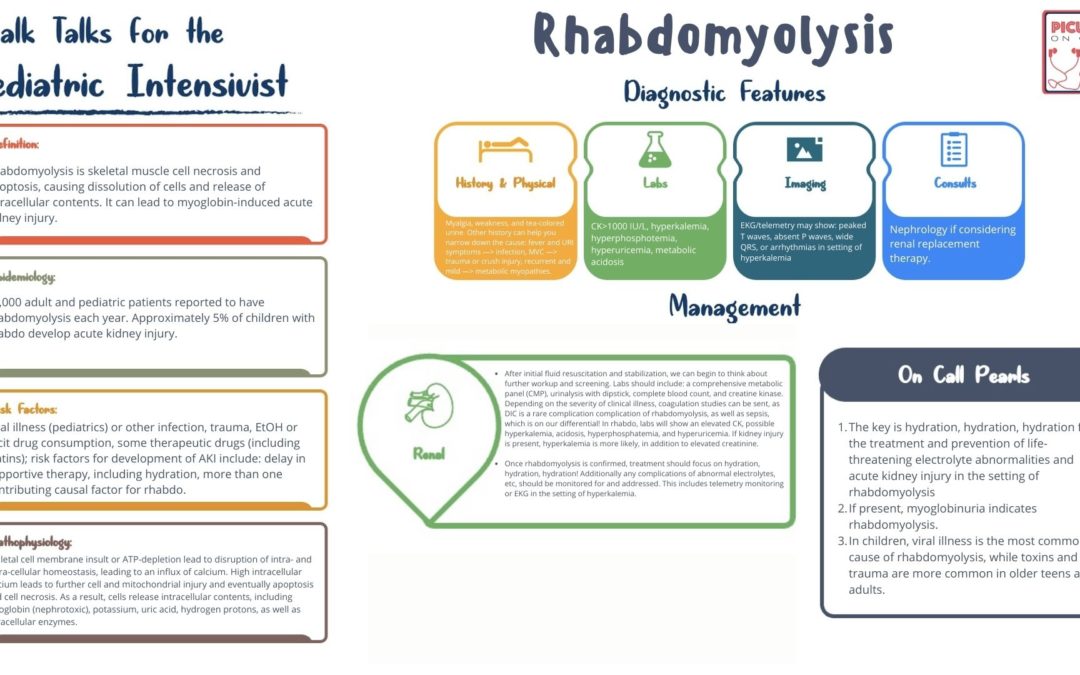
Rhabdomyolysis is a medical condition characterized by the breakdown and degeneration of skeletal muscle fibers, leading to the release of their intracellular contents into the bloodstream. This can result in various complications, including electrolyte imbalances, kidney injury or failure, and potentially life-threatening conditions if not promptly diagnosed and treated.
The process of rhabdomyolysis typically involves three key components:
1. Muscle injury: Direct trauma, excessive exertion, prolonged immobilization, infections, metabolic disorders, toxins, or medications can cause muscle damage, leading to the release of intracellular components into the bloodstream.
2. Release of muscle contents: When muscle fibers break down, they release various substances, such as myoglobin, creatine kinase (CK), lactate dehydrogenase (LDH), aldolase, and potassium ions. Myoglobin is a protein that can cause kidney damage when present in high concentrations in the bloodstream, particularly when it is filtered through the kidneys and deposits in the renal tubules.
3. Systemic effects: The release of muscle contents into the bloodstream can lead to various systemic complications, such as electrolyte imbalances (particularly hyperkalemia), acidosis, hypocalcemia, and kidney injury or failure due to myoglobin-induced tubular damage.
Symptoms of rhabdomyolysis can vary widely depending on the severity and extent of muscle damage but may include muscle pain, weakness, swelling, stiffness, dark urine, and tea-colored or cola-colored urine due to myoglobinuria. In severe cases, patients may experience symptoms related to kidney failure, such as nausea, vomiting, fatigue, and decreased urine output.
Diagnosis of rhabdomyolysis typically involves measuring blood levels of muscle enzymes (such as CK and LDH) and evaluating renal function through blood tests and urinalysis. Treatment generally focuses on addressing the underlying cause of muscle damage, maintaining fluid balance, correcting electrolyte imbalances, and preventing or managing kidney injury.
Glycogen Storage Disease Type V, also known as McArdle's disease, is a genetic disorder that affects the body's ability to break down glycogen, a complex carbohydrate stored in muscles, into glucose, which provides energy for muscle contraction.
This condition results from a deficiency of the enzyme myophosphorylase, which is responsible for breaking down glycogen into glucose-1-phosphate within the muscle fibers. Without sufficient myophosphorylase activity, muscles become easily fatigued and may cramp or become rigid during exercise due to a lack of available energy.
Symptoms typically appear in childhood or adolescence and can include muscle weakness, stiffness, cramps, and myoglobinuria (the presence of myoglobin, a protein found in muscle cells, in the urine) following exercise. Diagnosis is usually confirmed through genetic testing and enzyme assays. Treatment typically involves avoiding strenuous exercise and ensuring adequate hydration and rest before and after physical activity. In some cases, dietary modifications such as high-protein or high-carbohydrate intake may be recommended to help manage symptoms.
Acute kidney injury (AKI), also known as acute renal failure, is a rapid loss of kidney function that occurs over a few hours or days. It is defined as an increase in the serum creatinine level by 0.3 mg/dL within 48 hours or an increase in the creatinine level to more than 1.5 times baseline, which is known or presumed to have occurred within the prior 7 days, or a urine volume of less than 0.5 mL/kg per hour for six hours.
AKI can be caused by a variety of conditions, including decreased blood flow to the kidneys, obstruction of the urinary tract, exposure to toxic substances, and certain medications. Symptoms of AKI may include decreased urine output, fluid retention, electrolyte imbalances, and metabolic acidosis. Treatment typically involves addressing the underlying cause of the injury and providing supportive care, such as dialysis, to help maintain kidney function until the injury resolves.
Muscular diseases, also known as myopathies, refer to a group of conditions that affect the functionality and health of muscle tissue. These diseases can be inherited or acquired and may result from inflammation, infection, injury, or degenerative processes. They can cause symptoms such as weakness, stiffness, cramping, spasms, wasting, and loss of muscle function.
Examples of muscular diseases include:
1. Duchenne Muscular Dystrophy (DMD): A genetic disorder that results in progressive muscle weakness and degeneration due to a lack of dystrophin protein.
2. Myasthenia Gravis: An autoimmune disease that causes muscle weakness and fatigue, typically affecting the eyes and face, throat, and limbs.
3. Inclusion Body Myositis (IBM): A progressive muscle disorder characterized by muscle inflammation and wasting, typically affecting older adults.
4. Polymyositis: An inflammatory myopathy that causes muscle weakness and inflammation throughout the body.
5. Metabolic Myopathies: A group of inherited disorders that affect muscle metabolism, leading to exercise intolerance, muscle weakness, and other symptoms.
6. Muscular Dystonias: Involuntary muscle contractions and spasms that can cause abnormal postures or movements.
It is important to note that muscular diseases can have a significant impact on an individual's quality of life, mobility, and overall health. Proper diagnosis and treatment are crucial for managing symptoms and improving outcomes.
Myoglobin is a protein found in the muscle tissue, particularly in red or skeletal muscles. It belongs to the globin family and has a similar structure to hemoglobin, another oxygen-binding protein found in red blood cells. Myoglobin's primary function is to store oxygen within the muscle cells, making it readily available for use during periods of increased oxygen demand, such as during physical exertion.
Myoglobin contains heme groups that bind to and release oxygen molecules. The protein has a higher affinity for oxygen than hemoglobin, allowing it to maintain its bound oxygen even in low-oxygen environments. When muscle cells are damaged or undergo necrosis (cell death), myoglobin is released into the bloodstream and can be detected in serum or urine samples. Elevated levels of myoglobin in the blood or urine may indicate muscle injury, trauma, or diseases affecting muscle integrity, such as rhabdomyolysis or muscular dystrophies.
Creatine kinase (CK) is a muscle enzyme that is normally present in small amounts in the blood. It is primarily found in tissues that require a lot of energy, such as the heart, brain, and skeletal muscles. When these tissues are damaged or injured, CK is released into the bloodstream, causing the levels to rise.
Creatine kinase exists in several forms, known as isoenzymes, which can be measured in the blood to help identify the location of tissue damage. The three main isoenzymes are:
1. CK-MM: Found primarily in skeletal muscle
2. CK-MB: Found primarily in heart muscle
3. CK-BB: Found primarily in the brain
Elevated levels of creatine kinase, particularly CK-MB, can indicate damage to the heart muscle, such as occurs with a heart attack. Similarly, elevated levels of CK-BB may suggest brain injury or disease. Overall, measuring creatine kinase levels is a useful diagnostic tool for assessing tissue damage and determining the severity of injuries or illnesses.
 Myoglobinuria
Myoglobinuria
Lactate dehydrogenase
Exercise intolerance
List of OMIM disorder codes
Statin
Hitting the wall
Second wind
LPIN1
Lactate dehydrogenase A
Carnitine palmitoyltransferase II deficiency
Rhabdomyolysis
Urinalysis
Microhematuria
Microwave burn
AMP deaminase
Cytochrome c oxidase subunit I
Carnitine palmitoyltransferase II
Cytochrome c oxidase subunit III
Nutritional muscular dystrophy
Equine exertional rhabdomyolysis
Cocaine intoxication
Urine test strip
Snakebites in Latin America
Hemoglobinuria
Yellow-bellied sea snake
Dystrophinopathy
MT-CYB
Atorvastatin
Chromopertubation
UQCRB
Myoglobinuria - Wikipedia
 Myoglobinuria Differential Diagnoses
Myoglobinuria Differential Diagnoses
Myoglobinuria Differential Diagnoses
 Tularemia | Tick-borne Diseases | Ticks | CDC
Tularemia | Tick-borne Diseases | Ticks | CDC
Mutations in LPIN1 Cause Recurrent Acute Myoglobinuria in Childhood<...
Recurrent myoglobinuria in a sporadic patient with a novel mitochondrial DNA tRNA<sup>Ile</sup>...
 Acute tubular necrosis: Video, Anatomy & Definition | Osmosis
Acute tubular necrosis: Video, Anatomy & Definition | Osmosis
 Myopathy with deficiency of iron-sulfur cluster assembly enzyme: MedlinePlus Genetics
Myopathy with deficiency of iron-sulfur cluster assembly enzyme: MedlinePlus Genetics
 Management of Acute Compartment Syndrome : JAAOS - Journal of the American Academy of Orthopaedic Surgeons
Management of Acute Compartment Syndrome : JAAOS - Journal of the American Academy of Orthopaedic Surgeons
Carnitine Deficiency Follow-up: Further Outpatient Care, Further Inpatient Care, Inpatient & Outpatient Medications
Search Results | AVMA
Community-Acquired Pneumonia (CAP): Practice Essentials, Overview, Etiology of Community-Acquired Pneumonia
Toluene | Medical Management Guidelines | Toxic Substance Portal | ATSDR
 Geodon (Ziprasidone): Uses, Dosage, Side Effects, Interactions, Warning
Geodon (Ziprasidone): Uses, Dosage, Side Effects, Interactions, Warning
 Brucine (PIM 082)
Brucine (PIM 082)
BCG Vaccine (Tice strain) (BCG vaccine live) dosing, indications, interactions, adverse effects, and more
Retrospective natural history of thymidine kinase 2 deficiency | Journal of Medical Genetics
Electrical Injuries: Engineering, Medical and Legal Aspects, Second Ed - Lawyers & Judges Publishing Company, Inc.
 DailyMed - HALOPERIDOL DECANOATE injection
DailyMed - HALOPERIDOL DECANOATE injection
 Lilla urinpose-syndrom | Tidsskrift for Den norske legeforening
Lilla urinpose-syndrom | Tidsskrift for Den norske legeforening
 Help, There is Blood In My Dog's Urine! - SitStay
Help, There is Blood In My Dog's Urine! - SitStay
 Avian astrovirus | PPT
Avian astrovirus | PPT
 Bath Salts - Special Subjects - Merck Manuals Consumer Version
Bath Salts - Special Subjects - Merck Manuals Consumer Version
 Update: Exertional Rhabdomyolysis, Active Component, U.S. Armed Forces, 2015-2019 | Health.mil
Update: Exertional Rhabdomyolysis, Active Component, U.S. Armed Forces, 2015-2019 | Health.mil
Update: Exertional Rhabdomyolysis, Active Component, U.S. Armed Forces, 2016-2020 | Health.mil
Rhabdomyolysis7
- Myoglobinuria is the presence of myoglobin in the urine, which usually results from rhabdomyolysis or muscle injury. (wikipedia.org)
- Hospitalization and IV hydration should be the first step in any patient suspected of having myoglobinuria or rhabdomyolysis. (wikipedia.org)
- Myoglobinuria is usually the result of rhabdomyolysis or muscle destruction. (wikipedia.org)
- The characteristic triad of rhabdomyolysis includes weakness, myalgias, and red to brown urine (due to myoglobinuria) accompanied by an elevated serum concentration of creatine kinase. (health.mil)
- Additional signs may include elevated creatine phosphokinase, myoglobinuria (rhabdomyolysis), and acute renal failure. (druglib.com)
- Myopathy sometimes takes the form of rhabdomyolysis with or without acute renal failure secondary to myoglobinuria, and rare fatalities have occurred. (tevapharm.com)
- Common adverse reactions include rhabdomyolysis with myoglobinuria , acute renal failure , myopathy (including myositis ) and liver enzyme abnormalities. (wikidoc.org)
Urine7
- After centrifuging, the urine of myoglobinuria is red, where the urine of hemoglobinuria after centrifuge is pink to clear. (wikipedia.org)
- The destruction of muscle tissue releases a protein called myoglobin, which is processed by the kidneys and released in the urine (myoglobinuria). (medlineplus.gov)
- The extreme symptom of this metabolic crisis is Myoglobinuria (3) which is the breakdown of muscle tissue to such an extent that it can be measured in the urine. (fodsupport.org)
- Urine and blood testing revealed myoglobinuria, leukocytosis and elevated levels of creatine kinase (129,250 IU/L) and myoglobin (15,450 ng/mL). (bmj.com)
- This disease causes exercise intolerance, cramps, muscle pain and, sometimes, myoglobinuria (acute muscle breakdown leading to rust-colored urine). (mda.org)
- At elevated levels, monensin can be toxic to cattle and can cause colic-like symptoms, hypokalemia (low potassium), myoglobinuria (breakdown of muscle in the urine), chronic cardiovascular issues, and possible death. (fda.gov)
- Dark brown urine suggests myoglobinuria. (msdmanuals.com)
Recurrent4
- Kilfoyle D, Hutchinson D, Potter H, George P. Recurrent myoglobinuria due to carnitine palmitoyltransferase II deficiency: clinical, biochemical, and genetic features of adult-onset cases. (medscape.com)
- Recurrent episodes of life-threatening myoglobinuria in childhood are caused by inborn errors of glycogenolysis, mitochondrial fatty acid beta-oxidation, and oxidative phosphorylation. (huji.ac.il)
- This novel mutation has to be added to the molecular causes of recurrent myoglobinuria. (elsevierpure.com)
- 1993). Identification of a common mutation in the carnitine palmitoyltransferase II gene in familial recurrent myoglobinuria patients. (cincinnatichildrens.org)
Hemoglobinuria2
- Trivedi DJ, Kulkarni SP, Mudaraddi R. Primary Myoglobinuria: Differentiate Myoglobinuria from Hemoglobinuria. (medscape.com)
- Hemoglobinuria and myoglobinuria are also possible. (sitstay.com)
Haemoglobinuria1
- There was no sign of transfusion reaction, haemoglobinuria, myoglobinuria or bilirubinuria. (tidsskriftet.no)
Carnitine1
- Other causes of myoglobinuria include: McArdle's disease Phosphofructokinase deficiency Carnitine palmitoyltransferase II deficiency Malignant hyperthermia Polymyositis Lactate dehydrogenase deficiency Adenosine monophosphate deaminase deficiency type 1 Thermal or electrical burn Muscular dystrophy Myoglobinuria pathophysiology consists of a series of metabolic actions in which damage to muscle cells affect calcium mechanisms, thereby increasing free ionized calcium in the cytoplasm of the myocytes (concurrently decreasing free ionized calcium in the bloodstream). (wikipedia.org)
Metabolic1
- Metabolic Myoglobinuria. (medscape.com)
Tubular1
- His heart had multiple microscopic foci of myocardial necrosis, and his kidney had pink tubular casts consistent with myoglobinuria. (cdc.gov)
Clinical2
- Signs and symptoms of myoglobinuria are usually nonspecific and needs some clinical prudence. (wikipedia.org)
- Ceravolo F, Messina S, Rodolico C, Strisciuglio P, Concolino D. Myoglobinuria as first clinical sign of a primary alpha-sarcoglycanopathy. (medscape.com)
Mutations2
- Primary respiratory chain dysfunction is a rare cause of myoglobinuria, but it has been described in sporadic cases with mutations in genes encoding cytochrome b or cytochrome c oxidase (COX) subunits and in four cases with tRNA mutations. (elsevierpure.com)
- Mutations in this gene have been linked to exertional myoglobinuria. (origene.com)
Trauma1
- If your dog has had strenuous exercise, prolonged seizures, or trauma, he may have myoglobinuria due to the break down of muscle. (sitstay.com)
Patients1
- Cette étude a permis de déterminer la fréquence et l'étiologie de l'insuffisance rénale aiguë chez des patients hospitalisés en Arabie saoudite sur une période de 2 ans. (who.int)
Myoglobin1
- Thus, the precipitation of myoglobin in the renal tubules with secondary obstruction, tubular toxicity, or both constitutes the primary causes for acute kidney injury during myoglobinuria. (medscape.com)
Renal4
- Recurrent acute renal failure with idiopathic paroxysmal myoglobinuria. (nih.gov)
- Myoglobinuria with acute renal failure in children. (nih.gov)
- Complications can include hyperkalemia , myoglobinuria, and renal failure . (logicalimages.com)
- Myoglobinuria and renal failure after status epilepticus. (derangedphysiology.com)
Exercise1
- Cramps or myoglobinuria usually occur when someone with exercise intolerance "overdoes it," and can happen during the overexertion or several hours afterward. (nih.gov)
Kidney2
Patients1
- Nous n'avons relevé aucune différence significative en termes de sensibilité, spécificité et précision entre les bandelettes urinaires et les dosages de la CPK sérique dans l'identification des patients présentant un risque d'insuffisance rénale aiguë. (who.int)
Muscle damage1
- Electric shock can cause enough muscle damage to precipitate myoglobinuria. (medscape.com)
Case1
- An unusual case of gross myoglobinuria in a child following Russell's viper (Daboia russelii) envenomation. (medscape.com)