Osteitis Fibrosa Cystica
Renal Osteodystrophy
Osteomalacia
Hyperparathyroidism
Primary hyperparathyroidism: pathophysiology and impact on bone. (1/38)
Primary hyperparathyroidism has been associated with bone loss, especially at cortical skeletal sites. Results from studies evaluating the mineral density of cancellous bone have been more difficult to interpret. Most densitometry studies support the concept that the parathyroid hormone appears to be catabolic at cortical sites and may have anabolic effects at cancellous bone sites. Studies completed to date, however, have been limited by design, definitions of fracture and inadequate control groups. Primary hyperparathyroidism is now increasingly being detected during the asymptomatic phase. The need for parathyroidectomy has been questioned in such patients because there may be no disease progression in the absence of surgery. Medical management of primary hyperparathyroidism has to date been limited to estrogen replacement therapy in postmenopausal women. Identification of the calcium receptor has improved our understanding of calcium homeostasis, and significant reductions in calcium receptor levels have been detected in parathyroid adenomas. Thus, a new class of therapeutics may include the calcimimetic agents. Bisphosphonates are also currently being evaluated with regard to their impact on fracture prevention and their beneficial effects on bone mineral density. (+info)Tracheobronchopathia osteoplastica: incidental finding at tracheal intubation. (2/38)
Subglottic papillomatous growths were observed on routine tracheal intubation for a scheduled colorectal procedure. Fibreoptic bronchoscopy revealed that the lesions extended down to the carina and into the main bronchi. The diagnosis of tracheobronchopathia osteoplastica was made after subsequent bronchoscopy and biopsy in the post-operative period. A brief review of this rare benign condition is given. (+info)Slipped epiphyses in renal osteodystrophy. (3/38)
Clinical, biochemical, roentgenological, and histological features of slipped epiphyses (epiphysiolysis) in 11 out of 112 children with renal osteodystrophy have been analysed. Characteristic age-related patterns of involvement of different epiphyses are described. Quantitative measurements of iliac bone histology, serum parathyroid hormone levels, and clinical history show the presence of more advanced osteitis fibrosa in children with epiphysiolysis than in those without. A good correlation was found between serum parathormone levels and osteoclastic resorption, endosteal fibrosis as well as osteoid. Histological studies show that the radiolucent zone between the epiphyseal ossification centre and the metaphysis in x-rays is not caused by accumulation of cartilage and chondro-osteoid (as usually found in vitamin D deficiency rickets) but by the accumulation of woven bone and/or fibrous tissue. The response to vitamin D therapy in most cases was good. Parathyroidectomy was required in only one case. (+info)Cytokine accumulation in osteitis fibrosa of renal osteodystrophy. (4/38)
Bone marrow fibrosis occurs in association with a number of pathological states. Despite the extensive fibrosis that sometimes characterizes renal osteodystrophy, little is known about the factors that contribute to marrow accumulation of fibrous tissue. Because circulating cytokines are elevated in uremia, possibly in response to elevated parathyroid hormone levels, we have examined bone biopsies from 21 patients with end-stage renal disease and secondary hyperparathyroidism. Bone sections were stained with antibodies to human interleukin-1alpha (IL-1alpha), IL-6, IL-11, tumor necrosis factor-alpha (TNF-alpha) and transforming growth factor-beta (TGF-beta) using an undecalcified plastic embedding method. Intense staining for IL-1alpha, IL-6, TNF-alpha and TGF-beta was evident within the fibrotic tissue of the bone marrow while minimal IL-11 was detected. The extent of cytokine deposition corresponded to the severity of fibrosis, suggesting their possible involvement in the local regulation of the fibrotic response. Because immunoreactive TGF-beta and IL-6 were also detected in osteoblasts and osteocytes, we conclude that selective cytokine accumulation may have a role in modulating bone and marrow cell function in parathyroid-mediated uremic bone disease. (+info)Parathyroid hormone-independent osteoclastic resorptive bone disease: a new variant of adynamic bone disease in haemodialysis patients. (5/38)
BACKGROUND: Osteitis fibrosa cystica (OFC) caused by secondary hyperparathyroidism is the pre-eminent form of uraemic osteodystrophy. In recent years, however, new bone abnormalities have been described. Among them adynamic bone disease (ABD) has become a focus of growing interest. Marked suppression of dynamic bone measurements with normal or near-normal static bone-forming parameters are the hallmarks of this disorder. Depressed parathyroid hormone (PTH) levels, frequently evident in this entity, have been linked causally with low bone turnover. METHODS: We reviewed bone biopsy specimens from 96 patients with end-stage renal disease undergoing chronic haemodialysis. RESULTS: We found OFC in 50% of our patients, 20% had mixed bone disease, 24% showed bone morphology of ABD and a minority (6%) had osteomalacia, mostly due to aluminium accumulation. In the patients that were affected by ABD there was a distinct subgroup with bone morphology featuring a striking increase in osteoclast number and osteoclast surface, whereas the osteoid volume, osteoid thickness, osteoblast surface, tetracycline uptake and bone formation rates were diminished as in ordinary ABD. Similarly the PTH levels in this subgroup were low or undetectable. CONCLUSION: We describe patients undergoing chronic haemodialysis with static and dynamic bone forming parameters, indistinguishable from that of ABD, but differing from the classic ABD by the presence of increased osteoclastic bone resorption. The suppressed PTH levels in this subgroup suggests that factors other than PTH activate osteoclasts in some patients on chronic haemodialysis. Uraemic cytokines and/or toxic metabolites, including beta-microglobulin, may be involved in this disorder. The precise nature of this bone abnormality remains to be defined by further studies. (+info)Quantitative observations on iliac bone marrow mast cells in chronic renal failure. (6/38)
Mast cells have been counted in sections of iliac bone from 61 control subjects at necropsy. Mast cells were found in all but three, and the range was 0-33-7, median 1-95 per mm2 marrow. The majority (82%) had less than 4-99 mast cells per mm2 marrow; in 37-7% there was less than 1 mast cell per mm2 marrow. In a group of 45 patients with chronic renal failure there was a significant increase in the numbers of mast cells (P less than 0-001) with a range of 0-96-55-63, median 9-55 per mm2 marrow. Mast cells were common in the areas of marrow fibrosis associated with osteitis fibrosa but this was not the sole cause of the increase since there was also an excess of mast cells in the non-fibrous parts of the marrow. There was a tendency towards greater numbers of mast cells in those cases with most marked osteitis fibrosa in association with the prominent marrow fibrosis, but there was no significant relationship between mast cell numbers and other features of oesteitis fibrosa such as the number of osteoclasts and the amount of woven bone formation. There was no relationship between the numbers of mast cells and the amounts of total bone, ostoid, percentage mineralization of cancellous bone, or the presence of osteomalacia. (+info)Technetium-99m-pyrophosphate kinetics and imaging in metabolic bone disease. (7/38)
A study was undertaken to investigate the behavior of 99mTc-Sn-pyrophosphate complex in metabolic bone disease. Of clinical importance was the generalized increased periarticular bone accumulation of the radiopharmaceutical in osteomalacia and in combined osteomalacia and osteitis fibrosa as found in patients with chronic renal failure. The pattern in primary hyperparathyroidism was variable. There was no correlation between the initial rates of accumulation of the radiophosphate complex or its bone to soft-tissue uptake ratio at 5 hr when compared with the degree of osteomalacia and osteitis fibrosa. It is postulated that the 99mTc-Sn-pyrophosphate complex has greater affinity for immature collagen than the crystal surface. (+info)Brown tumors mimicking bone metastases. (8/38)
Brown tumors are rare skeletal manifestations of hyperparathyroidism (HPT) that may mimic cancer metastasis. Here, we present a 52-year-old woman with HPT and multiple foci of technetium uptake due to brown tumors on bone scintigraphy. Screening tests were negative for cancer and serum parathormon (PTH) measurement; parathyroid ultrasonography and scintigraphy suggested HPT. A chief cell adenoma in right and hyperplasia in the left parathyroid glands were surgically removed after which hungry bone syndrome emerged. Biopsy of the femur lesion during an open reduction with fixation operation due to a fracture established the diagnosis of a brown tumor. Brown tumors are important to consider in the evaluation of patients presenting with multiple foci of uptake on bone scanning and without an established primary neoplasm. (+info)Osteitis fibrosa cystica is a medical condition that refers to the abnormal bone remodeling process characterized by increased bone resorption and formation, leading to bone thickening and weakening. It is also known as "von Recklinghausen's disease of bone" or "monostotic fibrous dysplasia."
This condition is typically caused by excessive production of parathyroid hormone (PTH) due to a benign or malignant tumor of the parathyroid gland, known as hyperparathyroidism. The overproduction of PTH leads to an imbalance in calcium and phosphorus metabolism, resulting in increased bone resorption and fibrous tissue deposition within the bone marrow.
The clinical features of osteitis fibrosa cystica include bone pain, fractures, bone deformities, and elevated levels of calcium and alkaline phosphatase in the blood. Radiographic findings may show characteristic "rugger jersey" or "salt and pepper" patterns of alternating areas of increased and decreased bone density.
Treatment typically involves surgical removal of the abnormal parathyroid gland tissue, followed by medical management to prevent further bone loss and promote healing.
Osteitis is a medical term that refers to the inflammation of bone tissue. It can occur as a result of various conditions, such as infection (osteomyelitis), trauma, or autoimmune disorders. The symptoms of osteitis may include pain, swelling, warmth, and redness in the affected area, as well as fever and general malaise. Treatment typically involves addressing the underlying cause of the inflammation, which may involve antibiotics for infection or anti-inflammatory medications for other causes. In some cases, surgery may be necessary to remove infected or damaged bone tissue.
Renal osteodystrophy is a bone disease that occurs in individuals with chronic kidney disease (CKD). It is characterized by abnormalities in the bones' structure and mineral composition due to disturbances in the metabolism of calcium, phosphorus, and vitamin D. These metabolic disturbances result from the kidneys' decreased ability to maintain balance in the levels of these minerals and hormones.
Renal osteodystrophy can manifest as several bone disorders, including:
1. Osteitis fibrosa cystica: Increased bone turnover due to excessive parathyroid hormone (PTH) production, leading to high levels of alkaline phosphatase and increased resorption of bones.
2. Adynamic bone disease: Decreased bone turnover due to reduced PTH levels, resulting in low bone formation rates and increased fracture risk.
3. Mixed uremic osteodystrophy: A combination of high and low bone turnover, with varying degrees of mineralization defects.
4. Osteomalacia: Defective mineralization of bones due to vitamin D deficiency or resistance, leading to soft and weak bones.
Symptoms of renal osteodystrophy may include bone pain, muscle weakness, fractures, deformities, and growth retardation in children. Diagnosis typically involves laboratory tests, imaging studies, and sometimes bone biopsies. Treatment focuses on correcting the metabolic imbalances through dietary modifications, medications (such as phosphate binders, vitamin D analogs, and calcimimetics), and addressing any secondary hyperparathyroidism if present.
Osteomalacia is a medical condition characterized by the softening of bones due to defective bone mineralization, resulting from inadequate vitamin D, phosphate, or calcium. It mainly affects adults and is different from rickets, which occurs in children. The primary symptom is bone pain, but muscle weakness can also occur. Prolonged osteomalacia may lead to skeletal deformities and an increased risk of fractures. Treatment typically involves supplementation with vitamin D, calcium, and sometimes phosphate.
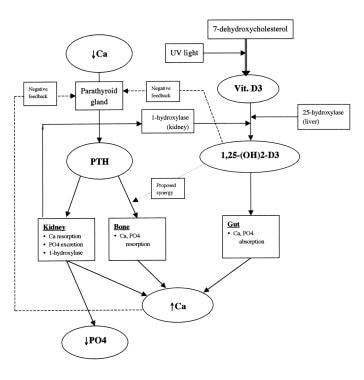
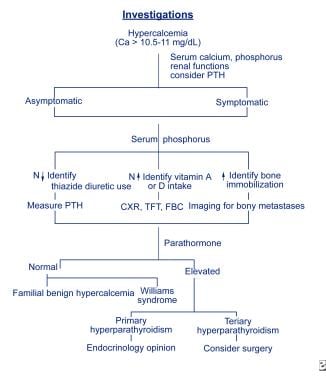
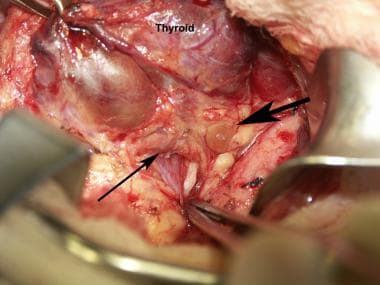
Hyperparathyroidism is a condition in which the parathyroid glands produce excessive amounts of parathyroid hormone (PTH). There are four small parathyroid glands located in the neck, near or within the thyroid gland. They release PTH into the bloodstream to help regulate the levels of calcium and phosphorus in the body.
In hyperparathyroidism, overproduction of PTH can lead to an imbalance in these minerals, causing high blood calcium levels (hypercalcemia) and low phosphate levels (hypophosphatemia). This can result in various symptoms such as fatigue, weakness, bone pain, kidney stones, and cognitive issues.
There are two types of hyperparathyroidism: primary and secondary. Primary hyperparathyroidism occurs when there is a problem with one or more of the parathyroid glands, causing them to become overactive and produce too much PTH. Secondary hyperparathyroidism develops as a response to low calcium levels in the body due to conditions like vitamin D deficiency, chronic kidney disease, or malabsorption syndromes.
Treatment for hyperparathyroidism depends on the underlying cause and severity of symptoms. In primary hyperparathyroidism, surgery to remove the overactive parathyroid gland(s) is often recommended. For secondary hyperparathyroidism, treating the underlying condition and managing calcium levels with medications or dietary changes may be sufficient.
 Osteitis fibrosa cystica
Osteitis fibrosa cystica Osteitis fibrosa: MedlinePlus Medical Encyclopedia
Osteitis fibrosa: MedlinePlus Medical Encyclopedia Secondary Hyperparathyroidism (SHPT) Imaging and Diagnosis: Practice Essentials, Radiography, Computed Tomography
Secondary Hyperparathyroidism (SHPT) Imaging and Diagnosis: Practice Essentials, Radiography, Computed Tomography Obesity Essay Topics For Free
Obesity Essay Topics For Free fibrosa - definition and meaning
fibrosa - definition and meaning McCune-Albright syndrome - Better Health Channel
McCune-Albright syndrome - Better Health Channel Shailendra B. Patel
Shailendra B. Patel head and neck, endocrine and breast Flashcards by Bryce Haac | Brainscape
head and neck, endocrine and breast Flashcards by Bryce Haac | Brainscape Brown Tumour in Chronic Kidney Disease: Revisiting an Old Disease with a New Perspective<...
Brown Tumour in Chronic Kidney Disease: Revisiting an Old Disease with a New Perspective<... Vincent Fong, MD,PhD | UC Health Provider Profile
Vincent Fong, MD,PhD | UC Health Provider Profile PPT - PARATHYROID GLAND PHYSIOLOGY PowerPoint presentation | free to download - id: 66e1d4-ZTdlM
PPT - PARATHYROID GLAND PHYSIOLOGY PowerPoint presentation | free to download - id: 66e1d4-ZTdlM Management challenges with brown tumor of primary hyperparathyroidism masked by severe vitamin D deficiency: a case report |...
Management challenges with brown tumor of primary hyperparathyroidism masked by severe vitamin D deficiency: a case report |... Hypocalcemia - Endocrine and Metabolic Disorders - MSD Manual Professional Edition
Hypocalcemia - Endocrine and Metabolic Disorders - MSD Manual Professional Edition Parathyroid Crisis as Presentation of Atypical Parathyroid Adenoma: Two Diagnostically Challenging Cases
Parathyroid Crisis as Presentation of Atypical Parathyroid Adenoma: Two Diagnostically Challenging Cases The Quizzes about Endocrinology disease - Part 1 (20 test) - MedQuizzes
The Quizzes about Endocrinology disease - Part 1 (20 test) - MedQuizzes Cancer Diagnosis & Prognosis
Cancer Diagnosis & Prognosis Pesquisa | Portal Regional da BVS
Pesquisa | Portal Regional da BVS Chau Vo | Harvard Catalyst Profiles | Harvard Catalyst
Chau Vo | Harvard Catalyst Profiles | Harvard Catalyst gland | Taber's Medical Dictionary
gland | Taber's Medical Dictionary