Pericardial Window Techniques
Skin Window Technique
Pericardial Effusion
Cardiac Tamponade
Pia Mater
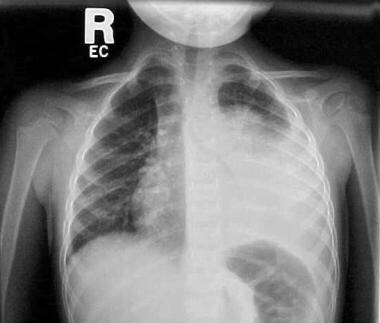
Occult cardiac lymphoma presenting with cardiac tamponade. (1/20)
Subxiphoid pericardiostomy is the procedure of choice for treatment of a pericardial effusion with tamponade. We report a case in which this procedure not only failed to reveal the presence of an occult malignancy, but also resulted in a recurrent symptomatic effusion. (+info)Thoracoscopic pericardial window creation and thoracic duct ligation in neonates. (2/20)
OBJECTIVE: We describe 2 newborn infants with persistent pericardial effusion treated with thoracoscopic pericardial window and thoracic duct ligation. METHODS: Patient 1 was a premature female newborn who presented with severe cardiac anomalies, including dextrocardia. She was treated with pulmonary artery handing and pacemaker placement for complete cardiac block. Postoperatively, she developed pericarditis with persistent symptomatic pericardial effusion. She did not improve despite pericardial drain placement. She was treated with a thoracoscopic pericardial window. Patient 2 was a newborn male who presented with cardiac tamponade secondary to congenital chylopericardium. He did not respond to pericardial drain placement or medical management with fasting, total parenteral nutrition, and octreotide. He was treated with thoracoscopic pericardial window and thoracic duct ligation. RESULTS: Patient 1 improved rapidly. The pericardial effusion disappeared. The chest tube was removed 5 days following surgery. She died 6 weeks later of a cardiac arrhythmia secondary to pacemaker failure. The pericardial effusion had resolved. Patient 2 responded to the pericardial window and thoracic duct ligation. He was discharged 10 days following the procedure. CONCLUSIONS: Thoracoscopy provides an excellent approach to the pericardium. Pericardial windows and biopsy can be safely performed with this approach. The thoracic duct can be easily identified and ligated even in small babies. Recovery can be fast with minimal postoperative discomfort. Cosmetic results are excellent and length of hospitalization is minimized. (+info)Subxiphoid pericardiostomy in the management of pericardial effusions: case series analysis of 368 patients. (3/20)
OBJECTIVE: To assess the effectiveness of subxiphoid pericardiostomy in the treatment and diagnosis of pericardial effusions. METHODS: 368 patients who underwent subxiphoid pericardiostomy and tube drainage for cardiac tamponade, moderate to severe pericardial effusion, or suspicious bacterial aetiology were retrospectively analysed. Biopsies of the pericardium and fluid samples for diagnostic tests were obtained from each patient. RESULTS: The mean age of the patients was 38.4 years, and the male to female ratio was 220:148. The pericardial effusion was classified by echocardiography as severe in 53% of the patients, moderate in 43%, and mild in 4%. The incidence of cardiac tamponade was 25%. Myocardial injury requiring sternotomy occurred as an operative complication in 0.8% of the patients and recurrent effusion necessitating further surgical intervention developed in 10% of patients. Histopathological examination and the polymerase chain reaction of specimens of pericardium and fluid were helpful for establishing a diagnosis in 90% of patients with malignancy and 92% of patients with tuberculous pericarditis. The overall 30 day mortality rate was 0.8%. Patients were followed up for at least one year. Pericardial constriction requiring pericardiectomy developed in 3% of the patients. CONCLUSIONS: Pericardial effusions of various causes can be safely, effectively, and quickly managed with subxiphoid pericardiostomy in both adults and children. (+info)Cardiac tamponade revisited: a postmortem look at a cautionary case. (4/20)
Cardiac tamponade is a life-threatening clinical syndrome that requires timely diagnosis. Herein, we present an instructive case of a patient who had cardiac tamponade. The condition went undiagnosed and resulted in the patient's death because almost all of the pathognomonic clinical findings of tamponade were unrecognized or not manifest. To better prepare health care professionals for similar challenges, we discuss the symptoms and clinical signs typical of cardiac tamponade, review the medical literature, and highlight current investigative methods that enable quick, efficient diagnosis and treatment. (+info)Bronchopericardial fistula, an unusual complication of oxytetracycline sclerosis therapy. (5/20)
Here we report a rare case of bronchopericardial fistula following intrapericardial instillation of oxytetracycline. A 63-year-old female patient was admitted for management of malignant pericardial effusion secondary to right-sided bronchogenic carcinoma. Medical therapy and recurrent percutaneous catheter drainage failed in resolving the problem, so subxiphoid pericardiostomy and drainage tube insertion was performed. There was no decrease in the drainage so we decided to perform pericardial sclerosis by intrapericardial tetracycline instillation. After the second time oxytetracycline instillation, the patient developed respiratory arrest with hemodynamic instability. A huge amount of yellow frothy secretion aspirated through the endotracheal tube. The presence of tetracycline in the bronchial secretion was proved by microbiological methods. The hemodynamic status of the patient deteriorated rapidly and despite all resuscitation measures we lost the patient within a few hours. (+info)Pericardial window used in the diagnosis of cardiac injury. (6/20)
PURPOSE: The purpose of the present study is to analyze the results of subxiphoid pericardial window (SPW) and transdiaphragmatic pericardial window (TDP) procedures comparing the two techniques. METHODS: During the period of January, 1994 to December, 2004, at UNICAMP, 245 patients underwent a pericardial window (PW) procedure to evaluate the possibility of cardiac injury. We reviewed the medical records of those patients in order to compare both procedures. RESULTS: Two hundred and seven patients (84.5%) underwent the SPW procedure, and 38 (15.5%) underwent the TDP procedure. Of the patients who underwent a SPW procedure, 151 (72.9%) had gunshots injuries, and 56 (27.1%) had stab wounds. In the group of patients submitted to TDP procedure, the wound was caused by gunshot in 26 (68.4%). The SPW method has shown a sensitivity of 97.5%, specificity of 95.8%, and an accuracy of 96.1%. The TDP method demonstrated a sensitivity of 100%, specificity of 97% and a 97.4% of accuracy rate. This review showed 8 (3.3%) false positive results. There was a single case (2.6%) of complications directly associated to the TDP, and this patient developed pericarditis. CONCLUSIONS: Both techniques presented an equally great result, with high sensitivity and specificity. Both surgical techniques must be carefully done to avoid false positive results. (+info)Cardiac tamponade as a sequela to ventriculoatrial shunting for congenital hydrocephalus. (7/20)
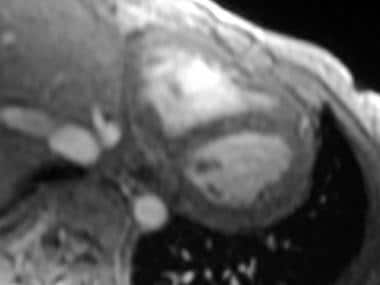
Cardiac tamponade is a life-threatening condition that demands prompt diagnosis and emergency intervention to prevent the sequelae of persistent low cardiac output, cardiopulmonary failure, and death. Cardiac tamponade due to pericardial collection of cerebrospinal fluid is a rare but recognized sequela associated with ventriculoatrial shunts used in the management of congenital hydrocephalus.Herein, we describe the treatment of an 8-month-old infant with multiple congenital anomalies who presented with cardiac tamponade. This condition was caused by cardiac perforation by the distal tip of a ventriculoatrial shunt catheter. Timely pericardiostomy and repair of the cardiac perforation through a left anterior thoracotomy resulted in an uneventful recovery. (+info)Iatrogenic intrapericardial diaphragmatic hernia diagnosed by cardiovascular magnetic resonance. (8/20)
(+info)A pericardial window technique is a surgical procedure that creates an opening or window in the pericardium, which is the sac-like membrane surrounding the heart. This procedure is typically performed to relieve excessive pressure on the heart caused by excess fluid accumulation in the pericardial space (pericardial effusion) or to obtain tissue samples for diagnostic purposes.
There are two primary approaches to creating a pericardial window:
1. Surgical Pericardial Window: This is an open surgical procedure, usually performed under general anesthesia. The surgeon makes an incision in the chest wall and then opens the pericardium to create a window. Excess fluid is drained from the pericardial space, and the pericardial edges are sutured together to keep the window open. This technique allows for continuous drainage of any future fluid accumulation.
2. Percutaneous Pericardial Window: This is a minimally invasive procedure that involves inserting a needle or catheter through the skin and into the pericardial space under local anesthesia and image guidance (fluoroscopy, echocardiography, or CT scan). A guidewire is then passed through the needle, followed by a dilator and sheath. A drainage catheter is placed through the sheath into the pericardial space to remove excess fluid. The catheter may be left in place for several days to allow for continued drainage.
Pericardial window techniques are used to treat various conditions, including cardiac tamponade (life-threatening compression of the heart due to pericardial effusion), infectious pericarditis, malignant pericardial effusions, and inflammatory disorders affecting the pericardium.
I'm sorry for any confusion, but "Skin Window Technique" is not a recognized or established term in medicine or dermatology. It may refer to a specific procedure or technique used in a particular study or clinical setting, but without more context, it's difficult to provide an accurate definition.
However, there is a similar term called "Skin as a Window Technique," which is a non-invasive method used in dermatology to evaluate the underlying structures and processes of the skin through transillumination or direct visualization. This technique can be used to diagnose various skin conditions such as hemangiomas, nevi, and other vascular anomalies.
Without more context, I cannot provide a precise definition of "Skin Window Technique." If you could provide more information about where you encountered this term or its intended meaning, I would be happy to try to help further.
Pericardial effusion is an abnormal accumulation of fluid in the pericardial space, which is the potential space between the two layers of the pericardium - the fibrous and serous layers. The pericardium is a sac that surrounds the heart to provide protection and lubrication for the heart's movement during each heartbeat. Normally, there is only a small amount of fluid (5-15 mL) in this space to ensure smooth motion of the heart. However, when an excessive amount of fluid accumulates, it can cause increased pressure on the heart, leading to various complications such as decreased cardiac output and even cardiac tamponade, a life-threatening condition that requires immediate medical attention.
Pericardial effusion may result from several causes, including infections (viral, bacterial, or fungal), inflammatory conditions (such as rheumatoid arthritis, lupus, or cancer), trauma, heart surgery, kidney failure, or iatrogenic causes. The symptoms of pericardial effusion can vary depending on the rate and amount of fluid accumulation. Slowly developing effusions may not cause any symptoms, while rapid accumulations can lead to chest pain, shortness of breath, cough, palpitations, or even hypotension (low blood pressure). Diagnosis is usually confirmed through imaging techniques such as echocardiography, CT scan, or MRI. Treatment depends on the underlying cause and severity of the effusion, ranging from close monitoring to drainage procedures or medications to address the root cause.
Cardiac tamponade is a serious medical condition that occurs when there is excessive fluid or blood accumulation in the pericardial sac, which surrounds the heart. This accumulation puts pressure on the heart, preventing it from filling properly and reducing its ability to pump blood effectively. As a result, cardiac output decreases, leading to symptoms such as low blood pressure, shortness of breath, chest pain, and a rapid pulse. If left untreated, cardiac tamponade can be life-threatening, requiring emergency medical intervention to drain the fluid and relieve the pressure on the heart.
Pia Mater is the inner-most layer of the meninges, which are the protective coverings of the brain and spinal cord. It is a very thin and highly vascularized (rich in blood vessels) membrane that closely adheres to the surface of the brain. The name "Pia Mater" comes from Latin, meaning "tender mother." This layer provides nutrition and protection to the brain, and it also allows for the movement and flexibility of the brain within the skull.
Arterioles are small branches of arteries that play a crucial role in regulating blood flow and blood pressure within the body's circulatory system. They are the smallest type of blood vessels that have muscular walls, which allow them to contract or dilate in response to various physiological signals.
Arterioles receive blood from upstream arteries and deliver it to downstream capillaries, where the exchange of oxygen, nutrients, and waste products occurs between the blood and surrounding tissues. The contraction of arteriolar muscles can reduce the diameter of these vessels, causing increased resistance to blood flow and leading to a rise in blood pressure upstream. Conversely, dilation of arterioles reduces resistance and allows for greater blood flow at a lower pressure.
The regulation of arteriolar tone is primarily controlled by the autonomic nervous system, local metabolic factors, and various hormones. This fine-tuning of arteriolar diameter enables the body to maintain adequate blood perfusion to vital organs while also controlling overall blood pressure and distribution.
 Pericardial window
Pericardial window