Post-Dural Puncture Headache
Blood Patch, Epidural
Spinal Puncture
Headache
Dura Mater
Analgesia, Epidural
Anesthesia, Obstetrical
Punctures
Analgesia, Obstetrical
Headache Disorders
Diagnostic lumbar puncture. Comparative study between 22-gauge pencil point and sharp bevel needle. (1/32)
Post-lumbar puncture headache is a frequent clinical problem. Needle design is expected to reduce post-puncture headache. In this study, we compared two different lumbar puncture needle designs in diagnostic lumbar puncture and analysed post-dural puncture headache (PDPH) and social and economical harm associated with the diagnostic lumbar puncture procedure. This prospective, controlled study consisted of 80 consecutive adult patients requiring elective diagnostic lumbar puncture due to various neurological symptoms. Lumbar puncture was completed either with Spinocan 22 G sharp bevel needle or Whitacre 22G pencil point needle. Patients were asked about previous headache symptoms and pain provoked by puncture. One week after the lumbar puncture all patients were interviewed by telephone and occurrence and type of headache, headache intensity, medication and frequency of impairment in activities of daily living were asked. Need for epidural blood patch was also recorded. Thirty-three of 78 (42%) patients experienced headache after diagnostic lumbar puncture and in 26 (33%) the headache could be classified as PDPH. There were no statistically significant differences between needle types in the frequency of common headache, PDPH, puncture pain intensity, need for epidural blood patch or sick leave. Also, there were no other complications except local back pain or headache. In this study, the needle design did not affect the frequency of PDPH. Also, PDPH was common, occurring in 33% cases and caused a considerable amount of disturbance in daily activities. Seeking help for this condition was insufficient and only part of these PDPH patients were treated with epidural blood patch. (+info)Gender and post-dural puncture headache. (2/32)
Gender is believed to be an independent risk factor for the development of post-dural puncture headache, but there are some of the inconsistencies in the available data. This systematic review examined a total of 18 trials (2,163 males, 1,917 females). The odds of developing a post-dural puncture headache were significantly lower for male than nonpregnant female subjects (odds ratio = 0.55; 95% confidence interval, 0.44-0.67). Although the authors found that nonpregnant female subjects seem to have a higher incidence of post-dural puncture headache than males, the etiology behind these findings is not clear from the current meta-analysis. (+info)Post lumbar puncture headache: diagnosis and management. (3/32)
Lumbar puncture is a frequently performed procedure in medical emergencies and anaesthesia. Headache after lumbar puncture is a common occurrence (32%) and carries a considerable morbidity, with symptoms lasting for several days, at times severe enough to immobilize the patient. If untreated, it can result in serious complications such as subdural haematoma and seizures, which could be fatal. Certain factors contribute to the development of headache after lumbar puncture. If these factors are taken into consideration, the incidence of headache could be markedly reduced. It is therefore important that the doctors are aware of the methods available for reducing the incidence of headaches after lumbar puncture. On the other hand, there are several misconceptions that are thought to decrease the incidence of headaches with no scientific basis. This article reviews the scientific literature and highlights the practical issues involved in the diagnosis and management of headaches after lumbar puncture, including the epidural blood patch treatment. (+info)Non-surgical management of intracranial subdural hematoma complicating spinal anesthesia. (4/32)
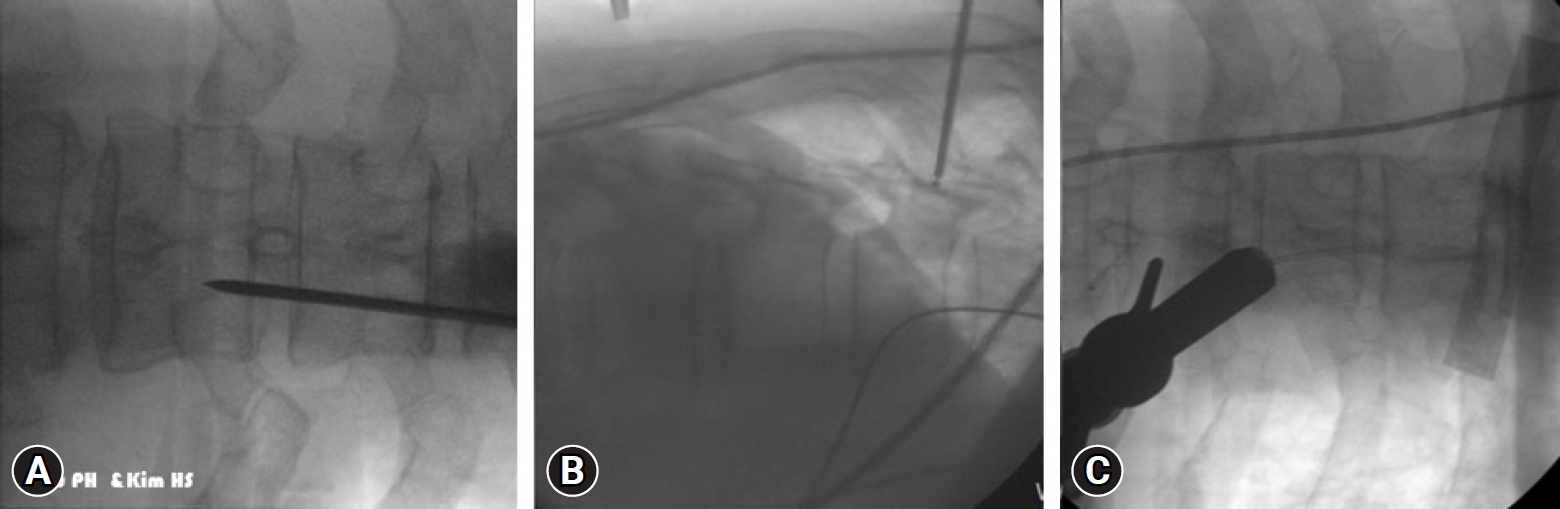
We report the case of a 29 year-old woman who presented a symptomatic intracranial subdural hematoma developing shortly after spinal anesthesia. The patient was fully conscious at clinical onset, and thus we treated her conservatively with an epidural autologous blood patch and close neurological observation. Given the clinical improvement the possibility of surgery was discauded in agreement with the neurosurgical team. Most cases of subdural hematoma appearing after spinal anesthesia are treated with surgery. In the present case the subdural hemorrhage was detected at our hospital 20 days after the anesthetic procedure, and given the excellent state of consciousness, we choosed a conservative management. (+info)Acute spinal pain during an attempted lumbar epidural blood patch in congenital lumbar spinal stenosis and epidural lipomatosis. (5/32)
Congenital lumbar spinal stenosis is an uncommon condition that is often asymptomatic in young adults. Herein, we document the first reported occurrence of acute radicular back pain and associated congenital lumbar spinal stenosis in a healthy 24-year-old woman undergoing an epidural blood patch for treatment of a post-dural puncture headache related to an accidental dural puncture sustained during placement of a labor epidural catheter. The acute pain symptoms were elicited twice with injection of less than 1 mL of fluid into the epidural space during the fluoroscopically assisted epidural blood patch. Subsequent magnetic resonance imaging of the lumbar spine demonstrated shortened pedicle length consistent with severe congenital lumbar spinal stenosis and prominent epidural fat. We speculate that the transient increase in pressure within the epidural compartment following injection of a small amount of fluid could have compressed neural structures resulting in severe radicular pain. The prominent epidural fat could have prevented rapid disbursement of the injected fluid which could have further served to propagate the pressure increase throughout the epidural compartment. The unique radiographic features of congenital spinal stenosis could predispose some patients with this unrecognized condition to develop acute pain upon injection of a small amount of fluid into the epidural compartment. Unrecognized congenital lumbar spinal stenosis is an important addition to the differential diagnosis of acute radicular pain elicited during an epidural blood patch in previously asymptomatic patients. (+info)Subdural hematoma following spinal cord stimulator implant. (6/32)
Headache following interventional procedures is a diagnostic challenge due to the multitude of possible etiologies involved. Presentation can be simple (PDPH alone) or complex (exacerbation of pre-existing chronic headache along with PDPH) or headache associated with a new onset intracranial process. Subdural hematoma is a rare complication of cranio-spinal trauma. Cranial subdural hematoma may present in an acute, sub-acute, or chronic fashion. Diagnosis of a subdural hematoma in the wake of a PDPH is difficult, requiring a high level of suspicion. Delayed diagnosis of subdural hematoma is usually related to failure to consider it in the differential diagnosis. Thorough history, assessment of the evolution of symptoms, and imaging studies may identify the possible cause and help direct treatment. Change in the character of initial presenting symptoms may be a sign of resolution of the headache or the onset of a secondary process. We report a case of acute intracranial subdural hematoma secondary to unintentional dural puncture during placement of a permanent spinal cord stimulator lead for refractory angina. There is need for careful follow-up of patients with a known post-dural tear. Failure to identify uncommon adverse events in patients with complicated spinal cord stimulator implantation may lead to permanent injury. (+info)Unusually early onset of post-dural puncture headache after spinal anaesthesia using a 27G Whittacre needle. (7/32)
(+info)Post-epidural headache: how late can it occur? (8/32)
(+info)Post-dural puncture headache (PDPH) is a type of headache that can occur following a procedure where the dura mater, the outer layer of the meninges that surrounds the brain and spinal cord, is punctured. This most commonly occurs during lumbar punctures (spinal taps), epidural anesthesia or central line placements.
The headache is typically described as a positional headache, meaning it worsens with sitting upright or standing and improves with lying down. The exact cause of PDPH is not fully understood, but it's thought to be due to the loss of cerebrospinal fluid (CSF) that cushions the brain and spinal cord. This leads to traction on pain-sensitive structures in the head and neck.
PDPH usually begins within 48 hours of the procedure, but can sometimes occur up to five days later. In addition to positional headache, symptoms may include nausea, vomiting, neck stiffness, photophobia (light sensitivity), tinnitus (ringing in the ears), and hearing loss. The headache usually resolves on its own within a few days or weeks, but in some cases, it can last for months or even become chronic. Treatment options include hydration, caffeine, analgesics, and in some refractory cases, an epidural blood patch.
A blood patch, epidural is a medical procedure used to treat a post-dural puncture headache (PDPH), which can occur after a lumbar puncture or spinal anesthesia. During the procedure, a small amount of the patient's own blood is withdrawn and injected into the epidural space, forming a clot that seals the dural tear and alleviates the headache.
The blood patch procedure involves several steps:
1. The patient is typically placed in a lateral decubitus position (lying on their side) to widen the intervertebral space.
2. The area is cleaned and prepared for the injection, similar to other sterile procedures.
3. Using a local anesthetic, the skin and underlying tissues are numbed to minimize discomfort during the procedure.
4. A thin needle is inserted into the epidural space, usually at the same level as the original dural puncture.
5. Once the needle is in the correct position, a small amount of blood (usually around 10-20 mL) is drawn from a vein in the patient's arm.
6. The withdrawn blood is then slowly injected into the epidural space through the needle.
7. After the injection, the needle is removed, and the patient is monitored for any adverse reactions or complications.
The clot formed by the injected blood helps to seal the dural tear, preventing cerebrospinal fluid (CSF) from leaking into the epidural space and causing a headache. The blood patch procedure typically provides rapid relief from PDPH, with most patients experiencing significant improvement within 30 minutes to an hour after the injection. However, in some cases, multiple blood patches may be required to achieve complete resolution of the headache.
A spinal puncture, also known as a lumbar puncture or a spinal tap, is a medical procedure in which a thin, hollow needle is inserted between two vertebrae in the lower back to extract cerebrospinal fluid (CSF) from the subarachnoid space. This procedure is typically performed to diagnose conditions affecting the central nervous system, such as meningitis, encephalitis, or subarachnoid hemorrhage, by analyzing the CSF for cells, chemicals, bacteria, or viruses. Additionally, spinal punctures can be used to administer medications or anesthetics directly into the CSF space, such as in the case of epidural anesthesia during childbirth.
The medical definition of a spinal puncture is: "A diagnostic and therapeutic procedure that involves introducing a thin needle into the subarachnoid space, typically at the lumbar level, to collect cerebrospinal fluid or administer medications."
A headache is defined as pain or discomfort in the head, scalp, or neck. It can be a symptom of various underlying conditions such as stress, sinus congestion, migraine, or more serious issues like meningitis or concussion. Headaches can vary in intensity, ranging from mild to severe, and may be accompanied by other symptoms such as nausea, vomiting, or sensitivity to light and sound. There are over 150 different types of headaches, including tension headaches, cluster headaches, and sinus headaches, each with their own specific characteristics and causes.
Dura Mater is the thickest and outermost of the three membranes (meninges) that cover the brain and spinal cord. It provides protection and support to these delicate structures. The other two layers are called the Arachnoid Mater and the Pia Mater, which are thinner and more delicate than the Dura Mater. Together, these three layers form a protective barrier around the central nervous system.
In the context of medicine, "needles" are thin, sharp, and typically hollow instruments used in various medical procedures to introduce or remove fluids from the body, administer medications, or perform diagnostic tests. They consist of a small-gauge metal tube with a sharp point on one end and a hub on the other, where a syringe is attached.
There are different types of needles, including:
1. Hypodermic needles: These are used for injections, such as intramuscular (IM), subcutaneous (SC), or intravenous (IV) injections, to deliver medications directly into the body. They come in various sizes and lengths depending on the type of injection and the patient's age and weight.
2. Blood collection needles: These are used for drawing blood samples for diagnostic tests. They have a special vacuum-assisted design that allows them to easily penetrate veins and collect the required amount of blood.
3. Surgical needles: These are used in surgeries for suturing (stitching) wounds or tissues together. They are typically curved and made from stainless steel, with a triangular or reverse cutting point to facilitate easy penetration through tissues.
4. Acupuncture needles: These are thin, solid needles used in traditional Chinese medicine for acupuncture therapy. They are inserted into specific points on the body to stimulate energy flow and promote healing.
It is essential to follow proper infection control procedures when handling and disposing of needles to prevent the spread of bloodborne pathogens and infectious diseases.
Spinal anesthesia is a type of regional anesthesia that involves injecting local anesthetic medication into the cerebrospinal fluid in the subarachnoid space, which is the space surrounding the spinal cord. This procedure is typically performed by introducing a needle into the lower back, between the vertebrae, to reach the subarachnoid space.
Once the local anesthetic is introduced into this space, it spreads to block nerve impulses from the corresponding levels of the spine, resulting in numbness and loss of sensation in specific areas of the body below the injection site. The extent and level of anesthesia depend on the amount and type of medication used, as well as the patient's individual response.
Spinal anesthesia is often used for surgeries involving the lower abdomen, pelvis, or lower extremities, such as cesarean sections, hernia repairs, hip replacements, and knee arthroscopies. It can also be utilized for procedures like epidural steroid injections to manage chronic pain conditions affecting the spine and lower limbs.
While spinal anesthesia provides effective pain relief during and after surgery, it may cause side effects such as low blood pressure, headache, or difficulty urinating. These potential complications should be discussed with the healthcare provider before deciding on this type of anesthesia.
Epidural analgesia is a type of regional anesthesia used to manage pain, most commonly during childbirth and after surgery. The term "epidural" refers to the location of the injection, which is in the epidural space of the spinal column.
In this procedure, a small amount of local anesthetic or narcotic medication is injected into the epidural space using a thin catheter. This medication blocks nerve impulses from the lower body, reducing or eliminating pain sensations without causing complete loss of feeling or muscle movement.
Epidural analgesia can be used for both short-term and long-term pain management. It is often preferred in situations where patients require prolonged pain relief, such as during labor and delivery or after major surgery. The medication can be administered continuously or intermittently, depending on the patient's needs and the type of procedure being performed.
While epidural analgesia is generally safe and effective, it can have side effects, including low blood pressure, headache, and difficulty urinating. In rare cases, it may also cause nerve damage or infection. Patients should discuss the risks and benefits of this procedure with their healthcare provider before deciding whether to undergo epidural analgesia.
Epidural anesthesia is a type of regional anesthesia that involves the injection of local anesthetic medication into the epidural space in the spine, which is the space surrounding the dura mater, a membrane that covers the spinal cord. The injection is typically administered through a catheter placed in the lower back using a needle.
The local anesthetic drug blocks nerve impulses from the affected area, numbing it and relieving pain. Epidural anesthesia can be used for various surgical procedures, such as cesarean sections, knee or hip replacements, and hernia repairs. It is also commonly used during childbirth to provide pain relief during labor and delivery.
The effects of epidural anesthesia can vary depending on the dose and type of medication used, as well as the individual's response to the drug. The anesthetic may take several minutes to start working, and its duration of action can range from a few hours to a day or more. Epidural anesthesia is generally considered safe when administered by trained medical professionals, but like any medical procedure, it carries some risks, including infection, bleeding, nerve damage, and respiratory depression.
Obstetrical anesthesia refers to the use of anesthetic techniques and medications during childbirth or obstetrical procedures. The goal is to provide pain relief and comfort to the birthing person while ensuring the safety of both the mother and the baby. There are different types of obstetrical anesthesia, including:
1. Local anesthesia: Injection of a local anesthetic agent to numb a specific area, such as the perineum (the area between the vagina and the anus) during childbirth.
2. Regional anesthesia: Numbing a larger region of the body using techniques like spinal or epidural anesthesia. These methods involve injecting local anesthetic agents near the spinal cord to block nerve impulses, providing pain relief in the lower half of the body.
3. General anesthesia: Using inhaled gases or intravenous medications to render the birthing person unconscious during cesarean sections (C-sections) or other surgical procedures related to childbirth.
The choice of anesthetic technique depends on various factors, including the type of delivery, the mother's medical history, and the preferences of both the mother and the healthcare team. Obstetrical anesthesia requires specialized training and expertise to ensure safe and effective pain management during labor and delivery.
A puncture, in medical terms, refers to a small hole or wound that is caused by a sharp object penetrating the skin or other body tissues. This can result in damage to underlying structures such as blood vessels, nerves, or organs, and may lead to complications such as bleeding, infection, or inflammation.
Punctures can occur accidentally, such as from stepping on a nail or getting pricked by a needle, or they can be inflicted intentionally, such as during medical procedures like injections or blood draws. In some cases, puncture wounds may require medical attention to clean and close the wound, prevent infection, and promote healing.
Obstetrical analgesia refers to the use of medications or techniques to relieve pain during childbirth. The goal of obstetrical analgesia is to provide comfort and relaxation for the mother during labor and delivery while minimizing risks to both the mother and the baby. There are several methods of obstetrical analgesia, including:
1. Systemic opioids: These medications, such as morphine or fentanyl, can be given intravenously to help reduce the pain of contractions. However, they can cause side effects such as drowsiness, nausea, and respiratory depression in the mother and may also affect the baby's breathing and alertness at birth.
2. Regional anesthesia: This involves numbing a specific area of the body using local anesthetics. The two most common types of regional anesthesia used during childbirth are epidural and spinal anesthesia.
a. Epidural anesthesia: A catheter is inserted into the lower back, near the spinal cord, to deliver a continuous infusion of local anesthetic and sometimes opioids. This numbs the lower half of the body, reducing the pain of contractions and allowing for a more comfortable delivery. Epidural anesthesia can also be used for cesarean sections.
b. Spinal anesthesia: A single injection of local anesthetic is given into the spinal fluid, numbing the lower half of the body. This type of anesthesia is often used for cesarean sections and can also be used for vaginal deliveries in some cases.
3. Nitrous oxide: Also known as laughing gas, this colorless, odorless gas can be inhaled through a mask to help reduce anxiety and provide some pain relief during labor. It is not commonly used in the United States but is more popular in other countries.
When choosing an obstetrical analgesia method, it's essential to consider the potential benefits and risks for both the mother and the baby. Factors such as the mother's health, the progression of labor, and personal preferences should all be taken into account when making this decision. It is crucial to discuss these options with a healthcare provider to determine the most appropriate choice for each individual situation.
Headache disorders refer to a group of conditions characterized by recurrent headaches that cause significant distress and impairment in daily functioning. The most common types of headache disorders are tension-type headaches, migraines, and cluster headaches.
Tension-type headaches are typically described as a dull, aching sensation around the head and neck, often accompanied by tightness or pressure. Migraines, on the other hand, are usually characterized by moderate to severe throbbing pain on one or both sides of the head, often accompanied by nausea, vomiting, sensitivity to light and sound, and visual disturbances.
Cluster headaches are relatively rare but extremely painful, with attacks lasting from 15 minutes to three hours and occurring several times a day for weeks or months. They typically affect one side of the head and are often accompanied by symptoms such as redness and tearing of the eye, nasal congestion, and sweating on the affected side of the face.
Headache disorders can have a significant impact on quality of life, and effective treatment often requires a multidisciplinary approach that may include medication, lifestyle changes, and behavioral therapies.
The epidural space is the potential space located outside the dura mater, which is the outermost of the three membranes covering the brain and spinal cord (the meninges). This space runs the entire length of the spinal canal and contains fatty tissue, blood vessels, and nerve roots. It is often used as a route for administering anesthesia during childbirth or surgery, as well as for pain management in certain medical conditions. The injection of medications into this space is called an epidural block.
 Post-dural-puncture headache
Post-dural-puncture headache Neostigmine and atropine as a treatment for Postdural Puncture Headache after spinal anesthesia in cesarean section: A Case...
Neostigmine and atropine as a treatment for Postdural Puncture Headache after spinal anesthesia in cesarean section: A Case... Management of post dural puncture headache Screening | Belfast Health & Social Care Trust website
Management of post dural puncture headache Screening | Belfast Health & Social Care Trust website Trans-nasal sphenopalatine ganglion block for post-dural puncture headache management: a meta-analysis of randomized trials |...
Trans-nasal sphenopalatine ganglion block for post-dural puncture headache management: a meta-analysis of randomized trials |... Treatment of post-dural puncture headache using epidural injection of fibrin sealant as an alternative to autologous epidural...
Treatment of post-dural puncture headache using epidural injection of fibrin sealant as an alternative to autologous epidural... Factors Predisposing to Postdural Puncture Headache after Spinal Anaesthesia among Elective Caesarean Section Patients at Thika...
Factors Predisposing to Postdural Puncture Headache after Spinal Anaesthesia among Elective Caesarean Section Patients at Thika... Obstetrics - ProProfs Quiz
Obstetrics - ProProfs Quiz Caffeine Uptake into the Vitreous after Peroral Coffee Consumption | Ophthalmic Research | Karger Publishers
Caffeine Uptake into the Vitreous after Peroral Coffee Consumption | Ophthalmic Research | Karger Publishers 5th ESRA Residents & Trainees Workshop - ESRA
5th ESRA Residents & Trainees Workshop - ESRA Randomised controlled trial of atraumatic versus standard needles for diagnostic lumbar puncture | The BMJ
Randomised controlled trial of atraumatic versus standard needles for diagnostic lumbar puncture | The BMJ Claes Möller - Institutionen för hälsovetenskaper - Örebro universitet
Claes Möller - Institutionen för hälsovetenskaper - Örebro universitet Magiran | جستجوی کلیدواژه «Orthopedics»
Magiran | جستجوی کلیدواژه «Orthopedics» LAVENDER: Overview, Uses, Side Effects, Precautions, Interactions, Dosing and Reviews
LAVENDER: Overview, Uses, Side Effects, Precautions, Interactions, Dosing and Reviews![がん情報サイト | がん情報各論:[医療専門家向け]Cancer Pain](data:image/png;base64,iVBORw0KGgoAAAANSUhEUgAAABAAAAAQCAYAAAAf8/9hAAAC0klEQVQ4jcWTzWscZQDGf+/7zuzMZPY72W6baEIlmGD8KkSKVK1FUfxCEKkHMZeCUBAvgr0pFUFPimChqAcpFIuKIHjxJkEvCmporajZbtpkTbr5aJLdnZ2dmfd9PRRs7x58/oAfv4eHB/7vCAC7MQ+N96H+FMQtKEwD+ERXXmZo/+dEjTV+OgGP/yiwqRUjh/4FOPZToPkReHtA+XfgFGeQwTy9xVkGa69hTR2neI77T99HvPQNjte2+g+EmrpuYK29brJ85hmyzpNEzZcQqonuj2D6dXLlayjRxyldoHrwBOVHF9AXrHDuAkByVEDryzKD9QNEjRfRnQCzM0PO1CkWoKgqVMMqo8MrFNrHMT/UEN0bFfjgq8Ok6w8jdo/hk8ctgOehXUWiLD2hGfJCHbjyXiF4AzG+ib16E0D4P5Mftih/HLF9EDfndLk21ehusBWlQJ7by5Nnfa/4ZhwX1wL/d6B6EyDsdAj3r2B7p1ATpwY6mWtuL41cjcOyNsJ6Koy2k8rfteyhrcBZzZFNJCjvxoxrSYOaWEXSA+dueWm3caux3pFuuv5qX+8ERXfP2Xxu9Ot99q8DCl1M4osf9itHcUUesEhho0A6h+SfAwukxtjB5cnS7JkhN/9K4OTPV/zRb8fy078txpeeWx6sDBaRuITerr5C32wiLsffP5aY6Alp3Y83k6WLY94scRbRzdYLFvN23qm9lZro6Yzuu54sPe/mTGCtOVJ0xt8zNi05EvlLZuOTme48W1B7Twaq/JkQIhHSxL1sc0tK7W9HG3dmxGaiMLY30qvvONJ1d/XytECeV3OvH44CVU5SE88Zmz2obTbf6v+6vBovmErulgcMSSvL5EKgStHAdqa6WfsRhA6VVEoK9xNZz81QdW/7IifDc8amtZ2kdTqUtWP3hHM5KUXbke6+kj+cIvR4O2oe7+ktT5M1AznyQtWZ/O4/v/EfNE86A/msCDkAAAAASUVORK5CYII=) がん情報サイト | がん情報各論:[医療専門家向け]Cancer Pain
がん情報サイト | がん情報各論:[医療専門家向け]Cancer Pain Meredith Barad, MD | Stanford Medicine
Meredith Barad, MD | Stanford Medicine Nate Mercaldo's Publications - MGH Institute for Technology Assessment
Nate Mercaldo's Publications - MGH Institute for Technology Assessment A-Z fact sheets | The Royal Women's Hospital
A-Z fact sheets | The Royal Women's Hospital Milestone Scientific Reports Ninth Published Study Reinforcing Efficacy of CompuFlo(R) Epidural Instrument as an Objective Tool...
Milestone Scientific Reports Ninth Published Study Reinforcing Efficacy of CompuFlo(R) Epidural Instrument as an Objective Tool... E-CONGRES ESRA
- Détails de l'Evenement
E-CONGRES ESRA
- Détails de l'Evenement
 Biologics
Biologics Journal of Anesthesia and Patient Care | Open Access Journal | Annex Publishers
Journal of Anesthesia and Patient Care | Open Access Journal | Annex Publishers