Rheumatic Diseases
Rheumatic Fever
Rheumatic Heart Disease
Arthritis, Rheumatoid
Lupus Erythematosus, Systemic
Spondylitis, Ankylosing
Rheumatology
Connective Tissue Diseases
Arthritis, Juvenile
Autoimmune Diseases
Arthritis
Rheumatic Nodule
Autoantibodies
Scleroderma, Systemic
Rheumatoid Factor
Sjogren's Syndrome
Arthritis, Psoriatic
Climatotherapy
Arthritis, Reactive
Antibodies, Antinuclear
Mixed Connective Tissue Disease
Gout
Osteoarthritis
Microscopic Angioscopy
Synovial Fluid
Portugal
Spondylarthropathies
Fibromyalgia
Vasculitis
Polymyalgia Rheumatica
HLA-B27 Antigen
Chorea
Polymyositis
Immunoglobulin G
MHC class II gene associations with autoantibodies to U1A and SmD1 proteins. (1/856)
Autoantibodies against U small nuclear ribonucleoproteins (snRNP) are frequently present in the serum of patients with systemic rheumatic diseases, and have been reported to be associated with HLA-DR and -DQ genes. To better define the role of HLA genes in the production of such antibodies, we studied immunogenetic associations with autoantibodies reacting with U1 RNP, U1A and SmD1 proteins, and synthetic peptides containing immunodominant linear epitopes of these proteins. Only two out of the 15 overlapping peptides of U1A (i.e. peptides 35-58 and 257-282) and three of 11 peptides of SmD1 (i.e. peptides 1-20, 44-67 and 97-119) were significantly recognized by patients' sera selected on the basis of their antibody positivity with RNP in immunodiffusion. The distribution of DRB1, DQB1 and DPB1 alleles among the anti-RNP antibody-positive patients (n = 28) and healthy control subjects was similar. Antibodies against U1A (tested in Western immunoblotting with HeLa cell extracts) were positively associated to DRB1*06 allele; antibodies reacting with SmD1 peptide 44-67 were negatively associated to DRB1*02 and DQB1*0602 alleles. No association was found between DPB1 alleles and antibodies reacting with U1A and SmD1 antigens. This first study reporting an association between autoantibodies reacting with U1A and SmD1 proteins (and peptides of these proteins), and immunogenetic markers suggest that the production of antibody subsets directed against different components (or regions of these proteins) bound to the same snRNP particle is associated with distinct MHC class II alleles. (+info)Cryoglobulinaemia and rheumatic manifestations in patients with hepatitis C virus infection. (2/856)
OBJECTIVES: To investigate the association of cryoglobulinaemia and rheumatic manifestations in Korean patients with hepatitis C virus (HCV) infection. METHODS: Forty nine Korean patients with HCV infection were recruited. The prevalence, concentration, and type of cryoglobulin (by immunofixation), rheumatoid factor (RF), antinuclear antibody (ANA), and various rheumatological symptoms were investigated and HCV genotype was determined by polymerase chain reaction with genotype specific primer. RESULTS: The prevalence of cryoglobulin was 59% in Korean HCV patients and the concentration of cryoglobulin was 9.8 (7.9) g/l (mean (SD)). The type of cryoglobulinaemia was identified in 23 (80%) of 29 HCV patients with cryoglobulinaemia and they were all type III. There were no differences in age, sex, history of operation and transfusion, proportion of liver cirrhosis between the patients with cryoglobulinaemia and those without cryoglobulinaemia. The frequencies of RF and ANA were 14% and 3.4% respectively in HCV patients with cryoglobulinaemia. There was no difference in HCV genotype between the patients with cryoglobulinaemia and those without cryoglobulinaemia. Clinical features of HCV patients were as follows: arthralgia/arthritis (35%), cutaneous manifestation (37%), Raynaud's phenomenon (8%), paresthesia (44%), dry eyes (22%), dry mouth (10%), oral ulcer (33%), and abdominal pain (14%). However, these rheumatological symptoms did not differ between the two groups. CONCLUSION: Although the rheumatological symptoms were not different between HCV patients with and without cryoglobulinaemia, HCV patients showed various rheumatological manifestations. These result suggests that HCV infection could be included as one of the causes in patients with unexplained rheumatological symptoms. (+info)Nuclear factor-kappa B activity in T cells from patients with rheumatic diseases: a preliminary report. (3/856)
OBJECTIVE: The NF-kappa B/Rel family of transcription factors regulates the expression of many genes involved in the immune or inflammatory response at the transcriptional level. The aim of this study was to determine whether distinctive patterns of NF-kappa B activation are seen in different forms of joint disease. METHODS: The DNA binding activity of these nucleoproteins was examined in purified synovial and peripheral T cells from patients with various chronic rheumatic diseases (12: four with rheumatoid arthritis; five with spondyloarthropathies; and three with osteoarthritis). RESULTS: Electrophoretic mobility shift assays disclosed two specific complexes bound to a NF-kappa B specific 32P-labelled oligonucleotide in nucleoproteins extracted from purified T cells isolated from synovial fluid and peripheral blood of patients with rheumatoid arthritis. The complexes consisted of p50/p50 homodimers and p50/p65 heterodimers. Increased NF-kappa B binding to DNA in synovial T cells was observed relative to peripheral T cells. In non-rheumatoid arthritis, binding of NF-kappa B in synovial T cells was exclusively mediated by p50/p50 homodimers. CONCLUSION: Overall, the results suggest that NF-kappa B may play a central part in the activation of infiltrating T cells in chronic rheumatoid arthritis. The activation of this nuclear factor is qualitatively different in rheumatoid synovial T cells to that in other forms of non-rheumatoid arthritis (for example, osteoarthritis, spondyloarthropathies). (+info)Inhibition of protein denaturation by fatty acids, bile salts and other natural substances: a new hypothesis for the mechanism of action of fish oil in rheumatic diseases. (4/856)
Natural hydrophobic substances like bile salts (cholate, deoxycholate, chenodeoxycholate, lithocholate and their conjugates with glycine and taurine), fatty acids (caprylic, capric, lauric, myristic, palmitic, stearic, oleic, linoleic, arachidonic, eicosapentaenoic and docosahexaenoic acid) were much more active (EC50 approximately 10(-4)-10(-5) M) than selected amino acids (EC50 > 10(-2) M) and inorganic salts (EC50 approximately 10(-1) M) in inhibiting heat-induced denaturation of human serum albumin in vitro. Fish oil, rich in n-3-polyunsaturated acids such as eicosapentaenoic acid and docosahexaenoic acid, administered p.o. (1 ml/kg) in the rat, protected ex vivo (after 2 hr) serum against heat-induced denaturation more than bendazac, a known antidenaturant drug. Thus, we speculated that the antidenaturant activity of fish oil may be partly (in addition to the known effect on endogenous eicosanoid composition) responsible for its beneficial effects in rheumatoid arthritis and other rheumatic conditions. In this connection, it is of note that the in vitro antidenaturant activity of fish oil fatty acids was higher than that of known antidenaturant drugs such as bendazac and bindarit and nonsteroidal anti-inflammatory drugs like phenylbutazone and indomethacin which could exert beneficial effects in chronic inflammatory conditions by stabilizing endogenous proteins. (+info)Rheumatic disease and the Australian aborigine. (5/856)
OBJECTIVE: To document the frequency and disease phenotype of various rheumatic diseases in the Australian Aborigine. METHODS: A comprehensive review was performed of the archaeological, ethnohistorical, and contemporary literature relating to rheumatic diseases in these indigenous people. RESULTS: No evidence was found to suggest that rheumatoid arthritis (RA), ankylosing spondylitis (AS), or gout occurred in Aborigines before or during the early stages of white settlement of Australia. Part of the explanation for the absence of these disorders in this indigenous group may relate to the scarcity of predisposing genetic elements, for example, shared rheumatoid epitope for RA, B27 antigen for AS. In contrast, osteoarthritis appeared to be common particularly involving the temporomandibular joint, right elbow and knees and, most probably, was related to excessive joint loading in their hunter gatherer lifestyle. Since white settlement, high frequency rates for rheumatic fever, systemic lupus erythematosus, and pyogenic arthritis have been observed and there are now scanty reports of the emergence of RA and gout in these original Australians. CONCLUSION: The occurrence and phenotype of various rheumatic disorders in Australian Aborigines is distinctive but with recent changes in diet, lifestyle, and continuing genetic admixture may be undergoing change. An examination of rheumatic diseases in Australian Aborigines and its changing phenotype may lead to a greater understanding of the aetiopathogenesis of these disorders. (+info)Impact of arthritis and other rheumatic conditions on the health-care system--United States, 1997. (6/856)
Arthritis and other rheumatic conditions are the leading cause of disability in the United States, affecting approximately 43 million persons and costing $65 billion in 1992. By 2020, these numbers will increase as the population ages. This report examines several measures of the impact of arthritis on the U.S. health-care system; the findings indicate that arthritis and other rheumatic conditions have a large impact on hospitalizations, ambulatory-care visits, and home health care, with women accounting for most of this impact and all persons aged <65 years accounting for a substantial portion. (+info)Economic comparison of nimesulide and diclofenac, and the incidence of adverse events in the treatment of rheumatic disease in Greece. (7/856)
In Greece a 15-day treatment of rheumatic disease with diclofenac costs 56% more than treatment with nimesulide. This is due to the lower incidence of gastrointestinal adverse events with nimesulide, and the absence of serious gastrointestinal complications leading to hospitalization, which more than offset the higher acquisition cost of nimesulide. The average saving by using nimesulide instead of diclofenac is about US$21 per patient for a 15-day treatment period. (+info)HLA-DRB1 genes in 5 rheumatic disease multi-case families. (8/856)
OBJECTIVE: To detect HLA-DRB1 (DR1-10) alleles in 5 families with multi-case rheumatic diseases, and to study the possible influence of DRB1 genes in the pathogenesis of rheumatic diseases. METHODS: Sequence-Specific Primer PCR (PCR-SSP) method was used to examine HLA-DRB1 alleles. Totally 36 members of 5 families and 166 healthy people were involved in this study. The results were assessed by Chi-square test. RESULTS: The HLA-DRB1 allele frequency in the patients and their relatives was similar. No significant difference was found. But DR4 allele frequency in the patients (90.9%) and their relatives (68%) was much higher than that in normal controls (16.8%) and the difference was statistically significant (P < 0.0001). In family 4, two RA patients have different DRB1 alleles, while in family 5, two patients have the same DRB1 alleles, one developed SLE and the other developed RA. CONCLUSIONS: DR4 is closely related to rheumatoid arthritis. The nelatives of RA patients may be at greater risk to develop RA than individuals without family history. Some patients had the same DRB1 allele but developed different rheumatic diseases. This suggested that there might be some common pathways in genetic predisposing of rheumatic diseases. On the other hand, only a few patients with the same DRB1 allele developed rheumatic diseases during their life, so other factors besides DRB1 gene might also be involved in the pathogenesis of rheumatic diseases. (+info)Rheumatic diseases are a group of disorders that cause pain, stiffness, and swelling in the joints, muscles, tendons, ligaments, or bones. They include conditions such as rheumatoid arthritis, osteoarthritis, systemic lupus erythematosus (SLE), gout, ankylosing spondylitis, psoriatic arthritis, and many others. These diseases can also affect other body systems including the skin, eyes, lungs, heart, kidneys, and nervous system. Rheumatic diseases are often chronic and may be progressive, meaning they can worsen over time. They can cause significant pain, disability, and reduced quality of life if not properly diagnosed and managed. The exact causes of rheumatic diseases are not fully understood, but genetics, environmental factors, and immune system dysfunction are believed to play a role in their development.
Rheumatic fever is a systemic inflammatory disease that may occur following an untreated Group A streptococcal infection, such as strep throat. It primarily affects children between the ages of 5 and 15, but it can occur at any age. The condition is characterized by inflammation in various parts of the body, including the heart (carditis), joints (arthritis), skin (erythema marginatum, subcutaneous nodules), and brain (Sydenham's chorea).
The onset of rheumatic fever usually occurs 2-4 weeks after a streptococcal infection. The exact cause of the immune system's overreaction leading to rheumatic fever is not fully understood, but it involves molecular mimicry between streptococcal antigens and host tissues.
The Jones Criteria are used to diagnose rheumatic fever, which include:
1. Evidence of a preceding streptococcal infection (e.g., positive throat culture or rapid strep test, elevated or rising anti-streptolysin O titer)
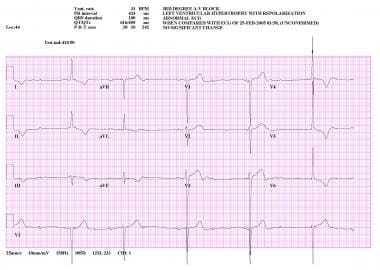
2. Carditis (heart inflammation), including new murmurs or changes in existing murmurs, electrocardiogram abnormalities, or evidence of heart failure
3. Polyarthritis (inflammation of multiple joints) – typically large joints like the knees and ankles, migratory, and may be associated with warmth, swelling, and pain
4. Erythema marginatum (a skin rash characterized by pink or red, irregularly shaped macules or rings that blanch in the center and spread outward)
5. Subcutaneous nodules (firm, round, mobile lumps under the skin, usually over bony prominences)
6. Sydenham's chorea (involuntary, rapid, irregular movements, often affecting the face, hands, and feet)
Treatment of rheumatic fever typically involves antibiotics to eliminate any residual streptococcal infection, anti-inflammatory medications like corticosteroids or nonsteroidal anti-inflammatory drugs (NSAIDs) to manage symptoms and prevent long-term heart complications, and secondary prophylaxis with regular antibiotic administration to prevent recurrent streptococcal infections.
Rheumatic Heart Disease (RHD) is defined as a chronic heart condition caused by damage to the heart valves due to untreated or inadequately treated streptococcal throat infection (strep throat). The immune system's response to this infection can mistakenly attack and damage the heart tissue, leading to inflammation and scarring of the heart valves. This damage can result in narrowing, leakage, or abnormal functioning of the heart valves, which can further lead to complications such as heart failure, stroke, or infective endocarditis.
RHD is a preventable and treatable condition if detected early and managed effectively. It primarily affects children and young adults in developing countries where access to healthcare and antibiotics for strep throat infections may be limited. Long-term management of RHD typically involves medications, regular monitoring, and sometimes surgical intervention to repair or replace damaged heart valves.
Rheumatoid arthritis (RA) is a systemic autoimmune disease that primarily affects the joints. It is characterized by persistent inflammation, synovial hyperplasia, and subsequent damage to the articular cartilage and bone. The immune system mistakenly attacks the body's own tissues, specifically targeting the synovial membrane lining the joint capsule. This results in swelling, pain, warmth, and stiffness in affected joints, often most severely in the hands and feet.
RA can also have extra-articular manifestations, affecting other organs such as the lungs, heart, skin, eyes, and blood vessels. The exact cause of RA remains unknown, but it is believed to involve a complex interplay between genetic susceptibility and environmental triggers. Early diagnosis and treatment are crucial in managing rheumatoid arthritis to prevent joint damage, disability, and systemic complications.
Systemic Lupus Erythematosus (SLE) is a complex autoimmune disease that can affect almost any organ or system in the body. In SLE, the immune system produces an exaggerated response, leading to the production of autoantibodies that attack the body's own cells and tissues, causing inflammation and damage. The symptoms and severity of SLE can vary widely from person to person, but common features include fatigue, joint pain, skin rashes (particularly a "butterfly" rash across the nose and cheeks), fever, hair loss, and sensitivity to sunlight.
Systemic lupus erythematosus can also affect the kidneys, heart, lungs, brain, blood vessels, and other organs, leading to a wide range of symptoms such as kidney dysfunction, chest pain, shortness of breath, seizures, and anemia. The exact cause of SLE is not fully understood, but it is believed to involve a combination of genetic, environmental, and hormonal factors. Treatment typically involves medications to suppress the immune system and manage symptoms, and may require long-term management by a team of healthcare professionals.
Ankylosing spondylitis is a type of inflammatory arthritis that primarily affects the spine, although other joints can also be involved. It causes swelling in the spinal joints (vertebrae) that can lead to stiffness and pain. Over time, some of these joints may grow together, causing new bone formation and resulting in a rigid spine. This fusion of the spine is called ankylosis.
The condition typically begins in the sacroiliac joints, where the spine connects to the pelvis. From there, it can spread up the spine and potentially involve other areas of the body such as the eyes, heart, lungs, and gastrointestinal system.
Ankylosing spondylitis has a strong genetic link, with most people carrying the HLA-B27 gene. However, not everyone with this gene will develop the condition. It primarily affects males more often than females and tends to start in early adulthood.
Treatment usually involves a combination of medication, physical therapy, and exercise to help manage pain, maintain mobility, and prevent deformity. In severe cases, surgery may be considered.
Rheumatology is a subspecialty of internal medicine that deals with the diagnosis and management of more than 200 diseases affecting the joints, muscles, and bones. These diseases are often complex, chronic, and systemic, meaning they can affect the whole body. Some common rheumatic diseases include rheumatoid arthritis, osteoarthritis, lupus, gout, osteoporosis, and various forms of vasculitis and connective tissue disorders.
Rheumatologists are medical doctors who have completed additional training in this field, becoming experts in the non-surgical treatment of musculoskeletal diseases. They use a combination of physical examination, patient history, laboratory testing, and imaging to diagnose and manage these conditions. Treatment may involve medications, lifestyle changes, physical therapy, or a combination of these approaches.
Connective tissue diseases (CTDs) are a group of disorders that involve the abnormal production and accumulation of abnormal connective tissues in various parts of the body. Connective tissues are the structural materials that support and bind other tissues and organs together. They include tendons, ligaments, cartilage, fat, and the material that fills the spaces between cells, called the extracellular matrix.
Connective tissue diseases can affect many different systems in the body, including the skin, joints, muscles, lungs, kidneys, gastrointestinal tract, and blood vessels. Some CTDs are autoimmune disorders, meaning that the immune system mistakenly attacks healthy connective tissues. Others may be caused by genetic mutations or environmental factors.
Some examples of connective tissue diseases include:
* Systemic lupus erythematosus (SLE)
* Rheumatoid arthritis (RA)
* Scleroderma
* Dermatomyositis/Polymyositis
* Mixed Connective Tissue Disease (MCTD)
* Sjogren's syndrome
* Ehlers-Danlos syndrome
* Marfan syndrome
* Osteogenesis imperfecta
The specific symptoms and treatment of connective tissue diseases vary depending on the type and severity of the condition. Treatment may include medications to reduce inflammation, suppress the immune system, or manage pain. In some cases, surgery may be necessary to repair or replace damaged tissues or organs.
Juvenile arthritis (JA) is a term used to describe a group of autoimmune and inflammatory disorders that can affect children aged 16 or younger. In JA, the immune system mistakenly attacks the body's own tissues, causing inflammation in the joints, which can lead to pain, swelling, stiffness, and damage over time.
There are several types of juvenile arthritis, including:
1. Juvenile Idiopathic Arthritis (JIA): This is the most common form of JA, and it includes several subtypes that are classified based on the number of joints affected and the presence or absence of certain symptoms.
2. Juvenile Systemic Lupus Erythematosus (JSLE): This is a type of lupus that affects children, and it can cause inflammation in various parts of the body, including the joints, skin, kidneys, and lungs.
3. Juvenile Dermatomyositis (JDM): This is a rare autoimmune disorder that causes inflammation of the blood vessels, leading to muscle weakness, skin rashes, and joint pain.
4. Juvenile Scleroderma: This is a group of disorders that cause hardening and tightening of the skin and connective tissues, which can also affect the joints.
5. Juvenile Psoriatic Arthritis (JPsA): This is a type of arthritis that affects children who have psoriasis, a chronic skin condition. JPsA can cause inflammation in the joints and skin.
The causes of juvenile arthritis are not fully understood, but it is believed to involve a combination of genetic and environmental factors. There is no cure for JA, but treatments such as medication, physical therapy, and lifestyle changes can help manage the symptoms and prevent long-term complications.
Autoimmune diseases are a group of disorders in which the immune system, which normally protects the body from foreign invaders like bacteria and viruses, mistakenly attacks the body's own cells and tissues. This results in inflammation and damage to various organs and tissues in the body.
In autoimmune diseases, the body produces autoantibodies that target its own proteins or cell receptors, leading to their destruction or malfunction. The exact cause of autoimmune diseases is not fully understood, but it is believed that a combination of genetic and environmental factors contribute to their development.
There are over 80 different types of autoimmune diseases, including rheumatoid arthritis, lupus, multiple sclerosis, type 1 diabetes, Hashimoto's thyroiditis, Graves' disease, psoriasis, and inflammatory bowel disease. Symptoms can vary widely depending on the specific autoimmune disease and the organs or tissues affected. Treatment typically involves managing symptoms and suppressing the immune system to prevent further damage.
Arthritis is a medical condition characterized by inflammation in one or more joints, leading to symptoms such as pain, stiffness, swelling, and reduced range of motion. There are many different types of arthritis, including osteoarthritis, rheumatoid arthritis, psoriatic arthritis, gout, and lupus, among others.
Osteoarthritis is the most common form of arthritis and is caused by wear and tear on the joints over time. Rheumatoid arthritis, on the other hand, is an autoimmune disorder in which the body's immune system mistakenly attacks the joint lining, causing inflammation and damage.
Arthritis can affect people of all ages, including children, although it is more common in older adults. Treatment for arthritis may include medications to manage pain and reduce inflammation, physical therapy, exercise, and in some cases, surgery.
Antirheumatic agents are a class of drugs used to treat rheumatoid arthritis, other inflammatory types of arthritis, and related conditions. These medications work by reducing inflammation in the body, relieving symptoms such as pain, swelling, and stiffness in the joints. They can also help slow down or prevent joint damage and disability caused by the disease.
There are several types of antirheumatic agents, including:
1. Nonsteroidal anti-inflammatory drugs (NSAIDs): These medications, such as ibuprofen and naproxen, reduce inflammation and relieve pain. They are often used to treat mild to moderate symptoms of arthritis.
2. Corticosteroids: These powerful anti-inflammatory drugs, such as prednisone and cortisone, can quickly reduce inflammation and suppress the immune system. They are usually used for short-term relief of severe symptoms or in combination with other antirheumatic agents.
3. Disease-modifying antirheumatic drugs (DMARDs): These medications, such as methotrexate and hydroxychloroquine, work by slowing down the progression of rheumatoid arthritis and preventing joint damage. They can take several weeks or months to become fully effective.
4. Biologic response modifiers (biologics): These are a newer class of DMARDs that target specific molecules involved in the immune response. They include drugs such as adalimumab, etanercept, and infliximab. Biologics are usually used in combination with other antirheumatic agents for patients who have not responded to traditional DMARD therapy.
5. Janus kinase (JAK) inhibitors: These medications, such as tofacitinib and baricitinib, work by blocking the action of enzymes called JAKs that are involved in the immune response. They are used to treat moderate to severe rheumatoid arthritis and can be used in combination with other antirheumatic agents.
It is important to note that antirheumatic agents can have significant side effects and should only be prescribed by a healthcare provider who is experienced in the management of rheumatoid arthritis. Regular monitoring and follow-up are essential to ensure safe and effective treatment.
A rheumatic nodule is not a specific medical definition, but rather a descriptive term for a type of nodule that can be found in certain medical conditions. These nodules are typically associated with rheumatoid arthritis (RA), although they can also occur in other diseases such as systemic lupus erythematosus (SLE) and dermatomyositis.
Rheumatic nodules are small, firm, round or oval-shaped lumps that develop under the skin or in certain organs such as the lungs. They can vary in size from a few millimeters to several centimeters in diameter. In RA, these nodules usually appear on the forearms, elbows, fingers, knees, and ankles, although they can occur in other areas of the body as well.
Histologically, rheumatic nodules are characterized by a central area of fibrinoid necrosis surrounded by palisading histiocytes and fibroblasts. They may also contain lymphocytes, plasma cells, and eosinophils. The presence of these nodules is thought to be related to the immune system's response to the underlying disease process, although their exact cause and significance are not fully understood.
It is important to note that rheumatic nodules can also occur in individuals without any known medical condition, and their presence does not necessarily indicate the presence of a specific disease. However, if you notice any new or unusual lumps or bumps on your body, it is always a good idea to consult with a healthcare professional for further evaluation and diagnosis.
Autoantibodies are defined as antibodies that are produced by the immune system and target the body's own cells, tissues, or organs. These antibodies mistakenly identify certain proteins or molecules in the body as foreign invaders and attack them, leading to an autoimmune response. Autoantibodies can be found in various autoimmune diseases such as rheumatoid arthritis, lupus, and thyroiditis. The presence of autoantibodies can also be used as a diagnostic marker for certain conditions.
Systemic Scleroderma, also known as Systemic Sclerosis (SSc), is a rare, chronic autoimmune disease that involves the abnormal growth and accumulation of collagen in various connective tissues, blood vessels, and organs throughout the body. This excessive collagen production leads to fibrosis or scarring, which can cause thickening, hardening, and tightening of the skin and damage to internal organs such as the heart, lungs, kidneys, and gastrointestinal tract.
Systemic Scleroderma is characterized by two main features: small blood vessel abnormalities (Raynaud's phenomenon) and fibrosis. The disease can be further classified into two subsets based on the extent of skin involvement: limited cutaneous systemic sclerosis (lcSSc) and diffuse cutaneous systemic sclerosis (dcSSc).
Limited cutaneous systemic sclerosis affects the skin distally, typically involving fingers, hands, forearms, feet, lower legs, and face. It is often associated with Raynaud's phenomenon, calcinosis, telangiectasias, and pulmonary arterial hypertension.
Diffuse cutaneous systemic sclerosis involves more extensive skin thickening and fibrosis that spreads proximally to affect the trunk, upper arms, thighs, and face. It is commonly associated with internal organ involvement, such as interstitial lung disease, heart disease, and kidney problems.
The exact cause of Systemic Scleroderma remains unknown; however, it is believed that genetic, environmental, and immunological factors contribute to its development. There is currently no cure for Systemic Scleroderma, but various treatments can help manage symptoms, slow disease progression, and improve quality of life.
Rheumatoid factor (RF) is an autoantibody, specifically an immunoglobulin M (IgM) antibody, that can be detected in the blood serum of some people with rheumatoid arthritis (RA), other inflammatory conditions, and infectious diseases. RF targets the Fc portion of IgG, leading to immune complex formation and subsequent inflammation, which contributes to the pathogenesis of RA. However, not all patients with RA test positive for RF, and its presence does not necessarily confirm a diagnosis of RA. Other conditions can also lead to elevated RF levels, such as infections, liver diseases, and certain malignancies. Therefore, the interpretation of RF results should be considered alongside other clinical, laboratory, and imaging findings for an accurate diagnosis and appropriate management.
Sjögren's syndrome is a chronic autoimmune disorder in which the body's immune system mistakenly attacks its own moisture-producing glands, particularly the tear and salivary glands. This can lead to symptoms such as dry eyes, dry mouth, and dryness in other areas of the body. In some cases, it may also affect other organs, leading to a variety of complications.
There are two types of Sjögren's syndrome: primary and secondary. Primary Sjögren's syndrome occurs when the condition develops on its own, while secondary Sjögren's syndrome occurs when it develops in conjunction with another autoimmune disease, such as rheumatoid arthritis or lupus.
The exact cause of Sjögren's syndrome is not fully understood, but it is believed to involve a combination of genetic and environmental factors. Treatment typically focuses on relieving symptoms and may include artificial tears, saliva substitutes, medications to stimulate saliva production, and immunosuppressive drugs in more severe cases.
Psoriatic arthritis is a form of inflammatory arthritis that occurs in some people with psoriasis, a skin condition characterized by scaly, red, and itchy patches. The Arthritis Foundation defines psoriatic arthritis as "a chronic disease characterized by swelling, pain, and stiffness in and around the joints. It usually affects the fingers and toes but can also affect the lower back, knees, ankles, and spine."
Psoriatic arthritis can cause a variety of symptoms, including:
* Joint pain, swelling, and stiffness
* Swollen fingers or toes (dactylitis)
* Tenderness, pain, and swelling where tendons and ligaments attach to bones (enthesitis)
* Changes in nail growth, such as pitting, ridging, or separation from the nail bed
* Fatigue and weakness
* Reduced range of motion and mobility
The exact cause of psoriatic arthritis is not fully understood, but it is believed to involve a combination of genetic, environmental, and immune system factors. Treatment typically involves a combination of medications, lifestyle changes, and physical therapy to manage symptoms and prevent joint damage.
Climatotherapy is a form of therapy that uses a specific climate or weather to treat various medical conditions. This type of therapy involves exposing the patient to a particular climate, such as high altitudes, dry heat, or cold temperatures, in order to achieve therapeutic benefits. The idea behind climatotherapy is that certain climates can have a positive impact on symptoms and overall health.
For example, people with respiratory conditions like asthma or chronic obstructive pulmonary disease (COPD) may benefit from living in a dry, desert climate, as the low humidity can help reduce inflammation and improve lung function. Similarly, those with rheumatoid arthritis or other joint diseases may find relief in warm, mineral-rich waters, such as those found in hot springs or spas.
Climatotherapy is often used as a complementary therapy alongside conventional medical treatments, and its effectiveness can vary depending on the individual and their specific medical condition. It's important to consult with a healthcare provider before starting any new treatment regimen, including climatotherapy.
Spondylitis is a term used to describe inflammation in the spinal vertebrae, often leading to stiffness and pain. The most common form is Ankylosing Spondylitis, which is a chronic autoimmune disease where the body's immune system mistakenly attacks the joints in the spine. This can cause the bones in the spine to grow together, resulting in a rigid and inflexible spine. Other forms of spondylitis include reactive spondylitis, infectious spondylitis, and seronegative spondyloarthropathies. Symptoms may also include pain and stiffness in the neck, lower back, hips, and small joints of the body.
Reactive arthritis is a form of inflammatory arthritis that occurs in response to an infection in another part of the body, such as the genitals, urinary tract, or gastrointestinal tract. It is also known as Reiter's syndrome. The symptoms of reactive arthritis include joint pain and swelling, typically affecting the knees, ankles, and feet; inflammation of the eyes, skin, and mucous membranes; and urethritis or cervicitis. It is more common in men than women and usually develops within 1-4 weeks after a bacterial infection. The diagnosis is made based on the symptoms, medical history, physical examination, and laboratory tests. Treatment typically includes antibiotics to eliminate the underlying infection and medications to manage the symptoms of arthritis.
Antinuclear antibodies (ANA) are a type of autoantibody that target structures found in the nucleus of a cell. These antibodies are produced by the immune system and attack the body's own cells and tissues, leading to inflammation and damage. The presence of ANA is often used as a marker for certain autoimmune diseases, such as systemic lupus erythematosus (SLE), Sjogren's syndrome, rheumatoid arthritis, scleroderma, and polymyositis.
ANA can be detected through a blood test called the antinuclear antibody test. A positive result indicates the presence of ANA in the blood, but it does not necessarily mean that a person has an autoimmune disease. Further testing is usually needed to confirm a diagnosis and determine the specific type of autoantibodies present.
It's important to note that ANA can also be found in healthy individuals, particularly as they age. Therefore, the test results should be interpreted in conjunction with other clinical findings and symptoms.
Mixed Connective Tissue Disease (MCTD) is a rare overlapping condition of the connective tissues, characterized by the presence of specific autoantibodies against a protein called "U1-snRNP" or "U1-small nuclear ribonucleoprotein." This disorder has features of various connective tissue diseases such as systemic lupus erythematosus (SLE), scleroderma, polymyositis, and rheumatoid arthritis. Symptoms may include swollen hands, joint pain and swelling, muscle weakness, skin thickening, lung involvement, and Raynaud's phenomenon. The exact cause of MCTD is unknown, but it is believed to involve both genetic and environmental factors leading to an autoimmune response. Early diagnosis and treatment are essential for better disease management and preventing severe complications.
Gout is a type of inflammatory arthritis that occurs when urate crystals accumulate in and around the joints, causing sudden attacks of severe pain, swelling, redness, and tenderness. Urate crystals can form when there are high levels of uric acid in the blood. Uric acid is a waste product that is produced when the body breaks down purines, substances that are found naturally in certain foods, such as steak, organ meats, and seafood. Other foods also promote higher levels of uric acid, such as alcoholic beverages, especially beer, and drinks sweetened with fruit sugar (fructose).
Normally, uric acid dissolves in the blood and passes through the kidneys and out of the body in urine. But sometimes either the body produces too much uric acid or the kidneys excrete too little uric acid. When this happens, uric acid can build up, forming sharp, needle-like urate crystals in a joint or surrounding tissue that cause pain, inflammation and swelling.
Gout most commonly affects the big toe but can also occur in any joint in the body. The symptoms of gout are often acute, occurring suddenly without warning and frequently at night. The attacks are characterized by a rapid onset of pain, swelling, warmth, and redness in the affected joint. An attack of gout can be so painful that it wakes you up from sleep.
Over time, gout can cause permanent damage to the joints and surrounding tissue, resulting in chronic arthritis. If left untreated, gout also can lead to an accumulation of uric acid crystals in the kidneys, which can result in kidney stones.
Osteoarthritis (OA) is a type of joint disease that is characterized by the breakdown and eventual loss of cartilage - the tissue that cushions the ends of bones where they meet in the joints. This breakdown can cause the bones to rub against each other, causing pain, stiffness, and loss of mobility. OA can occur in any joint, but it most commonly affects the hands, knees, hips, and spine. It is often associated with aging and can be caused or worsened by obesity, injury, or overuse.
The medical definition of osteoarthritis is: "a degenerative, non-inflammatory joint disease characterized by the loss of articular cartilage, bone remodeling, and the formation of osteophytes (bone spurs). It is often associated with pain, stiffness, and decreased range of motion in the affected joint."
Microscopic angioscopy is not a widely recognized or established medical term. However, based on the individual terms, it can be interpreted as the use of a microscope with an angioscope (a type of endoscope used for visualizing the interior of blood vessels) to examine the microscopic structures of the inner walls of blood vessels. This technique would allow for detailed examination of the vasculature at a cellular level, potentially providing valuable information for research and diagnosis of various vascular diseases. However, as this is not a standard medical procedure or term, it's essential to consult the relevant literature or experts in the field for more precise information.
Synovial fluid is a viscous, clear, and straw-colored fluid found in the cavities of synovial joints, bursae, and tendon sheaths. It is produced by the synovial membrane, which lines the inner surface of the capsule surrounding these structures.
The primary function of synovial fluid is to reduce friction between articulating surfaces, providing lubrication for smooth and painless movement. It also acts as a shock absorber, protecting the joints from external forces during physical activities. Synovial fluid contains nutrients that nourish the articular cartilage, hyaluronic acid, which provides its viscoelastic properties, and lubricin, a protein responsible for boundary lubrication.
Abnormalities in synovial fluid composition or volume can indicate joint-related disorders, such as osteoarthritis, rheumatoid arthritis, gout, infection, or trauma. Analysis of synovial fluid is often used diagnostically to determine the underlying cause of joint pain, inflammation, or dysfunction.
I'm sorry for any confusion, but "Portugal" is not a medical term. It is a country located in southwestern Europe, known officially as the Portuguese Republic. If you have any questions about medical terminology or health-related topics, I would be happy to help!
Spondylarthropathies is a term used to describe a group of interrelated inflammatory diseases that primarily affect the joints of the spine (vertebral column) and the sites where the ligaments and tendons attach to the bones (entheses). These conditions also often have associations with extra-articular features, such as skin, eye, and intestinal manifestations. The most common spondylarthropathies are ankylosing spondylitis, psoriatic arthritis, reactive arthritis (formerly known as Reiter's syndrome), enteropathic arthritis (associated with inflammatory bowel disease), and undifferentiated spondyloarthropathies.
The primary hallmark of these conditions is enthesitis, which is an inflammation at the sites where ligaments or tendons attach to bones. This can lead to pain, stiffness, and limited mobility in the affected areas, particularly in the spine and sacroiliac joints (the joints that connect the base of the spine to the pelvis).
Spondylarthropathies have a strong genetic association with the human leukocyte antigen B27 (HLA-B27) gene. However, not all individuals with this gene will develop spondylarthropathies, and many people without the gene can still be affected by these conditions.
Early diagnosis and appropriate treatment of spondylarthropathies are essential to help manage symptoms, prevent joint damage, and maintain mobility and quality of life. Treatment options typically include a combination of medications, physical therapy, and lifestyle modifications.
Fibromyalgia is a chronic disorder characterized by widespread musculoskeletal pain, fatigue, sleep disturbances, and cognitive difficulties. The pain typically occurs in specific tender points or trigger points, which are located on the neck, shoulders, back, hips, arms, and legs. These points are painful when pressure is applied.
The exact cause of fibromyalgia is unknown, but it appears to be related to abnormalities in the way the brain processes pain signals. It may also be associated with certain genetic factors, physical trauma, infection, or emotional stress. Fibromyalgia is more common in women than men and tends to develop between the ages of 20 and 50.
Fibromyalgia can be difficult to diagnose because its symptoms are similar to those of other conditions, such as rheumatoid arthritis, lupus, and chronic fatigue syndrome. However, a diagnosis of fibromyalgia may be made if a person has widespread pain for at least three months and tenderness in at least 11 of 18 specific points on the body when pressure is applied.
There is no cure for fibromyalgia, but medications, therapy, and lifestyle changes can help manage its symptoms. Treatment may include pain relievers, antidepressants, anti-seizure drugs, physical therapy, counseling, stress reduction techniques, and regular exercise.
Health Planning Organizations (HPOs) are entities that are responsible for planning, coordinating, and evaluating health services within a specific geographic area. The primary goal of HPOs is to ensure the delivery of high-quality, cost-effective healthcare services that meet the needs of the population they serve.
HPOs may be involved in various activities, including:
1. Needs assessment: Identifying the health needs and priorities of the population, including any disparities or inequities in access to care.
2. Resource allocation: Deciding how to allocate resources to address identified needs and priorities.
3. Service planning: Developing plans for the delivery of healthcare services that are evidence-based, efficient, and effective.
4. Quality improvement: Monitoring and evaluating the quality of healthcare services and implementing strategies to improve them.
5. Coordination: Coordinating the delivery of healthcare services across different providers and settings to ensure continuity of care.
6. Advocacy: Advocating for policies and practices that promote health equity, access to care, and improved health outcomes.
HPOs can take various forms, including local health departments, regional health authorities, hospital networks, and other types of collaborative entities. They may be public or private, non-profit or for-profit, and their governance structures and funding mechanisms can vary widely.
Overall, the role of HPOs is to ensure that healthcare services are designed and delivered in a way that meets the needs of the population, improves health outcomes, and promotes health equity.
Vasculitis is a group of disorders characterized by inflammation of the blood vessels, which can cause changes in the vessel walls including thickening, narrowing, or weakening. These changes can restrict blood flow, leading to organ and tissue damage. The specific symptoms and severity of vasculitis depend on the size and location of the affected blood vessels and the extent of inflammation. Vasculitis can affect any organ system in the body, and its causes can vary, including infections, autoimmune disorders, or exposure to certain medications or chemicals.
Polymyalgia Rheumatica (PMR) is a geriatric rheumatic disease characterized by widespread musculoskeletal pain and stiffness, particularly affecting the neck, shoulders, hips, and thighs. It is often accompanied by symptoms such as fatigue, weakness, loss of appetite, and low-grade fever. The onset of PMR can be sudden or gradual, and it tends to affect individuals over 50 years of age, more commonly women than men.
The exact cause of Polymyalgia Rheumatica remains unknown; however, it is believed to involve an autoimmune response leading to inflammation in the affected areas. Diagnosis typically involves a combination of clinical evaluation, laboratory tests (such as elevated erythrocyte sedimentation rate or C-reactive protein), and sometimes imaging studies. Treatment usually includes corticosteroids to reduce inflammation and manage symptoms, along with monitoring for potential side effects from long-term steroid use. In many cases, PMR can be successfully managed with appropriate treatment, allowing individuals to return to their normal activities.
HLA-B27 antigen is a type of human leukocyte antigen (HLA) found on the surface of white blood cells. HLAs are proteins that help the body's immune system distinguish its own cells from foreign substances such as viruses and bacteria.
HLA-B27 is a specific type of HLA-B antigen, which is part of the major histocompatibility complex (MHC) class I molecules. The presence of HLA-B27 antigen can be inherited from parents to their offspring.
While most people with the HLA-B27 antigen do not develop any health problems, this antigen is associated with an increased risk of developing certain inflammatory diseases, particularly spondyloarthritis, a group of disorders that affect the joints and spine. Examples of these conditions include ankylosing spondylitis, reactive arthritis, psoriatic arthritis, and enteropathic arthritis associated with inflammatory bowel disease. However, not everyone with HLA-B27 will develop these diseases, and many people without the antigen can still develop spondyloarthritis.
Chorea is a medical term that describes an involuntary movement disorder characterized by brief, irregular, and abrupt jerky movements. These movements often occur randomly and can affect any part of the body. Chorea can also cause difficulty with coordination and balance, and can sometimes be accompanied by muscle weakness or rigidity.
The term "chorea" comes from the Greek word "χορεία" (khoréia), which means "dance," reflecting the graceful, dance-like movements that are characteristic of this condition. Chorea can occur as a symptom of various underlying medical conditions, including neurological disorders such as Huntington's disease, Sydenham's chorea, and cerebral palsy, as well as metabolic disorders, infections, and certain medications.
Treatment for chorea depends on the underlying cause of the condition and may include medications to help control the involuntary movements, physical therapy to improve coordination and balance, and lifestyle modifications to reduce the risk of injury from falls or other accidents. In some cases, surgery may be recommended as a last resort for severe or refractory chorea.
Polymyositis is defined as a rare inflammatory disorder that causes muscle weakness and inflammation (swelling) of the muscles. It primarily affects the skeletal muscles, which are the muscles responsible for voluntary movements such as walking, talking, and swallowing. The onset of polymyositis can occur at any age but is most commonly seen in adults between 31 to 60 years old, with women being slightly more affected than men.
The exact cause of polymyositis remains unknown; however, it is believed to be an autoimmune disorder, where the body's immune system mistakenly attacks its own muscle tissue. Certain factors such as genetics, viral infections, and exposure to certain drugs may contribute to the development of this condition.
Polymyositis can cause various symptoms, including:
- Progressive muscle weakness and wasting, particularly affecting the proximal muscles (those closest to the trunk of the body) such as the hips, thighs, shoulders, and upper arms.
- Difficulty climbing stairs, lifting objects, or rising from a seated position.
- Fatigue and stiffness, especially after periods of inactivity.
- Joint pain and swelling.
- Difficulty swallowing or speaking.
- Shortness of breath due to weakened respiratory muscles.
Diagnosis of polymyositis typically involves a combination of medical history, physical examination, laboratory tests, electromyography (EMG), and muscle biopsy. Treatment usually includes medications such as corticosteroids and immunosuppressants to reduce inflammation and control the immune response. Physical therapy may also be recommended to help maintain muscle strength and flexibility.
If left untreated, polymyositis can lead to significant disability and complications, including respiratory failure, malnutrition, and cardiovascular disease. Early diagnosis and treatment are crucial for improving outcomes and preventing long-term complications.
Myositis is a medical term that refers to inflammation of the muscle tissue. This condition can cause various symptoms, including muscle weakness, pain, swelling, and stiffness. There are several types of myositis, such as polymyositis, dermatomyositis, and inclusion body myositis, which have different causes and characteristics.
Polymyositis is a type of myositis that affects multiple muscle groups, particularly those close to the trunk of the body. Dermatomyositis is characterized by muscle inflammation as well as a skin rash. Inclusion body myositis is a less common form of myositis that typically affects older adults and can cause both muscle weakness and wasting.
The causes of myositis vary depending on the type, but they can include autoimmune disorders, infections, medications, and other medical conditions. Treatment for myositis may involve medication to reduce inflammation, physical therapy to maintain muscle strength and flexibility, and lifestyle changes to manage symptoms and prevent complications.
Immunoglobulin G (IgG) is a type of antibody, which is a protective protein produced by the immune system in response to foreign substances like bacteria or viruses. IgG is the most abundant type of antibody in human blood, making up about 75-80% of all antibodies. It is found in all body fluids and plays a crucial role in fighting infections caused by bacteria, viruses, and toxins.
IgG has several important functions:
1. Neutralization: IgG can bind to the surface of bacteria or viruses, preventing them from attaching to and infecting human cells.
2. Opsonization: IgG coats the surface of pathogens, making them more recognizable and easier for immune cells like neutrophils and macrophages to phagocytose (engulf and destroy) them.
3. Complement activation: IgG can activate the complement system, a group of proteins that work together to help eliminate pathogens from the body. Activation of the complement system leads to the formation of the membrane attack complex, which creates holes in the cell membranes of bacteria, leading to their lysis (destruction).
4. Antibody-dependent cellular cytotoxicity (ADCC): IgG can bind to immune cells like natural killer (NK) cells and trigger them to release substances that cause target cells (such as virus-infected or cancerous cells) to undergo apoptosis (programmed cell death).
5. Immune complex formation: IgG can form immune complexes with antigens, which can then be removed from the body through various mechanisms, such as phagocytosis by immune cells or excretion in urine.
IgG is a critical component of adaptive immunity and provides long-lasting protection against reinfection with many pathogens. It has four subclasses (IgG1, IgG2, IgG3, and IgG4) that differ in their structure, function, and distribution in the body.
According to the United States Food and Drug Administration (FDA), biological products are "products that are made from or contain a living organism or its derivatives, such as vaccines, blood and blood components, cells, genes, tissues, and proteins." These products can be composed of sugars, proteins, nucleic acids, or complex combinations of these substances, and they can come from many sources, including humans, animals, microorganisms, or plants.
Biological products are often used to diagnose, prevent, or treat a wide range of medical conditions, and they can be administered in various ways, such as through injection, inhalation, or topical application. Because biological products are derived from living organisms, their manufacturing processes can be complex and must be tightly controlled to ensure the safety, purity, and potency of the final product.
It's important to note that biological products are not the same as drugs, which are chemically synthesized compounds. While drugs are designed to interact with specific targets in the body, such as enzymes or receptors, biological products can have more complex and varied mechanisms of action, making them potentially more difficult to characterize and regulate.
 Annals of the Rheumatic Diseases
Annals of the Rheumatic Diseases Rheumatic Fever: All You Need to Know | CDC
Rheumatic Fever: All You Need to Know | CDC Pregnancy in Rheumatic Disease Quadruples CVE Risk
Pregnancy in Rheumatic Disease Quadruples CVE Risk Rheumatic heart disease: Risk factors, symptoms, treatment, and more
Rheumatic heart disease: Risk factors, symptoms, treatment, and more Annals of the Rheumatic Diseases
Annals of the Rheumatic Diseases NIH Guide: BIOMARKERS FOR RHEUMATIC AND SKIN DISEASES
NIH Guide: BIOMARKERS FOR RHEUMATIC AND SKIN DISEASES 'Utter neglect' of rheumatic heart disease revealed by results from global study |...
'Utter neglect' of rheumatic heart disease revealed by results from global study |... Rheumatic Diseases: Observational Study of Pediatric Rheumatic Diseases - The CARRA Registry
Rheumatic Diseases: Observational Study of Pediatric Rheumatic Diseases - The CARRA Registry Disease-modifying anti-rheumatic drugs (DMARDs) for Sjogren's syndrome | Cochrane
Disease-modifying anti-rheumatic drugs (DMARDs) for Sjogren's syndrome | Cochrane Remote Area Nurse - Rheumatic Heart Disease Program Coordinator - NACCHO
Remote Area Nurse - Rheumatic Heart Disease Program Coordinator - NACCHO National Rheumatic Heart Disease Data Collection - Australian Institute of Health and Welfare
National Rheumatic Heart Disease Data Collection - Australian Institute of Health and Welfare The Deadly Link: Strep Throat and Rheumatic Heart Disease (RHD) Video - Cardiology | Children's National Hospital
The Deadly Link: Strep Throat and Rheumatic Heart Disease (RHD) Video - Cardiology | Children's National Hospital Quality and continuity of care in Dutch nurse clinics for people with rheumatic diseases. | Nivel
Quality and continuity of care in Dutch nurse clinics for people with rheumatic diseases. | Nivel Immunological Consequences of COVID-19 Vaccination in Patients with Rheumatic Diseases - Mayo Clinic
Immunological Consequences of COVID-19 Vaccination in Patients with Rheumatic Diseases - Mayo Clinic Neuropsychiatric Symptoms in Rheumatic Disease Greatly Underestimated by Clinicians
Neuropsychiatric Symptoms in Rheumatic Disease Greatly Underestimated by Clinicians Reactivation of Chagas Disease in a Patient With an Autoimmune Rheumatic Disease: Case Report and Review of the Literature
Reactivation of Chagas Disease in a Patient With an Autoimmune Rheumatic Disease: Case Report and Review of the Literature Anticoagulation & rheumatic disease | MDedge Internal Medicine
Anticoagulation & rheumatic disease | MDedge Internal Medicine SA Rheumatic Heart Disease Control Program: Annual Report 2020 | SA Health
SA Rheumatic Heart Disease Control Program: Annual Report 2020 | SA Health