Sick Sinus Syndrome
Pacemaker, Artificial
Arrhythmia, Sinus
Cardiac Pacing, Artificial
Bradycardia
Heart Block
Electrocardiography
Syncope
Sinoatrial Node
Atrial Fibrillation
NAV1.5 Voltage-Gated Sodium Channel
Azygos Vein
Carotid Sinus
Telemetry
Arrhythmias, Cardiac
Atrioventricular Block
Atrioventricular Node
Electrocardiography, Ambulatory
Cavernous Sinus
Heart Conduction System
Maxillary Sinus
Sick Leave
Arterial thromboembolism in patients with sick sinus syndrome: prediction from pacing mode, atrial fibrillation, and echocardiographic findings. (1/234)
OBJECTIVE: To evaluate whether thromboembolism in sick sinus syndrome can be predicted by pacing mode, atrial fibrillation, or echocardiographic findings. METHODS: Patients were randomised to single chamber atrial (n = 110) or ventricular (n = 115) pacing. They were divided into subgroups with and without brady-tachy syndrome at time of randomisation. The occurrence of atrial fibrillation and thromboembolism during follow up were investigated and compared with echocardiographic findings. RESULTS: The annual risk of thromboembolism was 5.8% in patients with brady-tachy syndrome randomised to ventricular pacing, 3.2% in patients without brady-tachy syndrome randomised to ventricular pacing, 3% in patients with brady-tachy syndrome randomised to atrial pacing, and 1.5% in patients without brady-tachy syndrome randomised to atrial pacing. In atrial paced patients without brady-tachy syndrome at randomisation and without atrial fibrillation during follow up, the annual risk of thromboembolism was 1.4%. Left atrial size measured by M mode echocardiography was of no value in predicting thromboembolism. CONCLUSIONS: Arterial thromboembolism in patients with sick sinus syndrome is very common and is associated primarily with brady-tachy syndrome at randomisation and with ventricular pacing. The risk of thromboembolism is small in atrial paced patients in whom atrial fibrillation has never been documented. (+info)Acute performance of steroid-eluting screw-in leads for atrial free wall pacing. (2/234)
The aim of this study was to clarify the acute performance of steroid-eluting screw-in leads in comparison with that of nonsteroid screw-in leads for atrial free wall pacing. In 114 cases (68 males, 46 females, average age 70 years) with atrial free wall pacing by screw-in leads, pacing thresholds and P-wave amplitudes were compared at the time of implantation and 1 week later between 68 cases of nonsteroid and 46 cases of steroid-eluting screw-in leads. No significant differences were seen between the 2 groups at implantation in either voltage or current thresholds measured at pulse widths of 0.1, 0.3, 0.6, 1.0, 2.0 ms, or P-wave amplitudes. Pulse width thresholds at outputs of 2.5 V and 5.0 V were significantly lower for steroid leads 1 week after implantation (2.5 V: 0.34+/-0.27 ms nonsteroid vs. 0.12+/-0.08 ms steroid, p<0.001; 5.0 V: 0.12+/-0.08 ms nonsteroid vs. 0.06+/-0.02 ms steroid, p<0.01). P-wave amplitudes after 1 week were significantly higher for steroid leads (2.6+/-0.7 mV nonsteroid vs 3.0+/-1.2 mV steroid, p<0.001). Threshold rise, including pacing failure, was observed in 15 (22%) of the non-steroid leads, but in only 1 (2%) of the steroid leads. In conclusion, steroid-eluting screw-in leads suppress the acute rise of pacing thresholds in the right atrial free wall and their acute performance is better than that of non-steroid leads. These results suggest that appropriate low-output atrial pacing is feasible immediately after implantation. (+info)Exercise-induced uncommon atrioventricular nodal reentrant tachycardia with sick sinus syndrome: a case report. (3/234)
Exercise seldom provokes tachycardia in patients with paroxysmal supraventricular tachycardia (PSVT). This report presents a case of exercise-induced uncommon atrioventricular nodal reentrant tachycardia (AVNRT) with sick sinus syndrome. Treadmill exercise testing provoked AVNRT of long RP' with good reproducibility. Uncommon AVNRT was confirmed by the lack of atrial pre-excitation during PSVT and para-Hisian pacing. The patient has been successfully treated with verapamil and DDD pacing for 5 years. (+info)Effect of physiological mechanical perturbations on intact human myocardial repolarization. (4/234)
OBJECTIVE: The objective of this study was to investigate the relationship between acute decreases in right ventricular volume during Valsalva strain (with resultant changes in autonomic neural tone) and measures of local endocardial repolarization time independent of heart rate and autonomic neural tone. METHODS: Patients implanted with a stimulus to T wave (Stim-T) sensing pacemaker specially adapted to output a validate measure of beat to beat local repolarization (n = 9) performed Valsalva manoeuvers (40 mmHg for 15 s) while paced at a cycle length of 500 ms. Stim-T intervals were measured before and after autonomic blockade (Block: 0.03 mg/kg i.v. atropine +/- 0.15 mg/kg propranolol). Right ventricular end diastolic volume was estimated by simultaneous 2D-echocardiography. RESULTS: Without autonomic blockade, compared to baseline, repolarization significantly prolonged during Valsalva strain (1.1 +/- 0.7%) and shortened during release (-1.4 +/- 1.0%). After block, strain related repolarization prolongation was also observed (1.0 +/- 0.6%), with significantly less release related repolarization shortening (-0.8 +/- 0.8%) compared to pre-block (P < 0.05). Right ventricular end diastolic volume decreased during strain by 11 +/- 10 and 9 +/- 16% from baseline, pre- and post-block respectively (P < 0.05). CONCLUSION: In a chronically instrumented human model, an acute physiologic volume reduction modestly prolongs right ventricular repolarization independent of changes in rate or autonomic tone. (+info)Concerns about sources of electromagnetic interference in patients with pacemakers. (5/234)
Electromagnetic noise is rapidly increasing in our environment so electromagnetic interference (EMI) with pacemakers (PM) may become a more important problem despite technological improvements in PM. The aim of this study was to evaluate the kinds of EMI which affect the quality of life of PM patients. The participants (1,942 Japanese Association for Pacemaker Patients: Pacemaker-Tomonokai) were asked to respond to a questionnaire about their major EMI troubles, and 1,567 patients (80.7%) responded by mail. The main concerns were from mobile telephones (MT) (39%), magnetic resonance imaging (MRI) (17%), electronic kitchen appliances, automobile engines and high voltage power lines. If possible, PM implantation sites should be carefully selected not only according to the physician's convenience but also considering information on each patient's habits and physical limitations. (+info)Regional myocardial blood flow in patients with sick sinus syndrome randomized to long-term single chamber atrial or dual chamber pacing--effect of pacing mode and rate. (6/234)
OBJECTIVES: This study aimed to evaluate regional myocardial blood flow (MBF) and global left ventricular ejection fraction (LVEF) during chronic pacing in patients with sick sinus syndrome (SSS) randomized to either single chamber atrial (AAI) or dual chamber (DDD) pacing. BACKGROUND: Experimental studies indicate that chronic pacing in the right ventricular apex changes regional MBF, thereby compromising left ventricular function. METHODS: Thirty patients (age 74 +/- 10 years) were randomized to AAI (n = 15) or DDD (n = 15) pacemakers. After 22 +/- 7 months of pacing, MBF was quantified with 13N-labeled ammonia positron emission tomography scanning at 60 beats per min and 90 beats per min. Patients in the DDD group furthermore underwent MBF measurement at temporary AAI pacing, 60 beats per min. Myocardial blood flow was assessed in the anterior, lateral, inferior and septal regions, and the global mean MBF was calculated. Left ventricular ejection fraction was determined by echocardiography at pacemaker implantation and at the time of MBF measurements. RESULTS: Myocardial blood flow at rates 60 and 90 beats per min did not differ between the AAI and DDD groups. During temporary AAI pacing in the DDD group, MBF was significantly higher than during DDD pacing in both the inferior (p = 0.001) and septal (p = 0.004) regions and also globally (0.61 +/- 0.15 vs. 0.53 +/- 0.13 mL x g(-1) x min(-1), p = 0.005). In the DDD group, LVEF decreased from pacemaker implantation to time of MBF measurements (0.61 +/- 0.09 vs. 0.56 +/- 0.07, p = 0.013). Left ventricular ejection fraction during temporary AAI pacing at time of MBF measurements was not different from LVEF at pacemaker implantation. CONCLUSIONS: In patients with SSS, chronic DDD pacing reduced inferior, septal and global mean MBF as well as LVEF, as compared with temporary AAI pacing. The LVEF reversed to baseline level during temporary AAI pacing despite 22 months of permanent ventricular pacing preceding it. Augmenting pace rate to 90 beats per min increased MBF equally in the two treatment groups. (+info)Exchange of pacing or defibrillator leads following laser sheath extraction of non-functional leads in patients with ipsilateral obstructed venous access. (7/234)
Occlusion of the subclavian or brachiocephalic vein in pacemaker or defibrillator patients prohibits ipsilateral implantation of new leads with standard techniques in the event of lead malfunction. Three patients are presented in whom laser sheath extraction of a non-functional lead was performed in order to recanalise the occluded vein and to secure a route for implantation of new leads. This technique avoids abandoning a useful subpectoral site for pacing or defibrillator therapy. The laser sheath does not affect normally functioning leads at the same site. (+info)Permanent pacemaker insertion in a district general hospital: indications, patient characteristics, and complications. (8/234)
This report reviews the experience of permanent pacemaker insertion in a district general hospital (catchment population of 350 000) and makes a comparison with the national database and other hospitals in the UK. METHODS: The records of all patients receiving a permanent pacemaker in the inclusive period January 1996 to December 1998 were reviewed. Data collected included number of patients paced each year, age, sex, indications, and complications. RESULTS: In the three years reviewed 200 patients received new permanent pacemakers, a rate of 190 per million population per year, which is similar to the national implantation rate of permanent pacemakers but lower than that of most European countries (see discussion). The majority of patients paced were elderly (75% were above the age of 70 years). Atrioventricular block (including complete heart block, 45%, and Mobitz type 2 block, 12.5%) was the commonest indication for permanent pacemaker insertion, followed by sick sinus syndrome (25%) and these findings are comparable to those reported previously. However, carotid sinus syndrome was responsible for 16% of the patients paced and this was higher than that reported in the national database (6.5%). Only 1% of the pacemaker modes used was inappropriate and the complication rate was low at 3%. CONCLUSIONS: This report confirms that permanent pacemaker insertion can be effectively and safely provided locally for the increasingly ageing population. The implantation rate both locally and nationally is still much lower than that of some countries in Europe. (+info)Sick Sinus Syndrome (SSS) is a term used to describe a group of abnormal heart rhythm disturbances that originates in the sinoatrial node (the natural pacemaker of the heart). This syndrome is characterized by impaired functioning of the sinoatrial node, resulting in various abnormalities such as sinus bradycardia (abnormally slow heart rate), sinus arrest (complete cessation of sinus node activity), and/or sinoatrial exit block (failure of the electrical impulse to leave the sinus node and spread to the atria).
People with SSS may experience symptoms such as palpitations, dizziness, fatigue, shortness of breath, or syncope (fainting) due to inadequate blood supply to the brain caused by slow heart rate. The diagnosis of SSS is typically made based on the patient's symptoms and the results of an electrocardiogram (ECG), Holter monitoring, or event recorder that shows evidence of abnormal sinus node function. Treatment options for SSS may include lifestyle modifications, medications, or implantation of a pacemaker to regulate the heart rate.
An artificial pacemaker is a medical device that uses electrical impulses to regulate the beating of the heart. It is typically used when the heart's natural pacemaker, the sinoatrial node, is not functioning properly and the heart rate is too slow or irregular. The pacemaker consists of a small generator that contains a battery and electronic circuits, which are connected to one or more electrodes that are placed in the heart.
The generator sends electrical signals through the electrodes to stimulate the heart muscle and cause it to contract, thereby maintaining a regular heart rhythm. Artificial pacemakers can be programmed to deliver electrical impulses at a specific rate or in response to the body's needs. They are typically implanted in the chest during a surgical procedure and can last for many years before needing to be replaced.
Artificial pacemakers are an effective treatment for various types of bradycardia, which is a heart rhythm disorder characterized by a slow heart rate. Pacemakers can significantly improve symptoms associated with bradycardia, such as fatigue, dizziness, shortness of breath, and fainting spells.
Sinus arrhythmia is a type of heart rhythm disorder (arrhythmia) where the normal rhythm generated by the sinus node in the heart varies in rate or pattern. The sinus node is the natural pacemaker of the heart and usually sets a steady pace for heartbeats. However, in sinus arrhythmia, the heart rate may speed up or slow down abnormally during breathing in (inspiration) or breathing out (expiration).
When the heart rate increases during inspiration, it is called "inspiratory sinus arrhythmia," and when the heart rate decreases during expiration, it is called "expiratory sinus arrhythmia." Most people experience a mild form of inspiratory sinus arrhythmia, which is considered normal, especially in children and young adults.
However, if the variation in heart rate is significant or accompanied by symptoms such as palpitations, dizziness, shortness of breath, or chest discomfort, it may require medical evaluation and treatment. Sinus arrhythmia can be caused by various factors, including lung disease, heart disease, electrolyte imbalances, or the use of certain medications.
Artificial cardiac pacing is a medical procedure that involves the use of an artificial device to regulate and stimulate the contraction of the heart muscle. This is often necessary when the heart's natural pacemaker, the sinoatrial node, is not functioning properly and the heart is beating too slowly or irregularly.
The artificial pacemaker consists of a small generator that produces electrical impulses and leads that are positioned in the heart to transmit the impulses. The generator is typically implanted just under the skin in the chest, while the leads are inserted into the heart through a vein.
There are different types of artificial cardiac pacing systems, including single-chamber pacemakers, which stimulate either the right atrium or right ventricle, and dual-chamber pacemakers, which stimulate both chambers of the heart. Some pacemakers also have additional features that allow them to respond to changes in the body's needs, such as during exercise or sleep.
Artificial cardiac pacing is a safe and effective treatment for many people with abnormal heart rhythms, and it can significantly improve their quality of life and longevity.
Bradycardia is a medical term that refers to an abnormally slow heart rate, typically defined as a resting heart rate of less than 60 beats per minute in adults. While some people, particularly well-trained athletes, may have a naturally low resting heart rate, bradycardia can also be a sign of an underlying health problem.
There are several potential causes of bradycardia, including:
* Damage to the heart's electrical conduction system, such as from heart disease or aging
* Certain medications, including beta blockers, calcium channel blockers, and digoxin
* Hypothyroidism (underactive thyroid gland)
* Sleep apnea
* Infection of the heart (endocarditis or myocarditis)
* Infiltrative diseases such as amyloidosis or sarcoidosis
Symptoms of bradycardia can vary depending on the severity and underlying cause. Some people with bradycardia may not experience any symptoms, while others may feel weak, fatigued, dizzy, or short of breath. In severe cases, bradycardia can lead to fainting, confusion, or even cardiac arrest.
Treatment for bradycardia depends on the underlying cause. If a medication is causing the slow heart rate, adjusting the dosage or switching to a different medication may help. In other cases, a pacemaker may be necessary to regulate the heart's rhythm. It is important to seek medical attention if you experience symptoms of bradycardia, as it can be a sign of a serious underlying condition.
Heart block is a cardiac condition characterized by the interruption of electrical impulse transmission from the atria (the upper chambers of the heart) to the ventricles (the lower chambers of the heart). This disruption can lead to abnormal heart rhythms, including bradycardia (a slower-than-normal heart rate), and in severe cases, can cause the heart to stop beating altogether. Heart block is typically caused by damage to the heart's electrical conduction system due to various factors such as aging, heart disease, or certain medications.
There are three types of heart block: first-degree, second-degree, and third-degree (also known as complete heart block). Each type has distinct electrocardiogram (ECG) findings and symptoms. Treatment for heart block depends on the severity of the condition and may include monitoring, medication, or implantation of a pacemaker to regulate the heart's electrical activity.
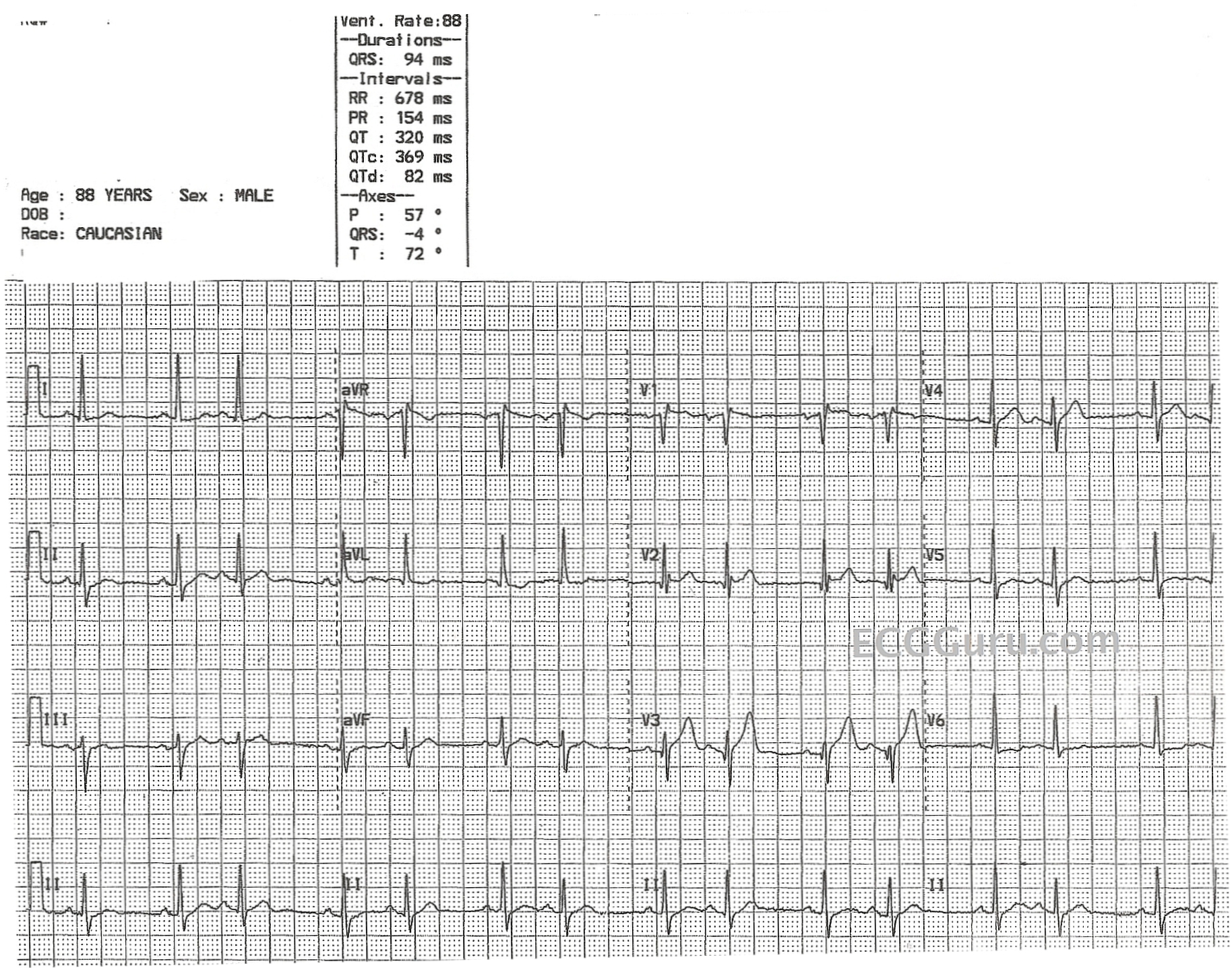
Electrocardiography (ECG or EKG) is a medical procedure that records the electrical activity of the heart. It provides a graphic representation of the electrical changes that occur during each heartbeat. The resulting tracing, called an electrocardiogram, can reveal information about the heart's rate and rhythm, as well as any damage to its cells or abnormalities in its conduction system.
During an ECG, small electrodes are placed on the skin of the chest, arms, and legs. These electrodes detect the electrical signals produced by the heart and transmit them to a machine that amplifies and records them. The procedure is non-invasive, painless, and quick, usually taking only a few minutes.
ECGs are commonly used to diagnose and monitor various heart conditions, including arrhythmias, coronary artery disease, heart attacks, and electrolyte imbalances. They can also be used to evaluate the effectiveness of certain medications or treatments.
Syncope is a medical term defined as a transient, temporary loss of consciousness and postural tone due to reduced blood flow to the brain. It's often caused by a drop in blood pressure, which can be brought on by various factors such as dehydration, emotional stress, prolonged standing, or certain medical conditions like heart diseases, arrhythmias, or neurological disorders.
During a syncope episode, an individual may experience warning signs such as lightheadedness, dizziness, blurred vision, or nausea before losing consciousness. These episodes usually last only a few minutes and are followed by a rapid, full recovery. However, if left untreated or undiagnosed, recurrent syncope can lead to severe injuries from falls or even life-threatening conditions related to the underlying cause.
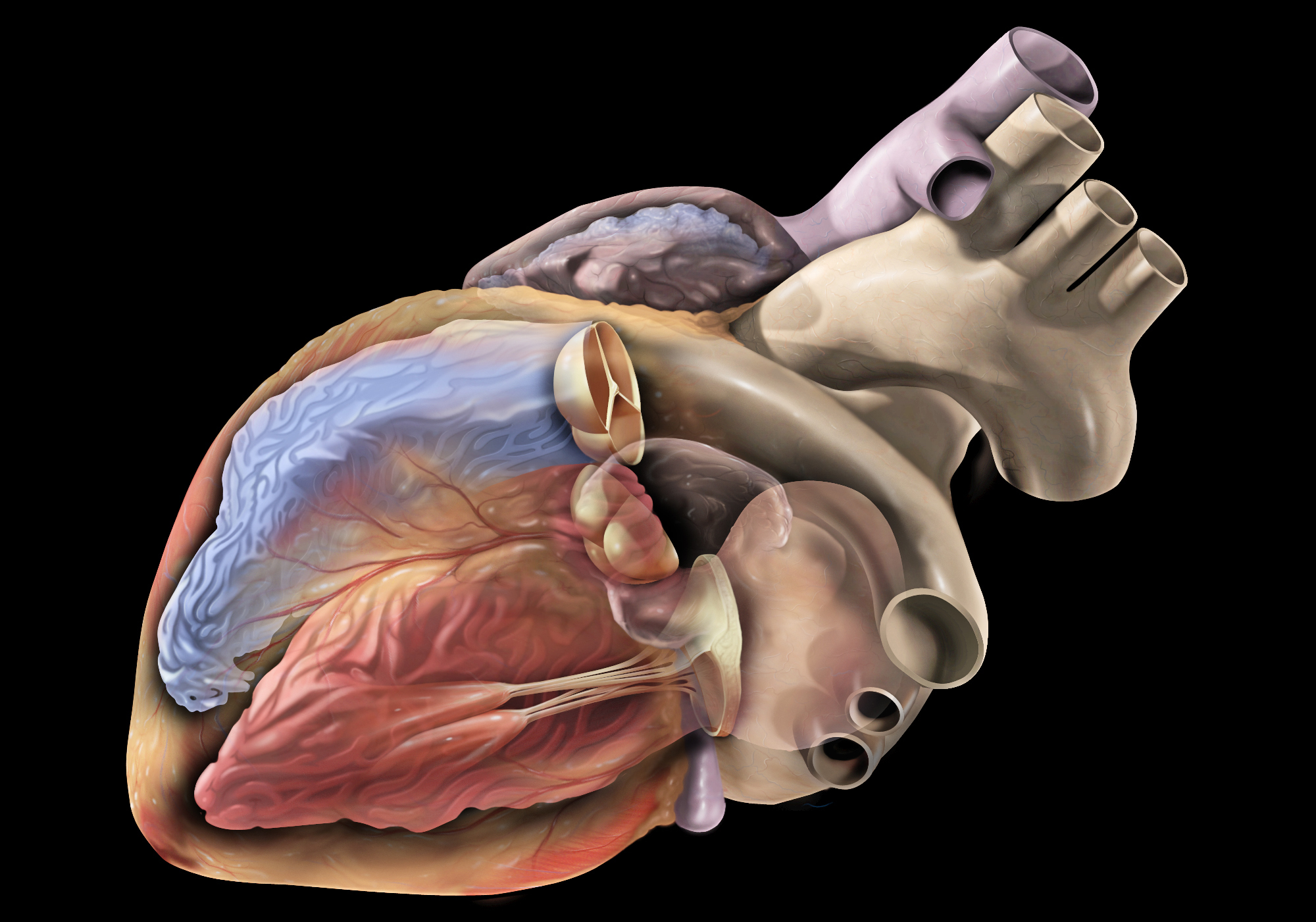
The sinoatrial (SA) node, also known as the sinus node, is the primary pacemaker of the heart. It is a small bundle of specialized cardiac conduction tissue located in the upper part of the right atrium, near the entrance of the superior vena cava. The SA node generates electrical impulses that initiate each heartbeat, causing the atria to contract and pump blood into the ventricles. This process is called sinus rhythm.
The SA node's electrical activity is regulated by the autonomic nervous system, which can adjust the heart rate in response to changes in the body's needs, such as during exercise or rest. The SA node's rate of firing determines the heart rate, with a normal resting heart rate ranging from 60 to 100 beats per minute.
If the SA node fails to function properly or its electrical impulses are blocked, other secondary pacemakers in the heart may take over, resulting in abnormal heart rhythms called arrhythmias.
A syndrome, in medical terms, is a set of symptoms that collectively indicate or characterize a disease, disorder, or underlying pathological process. It's essentially a collection of signs and/or symptoms that frequently occur together and can suggest a particular cause or condition, even though the exact physiological mechanisms might not be fully understood.
For example, Down syndrome is characterized by specific physical features, cognitive delays, and other developmental issues resulting from an extra copy of chromosome 21. Similarly, metabolic syndromes like diabetes mellitus type 2 involve a group of risk factors such as obesity, high blood pressure, high blood sugar, and abnormal cholesterol or triglyceride levels that collectively increase the risk of heart disease, stroke, and diabetes.
It's important to note that a syndrome is not a specific diagnosis; rather, it's a pattern of symptoms that can help guide further diagnostic evaluation and management.
Atrial fibrillation (A-tre-al fi-bru-la'shun) is a type of abnormal heart rhythm characterized by rapid and irregular beating of the atria, the upper chambers of the heart. In this condition, the electrical signals that coordinate heartbeats don't function properly, causing the atria to quiver instead of contracting effectively. As a result, blood may not be pumped efficiently into the ventricles, which can lead to blood clots, stroke, and other complications. Atrial fibrillation is a common type of arrhythmia and can cause symptoms such as palpitations, shortness of breath, fatigue, and dizziness. It can be caused by various factors, including heart disease, high blood pressure, age, and genetics. Treatment options include medications, electrical cardioversion, and surgical procedures to restore normal heart rhythm.
NAV1.5, also known as SCN5A, is a specific type of voltage-gated sodium channel found in the heart muscle cells (cardiomyocytes). These channels play a crucial role in the generation and transmission of electrical signals that coordinate the contraction of the heart.
More specifically, NAV1.5 channels are responsible for the rapid influx of sodium ions into cardiomyocytes during the initial phase of the action potential, which is the electrical excitation of the cell. This rapid influx of sodium ions helps to initiate and propagate the action potential throughout the heart muscle, allowing for coordinated contraction and proper heart function.
Mutations in the SCN5A gene, which encodes the NAV1.5 channel, have been associated with various cardiac arrhythmias, including long QT syndrome, Brugada syndrome, and familial atrial fibrillation, among others. These genetic disorders can lead to abnormal heart rhythms, syncope, and in some cases, sudden cardiac death.
Right atrial function refers to the role and performance of the right atrium in the heart. The right atrium is one of the four chambers of the heart and is responsible for receiving deoxygenated blood from the body via the superior and inferior vena cava. It then contracts to help pump the blood into the right ventricle, which subsequently sends it to the lungs for oxygenation.
Right atrial function can be assessed through various methods, including echocardiography, cardiac magnetic resonance imaging (MRI), and electrocardiogram (ECG). Abnormalities in right atrial function may indicate underlying heart conditions such as right-sided heart failure, atrial fibrillation, or other cardiovascular diseases. Proper evaluation and monitoring of right atrial function are essential for effective diagnosis, treatment, and management of these conditions.
The azygos vein is a large, unpaired venous structure in the thoracic cavity of the human body. It begins as the ascending lumbar vein, which receives blood from the lower extremities and abdominal organs. As it enters the thorax through the diaphragm, it becomes the azygos vein and continues to ascend along the vertebral column.
The azygos vein receives blood from various tributaries, including the intercostal veins, esophageal veins, mediastinal veins, and bronchial veins. It then arches over the right mainstem bronchus and empties into the superior vena cava, which returns blood to the right atrium of the heart.
The azygos vein provides an important collateral pathway for venous return in cases where the inferior vena cava is obstructed or occluded. It also plays a role in the spread of certain thoracic diseases, such as tuberculosis and cancer.
The carotid sinus is a small, dilated area located at the bifurcation (or fork) of the common carotid artery into the internal and external carotid arteries. It is a baroreceptor region, which means it contains specialized sensory nerve endings that can detect changes in blood pressure. When the blood pressure increases, the walls of the carotid sinus stretch, activating these nerve endings and sending signals to the brain. The brain then responds by reducing the heart rate and relaxing the blood vessels, which helps to lower the blood pressure back to normal.
The carotid sinus is an important part of the body's autonomic nervous system, which regulates various involuntary functions such as heart rate, blood pressure, and digestion. It plays a crucial role in maintaining cardiovascular homeostasis and preventing excessive increases in blood pressure that could potentially damage vital organs.
Telemetry is the automated measurement and wireless transmission of data from remote or inaccessible sources to receiving stations for monitoring and analysis. In a medical context, telemetry is often used to monitor patients' vital signs such as heart rate, blood pressure, oxygen levels, and other important physiological parameters continuously and remotely. This technology allows healthcare providers to track patients' conditions over time, detect any abnormalities or trends, and make informed decisions about their care, even when they are not physically present with the patient. Telemetry is commonly used in hospitals, clinics, and research settings to monitor patients during procedures, after surgery, or during extended stays in intensive care units.
Cardiac arrhythmias are abnormal heart rhythms that result from disturbances in the electrical conduction system of the heart. The heart's normal rhythm is controlled by an electrical signal that originates in the sinoatrial (SA) node, located in the right atrium. This signal travels through the atrioventricular (AV) node and into the ventricles, causing them to contract and pump blood throughout the body.
An arrhythmia occurs when there is a disruption in this electrical pathway or when the heart's natural pacemaker produces an abnormal rhythm. This can cause the heart to beat too fast (tachycardia), too slow (bradycardia), or irregularly.
There are several types of cardiac arrhythmias, including:
1. Atrial fibrillation: A rapid and irregular heartbeat that starts in the atria (the upper chambers of the heart).
2. Atrial flutter: A rapid but regular heartbeat that starts in the atria.
3. Supraventricular tachycardia (SVT): A rapid heartbeat that starts above the ventricles, usually in the atria or AV node.
4. Ventricular tachycardia: A rapid and potentially life-threatening heart rhythm that originates in the ventricles.
5. Ventricular fibrillation: A chaotic and disorganized electrical activity in the ventricles, which can be fatal if not treated immediately.
6. Heart block: A delay or interruption in the conduction of electrical signals from the atria to the ventricles.
Cardiac arrhythmias can cause various symptoms, such as palpitations, dizziness, shortness of breath, chest pain, and fatigue. In some cases, they may not cause any symptoms and go unnoticed. However, if left untreated, certain types of arrhythmias can lead to serious complications, including stroke, heart failure, or even sudden cardiac death.
Treatment for cardiac arrhythmias depends on the type, severity, and underlying causes. Options may include lifestyle changes, medications, cardioversion (electrical shock therapy), catheter ablation, implantable devices such as pacemakers or defibrillators, and surgery. It is essential to consult a healthcare professional for proper evaluation and management of cardiac arrhythmias.
Atrioventricular (AV) block is a disorder of the electrical conduction system of the heart that causes a delay or interruption in the transmission of electrical signals from the atria (the upper chambers of the heart) to the ventricles (the lower chambers of the heart). This results in an abnormal heart rhythm, also known as an arrhythmia.
There are three degrees of AV block:
1. First-degree AV block: In this type of AV block, there is a delay in the conduction of electrical signals from the atria to the ventricles, but all signals are eventually conducted. This condition may not cause any symptoms and is often discovered during a routine electrocardiogram (ECG).
2. Second-degree AV block: In this type of AV block, some electrical signals from the atria are not conducted to the ventricles. There are two types of second-degree AV block: Mobitz type I and Mobitz type II. Mobitz type I is characterized by a progressive prolongation of the PR interval (the time between the electrical activation of the atria and ventricles) until a QRS complex (which represents the electrical activation of the ventricles) is dropped. Mobitz type II is characterized by a constant PR interval with occasional non-conducted P waves.
3. Third-degree AV block: In this type of AV block, no electrical signals are conducted from the atria to the ventricles. The atria and ventricles beat independently of each other, resulting in a slow heart rate (bradycardia) and an irregular rhythm. This condition can be life-threatening if not treated promptly.
The causes of AV block include aging, heart disease, medications, and certain medical conditions such as hypothyroidism and Lyme disease. Treatment depends on the severity of the condition and may include medication, a pacemaker, or surgery.
The atrioventricular (AV) node is a critical part of the electrical conduction system of the heart. It is a small cluster of specialized cardiac muscle cells located in the lower interatrial septum, near the opening of the coronary sinus. The AV node receives electrical impulses from the sinoatrial node (the heart's natural pacemaker) via the internodal pathways and delays their transmission for a brief period before transmitting them to the bundle of His and then to the ventricles. This delay allows the atria to contract and empty their contents into the ventricles before the ventricles themselves contract, ensuring efficient pumping of blood throughout the body.
The AV node plays an essential role in maintaining a normal heart rhythm, as it can also function as a backup pacemaker if the sinoatrial node fails to generate impulses. However, certain heart conditions or medications can affect the AV node's function and lead to abnormal heart rhythms, such as atrioventricular block or atrial tachycardia.
Ambulatory electrocardiography, also known as ambulatory ECG or Holter monitoring, is a non-invasive method of recording the electrical activity of the heart over an extended period of time (typically 24 hours or more) while the patient goes about their daily activities. The device used to record the ECG is called a Holter monitor, which consists of a small, portable recorder that is attached to the patient's chest with electrodes.
The recorded data provides information on any abnormalities in the heart's rhythm or electrical activity during different stages of activity and rest, allowing healthcare providers to diagnose and evaluate various cardiac conditions such as arrhythmias, ischemia, and infarction. The ability to monitor the heart's activity over an extended period while the patient performs their normal activities provides valuable information that may not be captured during a standard ECG, which only records the heart's electrical activity for a few seconds.
In summary, ambulatory electrocardiography is a diagnostic tool used to evaluate the electrical activity of the heart over an extended period, allowing healthcare providers to diagnose and manage various cardiac conditions.
The cavernous sinus is a venous structure located in the middle cranial fossa, which is a depression in the skull that houses several important nerves and blood vessels. The cavernous sinus is situated on either side of the sphenoid bone, near the base of the skull, and it contains several important structures:
* The internal carotid artery, which supplies oxygenated blood to the brain
* The abducens nerve (cranial nerve VI), which controls lateral movement of the eye
* The oculomotor nerve (cranial nerve III), which controls most of the muscles that move the eye
* The trochlear nerve (cranial nerve IV), which controls one of the muscles that moves the eye
* The ophthalmic and maxillary divisions of the trigeminal nerve (cranial nerve V), which transmit sensory information from the face and head
The cavernous sinus is an important structure because it serves as a conduit for several critical nerves and blood vessels. However, it is also vulnerable to various pathological conditions such as thrombosis (blood clots), infection, tumors, or aneurysms, which can lead to serious neurological deficits or even death.
The heart conduction system is a group of specialized cardiac muscle cells that generate and conduct electrical impulses to coordinate the contraction of the heart chambers. The main components of the heart conduction system include:
1. Sinoatrial (SA) node: Also known as the sinus node, it is located in the right atrium near the entrance of the superior vena cava and functions as the primary pacemaker of the heart. It sets the heart rate by generating electrical impulses at regular intervals.
2. Atrioventricular (AV) node: Located in the interatrial septum, near the opening of the coronary sinus, it serves as a relay station for electrical signals between the atria and ventricles. The AV node delays the transmission of impulses to allow the atria to contract before the ventricles.
3. Bundle of His: A bundle of specialized cardiac muscle fibers that conducts electrical impulses from the AV node to the ventricles. It divides into two main branches, the right and left bundle branches, which further divide into smaller Purkinje fibers.
4. Right and left bundle branches: These are extensions of the Bundle of His that transmit electrical impulses to the respective right and left ventricular myocardium. They consist of specialized conducting tissue with large diameters and minimal resistance, allowing for rapid conduction of electrical signals.
5. Purkinje fibers: Fine, branching fibers that arise from the bundle branches and spread throughout the ventricular myocardium. They are responsible for transmitting electrical impulses to the working cardiac muscle cells, triggering coordinated ventricular contraction.
In summary, the heart conduction system is a complex network of specialized muscle cells responsible for generating and conducting electrical signals that coordinate the contraction of the atria and ventricles, ensuring efficient blood flow throughout the body.
The heart atria are the upper chambers of the heart that receive blood from the veins and deliver it to the lower chambers, or ventricles. There are two atria in the heart: the right atrium receives oxygen-poor blood from the body and pumps it into the right ventricle, which then sends it to the lungs to be oxygenated; and the left atrium receives oxygen-rich blood from the lungs and pumps it into the left ventricle, which then sends it out to the rest of the body. The atria contract before the ventricles during each heartbeat, helping to fill the ventricles with blood and prepare them for contraction.
Heart rate is the number of heartbeats per unit of time, often expressed as beats per minute (bpm). It can vary significantly depending on factors such as age, physical fitness, emotions, and overall health status. A resting heart rate between 60-100 bpm is generally considered normal for adults, but athletes and individuals with high levels of physical fitness may have a resting heart rate below 60 bpm due to their enhanced cardiovascular efficiency. Monitoring heart rate can provide valuable insights into an individual's health status, exercise intensity, and response to various treatments or interventions.
The maxillary sinuses, also known as the antrums of Highmore, are the largest of the four pairs of paranasal sinuses located in the maxilla bones. They are air-filled cavities that surround the nasolacrimal duct and are situated superior to the upper teeth and lateral to the nasal cavity. Each maxillary sinus is lined with a mucous membrane, which helps to warm, humidify, and filter the air we breathe. Inflammation or infection of the maxillary sinuses can result in conditions such as sinusitis, leading to symptoms like facial pain, headaches, and nasal congestion.
"Sick leave" is not a medical term, but rather a term used in the context of employment and human resources. It refers to the time off from work that an employee is allowed to take due to illness or injury, for which they may still receive payment. The specific policies regarding sick leave, such as how much time is granted and whether it is paid or unpaid, can vary based on the employer's policies, labor laws, and collective bargaining agreements.
Paranasal sinus diseases refer to a group of medical conditions that affect the paranasal sinuses, which are air-filled cavities located within the skull near the nasal cavity. These sinuses include the maxillary, frontal, ethmoid, and sphenoid sinuses.
Paranasal sinus diseases can be caused by a variety of factors, including viral, bacterial, or fungal infections, allergies, structural abnormalities, or autoimmune disorders. Some common paranasal sinus diseases include:
1. Sinusitis: Inflammation or infection of the sinuses, which can cause symptoms such as nasal congestion, thick nasal discharge, facial pain or pressure, and reduced sense of smell.
2. Nasal polyps: Soft, benign growths that develop in the lining of the nasal passages or sinuses, which can obstruct airflow and cause difficulty breathing through the nose.
3. Sinonasal tumors: Abnormal growths that can be benign or malignant, which can cause symptoms such as nasal congestion, facial pain, and bleeding from the nose.
4. Sinus cysts: Fluid-filled sacs that form in the sinuses, which can cause symptoms similar to those of sinusitis.
5. Fungal sinusitis: Infection of the sinuses with fungi, which can cause symptoms such as nasal congestion, facial pain, and thick, discolored mucus.
Treatment for paranasal sinus diseases depends on the underlying cause and severity of the condition. Treatment options may include medications, such as antibiotics, antihistamines, or corticosteroids, as well as surgical intervention in more severe cases.
 Sick sinus syndrome: MedlinePlus Genetics
Sick sinus syndrome: MedlinePlus Genetics Sick Sinus Syndrome - WellSpan Health Library
Sick Sinus Syndrome - WellSpan Health Library Sick Sinus Syndrome
Sick Sinus Syndrome Sick sinus syndrome Treatment Hyderabad - ₹756 Rs NPS Cosmetic Hospital
Sick sinus syndrome Treatment Hyderabad - ₹756 Rs NPS Cosmetic Hospital Atrial Fibrillation and Sick Sinus Syndrome: A Clinical Catch-22
Atrial Fibrillation and Sick Sinus Syndrome: A Clinical Catch-22 A Case of Sick Sinus Syndrome Presenting as Exploding Head Syndrome
A Case of Sick Sinus Syndrome Presenting as Exploding Head Syndrome PROGNOSIS IN SINUATRIAL DISORDER (SICK SINUS SYNDROME) - Radcliffe Department of Medicine
PROGNOSIS IN SINUATRIAL DISORDER (SICK SINUS SYNDROME) - Radcliffe Department of Medicine Sinus node dysfunction - Wikipedia
Sinus node dysfunction - Wikipedia Heart Disease articles - Heart Disease Health Center
Heart Disease articles - Heart Disease Health Center Sick Sinus Syndrome | Syndromes: Rapid Recognition and Perioperative Implications, 2e | AccessAnesthesiology | McGraw Hill...
Sick Sinus Syndrome | Syndromes: Rapid Recognition and Perioperative Implications, 2e | AccessAnesthesiology | McGraw Hill... Other Heart Rhythm Disorders | American Stroke Association
Other Heart Rhythm Disorders | American Stroke Association Sick sinus syndrome diagnosed after a sinus arrest during treatment for zygomatic fracture: a case report. | BMC Oral Health...
Sick sinus syndrome diagnosed after a sinus arrest during treatment for zygomatic fracture: a case report. | BMC Oral Health... Dr. Thomas Knox, MD - Cardiology Specialist in Hartford, CT | Healthgrades
Dr. Thomas Knox, MD - Cardiology Specialist in Hartford, CT | Healthgrades Heart arrhythmia - Symptoms and causes - Mayo Clinic
Heart arrhythmia - Symptoms and causes - Mayo Clinic Coronary CT Angiography: Practice Essentials, Overview, Clinical Applications: Coronary Artery Disease
Coronary CT Angiography: Practice Essentials, Overview, Clinical Applications: Coronary Artery Disease Sinus Bradycardia: Causes, Symptoms & Treatment
Sinus Bradycardia: Causes, Symptoms & Treatment DailyMed - METOPROLOL TARTRATE AND HYDROCHLOROTHIAZIDE tablet
DailyMed - METOPROLOL TARTRATE AND HYDROCHLOROTHIAZIDE tablet Dr. Sriram Padmanabhan, MD, Nuclear Cardiology Specialist - Baltimore, MD | Sharecare
Dr. Sriram Padmanabhan, MD, Nuclear Cardiology Specialist - Baltimore, MD | Sharecare Ivabradine 2.5 mg film-coated Tablets - Summary of Product Characteristics (SmPC) - (emc)
Ivabradine 2.5 mg film-coated Tablets - Summary of Product Characteristics (SmPC) - (emc) Visken - Uses, Side Effects, Interactions - MedBroadcast.com
Visken - Uses, Side Effects, Interactions - MedBroadcast.com Intracardiac electrophysiology study (EPS) Information | Mount Sinai - New York
Intracardiac electrophysiology study (EPS) Information | Mount Sinai - New York








![APA format] Physiology References for the Native American Flute](https://flutopedia.com/img/JoinCVFluteNewsletter_150.jpg)