Vaginal Fistula
Fistula
Arteriovenous Fistula
Intestinal Fistula
Cutaneous Fistula
Bronchial Fistula
Vascular Fistula
Rectal Fistula
Urinary Fistula
Esophageal Fistula
Pelvic fistulas complicating pelvic surgery or diseases: spectrum of imaging findings. (1/34)
Pelvic fistulas may result from obstetric complications, inflammatory bowel disease, pelvic malignancy, pelvic radiation therapy, pelvic surgery, or other traumatic causes, and their symptoms may be distressing. In our experience, various types of pelvic fistulas are identified after pelvic disease or pelvic surgery. Because of its close proximity, the majority of such fistulas occur in the pelvic cavity and include the vesicovaginal, vesicouterine, vesicoenteric, ureterovaginal, ureteroenteric and enterovaginal type. The purpose of this article is to illustrate the spectrum of imaging features of pelvic fistulas. (+info)Surgical outcome of female genital fistula in Korea. (2/34)
This purpose of this study was to establish a new standard for the surgical management of female genital fistula in Korea. From January 1992 to October 2001, 117 patients with female genital fistula who were admitted to the departments of obstetrics and gynecology, urology and general surgery were analyzed. Nine patients with congenital etiologies and 48 patients who were treated conservatively were excluded. The relationships between surgical outcome and the cause of fistula, the location of fistula, and the various surgical methods were analyzed. In spite of appropriate surgical treatment, fistulas due to cervix cancer management had the worst prognosis. In terms of location, fistula recurrence after surgical repair was most common in the bladder fundus and base. The transvaginal and transrectal approaches are suitable for fistulas located in the lower vagina. The transabdominal approach is appropriate for fistulas located in the functional portions such as the bladder and ureter, for fistulas which are difficult to expose surgically by either the vaginal or rectal approach, or in cases with severe adhesions. In cases of cervix cancer, extra care should be taken during surgical expiration or definitive radiotherapy, especially when the areas involved are the bladder fundus and base. The nature of the surgical approach should be decided by the location of the fistula, the functional importance of the area, and the degree of surgical exposure during the corrective procedures. (+info)Response of fistulating Crohn's disease to infliximab treatment assessed by magnetic resonance imaging. (3/34)
AIMS: To assess fistula track healing after infliximab treatment using magnetic resonance imaging. METHODS: Magnetic resonance imaging and clinical evaluation were performed before and after three infliximab infusions given over a 6-week period. Magnetic resonance images were evaluated for abscesses and fistula tracks. Paired magnetic resonance image examinations were rated 'better', 'unchanged' or 'worse'. Magnetic resonance imaging and clinical outcomes were then compared. RESULTS: Of the 12 referred patients, pre-treatment magnetic resonance imaging detected abscesses in three (two not treated). Of the 10 treated patients, seven had peri-anal fistulas, two of whom also had recto-vaginal fistulas, and three had abdominal wall entero-cutaneous fistulas. After infliximab, four were in remission, one had a response and five were non-responders. One developed a peri-anal abscess. Magnetic resonance imaging improved in six, was unchanged in two and was worse in two. In four of the six with improvement in magnetic resonance imaging, the fistula track resolved, but two of these had clinically persistent entero-cutaneous fistulas. The clinical outcome and magnetic resonance imaging correlated in seven of the 10 patients; in three (two entero-cutaneous and one peri-anal), there was discordance. CONCLUSIONS: Magnetic resonance imaging identifies clinically silent sepsis. Fistulas may persist despite clinical remission. Clinical response to infliximab and clinical correlation with magnetic resonance imaging were poor in patients with abdominal entero-cutaneous fistulas. (+info)Infliximab in refractory pouchitis complicated by fistulae following ileo-anal pouch for ulcerative colitis. (4/34)
AIM: To determine the efficacy of infliximab in the treatment of chronic refractory pouchitis complicated by fistulae following ileal pouch-anal anastomosis for ulcerative colitis. METHODS: This open study included seven patients (four females, three males) with chronic refractory pouchitis complicated by fistulae. Pouchitis was diagnosed by clinical, endoscopic and histological criteria. The sites of the fistulae were as follows: pouch-bladder in one, vaginal in three, perianal in two, and both vaginal and perianal in one. Extra-intestinal manifestations (erythema nodosum, arthralgia) were present in four patients. Crohn's disease was carefully excluded in all patients after re-evaluation of the history, re-examination of the original proctocolectomy specimen and examination of the proximal small bowel. All patients had been treated with antibiotics and three with steroids. Patients received infliximab, 5 mg/kg, at 0, 2 and 6 weeks. Azathioprine (2.5 mg/kg) was also started for all patients as bridge therapy. Clinical response was classified as complete, partial or no response. Fistulae closure was classified as complete (cessation of fistulae drainage and total closure of all fistulae), partial (a reduction in the number, size, drainage or discomfort associated with fistulae) or no closure. The pouchitis disease activity index and quality of life were also used as outcome measures. RESULTS: Clinically, all patients improved. At the 10-week follow-up, six of the seven patients had a complete clinical response, and five had complete fistulae closure. At the 10-week follow-up, the median pouchitis disease activity index decreased from 12 (baseline) (range, 10-15) to 5 (range, 3-8); the median quality of life decreased from 37 points (range, 33-40) to 14 (range, 9-18). Erythema nodosum and arthralgia showed complete remission soon after the first infusion of infliximab. CONCLUSIONS: These preliminary results indicate that infliximab may be recommended for the treatment of refractory pouchitis complicated by fistulae following ileal pouch-anal anastomosis for ulcerative colitis. (+info)Gynecological aspects of obstetrical delivery. (5/34)
Parturition should be looked upon as a physiological exercise, and ideally the multiparous state should be one of asymptomatic change associated with comfortable function. However, because obstetrics is a field in which serious complications may suddenly occur, the ideal is not always possible. Among the delayed effects of delivery is a group of gynecological complications which may affect the well-being of the woman so involved in later life. Such complications as uterine prolapse, cystocele, rectocele, enterocele, and genital fistula may be the grim aftermath of poor obstetric practice.The article reviews some of the advances in the prevention of maternal mortality and morbidity and emphasizes the important place of intelligent conservative obstetrics in the hands of both general physicians and specialists. (+info)Fistula response to methotrexate in Crohn's disease: a case series. (6/34)
BACKGROUND: Controlled trials have demonstrated the efficacy of methotrexate in the induction and maintenance of remission in luminal Crohn's disease; however, its effect on fistulizing disease is unknown. AIM: To describe the response to methotrexate therapy in a series of patients with fistulizing Crohn's disease. METHODS: A retrospective chart review was conducted of all patients with Crohn's disease receiving methotrexate in one practice. The response of patients with fistulizing and luminal disease was assessed using clinical and laboratory criteria. Fistula response was categorized as either complete or partial closure. RESULTS: Thirty-seven courses of methotrexate therapy were given to 33 patients with luminal and/or fistulizing Crohn's disease. In 16 patients with fistulas, four (25%) had complete closure, five (31%) had partial closure and all had failed or were intolerant to 6-mercaptopurine therapy. Overall, response to methotrexate was seen in 23 of 37 (62%) treatment courses in patients with luminal and/or fistulizing Crohn's disease. Two of the 33 patients (6%) had a significant adverse event. CONCLUSIONS: In this case series, 56% of patients with Crohn's fistulas on methotrexate showed a complete or partial response to therapy. Further studies are needed to confirm the role of methotrexate alone, and in combination with other therapies, for the treatment of fistulizing Crohn's disease. (+info)Biliary stent causing colovaginal fistula: case report. (7/34)
OBJECTIVES: Perforation of the bowel during placement of a biliary stent is a known complication of this procedure. We report the endoluminal loss of a biliary stent during routine stent extraction that ultimately led to a chronic colovaginal fistula. This case emphasizes the need for evaluation of fecal passage of stents in patients with a known dislodged prosthesis. CASE REPORT: A 65-year-old white female underwent biliary stent placement for an episode of choledocholithiasis. The stent was lost in the duodenum during routine extraction. The patient was managed expectantly. She denied ever passing this stent via the rectum and began to develop symptoms of colovaginal fistula. Evaluation found a retained biliary stent in the sigmoid colon and a fistula into the vagina. The patient underwent elective low anterior resection and colovaginal fistula repair. DISCUSSION: Reports exist of migration of stents that lead to acute colonic perforation and the need for emergent surgery. For this reason, it has been suggested that dropped or migrated stents be purposefully retrieved. However, if the option of expectant observation is used, it is important to clearly document the fecal passage of these stents and be prepared to retrieve these objects if they have a prolonged bowel transit time. (+info)Transvaginal sonographic diagnosis of a tumor fistula. (8/34)
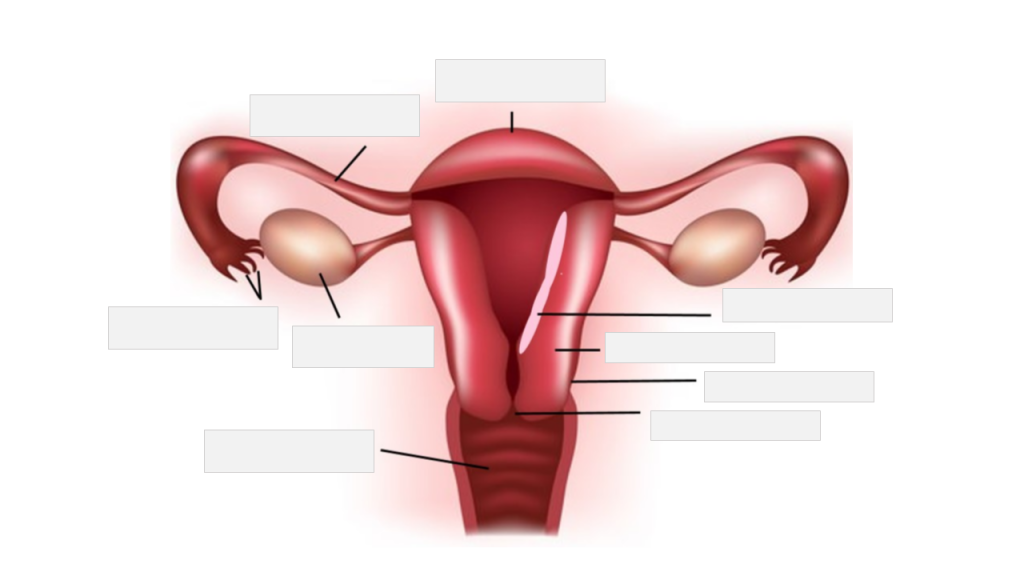
We report on two cases of advanced pelvic cancer in women who presented with profuse vaginal watery discharge. In both cases, transvaginal ultrasound revealed a fistulous tract connecting the tumor to the apex of the vaginal vault. The differential diagnoses and a review of the literature are discussed. (+info)A vaginal fistula is an abnormal opening or connection between the vagina and another organ, such as the bladder (resulting in a vesicovaginal fistula), the rectum (resulting in a rectovaginal fistula), or the colon (resulting in a colovaginal fistula). This condition can lead to various complications, including chronic urinary or fecal incontinence, infection, and difficulty with sexual intercourse.
Vaginal fistulas are often caused by obstetric trauma, such as prolonged labor, or may be the result of surgery, radiation therapy, injury, or infection. Symptoms can vary depending on the size and location of the fistula but typically include abnormal discharge, pain, and foul-smelling odor. Treatment usually involves surgical repair of the fistula, although smaller fistulas may sometimes heal on their own with proper care and management.
A fistula is an abnormal connection or passage between two organs, vessels, or body parts that usually do not connect. It can form as a result of injury, infection, surgery, or disease. A fistula can occur anywhere in the body but commonly forms in the digestive system, genital area, or urinary system. The symptoms and treatment options for a fistula depend on its location and underlying cause.
An arteriovenous fistula is an abnormal connection or passageway between an artery and a vein. This connection causes blood to flow directly from the artery into the vein, bypassing the capillary network that would normally distribute the oxygen-rich blood to the surrounding tissues.
Arteriovenous fistulas can occur as a result of trauma, disease, or as a planned surgical procedure for patients who require hemodialysis, a treatment for advanced kidney failure. In hemodialysis, the arteriovenous fistula serves as a site for repeated access to the bloodstream, allowing for efficient removal of waste products and excess fluids.
The medical definition of an arteriovenous fistula is:
"An abnormal communication between an artery and a vein, usually created by surgical means for hemodialysis access or occurring as a result of trauma, congenital defects, or disease processes such as vasculitis or neoplasm."
An intestinal fistula is an abnormal communication or connection between the intestines (or a portion of the intestine) and another organ or the skin surface. This connection forms a tract or passage, allowing the contents of the intestines, such as digestive enzymes, bacteria, and waste materials, to leak into other body areas or outside the body. Intestinal fistulas can develop due to various reasons, including inflammatory bowel diseases (like Crohn's disease), infections, complications from surgery, radiation therapy, or trauma. They can cause symptoms such as abdominal pain, diarrhea, skin irritation, and infection. Treatment of intestinal fistulas often involves a combination of medical management, nutritional support, and surgical intervention.
A cutaneous fistula is a type of fistula that occurs when a tract or tunnel forms between the skin (cutaneous) and another organ or structure, such as the gastrointestinal tract, vagina, or urinary system. Cutaneous fistulas can result from various medical conditions, including infections, inflammatory diseases, surgical complications, trauma, or malignancies.
Cutaneous fistulas may present with symptoms such as drainage of fluid or pus from the skin, pain, redness, swelling, or irritation around the affected area. The treatment for cutaneous fistulas depends on their underlying cause and can range from conservative management with antibiotics and wound care to surgical intervention.
It is essential to seek medical attention if you suspect a cutaneous fistula, as untreated fistulas can lead to complications such as infection, sepsis, or tissue damage. A healthcare professional can provide an accurate diagnosis and develop an appropriate treatment plan based on the individual's needs.
A bronchial fistula is an abnormal connection or passage between the bronchial tree (the airways in the lungs) and the surrounding tissues, such as the pleural space (the space between the lungs and the chest wall), blood vessels, or other organs. This condition can result from various causes, including lung injury, infection, surgery, or certain diseases such as cancer or tuberculosis.
Bronchial fistulas can lead to symptoms like coughing, wheezing, shortness of breath, and chest pain. They may also cause air leaks, pneumothorax (collapsed lung), or chronic infections. Treatment for bronchial fistulas depends on the underlying cause and severity of the condition but often involves surgical repair or closure of the abnormal connection.
A vascular fistula is an abnormal connection or passage between the artery and vein, which usually results from a surgical procedure to create access for hemodialysis in patients with chronic kidney disease. This communication allows blood to flow directly from the artery into the vein, bypassing the capillary network and causing high-flow conditions in the affected area. Over time, the increased pressure and flow can lead to various complications such as venous hypertension, stenosis, aneurysm formation, or even heart failure if left untreated. Vascular fistulas may also occur spontaneously due to certain medical conditions like vasculitis, trauma, or infection, although this is less common.
A rectal fistula is an abnormal connection or tunnel that develops between the rectum, which is the lower end of the colon, and another organ or the skin surface surrounding the anus. This condition often results from inflammation, infection, trauma, or surgery in the anal area. The fistula can cause symptoms such as pain, discharge, irritation, and swelling around the anus. In some cases, it may also lead to complications like abscesses or recurrent infections if not treated promptly and effectively. Treatment options typically include surgical intervention to close the fistula and promote healing of the affected tissues.
A gastric fistula is an abnormal connection or passage between the stomach and another organ or the skin surface. This condition can occur as a result of complications from surgery, injury, infection, or certain diseases such as cancer. Symptoms may include persistent drainage from the site of the fistula, pain, malnutrition, and infection. Treatment typically involves surgical repair of the fistula and management of any underlying conditions.
A urinary fistula is an abnormal connection or passage between the urinary tract and another organ or tissue, such as the bladder, ureter, or kidney, and the skin, vagina, or intestine. This condition can lead to urine leakage through the abnormal opening, causing discomfort, infection, and other complications if not treated promptly and effectively. Urinary fistulas can be caused by various factors, including surgery, injury, radiation therapy, inflammation, or cancer. The type and location of the fistula will determine the specific symptoms and treatment options.
An esophageal fistula is an abnormal connection or passage between the esophagus (the tube that carries food and liquids from the throat to the stomach) and another organ, such as the trachea (windpipe) or the skin. This condition can result from complications of certain medical conditions, including cancer, prolonged infection, or injury to the esophagus.
Esophageal fistulas can cause a variety of symptoms, including difficulty swallowing, coughing, chest pain, and fever. They can also lead to serious complications, such as pneumonia or sepsis, if left untreated. Treatment for an esophageal fistula typically involves surgical repair of the abnormal connection, along with management of any underlying conditions that may have contributed to its development.
A biliary fistula is an abnormal connection or passage between the biliary system (which includes the gallbladder, bile ducts, and liver) and another organ or structure, usually in the abdominal cavity. This connection allows bile, which is a digestive fluid produced by the liver, to leak out of its normal pathway and into other areas of the body.
Biliary fistulas can occur as a result of trauma, surgery, infection, or inflammation in the biliary system. Symptoms may include abdominal pain, fever, jaundice (yellowing of the skin and eyes), nausea, vomiting, and clay-colored stools. Treatment typically involves addressing the underlying cause of the fistula, such as draining an infection or repairing damaged tissue, and diverting bile flow away from the site of the leak. In some cases, surgery may be necessary to repair the fistula.
 Wartime sexual violence
Wartime sexual violence