Hyperaldosteronism
Aldosterone
Hypokalemia
Aldosterone Synthase
Spironolactone
Adrenocortical Adenoma
Steroid 11-beta-Hydroxylase
Mineralocorticoid Receptor Antagonists
Gitelman Syndrome
Adrenal Glands
Renin
Polydipsia
Hypertension
Mineralocorticoids
18-Hydroxydesoxycorticosterone
Adrenocortical Hyperfunction
Adrenal Hyperplasia, Congenital
G Protein-Coupled Inwardly-Rectifying Potassium Channels
Adrenocorticotropic Hormone
Myelolipoma
Potassium
Hyperplasia
Hydrocortisone
Receptors, Mineralocorticoid
Sodium
Antihypertensive Agents
Tomography, X-Ray Computed
Glucocorticoids
Primary aldosteronism with aldosterone-producing adrenal adenoma in a pregnant woman. (1/516)
A 30-year-old pregnant woman complained of muscle weakness at 29 weeks' gestation. She was hypertensive with severe hypokalemia. Lower plasma renin activity and higher aldosterone level than the normal values in pregnancy suggested primary aldosteronism. A cesarean delivery was performed at 31 weeks' gestation because of pulmonary congestion. The neonatal course was uncomplicated. The laparoscopic adrenalectomy for a 2.0-cm right adrenal adenoma resulted in normalizing of her blood pressure and serum potassium level. Although primary aldosteronism is rare, especially during pregnancy, it should be always considered as one of etiologies of hypertension in pregnancy. (+info)A case of aldosterone-producing adenoma with severe postoperative hyperkalemia. (2/516)
It is known that some patients with primary aldosteronism show postoperative hyperkalemia, which is due to inability of the adrenal gland to secrete sufficient amounts of aldosterone. However, hyperkalemia is generally neither severe nor prolonged, in which replacement therapy with mineralocorticoid is seldom necessary. We report a case of a 46-year-old woman with an aldosterone-producing adenoma associated with severe postoperative hyperkalemia. After unilateral adrenalectomy, the patient showed episodes of severe hyperkalemia for four months, which required not only cation-exchange resin, but also mineralocorticoid replacement. Plasma aldosterone concentration (PAC) was low, although PAC was increased after rapid ACTH test. Histological examination indicated the presence of adrenocortical tumor and paradoxical hyperplasia of zona glomerulosa in the adjacent adrenal. Immunohistochemistry demonstrated that the enzymes involved in aldosterone synthesis, such as cholesterol side chain cleavage (P-450scc), 3beta-hydroxysteroid dehydrogenase (3beta-HSD), and 21-hydroxylase (P-450c21), or the enzyme involved in glucocorticoid synthesis, 11beta-hydroxylase (P-450c11beta), were expressed in the tumor, but they were completely absent in zona glomerulosa of the adjacent adrenal. These findings were consistent with the patterns of primary aldosteronism. Serum potassium level was gradually decreased with concomitant increase in PAC. These results suggest that severe postoperative hyperkalemia of the present case was attributable to severe suppression of aldosterone synthesis in the adjacent and contralateral adrenal, which resulted in slow recovery of aldosterone secretion. It is plausible that aldosterone synthesis of adjacent and contralateral adrenal glands is severely impaired in some cases with primary aldosteronism, as glucocorticoid synthesis in Cushing syndrome. (+info)Gene targeting approaches to analyzing hypertension. (3/516)
Essential hypertension probably results from combinations of small genetic variations that are partly normal variations and may not be appreciably harmful individually. Strategies to identify genes contributing to hypertension are discussed in this review. Gene targeting approaches, especially gene titration, have been used in these studies of hypertension. Gene titration experiments vary the expression of a chosen gene product by generating animals having different numbers of copies of the gene coding for the product. Gene titration is powerful for analyzing quantitative variations seen in common polygenic disorders, such as kidney diseases, diabetes mellitus, and atherosclerosis, as well as hypertension, because it allows tests of causation by determining the effects on a phenotype by changes in expression of the altered gene and because it matches normal quantitative variations more closely than is possible with classic transgenic mice. The use of zero-copy (gene "knockout") animals generated by gene disruption for studies of qualitative gene effects is also discussed. These various gene targeting experiments help identify genes regulating BP, promote a better understanding of the pathophysiology of the condition, and help identify potential targets for therapies. (+info)Maximizing efficacy of endocrine tests: importance of decision-focused testing strategies and appropriate patient preparation. (4/516)
The efficacy of endocrine tests depends on the choice of tests, the preparation of the patients, the integrity of the specimens, the quality of the measurements, and the validity of the reference data. Close dialogue among the clinicians, the laboratory, and the patients is a key factor for optimal patient care. The characteristics of urine and plasma samples and the advantages and limitations of paired test measurements are presented. The importance of test sequence strategies, provocative or inhibitory procedures, and elimination of drug interferences is illustrated with four cases involving Cushing syndrome, pheochromocytoma, primary aldosteronism, and hypercalcemia. For each of these scenarios, key clinical issues are highlighted, along with discussions of the best test strategies, including which medications are likely to interfere. The importance of targeting laboratory tests to answer well-focused clinical decisions is emphasized. The roles of some time-honored provocative procedures are questioned in light of more sensitive and specific analytic methods. The importance of decision-focused analytical tolerance limits is emphasized by demonstrating the impact of analytic bias on downstream medical resource utilization. User-friendly support systems to facilitate the implementation of test strategies and postanalytic tracking of patient outcomes are presented as essential requirements for quality medical practice. (+info)A probable relationship between an endogenous digitalis-like substance and concentric cardiac hypertrophy in primary aldosteronism. (5/516)
A 44-year-old woman was admitted to our hospital due to severe hypertension. An electrocardiogram (ECG) and an echocardiogram showed severe left ventricular hypertrophy. Her plasma aldosterone level was elevated. Magnetic resonance imaging revealed a small mass in the right adrenal gland. Before removal of the tumor, plasma endogenous digitalis-like substance (EDLS) levels were elevated. After removal of the tumor, EDLS levels quickly returned to the normal level. A series of echocardiograms and ECGs over a 6- year period after removal of the tumor showed marked regression of cardiac hypertrophy. These findings suggest that EDLS may be closely related to the development of concentric cardiac hypertrophy in primary aldosteronism. (+info)Aldosterone-producing adenoma without hypertension: a report of two cases. (6/516)
Normotensive primary hyperaldosteronism is exceedingly rare. We report two new cases of this syndrome in two middle-aged women, one of Asian origin. The presenting signs were tetany in one case and an adrenal mass in the other. Neither patient had hypertension, despite repeated measurements with a manual armlet. A typical biological profile of primary hyperaldosteronism was demonstrated in both patients, including hypokalemia with inappropriate kaliuresis, elevated resting plasma aldosterone, and undetectable plasma renin activity. The circadian rhythm of blood pressure was studied by ambulatory monitoring pre- and post-operatively. It confirmed the lack of hypertension, but the circadian rhythm of blood pressure was lost before surgery in one patient. Surgical removal of the histologically typical aldosterone-producing adenomas normalized the kalemia. The main finding in these two patients was spontaneously low blood pressure in the post-operative period. This suggests that excess aldosterone induced relative hypertension in these patients whose blood pressure was spontaneously very low. Genetic screening for dexamethasone-sensitive hyperaldosteronism was negative in both patients. (+info)Accuracy of CT scanning and adrenal vein sampling in the pre-operative localization of aldosterone-secreting adrenal adenomas. (7/516)
In primary hyperaldosteronism, it is important to distinguish between unilateral and bilateral disease, as management strategies differ. In the period 1983-95, we identified 34 patients with primary hyperaldosteronism. Following further investigations, a diagnosis of aldosterone-secreting adenoma was made in 17 patients, and surgery was performed. Computed tomography clearly localized an apparent adenoma (discrete adenoma=1 cm diameter; normal contralateral gland) in only 10 of these patients (59%); two of these 'adenomas' were subsequently shown to be hyperplastic glands without adenomas. Histological examination showed adrenal adenomas in the remaining 15 patients. An 'adenoma' also appeared to be clearly localized in 3/17 patients later classified as having bilateral adrenal hyperplasia by adrenal vein sampling. CT scanning, therefore clearly localizes adenomas in only 50% of histologically proven cases, and can also produce misleading results. Adrenal vein sampling results altered our management approach in one third of cases. On the basis of our detailed results we would recommend surgery if there is clear evidence of unilateral aldosterone secretion along with CT findings which may not be strictly localizing but are in keeping with the dominant side on adrenal vein sampling. The decision to refer for surgery in primary hyperaldosteronism can be difficult, and we would caution against too heavy a reliance on CT results when recommending adrenalectomy, and suggest that adrenal vein sampling should remain a routine part of the investigation of patients with primary hyperaldosteronism. (+info)Hyperaldosteronemia in rabbits inhibits the cardiac sarcolemmal Na(+)-K(+) pump. (8/516)
Aldosterone upregulates the Na(+)-K(+) pump in kidney and colon, classical target organs for the hormone. An effect on pump function in the heart is not firmly established. Because the myocardium contains mineralocorticoid receptors, we examined whether aldosterone has an effect on Na(+)-K(+) pump function in cardiac myocytes. Myocytes were isolated from rabbits given aldosterone via osmotic minipumps and from controls. Electrogenic Na(+)-K(+) pump current, arising from the 3:2 Na(+):K(+) exchange ratio, was measured in single myocytes using the whole-cell patch clamp technique. Treatment with aldosterone induced a decrease in pump current measured when myocytes were dialyzed with patch pipette solution containing Na(+) in a concentration of 10 mmol/L, whereas there was no effect measured when the solution contained 80 mmol/L Na(+). Aldosterone had no effect on myocardial Na(+)-K(+) pump concentration evaluated by vanadate-facilitated [(3)H]ouabain binding or by K(+)-dependent paranitrophenylphosphatase activity in crude homogenates. Aldosterone induced an increase in intracellular Na(+) activity. The aldosterone-induced decrease in pump current and increased intracellular Na(+) were prevented by cotreatment with the mineralocorticoid receptor antagonist spironolactone. Our results indicate that hyperaldosteronemia decreases the apparent Na(+) affinity of the Na(+)-K(+) pump, whereas it has no effect on maximal pump capacity. (+info)Hyperaldosteronism is a medical condition characterized by the overproduction of aldosterone, a hormone produced by the adrenal glands. Aldosterone helps regulate sodium and potassium balance and blood pressure by promoting sodium retention and potassium excretion in the kidneys.
There are two types of hyperaldosteronism: primary and secondary. Primary hyperaldosteronism is caused by an overproduction of aldosterone from an abnormality within the adrenal gland, such as a tumor (Conn's syndrome) or hyperplasia. Secondary hyperaldosteronism occurs when there is an excess production of renin, a hormone produced by the kidneys, which then stimulates the adrenal glands to produce more aldosterone. This can be caused by various conditions that affect kidney function, such as renal artery stenosis or heart failure.
Symptoms of hyperaldosteronism may include high blood pressure, low potassium levels (hypokalemia), muscle weakness, and frequent urination. Diagnosis typically involves measuring aldosterone and renin levels in the blood, as well as other tests to determine the underlying cause. Treatment depends on the type and cause of hyperaldosteronism but may include medications, surgery, or lifestyle changes.
Aldosterone is a hormone produced by the adrenal gland. It plays a key role in regulating sodium and potassium balance and maintaining blood pressure through its effects on the kidneys. Aldosterone promotes the reabsorption of sodium ions and the excretion of potassium ions in the distal tubules and collecting ducts of the nephrons in the kidneys. This increases the osmotic pressure in the blood, which in turn leads to water retention and an increase in blood volume and blood pressure.
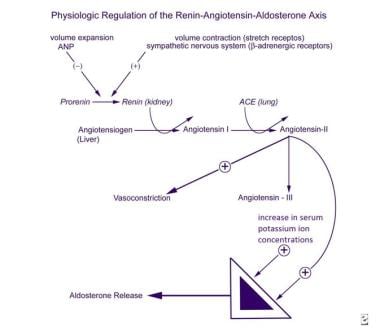
Aldosterone is released from the adrenal gland in response to a variety of stimuli, including angiotensin II (a peptide hormone produced as part of the renin-angiotensin-aldosterone system), potassium ions, and adrenocorticotropic hormone (ACTH) from the pituitary gland. The production of aldosterone is regulated by a negative feedback mechanism involving sodium levels in the blood. High sodium levels inhibit the release of aldosterone, while low sodium levels stimulate its release.
In addition to its role in maintaining fluid and electrolyte balance and blood pressure, aldosterone has been implicated in various pathological conditions, including hypertension, heart failure, and primary hyperaldosteronism (a condition characterized by excessive production of aldosterone).
Hypokalemia is a medical condition characterized by abnormally low potassium levels in the blood, specifically when the concentration falls below 3.5 milliequivalents per liter (mEq/L). Potassium is an essential electrolyte that helps regulate heart function, nerve signals, and muscle contractions.
Hypokalemia can result from various factors, including inadequate potassium intake, increased potassium loss through the urine or gastrointestinal tract, or shifts of potassium between body compartments. Common causes include diuretic use, vomiting, diarrhea, certain medications, kidney diseases, and hormonal imbalances.
Mild hypokalemia may not cause noticeable symptoms but can still affect the proper functioning of muscles and nerves. More severe cases can lead to muscle weakness, fatigue, cramps, paralysis, heart rhythm abnormalities, and in rare instances, respiratory failure or cardiac arrest. Treatment typically involves addressing the underlying cause and replenishing potassium levels through oral or intravenous (IV) supplementation, depending on the severity of the condition.
Aldosterone synthase is a steroidogenic enzyme that is primarily responsible for the production of the hormone aldosterone in the adrenal gland. It is encoded by the CYP11B2 gene and is located within the mitochondria of the zona glomerulosa cells in the adrenal cortex.
Aldosterone synthase catalyzes two key reactions in the biosynthesis of aldosterone: the conversion of corticosterone to 18-hydroxycorticosterone and the subsequent conversion of 18-hydroxycorticosterone to aldosterone. These reactions involve the sequential addition of hydroxyl groups at the C18 position of the steroid molecule, which is a critical step in the synthesis of aldosterone.
Aldosterone plays an important role in regulating blood pressure and electrolyte balance by increasing the reabsorption of sodium and water in the distal nephron of the kidney, while promoting the excretion of potassium. Disorders of aldosterone synthase can lead to conditions such as primary hyperaldosteronism, which is characterized by excessive production of aldosterone and can result in hypertension and hypokalemia.
Spironolactone is a prescription medication that belongs to a class of drugs known as potassium-sparing diuretics. It works by blocking the action of aldosterone, a hormone that helps regulate sodium and potassium balance in your body. This results in increased urine production (diuresis) and decreased salt and fluid retention.
Spironolactone is primarily used to treat edema (fluid buildup) associated with heart failure, liver cirrhosis, or kidney disease. It's also prescribed for the treatment of high blood pressure and primary hyperaldosteronism, a condition where the adrenal glands produce too much aldosterone.
Furthermore, spironolactone is used off-label to treat conditions such as acne, hirsutism (excessive hair growth in women), and hormone-sensitive breast cancer in postmenopausal women.
It's important to note that spironolactone can cause increased potassium levels in the blood (hyperkalemia) and should be used with caution in patients with kidney impairment or those taking other medications that affect potassium balance. Regular monitoring of electrolyte levels, including potassium and sodium, is essential during spironolactone therapy.
Adrenal gland neoplasms refer to abnormal growths or tumors in the adrenal glands. These glands are located on top of each kidney and are responsible for producing hormones that regulate various bodily functions such as metabolism, blood pressure, and stress response. Adrenal gland neoplasms can be benign (non-cancerous) or malignant (cancerous).
Benign adrenal tumors are called adenomas and are usually small and asymptomatic. However, some adenomas may produce excessive amounts of hormones, leading to symptoms such as high blood pressure, weight gain, and mood changes.
Malignant adrenal tumors are called adrenocortical carcinomas and are rare but aggressive cancers that can spread to other parts of the body. Symptoms of adrenocortical carcinoma may include abdominal pain, weight loss, and hormonal imbalances.
It is important to diagnose and treat adrenal gland neoplasms early to prevent complications and improve outcomes. Diagnostic tests may include imaging studies such as CT scans or MRIs, as well as hormone level testing and biopsy. Treatment options may include surgery, radiation therapy, chemotherapy, or a combination of these approaches.
An adrenocortical adenoma is a benign tumor that arises from the cells of the adrenal cortex, which is the outer layer of the adrenal gland. These tumors can produce and release various hormones, such as cortisol, aldosterone, or androgens, depending on the type of cells they originate from.
Most adrenocortical adenomas are nonfunctioning, meaning that they do not secrete excess hormones and may not cause any symptoms. However, some functioning adenomas can produce excessive amounts of hormones, leading to a variety of clinical manifestations. For example:
* Cortisol-secreting adenomas can result in Cushing's syndrome, characterized by weight gain, muscle wasting, thin skin, easy bruising, and mood changes.
* Aldosterone-producing adenomas can cause Conn's syndrome, marked by hypertension (high blood pressure), hypokalemia (low potassium levels), and metabolic alkalosis.
* Androgen-secreting adenomas may lead to hirsutism (excessive hair growth) or virilization (development of male secondary sexual characteristics) in women.
The diagnosis of an adrenocortical adenoma typically involves imaging tests, such as CT or MRI scans, and hormonal evaluations to determine if the tumor is functioning or not. Treatment usually consists of surgical removal of the tumor, especially if it is causing hormonal imbalances or growing in size.
Steroid 11-beta-hydroxylase is a crucial enzyme involved in the steroidogenesis pathway, specifically in the synthesis of cortisol and aldosterone, which are vital hormones produced by the adrenal glands. This enzyme is encoded by the CYP11B1 gene in humans.
The enzyme's primary function is to catalyze the conversion of 11-deoxycortisol to cortisol and 11-deoxycorticosterone to aldosterone through the process of hydroxylation at the 11-beta position of the steroid molecule. Cortisol is a critical glucocorticoid hormone that helps regulate metabolism, immune response, and stress response, while aldosterone is a mineralocorticoid hormone responsible for maintaining electrolyte and fluid balance in the body.
Deficiencies or mutations in the CYP11B1 gene can lead to various disorders, such as congenital adrenal hyperplasia (CAH), which may result in impaired cortisol and aldosterone production, causing hormonal imbalances and associated symptoms.
Adrenalectomy is a surgical procedure in which one or both adrenal glands are removed. The adrenal glands are small, triangular-shaped glands located on top of each kidney that produce hormones such as cortisol, aldosterone, and adrenaline (epinephrine).
There are several reasons why an adrenalectomy may be necessary. For example, the procedure may be performed to treat tumors or growths on the adrenal glands, such as pheochromocytomas, which can cause high blood pressure and other symptoms. Adrenalectomy may also be recommended for patients with Cushing's syndrome, a condition in which the body is exposed to too much cortisol, or for those with adrenal cancer.
During an adrenalectomy, the surgeon makes an incision in the abdomen or back and removes the affected gland or glands. In some cases, laparoscopic surgery may be used, which involves making several small incisions and using specialized instruments to remove the gland. After the procedure, patients may need to take hormone replacement therapy to compensate for the loss of adrenal gland function.
Mineralocorticoid receptor antagonists (MRAs) are a class of medications that block the action of aldosterone, a hormone produced by the adrenal glands. Aldosterone helps regulate sodium and potassium balance and blood pressure by binding to mineralocorticoid receptors in the kidneys, heart, blood vessels, and brain.
When aldosterone binds to these receptors, it promotes sodium retention and potassium excretion, which can lead to an increase in blood volume and blood pressure. MRAs work by blocking the binding of aldosterone to its receptors, thereby preventing these effects.
MRAs are primarily used to treat heart failure, hypertension, and kidney disease. By reducing sodium retention and increasing potassium excretion, MRAs can help lower blood pressure, reduce fluid buildup in the body, and improve heart function. Examples of MRAs include spironolactone and eplerenone.
Gitelman Syndrome is a genetic disorder that affects the electrolyte and fluid balance in the body. It is characterized by low levels of potassium, magnesium, and chloride in the blood due to defects in the function of the distal convoluted tubule in the kidney. This results in increased urinary excretion of these ions.
The condition is caused by mutations in the SLC12A3 gene, which provides instructions for making a protein called thiazide-sensitive sodium chloride cotransporter (NCC). The NCC protein is responsible for reabsorbing sodium and chloride ions from the urine back into the bloodstream. In Gitelman Syndrome, the mutations in the SLC12A3 gene lead to reduced function of the NCC protein, resulting in increased excretion of sodium, chloride, potassium, and magnesium in the urine.
Symptoms of Gitelman Syndrome may include muscle weakness, cramps, spasms, fatigue, salt cravings, thirst, and decreased appetite. The condition is usually diagnosed in childhood or adolescence but can also present in adulthood. Treatment typically involves supplementation with potassium and magnesium to correct the electrolyte imbalances. In some cases, a medication called indapamide may be used to increase sodium reabsorption in the kidney and reduce potassium excretion.
The adrenal glands are a pair of endocrine glands that are located on top of the kidneys. Each gland has two parts: the outer cortex and the inner medulla. The adrenal cortex produces hormones such as cortisol, aldosterone, and androgens, which regulate metabolism, blood pressure, and other vital functions. The adrenal medulla produces catecholamines, including epinephrine (adrenaline) and norepinephrine (noradrenaline), which help the body respond to stress by increasing heart rate, blood pressure, and alertness.
Renin is a medically recognized term and it is defined as:
"A protein (enzyme) that is produced and released by specialized cells (juxtaglomerular cells) in the kidney. Renin is a key component of the renin-angiotensin-aldosterone system (RAAS), which helps regulate blood pressure and fluid balance in the body.
When the kidney detects a decrease in blood pressure or a reduction in sodium levels, it releases renin into the bloodstream. Renin then acts on a protein called angiotensinogen, converting it to angiotensin I. Angiotensin-converting enzyme (ACE) subsequently converts angiotensin I to angiotensin II, which is a potent vasoconstrictor that narrows blood vessels and increases blood pressure.
Additionally, angiotensin II stimulates the adrenal glands to release aldosterone, a hormone that promotes sodium reabsorption in the kidneys and increases water retention, further raising blood pressure.
Therefore, renin plays a critical role in maintaining proper blood pressure and electrolyte balance in the body."
Adrenal cortex neoplasms refer to abnormal growths (tumors) in the adrenal gland's outer layer, known as the adrenal cortex. These neoplasms can be benign or malignant (cancerous). Benign tumors are called adrenal adenomas, while cancerous tumors are called adrenocortical carcinomas.
Adrenal cortex neoplasms can produce various hormones, leading to different clinical presentations. For instance, they may cause Cushing's syndrome (characterized by excessive cortisol production), Conn's syndrome (caused by aldosterone excess), or virilization (due to androgen excess). Some tumors may not produce any hormones and are discovered incidentally during imaging studies for unrelated conditions.
The diagnosis of adrenal cortex neoplasms typically involves a combination of imaging techniques, such as CT or MRI scans, and hormonal assessments to determine if the tumor is functional or non-functional. In some cases, a biopsy may be necessary to confirm the diagnosis and differentiate between benign and malignant tumors. Treatment options depend on the type, size, location, and hormonal activity of the neoplasm and may include surgical excision, radiation therapy, chemotherapy, or a combination of these approaches.
Polydipsia is a medical term that describes excessive thirst or an abnormally increased desire to drink fluids. It is often associated with conditions that cause increased fluid loss, such as diabetes insipidus and diabetes mellitus, as well as certain psychiatric disorders that can lead to excessive water intake. Polydipsia should not be confused with simple dehydration, where the body's overall water content is reduced due to inadequate fluid intake or excessive fluid loss. Instead, polydipsia refers to a persistent and strong drive to drink fluids, even when the body is adequately hydrated. Prolonged polydipsia can lead to complications such as hyponatremia (low sodium levels in the blood) and may indicate an underlying medical issue that requires further evaluation and treatment.
18-Hydroxycorticosterone is a steroid hormone that is produced in the adrenal gland. It is an intermediate in the biosynthesis of aldosterone, which is the major hormone responsible for regulating sodium and potassium balance in the body. 18-Hydroxycorticosterone gets its name from the hydroxyl group (-OH) that is added to the 18th carbon atom of the steroid molecule.
This hormone plays a role in the body's response to stress and helps to regulate various physiological processes, including metabolism, immune function, and sexual development and reproduction. However, abnormal levels of 18-hydroxycorticosterone have been associated with certain medical conditions, such as primary aldosteronism, which is a condition characterized by the overproduction of aldosterone.
It's important to note that while 18-hydroxycorticosterone is an important hormone in the body, it is not typically measured in routine clinical testing. Instead, tests for aldosterone and related hormones are more commonly used to diagnose and manage conditions related to the adrenal gland.
Canrenone is a synthetic steroid hormone that is used primarily as a diuretic to treat high blood pressure and edema (fluid retention) associated with heart, kidney, or liver disease. It works by increasing the amount of salt and water that the kidneys remove from the blood, which helps to reduce fluid buildup in the body. Canrenone is also known as a "aldosterone antagonist" because it blocks the action of aldosterone, a hormone that regulates sodium and potassium balance in the body.
Canrenone is not available as a standalone medication in many countries, but is instead found in combination with other medications such as spironolactone. It is important to note that canrenone and other aldosterone antagonists may increase potassium levels in the blood, so regular monitoring of potassium levels is necessary during treatment.
Here are some medical resources where you can find more information about Canrenone:
* National Library of Medicine's MedlinePlus:
* Drugs.com:
* Mayo Clinic:
An adenoma is a benign (noncancerous) tumor that develops from glandular epithelial cells. These types of cells are responsible for producing and releasing fluids, such as hormones or digestive enzymes, into the surrounding tissues. Adenomas can occur in various organs and glands throughout the body, including the thyroid, pituitary, adrenal, and digestive systems.
Depending on their location, adenomas may cause different symptoms or remain asymptomatic. Some common examples of adenomas include:
1. Colorectal adenoma (also known as a polyp): These growths occur in the lining of the colon or rectum and can develop into colorectal cancer if left untreated. Regular screenings, such as colonoscopies, are essential for early detection and removal of these polyps.
2. Thyroid adenoma: This type of adenoma affects the thyroid gland and may result in an overproduction or underproduction of hormones, leading to conditions like hyperthyroidism (overactive thyroid) or hypothyroidism (underactive thyroid).
3. Pituitary adenoma: These growths occur in the pituitary gland, which is located at the base of the brain and controls various hormonal functions. Depending on their size and location, pituitary adenomas can cause vision problems, headaches, or hormonal imbalances that affect growth, reproduction, and metabolism.
4. Liver adenoma: These rare benign tumors develop in the liver and may not cause any symptoms unless they become large enough to press on surrounding organs or structures. In some cases, liver adenomas can rupture and cause internal bleeding.
5. Adrenal adenoma: These growths occur in the adrenal glands, which are located above the kidneys and produce hormones that regulate stress responses, metabolism, and blood pressure. Most adrenal adenomas are nonfunctioning, meaning they do not secrete excess hormones. However, functioning adrenal adenomas can lead to conditions like Cushing's syndrome or Conn's syndrome, depending on the type of hormone being overproduced.
It is essential to monitor and manage benign tumors like adenomas to prevent potential complications, such as rupture, bleeding, or hormonal imbalances. Treatment options may include surveillance with imaging studies, medication to manage hormonal issues, or surgical removal of the tumor in certain cases.
Hypertension is a medical term used to describe abnormally high blood pressure in the arteries, often defined as consistently having systolic blood pressure (the top number in a blood pressure reading) over 130 mmHg and/or diastolic blood pressure (the bottom number) over 80 mmHg. It is also commonly referred to as high blood pressure.
Hypertension can be classified into two types: primary or essential hypertension, which has no identifiable cause and accounts for about 95% of cases, and secondary hypertension, which is caused by underlying medical conditions such as kidney disease, hormonal disorders, or use of certain medications.
If left untreated, hypertension can lead to serious health complications such as heart attack, stroke, heart failure, and chronic kidney disease. Therefore, it is important for individuals with hypertension to manage their condition through lifestyle modifications (such as healthy diet, regular exercise, stress management) and medication if necessary, under the guidance of a healthcare professional.
Mineralocorticoids are a class of steroid hormones that primarily regulate electrolyte and fluid balance in the body. The most important mineralocorticoid is aldosterone, which is produced by the adrenal gland in response to signals from the renin-angiotensin system. Aldosterone acts on the distal tubules and collecting ducts of the nephrons in the kidneys to increase the reabsorption of sodium ions (Na+) and water into the bloodstream, while promoting the excretion of potassium ions (K+) and hydrogen ions (H+) into the urine. This helps maintain blood pressure and volume, as well as ensuring a proper balance of electrolytes in the body. Other mineralocorticoids include cortisol and corticosterone, which have weak mineralocorticoid activity and play a more significant role as glucocorticoids, regulating metabolism and immune response.
18-Hydroxydesoxycorticosterone is a steroid hormone that is produced by the adrenal gland. It is an intermediate in the biosynthesis of aldosterone, which is the major hormone responsible for regulating sodium and potassium balance in the body. 18-Hydroxydesoxycorticosterone itself has minimal biological activity, but it is converted to aldosterone by the enzyme aldosterone synthase.
The medical relevance of 18-Hydroxydesoxycorticosterone lies in its role as a precursor to aldosterone and its potential use as a marker for certain adrenal gland disorders. For example, increased production of 18-Hydroxydesoxycorticosterone has been observed in some cases of primary hyperaldosteronism, which is a condition characterized by excessive aldosterone production leading to high blood pressure and low potassium levels. Measuring the levels of this hormone can help diagnose and manage such conditions.
Adrenocortical hyperfunction, also known as Cushing's syndrome, is a condition characterized by the overproduction of cortisol hormone from the adrenal glands. The adrenal glands are located on top of the kidneys and are responsible for producing several essential hormones, including cortisol. Cortisol helps regulate metabolism, blood pressure, and the body's response to stress.
In Adrenocortical hyperfunction, the adrenal glands produce too much cortisol, leading to a range of symptoms such as weight gain, particularly around the trunk and face, thinning of the skin, easy bruising, muscle weakness, mood changes, and high blood pressure. The condition can be caused by several factors, including tumors in the pituitary gland or adrenal glands, long-term use of corticosteroid medications, or genetic disorders that affect the adrenal glands.
Treatment for Adrenocortical hyperfunction depends on the underlying cause of the condition and may include surgery to remove tumors, medication to reduce cortisol production, or radiation therapy. It is essential to diagnose and treat this condition promptly, as long-term exposure to high levels of cortisol can lead to serious health complications such as diabetes, osteoporosis, and heart disease.
Congenital Adrenal Hyperplasia (CAH) is a group of inherited genetic disorders that affect the adrenal glands, which are triangular-shaped glands located on top of the kidneys. The adrenal glands are responsible for producing several essential hormones, including cortisol, aldosterone, and androgens.
CAH is caused by mutations in genes that code for enzymes involved in the synthesis of these hormones. The most common form of CAH is 21-hydroxylase deficiency, which affects approximately 90% to 95% of all cases. Other less common forms of CAH include 11-beta-hydroxylase deficiency and 3-beta-hydroxysteroid dehydrogenase deficiency.
The severity of the disorder can vary widely, depending on the degree of enzyme deficiency. In severe cases, the lack of cortisol production can lead to life-threatening salt wasting and electrolyte imbalances in newborns. The excess androgens produced due to the enzyme deficiency can also cause virilization, or masculinization, of female fetuses, leading to ambiguous genitalia at birth.
In milder forms of CAH, symptoms may not appear until later in childhood or even adulthood. These may include early puberty, rapid growth followed by premature fusion of the growth plates and short stature, acne, excessive hair growth, irregular menstrual periods, and infertility.
Treatment for CAH typically involves replacing the missing hormones with medications such as hydrocortisone, fludrocortisone, and/or sex hormones. Regular monitoring of hormone levels and careful management of medication doses is essential to prevent complications such as adrenal crisis, growth suppression, and osteoporosis.
In severe cases of CAH, early diagnosis and treatment can help prevent or minimize the risk of serious health problems and improve quality of life. Genetic counseling may also be recommended for affected individuals and their families to discuss the risks of passing on the disorder to future generations.
Adrenal gland diseases refer to a group of medical conditions that affect the function or structure of the adrenal glands. The adrenal glands are small, triangular-shaped glands located on top of each kidney. They are responsible for producing several essential hormones, including cortisol, aldosterone, and adrenaline (epinephrine).
There are various types of adrenal gland diseases, some of which include:
1. Adrenal Insufficiency: A condition where the adrenal glands do not produce enough hormones, particularly cortisol and aldosterone. This can lead to symptoms such as fatigue, weight loss, low blood pressure, and skin hyperpigmentation.
2. Cushing's Syndrome: A condition characterized by an excess of cortisol in the body. It can be caused by a tumor in the pituitary gland or adrenal glands, or it can result from long-term use of steroid medications.
3. Adrenal Cancer: A rare type of cancer that affects the adrenal glands. Symptoms may include abdominal pain, weight loss, and high blood pressure.
4. Pheochromocytoma: A tumor that develops in the adrenal glands and causes an overproduction of adrenaline (epinephrine) and noradrenaline (norepinephrine). Symptoms may include high blood pressure, headaches, sweating, and anxiety.
5. Adrenal Hemorrhage: A condition where bleeding occurs in the adrenal glands, often as a result of severe trauma or infection. This can lead to adrenal insufficiency and other complications.
6. Congenital Adrenal Hyperplasia: An inherited disorder that affects the production of cortisol and other hormones in the adrenal glands. Symptoms may include ambiguous genitalia, precocious puberty, and short stature.
Treatment for adrenal gland diseases varies depending on the specific condition and its severity. Treatment options may include medication, surgery, or radiation therapy.
G protein-coupled inwardly-rectifying potassium channels (GIRK channels) are a type of potassium channel that are activated by G proteins, which are molecules that help transmit signals within cells. These channels are characterized by their ability to allow potassium ions to flow into the cell more easily than they allow potassium ions to flow out of the cell, hence the term "inwardly-rectifying."
GIRK channels play a role in regulating various physiological processes, including neurotransmission, heart rate, and insulin secretion. They are activated by several different G proteins, including those that are activated by certain neurotransmitters and hormones. When these G proteins bind to the channel, they cause it to open, allowing potassium ions to flow into the cell. This can have various effects on the cell, depending on the type of cell and the specific signals being transmitted.
GIRK channels are composed of four subunits, each of which contains a pore through which potassium ions can pass. These subunits can be made up of different types of proteins, and the specific combination of subunits in a channel can affect its properties and regulation. Mutations in genes that encode GIRK channel subunits have been linked to various diseases, including certain forms of epilepsy and cardiac arrhythmias.
Adrenocorticotropic Hormone (ACTH) is a hormone produced and released by the anterior pituitary gland, a small endocrine gland located at the base of the brain. ACTH plays a crucial role in the regulation of the body's stress response and has significant effects on various physiological processes.
The primary function of ACTH is to stimulate the adrenal glands, which are triangular-shaped glands situated on top of the kidneys. The adrenal glands consist of two parts: the outer cortex and the inner medulla. ACTH specifically targets the adrenal cortex, where it binds to specific receptors and initiates a series of biochemical reactions leading to the production and release of steroid hormones, primarily cortisol (a glucocorticoid) and aldosterone (a mineralocorticoid).
Cortisol is involved in various metabolic processes, such as regulating blood sugar levels, modulating the immune response, and helping the body respond to stress. Aldosterone plays a vital role in maintaining electrolyte and fluid balance by promoting sodium reabsorption and potassium excretion in the kidneys.
ACTH release is controlled by the hypothalamus, another part of the brain, which produces corticotropin-releasing hormone (CRH). CRH stimulates the anterior pituitary gland to secrete ACTH, which in turn triggers cortisol production in the adrenal glands. This complex feedback system helps maintain homeostasis and ensures that appropriate amounts of cortisol are released in response to various physiological and psychological stressors.
Disorders related to ACTH can lead to hormonal imbalances, resulting in conditions such as Cushing's syndrome (excessive cortisol production) or Addison's disease (insufficient cortisol production). Proper diagnosis and management of these disorders typically involve assessing the function of the hypothalamic-pituitary-adrenal axis and addressing any underlying issues affecting ACTH secretion.
Myelolipoma is a type of benign tumor that occurs in the adrenal gland, which is located on top of each kidney. This tumor is composed of both fatty tissue (lipoma) and cells that are similar to those found in the bone marrow (myeloid). Myelolipomas are usually small and asymptomatic, but they can grow larger and cause symptoms such as abdominal pain or discomfort, depending on their size and location.
Myelolipomas are rare tumors that typically affect middle-aged to older adults, with a slight female predominance. They are usually discovered incidentally during imaging studies performed for other medical conditions. In most cases, myelolipomas do not require treatment unless they cause symptoms or grow large enough to pose a risk of bleeding or rupture. Surgical removal is the standard treatment for symptomatic or complicated myelolipomas.
Potassium is a essential mineral and an important electrolyte that is widely distributed in the human body. The majority of potassium in the body (approximately 98%) is found within cells, with the remaining 2% present in blood serum and other bodily fluids. Potassium plays a crucial role in various physiological processes, including:
1. Regulation of fluid balance and maintenance of normal blood pressure through its effects on vascular tone and sodium excretion.
2. Facilitation of nerve impulse transmission and muscle contraction by participating in the generation and propagation of action potentials.
3. Protein synthesis, enzyme activation, and glycogen metabolism.
4. Regulation of acid-base balance through its role in buffering systems.
The normal serum potassium concentration ranges from 3.5 to 5.0 mEq/L (milliequivalents per liter) or mmol/L (millimoles per liter). Potassium levels outside this range can have significant clinical consequences, with both hypokalemia (low potassium levels) and hyperkalemia (high potassium levels) potentially leading to serious complications such as cardiac arrhythmias, muscle weakness, and respiratory failure.
Potassium is primarily obtained through the diet, with rich sources including fruits (e.g., bananas, oranges, and apricots), vegetables (e.g., leafy greens, potatoes, and tomatoes), legumes, nuts, dairy products, and meat. In cases of deficiency or increased needs, potassium supplements may be recommended under the guidance of a healthcare professional.
Hyperplasia is a medical term that refers to an abnormal increase in the number of cells in an organ or tissue, leading to an enlargement of the affected area. It's a response to various stimuli such as hormones, chronic irritation, or inflammation. Hyperplasia can be physiological, like the growth of breast tissue during pregnancy, or pathological, like in the case of benign or malignant tumors. The process is generally reversible if the stimulus is removed. It's important to note that hyperplasia itself is not cancerous, but some forms of hyperplasia can increase the risk of developing cancer over time.
Hydrocortisone is a synthetic glucocorticoid, which is a class of steroid hormones. It is identical to the naturally occurring cortisol, a hormone produced by the adrenal gland that helps regulate metabolism and helps your body respond to stress. Hydrocortisone has anti-inflammatory effects and is used to treat various inflammatory conditions such as allergies, skin disorders, and autoimmune diseases. It works by suppressing the immune system's response to reduce swelling, redness, itching, and other symptoms caused by inflammation.
Hydrocortisone is available in different forms, including oral tablets, topical creams, lotions, gels, and ointments, as well as injectable solutions. The specific use and dosage depend on the condition being treated and the individual patient's medical history and current health status.
As with any medication, hydrocortisone can have side effects, especially when used in high doses or for extended periods. Common side effects include increased appetite, weight gain, mood changes, insomnia, and skin thinning. Long-term use of hydrocortisone may also increase the risk of developing osteoporosis, diabetes, cataracts, and other health problems. Therefore, it is essential to follow your healthcare provider's instructions carefully when using this medication.
Blood pressure is the force exerted by circulating blood on the walls of the blood vessels. It is measured in millimeters of mercury (mmHg) and is given as two figures:
1. Systolic pressure: This is the pressure when the heart pushes blood out into the arteries.
2. Diastolic pressure: This is the pressure when the heart rests between beats, allowing it to fill with blood.
Normal blood pressure for adults is typically around 120/80 mmHg, although this can vary slightly depending on age, sex, and other factors. High blood pressure (hypertension) is generally considered to be a reading of 130/80 mmHg or higher, while low blood pressure (hypotension) is usually defined as a reading below 90/60 mmHg. It's important to note that blood pressure can fluctuate throughout the day and may be affected by factors such as stress, physical activity, and medication use.
Medical Definition:
Mineralocorticoid Receptors (MRs) are a type of nuclear receptor protein that are activated by the binding of mineralocorticoid hormones, such as aldosterone. These receptors are expressed in various tissues and cells, including the kidneys, heart, blood vessels, and brain.
When activated, MRs regulate gene expression related to sodium and potassium homeostasis, water balance, and electrolyte transport. This is primarily achieved through the regulation of ion channels and transporters in the distal nephron of the kidney, leading to increased sodium reabsorption and potassium excretion.
Abnormalities in mineralocorticoid receptor function have been implicated in several diseases, including hypertension, heart failure, and primary aldosteronism.
Sodium is an essential mineral and electrolyte that is necessary for human health. In a medical context, sodium is often discussed in terms of its concentration in the blood, as measured by serum sodium levels. The normal range for serum sodium is typically between 135 and 145 milliequivalents per liter (mEq/L).
Sodium plays a number of important roles in the body, including:
* Regulating fluid balance: Sodium helps to regulate the amount of water in and around your cells, which is important for maintaining normal blood pressure and preventing dehydration.
* Facilitating nerve impulse transmission: Sodium is involved in the generation and transmission of electrical signals in the nervous system, which is necessary for proper muscle function and coordination.
* Assisting with muscle contraction: Sodium helps to regulate muscle contractions by interacting with other minerals such as calcium and potassium.
Low sodium levels (hyponatremia) can cause symptoms such as confusion, seizures, and coma, while high sodium levels (hypernatremia) can lead to symptoms such as weakness, muscle cramps, and seizures. Both conditions require medical treatment to correct.
Veins are blood vessels that carry deoxygenated blood from the tissues back to the heart. They have a lower pressure than arteries and contain valves to prevent the backflow of blood. Veins have a thin, flexible wall with a larger lumen compared to arteries, allowing them to accommodate more blood volume. The color of veins is often blue or green due to the absorption characteristics of light and the reduced oxygen content in the blood they carry.
Diuretics are a type of medication that increase the production of urine and help the body eliminate excess fluid and salt. They work by interfering with the reabsorption of sodium in the kidney tubules, which in turn causes more water to be excreted from the body. Diuretics are commonly used to treat conditions such as high blood pressure, heart failure, liver cirrhosis, and kidney disease. There are several types of diuretics, including loop diuretics, thiazide diuretics, potassium-sparing diuretics, and osmotic diuretics, each with its own mechanism of action and potential side effects. It is important to use diuretics under the guidance of a healthcare professional, as they can interact with other medications and have an impact on electrolyte balance in the body.
Antihypertensive agents are a class of medications used to treat high blood pressure (hypertension). They work by reducing the force and rate of heart contractions, dilating blood vessels, or altering neurohormonal activation to lower blood pressure. Examples include diuretics, beta blockers, ACE inhibitors, ARBs, calcium channel blockers, and direct vasodilators. These medications may be used alone or in combination to achieve optimal blood pressure control.
Dexamethasone is a type of corticosteroid medication, which is a synthetic version of a natural hormone produced by the adrenal glands. It is often used to reduce inflammation and suppress the immune system in a variety of medical conditions, including allergies, asthma, rheumatoid arthritis, and certain skin conditions.
Dexamethasone works by binding to specific receptors in cells, which triggers a range of anti-inflammatory effects. These include reducing the production of chemicals that cause inflammation, suppressing the activity of immune cells, and stabilizing cell membranes.
In addition to its anti-inflammatory effects, dexamethasone can also be used to treat other medical conditions, such as certain types of cancer, brain swelling, and adrenal insufficiency. It is available in a variety of forms, including tablets, liquids, creams, and injectable solutions.
Like all medications, dexamethasone can have side effects, particularly if used for long periods of time or at high doses. These may include mood changes, increased appetite, weight gain, acne, thinning skin, easy bruising, and an increased risk of infections. It is important to follow the instructions of a healthcare provider when taking dexamethasone to minimize the risk of side effects.
X-ray computed tomography (CT or CAT scan) is a medical imaging method that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional (tomographic) images (virtual "slices") of the body. These cross-sectional images can then be used to display detailed internal views of organs, bones, and soft tissues in the body.
The term "computed tomography" is used instead of "CT scan" or "CAT scan" because the machines take a series of X-ray measurements from different angles around the body and then use a computer to process these data to create detailed images of internal structures within the body.
CT scanning is a noninvasive, painless medical test that helps physicians diagnose and treat medical conditions. CT imaging provides detailed information about many types of tissue including lung, bone, soft tissue and blood vessels. CT examinations can be performed on every part of the body for a variety of reasons including diagnosis, surgical planning, and monitoring of therapeutic responses.
In computed tomography (CT), an X-ray source and detector rotate around the patient, measuring the X-ray attenuation at many different angles. A computer uses this data to construct a cross-sectional image by the process of reconstruction. This technique is called "tomography". The term "computed" refers to the use of a computer to reconstruct the images.
CT has become an important tool in medical imaging and diagnosis, allowing radiologists and other physicians to view detailed internal images of the body. It can help identify many different medical conditions including cancer, heart disease, lung nodules, liver tumors, and internal injuries from trauma. CT is also commonly used for guiding biopsies and other minimally invasive procedures.
In summary, X-ray computed tomography (CT or CAT scan) is a medical imaging technique that uses computer-processed combinations of many X-ray images taken from different angles to produce cross-sectional images of the body. It provides detailed internal views of organs, bones, and soft tissues in the body, allowing physicians to diagnose and treat medical conditions.
Glucocorticoids are a class of steroid hormones that are naturally produced in the adrenal gland, or can be synthetically manufactured. They play an essential role in the metabolism of carbohydrates, proteins, and fats, and have significant anti-inflammatory effects. Glucocorticoids suppress immune responses and inflammation by inhibiting the release of inflammatory mediators from various cells, such as mast cells, eosinophils, and lymphocytes. They are frequently used in medical treatment for a wide range of conditions, including allergies, asthma, rheumatoid arthritis, dermatological disorders, and certain cancers. Prolonged use or high doses of glucocorticoids can lead to several side effects, such as weight gain, mood changes, osteoporosis, and increased susceptibility to infections.
 Hyperaldosteronism
Hyperaldosteronism
Familial hyperaldosteronism
Feline hyperaldosteronism
Adrenalism
Glucocorticoid remediable aldosteronism
Primary aldosteronism
Antihypertensive drug
Secondary hypertension
Hypokalemia
Aldosterone escape
Michael Palese
Paraneoplastic syndrome
Ectopic hormone
Adrenocortical hyperfunction
Kearns-Sayre syndrome
Pharmacodynamics of spironolactone
Bartter syndrome
Hypoaldosteronism
Pyloric stenosis
Frederic Bartter
Leuprorelin
Adrenocortical adenoma
Spironolactone
Aldosterone-to-renin ratio
Aldosterone
Jerome W. Conn
Apparent mineralocorticoid excess syndrome
Glucocorticoid
Michał Lityński
Cat health
Hyperaldosteronism - Wikipedia
 Primary and secondary hyperaldosteronism: MedlinePlus Medical Encyclopedia
Primary and secondary hyperaldosteronism: MedlinePlus Medical Encyclopedia
 Hyperaldosteronism: Practice Essentials, Pathophysiology, Etiology
Hyperaldosteronism: Practice Essentials, Pathophysiology, Etiology
 Lack of cardiac fibrosis in a new model of high prorenin hyperaldosteronism
Lack of cardiac fibrosis in a new model of high prorenin hyperaldosteronism
Dopamine reduces aldosterone and 18-hydroxycorticosterone response to angiotensin II in patients with essential low-renin...
 Primary Aldosteronism (Hyperaldosteronism) | Cedars-Sinai
Primary Aldosteronism (Hyperaldosteronism) | Cedars-Sinai
 Help cats with hyperaldosteronism hold their heads high
Help cats with hyperaldosteronism hold their heads high
 Sodium depletion and secondary hyperaldosteronism in outpatients with an ileostomy: a cross-sectional study - Videnskabeligt...
Sodium depletion and secondary hyperaldosteronism in outpatients with an ileostomy: a cross-sectional study - Videnskabeligt...
Hyperaldosteronism: Background, Pathophysiology, Etiology
 Quick Facts: Hyperaldosteronism - MSD Manual Consumer Version
Quick Facts: Hyperaldosteronism - MSD Manual Consumer Version
 HYPERALDOSTERONISM, FAMILIAL, TYPE II; HALD2 | MENDELIAN.CO
HYPERALDOSTERONISM, FAMILIAL, TYPE II; HALD2 | MENDELIAN.CO
 DailyMed - SPIRONOLACTONE tablet
DailyMed - SPIRONOLACTONE tablet
 Sodium Imbalance With Excessive Urination | livestrong
Sodium Imbalance With Excessive Urination | livestrong
 Aldosteronism glucocorticoid remediable familial hyperaldosteronism type I GRA Archieven - Amsterdam UMC Genome Diagnostics
Aldosteronism glucocorticoid remediable familial hyperaldosteronism type I GRA Archieven - Amsterdam UMC Genome Diagnostics
 38 CFR Appendix C to Part 4 - Appendix C to Part 4-Alphabetical Index of Disabilities | Electronic Code of Federal Regulations ...
38 CFR Appendix C to Part 4 - Appendix C to Part 4-Alphabetical Index of Disabilities | Electronic Code of Federal Regulations ...
Sodium depletion and secondary hyperaldosteronism in outpatients with an ileostomy: a cross-sectional study - Publications
RXQ RX H
 Endocrine Surgery Fellowship
Endocrine Surgery Fellowship
 Adrenocortical Carcinoma Treatment (PDQ®) - NCI
Adrenocortical Carcinoma Treatment (PDQ®) - NCI
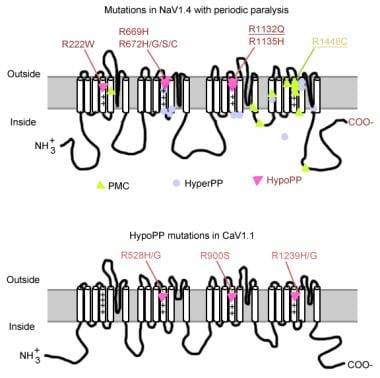
Periodic Paralyses Follow-up: Prognosis, Patient Education
Aldactone, CaroSpir (spironolactone) dosing, indications, interactions, adverse effects, and more
 Dr. Thomas Knox, MD - Cardiology Specialist in Hartford, CT | Healthgrades
Dr. Thomas Knox, MD - Cardiology Specialist in Hartford, CT | Healthgrades
 Endocrinology - Yale New Haven Hospital - Nationally Ranked
Endocrinology - Yale New Haven Hospital - Nationally Ranked
 Systematic Review of Therapeutic Agents and Long-Term Outcomes of Familial Hyperaldosteronism Type 1. | Hypertension;80(7):...
Systematic Review of Therapeutic Agents and Long-Term Outcomes of Familial Hyperaldosteronism Type 1. | Hypertension;80(7):...
 Hypokalemia | Diagnosaurus
Hypokalemia | Diagnosaurus
Torsade de Pointes: Overview, Pathophysiology, Etiology of Torsade
JCI - Spironolactone ameliorates PIT1-dependent vascular osteoinduction in klotho-hypomorphic mice
 Steroid Hormone Pathway
Steroid Hormone Pathway
 Secondary Hypertension - Harvard Health
Secondary Hypertension - Harvard Health
 Dr. Sarena Ravi, MD, Endocrinology, Diabetes & Metabolism Specialist - Silverdale, WA | Sharecare
Dr. Sarena Ravi, MD, Endocrinology, Diabetes & Metabolism Specialist - Silverdale, WA | SharecareSymptoms of hyperaldosteronism2
- Contact your provider for an appointment if you develop symptoms of hyperaldosteronism. (medlineplus.gov)
- What are the symptoms of hyperaldosteronism? (msdmanuals.com)
Primary20
- This cause of mineralocorticoid excess is primary hyperaldosteronism reflecting excess production of aldosterone by adrenal zona glomerulosa. (wikipedia.org)
- It can be asymptomatic, but these symptoms may be present: Fatigue Headache High blood pressure Hypokalemia Hypernatraemia Hypomagnesemia Intermittent or temporary paralysis Muscle spasms Muscle weakness Numbness Polyuria Polydipsia Tingling Metabolic alkalosis Nocturia Blurry Vision Dizziness/Vertigo The causes of primary hyperaldosteronism are adrenal hyperplasia and adrenal adenoma (Conn's syndrome). (wikipedia.org)
- These cause hyperplasia of aldosterone-producing cells of the adrenal cortex resulting in primary hyperaldosteronism. (wikipedia.org)
- citation needed] When taking a blood test, the aldosterone-to-renin ratio is abnormally increased in primary hyperaldosteronism, and decreased or normal but with high renin in secondary hyperaldosteronism. (wikipedia.org)
- citation needed] Primary aldosteronism (hyporeninemic hyperaldosteronism) was previously thought to be most commonly caused by an adrenal adenoma, termed Conn's syndrome. (wikipedia.org)
- Adrenal carcinoma is an extremely rare cause of primary hyperaldosteronism. (wikipedia.org)
- Hyperaldosteronism can be primary or secondary. (medlineplus.gov)
- Primary hyperaldosteronism is due to a problem of the adrenal glands themselves. (medlineplus.gov)
- Primary hyperaldosteronism caused by an adrenal gland tumor is often treated with surgery. (medlineplus.gov)
- The outlook for primary hyperaldosteronism is good with early diagnosis and treatment. (medlineplus.gov)
- Primary hyperaldosteronism may be asymptomatic, particularly in its early stages. (medscape.com)
- The aldosterone-to-renin ratio (ARR)-that is, the ratio of plasma aldosterone (expressed in ng/dL) to plasma renin activity (PRA, expressed in ng/mL/h)-is the most sensitive means of differentiating primary from secondary causes of hyperaldosteronism. (medscape.com)
- Primary aldosteronism (hyperaldosteronism) is a condition that occurs when the adrenal glands produce too much aldosterone, the hormone responsible for balancing potassium and sodium in the body. (cedars-sinai.org)
- Although ANP levels are clearly increased in hyperaldosteronism, neither ANP nor dopamine has been implicated as a primary cause of clinically disordered aldosterone secretion. (medscape.com)
- Familial hyperaldosteronism type II (FH-II) is a heritable form of primary aldosteronism (PA) characterized by hypertension of varying severity, and non glucocticoid remediable hyperaldosteronism. (mendelian.co)
- Primary hyperaldosteronism: Initiate treatment at 100 to 400 mg in preparation for surgery. (nih.gov)
- Primary hyperaldosteronism, or excess aldosterone production as a result of a tumor, can cause high blood sodium. (livestrong.com)
- Familial hyperaldosteronism type 1 (FH1), previously known as glucocorticoid -remediable aldosteronism , was the first identified monogenic cause of primary aldosteronism . (bvsalud.org)
- This talk will focus on hyperaldosteronism, specifically, its primary form, and commonly referred to as primary aldosteronism (PA). (aacc.org)
- The term primary indicates the hypersecretory defect is at the adrenal glands, as opposed to secondary in which the hyperaldosteronism is of extra-adrenal origin. (aacc.org)
Idiopathic1
- 2. As compared with the other groups, an exaggerated angiotensin II-induced response of plasma aldosterone and 18-OH-B levels was observed in the five patients with low-renin essential hypertension (LREH) and in five patients with idiopathic hyperaldosteronism (IHA). (portlandpress.com)
Secondary11
- These act either by decreasing circulating fluid volume or by decreasing cardiac output, with resulting increase in renin release leading to secondary hyperaldosteronism. (wikipedia.org)
- Secondary hyperaldosteronism can also be caused by proximal renal tubular acidosis Secondary hyperaldosteronism can also be a symptom of genetic conditions Bartter's Syndrome and Gitelman's Syndrome. (wikipedia.org)
- Features Hypertension Hypokalemia (e.g., may cause muscle weakness) Alkalosis Investigations High serum aldosterone Low serum renin High-resolution CT abdomen Management Adrenal adenoma: surgery Bilateral adrenocortical hyperplasia: aldosterone antagonist, e.g., spironolactone Secondary hyperaldosteronism (also hyperreninism, or hyperreninemic hyperaldosteronism) is due to overactivity of the renin-angiotensin-aldosterone system (RAAS). (wikipedia.org)
- Likewise, fibromuscular dysplasia may cause stenosis of the renal artery, and therefore secondary hyperaldosteronism. (wikipedia.org)
- Secondary hyperaldosteronism can also be caused by excessive ingestion of licorice or other members of the Glycyrrhiza genus of plants that contain the triterpenoid saponin glycoside known as glycyrrhizin. (wikipedia.org)
- Secondary hyperaldosteronism is due to a problem elsewhere in the body that causes the adrenal glands to release too much aldosterone. (medlineplus.gov)
- Secondary hyperaldosteronism is treated with medicines (as described above) and limiting salt intake. (medlineplus.gov)
- The outlook for secondary hyperaldosteronism depends on the cause of the condition. (medlineplus.gov)
- A high proportion of patients with an ileostomy may be chronically sodium depleted, indicated by absent urinary sodium excretion, secondary hyperaldosteronism and chronic renal impairment, despite normal standard biochemical tests. (ku.dk)
- Hyponatraemia was interpreted as being secondary to prolonged diarrhoea and vomiting, hypokalaemia to stool losses, metabolic alkalosis to extra cellular compartment contraction and the initial but transient rise in blood pressure to secondary hyperaldosteronism. (who.int)
- was low with only slightly elevated levels contraction and the initial but transient of serum renin (320 ng/dL at rest and rise in blood pressure to secondary standing) and aldosterone (195 ng/dL hyperaldosteronism. (who.int)
Hypertension2
- Most had early-onset hypertension but variable hypokalemia , hyperaldosteronism , and hyporeninemia. (bvsalud.org)
- Spironolactone could be prescribed to help remedy high hypertension, hyperaldosteronism, low potassium levels, or water retention. (maroon5.com)
Occurs when the adrenal glands1
- Hyperaldosteronism occurs when the adrenal glands release too much aldosterone. (medlineplus.gov)
Familial1
- Systematic Review of Therapeutic Agents and Long-Term Outcomes of Familial Hyperaldosteronism Type 1. (bvsalud.org)
Mineralocorticoid1
- [ 1 , 2 ] Hyperaldosteronism represents part of a larger entity of hypermineralocorticoidism that may be caused by aldosterone, its mineralocorticoid precursors, or defects that modulate aldosterone effects on its target tissues. (medscape.com)
Treat hyperaldosteronism1
- How do doctors treat hyperaldosteronism? (msdmanuals.com)
Renal1
- Based on the abnormal FE potassium , and the association of renal disease in cheetahs with adrenocortical hyperplasia, 2 further diagnostics are currently in progress to rule out hyperaldosteronism as a cause of the electrolyte abnormality. (vin.com)
Adrenal gland3
- Hyperaldosteronism is a disorder in which the adrenal gland releases too much of the hormone aldosterone into the blood. (medlineplus.gov)
- Surgical excision of the affected adrenal gland is recommended for all patients with hyperaldosteronism who have a proven aldosterone-producing adenoma (APA). (medscape.com)
- In both sexes, overall rates of other disorders of adrenal gland and Cushing's syndrome were lower than for adrenal insufficiency but higher than for hyperaldosteronism, adrenogenital disorders, and adrenomedullary hyperfunction. (health.mil)
Spironolactone1
- Spironolactone is the most effective drug for controlling the effects of hyperaldosteronism, though it may interfere with the progression of puberty. (medscape.com)
Hypokalemia1
- Hyperaldosteronism is a medical condition wherein too much aldosterone is produced by the adrenal glands, which can lead to lowered levels of potassium in the blood (hypokalemia) and increased hydrogen ion excretion (alkalosis). (wikipedia.org)
Sodium1
- Hyperaldosteronism is characterized by excessive secretion of aldosterone, which causes increases in sodium reabsorption and loss of potassium and hydrogen ions. (medscape.com)
Cushing1
- Diseases associated with excessive cortical hormone production include hyperaldosteronism and Cushing syndrome. (aacc.org)
Doctors2
- How do doctors tell if I have hyperaldosteronism? (msdmanuals.com)
- was caused by hyperaldosteronism.1 2006, Plaintiff also began Her doctors believed it (Id. (justia.com)
High1
- Treating hyperaldosteronism focuses on reducing your aldosterone levels or blocking the effects of aldosterone, high blood pressure, and low blood potassium. (moviecultists.com)
Block1
- Erection problems and enlarged breast tissue in men ( gynecomastia ) may occur with long-term use of medicines to block the effect of hyperaldosteronism. (medlineplus.gov)
Forms of hyperaldosteronism2
- There are other forms of hyperaldosteronism that are not familial. (medlineplus.gov)
- The clinical presentation resembles that of the other familial forms of hyperaldosteronism (FH-I, FH-II) (see these terms). (rareguru.com)
Adrenal Hyperplasia2
- It can be asymptomatic, but these symptoms may be present: Fatigue Headache High blood pressure Hypokalemia Hypernatraemia Hypomagnesemia Intermittent or temporary paralysis Muscle spasms Muscle weakness Numbness Polyuria Polydipsia Tingling Metabolic alkalosis Nocturia Blurry Vision Dizziness/Vertigo The causes of primary hyperaldosteronism are adrenal hyperplasia and adrenal adenoma (Conn's syndrome). (wikipedia.org)
- An important condition to be considered in the differential diagnosis of primary hyperaldosteronism is congenital adrenal hyperplasia . (medscape.com)
Cause of primary hyperaldosteronism2
- Adrenal carcinoma is an extremely rare cause of primary hyperaldosteronism. (wikipedia.org)
- The cause of primary hyperaldosteronism is considered to be an abnormality in one or both the adrenal glands. (alwaysayurveda.net)
Increased in primary hyperaldosteronism1
- citation needed] When taking a blood test, the aldosterone-to-renin ratio is abnormally increased in primary hyperaldosteronism, and decreased or normal but with high renin in secondary hyperaldosteronism. (wikipedia.org)
Aldosteronism4
- A rare heritable form of primary aldosteronism (PA) that is characterized by early-onset severe hypertension, non- glucocorticoid-remediable hyperaldosteronism, overproduction of 18-oxocortisol and 18-hydroxycortisol, and profound hypokalemia. (nih.gov)
- citation needed] Primary aldosteronism (hyporeninemic hyperaldosteronism) was previously thought to be most commonly caused by an adrenal adenoma, termed Conn's syndrome. (wikipedia.org)
- Aldosteronism may be classified into three types, primary hyperaldosteronism (Conn's syndrome), secondary hyperaldosteronism, and pseudohyperaldosteronism. (wikidoc.org)
- Hyperaldosteronism, also commonly known as aldosteronism, is a disorder in which the adrenal glands produce abnormally high levels of aldosterone, which can lead to decreased levels of potassium in the blood. (naturalcurefor.com)
Secretion of aldosterone2
- Primary hyperaldosteronism can caused by aldosterone -secreting adenoma , bilateral hyperplasia of the adrenal glands, and ectopic secretion of aldosterone from ovaries and kidneys. (wikidoc.org)
- Hyperaldosteronism is characterized by excessive secretion of aldosterone, which causes increases in sodium reabsorption and loss of potassium and hydrogen ions. (medscape.com)
Renin6
- These act either by decreasing circulating fluid volume or by decreasing cardiac output, with resulting increase in renin release leading to secondary hyperaldosteronism. (wikipedia.org)
- Features Hypertension Hypokalemia (e.g., may cause muscle weakness) Alkalosis Investigations High serum aldosterone Low serum renin High-resolution CT abdomen Management Adrenal adenoma: surgery Bilateral adrenocortical hyperplasia: aldosterone antagonist, e.g., spironolactone Secondary hyperaldosteronism (also hyperreninism, or hyperreninemic hyperaldosteronism) is due to overactivity of the renin-angiotensin-aldosterone system (RAAS). (wikipedia.org)
- Primary hyperaldosteronism features overproduction of aldosterone despite suppressed plasma renin activity (PRA). (wikidoc.org)
- Secondary hyperaldosteronism is caused by high renin and subsequently aldosterone level, such as renovascular causes and reninoma. (wikidoc.org)
- Pseudohyperaldosteronism is the clinical presentation of hyperaldosteronism such as resistant hypertension , hypokalemia , and metabolic alkalosis due to factors other than renin and aldosterone . (wikidoc.org)
- Renin activity is elevated in renal vascular diseases and suppressed in primary hyperaldosteronism. (loinc.org)
Glucocorticoid-remediable2
- In familial hyperaldosteronism type I (FH-I), glucocorticoid-remediable PAL is caused by inheritance of an ACTH-regulated, hybrid CYP11B1/CYP11B2 gene. (nih.gov)
- Familial hyperaldosteronism type II is not glucocorticoid-remediable, and is clinically, biochemically and morphologically indistinguishable from apparently sporadic PAL. (nih.gov)
Treatment at 1001
- Primary hyperaldosteronism: Initiate treatment at 100 to 400 mg in preparation for surgery. (nih.gov)
Hyperplasia3
- These cause hyperplasia of aldosterone-producing cells of the adrenal cortex resulting in primary hyperaldosteronism. (wikipedia.org)
- Bartter FC et al: Hyperplasia of the juxtaglomerular complex with hyperaldosteronism and hypokalemic alkalosis: a new syndrome. (medprep.info)
- In bilateral hyperaldosteronism, aldosterone-producing diffuse hyperplasia and aldosterone-producing micronodules or nodules are the major subtypes. (go.jp)
Diagnosis3
- The outlook for primary hyperaldosteronism is good with early diagnosis and treatment. (nih.gov)
- SPECT/CT can identify small adenomas (0.8-1.5 cm) even in patients with chronic renal disease where the biochemical diagnosis of primary hyperaldosteronism is difficult. (medscape.com)
- The diagnosis of hyperaldosteronism will require both, the physical examination and the laboratory diagnosis. (alwaysayurveda.net)
Symptoms5
- When Do Symptoms of Familial hyperaldosteronism type III Begin? (nih.gov)
- Contact your provider for an appointment if you develop symptoms of hyperaldosteronism. (nih.gov)
- What are the symptoms of hyperaldosteronism? (merckmanuals.com)
- Hyperaldosteronism, a condition marked by the overproduction of the hormone aldosterone, often lurks undetected behind a façade of seemingly benign symptoms. (localquoter.net)
- Hyperaldosteronism can play a relentless game of hide-and-seek with one's health, making the correlation of symptoms to the disorder a critical step toward reclaiming well-being. (localquoter.net)
Mineralocorticoid excess2
- This cause of mineralocorticoid excess is primary hyperaldosteronism reflecting excess production of aldosterone by adrenal zona glomerulosa. (wikipedia.org)
- Hyperaldosteronism is a clinical scenario of mineralocorticoid excess with resistant hypertension , hypokalemia , and metabolic alkalosis due to increased hydrogen ion excretion. (wikidoc.org)
Tumors1
- The primary cases (which present tumors in adrenal glands) of hyperaldosteronism are usually managed with surgery. (alwaysayurveda.net)
Secondary hypertension1
- Hyperaldosteronism - a condition in which the adrenal glands produce too much aldosterone - is the most common cause of secondary hypertension. (drugtargetreview.com)
Primary and secondary3
- The terms "primary" and "secondary" are often used to describe the level and/or type of abnormality in Hyperaldosteronism. (naturalcurefor.com)
- Increased levels of the mineralocorticoid, aldosterone, are present in primary and secondary hyperaldosteronism. (nih.gov)
- Hyperaldosteronism is tentatively classified into primary and secondary types. (go.jp)
Genetic3
- The genetic cause of familial hyperaldosteronism type II is unknown. (medlineplus.gov)
- Among the subsets of PA, 3 familiar cases of dex-suppressible hyperaldosteronism were recognized, with characteristically high levels of aldo, 18-OH-B, 18-OH-cortisol and 18-oxo-cortisol, due to the genetic abnormalities of the 11-18 hydroxylase system. (unipd.it)
- Commenting on their new findings, Ze'ev Ronai , Ph.D., Chief Scientific Advisor of SBP and senior author of the study, said: "Our research, based on a genetic model, identifies an unexpected layer in the regulation of adrenal gland development and in hyperaldosteronism. (drugtargetreview.com)
Caused by an adrenal1
- Primary hyperaldosteronism caused by an adrenal gland tumor is often treated with surgery. (nih.gov)
Adenoma2
- Aldosterone producing adenoma (APA) and idiopathic hyperaldosteronism (IHA) were the most frequent forms, 51% and 44% respectively. (unipd.it)
- Hyperaldosteronism most commonly results in the invasion of high levels of adenoma. (naturalcurefor.com)
Hormone5
- Familial hyperaldosteronism is a group of inherited conditions in which the adrenal glands, which are small glands located on top of each kidney, produce too much of the hormone aldosterone . (medlineplus.gov)
- Hyperaldosteronism is a disorder in which the adrenal gland releases too much of the hormone aldosterone into the blood. (nih.gov)
- In hyperaldosteronism, you have too much of the adrenal hormone called aldosterone. (merckmanuals.com)
- The term hyperaldosteronism refers to the excessive amount of a hormone namely aldosterone. (alwaysayurveda.net)
- Hyperaldosteronism is therefore an endocrine disorder which is a result of abnormality in one or both the adrenal glands thus resulting in the hyper or too much secretion of the aldosterone hormone. (alwaysayurveda.net)
Metabolic1
- Hyponatraemia was interpreted as being secondary to prolonged diarrhoea and vomiting, hypokalaemia to stool losses, metabolic alkalosis to extra cellular compartment contraction and the initial but transient rise in blood pressure to secondary hyperaldosteronism. (who.int)
Endocrinology1
- Patients that suffer from hyperaldosteronism exhibit mutations or epigenetic deregulation of the key pathway components, pointing to the relevance of our findings to humans and the justification for further exploration of this pathway for therapeutic purposes," finishes Constantine Stratakis , M.D., Head of the Section on Endocrinology and Genetics at the National Institute of Child Health and Human Development (NICHD) at the NIH, and co-author of the study. (drugtargetreview.com)
Potassium1
- In hyperaldosteronism, the adrenal glands produce too much aldosterone, leading to low levels of potassium and increased sodium. (drugtargetreview.com)
Genetics2
- Reference Link Familial hyperaldosteronism Genetics Home Reference. (rareguru.com)
- 8. Genetics of primary hyperaldosteronism. (nih.gov)
Mutations1
- Familial hyperaldosteronism type III is caused by mutations in the KCNJ5 gene. (medlineplus.gov)
Type5
- In most individuals with familial hyperaldosteronism type III, the adrenal glands are enlarged up to six times their normal size. (medlineplus.gov)
- Familial hyperaldosteronism type II appears to be the most common variety. (medlineplus.gov)
- Familial hyperaldosteronism type I is caused by the abnormal joining together (fusion) of two similar genes called CYP11B1 and CYP11B2 , which are located close together on chromosome 8. (medlineplus.gov)
- Don't fight Familial hyperaldosteronism type III alone. (rareguru.com)
- Connect with other caregivers and patients with Familial hyperaldosteronism type III and get the support you need. (rareguru.com)
Patients1
- If patients suspected of Hyperaldosteronism are in some form of medication for high blood pressure, it's imperative for physicians to order that these drugs be stopped for a duration prior to the tests. (naturalcurefor.com)
Clinically1
- Secondary hyperaldosteronism can be distinguished clinically and biochemically from primary hyperaldosteronism. (medscape.com)